Prevalence and Persistence of Anxiety and Depression over Five Years since Breast Cancer Diagnosis—The NEON-BC Prospective Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
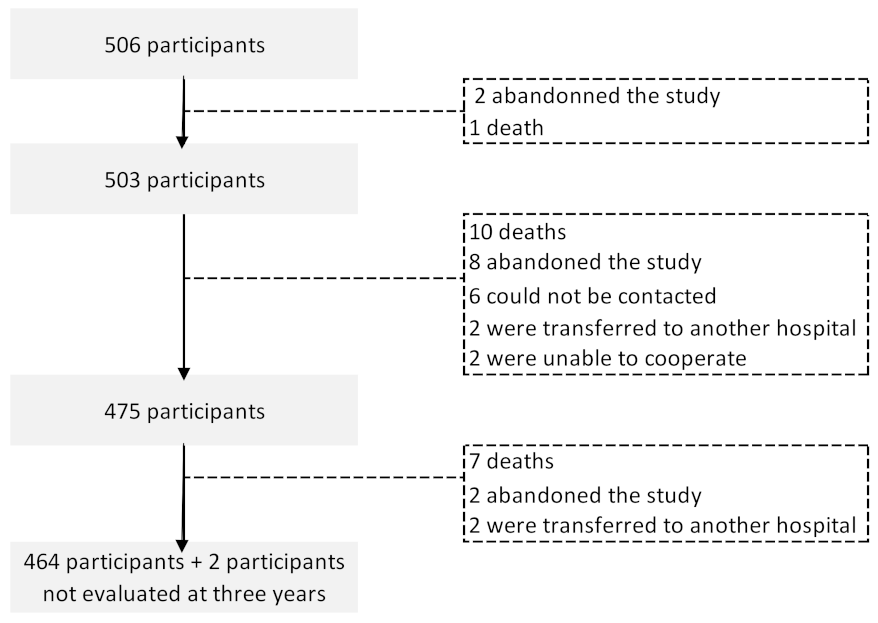
2.1. The NEON-BC Cohort
2.2. Measures
2.3. Statistical Analysis
2.4. Ethic Approval
3. Results
3.1. Participants Sociodemographic, Lifestyles and Clinical Characterization
3.2. Prevalence of Anxiety and Depression Overt the 5-Year Follow-Up
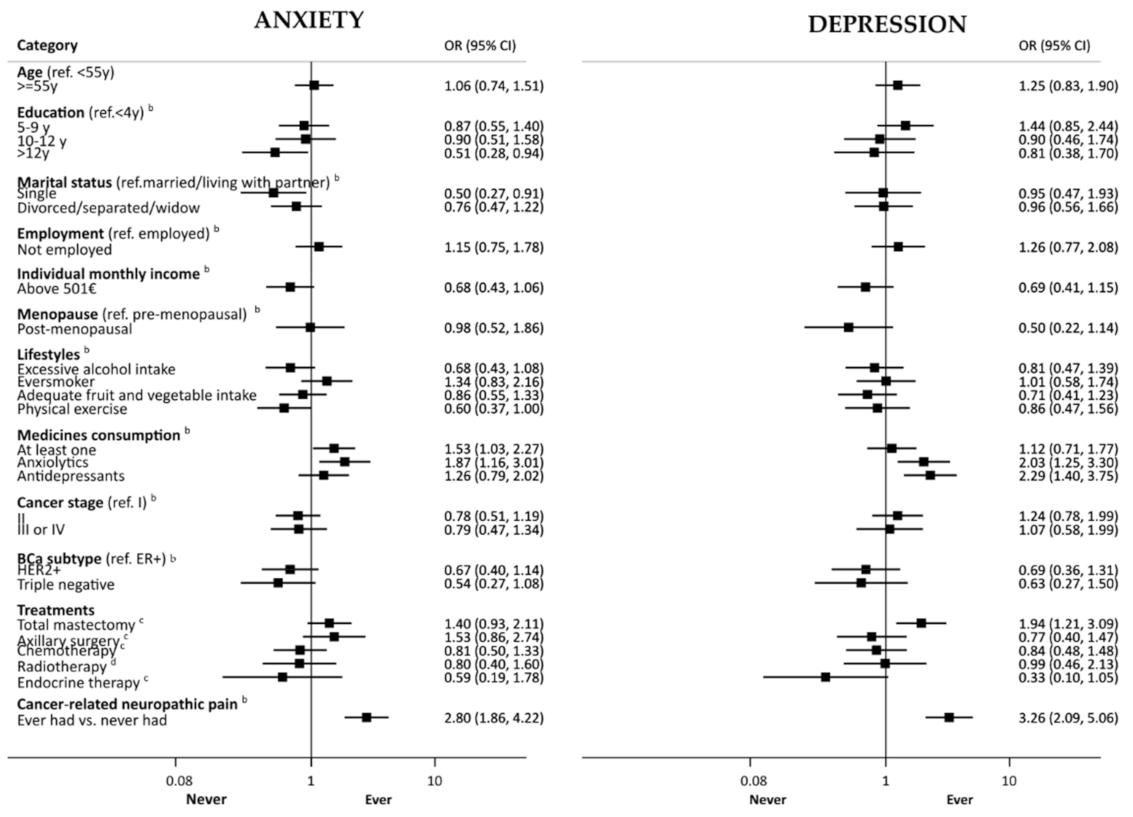
3.3. Factors Associated with Anxiety and Depression
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Maajani, K.; Jalali, A.; Alipour, S.; Khodadost, M.; Tohidinik, H.R.; Yazdani, K. The Global and Regional Survival Rate of Women With Breast Cancer: A Systematic Review and Meta-analysis. Clin. Breast Cancer 2019, 19, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Carreira, H.; Williams, R.; Müller, M.; Harewood, R.; Stanway, S.; Bhaskaran, K. Associations Between Breast Cancer Survivorship and Adverse Mental Health Outcomes: A Systematic Review. J. Natl. Cancer Inst. 2018, 110, 1311–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Zhou, Y.; Feng, Z.; Xu, Y.; Zeng, G. Longitudinal Trends in Anxiety, Depression, and Quality of Life During Different Intermittent Periods of Adjuvant Breast Cancer Chemotherapy. Cancer Nurs. 2018, 41, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wang, N.; Zhong, L.; Wang, S.; Zheng, Y.; Yang, B.; Zhang, J.; Lin, Y.; Wang, Z. Prognostic value of depression and anxiety on breast cancer recurrence and mortality: A systematic review and meta-analysis of 282,203 patients. Mol. Psychiatry 2020, 25, 3186–3197. [Google Scholar] [CrossRef]
- Pereira, S.; Fontes, F.; Sonin, T.; Dias, T.; Fragoso, M.; Castro-Lopes, J.; Lunet, N. Neuropathic Pain After Breast Cancer Treatment: Characterization and Risk Factors. J. Pain Symptom Manag. 2017, 54, 877–888. [Google Scholar] [CrossRef] [Green Version]
- Araújo, N.; Severo, M.; Lopes-Conceição, L.; Fontes, F.; Dias, T.; Branco, M.; Morais, S.; Cruz, V.T.; Ruano, L.; Pereira, S.; et al. Trajectories of cognitive performance over five years in a prospective cohort of patients with breast cancer (NEON-BC). Breast 2021, 58, 130–137. [Google Scholar] [CrossRef]
- Cook, S.A.; Salmon, P.; Hayes, G.; Byrne, A.; Fisher, P.L. Predictors of emotional distress a year or more after diagnosis of cancer: A systematic review of the literature. Psycho-Oncology 2018, 27, 791–801. [Google Scholar] [CrossRef]
