Interdisciplinary Collaboration in Head and Neck Cancer Care: Optimizing Oral Health Management for Patients Undergoing Radiation Therapy


Abstract
:1. Introduction
2. Material and Methods
3. Radiation Therapy
3.1. Concept of Radiation Therapy
3.2. Radiation Therapy Techniques
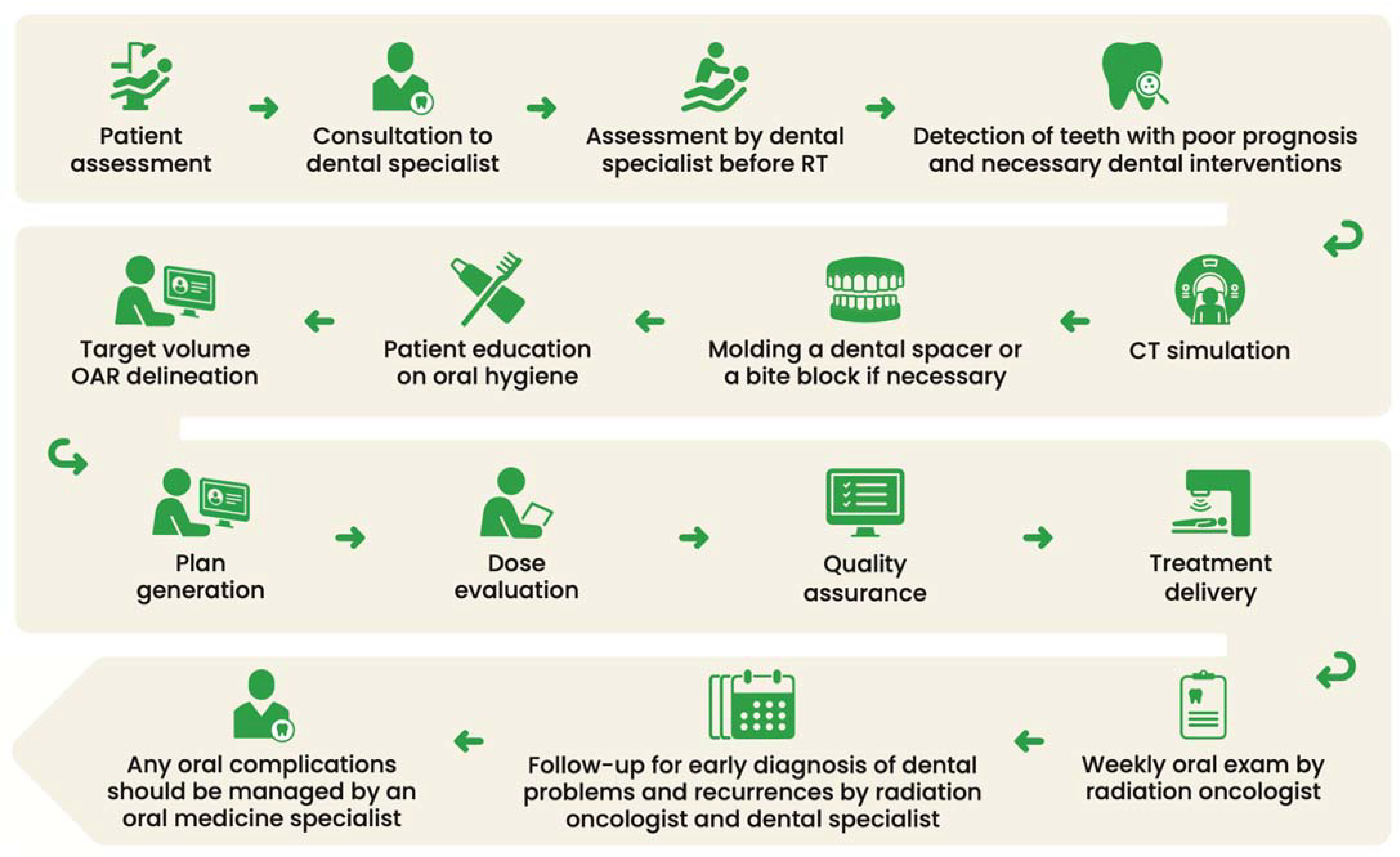
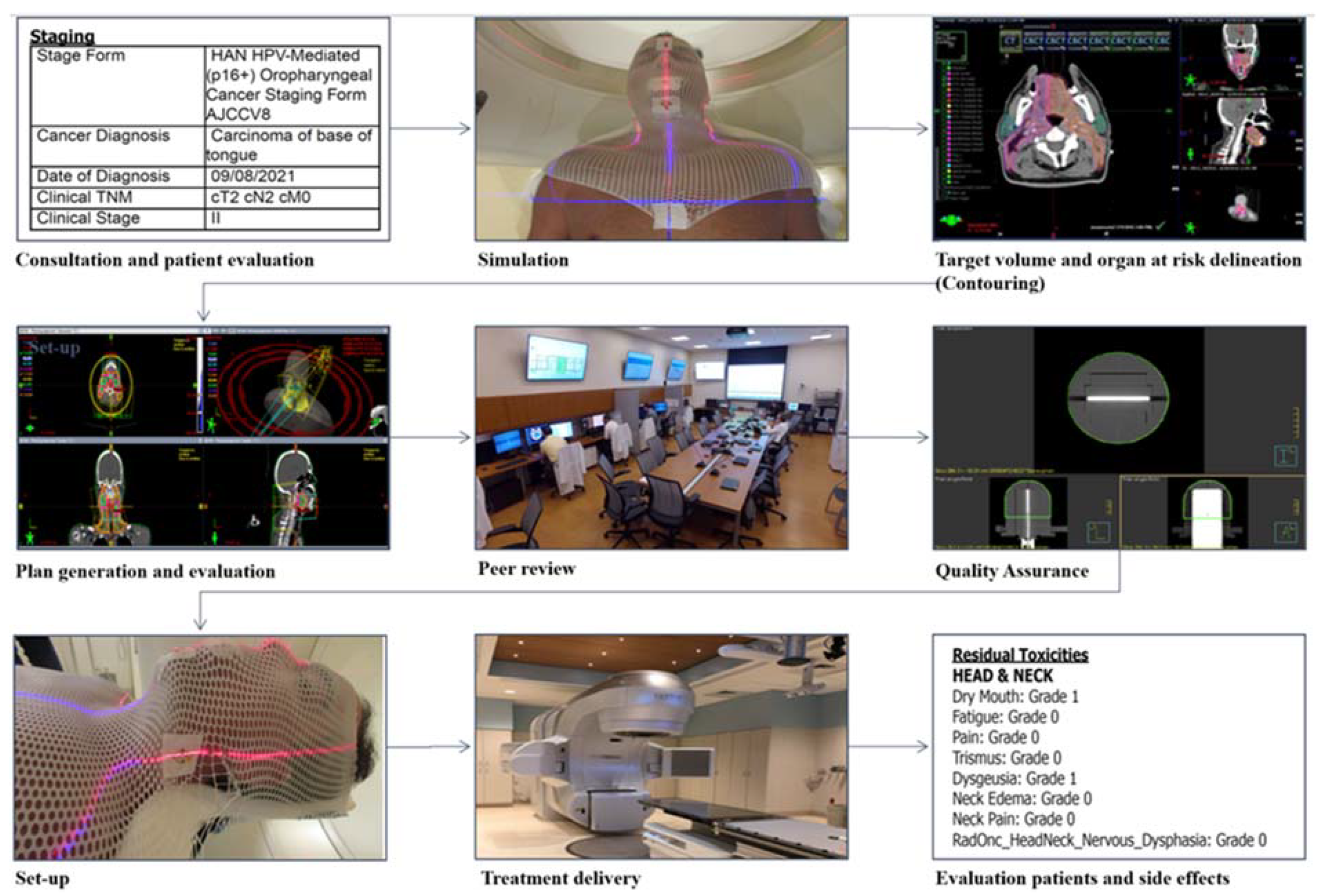
3.3. Treatment Steps
3.3.1. Pre-Radiation Therapy Patient Evaluation
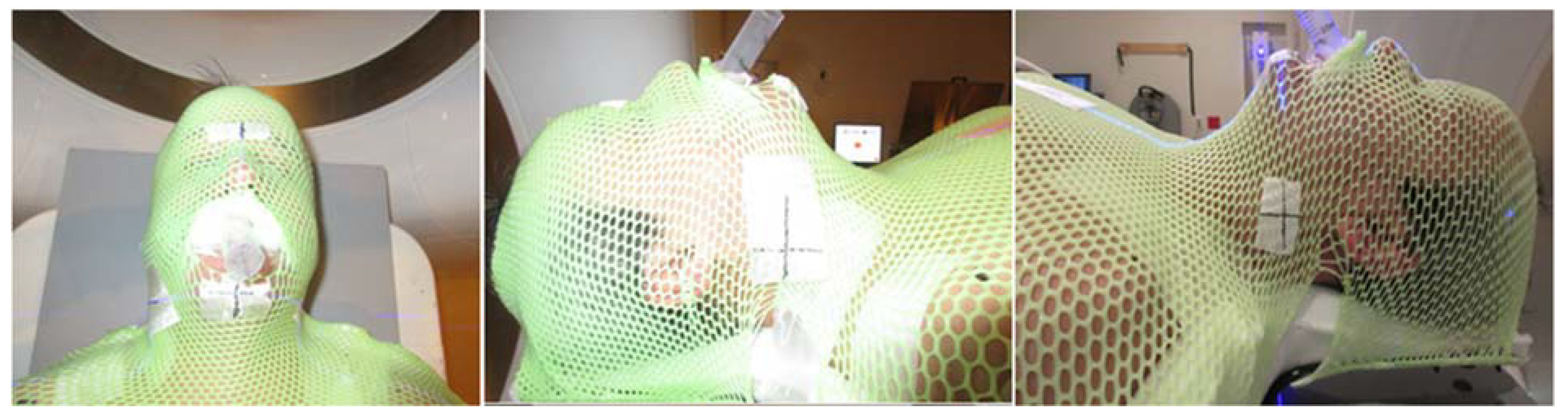
3.3.2. Patient Simulation
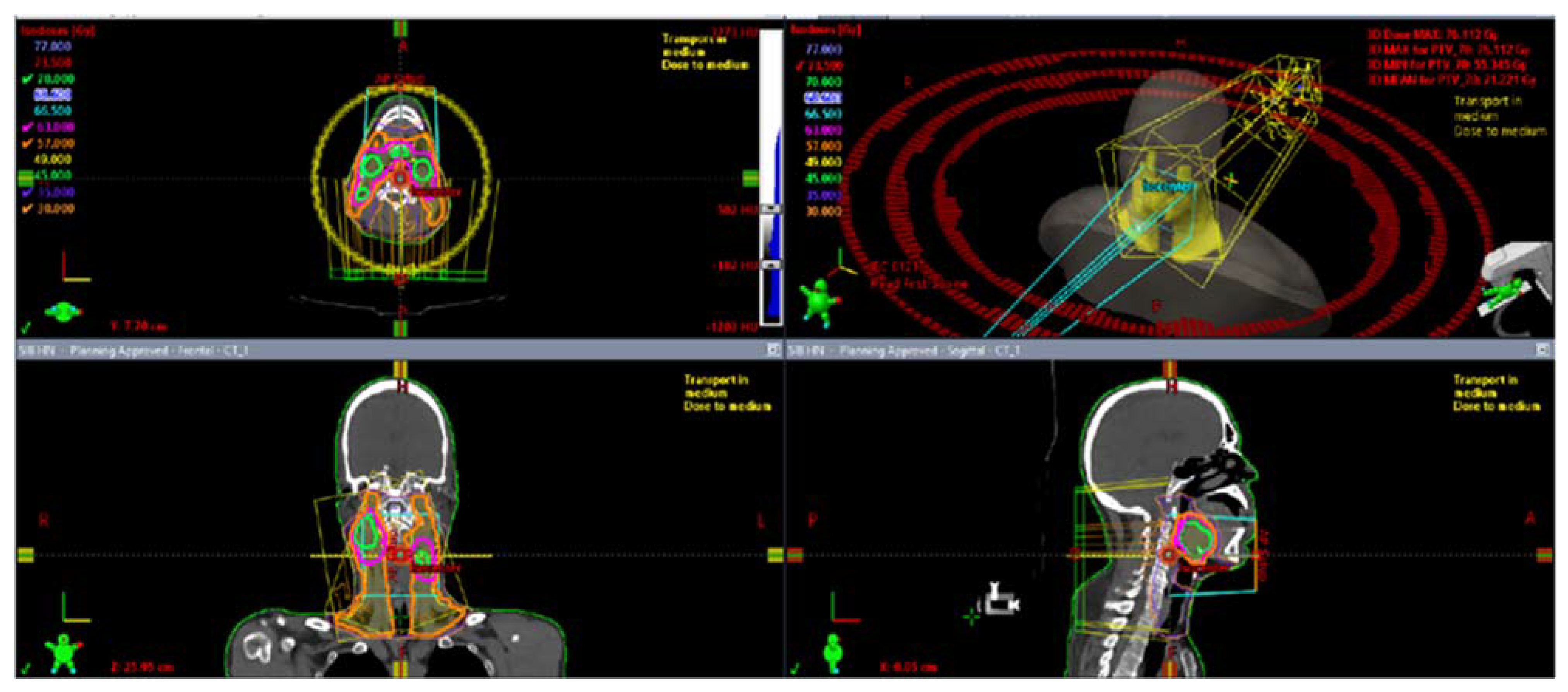
3.3.3. Radiation Therapy Planning
3.3.4. Radiation Therapy Delivery
4. Treatment-Related Side Effects and Management
4.1. Management of Acute Side Effects during Radiation Therapy
4.1.1. Oral Mucositis
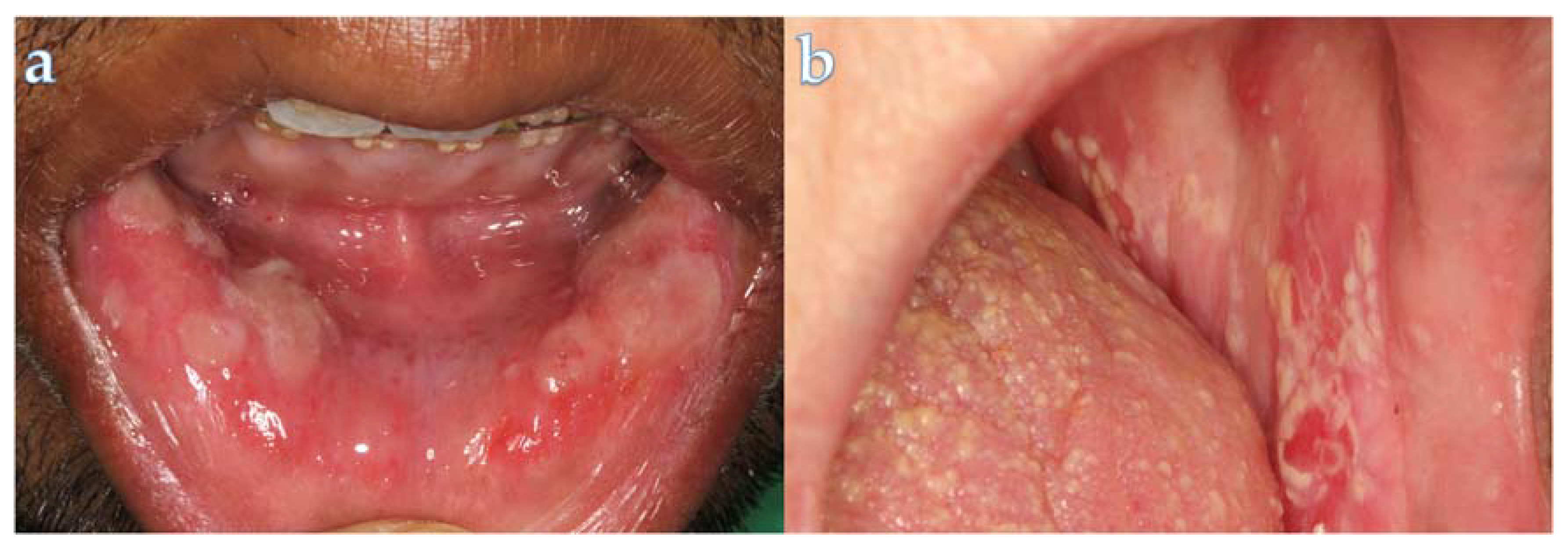
4.1.2. Oral Fungal Infections
4.1.3. Dry Mouth
4.2. Management of Post-Radiation Therapy Complications
4.2.1. Dental Caries
4.2.2. Periodontal Diseases
4.2.3. Trismus
4.2.4. Dysgeusia
4.2.5. Osteoradionecrosis
5. Follow-Up Recommendations
Dental Implants Post Radiotherapy
6. Future Directions
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef] [PubMed]
- Lo Nigro, C.; Denaro, N.; Merlotti, A.; Merlano, M. Head and neck cancer: Improving outcomes with a multidisciplinary approach. Cancer Manag. Res. 2017, 9, 363–371. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef] [PubMed]
- Cognetti, D.M.; Weber, R.S.; Lai, S.Y. Head and neck cancer: An evolving treatment paradigm. Cancer 2008, 113, 1911–1932. [Google Scholar] [CrossRef] [PubMed]
- Groth, P.; Orta, M.L.; Elvers, I.; Majumder, M.M.; Lagerqvist, A.; Helleday, T. Homologous recombination repairs secondary replication induced DNA double-strand breaks after ionizing radiation. Nucleic Acids Res. 2012, 40, 6585–6594. [Google Scholar] [CrossRef]
- De Ruysscher, D.; Niedermann, G.; Burnet, N.G.; Siva, S.; Lee, A.W.M.; Hegi-Johnson, F. Radiotherapy toxicity. Nat. Rev. Dis. Primers 2019, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Baudelet, M.; Van den Steen, L.; Tomassen, P.; Bonte, K.; Deron, P.; Huvenne, W.; Rottey, S.; De Neve, W.; Sundahl, N.; Van Nuffelen, G.; et al. Very late xerostomia, dysphagia, and neck fibrosis after head and neck radiotherapy. Head Neck 2019, 41, 3594–3603. [Google Scholar] [CrossRef] [PubMed]
- Daly-Schveitzer, N.; Julieron, M.; Tao, Y.G.; Moussier, A.; Bourhis, J. Intensity-modulated radiation therapy (IMRT): Toward a new standard for radiation therapy of head and neck cancer? Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2011, 128, 241–247. [Google Scholar] [CrossRef]
- Li, X.; Lee, A.; Cohen, M.A.; Sherman, E.J.; Lee, N.Y. Past, present and future of proton therapy for head and neck cancer. Oral. Oncol. 2020, 110, 104879. [Google Scholar] [CrossRef]
- Moreno, A.C.; Frank, S.J.; Garden, A.S.; Rosenthal, D.I.; Fuller, C.D.; Gunn, G.B.; Reddy, J.P.; Morrison, W.H.; Williamson, T.D.; Holliday, E.B.; et al. Intensity modulated proton therapy (IMPT)—The future of IMRT for head and neck cancer. Oral Oncol. 2019, 88, 66–74. [Google Scholar] [CrossRef]
- Mohamed, N.; Lee, A.; Lee, N.Y. Proton beam radiation therapy treatment for head and neck cancer. Precis. Radiat. Oncol. 2021, 6, 59–68. [Google Scholar] [CrossRef]
- Nogueira, L.M.; Jemal, A.; Yabroff, K.R.; Efstathiou, J.A. Assessment of Proton Beam Therapy Use Among Patients With Newly Diagnosed Cancer in the US, 2004–2018. JAMA Netw. Open 2022, 5, e229025. [Google Scholar] [CrossRef] [PubMed]
