Breast Cancer Screening and Perceptions of Harm among Young Adults in Japan: Results of a Cross-Sectional Online Survey

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
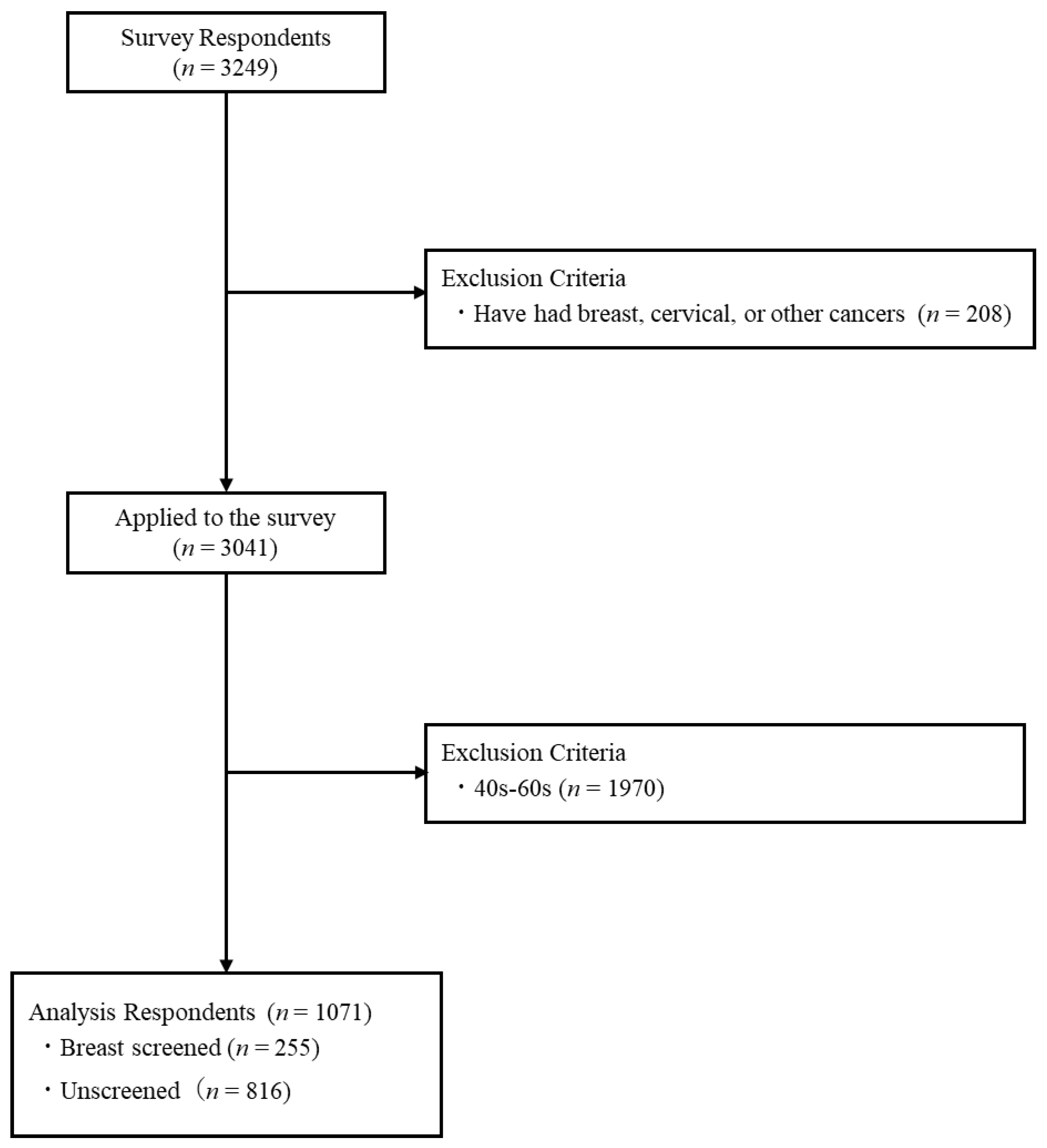
2.1. Analysis Target
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Factors Affecting Participation in BCS
3.2. Status of Participation in BCS
3.3. Status of Non-Participation in BCS
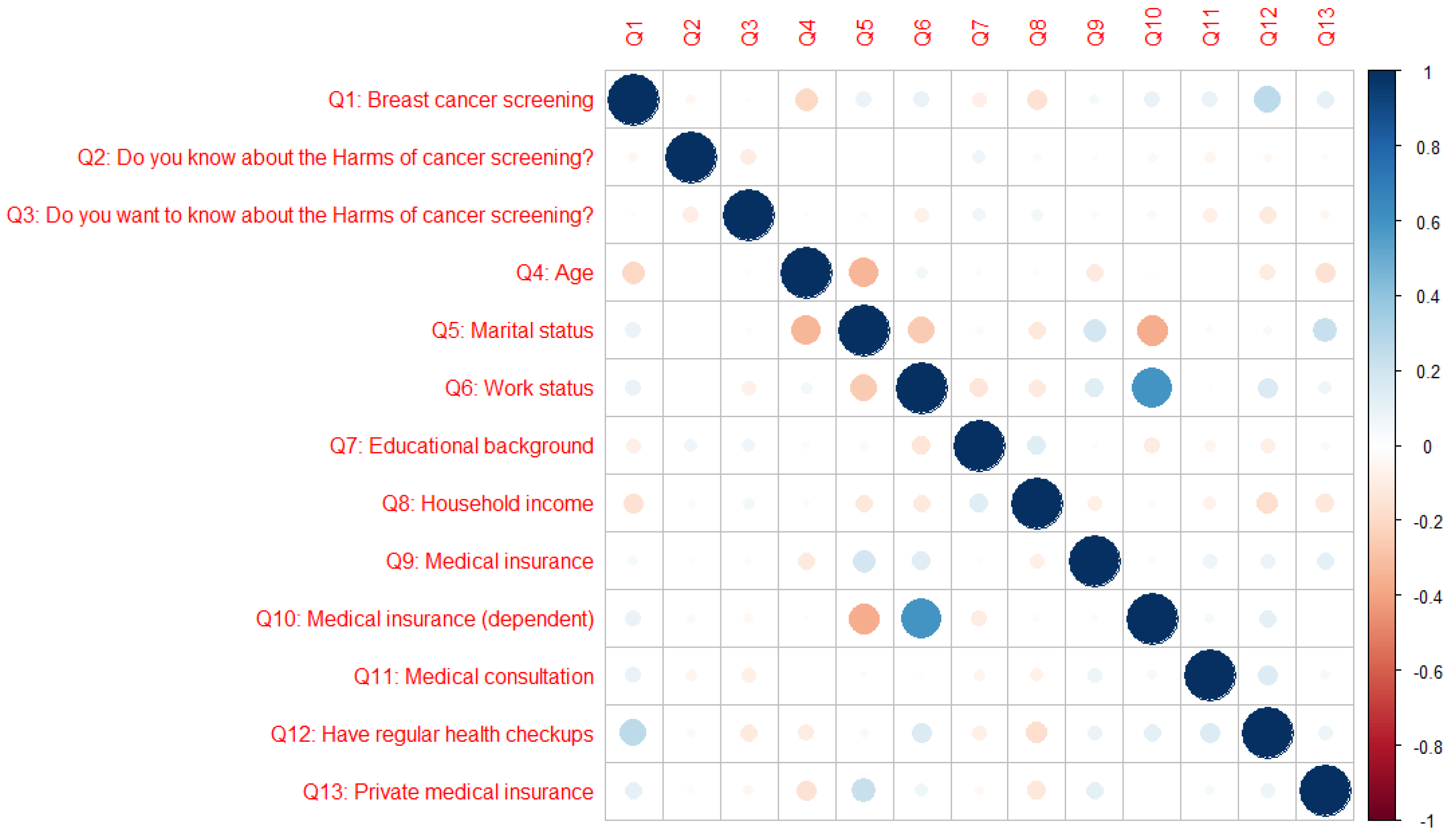
3.4. Correlation between BCS and Personal Characteristics
3.5. Psychological and Personal Characteristics Affecting Participation in BCS
3.6. Psychological and Personal Characteristics Affecting Participation in Knowledge of the Harms of Cancer Screening
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Cancer Information Service. Statistical Information by Cancer Type. Breast. Available online: https://ganjoho.jp/reg_stat/statistics/stat/cancer/14_breast.html#anchor1 (accessed on 1 December 2022).
- Njor, S.H.; Schwartz, W.; Blichert-Toft, M.; Lynge, E. Decline in Breast Cancer Mortality: How Much Is Attributable to Screening? J. Med. Screen 2015, 22, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Yaffe, M.J.; Mainprize, J.G. Risk of Radiation-Induced Breast Cancer from Mammographic Screening. Radiology 2011, 258, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Brodersen, J.; Siersma, V.D. Long-Term Psychosocial Consequences of False-Positive Screening Mammography. Ann. Fam. Med. 2013, 11, 106–115. [Google Scholar] [CrossRef]