- Breidenbach, C.; Heidkamp, P.; Hiltrop, K.; Pfaff, H.; Enders, A.; Ernstmann, N.; Kowalski, C. Prevalence and determinants of anxiety and depression in long-term breast cancer survivors. BMC Psychiatry 2022, 22, 101. [Google Scholar] [CrossRef]
- Liu, B.; Wu, X.; Shi, L.; Li, H.; Wu, D.; Lai, X.; Li, Y.; Yang, Y.; Li, D. Correlations of social isolation and anxiety and depression symptoms among patients with breast cancer of Heilongjiang province in China: The mediating role of social support. Nurs. Open 2021, 8, 1981–1989. [Google Scholar] [CrossRef]
- Okati-Aliabad, H.; Ansari-Moghadam, A.; Mohammadi, M.; Kargar, S.; Shahraki-Sanavi, F. The prevalence of anxiety and depression and its association with coping strategies, supportive care needs, and social support among women with breast cancer. Supportive Care Cancer 2022, 30, 703–710. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Fontes, F.; Sonin, T.; Dias, T.; Fragoso, M.; Castro-Lopes, J.; Lunet, N. Neurological complications of breast cancer: Study protocol of a prospective cohort study. BMJ Open 2014, 4, e006301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitas, S.; Simões, M.R.; Alves, L.; Santana, I. Montreal Cognitive Assessment (MoCA): Normative study for the Portuguese population. J. Clin. Exp. Neuropsychol. 2011, 33, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Pais-Ribeiro, J.; Silva, I.; Ferreira, T.; Martins, A.; Meneses, R.; Baltar, M. Validation study of a Portuguese version of the Hospital Anxiety and Depression Scale. Psychol. Health Med. 2007, 12, 225–235. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Meader, N.; Symonds, P. Diagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: A meta-analysis. J. Affect. Disord. 2010, 126, 335–348. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Kim, S.-W.; Shin, I.-S.; Park, M.-H.; Yoon, J.-H.; Yoon, J.-S.; Kim, J.-M. Changes in depression status during the year after breast cancer surgery and impact on quality of life and functioning. Gen. Hosp. Psychiatry 2018, 50, 33–37. [Google Scholar] [CrossRef]
- Faye-Schjøll, H.H.; Schou-Bredal, I. Pessimism predicts anxiety and depression in breast cancer survivors: A 5-year follow-up study. Psychooncology 2019, 28, 1314–1320. [Google Scholar] [CrossRef]
- Hopwood, P.; Sumo, G.; Mills, J.; Haviland, J.; Bliss, J.M. The course of anxiety and depression over 5 years of follow-up and risk factors in women with early breast cancer: Results from the UK Standardisation of Radiotherapy Trials (START). Breast 2010, 19, 84–91. [Google Scholar] [CrossRef]
