
Esophageal Magnetic Compression Anastomosis in Esophageal Atresia Repair: A PRISMA-Compliant Systematic Review and Comparison with a Novel Approach

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
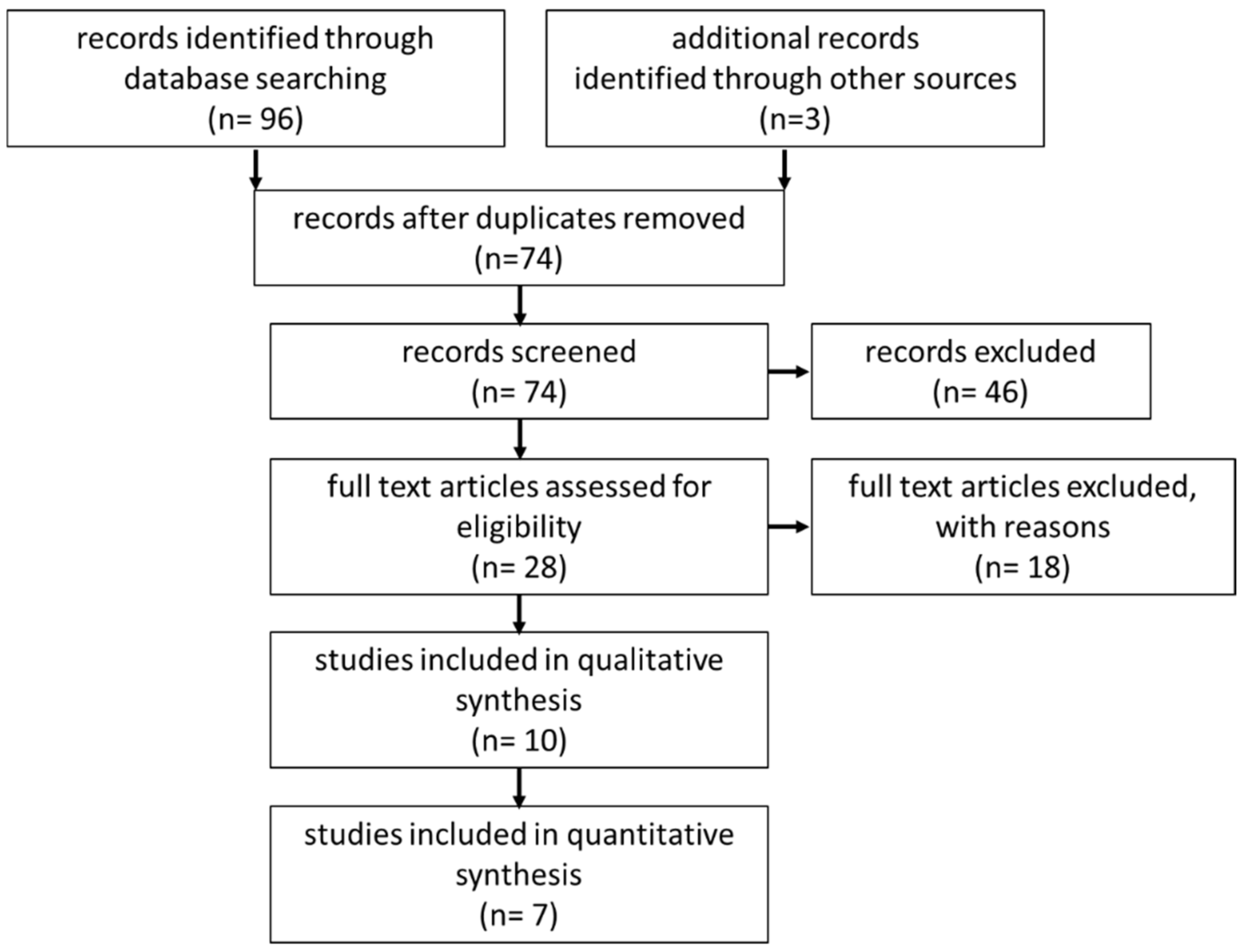
2.1. Systematic Review
2.2. Subgroup Analysis
2.3. Statistical Analysis
3. Results
3.1. Systematic Review
3.2. Subgroup Analysis
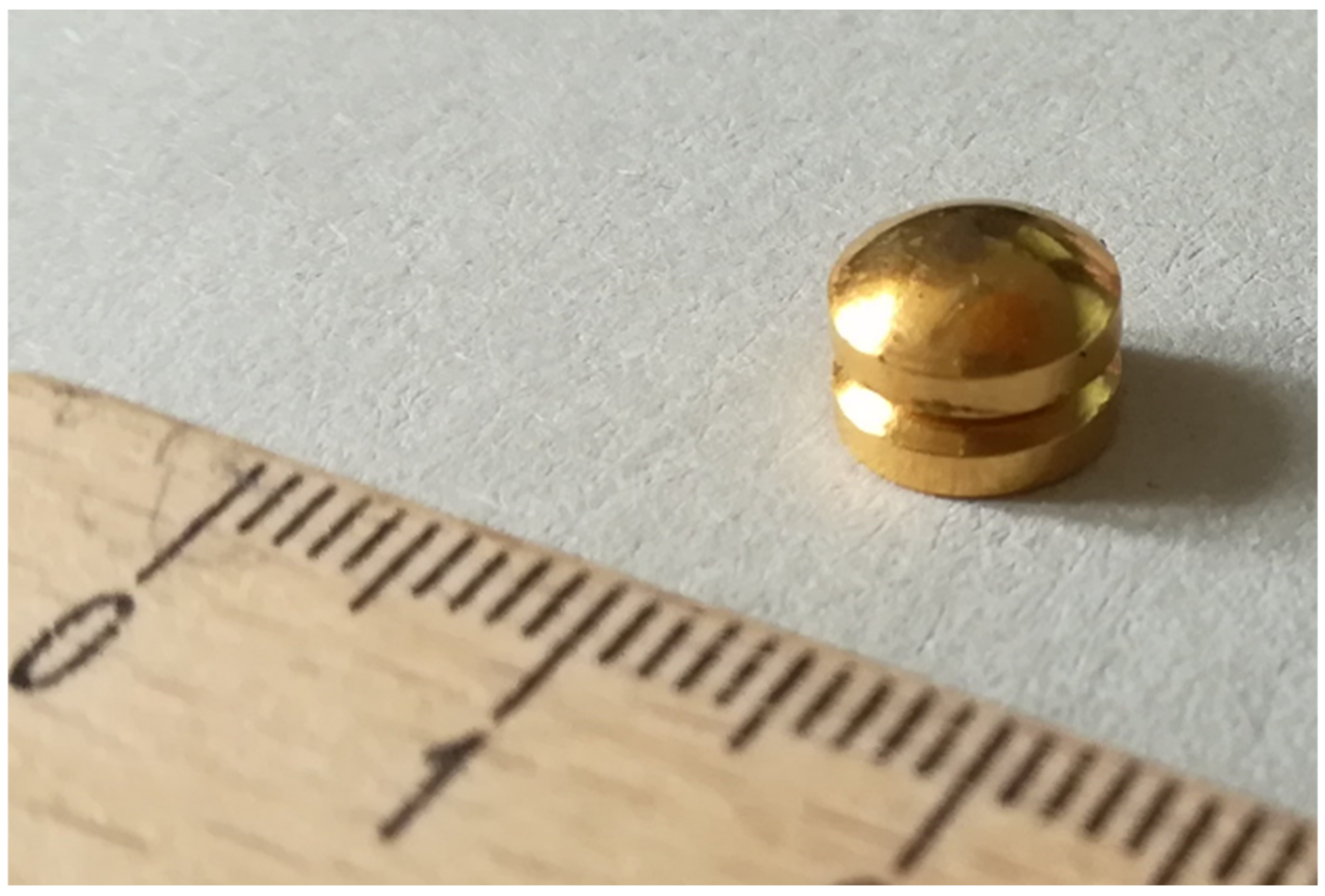
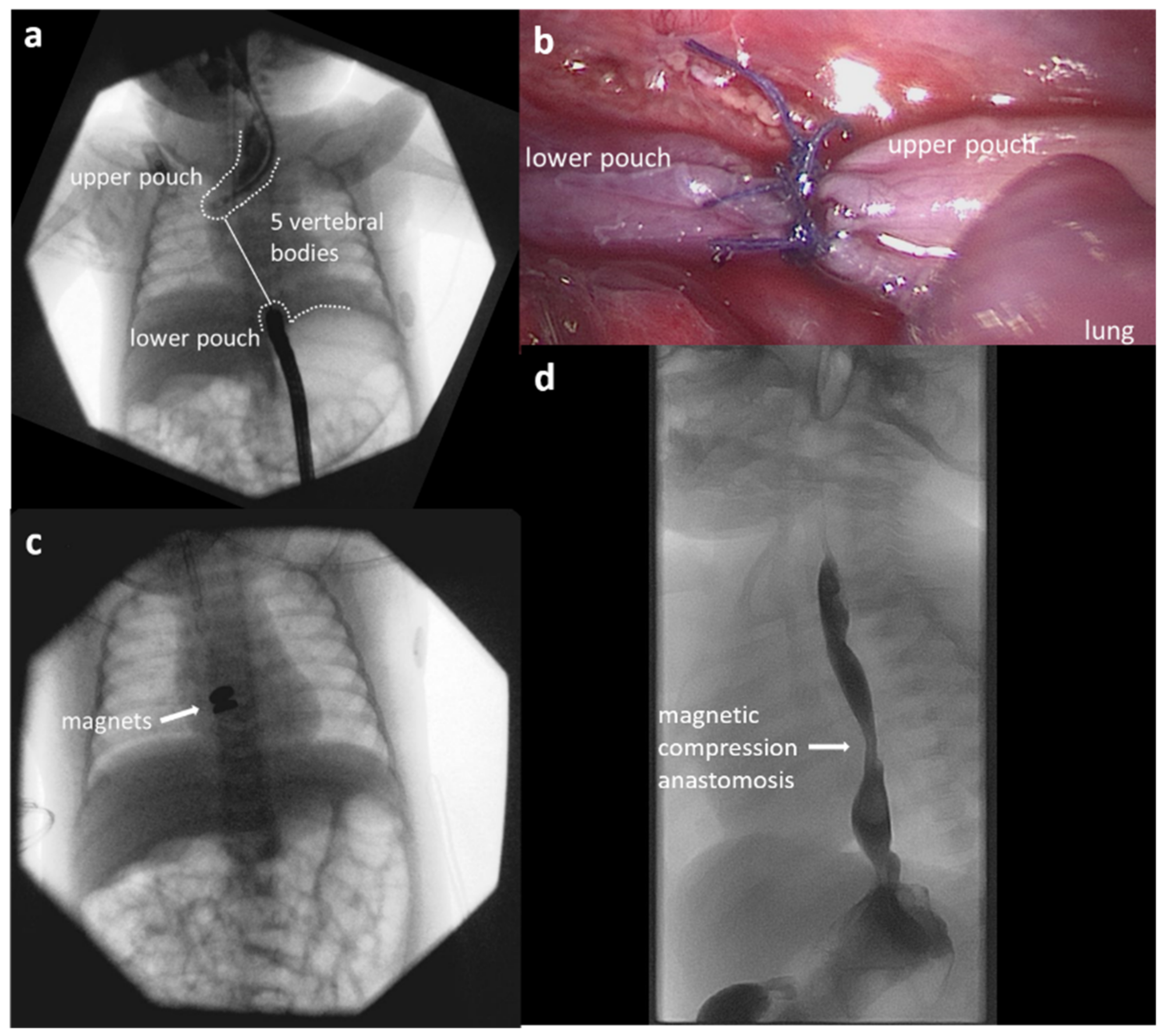
3.3. Case Report
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Holcomb, G.W., 3rd. Thoracoscopic surgery for esophageal atresia. Pediatr. Surg. Int. 2017, 33, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Okuyama, H.; Tazuke, Y.; Ueno, T.; Yamanaka, H.; Takama, Y.; Saka, R.; Usui, N.; Soh, H.; Yonekura, T. Learning curve for the thoracoscopic repair of esophageal atresia with tracheoesophageal fistula. Asian J. Endosc. Surg. 2018, 11, 30–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadil, T.; Koivusalo, A.; Pakarinen, M.; Mikkelsen, A.; Emblem, R.; Svensson, J.F.; Ehrén, H.; Jönsson, L.; Bäckstrand, J.; Lilja, H.E.; et al. Surgical repair of long-gap esophageal atresia: A retrospective study comparing the management of long-gap esophageal atresia in the Nordic countries. J. Pediatr. Surg. 2019, 54, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Yang, Y.; Zheng, C.; Dong, R.; Zheng, S. Surgical outcomes of different approaches to esophageal replacement in long-gap esophageal atresia: A systematic review. Medicine 2017, 96, e6942. [Google Scholar] [CrossRef]
- Lee, H.Q.; Hawley, A.; Doak, J.; Nightingale, M.G.; Hutson, J.M. Long-gap oesophageal atresia: Comparison of delayed primary anastomosis and oesophageal replacement with gastric tube. J. Pediatr. Surg. 2014, 49, 1762–1766. [Google Scholar] [CrossRef]
