
A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review



1
College of Nursing, The Ohio State University, 1585 Neil Ave, Columbus, OH 43210, USA
2
VA Cooperative Studies Program Coordinating Center, Boston, MA 02111, USA
3
School of Medicine, Case Western Reserve University, Cleveland, OH 44106, USA
*
Author to whom correspondence should be addressed.
Diabetology 2023, 4(3), 323-338; https://doi.org/10.3390/diabetology4030028
Submission received: 1 July 2023
/
Revised: 4 August 2023
/
Accepted: 10 August 2023
/
Published: 14 August 2023
(This article belongs to the Special Issue Exclusive Papers Collection of Editorial Board Members in Diabetology)
{kind=link}
{kind=link}
Abstract
:Diabetes is an independent risk factor for cognitive impairment, with the latter presenting challenges for diabetes self-management and glycemic control in individuals with type 2 diabetes. Predicated on the theory of unpleasant symptoms, the purpose of the current narrative review of the literature was to identify etiologic factors that influence cognitive impairment as a precursor to dementia in individuals with diabetes. Physiological, psychological, and situational factors were recognized as important life course components of cognitive impairment in later adulthood. Developing interventions targeting modifiable factors is warranted in preventing cognitive impairment in adults with diabetes.
1. Introduction
Diabetes is a risk factor for dementia resulting from vascular or neurodegenerative changes [1]. In 2021, approximately 537 million people worldwide had diabetes, predicted to increase to 783 million people by 2045 [2]. Study indicates that 45% of adults with type 2 diabetes experience mild cognitive impairment, and this prevalence has been increasing as the world’s population ages [3]. Individuals with diabetes have a significantly higher likelihood of developing cognitive impairment and experiencing subjective cognitive decline (SCD) than individuals without diabetes [4,5]. Given that cognitive impairment precedes dementia [6], it is important to identify factors that predict cognitive impairment in individuals with diabetes.
Cognitive impairment in diabetes is defined as a loss of ability in major cognitive domains, such as memory, attention, processing speed, learning, and executive function [1]. Cognitive impairment can exacerbate conditions such as hearing loss, chronic pain, and physical disabilities [1]. Individuals with type 2 diabetes and cognitive impairment experience difficulties with concentration and attention, frequent forgetfulness, and slower processing speed [7]. SCD is one of the first symptoms of cognitive impairment [8], and it predicts worsening memory abilities and a faster rate of subsequent memory decline [9]. SCD may also interfere with one’s ability to participate in activities, such as taking medication [10].
Diabetes is related to cognitive impairment through pathophysiological mechanisms [11,12]. Chronic hyperglycemia and hypoglycemic events are risk factors for cognitive impairment and dementia in type 2 diabetes [12,13]. Hyperglycemia may hasten cognitive impairment by accelerating larger vessel disease and reducing capillary perfusion in the brain [14], and it may also affect multiple brain regions (i.e., white and gray matter in the frontal lobe) involved in cognitive performance [15]. Furthermore, insulin resistance in type 2 diabetes may affect insulin signaling and reception in the brain, which can accelerate cognitive impairment [16,17,18]. Individuals with poor glycemic control are at a high risk of memory impairment, decreased volume of the hippocampus [19], and cognitive decline [20].
Cognitive impairment in type 2 diabetes may negatively affect diabetes self-management. A significant negative correlation has been found between impairment of executive function and self-management in older adults with type 2 diabetes. Moreover, cognitive impairment can hamper the achievement of optimal glycemic control [21]. Patients with type 2 diabetes and cognitive impairment had significantly lower levels of self-management than those with type 2 diabetes who do not have cognitive impairment [22]. Specifically, patients with cognitive impairment are less likely to adhere to their diet and exercise regimens [23]. Consequently, cognitive impairment may lead to poor glycemic control, diabetes-related complications, and more frequent hospital admissions [24].
Controlling modifiable factors is central to preventing and slowing the progression of cognitive impairment and dementia in individuals with diabetes and avoiding severe diabetes-related complications. Thus, it is important to thoroughly examine the multiple factors contributing to SCD and cognitive impairment in diabetes. This is especially salient, noting that brain structure and cognitive impairment symptoms in individuals with diabetes across the lifespan may be influenced by multiple factors [25], not solely the presence of diabetes. However, studies have predominantly focused on disease-related factors, frequently overlooking the impact of an individual’s early life and situational factors surrounding individuals. Although prior studies have examined multiple factors (i.e., genetics, comorbidities, and depression) associated with cognitive impairment [26], there is limited literature using life course trajectory to examine factors of cognitive impairment in adults with diabetes. The purpose of this narrative review was to apply the theory of unpleasant symptoms from the life course perspective to better understand the association between multiple factors and cognitive impairment in individuals with diabetes. Furthermore, we aimed to identify the possible influencing factors contributing to SCD and cognitive impairment and to provide future directions for the amelioration of these concerns.
2. The Theory of Unpleasant Symptoms
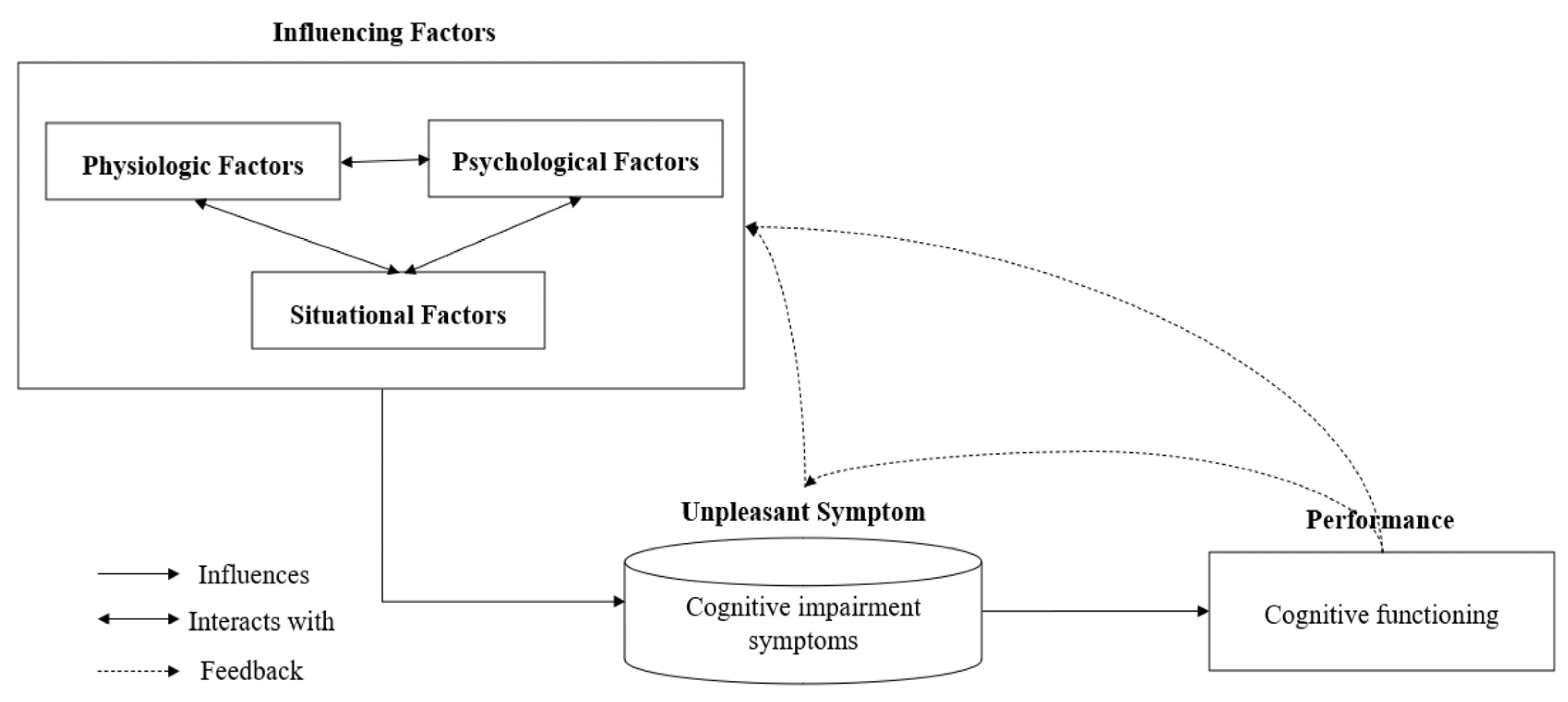
The theory of unpleasant symptoms views the multiple factors that contribute to the experience of unpleasant symptoms and performance [27]. The theory encompasses three main components: (a) influencing factors (physiological, situational, and psychological factors), (b) unpleasant symptoms, and (c) performance.
Physiological influencing factors include genetic, disease-related, physiological, and anatomical variables (i.e., age, race/ethnicity, nutrition status, inflammation response attributable to infection, variation in energy or hormonal levels, and disease duration and stage). Psychological influencing factors encompass both cognitive and affective variables, including a person’s level of knowledge about their disease, mood, and affective state. Situational influencing factors include one’s social/physical environment (i.e., culture, access to social support/health care, socioeconomic status, lifestyle behaviors, family status, and occupation). All these factors are interrelated and can affect a person’s experience of unpleasant symptoms. The consequences of symptom experience could impact performance, which is one’s ability to perform or function cognitively, physically, and socially (Figure 1).