- Checka, C.M.; Chun, J.E.; Schnabel, F.R.; Lee, J.; Toth, H. The Relationship of Mammographic Density and Age: Implications for Breast Cancer Screening. Am. J. Roentgenol. 2012, 198, W292–W295. [Google Scholar] [CrossRef]
- Hofvind, S.; Ponti, A.; Patnick, J.; Ascunce, N.; Njor, S.; Broeders, M.; Giordano, L.; Frigerio, A.; Törnberg, S. False-Positive Results in Mammographic Screening for Breast Cancer in Europe: A Literature Review and Survey of Service Screening Programmes. J. Med. Screen 2012, 19, 57–66. [Google Scholar] [CrossRef]
- Elmore, J.G.; Barton, M.B.; Moceri, V.M.; Polk, S.; Arena, P.J.; Fletcher, S.W. Ten-Year Risk of False Positive Screening Mammograms and Clinical Breast Examinations. N. Engl. J. Med. 1998, 338, 1089–1096. [Google Scholar] [CrossRef]
- Hubbard, R.A.; Kerlikowske, K.; Flowers, C.I.; Yankaskas, B.C.; Zhu, W.; Miglioretti, D.L. Cumulative Probability of False-Positive Recall or Biopsy Recommendation After 10 Years of Screening Mammography: A Cohort Study. Ann. Intern. Med. 2011, 155, 481. [Google Scholar] [CrossRef]
- Cancer Information Service. The Disadvantages of Breast Cancer Screening. Available online: https://ganjoho.jp/med_pro/cancer_control/screening/screening_breast.html (accessed on 16 January 2023).
