
Visual Function and Neuropsychological Profile in Children with Cerebral Visual Impairment

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
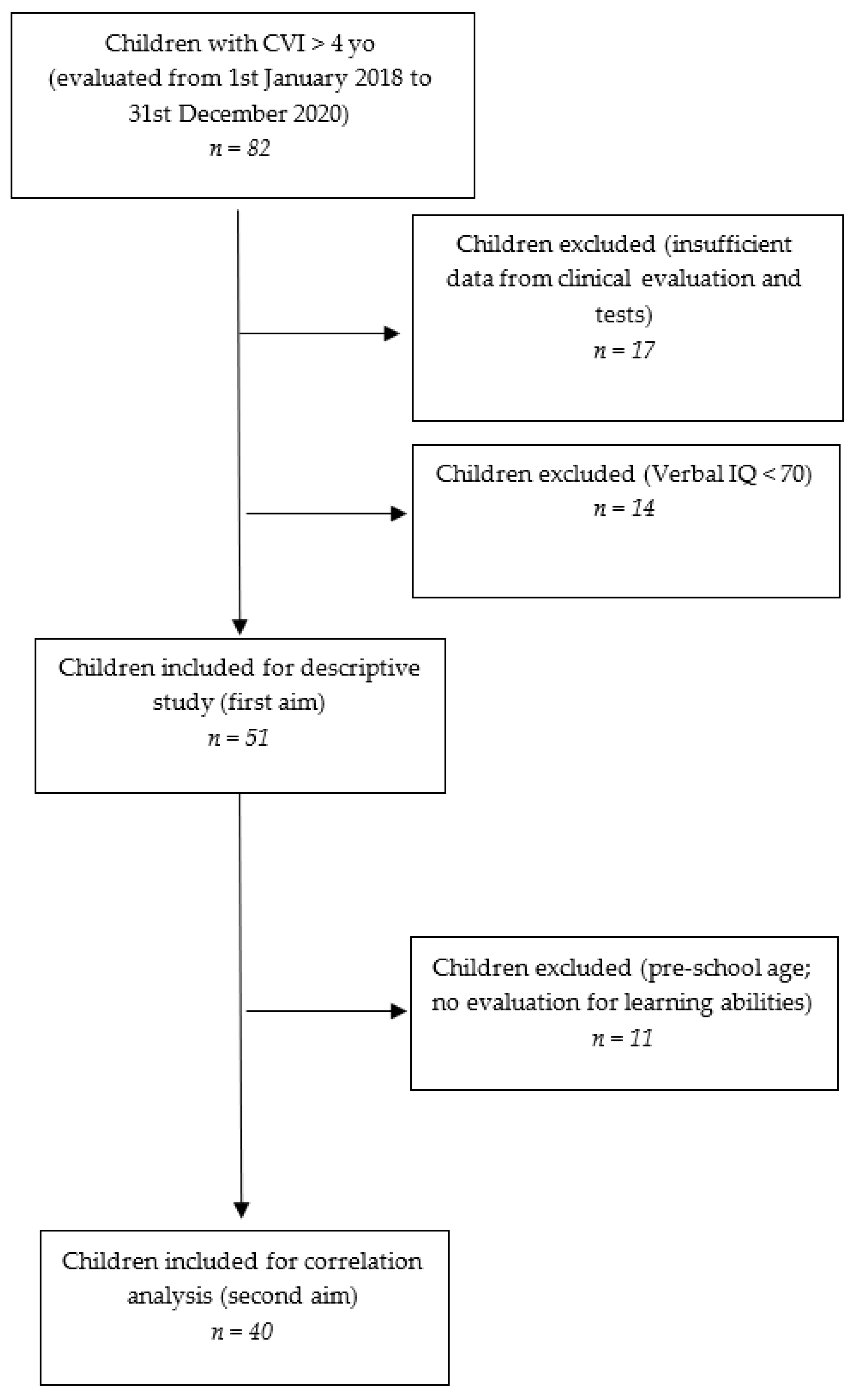
2.1. Patients
2.2. Procedure

{kind=link}
| Parameter | Category | N (%) |
| Sex | Male | 25 (49) |
| Female | 26 (51) | |
| Mean age (months) | 113.07 (range 62–213) ± 35.7 | |
| Gestational age | Term | 4 (8) |
| Late preterm (34–36 weeks) | 15 (29) | |
| Moderate preterm (32–34 weeks) | 3 (6) | |
| Very preterm (28–32 weeks) | 8 (16) | |
| Extremely preterm (<28 weeks) | 17 (33) | |
| Unknown | 4 (8) | |
| GMFCS | Level I | 14 (27) |
| Level II | 18 (35) | |
| Level III | 15 (29) | |
| Level IV | 3 (6) | |
| Level V | 1 (2) | |
| Neuroradiological findings ** | PVL (mild/severe) | 33 (65) |
| Sequelae of IVH or periventricular haemorrhagic Infarction | 5 (10) | |
| Combination of PVL and IVH sequelae | 1 (2) | |
| Basal ganglia/thalamus lesions (mild/moderate/severe) | 1 (2) | |
| Cortico-subcortical lesions only (watershed lesions in parasagittal distribution/multicystic encephalomalacia) not covered under C3 | 1 (2) | |
| Arterial infarctions (middle cerebral artery/other) | 2 (4) | |
| Miscellaneous | 2 (4) | |
| Normal | 1 (2) | |
| Unknown | 5 (10) | |
| Neurological Picture | Unilateral cerebral palsy | 14 (27) * |
| Bilateral cerebral palsy | 30 (59) * | |
| Early CNS injury w/out neuromotor deficit | 7 (14) | |
| Neurologic comorbidity (epileptic abnormalities) | Not reported | 44 (86) |
| Reported | 7 (14) | |
| Psychiatric comorbidity (anxiety, hyperactivity) | Not reported | 43 (84) |
| Reported | 8 (16) | |