- Tsaras, K.; Papathanasiou, I.V.; Mitsi, D.; Veneti, A.; Kelesi, M.; Zyga, S.; Fradelos, E.C. Assessment of Depression and Anxiety in Breast Cancer Patients: Prevalence and Associated Factors. Asian Pac. J. Cancer Prev. 2018, 19, 1661–1669. [Google Scholar] [CrossRef] [PubMed]
- Civilotti, C.; Botto, R.; Maran, D.A.; Leonardis, B.D.; Bianciotto, B.; Stanizzo, M.R. Anxiety and Depression in Women Newly Diagnosed with Breast Cancer and Waiting for Surgery: Prevalence and Associations with Socio-Demographic Variables. Medicina 2021, 57, 454. [Google Scholar] [CrossRef] [PubMed]
- Avis, N.E.; Levine, B.; Marshall, S.A.; Ip, E.H. Longitudinal Examination of Symptom Profiles Among Breast Cancer Survivors. J. Pain Symptom Manag. 2017, 53, 703–710. [Google Scholar] [CrossRef] [Green Version]
- Borstelmann, N.A.; Rosenberg, S.M.; Ruddy, K.J.; Tamimi, R.M.; Gelber, S.; Schapira, L.; Come, S.; Borges, V.; Morgan, E.; Partridge, A.H. Partner support and anxiety in young women with breast cancer. Psychooncology 2015, 24, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- Landeiro, L.C.G.; Gagliato, D.M.; Fêde, A.B.; Fraile, N.M.; Lopez, R.M.; Da Fonseca, L.G.; Petry, V.; Testa, L.; Hoff, P.M.; Mano, M.S. Return to work after breast cancer diagnosis: An observational prospective study in Brazil. Cancer 2018, 124, 4700–4710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monteiro, I.; Morais, S.; Costa, A.R.; Lopes-Conceição, L.; Araújo, N.; Fontes, F.; Dias, T.; Pereira, S.; Lunet, N. Changes in employment status up to 5 years after breast cancer diagnosis: A prospective cohort study. Breast 2019, 48, 38–44. [Google Scholar] [CrossRef]
- Quintana López, V.A.; Díaz López, K.J.; Caire Juvera, G. Interventions to improve healthy lifestyles and their effects on psychological variables among breast cancer survivors: A systematic review. Nutr. Hosp. 2018, 35, 979–992. [Google Scholar] [CrossRef]
- Aydin, M.; Kose, E.; Odabas, I.; Meric Bingul, B.; Demirci, D.; Aydin, Z. The Effect of Exercise on Life Quality and Depression Levels of Breast Cancer Patients. Asian Pac. J. Cancer Prev. 2021, 22, 725–732. [Google Scholar] [CrossRef]
- Padmalatha, S.; Tsai, Y.-T.; Ku, H.-C.; Wu, Y.-L.; Yu, T.; Fang, S.-Y.; Ko, N.-Y. Higher Risk of Depression After Total Mastectomy Versus Breast Reconstruction Among Adult Women With Breast Cancer: A Systematic Review and Metaregression. Clin. Breast Cancer 2021, 21, e526–e538. [Google Scholar] [CrossRef]