- The Independent UK Panel on Breast Cancer Screening; Marmot, M.G.; Altman, D.G.; Cameron, D.A.; Dewar, J.A.; Thompson, S.G.; Wilcox, M. The Benefits and Harms of Breast Cancer Screening: An Independent Review: A Report Jointly Commissioned by Cancer Research UK and the Department of Health (England) October 2012. Br. J. Cancer 2013, 108, 2205–2240. [Google Scholar] [CrossRef]
- Kalager, M.; Adami, H.-O.; Bretthauer, M.; Tamimi, R.M. Overdiagnosis of Invasive Breast Cancer Due to Mammography Screening: Results From the Norwegian Screening Program. Ann. Intern. Med. 2012, 156, 491. [Google Scholar] [CrossRef]
- de Koning, H.J.; Draisma, G.; Fracheboud, J.; de Bruijn, A. Overdiagnosis and Overtreatment of Breast Cancer: Microsimulation Modelling Estimates Based on Observed Screen and Clinical Data. Breast Cancer Res. 2005, 8, 202. [Google Scholar] [CrossRef] [PubMed]
- Puliti, D.; Duffy, S.W.; Miccinesi, G.; De Koning, H.; Lynge, E.; Zappa, M.; Paci, E. Overdiagnosis in Mammographic Screening for Breast Cancer in Europe: A Literature Review. J. Med. Screen 2012, 19, 42–56. [Google Scholar] [CrossRef] [PubMed]
- Zahl, P.-H.; Mæhlen, J.; Welch, H.G. The Natural History of Invasive Breast Cancers Detected by Screening Mammography. Arch. Intern. Med. 2008, 168, 2311. [Google Scholar] [CrossRef] [PubMed]
- Altobelli, E.; Lattanzi, A. Breast Cancer in European Union: An Update of Screening Programmes as of March 2014 (Review). Int. J. Oncol. 2014, 45, 1785–1792. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Type of Cancer Screening. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000059490.html (accessed on 1 December 2022).
- Hamashima, C.; on behalf of the Japanese Research Group for the Development of Breast Cancer Screening Guidelines; Hamashima, C.C.; Hattori, M.; Honjo, S.; Kasahara, Y.; Katayama, T.; Nakai, M.; Nakayama, T.; Morita, T.; et al. The Japanese Guidelines for Breast Cancer Screening. Jpn. J. Clin. Oncol. 2016, 46, 482–492. [Google Scholar] [CrossRef]
- Siu, A.L.; on behalf of the U.S. Preventive Services Task Force. Screening for Breast Cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2016, 164, 279. [Google Scholar] [CrossRef]
- Kawasaki, H.; Yamasaki, S.; Kohama, N.; Fukita, S.; Tsunematsu, M.; Kakehashi, M. Analysis of the Training Effect of a Nursing Undergraduate Course on the Management of Radiation-Related Health Concerns—A Single Group Experiment. Int. J. Environ. Res. Public Health 2020, 17, 7649. [Google Scholar] [CrossRef]
- Hiromi, K.; Rahman, M.M.; Mika, I.; Chieko, K. Effectiveness of a Basic Education Program on RadiationRelated Health Concerns for Nurses of Public Health and School Health in Japan. Int. J. Public Health 2020, 49, 1087–1096. [Google Scholar] [CrossRef]
- National Cancer Center Institute for Cancer Control. Available online: http://canscreen.ncc.go.jp/kangae/kangae7.html (accessed on 15 December 2022).
- Cancer Information Service. Cancer Mortality, Cancer incidenceNCR. Available online: https://ganjoho.jp/reg_stat/statistics/data/dl/index.html (accessed on 6 December 2022).