| Neurological signs | Diplegia | 21 (41) |
| Hemiplegia | 15 (29) | |
| Tetraplegia | 8 (16) | |
| Motor incoordination | 4 (8) | |
| None | 3 (6) | |
| Motor delay | Unknown | 6 (12) |
| Not reported | 14 (27) | |
| Reported | 31 (61) | |
| Language delay | Unknown | 3 (6) |
| Not reported | 36 (71) | |
| Reported | 12 (24) | |
| Type of therapy | No habilitation | 5 (10) |
| Only physical therapy | 24 (52) | |
| Physical and psychomotor | 7 (15) | |
| Physical and speech therapy | 3 (7) | |
| Physical, psychomotor, and speech therapy | 2 (4) | |
| Psychomotor only | 7 (15) | |
| Speech only | 2 (4) | |
| Psychomotor and speech | 1 (2) |
- Best Corrected Visual Acuity (BCVA). All children in the sample were above 4 years of age (mean age: 113.07 months, SD: ±35.7; age range: 62–213 months), and their visual acuity was assessed using line tests (symbolic or literal optotypes, according to their age), both for near (40 cm) and far (3 m) distances. Recognition acuity was measured with the Snellen chart [33] or LEA vision test [34].
- Contrast Sensitivity (CS): the ability to detect an image’s photometric contrast and spatial frequency, evaluated with the LEA low contrast symbols test or Hiding Heidi [35], based on the age and level of cooperation of the patient.
- Fixation (F), indicated as the ability to maintain fixation on a target.
- Smooth Pursuit (SP), indicated as the ability to follow the trajectory of a slow-moving object both on a horizontal and vertical arc.
- Saccades (SC), indicated as rapid re-fixation eye movements.
- Extrinsic Ocular Motility (OM) indicated as extraocular movements.