3. Life Course Perspective
According to the life course approach, the development of cognitive function is a dynamic process that is impacted by cumulative life experiences, and one’s health is shaped by adaptations made over the lifespan [28]. Cognitive function is formed by multiple factors operating across the life course, from prenatal to later adulthood [29]. The prenatal period is the starting point for people’s cognitive development, and the peak of cognitive functioning is reached in the mid-20s, followed by a decline that begins in middle adulthood (mid-40s), which is a critical point for comprehending the trajectory of cognitive functioning. Cognitive ability in later adulthood is affected by the accumulation of the influences of risk factors (i.e., environment, demographics, and lifestyle) throughout a person’s life [30]. Adults between 45 years and 65 years of age (middle adulthood) comprise the age group most frequently newly diagnosed with diabetes [31]; thus, middle adulthood is a crucial period for understanding the cognitive impairment trajectory because diabetes is an independent risk factor for cognitive impairment [1].
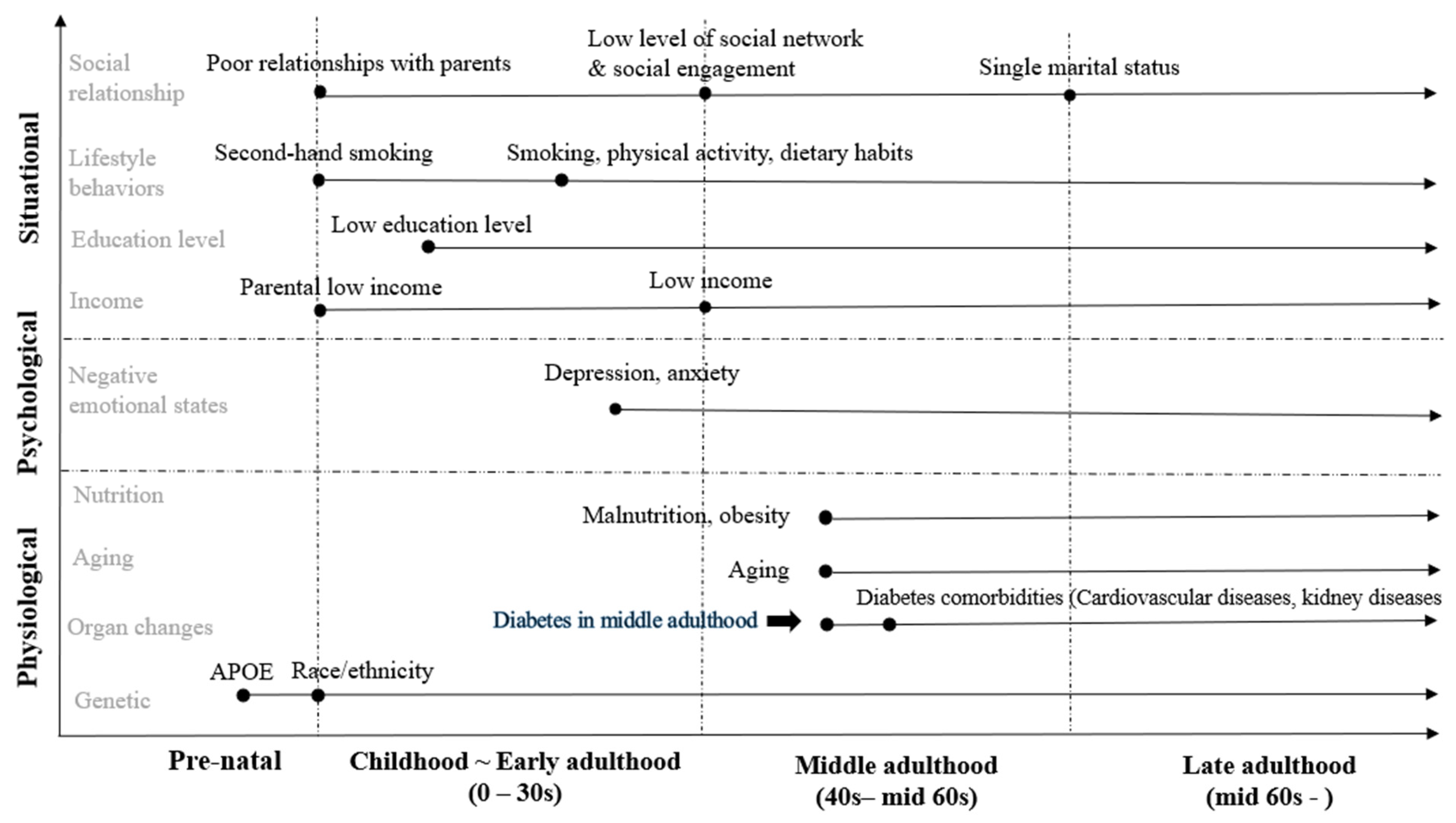
Taking a life course perspective on cognitive impairment may enhance preventive efforts [32]. Therefore, this study aimed to apply a life course perspective to the theory of unpleasant symptoms to better understand the trajectory of cognitive impairment in adults with diabetes. We identified potential influencing factors (i.e., physiological, psychological, and situational factors based on the theory of unpleasant symptoms) across four periods of the lifespan: the prenatal period, childhood to early adulthood, middle adulthood, and late adulthood that might contribute to cognitive impairment symptoms in middle and later life in patients with diabetes.
4. Physiological Factors and Cognitive Impairment
Recent studies have indicated that physiological factors, such as genetic factors, aging, sex, nutritional status, and diabetes comorbidities, are linked to a greater risk of cognitive impairment [1,17,33].
4.1. Apolipoprotein E (APOE) Gene
In the prenatal stage, a genetic predisposition toward cognitive decline may be established. Recent studies have reported a link between the APOE gene and cognitive impairment in patients with diabetes [34]. The literature indicates that APOE ε4 carriers exhibit poorer performance on a range of cognitive tasks in late adulthood, particularly tasks that assess executive function, global cognition, and memory [35,36,37,38]. The prevalence of Alzheimer’s dementia was found to be approximately 50% in individuals who were carriers of the APOE ε4 gene. Furthermore, there are differences between ethnic groups; the highest prevalence of the APOE ε4 carrier was found in people from Northern Europe and the lowest in those from Southern Europe and Asia [39]. Prior studies have also found a link between APOE and the risk of type 2 diabetes [40,41]. Moreover, the APOE E3/E4 genotype is a strong predictor of CVD in adults with type 2 diabetes [42]. The presence of the APOE e4 allele in adults with diabetes showed an increase in the development of dementia [33].
4.2. Aging
Middle adulthood has been characterized by cognitive decline, particularly related to executive function, processing speed, and learning [43]. The effects of aging on cognitive function are extensive and have several etiologies. The volume of the brain area, which is important in memory, decreases as people become older [44]. Additionally, the accumulation of the amyloid beta protein with aging can contribute to the loss of grey matter volume [45]. Amyloid beta and the loss of brain volume may be related to an increased risk of cognitive impairment over time [44]. Furthermore, the severity of SCD in memory function was found to be linked to the aggregation of amyloid beta plaques in the frontal cortex [46]. Middle-aged adults with diabetes could aggravate cognitive impairment. A large longitudinal cohort study among middle-aged adults demonstrated that individuals with type 2 diabetes experienced an accelerated cognitive decline than those without diabetes. Specifically, adults with type 2 diabetes exhibited a 45% faster decline in memory, 29% in reasoning, and 24% in global cognitive scores in 10 years compared with individuals without diabetes [47]. Duration of diabetes and glycemic control are major factors contributing to cognitive impairment in middle-aged adults with diabetes [47]. Similar findings were also reported in the community-based Atherosclerosis Risk in Communities (ARIC) Study among middle-aged adults [20].
4.3. Sex
The presence of sex differences may be associated with cognitive function in middle and later adulthood in patients with type 2 diabetes. To date, the impact of sex-specificity on cognitive impairment in patients with diabetes remains unclear. Evidence indicated that females with type 2 diabetes were more likely to have a higher risk of cognitive impairment and dementia than males with type 2 diabetes. A cross-sectional study found that the presence of diabetes was linked to an increased risk of brain atrophy in females but not in males [48]. Another study showed that females with type 2 diabetes were associated with worse cognitive function than males [49]. Additionally, a longitudinal study involving patients with type 2 diabetes found that females had an accelerated rate of cognitive decline partially mediated by depression compared with males [50].
4.4. Nutritional Status
Nutritional status, including obesity, malnutrition, and unintentional loss of body weight, is associated with cognitive impairment in adults with diabetes [51,52]. Nutritional state significantly correlates with cognitive function in older adults, and poor nutritional state has a strong correlation with cognitive deterioration [53]. Individuals with diabetes who gained more than 10% of weight were more likely to develop dementia than those who gained less than 5% of weight (Hazard ratios [HR] 1.4, 95% confidence interval [CI]: 1.1–1.8). Similarly, individuals with diabetes who lost more than 10% of their weight increased the risk of dementia incidence than those who lost less than 5% (HR 1.3, 95% CI: 1.1–1.6) [51].
Obesity has a strong association with cognitive impairment in patients with type 2 diabetes. Obesity is prevalent in individuals with type 2 diabetes, and it could lead to insulin resistance [54]. According to a cross-sectional study, higher body mass index (BMI) in adults aged 50 and over with type 2 diabetes was linked to poor cognitive function [49]. Furthermore, a longitudinal study in older adults with type 2 diabetes found that central fat distribution and total fat mass were associated with cognitive decline after a 2-year follow-up [55]. However, there is controversy surrounding the relationship between obesity and cognitive impairment in patients with type 2 diabetes. Some evidence suggests that obesity may have a protective effect against cognitive decline. A study demonstrated that obesity was associated with better cognitive function in adults with type 2 diabetes [56].