- Koçan, S.; Gürsoy, A. Body Image of Women with Breast Cancer After Mastectomy: A Qualitative Research. J. Breast Health 2016, 12, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Schou Bredal, I.; Smeby, N.A.; Ottesen, S.; Warncke, T.; Schlichting, E. Chronic Pain in Breast Cancer Survivors: Comparison of Psychosocial, Surgical, and Medical Characteristics Between Survivors With and Without Pain. J. Pain Symptom Manag. 2014, 48, 852–862. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable (Number of Respondents) | n (%) | ||
|---|---|---|---|
| Socio-demographics | |||
| Age (years) (n = 506) | |||
| <55 | 254 (50.2) | ||
| ≥55 | 252 (49.8) | ||
| Education (years) (n = 506) | |||
| ≤4 | 216 (42.7) | ||
| 5–9 | 145 (28.7) | ||
| ≥10 | 145 (28.7) | ||
| Living in Greater Porto area (n = 506) | 226 (44.7) | ||
| Marital status (n = 506) | |||
| Married/living together | 353 (69.8) | ||
| Single | 53 (10.5) | ||
| Widower/divorced | 100 (19.8) | ||
| Employed (n = 503) | 279 (55.5) | ||
| Individual monthly income above 500€ (n = 467) | 210 (45.0) | ||
| Post-menopausal (n = 506) | 288 (56.9) | ||
| Lifestyles | |||
| Alcohol consumption, more than 10 g/day (n = 505) | 97 (19.2) | ||
| Ever smoker (n = 475) | 97 (20.4) | ||
| Fruits and vegetables ≥ 5 portions/day (n = 472) | 104 (22.0) | ||
| Practicing physical activity (n = 475) | 80 (16.8) | ||
| Comorbidities | |||
| Hypertension (n = 506) | 169 (33.4) | ||
| Diabetes (n = 506) | 50 (9.9) | ||
| Previous cancer (n = 475) | 17 (3.6) | ||
| Chronic medicines consumption (n = 462) | |||
| None | 181 (35.8) | ||
| One | 85 (16.8) | ||
| Two to five | 161 (31.8) | ||
| More than five | 79 (15.6) | ||
| Anxiolytics | 98 (19.4) | ||
| Antidepressants | 95 (18.8) | ||
| Clinical characteristics of the breast tumor | |||
| Cancer stage (n = 505) | |||
| 0/I | 270 (53.5) | ||
| II | 156 (30.9) | ||
| III/IV | 79 (15.6) | ||
| Breast cancer subtype (n = 474) | |||
| HR+/HER2− | 363 (76.4) | ||
| HER2+ | 73 (15.4) | ||
| Triple negative | 39 (8.2) | ||
| Period of Follow-Up | |||
|---|---|---|---|
| During the First Year | Between the First and the Third Year | Between the Third and the Fifth Year | |
| n (%) | n (%) | n (%) | |
| Breast cancer treatment | |||
| Breast conserving surgery a | 250 (49.5) | 0 | 0 |
| Mastectomy a | 254 (50.3) | 0 | 0 |
| Breast reconstruction a | 58 (11.5) | 26 (5.5) | 34 (7.3) |
| Axillary lymph node dissection a | 174 (34.5) | 1 (0.2) | 0 |
| Chemotherapy b | 298 (59.2) | 8 (1.7) | 9 (1.9) |
| Radiotherapy b | 370 (73.6) | 6 (1.3) | 2 (0.4) |