- Cognitive assessment, with the following tests:
- ▪
- The Wechsler Preschool and Primary Scale of Intelligence (WPPSI-III) [36] or Wechsler Intelligence Scale for Children (WISC-IV) [37] were performed according to the age of the child. For the WISC-IV scale, we collected the following scores: (i) Verbal Comprehension Index (VCI); (ii) Perceptual Reasoning Index (PRI); (iii) Working Memory Index (WMI); (iv) Processing Speed Index (PSI); (v) (TIQ). For WPPSI-III scale, we collected the following scores: (i) Verbal Comprehension Index (VCI); (ii) Performance Index (PI); (iii) Processing Speed Index (PSI); (iv) Total Intelligence Quotient (TIQ); (v) General Language Index (GLI). Additionally, we included the weighted scores derived from each subtest.
- Cognitive visual assessment, with the following parameters:
- ▪
- The Developmental Test of Visual-Motor Integration (VMI) [38], performed along with its subtests, i.e., Visual Perception (VMI-V) and Motor Coordination (VMI-M), expressed in terms of percentile scores and categorized into normal (>16°P), frailty (5°–16°P), and deficient (<5°P);
- ▪
- The Developmental Test for Visual Perception (DTVP) [39]: General Visual-Perceptual (DTVP-GVP), Non-Motor Visual-Perceptual (DTVP-NMVP), and Visual-Motor Integration (DTVP-VMI) quotients were collected and categorized as normal (>16°P), frail (5°–16°P) and deficient (<5°P).
- Learning abilities, with the following parameters, categorized as normal or deficient based on the Z-score:
- ▪
- The Battery for Dyslexia and Developmental Dysorthography (DDE-2) [40], which is a commonly used Italian battery for the assessment of dyslexia and dysorthography. Specifically, the battery evaluates the ability to read and write both meaningful (DDE-MF) and non-meaningful (DDE-NMF) words by taking into account speed (VEL) and accuracy (ERR);
- ▪
- The MT-3 test [41], which is a currently used Italian instrument aimed to evaluate comprehension (MT-COMP), reading accuracy (MT-RCOR), and reading speed (MT-RVEL) by proposing tests appropriate to the patient’s level of education.
2.3. Data Analysis and Statistics
- −
- Effect size dz: 1.20;
- −
- α err. prob. = 0.05;
- −
- Power (1-β err. prob.) = 0.95.
3. Results
4. Discussion
4.1. Clinical, Visual Function and Neuropsychological Profiles
4.2. Relation between Visual Functions and Neuropsychological Profile
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sakki, H.E.A.; Dale, N.J.; Sargent, J.; Perez-roche, T.; Bowman, R. Is there consensus in defining childhood cerebral visual impairment? A systematic review of terminology and definitions. Br. J. Ophthalmol. 2018, 102, 424–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fazzi, E.; Signorini, S.G.; Bova, S.M.; La Piana, R.; Ondei, P.; Bertone, C.; Misefari, W.; Bianchi, P.E. Spectrum of Visual Disorders in Children With Cerebral Visual Impairment. J. Child Neurol. 2007, 22, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Bauer, C.M.; Merabet, L.B. Perspectives on Cerebral Visual Impairment. Semin. Pediatr. Neurol. 2019, 31, 1–2. [Google Scholar] [CrossRef]
- Pehere, N.; Chougule, P.; Dutton, G.N. Cerebral visual impairment in children: Causes and associated ophthalmological problems. Indian J. Ophthalmol. 2018, 66, 812–815. [Google Scholar] [CrossRef] [PubMed]