- Bankhead, C. ASTRO Says Few Cancers Qualify for Proton Therapy. Available online: https://www.medpagetoday.com/radiology/therapeuticradiology/46170 (accessed on 27 February 2024).
- Zientara, N.; Giles, E.; Le, H.; Short, M. A scoping review of patient selection methods for proton therapy. J. Med. Radiat. Sci. 2022, 69, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Tambas, M.; van der Laan, H.P.; Steenbakkers, R.; Doyen, J.; Timmermann, B.; Orlandi, E.; Hoyer, M.; Haustermans, K.; Georg, P.; Burnet, N.G.; et al. Current practice in proton therapy delivery in adult cancer patients across Europe. Radiother. Oncol. 2022, 167, 7–13. [Google Scholar] [CrossRef] [PubMed]
- de Jong, B.A.; Korevaar, E.W.; Maring, A.; Werkman, C.I.; Scandurra, D.; Janssens, G.; Both, S.; Langendijk, J.A. Proton arc therapy increases the benefit of proton therapy for oropharyngeal cancer patients in the model based clinic. Radiother. Oncol. 2023, 184, 109670. [Google Scholar] [CrossRef] [PubMed]
- Beech, N.; Robinson, S.; Porceddu, S.; Batstone, M. Dental management of patients irradiated for head and neck cancer. Aust. Dent. J. 2014, 59, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Frankart, A.J.; Frankart, M.J.; Cervenka, B.; Tang, A.L.; Krishnan, D.G.; Takiar, V. Osteoradionecrosis: Exposing the Evidence Not the Bone. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 1206–1218. [Google Scholar] [CrossRef] [PubMed]
- Network, N.C.C. Head and Neck Cancers (Version 1.2024). Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck.pdf (accessed on 27 October 2023).
- Lee, J.; Hueniken, K.; Cuddy, K.; Pu, J.; El Maghrabi, A.; Hope, A.; Hosni, A.; Glogauer, M.; Watson, E. Dental Extractions Before Radiation Therapy and the Risk of Osteoradionecrosis in Patients With Head and Neck Cancer. JAMA Otolaryngol. Head Neck Surg. 2023, 149, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Motoi, T.; Oho, T. Comparison of methods for the handling of metallic dental restorations before head and neck radiotherapy. Support. Care Cancer 2022, 30, 10285–10290. [Google Scholar] [CrossRef]
- Devi, S.; Singh, N. Dental care during and after radiotherapy in head and neck cancer. Natl. J. Maxillofac. Surg. 2014, 5, 117–125. [Google Scholar] [CrossRef]
- van der Veen, J.; Nuyts, S. Can Intensity-Modulated-Radiotherapy Reduce Toxicity in Head and Neck Squamous Cell Carcinoma? Cancers 2017, 9, 135. [Google Scholar] [CrossRef]
- Kawashita, Y.; Hayashida, S.; Funahara, M.; Umeda, M.; Saito, T. Prophylactic bundle for radiation-induced oral mucositis in oral or oropharyngeal cancer patients. J. Cancer Res. Ther. 2014, 2, 9–13. [Google Scholar] [CrossRef]
- Kawashita, Y.; Koyama, Y.; Kurita, H.; Otsuru, M.; Ota, Y.; Okura, M.; Horie, A.; Sekiya, H.; Umeda, M. Effectiveness of a comprehensive oral management protocol for the prevention of severe oral mucositis in patients receiving radiotherapy with or without chemotherapy for oral cancer: A multicentre, phase II, randomized controlled trial. Int. J. Oral. Maxillofac. Surg. 2019, 48, 857–864. [Google Scholar] [CrossRef]
- Falek, S.; Regmi, R.; Herault, J.; Dore, M.; Vela, A.; Dutheil, P.; Moignier, C.; Marcy, P.Y.; Drouet, J.; Beddok, A.; et al. Dental management in head and neck cancers: From intensity-modulated radiotherapy with photons to proton therapy. Support Care Cancer 2022, 30, 8377–8389. [Google Scholar] [CrossRef] [PubMed]