| Endocrine therapy b | 422 (83.9) | 394 (82.9) | 381 (81.8) |
| Targeted therapy b | 67 (13.3) | 3 (0.6) | 3 (0.6) |
| Breast cancer recurrence b | 6 (1.2) | 7 (1.5) | 3 (0.7) |
| New primary tumor b | 4 (0.8) | 11 (2.2) | 10 (2.1) |
| Changes in socio-demographic conditions | |||
| Became widowed/divorced/separated c | 13 (3.7) | 17 (5.0) | 9 (3.0) |
| Loss of job d | not evaluated | 24 (9.8) | 5 (2.1) |
| Became retired d | not evaluated | 27 (11.1) | 14 (5.7) |
| Loss of income e | not evaluated | 48 (10.3) | 98 (20.5) |
| Baseline | One-Year | Three-Year | Five-Year | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| Anxiety | ||||
| Prevalent cases | 192 (38.0) | 127 (25.3) | 100 (21.1) | 118 (25.4) |
| Incident cases a | - | 38 (12.1) | 22 (7.0) | 13 (4.2) |
| Permanent recovery b | - | 21 (10.9) | 10 (5.2) | 3 (1.6) |
| Persistent anxiety c | - | 89 (46.4) | 46 (24.0) | 35 (18.2) |
| Depression | ||||
| Prevalent cases | 41 (8.1) | 66 (13.1) | 43 (9.1) | 48 (10.3) |
| Incident cases a | - | 50 (10.8) | 16 (3.4) | 13 (2.8) |
| Permanent recovery b | - | 9 (22.0) | 0 | 7 (17.0) |
| Persistent depression c | - | 16 (39.0) | 8 (19.5) | 7 (17.0) |
| Anxiety during Follow-Up (Ever vs. Never) | Depression during Follow-Up (Ever vs. Never) | ||
|---|---|---|---|
| OR [95% CI] | OR [95% CI] | ||
| Age (years) ≥55 vs. <55 | 1.20 [0.71, 2.05] | 1.09 [0.67, 1.77] | |
| Education (years) 5–9 vs. ≤4 | 1.08 [0.55, 2.12] | 1.36 [0.74, 2.51] | a |
| Education (years) 10–12 vs. ≤4 | 1.46 [0.67, 3.17] | 0.78 [0.35, 1.74] | b |
| Education (years) >12 vs. ≤4 | 0.33 [0.10, 1.05] | 0.64 [0.25, 1.60] | b |
| Post-menopausal vs. pre-menopausal | 1.02 [0.38, 2.68] | 0.57 [0.22, 1.44] | b |
| Single vs. married/living with partner | 0.35 [0.12, 1.07] | 1.11 [0.50, 2.46] | b |
| Widow/divorced/separated vs. married/living with partner | 0.70 [0.34, 1.42] | 0.92 [0.47, 1.77] | b |
| Became widowed/divorced/separated | 2.10 [0.79, 5.57] | 1.72 [0.76, 3.89] | b |
| Employed vs. unemployed | 0.93 [0.49, 1.75] | 1.55 [0.87, 2.77] | b |
| Lost job vs. still employed | 1.62 [0.52, 5.08] | 2.62 [1.10, 6.20] | b |
| Retired vs. still employed | 0.59 [0.21, 1.65] | 1.52 [0.70, 3.33] | b |
| Individual monthly income ≤500€ vs. >500€ | 0.51 [0.26, 1.01] | 0.76 [0.42, 1.38] | b |
| Lost income | 1.16 [0.61, 2.23] | 1.99 [1.16, 3.41] | b |
| Alcohol >10 g/day vs. ≤10 g/day | 0.73 [0.36, 1.46] | 0.84 [0.45, 1.58] | b |
| Ever smoker vs. never smoker | 1.29 [0.65, 2.58] | 1.22 [0.65, 2.27] | b |