- Hendren, W.H.; Hale, J.R. Esophageal atresia treated by electromagnetic bougienage and subsequent repair. J. Pediatr. Surg. 1976, 11, 713–722. [Google Scholar] [CrossRef]
- Zaritzky, M.; Ben, R.; Johnston, K. Magnetic gastrointestinal anastomosis in pediatric patients. J. Pediatr. Surg. 2014, 49, 1131–1137. [Google Scholar] [CrossRef]
- Slater, B.J.; Borobia, P.; Lovvorn, H.N.; Raees, M.A.; Bass, K.D.; Almond, S.; Hoover, J.D.; Kumar, T.; Zaritzky, M. Use of Magnets as a Minimally Invasive Approach for Anastomosis in Esophageal Atresia: Long-Term Outcomes. J. Laparoendosc. Adv. Surg. Tech. 2019, 29, 1202–1206. [Google Scholar] [CrossRef]
- Liu, S.Q.; Lv, Y.; Fang, Y.; Luo, R.X.; Zhao, J.R.; Luo, R.G.; Li, Y.M.; Zhang, J.; Zhang, P.F.; Guo, J.Z.; et al. Magnetic compression for anastomosis in treating an infant born with long-gap oesophageal atresia: A case report. Medicine 2020, 99, e22472. [Google Scholar] [CrossRef]
- Ellebaek, M.B.B.; Qvist, N.; Rasmussen, L. Magnetic Compression Anastomosis in Long-Gap Esophageal Atresia Gross Type A: A Case Report. Eur. J. Pediatr. Surg. Rep. 2018, 6, e37–e39. [Google Scholar] [CrossRef] [Green Version]
- Dorman, R.M.; Vali, K.; Harmon, C.M.; Zaritzky, M.; Bass, K.D. Repair of esophageal atresia with proximal fistula using endoscopic magnetic compression anastomosis (magnamosis) after staged lengthening. Pediatr. Surg. Int. 2016, 32, 525–528. [Google Scholar] [CrossRef]
- Wolfe, E.; Zidane, M.; Hancock, B.J.; Min, S.A.L.; Zaritzky, M.; Keijzer, R. Magnamosis for esophageal atresia is associated with anastomotic strictures requiring an increased number of dilatations. J. Pediatr. Surg. 2020, 55, 821–823. [Google Scholar] [CrossRef]