- Mayo, C.S.; Moran, J.M.; Bosch, W.; Xiao, Y.; McNutt, T.; Popple, R.; Michalski, J.; Feng, M.; Marks, L.B.; Fuller, C.D.; et al. American Association of Physicists in Medicine Task Group 263: Standardizing Nomenclatures in Radiation Oncology. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 1057–1066. [Google Scholar] [CrossRef]
- Chavaudra, J.; Bridier, A. Definition of volumes in external radiotherapy: ICRU reports 50 and 62. Cancer Radiother. 2001, 5, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Castelli, J.; Simon, A.; Louvel, G.; Henry, O.; Chajon, E.; Nassef, M.; Haigron, P.; Cazoulat, G.; Ospina, J.D.; Jegoux, F.; et al. Impact of head and neck cancer adaptive radiotherapy to spare the parotid glands and decrease the risk of xerostomia. Radiat. Oncol. 2015, 10, 6. [Google Scholar] [CrossRef]
- Castelli, J.; Simon, A.; Lafond, C.; Perichon, N.; Rigaud, B.; Chajon, E.; De Bari, B.; Ozsahin, M.; Bourhis, J.; de Crevoisier, R. Adaptive radiotherapy for head and neck cancer. Acta Oncol. 2018, 57, 1284–1292. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, P.G.; Kadam, A.S.; Jackson, W.C.; Eisbruch, A. Organ-Sparing in Radiotherapy for Head-and-Neck Cancer: Improving Quality of Life. Semin. Radiat. Oncol. 2018, 28, 46–52. [Google Scholar] [CrossRef]
- Lalla, R.V.; Bowen, J.; Barasch, A.; Elting, L.; Epstein, J.; Keefe, D.M.; McGuire, D.B.; Migliorati, C.; Nicolatou-Galitis, O.; Peterson, D.E.; et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2014, 120, 1453–1461. [Google Scholar] [CrossRef]
- Villa, A.; Sonis, S.T. Radiotherapy-induced severe oral mucositis: Pharmacotherapies in recent and current clinical trials. Expert Opin. Investig. Drugs 2023, 32, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Raber-Durlacher, J.E.; Elad, S.; Barasch, A. Oral mucositis. Oral Oncol. 2010, 46, 452–456. [Google Scholar] [CrossRef]
- Chen, S.C.; Lai, Y.H.; Huang, B.S.; Lin, C.Y.; Fan, K.H.; Chang, J.T. Changes and predictors of radiation-induced oral mucositis in patients with oral cavity cancer during active treatment. Eur. J. Oncol. Nurs. 2015, 19, 214–219. [Google Scholar] [CrossRef]
- Elad, S.; Cheng, K.K.F.; Lalla, R.V.; Yarom, N.; Hong, C.; Logan, R.M.; Bowen, J.; Gibson, R.; Saunders, D.P.; Zadik, Y.; et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2020, 126, 4423–4431. [Google Scholar] [CrossRef]
- Ariyawardana, A.; Cheng, K.K.F.; Kandwal, A.; Tilly, V.; Al-Azri, A.R.; Galiti, D.; Chiang, K.; Vaddi, A.; Ranna, V.; Nicolatou-Galitis, O.; et al. Systematic review of anti-inflammatory agents for the management of oral mucositis in cancer patients and clinical practice guidelines. Support. Care Cancer 2019, 27, 3985–3995. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.B.; Silverman, S., Jr.; Paggiarino, D.A.; Crockett, S.; Schubert, M.M.; Senzer, N.N.; Lockhart, P.B.; Gallagher, M.J.; Peterson, D.E.; Leveque, F.G. Benzydamine HCl for prophylaxis of radiation-induced oral mucositis: Results from a multicenter, randomized, double-blind, placebo-controlled clinical trial. Cancer 2001, 92, 875–885. [Google Scholar] [CrossRef]
- Kazemian, A.; Kamian, S.; Aghili, M.; Hashemi, F.A.; Haddad, P. Benzydamine for prophylaxis of radiation-induced oral mucositis in head and neck cancers: A double-blind placebo-controlled randomized clinical trial. Eur. J. Cancer Care 2009, 18, 174–178. [Google Scholar] [CrossRef]
- Sroussi, H.Y.; Epstein, J.B.; Bensadoun, R.J.; Saunders, D.P.; Lalla, R.V.; Migliorati, C.A.; Heaivilin, N.; Zumsteg, Z.S. Common oral complications of head and neck cancer radiation therapy: Mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Med. 2017, 6, 2918–2931. [Google Scholar] [CrossRef] [PubMed]