- Pashayan, N.; Morris, S.; Gilbert, F.J.; Pharoah, P.D.P. Cost-Effectiveness and Benefit-to-Harm Ratio of Risk-Stratified Screening for Breast Cancer: A Life-Table Model. JAMA Oncol. 2018, 4, 1504. [Google Scholar] [CrossRef]
- Ersin, F.; Bahar, Z. Effect of Health Belief Model and Health Promotion Model on Breast Cancer Early Diagnosis Behavior: A Systematic Review. Asian Pac. J. Cancer Prev. 2011, 12, 2555–2562. [Google Scholar]
- Cui, Z.; Kawasaki, H.; Tsunematsu, M.; Cui, Y.; Kakehashi, M. Factors Affecting the Cervical Cancer Screening Behaviors of Japanese Women in Their 20s and 30s Using a Health Belief Model: A Cross-Sectional Study. Curr. Oncol. 2022, 29, 6287–6302. [Google Scholar] [CrossRef] [PubMed]
- Murakami, S. Risk factors of breast cancer (life style and environmental factors). Nippon Rinsho 2012, 70 (Suppl. S7), 50–54. [Google Scholar] [PubMed]
- Seki, A.; Hirai, K.; Nagatsuka, M. Measurement of the attitude regarding breast cancer screening. J. Health Welf. Stat. 2011, 58, 14–20. [Google Scholar]
- Lemon, S.; Zapka, J.; Puleo, E.; Luckmann, R.; Chasan-Taber, L. Colorectal Cancer Screening Participation: Comparisons with Mammography and Prostate-Specific Antigen Screening. Am. J. Public Health 2001, 91, 1264–1272. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Leadbetter, S.; Richards, T.; Sabatino, S.A. Contextual Analysis of Breast and Cervical Cancer Screening and Factors Associated with Health Care Access among United States Women, 2002. Soc. Sci. Med. 2008, 66, 260–275. [Google Scholar] [CrossRef] [PubMed]
- Outline of the “Public Opinion Survey on Cancer Control”. Available online: https://survey.gov-online.go.jp/h28/h28-gantaisaku/gairyaku.pdf (accessed on 15 December 2022).
- Hata, E.; Doi, Y. Kodo Kagaku: Kenkozukuri No Tame No Riron to Oyo; Nankodo: Tokyo, Japan, 2009; ISBN 978-4-524-25311-1. [Google Scholar]
- Uchida, K.; Ohashi, H.; Kinoshita, S.; Nogi, H.; Kato, K.; Toriumi, Y.; Yamashita, A.; Kamio, M.; Mimoto, R.; Takeyama, H. Breast Cancer Screening and the Changing Population Pyramid of Japan. Breast Cancer 2015, 22, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.K.; Larson, S.; Correa-de-Araujo, R. Women’s Health Care Utilization and Expenditures. Women’s Health Issues 2006, 16, 66–79. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Manual on Cancer Screening in the Workplace. Available online: https://www.mhlw.go.jp/file/05-Shingikai-10901000-Kenkoukyoku-Soumuka/0000204422.pdf (accessed on 7 December 2022).
- Marlow, L.A.V.; Chorley, A.J.; Haddrell, J.; Ferrer, R.; Waller, J. Understanding the Heterogeneity of Cervical Cancer Screening Non-Participants: Data from a National Sample of British Women. Eur. J. Cancer 2017, 80, 30–38. [Google Scholar] [CrossRef]
- Walton, A.; Albrecht, T.; Lux, L.; Judge Santacroce, S. Social Media: Support for Survivors and Young Adults With Cancer. CJON 2017, 21, 537–540. [Google Scholar] [CrossRef]
- Han, C.J.; Lee, Y.J.; Demiris, G. Interventions Using Social Media for Cancer Prevention and Management: A Systematic Review. Cancer Nurs. 2018, 41, E19–E31. [Google Scholar] [CrossRef]
- Phillips, J.; Cohen, M.Z. The Meaning of Breast Cancer Risk for African American Women. J. Nurs. Scholarsh. 2011, 43, 239–247. [Google Scholar] [CrossRef]
- Sheppard, V.B.; Christopher, J.; Nwabukwu, I. Breaking the Silence Barrier: Opportunities to Address Breast Cancer in African-Born Women. J. Natl. Med. Assoc. 2010, 102, 461–468. [Google Scholar] [CrossRef]
- Dillard, A.J.; Couper, M.P.; Zikmund-Fisher, B.J. Perceived Risk of Cancer and Patient Reports of Participation in Decisions about Screening: The DECISIONS Study. Med. Decis. Mak. 2010, 30, 96–105. [Google Scholar] [CrossRef]
- Wong, N.C.H. Interaction of Comparative Cancer Risk and Cancer Efficacy Perceptions on Cancer-Related Information Seeking and Scanning Behaviors. Commun. Res. Rep. 2012, 29, 193–203. [Google Scholar] [CrossRef]