- Salati, R.; Borgatti, R.; Giammari, G.; Jacobson, L. Oculomotor dysfunction in cerebral visual impairment following perinatal hypoxia. Dev. Med. Child Neurol. 2002, 44, 542–550. [Google Scholar] [CrossRef]
- Solebo, A.; Rahi, J. Epidemiology, aetiology and management of visual impairment in children. Arch. Dis. Child. 2013, 99, 375–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, L.S.; Skov, L.J.H. Visual dysfunctions and ocular disorders in children with developmental delay. I. prevalence, diagnoses and aetiology of visual impairment. Acta Ophthalmol. Scand. 2007, 85, 149–156. [Google Scholar] [CrossRef]
- Dutton, G.N.; Jacobson, L. Cerebral visual impairment in children. Semin. Neonatol. 2001, 6, 477–485. [Google Scholar] [CrossRef]
- Edmond, J.C.; Foroozan, R. Cortical visual impairment in children. Curr. Opin. Ophthalmol. 2006, 17, 509–512. [Google Scholar] [CrossRef]
- Gorrie, F.; Goodall, K.; Rush, R.; Ravenscroft, J. Towards population screening for Cerebral Visual Impairment: Validity of the Five Questions and the CVI Questionnaire. PLoS ONE 2019, 14, e0214290. [Google Scholar] [CrossRef]
- Philip, S.S.; Dutton, G.N. Identifying and characterising cerebral visual impairment in children: A review. Clin. Exp. Optom. 2014, 97, 196–208. [Google Scholar] [CrossRef]
- Pagliano, E.; Fedrizzi, E.; Erbetta, A.; Bulgheroni, S.; Solari, A.; Bono, R.; Fazzi, E.; Andreucci, E.; Riva, D. Cognitive Profiles and Visuoperceptual Abilities in Preterm and Term Spastic Diplegic Children With Periventricular Leukomalacia. J. Child Neurol. 2007, 22, 282–288. [Google Scholar] [CrossRef]
- Bosch, D.G.M.; Boonstra, F.N.; De Leeuw, N.; Pfundt, R.; Nillesen, W.M.; de Ligt, J.; Gilissen, C.; Jhangiani, S.N.; Lupski, J.R.; Cremers, F.P.M.; et al. Novel genetic causes for cerebral visual impairment. Eur. J. Hum. Genet. 2015, 24, 660–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortibus, E.; Lagae, L.; Casteels, I.; Demaerel, P.; Stiers, P. Assessment of cerebral visual impairment with the L94 visual perceptual battery: Clinical value and correlation with MRI findings. Dev. Med. Child Neurol. 2009, 51, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Boot, F.; Pel, J.; van der Steen, J.; Evenhuis, H. Cerebral Visual Impairment: Which perceptive visual dysfunctions can be expected in children with brain damage? A systematic review. Res. Dev. Disabil. 2010, 31, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Chokron, S.; Kovarski, K.; Zalla, T.; Dutton, G. The inter-relationships between cerebral visual impairment, autism and intellectual disability. Neurosci. Biobehav. Rev. 2020, 114, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Fazzi, E.; Micheletti, S. Questionnaires as screening tools for children with cerebral visual impairment. Dev. Med. Child Neurol. 2020, 62, 891. [Google Scholar] [CrossRef] [Green Version]
- Ben Itzhak, N.; Vancleef, K.; Franki, I.; Laenen, A.; Wagemans, J.; Ortibus, E. Visuoperceptual profiles of children using the Flemish cerebral visual impairment questionnaire. Dev. Med. Child Neurol. 2019, 62, 969–976. [Google Scholar] [CrossRef]
- Sakki, H.; Bowman, R.; Sargent, J.; Kukadia, R.; Dale, N. Visual function subtyping in children with early-onset cerebral visual impairment. Dev. Med. Child Neurol. 2020, 63, 303–312. [Google Scholar] [CrossRef]