- Lovvorn, H.N.; Baron, C.M.; Danko, M.E.; Novotny, N.M.; Bucher, B.T.; Johnston, K.K.; Zaritzky, M.F. Staged repair of esophageal atresia: Pouch approximation and catheter-based magnetic anastomosis. J. Pediatr. Surg. Case Rep. 2014, 2, 170–175. [Google Scholar] [CrossRef] [Green Version]
- Sterlin, A.; Evans, L.; Mahler, S.; Lindner, A.; Dickmann, J.; Heimann, A.; Sahlabadi, M.; Aribindi, V.; Harrison, M.R.; Muensterer, O.J. An experimental study on long term outcomes after magnetic esophageal compression anastomosis in piglets. J. Pediatr. Surg. 2022, 57, 34–40. [Google Scholar] [CrossRef]
- Muensterer, O.J.; Evans, L.L.; Sterlin, A.; Sahlabadi, M.; Aribindi, V.; Lindner, A.; König, T.; Harrison, M.R. Novel Device for Endoluminal Esophageal Atresia Repair: First-in-Human Experience. Pediatrics 2021, 148, e2020049627. [Google Scholar] [CrossRef]
- Muensterer, O.J.; Sterlin, A.; von Sochaczewski, C.O.; Lindner, A.; Heimann, A.; Balus, A.; Dickmann, J.; Nuber, M.; Patel, V.H.; Manfredi, M.A.; et al. An experimental study on magnetic esophageal compression anastomosis in piglets. J. Pediatr. Surg. 2020, 55, 425–432. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Zaritzky, M.; Ben, R.; Zylberg, G.I.; Yampolsky, B. Magnetic compression anastomosis as a nonsurgical treatment for esophageal atresia. Pediatr. Radiol. 2009, 39, 945–949. [Google Scholar] [CrossRef]
- Conforti, A.; Pellegrino, C.; Fusaro, F.; Iacobelli, B.D.; Valfre, L.; Iacusso, C.; Lars, R.; Bagolan, P. Magnetic anastomosis for long gap EA: Early outcomes of a minimally invasive technique. In Proceedings of the 22nd European Congress of the European Paediatric Surgeon’s Association 2021, Athens, Greece, 1–4 September 2021. [Google Scholar]