- Ranasinghe, H.M.; Ranasinghe, N.; Rodrigo, C.; Seneviratne, R.D.A.; Rajapakse, S. Awareness of Breast Cancer among Adolescent Girls in Colombo, Sri Lanka: A School Based Study. BMC Public Health 2013, 13, 1209. [Google Scholar] [CrossRef]
- Karayurt, O.; Ozmen, D.; Cetinkaya, A.C. Awareness of Breast Cancer Risk Factors and Practice of Breast Self Examination among High School Students in Turkey. BMC Public Health 2008, 8, 359. [Google Scholar] [CrossRef]
- Fondjo, L.A.; Owusu-Afriyie, O.; Sakyi, S.A.; Wiafe, A.A.; Amankwaa, B.; Acheampong, E.; Ephraim, R.K.D.; Owiredu, W.K.B.A. Comparative Assessment of Knowledge, Attitudes, and Practice of Breast Self-Examination among Female Secondary and Tertiary School Students in Ghana. Int. J. Breast Cancer 2018, 2018, 7502047. [Google Scholar] [CrossRef]
- Marzo, R.; Salam, A. Teachers’ Knowledge, Beliefs and Practices of Breast Self-Examination in a City of Philippine: A Most Cost-Effective Tool for Early Detection of Breast Cancer. J. App. Pharm. Sci. 2016, 6, 16–21. [Google Scholar] [CrossRef]
- Abo Al-Shiekh, S.S.; Ibrahim, M.A.; Alajerami, Y.S. Breast Cancer Knowledge and Practice of Breast Self-Examination among Female University Students, Gaza. Sci. World J. 2021, 2021, 6640324. [Google Scholar] [CrossRef]
- Mekuria, M.; Nigusse, A.; Tadele, A. Breast Self-Examination Practice and Associated Factors Among Secondary School Female Teachers in Gammo Gofa Zone, Southern, Ethiopia. Breast Cancer (Dove Med. Press) 2020, 12, 1–10. [Google Scholar] [CrossRef]
- Nde, F.P.; Assob, J.C.N.; Kwenti, T.E.; Njunda, A.L.; Tainenbe, T.R.G. Knowledge, Attitude and Practice of Breast Self-Examination among Female Undergraduate Students in the University of Buea. BMC Res. Notes 2015, 8, 43. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| (1) Susceptibility to cancer | I may develop female cancer in the future. |
| I may develop female cancer within a few years. | |
| I am more likely to develop female cancer than other women. | |
| (2) Seriousness of cancer | I am afraid of developing female cancer. |
| If I develop female cancer, my life will be changed. | |
| If I develop female cancer, my activities of daily living will be limited. | |
| If I develop female cancer, my family will be affected negatively. | |
| I’m scared that I’ll find a woman’s cancer by having a cancer screening. | |
| (3) Benefits of cancer screening | Participation in female cancer screening can lead to reduction in mortality from female cancer. |
| Participation in female cancer screening can lead to early detection of female cancer. | |
| Having a women’s cancer screening can give me peace of mind about my health. | |
| Participation in female cancer screening can lead to better management of my health. | |
| (4) Burden to participation before cancer screening | I do not have time to participate in female cancer screening. |
| Participation in female cancer screening is costly. | |
| I don’t know where to go for a female cancer screening. | |
| I forget to regularly participate in female cancer screening. | |
| (5) Burden to participation at the time of cancer screening | I am embarrassed about participating in female cancer screening because it includes examination of a delicate area. |
| Female cancer screening causes discomfort, even pain. | |
| I do not want to participate in female cancer screening that is performed by male doctors/staff members. | |
| (6) Importance of cancer screening | There are other things in my life that are more important than getting screened for women’s cancer. |
| I do not need to participate in female cancer screening because I can visit a medical institution whenever there is any concern. | |
| I do not need to participate in female cancer screening because I have no particular subjective symptoms. | |
| Participation in female cancer screening is less important than other health issues. | |