- Lueck, A.H.; Dutton, G.N.; Chokron, S. Profiling Children With Cerebral Visual Impairment Using Multiple Methods of Assessment to Aid in Differential Diagnosis. Semin. Pediatr. Neurol. 2019, 31, 5–14. [Google Scholar] [CrossRef]
- Vancleef, K.; Janssens, E.; Petré, Y.; Wagemans, J.; Ortibus, E. Assessment tool for visual perception deficits in cerebral visual impairment: Reliability and validity. Dev. Med. Child Neurol. 2019, 62, 118–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortibus, E.; Fazzi, E.; Dale, N. Cerebral Visual Impairment and Clinical Assessment: The European Perspective. Semin. Pediatr. Neurol. 2019, 31, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Ortibus, E.L.; De Cock, P.P.; Lagae, L.G. Visual Perception in Preterm Children: What Are We Currently Measuring? Pediatr. Neurol. 2011, 45, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ben Itzhak, N.; Vancleef, K.; Franki, I.; Laenen, A.; Wagemans, J.; Ortibus, E. Quantifying visuoperceptual profiles of children with cerebral visual impairment. Child Neuropsychol. 2021, 27, 995–1023. [Google Scholar] [CrossRef] [PubMed]
- Fazzi, E.; Bova, S.; Giovenzana, A.; Signorini, S.; Uggetti, C.; Bianchi, P. Cognitive visual dysfunctions in preterm children with periventricular leukomalacia. Dev. Med. Child Neurol. 2009, 51, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L.; Ek, U.; Fernell, E.; Flodmark, O.; Broberger, U. Visual impairment in preterm children with periventricular leukomalacia—Visual, cognitive and neuropaediatric characteristics related to cerebral imaging. Dev. Med. Child Neurol. 1996, 38, 724–735. [Google Scholar] [CrossRef]
- Ortibus, E.; Laenen, A.; Verhoeven, J.; De Cock, P.; Casteels, I.; Schoolmeesters, B.; Buyck, A.; Lagae, L. Screening for Cerebral Visual Impairment: Value of a CVI Questionnaire. Neuropediatrics 2011, 42, 138–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geldof, C.J.A.; Van Wassenaer-Leemhuis, A.G.; Dik, M.; Kok, J.H.; Oosterlaan, J. A functional approach to cerebral visual impairments in very preterm/very-low-birth-weight children. Pediatr. Res. 2015, 78, 190–197. [Google Scholar] [CrossRef]
- Geldof, C.J.; Oosterlaan, J.; Vuijk, P.; De Vries, M.J.; Kok, J.H.; Van Wassenaer-Leemhuis, A.G.; Wassenaer-Leemhuis, A.G. Visual sensory and perceptive functioning in 5-year-old very preterm/very-low-birthweight children. Dev. Med. Child Neurol. 2014, 56, 862–868. [Google Scholar] [CrossRef] [Green Version]
- Colenbrander, A. Assessment of functional vision and its rehabilitation. Acta Ophthalmol. 2010, 88, 163–173. [Google Scholar] [CrossRef]
- Himmelmann, K.; Horber, V.; De La Cruz, J.; Horridge, K.; Mejaski-Bosnjak, V.; Hollody, K.; Krägeloh-Mann, I.; the SCPE Working Group. MRI classification system (MRICS) for children with cerebral palsy: Development, reliability, and recommendations. Dev. Med. Child Neurol. 2016, 59, 57–64. [Google Scholar] [CrossRef]
- Fazzi, E.; Bova, S.M.; Uggetti, C.; Signorini, S.G.; Bianchi, P.E.; Maraucci, I.; Zoppello, M.; Lanzi, G. Visual–perceptual impairment in children with periventricular leukomalacia. Brain Dev. 2004, 26, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Azzam, D.; Ronquillo, Y. Snellen Chart; StatPearls: Treasure Island, FL, USA, 2020. [Google Scholar]
- Hyvärinen, L.; Näsänen, R.; Laurinen, P. New Visual Acuity Test for Pre-School Children. Acta Ophthalmol. 2009, 58, 507–511. [Google Scholar] [CrossRef]