- Quindós, G.; Gil-Alonso, S.; Marcos-Arias, C.; Sevillano, E.; Mateo, E.; Jauregizar, N.; Eraso, E. Therapeutic tools for oral candidiasis: Current and new antifungal drugs. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e172–e180. [Google Scholar] [CrossRef]
- Mercadante, V.; Jensen, S.B.; Smith, D.K.; Bohlke, K.; Bauman, J.; Brennan, M.T.; Coppes, R.P.; Jessen, N.; Malhotra, N.K.; Murphy, B.; et al. Salivary Gland Hypofunction and/or Xerostomia Induced by Nonsurgical Cancer Therapies: ISOO/MASCC/ASCO Guideline. J. Clin. Oncol. 2021, 39, 2825–2843. [Google Scholar] [CrossRef]
- Greenspan, D. Xerostomia: Diagnosis and management. Oncol. (Williston Park) 1996, 10, 7–11. [Google Scholar]
- Nutting, C.M.; Morden, J.P.; Harrington, K.J.; Urbano, T.G.; Bhide, S.A.; Clark, C.; Miles, E.A.; Miah, A.B.; Newbold, K.; Tanay, M.; et al. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (PARSPORT): A phase 3 multicentre randomised controlled trial. Lancet Oncol. 2011, 12, 127–136. [Google Scholar] [CrossRef]
- Dijkema, T.; Raaijmakers, C.P.; Ten Haken, R.K.; Roesink, J.M.; Braam, P.M.; Houweling, A.C.; Moerland, M.A.; Eisbruch, A.; Terhaard, C.H. Parotid gland function after radiotherapy: The combined michigan and utrecht experience. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 449–453. [Google Scholar] [CrossRef] [PubMed]
- Sio, T.T.; Lin, H.K.; Shi, Q.; Gunn, G.B.; Cleeland, C.S.; Lee, J.J.; Hernandez, M.; Blanchard, P.; Thaker, N.G.; Phan, J.; et al. Intensity Modulated Proton Therapy Versus Intensity Modulated Photon Radiation Therapy for Oropharyngeal Cancer: First Comparative Results of Patient-Reported Outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Steneker, M.; Lomax, A.; Schneider, U. Intensity modulated photon and proton therapy for the treatment of head and neck tumors. Radiother. Oncol. 2006, 80, 263–267. [Google Scholar] [CrossRef]
- van de Water, T.A.; Lomax, A.J.; Bijl, H.P.; Schilstra, C.; Hug, E.B.; Langendijk, J.A. Using a reduced spot size for intensity-modulated proton therapy potentially improves salivary gland-sparing in oropharyngeal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e313–e319. [Google Scholar] [CrossRef]
- Youssef, I.; Yoon, J.; Mohamed, N.; Zakeri, K.; Press, R.H.; Chen, L.; Gelblum, D.Y.; McBride, S.M.; Tsai, C.J.; Riaz, N.; et al. Toxicity Profiles and Survival Outcomes Among Patients With Nonmetastatic Oropharyngeal Carcinoma Treated With Intensity-Modulated Proton Therapy vs Intensity-Modulated Radiation Therapy. JAMA Netw. Open 2022, 5, e2241538. [Google Scholar] [CrossRef] [PubMed]
- Golusinski, P.; Corry, J.; Poorten, V.V.; Simo, R.; Sjogren, E.; Makitie, A.; Kowalski, L.P.; Langendijk, J.; Braakhuis, B.J.M.; Takes, R.P.; et al. De-escalation studies in HPV-positive oropharyngeal cancer: How should we proceed? Oral Oncol. 2021, 123, 105620. [Google Scholar] [CrossRef]
- Dolezel, M.; Slavik, M.; Blazek, T.; Kazda, T.; Koranda, P.; Veverkova, L.; Burkon, P.; Cvek, J. FMISO-Based Adaptive Radiotherapy in Head and Neck Cancer. J. Pers. Med. 2022, 12, 1245. [Google Scholar] [CrossRef]
- Jensen, S.B.; Vissink, A.; Limesand, K.H.; Reyland, M.E. Salivary Gland Hypofunction and Xerostomia in Head and Neck Radiation Patients. JNCI Monogr. 2019, 2019, lgz016. [Google Scholar] [CrossRef]