4.5. Diabetes Comorbidities
Individuals with type 2 diabetes have a high risk of developing diabetes-related comorbidities, such as cardiovascular disease (CVD) and kidney disease, that may affect cognitive impairment [57]. Poor glycemic control over the long term can lead to an increased prevalence of CVD in late adulthood [58]. Chronic hyperglycemia leads to oxidative stress and an inflammatory response, resulting in cell damage and dyslipidemia [59]. This, in turn, contributes to the formation of atherosclerotic plaques, leading to cardiovascular disease. CVD can influence cognitive impairment by accelerating brain aging and causing vascular brain injuries such as ischemia, hypoxic events, and blood-brain barrier leakage [18]. Older adults with diabetes are particularly at increased risk of developing CVD, which is a significant predictor of mild cognitive impairment [60]. According to a six-year observational study, severe systolic hypertension co-existing with diabetes significantly increased the risk of developing dementia and its subtypes, such as vascular dementia [61].
Reduced kidney function may increase the risk of cognitive impairment and dementia. For example, amyloid beta is typically cleared by the kidney or liver. However, poor kidney function can lead to inadequate clearance of amyloid beta [62]. Consequently, the accumulation of amyloid beta may contribute to the development of Alzheimer’s disease. A cross-sectional study among middle-aged adults with type 2 diabetes revealed that individuals with albuminuria demonstrated significantly lower scores in tests assessing executive function, memory, and processing speed than those without kidney disease [63]. Additionally, a study found that decreased estimated glomerular filtration rate and albuminuria were associated with abnormal brain magnetic resonance imaging and poor cognitive function in adults with type 2 diabetes [64].
5. Psychological Factors and Cognitive Impairment
Increasingly, evidence indicates that psychological factors are associated with cognitive impairment and SCD in individuals with diabetes. Negative emotional states (i.e., repeated stress exposure, depression, and anxiety) may be predictors of cognitive impairment and dementia in individuals with diabetes [65,66]. Among adults with SCD, 34% experienced mental distress, and mental health co-morbidities in diabetes are commonly associated with cognitive impairment [1]. Higher levels of depressive symptoms and anxiety are associated with more subjective memory decline [67].
Depressive and Anxiety Symptoms
Depressive and anxiety symptoms in both middle and later adulthood may affect SCD [68] and cognitive impairment in patients with diabetes [66]. The onset of depression in middle adulthood and depression in late adulthood has been associated with a greater risk of cognitive impairment [69,70]. Depressive symptoms are also strongly related to cognitive impairment in middle adulthood, late adulthood, and early adulthood [71]. Depression is associated with a high risk of CVD and the presence of vascular lesions on magnetic resonance images [72], which can lead to brain neuronal damage [73]. Depression may lead to hypothalamic–pituitary–adrenal axis dysregulation, resulting in increased glucocorticoid secretion, which hampers negative feedback. Increased cortisol levels can damage memory areas in the brain in patients with type 2 diabetes [74]. Anxiety may accelerate brain aging through the accumulation of beta-amyloid plaques, resulting in a faster rate of decline in cognitive function. Over a 10-year period, severe anxiety in mid-adulthood was linked to a greater risk of dementia [75]. Furthermore, high levels of anxiety can negatively affect attention and lead to cognitive impairment in late adulthood [76]. Adults with type 2 diabetes usually have a high prevalence of microvascular dysfunction, which impairs cerebral processes and contributes to cognitive impairment and depression [77]. A longitudinal study found that females had a higher tendency to experience depressive symptoms, and longer duration of diabetes and lower levels of education were linked to the presence of anxiety symptoms and cognitive impairment among individuals with type 2 diabetes [78].
6. Situational Factors and Cognitive Impairment
Considerable evidence indicates that situational factors can accelerate cognitive decline in late adulthood. Many recent studies have shown that social factors (i.e., socioeconomic status, marital status, educational level, lifestyle behaviors, and social relationships) are linked to a greater risk of cognitive impairment [17].
6.1. Socioeconomic Status (SES)
Low SES is a well-known influencing factor in cognitive impairment. Low SES may affect cognitive function through many mechanisms, including unhealthy dietary habits and physical inactivity [79]. A low level of education, occupation status, and low income were predictors of cognitive impairment in adults with type 2 diabetes [80]. Mounting data suggests that SES in early life can influence cognitive function in later adulthood [81]. For example, exposure to famine during childhood has been associated with impaired executive function in adulthood [82]. Additionally, individuals with a low SES in early life are more likely to experience environmental toxins, repeated stress, poor nutrition, and poor social relationships that could influence cognitive impairment in middle and later adulthood [83,84].
Education is regarded as one of the SES factors that influence cognitive function in later adulthood [85]. Higher educational attainment can be a dampening factor in the development of cognitive impairment in diabetes [86,87]. The association between educational attainment and cognitive impairment can be explained by the cognitive reserve theory, suggesting that mental stimulation in early life provides an extra capacity for cognition to compensate for cognitive decline in later adulthood [88]. Education level is negatively associated with cognitive impairment in older adults with diabetes. For example, older adults with type 2 diabetes who have completed tertiary education have a 95% lower risk of developing cognitive impairment than those with an education level below primary school [89]. Additionally, higher levels of education in early life are associated with a slower cognitive decline in later life, which is mediated by higher income [90]. Conversely, lower levels of education are related to a decline in cognitive function in older adults with diabetes [91,92,93].
6.2. Lifestyle Behaviors
Unhealthy behaviors, such as physical activity, smoking, and dietary habits, are regarded as the major modifiable factors in diabetes for mitigating progressive cognitive impairment [94]. Additionally, physical inactivity, smoking, and alcohol consumption are associated with SCD [95].
6.2.1. Smoking
Smoking is known to be associated with cognitive impairment, but the underlying mechanisms are unclear. It is believed that carbon monoxide present in tobacco smoke may interrupt the provision of oxygen to the brain, which could affect cognitive function through vascular pathways. Exposure to second-hand smoke during childhood is also related to cognitive impairment in middle and later adulthood [96,97]. Additionally, smoking may decrease insulin secretion and increase insulin resistance in adults with diabetes [98]. Nicotine may stimulate the secretion of hormones, such as growth hormone, catecholamines, and cortisol, which counteract the effects of insulin and increase insulin resistance [99]. Consequently, increased insulin resistance may lead to the accumulation of amyloid β-protein and abnormal tau phosphorylation, which subsequently increases the risk of Alzheimer’s disease [100].
Recent studies have shown that individuals who currently smoke cigarettes have a higher risk of developing mild cognitive impairment than those who do not smoke. Among adults with diabetes, current smokers have a 3.6 times higher risk of developing mild cognitive impairment than individuals who do not smoke [101]. Smokers also tend to suffer from SCD more than non-smokers in middle and later adulthood [95]. The long-term effects of smoking in terms of pack years can increase the risk of cognitive impairment and accelerate cognitive decline in people with diabetes, affecting global cognitive performance [101,102]. Specifically, each additional pack-year smoked was found to increase the likelihood of a speed-up four-year cognitive decline by 1% [102].
6.2.2. Physical Activity
Accumulating evidence indicates that physical activity plays a role as a protective factor against cognitive impairment. Adequate physical activity is associated with enhanced memory function [103]. Most of all, healthy eating and exercise habits can affect proper glycemic control, which, in turn, can positively affect cognitive function. Physical activity improves glycemic control by increasing insulin sensitivity and the use of glucose by the peripheral blood vessels [104]. Furthermore, moderate physical activity can influence cognitive function across the life course, including working memory, and can reduce simple reaction time [105]. In middle and later adulthood, individuals with diabetes with a higher physical activity level are more likely to have better memory function [106], while individuals experiencing SCD tend to have lower levels of physical activity [107]. Moreover, evidence suggests that higher physical activity has been linked to a larger hippocampal volume, and older adults with type 2 diabetes who participate in more moderate-to-vigorous physical activity tend to exhibit improved attention-processing speed [108].
6.2.3. Diet
In the prenatal stage, maternal undernutrition can lead to accelerated cognitive impairment in later adulthood [109]. Additionally, maternal gestational diabetes can increase the risk of type 2 diabetes and obesity in fetuses later in life [110]. Interestingly, patients with intrauterine exposure to diabetes tended to grow up to prefer high-fat and sweet foods [111]. Evidence shows that early-life dietary patterns are related to cognitive impairment in later life. For example, an unhealthy diet and obesity in early life can negatively affect psychological status and cognitive function [112]. In middle and later adulthood, poor diet, including the consumption of packaged foods and frequent alcohol use, are linked to cognitive impairment in individuals with type 2 diabetes [113]. Poor diet patterns can cause an increased risk of diabetes that leads to accelerated cognitive impairment. The Mediterranean diet, which is characterized by a reduced intake of meat and saturated fat and an increased intake of vegetables, fruits, and fish, can positively influence cognitive function, specifically verbal memory, in older adults [114]. Thus, healthy eating habits may be a protective factor against cognitive impairment in individuals with diabetes.
6.3. Social Relationship
A growing body of studies suggested that social relationships are considered influencing factors for progressive cognitive impairment. Some studies have reported that adversity in childhood (i.e., poor childhood relationships with parents and insufficient social support) can negatively influence cognitive impairment in middle and later adulthood [115,116]. This early-life stress causes brain changes associated with cognitive function [117] and can also indirectly affect cognitive impairment through negative emotions, such as depression [118].