- Chen, A.H.; Mohamed, D. New paediatric contrast test: Hiding Heidi low-contrast ‘face’ test. Clin. Exp. Ophthalmol. 2003, 31, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Gordon, B. Test Review: Wechsler, D. The Wechsler Preschool and Primary Scale of Intelligence, (WPPSI-III). San Antonio, TX: The Psychological Corporation. Can. J. Sch. Psychol. 2004, 19, 205–220. [Google Scholar] [CrossRef]
- Vaughn-Blount, K.; Watson, S.T.; Kokol, A.L.; Grizzle, R.; Carney, R.N.; Rich, S.S.; Maricle, D.E. Wechsler Intelligence Scale for Children. In Encyclopedia of Child Behavior and Development, 4th ed.; Springer: Boston, MA, USA, 2011. [Google Scholar] [CrossRef]
- Article, O. Child: Beery-Buktenica Developmental Test of Visual-Motor Integration (Beery-VMI): Lessons from integration performance of preschoolers. Child Care Health Dev. 2015, 41, 213–221. [Google Scholar] [CrossRef]
- Brown, T.; Hockey, S.C. The Validity and Reliability of Developmental Test of Visual Perception—2nd Edition (DTVP-2). Phys. Occup. Ther. Pediatr. 2013, 33, 426–439. [Google Scholar] [CrossRef]
- Sartori, G.; Job, R.; Tressoldi, P.E. Batteria Per La Valutazione Della Dislessia e Della Disortografia Evolutiva; Giunti Psychometrics: Firenze FI, Italy, 1995. [Google Scholar]
- Cornoldi, C.; Carretti, B. Prove MT-3 Clinica La Valutazione Delle Abilità Di Lettura e Comprensione per La Scuola Primaria e Secondaria Di I Grado; Giunti Editore: Milano, MI, Italy, 2016. [Google Scholar]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Baranello, G.; Signorini, S.; Tinelli, F.; Guzzetta, A.; Pagliano, E.; Rossi, A.; Foscan, M.; Tramacere, I.; Romeo, D.M.M.; Ricci, D.; et al. Visual Function Classification System for children with cerebral palsy: Development and validation. Dev. Med. Child Neurol. 2019, 62, 104–110. [Google Scholar] [CrossRef] [Green Version]
- Krägeloh-Mann, I.; Horber, V. The role of magnetic resonance imaging in elucidating the pathogenesis of cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2007, 49, 144–151. [Google Scholar] [CrossRef]
- Chong, C.; Dai, S. Cross-sectional study on childhood cerebral visual impairment in New Zealand. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2014, 18, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.Y.; Borchert, M.S. Advances in the evaluation and management of cortical/cerebral visual impairment in children. Surv. Ophthalmol. 2020, 65, 708–724. [Google Scholar] [CrossRef] [PubMed]
- Khetpal, V.; Donahue, S.P. Cortical visual impairment: Etiology, associated findings, and prognosis in a tertiary care setting. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 2007, 11, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Huurneman, B.; Boonstra, F.N.; Cox, R.F.; Cillessen, A.H.; Van Rens, G. A systematic review on ‘Foveal Crowding’ in visually impaired children and perceptual learning as a method to reduce Crowding. BMC Ophthalmol. 2012, 12, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, D.G.; Boonstra, F.N.; Willemsen, M.A.; Cremers, F.P.; De Vries, B.B. Low vision due to cerebral visual impairment: Differentiating between acquired and genetic causes. BMC Ophthalmol. 2014, 14, 59. [Google Scholar] [CrossRef] [Green Version]
- Bennett, C.R.; Bex, P.J.; Bauer, C.M.; Merabet, L.B. The Assessment of Visual Function and Functional Vision. Semin. Pediatr. Neurol. 2019, 31, 30–40. [Google Scholar] [CrossRef]