- Vistoso Monreal, A.; Polonsky, G.; Shiboski, C.; Sankar, V.; Villa, A. Salivary Gland Dysfunction Secondary to Cancer Treatment. Front. Oral Health 2022, 3, 907778. [Google Scholar] [CrossRef] [PubMed]
- Michelet, M. Caries and periodontal disease in cancer survivors. Evid. Based Dent. 2012, 13, 70–73. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, G.; Jham, B.; Magalhães, C.; Sensi, L.; Freire, A. A Review of the Biological and Clinical Aspects of Radiation Caries. J. Contemp. Dent. Pract. 2009, 10, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Schuurhuis, J.M.; Stokman, M.A.; Witjes, M.J.H.; Reintsema, H.; Langendijk, J.A.; Vissink, A.; Spijkervet, F.K.L. Patients with advanced periodontal disease before intensity-modulated radiation therapy are prone to develop bone healing problems: A 2-year prospective follow-up study. Support. Care Cancer 2018, 26, 1133–1142. [Google Scholar] [CrossRef] [PubMed]
- Irie, M.S.; Mendes, E.M.; Borges, J.S.; Osuna, L.G.; Rabelo, G.D.; Soares, P.B. Periodontal therapy for patients before and after radiotherapy: A review of the literature and topics of interest for clinicians. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, e524–e530. [Google Scholar] [CrossRef] [PubMed]
- Abboud, W.A.; Hassin-Baer, S.; Alon, E.E.; Gluck, I.; Dobriyan, A.; Amit, U.; Yahalom, R.; Yarom, N. Restricted Mouth Opening in Head and Neck Cancer: Etiology, Prevention, and Treatment. JCO Oncol. Pract. 2020, 16, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Louise Kent, M.; Brennan, M.T.; Noll, J.L.; Fox, P.C.; Burri, S.H.; Hunter, J.C.; Lockhart, P.B. Radiation-Induced trismus in head and neck cancer patients. Support. Care Cancer 2008, 16, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Rapidis, A.D.; Dijkstra, P.U.; Roodenburg, J.L.; Rodrigo, J.P.; Rinaldo, A.; Strojan, P.; Takes, R.P.; Ferlito, A. Trismus in patients with head and neck cancer: Etiopathogenesis, diagnosis and management. Clin. Otolaryngol. 2015, 40, 516–526. [Google Scholar] [CrossRef]
- Hartl, D.M.; Cohen, M.; Juliéron, M.; Marandas, P.; Janot, F.; Bourhis, J. Botulinum toxin for radiation-induced facial pain and trismus. Otolaryngol. Head Neck Surg. 2008, 138, 459–463. [Google Scholar] [CrossRef]
- Bhrany, A.D.; Izzard, M.; Wood, A.J.; Futran, N.D. Coronoidectomy for the treatment of trismus in head and neck cancer patients. Laryngoscope 2007, 117, 1952–1956. [Google Scholar] [CrossRef]
- Ruo Redda, M.G.; Allis, S. Radiotherapy-induced taste impairment. Cancer Treat. Rev. 2006, 32, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Jafari, A.; Alaee, A.; Ghods, K. The etiologies and considerations of dysgeusia: A review of literature. J. Oral Biosci. 2021, 63, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Kielbassa, A.M.; Hinkelbein, W.; Hellwig, E.; Meyer-Luckel, H. Radiation-related damage to dentition. Lancet Oncol. 2006, 7, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Mossman, K.; Shatzman, A.; Chencharick, J. Long-term effects of radiotherapy on taste and salivary function in man. Int. J. Radiat. Oncol. Biol. Phys. 1982, 8, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Rivero, J.A.; Shamji, O.; Kolokythas, A. Osteoradionecrosis: A review of pathophysiology, prevention and pharmacologic management using pentoxifylline, α-tocopherol, and clodronate. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2017, 124, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Nabil, S.; Samman, N. Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: A systematic review. Int. J. Oral. Maxillofac. Surg. 2011, 40, 229–243. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.B.; Guneri, P.; Barasch, A. Appropriate and necessary oral care for people with cancer: Guidance to obtain the right oral and dental care at the right time. Support. Care Cancer 2014, 22, 1981–1988. [Google Scholar] [CrossRef]