Strong social support is linked to improved cognitive function and reduced cognitive impairment in later adulthood [119]. Interestingly, social engagement and family function can mitigate cognitive impairment in diabetes, as social networks may have positive impacts on cognitive functioning, and social engagement is related to a lower risk of cognitive impairment [120]. Individuals with larger social networks and more social engagement are more likely to have better diabetes self-management behaviors, which decrease the risk of diabetes-related cognitive impairment [121]; thus, there may be a pathway that associates social relationships and cognitive impairment. Moreover, adults who live alone but engage in social interaction (i.e., family, friends, and neighbors) less frequently tend to experience SCD in middle and later adulthood [95]. In individuals with diabetes, single marital status was shown to be associated with cognitive impairment, possibly because unmarried adults had fewer opportunities to interact and communicate with others [93].
Social relationships have both objective and subjective aspects, and each aspect is varied and complex [122]. Individuals who lack social relationships and social connections may experience loneliness, which has also been linked to cognitive impairment in middle and later adulthood [123]. Loneliness is defined as the subjectively perceived difference between an individual’s actual social relationships and their desired social relationships. It is distinct from social isolation, which is defined as an objective deficit of social interactions and ties [124]. Individuals who are lonely could experience emotional distress, such as depression and anxiety, leading to metabolic syndrome through poor health behaviors (i.e., a lack of physical activity participation and functional limitations) [125]. Loneliness can also have an impact on cognitive impairment through physical health problems, including increased systolic blood pressure [126]. Additionally, loneliness mediated the relationship between social isolation and SCD in late adulthood of diabetes and was significantly related to SCD [127]. However, since the evidence between loneliness and cognitive impairment in individuals with diabetes is still scarce, more studies are needed.
Taken together, multiple influencing factors may affect cognitive impairment in individuals with diabetes, and the accumulation of these factors can accelerate cognitive decline in later adulthood (Figure 2). Some factors are latent modifiable factors and thus may be targeted for intervention to slow or prevent the progression of cognitive impairment and dementia in patients with diabetes.
7. Discussion and Future Directions
The paper discusses the possible influencing factors that may contribute to SCD and cognitive impairment in individuals with type 2 diabetes across the lifespan, based on the theory of unpleasant symptoms. The life course approach framework is valuable for understanding these complex factors, as the degree to which they contribute to cognitive impairment risk in middle-aged and older adults with type 2 diabetes depends on the life course trajectory.
According to the life course theory, the development of cognitive reserve may be affected by one’s life and experiences, and the accumulation of risk factors has a significant impact on cognitive impairment in middle-aged and older adults [128]. The influencing factors guided by the theory of unpleasant symptoms discussed in this article may help develop interventions tailored to individual levels based on exposures and experiences across the life span. Identifying and controlling modifiable factors may help prevent the development of cognitive impairment and dementia in individuals with type 2 diabetes. This approach is consistent with the findings of a recent study on cognitive impairment in type 2 diabetes [113], which highlighted the importance of modifiable factors in preventive strategies for cognitive impairment in individuals with diabetes.
The theory of unpleasant symptoms predicates that the influencing factors may affect an individual’s performance (i.e., cognitive functioning, including executive function, memory and learning, motor function, and processing speed) through cognitive impairment symptoms [27]. One notable feature of this conceptual framework is that influencing factors and cognitive impairment symptoms affect cognitive functioning which can impact diabetes self-management. Effective executive function is significantly associated with the long-term performance of diabetes self-management behaviors [129], and cognitive impairment may lead to poor self-management behaviors, resulting in poor glycemic control [11,130], which further contributes to cognitive impairment. Thus, it is crucial to consider the relationship between influencing factors, cognitive impairment, and self-management in diabetes. In addition, healthcare providers must be aware of the association between poor diabetes self-management and cognitive impairment in middle-aged and older adults with type 2 diabetes. Despite the relationship between diabetes and cognitive impairment, most clinicians tend to overlook the diagnosis of cognitive impairment in individuals with type 2 diabetes [131]. Clinical assessment of cognitive impairment and clinical guidelines for older adults with type 2 diabetes are needed [132].
We present several future research directions based on our conceptual framework. First, interventions targeting modifiable influencing factors (i.e., lifestyle behaviors) should be developed to prevent cognitive impairment in middle-aged and older adults with diabetes. We recommend conducting longitudinal intervention studies that combine cognitive training and lifestyle changes in physical activity and healthy eating habits to improve cognitive ability and diabetes self-management behaviors. Second, future studies are needed to examine the potential pathways of the effect of cognitive impairment on diabetes self-management through mediating or moderating factors (i.e., physiological, psychological, and situational factors) in middle-aged and older adults with type 2 diabetes. Impaired memory and executive functions may negatively affect multiple aspects of diabetes self-management [130]. Little is known about the role of mediating factors in the association between cognitive impairment and diabetes self-management. However, psychological factors, such as depression, may play a crucial role in this relationship. Third, future studies directly targeting education on the links between cognitive impairment and diabetes for middle-aged adults and older adults with diabetes, particularly for patients with low SES, low educational attainment, and racial minority groups, are needed.
There are some limitations to this review. First, the theory of unpleasant symptoms does not include spiritual factors [133]. A systematic review examined the effects of religion and spirituality on cognitive ability and found that spirituality could protect against cognitive impairment in middle-aged and older adults [134]. Religious and spiritual factors may affect cognitive impairment through various mechanisms [135]. For instance, coping strategies promoted by spiritual and religious practices may positively affect mental health outcomes [134,136], which can affect the memory areas in the brain through reductions in cortisol levels [134]. In addition, spirituality and religion can protect against cognitive impairment by promoting social engagement activities, including praying, singing, and studying the Bible in a group setting [137]. Future studies should consider the role of spiritual factors in the prevention of cognitive impairment. Second, although the theory of unpleasant symptoms presumes that influencing factors interact with each other and all such factors are intertwined in each life course trajectory, this review does not systemically identify these interactions. For example, loneliness, social support, and depression in older adults are interrelated and influence each other [138,139]. In future studies, it will be necessary to closely examine the intricate relationships between influencing factors.
In contrast to a comprehensive systemic review, we aimed to present information in such a way to be easily comprehended by a reader who is not necessarily well-versed on the topic. Thus, the focus of this narrative review was to provide a succinct, best-evidence synthesis of the literature, only highlighting those articles that we trust conveyed the key points needing to be emphasized while striving for parsimony. This involved screening and condensing a vast array of data into a brief constructive critique to benefit the reader. We opted not to include a lengthy table outlining the various details of each study in the literature (e.g., author names, country of publication, institution, research design, sample size, advantages, and disadvantages) but rather refer interested readers to our carefully selected reference list or the various systematic reviews on the topic.
8. Conclusions
In this narrative review, we have applied a life course perspective to the theory of unpleasant symptoms, presented a conceptual framework based on the theory for addressing the development of cognitive impairment in type 2 diabetes, and discussed future directions. This paper identifies the influencing factors in cognitive impairment symptoms across four periods of the lifespan. Also, this paper demonstrates that multiple influencing factors, including physiological, psychological, and situational factors, may affect cognitive impairment in individuals with type 2 diabetes over the life course trajectory. Each of these variables should be considered in developing effective interventions to prevent dementia and slow cognitive decline. It is important to note that cognitive impairment in adults with type 2 diabetes is associated with diabetes self-management. Therefore, healthcare providers must understand the effect of cognitive impairment on self-management in individuals with type 2 diabetes.
Author Contributions
Conceptualization, B.K. and J.H.; investigation, B.K.; methodology, B.K. and J.H.; writing—original draft preparation, B.K.; writing—review and editing, J.T.E. and J.H.; validation, J.T.E. and J.H.; visualization, B.K.; supervision: J.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed.
Conflicts of Interest
The authors have no competing interest to declare.
References
- Munshi, M.N. Cognitive dysfunction in older adults with diabetes: What a clinician needs to know. Diabetes Care 2017, 40, 461–467. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- You, Y.; Liu, Z.; Chen, Y.; Xu, Y.; Qin, J.; Guo, S.; Huang, J.; Tao, J. The prevalence of mild cognitive impairment in type 2 diabetes mellitus patients: A systematic review and meta-analysis. Acta Diabetol. 2021, 58, 671–685. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-C.; Cuevas, H.E.; Zuñiga, J.A.; García, A.A. Predictors of subjective cognitive decline among people with diabetes: Data from the Behavioral Risk Factor Surveillance System. Sci. Diabetes Self-Manag. Care 2021, 47, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Varghese, S.M.; Joy, N.; John, A.M.; George, G.; Chandy, G.M.; Benjamin, A.I. Sweet memories or not? A comparative study on cognitive impairment in diabetes mellitus. Front. Public Health 2022, 10, 822062. [Google Scholar] [CrossRef] [PubMed]
- Cadar, D. A Life Course Approach to Dementia Prevention. J. Aging Geriatr. Med. 2017, 1, 1–6. [Google Scholar]
- Kodl, C.T.; Seaquist, E.R. Cognitive dysfunction and diabetes mellitus. Endocr. Rev. 2008, 29, 494–511. [Google Scholar] [CrossRef] [Green Version]
- Jessen, F.; Amariglio, R.E.; van Boxtel, M.; Breteler, M.; Ceccaldi, M.; Chételat, G.; Dubois, B.; Dufouil, C.; Ellis, K.A.; van der Flier, W.M.; et al. A conceptual framework for research on subjective cognitive decline in preclinical Alzheimer’s disease. Alzheimers Dement. 2014, 10, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Samieri, C.; Proust-Lima, C.; Glymour, M.M.; Okereke, O.I.; Amariglio, R.E.; Sperling, R.A.; Rentz, D.M.; Grodstein, F. Subjective cognitive concerns, episodic memory, and the APOE Ε4 allele. Alzheimers Dement. 2014, 10, 752–759.e1. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Subjective Cognitive Decline—A Public Health Issue. Available online: http://www.cdc.gov/aging/healthybrain/ (accessed on 13 May 2022).