- Okata, Y.; Maeda, K.; Bitoh, Y.; Mishima, Y.; Tamaki, A.; Morita, K.; Endo, K.; Hisamatsu, C.; Fukuzawa, H.; Yokoi, A. Evaluation of the intraoperative risk factors for esophageal anastomotic complications after primary repair of esophageal atresia with tracheoesophageal fistula. Pediatr. Surg. Int. 2016, 32, 869–873. [Google Scholar] [CrossRef]
- Shah, R.; Varjavandi, V.; Krishnan, U. Predictive factors for complications in children with esophageal atresia and tracheoesophageal fistula. Dis. Esophagus 2015, 28, 216–223. [Google Scholar] [CrossRef]
- Tambucci, R.; Angelino, G.; De Angelis, P.; Torroni, F.; Caldaro, T.; Balassone, V.; Contini, A.C.; Romeo, E.F.; Rea, F.; Faraci, S.; et al. Anastomotic Strictures after Esophageal Atresia Repair: Incidence, Investigations, and Management, Including Treatment of Refractory and Recurrent Strictures. Front. Pediatr. 2017, 5, 120. [Google Scholar] [CrossRef] [Green Version]
- Bagolan, P.; Valfre, L.; Morini, F.; Conforti, A. Long-gap esophageal atresia: Traction-growth and anastomosis—Before and beyond. Dis. Esophagus 2013, 26, 372–379. [Google Scholar] [CrossRef]
- Campos, J.; Tanny, S.P.T.; Kuyruk, S.; Sekaran, P.; Hawley, A.; Brooks, J.-A.; Bekhit, E.; Hutson, J.M.; Crameri, J.; McLeod, E.; et al. The burden of esophageal dilatations following repair of esophageal atresia. J. Pediatr. Surg. 2020, 55, 2329–2334. [Google Scholar] [CrossRef]
- Dingemann, C.; Dietrich, J.; Zeidler, J.; Blaser, J.; Gosemann, J.-H.; Ure, B.M.; Lacher, M. Early complications after esophageal atresia repair: Analysis of a German health insurance database covering a population of 8 million. Dis. Esophagus 2016, 29, 780–786. [Google Scholar] [CrossRef]