- Aggarwal, K.; Goutam, M.; Singh, M.; Kharat, N.; Singh, V.; Vyas, S.; Singh, H.P. Prophylactic Use of Pentoxifylline and Tocopherol in Patients Undergoing Dental Extractions Following Radiotherapy for Head and Neck Cancer. Niger. J. Surg. 2017, 23, 130–133. [Google Scholar] [CrossRef] [PubMed]
- Arqueros-Lemus, M.; Mariño-Recabarren, D.; Niklander, S.; Martínez-Flores, R.; Moraga, V. Pentoxifylline and tocopherol for the treatment of osteoradionecrosis of the jaws. A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2023, 28, e293–e300. [Google Scholar] [CrossRef]
- Patel, V.; Gadiwalla, Y.; Sassoon, I.; Sproat, C.; Kwok, J.; McGurk, M. Prophylactic use of pentoxifylline and tocopherol in patients who require dental extractions after radiotherapy for cancer of the head and neck. Br. J. Oral Maxillofac. Surg. 2016, 54, 547–550. [Google Scholar] [CrossRef]
- Banjar, A.; Patel, V.; Abed, H. Pentoxifylline and tocopherol (vitamin E) with/without clodronate for the management of osteoradionecrosis: A scoping review. Oral Dis. 2023, 29, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Raggio, B.S.; Winters, R. Modern management of osteoradionecrosis. Curr. Opin. Otolaryngol. Head Neck Surg. 2018, 26, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Sultan, A.; Hanna, G.J.; Margalit, D.N.; Chau, N.; Goguen, L.A.; Marty, F.M.; Rabinowits, G.; Schoenfeld, J.D.; Sonis, S.T.; Thomas, T.; et al. The Use of Hyperbaric Oxygen for the Prevention and Management of Osteoradionecrosis of the Jaw: A Dana-Farber/Brigham and Women’s Cancer Center Multidisciplinary Guideline. Oncologist 2017, 22, 1413. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.J.; Butterworth, C.J.; Silcocks, P.; Tesfaye, B.T.; Bickerstaff, M.; Jackson, R.; Kanatas, A.; Nixon, P.; McCaul, J.; Praveen, P.; et al. HOPON (Hyperbaric Oxygen for the Prevention of Osteoradionecrosis): A Randomized Controlled Trial of Hyperbaric Oxygen to Prevent Osteoradionecrosis of the Irradiated Mandible After Dentoalveolar Surgery. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Kufta, K.; Forman, M.; Swisher-McClure, S.; Sollecito, T.P.; Panchal, N. Pre-Radiation dental considerations and management for head and neck cancer patients. Oral Oncol. 2018, 76, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.I.; Chan, H.L.; Tindle, D.I.; Maceachern, M.; Oh, T.J. Updated clinical considerations for dental implant therapy in irradiated head and neck cancer patients. J. Prosthodont. 2013, 22, 432–438. [Google Scholar] [CrossRef] [PubMed]
- Somay, E.; Yilmaz, B.; Topkan, E.; Pehlivan, B.; Selek, U. Radiotherapy and Dental Implant Applications in Patients with Head and Neck Cancer. In Advancements in Cancer Research; Sergi, C.M., Ed.; Exon Publications: Brisbane City, QLD, Australia, 2023. [Google Scholar]
- Epstein, J.; van der Meij, E.; McKenzie, M.; Wong, F.; Lepawsky, M.; Stevenson-Moore, P. Postradiation osteonecrosis of the mandible: A long-term follow-up study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1997, 83, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Al-Hezaimi, K.; Al-Rasheed, A.; Almas, K.; Romanos, G.E. Implant survival rate after oral cancer therapy: A review. Oral Oncol. 2010, 46, 854–859. [Google Scholar] [CrossRef]