- Sinclair, A.; Abdelhafiz, A. Cognitive dysfunction in older adults with type 2 diabetes: Links, risks, and clinical implications. Clin. Geriatr. Med. 2020, 36, 407–417. [Google Scholar] [CrossRef]
- Van Bussel, F.C.G.; Backes, W.H.; Van Veenendaal, T.M.; Hofman, P.A.M.; Van Boxtel, M.P.J.; Schram, M.T.; Sep, S.J.S.; Dagnelie, P.C.; Schaper, N.; Stehouwer, C.D.A.; et al. Functional brain networks are altered in type 2 diabetes and prediabetes: Signs for compensation of cognitive decrements? The Maastricht study. Diabetes 2016, 65, 2404–2413. [Google Scholar] [CrossRef] [Green Version]
- Crane, P.K.; Walker, R.; Hubbard, R.A.; Li, G.; Nathan, D.M.; Zheng, H.; Haneuse, S.; Craft, S.; Montine, T.J.; Kahn, S.E.; et al. Glucose levels and risk of dementia. N. Engl. J. Med. 2013, 369, 540–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cukierman-Yaffe, T.; McClure, L.A.; Risoli, T.; Bosch, J.; Sharma, M.; Gerstein, H.C.; Benavente, O. The relationship between glucose control and cognitive function in people with diabetes after a lacunar stroke. J. Clin. Endocrinol. Metab. 2021, 106, E1521–E1528. [Google Scholar] [CrossRef] [PubMed]
- Mortby, M.E.; Janke, A.L.; Anstey, K.J.; Sachdev, P.S.; Cherbuin, N. High “Normal” blood glucose is associated with decreased brain volume and cognitive performance in the 60s: The PATH through life study. PLoS ONE 2013, 8, e73697. [Google Scholar] [CrossRef] [Green Version]
- Snyder, H.M.; Corriveau, R.A.; Craft, S.; Faber, J.E.; Greenberg, S.M.; Knopman, D.; Lamb, B.T.; Montine, T.J.; Nedergaard, M.; Schaffer, C.B.; et al. Vascular contributions to cognitive impairment and dementia including Alzheimer’s disease. Alzheimers Dement. 2015, 11, 710–717. [Google Scholar] [CrossRef] [Green Version]
- Xue, M.; Xu, W.; Ou, Y.N.; Cao, X.P.; Tan, M.S.; Tan, L.; Yu, J.T. Diabetes mellitus and risks of cognitive impairment and dementia: A systematic review and meta-analysis of 144 prospective studies. Ageing Res. Rev. 2019, 55, 100944. [Google Scholar] [CrossRef]
- Cholerton, B.; Baker, L.D.; Montine, T.J.; Craft, S. Type 2 diabetes, cognition, and dementia in older adults: Toward a precision health approach. Diabetes Spectr. 2016, 29, 210–219. [Google Scholar] [CrossRef] [Green Version]
- Kerti, L.; Veronica Witte, A.; Winkler, A.; Ulrike Grittner, M.; Rujescu, D.; Flöel, A. Higher glucose levels associated with lower memory and reduced hippocampal microstructure. Neurology 2013, 81, 1746–1752. [Google Scholar] [CrossRef]
- Rawlings, A.M.; Sharrett, A.R.; Schneider, A.L.C.; Coresh, J.; Albert, M.; Couper, D.; Griswold, M.; Gottesman, R.F.; Wagenknecht, L.E.; Windham, B.G.; et al. Diabetes in midlife and cognitive change over 20 years: A cohort study. Ann. Intern. Med. 2014, 161, 785–793. [Google Scholar] [CrossRef] [Green Version]
- Thabit, H.; Kennelly, S.M.; Bhagarva, A.; Ogunlewe, M.; McCormack, P.M.E.; McDermott, J.H.; Sreenan, S. Utilization of frontal assessment battery and executive interview 25 in assessing for dysexecutive syndrome and its association with diabetes self-care in elderly patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2009, 86, 208–212. [Google Scholar] [CrossRef]
- Świątoniowska-Lonc, N.; Polański, J.; Tański, W.; Jankowska-Polańska, B. Impact of cognitive impairment on adherence to treatment and self-care in patients with type 2 diabetes mellitus. Diabetes Metab. Syndr. Obes. 2021, 14, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Feil, D.G.; Zhu, C.W.; Sultzer, D.L. The relationship between cognitive impairment and diabetes self-management in a population-based community sample of older adults with type 2 diabetes. J. Behav. Med. 2012, 35, 190–199. [Google Scholar] [CrossRef]
- Biessels, G.J.; Despa, F. Cognitive decline and dementia in diabetes mellitus: Mechanisms and clinical implications. Nat. Rev. Endocrinol. 2018, 14, 591–604. [Google Scholar] [CrossRef] [PubMed]
- Sperling, R.A.; Aisen, P.S.; Beckett, L.A.; Bennett, D.A.; Craft, S.; Fagan, A.M.; Iwatsubo, T.; Jack, C.R.; Kaye, J.; Montine, T.J.; et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement. 2011, 7, 280–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, N.L.; Unverzagt, F.; LaMantia, M.A.; Khan, B.A.; Boustani, M.A. Risk factors for the progression of mild cognitive impairment to dementia. Clin. Geriatr. Med. 2013, 29, 873–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenz, E.R.; Pugh, L.C.; Milligan, R.A.; Gift, A.; Suppe, F. The middle-range theory of unpleasant symptoms: An update. Adv. Nurs. Sci. 1997, 19, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.L.; Gilman, S.E.; Cheng, T.L.; Drury, S.S.; Hill, C.; Geronimus, A.T. Life course approaches to the causes of health disparities. Am. J. Public Health 2019, 109, 48–55. [Google Scholar] [CrossRef]
- Richards, M.; Deary, I.J. A life course approach to cognitive capability. In A Life Course Approach to Healthy Ageing; Kua, D., Cooper, R., Hardy, R., Richards, M., Ben-Shlomo, Y., Eds.; Oxford University Press: Oxford, UK, 2013; pp. 32–45. [Google Scholar] [CrossRef]
- Anstey, K. Enhancing cognitive capacities over the life-span. In Population Ageing and Australia’s Future; ANU Press: Canberra, Australia, 2016; pp. 165–183. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report Website. Available online: https://www.cdc.gov/diabetes/data/statistics-report/index.html (accessed on 10 June 2022).