- Vergouwe, F.W.T.; Vlot, J.; Ijsselstijn, H.; Spaander, M.C.W.; Van Rosmalen, J.; Oomen, M.W.N.; Hulscher, J.B.F.; Dirix, M.; Bruno, M.J.; Schurink, M.; et al. Risk factors for refractory anastomotic strictures after oesophageal atresia repair: A multicentre study. Arch. Dis. Child. 2019, 104, 152–157. [Google Scholar] [CrossRef]
- McCann, M.E.; de Graaff, J.C.; Dorris, L.; Disma, N.; Withington, D.; Bell, G.; Grobler, A.; Stargatt, R.; Hunt, R.W.; Sheppard, S.J.; et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS): An international, multicentre, randomised, controlled equivalence trial. Lancet 2019, 393, 664–677. [Google Scholar] [CrossRef]
- Powell, L.; Frawley, J.; Crameri, J.; Teague, W.J.; Frawley, G.P. Oesophageal atresia: Are “long gap” patients at greater anesthetic risk? Paediatr. Anaesth. 2018, 28, 249–256. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Language | English |
| Date | Any |
| Subject | Human studies |
| Study type | Retrospective Prospective Case reports Congress abstracts |
| Excluded | Videos |
| Search terms | Magnets Anastomosis Esophagus |
| Author | Year of Publication | Number of Patients | Type of Esophageal Atresia | Age at Intervention (Mean/Days (d), Months (mo)) | Time to Patency (Days) | Anastomotic Leakage |
|---|---|---|---|---|---|---|
| Zaritky et al. [18] | 2009 | 5 | Type A: 40% Type B: 40% Type C: 20% | range 30–120 d | 4.8 (range 2–7) | none |
| Zaritky et al. [7] | 2014 | 9 | Type A: 66.7% Type C: 33.4% | 3 mo (range 23 d–5 mo) | 4.2 (range 3–6) | none |
| Slater et al. [8] | 2019 | 13 | Type A: 85% Type C: 15% | 4.5 mo (range 2–7.5 mo) | 6.3 (range 3–13) | none |
| Wolfe et al. [12] | 2020 | 1 | Type A | n.d. | 5 | none |
| Lovvorn et al. [13] | 2014 | 2 | Type A: 100% | 5.25 mo (range 4–6.5 mo) | 7.5 (range 6–10) | none |