| Fruit and vegetables ≥5 pieces/day vs. <5/day | 0.68 [0.34, 1.38] | 0.47 [0.22, 0.99] | b |
| Practicing physical activity vs. not | 0.51 [0.22, 1.17] | 0.67 [0.31, 1.45] | b |
| Consumption of at least one medicine vs. none | 1.13 [0.63, 2.02] | 1.06 [0.62, 1.81] | b |
| Anxiolytics vs. no anxiolytics | 1.46 [0.73, 2.91] | 1.54 [0.85, 2.78] | b |
| Antidepressants vs. no antidepressants | 1.36 [0.70, 2.63] | 2.06 [1.16, 3.68] | b |
| Cancer stage II vs. 0/I | 0.43 [0.22, 0.85] | 1.27 [0.73, 2.20] | b |
| Cancer stage III/IV vs. 0/I | 0.61 [0.27, 1.35] | 0.96 [0.46, 2.03] | b |
| Subtype HER2+ vs. HR+/HER2− | 0.87 [0.41, 1.82] | 0.88 [0.44, 1.76] | b |
| Subtype Triple negative vs. HR+/HER2− | 0.12 [0.02, 0.95] | 0.39 [0.11, 1.32] | b |
| Mastectomy vs. breast conserving surgery | 1.25 [0.67, 2.36] | 1.87 [1.08, 3.23] | c |
| Breast reconstruction vs. none | 0.95 [0.44, 2.05] | 0.82 [0.42, 1.59] | d |
| Axillary surgery vs. LND | 1.01 [0.40, 2.55] | 0.65 [0.30, 1.38] | c |
| Chemotherapy vs. no chemotherapy | 0.60 [0.29, 1.26] | 0.84 [0.43, 1.63] | c |
| Radiotherapy vs. no radiotherapy | 0.47 [0.15, 1.51] | 0.77 [0.31, 1.94] | e |
| Endocrine therapy vs. no endocrine therapy | 0.58 [0.12, 2.80] | 0.31 [0.09, 1.06] | c |
| Trastuzumab vs. no trastuzumab | 0.17 [0.01, 2.22] | 0.57 [0.05, 6.19] | c |
| Cancer-related neuropathic pain anytime during the Follow-up vs. never | 2.43 [1.35, 4.36] | 2.72 [1.63, 4.55] | b |
| Recurrence | 0.83 [0.09, 7.85] | 0.68 [0.08, 5.72] | b |
| Second primary cancer | 1.33 [0.39, 4.57] | 0.75 [0.21, 2.63] | b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopes, C.; Lopes-Conceição, L.; Fontes, F.; Ferreira, A.; Pereira, S.; Lunet, N.; Araújo, N. Prevalence and Persistence of Anxiety and Depression over Five Years since Breast Cancer Diagnosis—The NEON-BC Prospective Study. Curr. Oncol. 2022, 29, 2141-2153. https://doi.org/10.3390/curroncol29030173
Lopes C, Lopes-Conceição L, Fontes F, Ferreira A, Pereira S, Lunet N, Araújo N. Prevalence and Persistence of Anxiety and Depression over Five Years since Breast Cancer Diagnosis—The NEON-BC Prospective Study. Current Oncology. 2022; 29(3):2141-2153. https://doi.org/10.3390/curroncol29030173
Chicago/Turabian StyleLopes, Catarina, Luisa Lopes-Conceição, Filipa Fontes, Augusto Ferreira, Susana Pereira, Nuno Lunet, and Natália Araújo. 2022. "Prevalence and Persistence of Anxiety and Depression over Five Years since Breast Cancer Diagnosis—The NEON-BC Prospective Study" Current Oncology 29, no. 3: 2141-2153. https://doi.org/10.3390/curroncol29030173