| (7) Cues to participation in screening | A close friend or acquaintance recommends that I have a cancer screening for women. |
| My closest family members recommend that I participate in female cancer screening. | |
| The doctors at the hospital which I regularly visit recommend that I participate in female cancer screening. | |
| My close friends/acquaintances recommend that I participate in female cancer screening. |
| Characteristic | Total (n = 1071) | Screened (n = 255) | Unscreened (n = 816) | p-Value * |
|---|---|---|---|---|
| Do you know about the harms of cancer screening? | 0.481 | |||
| I don’t know at all | 458 (42.8%) | 97 (21.2%) | 361 (78.8%) | |
| I don’t know so much | 453 (42.3%) | 115 (25.4%) | 338 (74.6%) | |
| I can’t say either | 111 (10.4%) | 31 (27.9%) | 80 (72.1%) | |
| I know | 44 (4.1%) | 11 (25.0%) | 33 (75.0%) | |
| I know very much | 5 (0.5%) | 1 (20.0%) | 4 (80.0%) | |
| Do you want to know about the harms of cancer screening? | 0.779 | |||
| I don’t want to know at all | 15 (1.4%) | 5 (33.3%) | 10 (66.7%) | |
| I don’t want to know so much | 24 (2.2%) | 4 (16.7%) | 20 (83.3%) | |
| I can’t say either | 231 (21.6%) | 52 (22.5%) | 179 (77.5%) | |
| I want to know | 587 (54.8%) | 141 (24.0%) | 446 (76.0%) | |
| I want to know very much | 214 (20.0%) | 53 (24.8%) | 161 (75.2%) | |
| Age | <0.001 | |||
| 20–24 | 108 (10.1%) | 11 (10.2%) | 97 (89.8%) | |
| 25–29 | 340 (31.8%) | 47 (13.8%) | 293 (86.2%) | |
| 30–34 | 304 (28.4%) | 93 (30.6%) | 211 (69.4%) | |
| 35–39 | 319 (29.8%) | 104 (32.6%) | 215 (67.4%) | |
| Marital status | 0.004 | |||
| Married | 630 (58.8%) | 170 (27.0%) | 460 (73.0%) | |
| Single | 441 (41.2%) | 85 (19.3%) | 356 (80.7%) | |
| Work status | <0.001 | |||
| Self-employed | 35 (3.3%) | 9 (25.7%) | 26 (74.3%) | |
| Regular employment | 478 (44.6%) | 138 (28.9%) | 340 (71.1%) | |
| Parttime job | 190 (17.7%) | 38 (20.0%) | 152 (80.0%) | |
| Student | 49 (4.6%) | 3 (6.1%) | 46 (93.9%) | |
| Housewife | 268 (25.0%) | 63 (23.5%) | 205 (76.5%) | |
| Unemployed | 51 (4.8%) | 4 (7.8%) | 47 (92.2%) | |
| Educational background | 0.001 | |||
| Primary and secondary school | 27 (2.5%) | 5 (18.5%) | 22 (81.5%) | |
| High School | 236 (22.0%) | 40 (17.0%) | 196 (83.1%) | |
| Junior colleges and vocational schools | 213 (19.9%) | 39 (18.3%) | 174 (81.7%) | |
| University | 430 (40.2%) | 131 (30.5%) | 299 (69.5%) | |
| Graduate School | 33 (3.1%) | 9 (27.3%) | 24 (72.7%) | |
| Others | 132 (12.3%) | 31 (23.5%) | 101 (76.5%) | |
| Household income ** | <0.001 | |||
| No income | 18 (1.7%) | 3 (16.7%) | 15 (83.3%) | |
| Less than USD 7000 | 27 (2.5%) | 4 (14.8%) | 23 (85.2%) | |
| USD 7000–USD 22,000 | 115 (10.7%) | 18 (15.7%) | 97 (84.4%) | |
| USD 22,000–USD 37,000 | 320 (29.9%) | 54 (16.9%) | 266 (83.1%) | |
| USD 37,000–USD 51,000 | 284 (26.5%) | 73 (25.7%) | 211 (74.3%) | |
| USD 51,000–USD 73,000 | 189 (17.7%) | 65 (34.4%) | 124 (65.6%) | |
| USD 73,000–USD 110,000 | 91 (8.5%) | 30 (33.0%) | 61 (67.0%) | |
| More than USD 110,000 | 27 (2.5%) | 8 (29.6%) | 19 (70.4%) | |
| Medical insurance *** | <0.001 | |||
| Association health insurance | 409 (38.2%) | 90 (22.0%) | 319 (78.0%) | |
| Union health insurance | 171 (16.0%) | 64 (37.4%) | 107 (62.6%) | |
| Mutual aid association | 104 (9.7%) | 29 (27.9%) | 75 (72.1%) | |
| National health insurance | 282 (26.3%) | 49 (17.4%) | 233 (82.6%) | |
| National health insurance association | 63 (5.9%) | 13 (20.6%) | 50 (79.4%) | |
| Others | 16 (1.5%) | 4 (25.0%) | 12 (75.0%) | |
| Unknown | 26 (2.4%) | 6 (23.1%) | 20 (76.9%) | |
| Medical insurance (dependent) | 0.003 | |||
| Myself | 638 (59.6%) | 173 (27.1%) | 465 (72.9%) | |
| Family | 433 (40.4%) | 82 (18.9%) | 351 (81.1%) | |
| Medical consultation | 0.002 | |||
| Yes | 286 (26.7%) | 88 (30.8%) | 198 (69.2%) | |
| No | 785 (73.3%) | 167 (21.3%) | 618 (78.7%) | |
| Have regular health checkups | <0.001 | |||