| Dorman et al. [11] | 2016 | 1 | Type B | 7 mo | 13 | none |
| Ellebaek et al. [10] | 2018 | 1 | Type A | 2.04 mo | 5 | none |
| Liu et al. [9] | 2020 | 1 | Type B | n.d. | 36 | 1 |
| Conforti et al. [19] | 2021 | 5 | Type A: 100% | 2.66 mo (range 1.25–3.91 mo) | 8 (range 7–9) | none |
| Muensterer et al. [15] | 2021 | 3 | Type A: 33.4% Type B: 33.4% Type C: 33.4% | 2.34 mo (range 1.68–3.45 mo) | 10.33 (range 7–12) | none |
| Author | Anastomotic Stricture | Number of Esophageal Dilatations (Mean) | Stent Placement | Surgery | Native Esophagus | Follow-Up (Years (y), Months (mo)) | Historic Group (HG)/Novel Group (NG) |
|---|---|---|---|---|---|---|---|
| Zaritky et al. [18] | 4/5 | n.d. | n.d. | 1/5 | 5/5 | n.d. | overlapping patients |
| Zaritky et al. [7] | 8/9 | n.d. | 2/9 | 1/9 | 9/9 | 9.3 y (range: 0.75–17.75) | overlapping patients |
| Slater et al. [8] | 13/13 | 9.8 (range 3–22) | 6/13 | 2/13 | 13/13 | n.d. | HG |
| Wolfe et al. [12] | 1/1 | 13.5 (+/−2.1 SD) | n.d. | n.d. | 1/1 | 11.38 mo (range 14.75–8) | HG |
| Lovvorn et al. [13] | 2/2 | 3.5 (range 3–4) | none | none | 2/2 | n.d. | HG |
| Dorman et al. [11] | 1/1 | serial dilatation every 2 weeks | n.d. | n.d. | 1/1 | 15 mo | HG |
| Ellebaek et al. [10] | 1/1 | 17 | none | none | 1/1 | 15 mo | HG |
| Liu et al. [9] | 0/1 | none | none | none | 1/1 | 18 mo | HG |
| Conforti et al. [19] | 4/5 * | 4 (range 3–6) | n.d. | n.d. | 5/5 | short term | short follow up |
| Muensterer et al. [15] | 3/3 | 4.33 (range 4–5) | none | none | 3/3 | 15.67 mo (range 14–18) | NG |
| Historic Group n = 19 | Novel Device Group n = 4 | p-Value | |
|---|---|---|---|
| Type of esophageal atresia | |||
| Type A | 15 (78.9%) | 2 (50%) | |
| Type B | 2 (10.5%) | 1 (25%) | 0.488 |
| Type C | 2 (10.5%) | 1 (25%) | |