- Guneri, P.; Epstein, J.B.; Ergun, S.; Boyacioglu, H. The Pathophysiology of Radiation-Induced Enamel Hypoplasia. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, 175–180. [Google Scholar]
- Borhan-Mojabi, K.; Tahani, B.; Shahsavari, F. Evaluation of Dentists’ Knowledge Regarding Oral Care of Patients Undergoing Radiotherapy in Qazvin. Iran. J. Dent. 2012, 9, 244–249. [Google Scholar]
- Akbari, M.; Malekzadeh, M.; Ardeshir Larijani, B.; Nejad, H.M. Dentists’ Knowledge Regarding Oral Care of Patients Under Radiation Therapy in Khorasan Province. Iran. J. Dent. 2015, 16, 343–347. [Google Scholar]
- Schache, A.; Kerawala, C.; Ahmed, O.; Brennan, P.A.; Cook, F.; Garrett, M.; Homer, J.; Hughes, C.; Mayland, C.; Mihai, R.; et al. British Association of Head and Neck Oncologists (BAHNO) standards 2020. J. Oral Pathol. Med. 2021, 50, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Clovis, J.B.; Horowitz, A.M.; Poel, D.H.; Oral, E.D. Dental Attitudes, Knowledge, and Education of Oncologists. J. Dent. Educ. 2002, 66, 1000–1007. [Google Scholar]
- Epstein, J.B.; Raber-Durlacher, J.E.; Wilkins, A.; Chavarria, M.G.; Myint, H.; Lepage, M.; Bossi, P. Advances in Hematologic Stem Cell Transplant: An Update for Oral Health Care Providers. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.M.; Martinez, A.D.; Patel, S.; Acharya, A.U.; Solanki, S.K. Dentists’ Knowledge, Attitudes, and Practices Regarding Oral Cancer in Gujarat, India. J. Cancer Educ. 2012, 27, 78–84. [Google Scholar]
- Suhaimi, A.A.M. Dentists’ Knowledge, Attitudes, and Practice Behaviors about Oral Cancer: Adapted SEM Model Findings. BMC Oral Health 2017, 17, 6. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of HNC | Regions Included |
|---|---|
| Oral Cavity Cancer | Lips, Buccal Mucosa, Gingiva, Tongue, Floor of Mouth, Retromolar Trigone, Hard Palatal mucosa |
| Oropharyngeal Cancer | Tonsils, Soft Palate, Base of Tongue, Posterior Pharyngeal Wall |
| Nasopharyngeal Cancer | Nasopharyngeal Tissue, Posterior Nasal Cavity |
| Sinonasal Cancer | Nasal Cavity, Paranasal Sinuses |
| Hypopharynx Cancer | Pyriform Sinus, Postcricoid Region |
| Larynx Cancer | Supraglottis, Glottis, Subglottis |
| Salivary Gland Cancer | Parotid Glands, Submandibular Glands, Sublingual Glands, Minor Salivary glands |
| Technique | Description | Advantages | Disadvantages |
|---|---|---|---|
| 3D Conformal Radiation Therapy (3DCRT) | Uses CT scans to shape radiation beams and conform them to the tumor’s geometry in the head and neck region |
|
|
| Intensity-Modulated Radiation Therapy (IMRT) | Precise radiation delivery with varying intensities to conform to the tumor’s shape in the head and neck area |
|
|
| Proton Therapy | Utilizes proton particles instead of X-rays for precise dose delivery, minimizing damage to surrounding tissues in head and neck cancers |
|
|
| Brachytherapy | Involves the placement of radioactive sources directly into or near the tumor in the head and neck |
|
|
| Recommendations | Educational Objectives |
|---|---|
| Consultation with a dental specialist | Gain insights into the importance of dental specialist consultations in assessing and planning treatment |
| Extractions of teeth with poor prognoses | Learn to identify and manage problematic teeth |
| Management of metallic dental restorations | Understand the significance of addressing metallic restorations in radiotherapy planning |