- Banerjee, D.; Mukhopadhyay, S.; Michael D’cruz, M.; Rodriguez, F.S. Life-course pathways to cognitive aging: The significance of intellectual stimulation in the form of education and occupation for public policy and prevention plans. Front. Psychiatry 2021, 12, 719609. [Google Scholar] [CrossRef]
- Gudala, K.; Bansal, D.; Schifano, F.; Bhansali, A. Diabetes mellitus and risk of dementia: A meta-analysis of prospective observational studies. J. Diabetes Investig. 2013, 4, 640–650. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, T.; Umemura, T.; Hotta, N. Cognitive impairment in diabetic patients: Can diabetic control prevent cognitive decline? J. Diabetes Investig. 2012, 3, 413–423. [Google Scholar] [CrossRef] [Green Version]
- O’Donoghue, M.C.; Murphy, S.E.; Zamboni, G.; Nobre, A.C.; Mackay, C.E. APOE genotype and cognition in healthy individuals at risk of Alzheimer’s disease: A review. Cortex 2018, 104, 103–123. [Google Scholar] [CrossRef] [PubMed]
- Quintino-Santos, S.; Diniz, B.S.; Firmo, J.O.A.; Moriguchi, E.H.; Lima-Costa, M.F.; Castro-Costa, E. APOE ε4 allele is associated with worse performance in memory dimensions of the mini-mental state examination: The Bambuí Cohort Study of Aging. Int. J. Geriatr. Psychiatry 2015, 30, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Izaks, G.J.; Gansevoort, R.T.; van der Knaap, A.M.; Navis, G.; Dullaart, R.P.F. The association of APOE genotype with cognitive function in persons aged 35 years or older. PLoS ONE 2011, 6, 27415. [Google Scholar] [CrossRef] [Green Version]
- Kerchner, G.A.; Berdnik, D.; Shen, J.C.; Bernstein, J.D.; Fenesy, M.C.; Deutsch, G.K.; Wyss-Coray, T.; Rutt, B.K. APOE ε4 worsens hippocampal CA1 apical neuropil atrophy and episodic memory. Neurology 2014, 82, 691–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, A.; Crean, S.; Mercaldi, C.J.; Collins, J.M.; Boyd, D.; Cook, M.N.; Arrighi, H.M. Prevalence of apolipoprotein E4 genotype and homozygotes (APOE e4/4) among patients diagnosed with Alzheimer’s disease: A systematic review and meta-analysis. Neuroepidemiology 2012, 38, 1–17. [Google Scholar] [CrossRef] [PubMed]
- El-Lebedy, D.; Raslan, H.M.; Mohammed, A.M. Apolipoprotein E gene polymorphism and risk of type 2 diabetes and cardiovascular disease. Cardiovasc. Diabetol. 2016, 15, 12. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, R.; Likidlilid, A.; Peerapatdit, T.; Tresukosol, D.; Srisuma, S.; Ratanamaneechat, S.; Sriratanasathavorn, C. Apolipoprotein E gene polymorphism: Effects on plasma lipids and risk of type 2 diabetes and coronary artery disease. Cardiovasc. Diabetol. 2012, 11, 36. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Liu, J.; Weng, R.; Gu, X.; Zhong, Z. Apolipoprotein E gene polymorphism and the risk of cardiovascular disease and type 2 diabetes. BMC Cardiovasc. Disord. 2019, 19, 213. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Rajagopal, L.; Ferreira, D.; Barroso, J.; Machado, A.; Molina, Y.; Nieto, A.; Correia, R.; Westman, E. Cognitive variability during middle-age: Possible association with neurodegeneration and cognitive reserve. Front. Aging Neurosci. 2017, 9, 188. [Google Scholar] [CrossRef] [Green Version]
- Harada, C.N.; Natelson Love, M.C.; Triebel, K. Normal cognitive aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef] [Green Version]
- Rodrigue, K.M.; Kennedy, K.M.; Park, D.C. Beta-amyloid deposition and the aging brain. Neuropsychol. Rev. 2009, 19, 436–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gerson Unschuld, P.; Araujo, T.; Bischof, G.N.; Schwarz, C.; Lange, C.; Benson, G.S.; Horn, N.; Wurdack, K.; Lukas, M.; Buchert, R.; et al. Severity of subjective cognitive complaints and worries in older adults are associated with cerebral amyloid-β load. Front. Aging Neurosci. 2021, 13, 675583. [Google Scholar] [CrossRef]
- Tuligenga, R.H.; Dugravot, A.; Tabák, A.G.; Elbaz, A.; Brunner, E.J.; Kivimäki, M.; Singh-Manoux, A. Midlife type 2 diabetes and poor glycaemic control as risk factors for cognitive decline in early old age: A post-hoc analysis of the Whitehall II cohort study. Lancet Diabetes Endocrinol. 2014, 2, 228–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, E.G.; Rhodius-Meester, H.; Exalto, L.; Peters, S.A.E.; van Bloemendaal, L.; Ponds, R.; Muller, M. Sex-specific associations of diabetes with brain structure and function in a geriatric population. Front. Aging Neurosci. 2022, 14, 885787. [Google Scholar] [CrossRef] [PubMed]
- Mallorquí-Bagué, N.; Lozano-Madrid, M.; Toledo, E.; Corella, D.; Salas-Salvadó, J.; Cuenca-Royo, A.; Vioque, J.; Romaguera, D.; Martínez, J.A.; Wärnberg, J.; et al. Type 2 diabetes and cognitive impairment in an older population with overweight or obesity and metabolic syndrome: Baseline cross-sectional analysis of the PREDIMED-plus study. Sci. Rep. 2018, 8, 16128. [Google Scholar] [CrossRef] [Green Version]
- Verhagen, C.; Janssen, J.; Biessels, G.J.; Johansen, O.E.; Exalto, L.G. Females with type 2 diabetes are at higher risk for accelerated cognitive decline than males: CAROLINA-COGNITION study. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 355–364. [Google Scholar] [CrossRef]
- Nam, G.E.; Park, Y.G.; Han, K.; Kim, M.K.; Koh, E.S.; Kim, E.S.; Lee, M.K.; Kim, B.; Hong, O.K.; Kwon, H.S. BMI, weight change, and dementia risk in patients with new-onset type 2 diabetes: A Nationwide Cohort Study. Diabetes Care 2019, 42, 1217–1224. [Google Scholar] [CrossRef]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition management in older adults with diabetes: A review on the importance of shifting prevention strategies from metabolic syndrome to frailty. Nutrients 2020, 12, 3367. [Google Scholar] [CrossRef]
- Malara, A.; Sgrò, G.; Caruso, C.; Ceravolo, F.; Curinga, G.; Renda, G.F.; Spadea, F.; Garo, M.; Rispoli, V. Relationship between cognitive impairment and nutritional assessment on functional status in Calabrian long-term-care. Clin. Interv. Aging 2014, 9, 105–110. [Google Scholar] [CrossRef] [Green Version]
- The GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Abbatecola, A.M.; Lattanzio, F.; Spazzafumo, L.; Molinari, A.M.; Cioffi, M.; Canonico, R.; DiCioccio, L.; Paolisso, G. Adiposity predicts cognitive decline in older persons with diabetes: A 2-year follow-up. PLoS ONE 2010, 5, e10333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xing, Z.; Long, C.; Hu, X.; Chai, X. Obesity is associated with greater cognitive function in patients with type 2 diabetes mellitus. Front. Endocrinol. 2022, 13, 953826. [Google Scholar] [CrossRef] [PubMed]
- Nowakowska, M.; Zghebi, S.S.; Ashcroft, D.M.; Buchan, I.; Chew-Graham, C.; Holt, T.; Mallen, C.; Van Marwijk, H.; Peek, N.; Perera-Salazar, R.; et al. The comorbidity burden of type 2 diabetes mellitus: Patterns, clusters and predictions from a large English primary care cohort. BMC Med. 2019, 17, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cukierman-Yaffe, T.; Gerstein, H.C.; Williamson, J.D.; Lazar, R.M.; Lovato, L.; Miller, M.E.; Coker, L.H.; Murray, A.; Sullivan, M.D.; Marcovina, S.M.; et al. Relationship between baseline glycemic control and cognitive function in individuals with type 2 diabetes and other cardiovascular risk factors the action to control cardiovascular risk in diabetes-memory in diabetes (ACCORD-MIND) trial. Diabetes Care 2009, 32, 221–226. [Google Scholar] [CrossRef] [Green Version]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [Green Version]
- Gorska-Ciebiada, M.; Saryusz-Wolska, M.; Ciebiada, M.; Loba, J. Mild cognitive impairment and depressive symptoms in elderly patients with diabetes: Prevalence, risk factors, and comorbidity. J. Diabetes Res. 2014, 2014, 179648. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.C.; Hsu, J.L.; Tung, H.Y.; Chou, C.C.; Bai, C.H. Increased dementia risk predominantly in diabetes mellitus rather than in hypertension or hyperlipidemia: A population-based cohort study. Alzheimers Res. Ther. 2017, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Xiang, Y.; Bu, X.-L.; Liu, Y.-H.; Zhu, C.; Shen, L.-L.; Jiao, S.-S.; Zhu, X.-Y.; Giunta, B.; Tan, J.; Song, W.-H.; et al. Physiological amyloid-beta clearance in the periphery and its therapeutic potential for Alzheimer’s disease. Acta Neuropathol. 2015, 130, 487–499. [Google Scholar] [CrossRef] [Green Version]
- Barzilay, J.I.; Younes, N.; Pop-Busui, R.; Florez, H.; Seaquist, E.; Falck-Ytter, C.; Luchsinger, J.A. The cross-sectional association of renal dysfunction with tests of cognition in middle-aged adults with early type 2 diabetes. J. Diabetes Complicat. 2021, 35, 107805. [Google Scholar] [CrossRef]
- Freedman, B.I.; Sink, K.M.; Hugenschmidt, C.E.; Hughes, T.M.; Williamson, J.D.; Whitlow, C.T.; Palmer, N.D.; Miller, M.E.; Lovato, L.C.; Xu, J.; et al. Associations of early kidney disease with brain magnetic resonance imaging and cognitive function in African Americans with type 2 diabetes mellitus. Am. J. Kidney Dis. 2017, 70, 627–637. [Google Scholar] [CrossRef]
- De Vito, A.; Calamia, M.; Greening, S.; Roye, S. Aging, The association of anxiety, depression, and worry symptoms on cognitive performance in older adults. Neuropsychol. Dev. Cognition. Sect. B Aging Neuropsychol. Cogn. 2019, 26, 161–173. [Google Scholar] [CrossRef]