| Interventions before magnetic compression anastomosis | |||
| Gastrostomy | 18 (94.7%) | 4 (100%) | 0.639 |
| Fistula ligation | 3 (15.8%) | 2 (50%) | 0.132 |
| Approximation | 4 (21.1%) | 4 (100%) | 0.003 |
| Age at intervention, months (mean +/− SD) | 4.63 +/− 1.71 | 2.4 +/− 0.8 | 0.009 |
| Time to patency, days (mean +/− SD) | 8.37 +/− 7.40 | 9.50 +/− 2.89 | 0.186 |
| Complications | |||
| Leakage | 1 (5.3%) | 0 | 0.639 |
| Stenosis | 18 (94.7%) | 4 (100%) | 0.639 |
| Number of dilatations (mean +/− SD) | 9.50 +/− 6.41 | 4.25 +/− 0.50 | 0.051 |
| Stent placement | 6 (35.3%) | 0 | 0.160 |
| Surgery | 2 (10.5%) | 0 | 0.497 |
| Maintenance of native esophagus | 19 (100%) | 4 (100%) | |
| Duration of follow up, years (mean +/− SD) | 6.89 +/− 6.24 | 1.16 +/− 0.33 | 0.066 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holler, A.-S.; König, T.T.; Chen, C.; Harrison, M.R.; Muensterer, O.J. Esophageal Magnetic Compression Anastomosis in Esophageal Atresia Repair: A PRISMA-Compliant Systematic Review and Comparison with a Novel Approach. Children 2022, 9, 1113. https://doi.org/10.3390/children9081113
Holler A-S, König TT, Chen C, Harrison MR, Muensterer OJ. Esophageal Magnetic Compression Anastomosis in Esophageal Atresia Repair: A PRISMA-Compliant Systematic Review and Comparison with a Novel Approach. Children. 2022; 9(8):1113. https://doi.org/10.3390/children9081113
Chicago/Turabian StyleHoller, Anne-Sophie, Tatjana Tamara König, Caressa Chen, Michael R. Harrison, and Oliver J. Muensterer. 2022. "Esophageal Magnetic Compression Anastomosis in Esophageal Atresia Repair: A PRISMA-Compliant Systematic Review and Comparison with a Novel Approach" Children 9, no. 8: 1113. https://doi.org/10.3390/children9081113