| Education for maintaining oral hygiene | Emphasize the role of proper oral hygiene in preventing radiation-related dental issues |
| Recommending prescription fluoride toothpaste | Explore the use of prescription fluoride toothpaste for dental caries prevention during and after treatment |
| Recommending smoking cessation | Highlight the importance of advising patients to quit smoking for better treatment outcomes |
| Implementation of dental spacers or prosthetics | Understand the use of dental spacers and prosthetics in protecting oral tissues during radiotherapy |
| Recommendations | Educational Objectives |
|---|---|
| Oral mucositis: | |
| Preventing radiation-induced oral mucositis | Learn the oral care protocols for the prevention of oral mucositis and management during radiotherapy |
| Early recognition of radiation-induced oral mucositis by weekly oral examination | Understand the importance of timely detection and the role of regular examinations in patient care |
| Oral infections: | |
| Prescription of antibiotics and antifungals when needed | Explore the use of antibiotics and antifungals in treating radiation-induced infections |
| Dry mouth: | |
| Maintaining adequate hydration | Learn how hydration techniques alleviate dry mouth and prevent dental complications |
| Prescription of anticholinergic medications | Understand the pharmacological approach to stimulating saliva production in dry mouth cases |
| Close follow-up for increased risk of dental caries | Gain awareness of the monitoring process to prevent dental caries in patients with dry mouth |
| Trismus: | |
| Mobilization exercises to maintain jaw opening | Learn exercises to preserve jaw mobility during and after radiotherapy |
| Alleviating symptoms to improve quality of life | Learn the indications of analgesics, muscle relaxants, and anti-inflammatory medications |
| Referring to a surgeon for release surgery in advanced cases | Learn when surgical intervention becomes necessary for severe trismus and how to make appropriate referrals |
| Osteoradionecrosis: | |
| Avoiding unnecessary dental interventions | Understand the significance of minimizing oral surgical procedures to reduce the risk of osteoradionecrosis |
| Pentoxyfylline and tocopherol prophylaxis | Learn the use of prophylactic medications to decrease the likelihood of osteoradionecrosis |
| Antibiotic therapy when needed | Learn the role of antibiotics in treating infections associated with osteoradionecrosis and when they are required |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kutuk, T.; Atak, E.; Villa, A.; Kalman, N.S.; Kaiser, A. Interdisciplinary Collaboration in Head and Neck Cancer Care: Optimizing Oral Health Management for Patients Undergoing Radiation Therapy. Curr. Oncol. 2024, 31, 2092-2108. https://doi.org/10.3390/curroncol31040155
Kutuk T, Atak E, Villa A, Kalman NS, Kaiser A. Interdisciplinary Collaboration in Head and Neck Cancer Care: Optimizing Oral Health Management for Patients Undergoing Radiation Therapy. Current Oncology. 2024; 31(4):2092-2108. https://doi.org/10.3390/curroncol31040155
Chicago/Turabian StyleKutuk, Tugce, Ece Atak, Alessandro Villa, Noah S. Kalman, and Adeel Kaiser. 2024. "Interdisciplinary Collaboration in Head and Neck Cancer Care: Optimizing Oral Health Management for Patients Undergoing Radiation Therapy" Current Oncology 31, no. 4: 2092-2108. https://doi.org/10.3390/curroncol31040155