- Chow, Y.Y.; Verdonschot, M.; McEvoy, C.T.; Peeters, G. Associations between depression and cognition, mild cognitive impairment and dementia in persons with diabetes mellitus: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 2022, 185, 109227. [Google Scholar] [CrossRef] [PubMed]
- Sabatini, S.; Woods, R.T.; Ukoumunne, O.C.; Ballard, C.; Collins, R.; Clare, L. Associations of subjective cognitive and memory decline with depression, anxiety, and two-year change in objectively-assessed global cognition and memory. Neuropsychol. Dev. Cognition. Sect. B Aging Neuropsychol. Cogn. 2022, 29, 840–866. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, C.; Zhu, B.; Fritschi, C. Subjective cognitive decline in diabetes: Associations with psychological, sleep, and diabetes-related factors. J. Adv. Nurs. 2021, 77, 693–702. [Google Scholar] [CrossRef]
- Yang, W.; Li, X.; Pan, K.-Y.; Yang, R.; Song, R.; Qi, X.; Pedersen, N.L.; Xu, W. Association of life-course depression with the risk of dementia in late life: A nationwide twin study. Alzheimers Dement. 2021, 17, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Legdeur, N.; Heymans, M.W.; Comijs, H.C.; Huisman, M.; Maier, A.B.; Visser, P.J. Age dependency of risk factors for cognitive decline. BMC Geriatr. 2018, 18, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenowitz, W.D.; Zeki Al Hazzouri, A.; Vittinghoff, E.; Golden, S.H.; Fitzpatrick, A.L.; Yaffe, K. Depressive symptoms imputed across the life course are associated with cognitive impairment and cognitive decline. J. Alzheimers Dis. 2021, 83, 1379–1389. [Google Scholar] [CrossRef] [PubMed]
- Steffens, D.C.; Krishnan, K.R.R.; Crump, C.; Burke, G.L. Cerebrovascular disease and evolution of depressive symptoms in the cardiovascular health study. Stroke 2002, 33, 1636–1644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and management of dementia: Review. JAMA 2019, 322, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.D.; Katon, W.J.; Lovato, L.C.; Miller, M.E.; Murray, A.M.; Horowitz, K.R.; Bryan, R.N.; Gerstein, H.C.; Marcovina, S.; Akpunonu, B.E.; et al. Association of depression with accelerated cognitive decline among patients with type 2 diabetes in the ACCORD-MIND Trial. JAMA Psychiatry 2013, 70, 1041–1047. [Google Scholar] [CrossRef]
- Perna, G.; Iannone, G.; Alciati, A.; Caldirola, D. Are anxiety disorders associated with accelerated aging? A focus on neuroprogression. Neural Plast. 2016, 2016, 8457612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Zhang, X.; Zhu, Y.; Dai, Y.; Liu, T.; Wang, Y. Cognitive impairment in generalized anxiety disorder revealed by event-related potential N270. Neuropsychiatr. Dis. Treat. 2015, 11, 1405–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Sloten, T.T.; Sedaghat, S.; Carnethon, M.R.; Launer, L.J.; Stehouwer, C.D.A. Cerebral microvascular complications of type 2 diabetes: Stroke, cognitive dysfunction, and depression. Lancet Diabetes Endocrinol. 2020, 8, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Trento, M.; Trevisan, M.; Raballo, M.; Passera, P.; Charrier, L.; Cavallo, F.; Porta, M. Depression, anxiety, cognitive impairment and their association with clinical and demographic variables in people with type 2 diabetes: A 4-year prospective study. J. Endocrinol. Investig. 2014, 37, 79–85. [Google Scholar] [CrossRef]
- Chapko, D.; Mccormack, R.; Black, C.; Staff, R.; Murray, A. Life-course determinants of cognitive reserve (CR) in cognitive aging and dementia-a systematic literature review. Aging Ment. Health 2018, 22, 915–926. [Google Scholar] [CrossRef]
- Bhaskar Yerrapragada, D.; Rao, C.R.; Karunakaran, K.; Seow, H.; Lee, E. Cognitive dysfunction among adults with type 2 diabetes mellitus in Karnataka, India. Ochsner J. 2019, 19, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Aartsen, M.J.; Cheval, B.; Sieber, S.; van der Linden, B.W.; Gabriel, R.; Courvoisier, D.S.; Guessous, I.; Burton-Jeangros, C.; Blane, D.; Ihle, A.; et al. Advantaged socioeconomic conditions in childhood are associated with higher cognitive functioning but stronger cognitive decline in older age. Proc. Natl. Acad. Sci. USA 2019, 116, 5478–5486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reichelt, A.C.; Westbrook, R.F.; Morris, M.J. Editorial: Impact of diet on learning, memory and cognition. Front. Behav. Neurosci. 2017, 11, 96. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Waite, L.J. The impact of childhood and adult SES on physical, mental, and cognitive well-being in later life. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2005, 60, S93–S101. [Google Scholar] [CrossRef] [Green Version]
- Hackman, D.A.; Farah, M.J. Socioeconomic status and the developing brain. Trends Cogn. Sci. 2009, 13, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Lyu, J.; Burr, J.A. Socioeconomic status across the life course and cognitive function among older adults: An examination of the latency, pathways, and accumulation hypotheses. J. Aging Health 2016, 28, 40–67. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef] [PubMed]
- Prostran, M.S.; Marra, C.; Li, G.; Xiao, S.; Li, W.; Sun, L. Prevalence, influence factors and cognitive characteristics of mild cognitive impairment in type 2 diabetes mellitus. Front. Aging Neurosci. 2019, 11, 180. [Google Scholar] [CrossRef] [Green Version]
- Stern, Y. What is cognitive reserve? Theory and research application of the reserve concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Suain Bon, R.; Ariaratnam, S.; Mat Saher, Z.; Mohamad, M.; Lee, F.S. Cognitive impairment and its associated risk factors in the elderly with type 2 diabetes mellitus. Front. Psychiatry 2021, 12, 669725. [Google Scholar] [CrossRef]
- Zahodne, L.B.; Stern, Y.; Manly, J.J. Differing effects of education on cognitive decline in diverse elders with low versus high educational attainment. Neuropsychology 2015, 29, 649–657. [Google Scholar] [CrossRef] [Green Version]
- Naguib, R.; Soliman, E.S.; Neimatallah, F.M.; AlKhudhairy, N.S.; ALGhamdi, A.M.; Almosa, R.S.; Aldashash, K.A.; Alkhalifah, B.Y.; Elmorshedy, H. Cognitive impairment among patients with diabetes in Saudi Arabia: A cross-sectional study. Middle East Curr. Psychiatry 2020, 27, 49. [Google Scholar] [CrossRef]
- Kim, C.; Kim, M.J.; Park, C.G. Heterogeneous trajectories of cognitive function in older adults with diabetes: Findings from the Korean Longitudinal Study of Aging (KLoSA). Stress 2019, 27, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Xiu, S.; Liao, Q.; Sun, L.; Chan, P. Risk factors for cognitive impairment in older people with diabetes: A community-based study. Ther. Adv. Endocrinol. Metab. 2019, 10, 2042018819836640. [Google Scholar] [CrossRef] [Green Version]
- Kivipelto, M.; Mangialasche, F.; Ngandu, T. Lifestyle interventions to prevent cognitive impairment, dementia and Alzheimer disease. Nat. Rev. Neurol. 2018, 14, 653–666. [Google Scholar] [CrossRef]
- Roh, M.; Dan, H.; Kim, O. Influencing factors of subjective cognitive impairment in middle-aged and older adults. Int. J. Environ. Res. Public Health 2021, 18, 11488. [Google Scholar] [CrossRef] [PubMed]
- Sabia, S.; Elbaz, A.; Dugravot, A.; Head, J.; Shipley, M.; Hagger-Johnson, G.; Kivimaki, M.; Singh-Manoux, A. Impact of smoking on cognitive decline in early old age: The Whitehall II cohort study. Arch. Gen. Psychiatry 2012, 69, 627–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, J.; Heffernan, T. The cognitive deficits associated with second-hand smoking. Front. Psychiatry 2016, 7, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durlach, V.; Vergès, B.; Al-Salameh, A.; Bahougne, T.; Benzerouk, F.; Berlin, I.; Clair, C.; Mansourati, J.; Rouland, A.; Thomas, D.; et al. Smoking and diabetes interplay: A comprehensive review and joint statement. Diabetes Metab. 2022, 48, 101370. [Google Scholar] [CrossRef]
- Artese, A.; Stamford, B.A.; Moffatt, R.J. Cigarette smoking: An accessory to the development of insulin resistance. Am. J. Lifestyle Med. 2019, 13, 602–605. [Google Scholar] [CrossRef]
- Wei, Z.; Koya, J.; Reznik, S.E. Insulin resistance exacerbates Alzheimer disease via multiple mechanisms. Front. Neurosci. 2021, 15, 687157. [Google Scholar] [CrossRef]
- Sonoda, N.; Morimoto, A.; Ugi, S.; Morino, K.; Sekine, O.; Nemoto, K.; Maegawa, H.; Miyamatsu, N. Smoking status is associated with mild cognitive impairment assessed with the mini-mental state examination in Japanese diabetic patients. Diabetol. Int. 2016, 7, 361–367. [Google Scholar] [CrossRef]
- Feinkohl, I.; Keller, M.; Robertson, C.M.; Morling, J.R.; McLachlan, S.; Frier, B.M.; Deary, I.J.; Strachan, M.W.J.; Price, J.F. Cardiovascular risk factors and cognitive decline in older people with type 2 diabetes. Diabetologia 2015, 58, 1637–1645. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.T. Physical activity and cognitive function in mild cognitive impairment. ASN Neuro 2020, 12, 1759091419901182. [Google Scholar] [CrossRef]
- Park, J.-H.; Lee, Y.-E. Effects of exercise on glycemic control in type 2 diabetes mellitus in Koreans: The fifth Korea National Health and Nutrition Examination Survey (KNHANES V). J. Phys. Ther. Sci. 2015, 27, 3559–3564. [Google Scholar] [CrossRef] [Green Version]