| Yes | 246 (23.0%) | 110 (44.7%) | 136 (55.3%) | |
| No | 825 (77.0%) | 145 (17.6%) | 680 (82.4%) | |
| Private medical insurance | 0.001 | |||
| Yes | 557 (52.0%) | 157 (28.2%) | 400 (71.8%) | |
| No | 514 (48.0%) | 98 (19.1%) | 416 (80.9%) |
| Characteristic | Total (n = 255) | Work Status | |||||
|---|---|---|---|---|---|---|---|
| Self-Employed (n = 9) | Regular Employment (n = 138) | Part-Time Job (n = 38) | Student (n = 3) | Housewife (n = 63) | Unemployed (n = 4) | ||
| Age | |||||||
| 20–24 | 9 (3.5%) | 0 (0.0%) | 7 (5.1%) | 1 (2.6%) | 3 (100.0%) | 0 (0.0%) | 0 (0.0%) |
| 25–29 | 138 (54.1%) | 1 (11.1%) | 29 (21.0%) | 5 (13.2%) | 0 (0.0%) | 10 (15.9%) | 2 (50.0%) |
| 30–34 | 38 (14.9%) | 6 (66.7%) | 54 (39.1%) | 9 (23.7%) | 0 (0.0%) | 24 (38.1%) | 0 (0.0%) |
| 35–39 | 3 (1.2%) | 2 (22.2%) | 48 (34.8%) | 23 (60.5%) | 0 (0.0%) | 29 (46.0%) | 2 (50.0%) |
| Medical insurance * | |||||||
| Association health insurance | 90 (22.0%) | 1 (11.1%) | 56 (40.6%) | 17 (44.7%) | 0 (0.0%) | 16 (25.4%) | 0 (0.0%) |
| Union health insurance | 64 (37.4%) | 1 (11.1%) | 35 (25.4%) | 5 (13.2%) | 0 (0.0%) | 23 (36.5%) | 0 (0.0%) |
| Mutual aid association | 29 (27.9%) | 1 (11.1%) | 17 (12.3%) | 3 (7.9%) | 0 (0.0%) | 8 (12.7%) | 0 (0.0%) |
| National health insurance | 49 (17.4%) | 5 (55.6%) | 15 (10.9%) | 12 (31.6%) | 3 (100.0%) | 11 (17.5%) | 3 (75.0%) |
| National health insurance association | 13 (20.6%) | 1 (11.1%) | 9 (6.5%) | 0 (0.0%) | 0 (0.0%) | 3 (4.8%) | 0 (0.0%) |
| Others | 4 (25.0%) | 0 (0.0%) | 2 (1.4%) | 1 (2.6%) | 0 (0.0%) | 1 (1.6%) | 0 (0.0%) |
| Unknown | 6 (23.1%) | 0 (0.0%) | 4 (2.9%) | 0 (0.0%) | 0 (0.0%) | 1 (1.6%) | 1 (25.0%) |
| Reason for BCS | |||||||
| Information from your municipality or workplace. | 68 (26.7%) | 4 (44.4%) | 31 (22.5%) | 10 (26.3%) | 1 (33.3%) | 22 (34.9%) | 0 (0.0%) |
| Recommendations from your family doctor. | 11 (4.3%) | 0 (0.0%) | 5 (3.6%) | 3 (7.9%) | 0 (0.0%) | 2 (3.2%) | 1 (25.0%) |
| My own health care. | 110 (43.1%) | 2 (22.2%) | 62 (44.9%) | 15 (39.5%) | 0 (0.0%) | 29 (46.0%) | 2 (50.0%) |
| Because I felt I needed to see a doctor. | 48 (18.8%) | 2 (22.2%) | 29 (21.0%) | 7 (18.4%) | 2 (66.7%) | 8 (12.7%) | 0 (0.0%) |
| Because a family member or acquaintance has cancer, and I am concerned. | 13 (5.1%) | 1 (11.1%) | 8 (5.8%) | 2 (5.3%) | 0 (0.0%) | 1 (1.6%) | 1 (25.0%) |
| Others. | 5 (2.0%) | 0 (0.0%) | 3 (2.2%) | 1 (2.6%) | 0 (0.0%) | 1 (1.6%) | 0 (0.0%) |
| Characteristic | Total (n = 816) | Age | |||
|---|---|---|---|---|---|
| 20–24 (n = 97) | 25–29 (n = 293) | 30–34 (n = 211) | 35–39 (n = 215) | ||
| Work status | |||||
| Self-employed | 26 (3.2%) | 1 (1.0%) | 6 (2.1%) | 7 (3.3%) | 12 (5.6%) |
| Regular employment | 340 (41.7%) | 33 (34.0%) | 150 (51.2%) | 81 (38.4%) | 76 (35.4%) |
| Part-time job | 152 (18.6%) | 14 (14.4%) | 49 (16.7%) | 44 (20.9%) | 45 (20.9%) |
| Student | 46 (5.6%) | 43 (44.3%) | 3 (1.0%) | 0 (0.0%) | 0 (0.0%) |
| Housewife | 205 (25.1%) | 3 (3.1%) | 69 (23.6%) | 66 (31.3%) | 67 (31.2%) |
| Unemployed | 47 (5.8%) | 3 (3.1%) | 16 (5.5%) | 13 (6.2%) | 15 (7.0%) |
| Medical insurance * | |||||
| Association health insurance | 319 (78.0%) | 15 (15.5%) | 122 (41.6%) | 94 (44.6%) | 88 (40.9%) |
| Union health insurance | 107 (62.6%) | 12 (12.4%) | 36 (12.3%) | 30 (14.2%) | 29 (13.5%) |
| Mutual aid association | 75 (72.1%) | 10 (10.3%) | 29 (9.9%) | 16 (7.6%) | 20 (9.3%) |
| National health insurance | 233 (82.6%) | 41 (42.3%) | 75 (25.6%) | 54 (25.6%) | 63 (29.3%) |
| National health insurance association | 50 (79.4%) | 8 (8.3%) | 20 (6.8%) | 10 (4.7%) | 12 (5.6%) |
| Unknown | 20 (76.9%) | 8 (8.3%) | 7 (2.4%) | 5 (2.4%) | 0 (0.0%) |
| Others | 12 (75.0%) | 3 (3.1%) | 4 (1.4%) | 2 (1.0%) | 3 (1.4%) |
| Reason for not participating in BCS | |||||
| Busy. | 76 (9.3%) | 8 (8.3%) | 22 (7.5%) | 23 (10.9%) | 23 (10.7%) |
| I’m healthy. | 38 (4.7%) | 3 (3.1%) | 9 (3.1%) | 12 (5.7%) | 14 (6.5%) |