- Fernandes, R.M.; Correa, M.G.; Santos, M.; Almeida, A.P.C.P.S.C.; Fagundes, N.C.F.; Lc, M.; Lima, R.R. The effects of moderate physical exercise on adult cognition: A systematic review. Front. Physiol. 2018, 9, 667. [Google Scholar] [CrossRef] [PubMed]
- Bai, A.; Tao, L.; Huang, J.; Tao, J.; Liu, J. Effects of physical activity on cognitive function among patients with diabetes in China: A nationally longitudinal study. BMC Public Health 2021, 21, 481. [Google Scholar] [CrossRef] [PubMed]
- Wion, R.K.; Hill, N.L.; Depasquale, N.; Mogle, J.; Bratlee-Whitaker, E. The relationship between subjective cognitive impairment and activity participation: A systematic review. Act. Adapt. Aging 2020, 44, 225–245. [Google Scholar] [CrossRef] [PubMed]
- Zabetian-Targhi, F.; Srikanth, V.K.; Beare, R.; Breslin, M.; Moran, C.; Wang, W.; Wu, F.; Smith, K.J.; Callisaya, M.L. The association between physical activity intensity, cognition, and brain structure in people with type 2 diabetes. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 2047–2053. [Google Scholar] [CrossRef]
- De Rooij, S.R.; Wouters, H.; Yonker, J.E.; Painter, R.C.; Roseboom, T.J.; Roberts, M. Prenatal undernutrition and cognitive function in late adulthood. Proc. Natl. Acad. Sci. USA 2010, 107, 16881–16886. [Google Scholar] [CrossRef] [PubMed]
- Dabelea, D.; Hanson, R.L.; Lindsay, R.S.; Pettitt, D.J.; Imperatore, G.; Gabir, M.M.; Roumain, J.; Bennett, P.H.; Knowler, W.C. Intrauterine exposure to diabetes conveys risks for type 2 diabetes and obesity a study of discordant sibships. Diabetes 2000, 49, 2208–2211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gugusheff, J.R.; Ong, Z.Y.; Muhlhausler, B.S. A maternal “junk-food” diet reduces sensitivity to the opioid antagonist naloxone in offspring postweaning. FASEB J. 2013, 27, 1275–1284. [Google Scholar] [CrossRef] [Green Version]
- Spencer, S.J.; Korosi, A.; Layé, S.; Shukitt-Hale, B.; Barrientos, R.M. Food for thought: How nutrition impacts cognition and emotion. NPJ Sci. Food 2017, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Sharma, G.; Parihar, A.; Talaiya, T.; Dubey, K.; Porwal, B.; Parihar, M.S. Cognitive impairments in type 2 diabetes, risk factors and preventive strategies. J. Basic Clin. Physiol. Pharmacol. 2020, 31, 20190105. [Google Scholar] [CrossRef]
- Okubo, H.; Inagaki, H.; Gondo, Y.; Kamide, K.; Ikebe, K.; Masui, Y.; Arai, Y.; Ishizaki, T.; Sasaki, S.; Nakagawa, T.; et al. Association between dietary patterns and cognitive function among 70-year-old Japanese elderly: A cross-sectional analysis of the SONIC study. Nutr. J. 2017, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Majer, M.; Nater, U.M.; Lin, J.-M.S.; Capuron, L.; Reeves, W.C. Association of childhood trauma with cognitive function in healthy adults: A pilot study. BMC Neurol. 2010, 10, 61. [Google Scholar] [CrossRef] [Green Version]
- Ranson, K.E.; Urichuk, L.J. The effect of parent-child attachment relationships on child biopsychosocial outcomes: A review. Early Child Dev. Care 2008, 178, 129–152. [Google Scholar] [CrossRef]
- Lupien, S.J.; McEwen, B.S.; Gunnar, M.R.; Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 2009, 10, 434–445. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Yang, Y.; Wan, Y.; Shen, C.; Qiu, P. The influence of childhood adversities on mid to late cognitive function: From the perspective of life course. PLoS ONE 2021, 16, e0256297. [Google Scholar] [CrossRef]
- Kelly, M.E.; Duff, H.; Kelly, S.; McHugh Power, J.E.; Brennan, S.; Lawlor, B.A.; Loughrey, D.G. The impact of social activities, social networks, social support and social relationships on the cognitive functioning of healthy older adults: A systematic review. Syst. Rev. 2017, 6, 259. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Li, J.; Wang, Z.; Lian, Z.; Zhu, Z.; Liu, Y. Social networks, community engagement, and cognitive impairment among community-dwelling Chinese older adults. Dement. Geriatr. Cogn. Disord. Extra 2019, 9, 330–337. [Google Scholar] [CrossRef]
- Marseglia, A.; Wang, H.X.; Rizzuto, D.; Fratiglioni, L.; Xu, W. Participating in mental, social, and physical leisure activities and having a rich social network reduce the incidence of diabetes-related dementia in a cohort of Swedish older adults. Diabetes Care 2019, 42, 232–239. [Google Scholar] [CrossRef] [Green Version]
- Cacioppo, J.T.; Cacioppo, S. Social relationships and health: The toxic effects of perceived social isolation. Soc. Personal. Psychol. Compass 2014, 8, 58–72. [Google Scholar] [CrossRef] [Green Version]
- Lara, E.; Caballero, F.F.; Rico-Uribe, A.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L.; Miret, M. Are loneliness and social isolation associated with cognitive decline? Int. J. Geriatr. Psychiatry 2019, 34, 1613–1622. [Google Scholar] [CrossRef]
- De Jong Gierveld, J.; Tilburg, T.G.; van Dykstra, P.A. New ways of theorizing and conducting research in the field of loneliness and social isolation. In The Cambridge Handbook of Personal Relationships; Cambridge University Press: Cambridge, UK, 2018; pp. 391–404. [Google Scholar] [CrossRef] [Green Version]
- Luo, Y.; Waite, L.J. Loneliness and mortality among older adults in China. J. Gerontology. Ser. B Psychol. Sci. Soc. Sci. 2014, 69, 633–645. [Google Scholar] [CrossRef] [Green Version]
- Zhong, B.L.; Chen, S.L.; Tu, X.; Conwell, Y. Loneliness and cognitive function in older adults: Findings from the Chinese longitudinal healthy longevity survey. J. Gerontology. Ser. B Psychol. Sci. Soc. Sci. 2017, 72, 120–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, Y.; Choi, E.Y.; Park, N.S.; Chiriboga, D.A.; Duan, L.; Kim, M.T. Cognitive health risks posed by social isolation and loneliness in older Korean Americans. BMC Geriatr. 2021, 21, 123. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xue, B.; Hu, Y. Cognitive reserve over life course and 7-year trajectories of cognitive decline: Results from China health and retirement longitudinal study. BMC Public Health 2022, 22, 231. [Google Scholar] [CrossRef]
- Zhao, Q.; Zhang, Y.; Liao, X.; Wang, W. Executive function and diabetes: A clinical neuropsychology perspective. Front. Psychol. 2020, 11, 2112. [Google Scholar] [CrossRef]
- Mendes, R.; Martins, S.; Fernandes, L. Adherence to medication, physical activity and diet in older adults with diabetes: Its association with cognition, anxiety and depression. J. Clin. Med. Res. 2019, 11, 583–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reijmer, Y.D.; van den Berg, E.; Ruis, C.; Jaap Kappelle, L.; Biessels, G.J. Cognitive dysfunction in patients with type 2 diabetes. Diabetes/Metab. Res. Rev. 2010, 26, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Srikanth, V.; Sinclair, A.J.; Hill-Briggs, F.; Moran, C.; Biessels, J. Type 2 diabetes and cognitive dysfunction-towards effective management of both comorbidities. Lancet Diabetes Endocrinol. 2020, 8, 535–545. [Google Scholar] [CrossRef]
- Moore, A.K. The holistic theory of unpleasant symptoms. J. Holist. Nurs. 2022, 40, 193–202. [Google Scholar] [CrossRef]
- Hosseini, S.; Chaurasia, A.; Oremus, M. The effect of religion and spirituality on cognitive function: A systematic review. Gerontologist 2019, 59, E76–E85. [Google Scholar] [CrossRef]
- Koenig, H.G. Religion, spirituality, and health: The research and clinical implications. ISRN Psychiatry 2012, 2012, 278730. [Google Scholar] [CrossRef] [Green Version]
- Isehunwa, O.O.; Warner, E.T.; Spiegelman, D.; Huang, T.; Tworoger, S.S.; Kent, B.V.; Shields, A.E. Religion, spirituality and diurnal rhythms of salivary cortisol and dehydroepiandrosterone in postmenopausal women. Compr. Psychoneuroendocrinology 2021, 7, 100064. [Google Scholar] [CrossRef] [PubMed]
- Hill, T.D. Religious involvement and healthy cognitive aging: Patterns, explanations, and future directions. J. Gerontology. Ser. A Biol. Sci. Med. Sci. 2008, 63, 478–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, T.; Xie, Y.; Mao, X.; Liu, Y.; Zhang, J.; Wen, J.; Chen, Y.; Luo, Z.; Cai, W. The mediating role of loneliness between social support and depressive symptoms among Chinese rural adolescents during COVID-19 outbreak: A comparative study between left-behind and non-left-behind students. Front. Psychiatry 2021, 12, 740094. [Google Scholar] [CrossRef] [PubMed]
- Son, H.; Cho, H.J.; Cho, S.; Ryu, J.; Kim, S. The moderating effect of social support between loneliness and depression: Differences between the young-old and the old-old. Int. J. Environ. Res. Public Health 2022, 19, 2322. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Conceptual framework of cognitive impairment based on the theory of unpleasant symptoms.

Figure 2.
A life course approach framework of cognitive impairment in type 2 diabetes.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kim, B.; Efird, J.T.; Hu, J. A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review. Diabetology 2023, 4, 323-338. https://doi.org/10.3390/diabetology4030028
AMA Style
Kim B, Efird JT, Hu J. A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review. Diabetology. 2023; 4(3):323-338. https://doi.org/10.3390/diabetology4030028
Chicago/Turabian StyleKim, Bohyun, Jimmy T. Efird, and Jie Hu. 2023. "A Life Course Approach to Understanding Cognitive Impairment in Adults with Type 2 Diabetes: A Narrative Literature Review" Diabetology 4, no. 3: 323-338. https://doi.org/10.3390/diabetology4030028