| I am anxious about the results. | 27 (3.3%) | 0 (0.0%) | 14 (4.8%) | 7 (3.3%) | 6 (2.8%) |
| Because I did not know about cancer screening. | 15 (1.8%) | 5 (5.2%) | 8 (2.7%) | 2 (1.0%) | 0 (0.0%) |
| Because I never had a chance to have a cancer screening. | 184 (22.6%) | 23 (23.7%) | 73 (24.9%) | 42 (19.9%) | 46 (21.4%) |
| Because I forgot to take the test. | 57 (7.0%) | 7 (7.2%) | 12 (4.1%) | 14 (6.6%) | 24 (11.2%) |
| I don’t think I am old enough to have a checkup. | 58 (7.1%) | 32 (33.0%) | 16 (5.5%) | 5 (2.4%) | 5 (2.3%) |
| Participation in cervical cancer screening. | 321 (39.3%) | 16 (16.5%) | 130 (44.4%) | 95 (45.0%) | 80 (37.2%) |
| Others. | 40 (4.9%) | 3 (3.1%) | 9 (3.1%) | 11 (5.2%) | 17 (7.9%) |
| Parameter | OR | 95%CI | p-Value |
|---|---|---|---|
| Do you want to know about the harms of cancer screening? | |||
| I want to know very much. | Ref. | ---- | ---- |
| I don’t want to know at all. | 5.34 | 1.31–21.73 | 0.019 |
| I don’t want to know so much. | 1.40 | 0.39–5.06 | 0.606 |
| I can’t say either. | 1.78 | 1.02–3.11 | 0.042 |
| I want to know. | 1.24 | 0.79–1.95 | 0.345 |
| Age | |||
| 35–39 | Ref. | ---- | ---- |
| 20–24 | 0.49 | 0.21-1.17 | 0.109 |
| 25–29 | 0.33 | 0.21–0.51 | <0.001 |
| 30–34 | 0.77 | 0.52–1.15 | 0.207 |
| Work status | |||
| Unemployed | Ref. | ---- | ---- |
| Self-employed | 5.44 | 1.14–25.97 | 0.034 |
| Regular employment | 6.96 | 1.78–27.14 | 0.005 |
| Part-time job | 5.38 | 1.34–21.59 | 0.018 |
| Student | 1.62 | 0.25–10.60 | 0.617 |
| Housewife | 5.16 | 1.28–20.91 | 0.021 |
| Have regular health checkups | |||
| No | Ref. | ---- | ---- |
| Yes | 1.80 | 1.23–2.63 | 0.003 |
| HBM | |||
| Susceptibility to cancer | 1.00 | 0.82–1.22 | 0.984 |
| Seriousness of cancer | 1.04 | 0.80–1.35 | 0.777 |
| Benefits of cancer screening | 1.13 | 0.86–1.47 | 0.380 |
| Burden to participation before cancer screening | 0.44 | 0.32–0.60 | <0.001 |
| Burden to participation at the time of cancer screening | 1.16 | 0.91–1.47 | 0.235 |
| Importance of cancer screening | 0.82 | 0.61–1.11 | 0.204 |
| Cues to participation in screening | 1.13 | 0.91–1.40 | 0.259 |
| Parameter | OR | 95%CI | p-Value |
|---|---|---|---|
| Work status | |||
| Unemployed | Ref. | ---- | ---- |
| Self-employed | 1.79 | 0.66–4.89 | 0.253 |
| Regular employment | 1.89 | 1.01–3.54 | 0.046 |
| Part-time job | 1.98 | 1.00–3.93 | 0.050 |
| Student | 1.71 | 0.60–4.85 | 0.315 |
| Housewife | 1.60 | 0.83–3.06 | 0.160 |
| HBM | |||
| Susceptibility to cancer | 1.20 | 1.00–1.43 | 0.045 |
| Seriousness of cancer | 0.99 | 0.80–1.21 | 0.892 |
| Benefits of cancer screening | 1.30 | 1.06–1.60 | 0.013 |
| Burden to participation before cancer screening | 1.05 | 0.79–1.38 | 0.744 |
| Burden to participation at the time of cancer screening | 1.17 | 0.94–1.44 | 0.161 |
| Importance of cancer screening | 0.61 | 0.48–0.78 | <0.001 |
| Cues to participation in screening | 1.02 | 0.84–1.23 | 0.839 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Z.; Kawasaki, H.; Tsunematsu, M.; Cui, Y.; Rahman, M.M.; Yamasaki, S.; Li, Y.; Kakehashi, M. Breast Cancer Screening and Perceptions of Harm among Young Adults in Japan: Results of a Cross-Sectional Online Survey. Curr. Oncol. 2023, 30, 2073-2087. https://doi.org/10.3390/curroncol30020161
Cui Z, Kawasaki H, Tsunematsu M, Cui Y, Rahman MM, Yamasaki S, Li Y, Kakehashi M. Breast Cancer Screening and Perceptions of Harm among Young Adults in Japan: Results of a Cross-Sectional Online Survey. Current Oncology. 2023; 30(2):2073-2087. https://doi.org/10.3390/curroncol30020161
Chicago/Turabian StyleCui, Zhengai, Hiromi Kawasaki, Miwako Tsunematsu, Yingai Cui, Md Moshiur Rahman, Satoko Yamasaki, Yuan Li, and Masayuki Kakehashi. 2023. "Breast Cancer Screening and Perceptions of Harm among Young Adults in Japan: Results of a Cross-Sectional Online Survey" Current Oncology 30, no. 2: 2073-2087. https://doi.org/10.3390/curroncol30020161