- Kran, B.S.; Lawrence, L.; Mayer, D.L.; Heidary, G. Cerebral/Cortical Visual Impairment: A Need to Reassess Current Definitions of Visual Impairment and Blindness. Semin. Pediatr. Neurol. 2019, 31, 25–29. [Google Scholar] [CrossRef]
- Cavascan, N.N.; Salomao, S.R.; Sacai, P.Y.; Pereira, J.M.; Rocha, D.M.; Berezovsky, A. Contributing factors to VEP grating acuity deficit and inter-ocular acuity difference in children with cerebral visual impairment. Doc. Ophthalmol. 2014, 128, 91–99. [Google Scholar] [CrossRef]
- Deramore Denver, B.; Froude, E.; Rosenbaum, P.; Wilkes-Gillan, S.; Imms, C. Measurement of visual ability in children with cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2016, 58, 1016–1029. [Google Scholar] [CrossRef] [Green Version]
- Good, W.V.; Jan, J.E.; Burden, S.K.; Skoczenski, A.; Candy, R. Recent advances in cortical visual impairment. Dev. Med. Child Neurol. 2001, 43, 56–60. [Google Scholar] [CrossRef] [Green Version]
- van Genderen, M.; Dekker, M.; Pilon, F.; Bals, I. Diagnosing Cerebral Visual Impairment in Children with Good Visual Acuity. Strabismus 2012, 20, 78–83. [Google Scholar] [CrossRef]
- Fedrizzi, E.; Anderloni, A.; Bono, R.; Bova, S.; Farinotti, M.; Inverno, M.; Savoiardo, S. Eye-movement disorders and visual-perceptual impairment in diplegia children born preterm: A clinical evaluation. Dev. Med. Child Neurol. 2008, 40, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Tinelli, F.; Guzzetta, A.; Purpura, G.; Pasquariello, R.; Cioni, G.; Fiori, S. Structural brain damage and visual disorders in children with cerebral palsy due to periventricular leukomalacia. NeuroImage Clin. 2020, 28, 102430. [Google Scholar] [CrossRef] [PubMed]
- Fazzi, E.; Signorini, S.G.; La Piana, R.; Bertone, C.; Misefari, W.; Galli, J.; Balottin, U.; Bianchi, P.E. Neuro-ophthalmological disorders in cerebral palsy: Ophthalmological, oculomotor, and visual aspects. Dev. Med. Child Neurol. 2012, 54, 730–736. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, L.; Dutton, G.N. Periventricular Leukomalacia: An Important Cause of Visual and Ocular Motility Dysfunction in Children. Surv. Ophthalmol. 2000, 45, 1–13. [Google Scholar] [CrossRef]
- Dutton, G.N.; Saaed, A.; Fahad, B.; Fraser, R.; McDaid, G.; McDade, J.; Mackintosh, A.; Rane, T.; Spowart, S. Association of binocular lower visual field impairment, impaired simultaneous perception, disordered visually guided motion and inaccurate saccades in children with cerebral visual dysfunction—A retrospective observational study. Eye 2004, 18, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyaci, A.; Akal, A.; Tutoglu, A.; Kandemir, H.; Koca, I.; Boyraz, I.; Celen, E.; Ozkan, U. Relationship among Ocular Diseases, Developmental Levels, and Clinical Characteristics of Children with Diplegic Cerebral Palsy. J. Phys. Ther. Sci. 2014, 26, 1679–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newsham, D.; Knox, P.C.; Cooke, R.W.I. Oculomotor Control in Children Who Were Born Very Prematurely. Investig. Opthalmol. Vis. Sci. 2007, 48, 2595–2601. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, L.; Ygge, J.; Flodmark, O. Oculomotor findings in preterm children with periventricular leukomalacia. Acta Ophthalmol. Scand. 2009, 74, 645. [Google Scholar] [CrossRef]
- Kaul, Y.F.; Rosander, K.; Von Hofsten, C.; Brodd, K.S.; Holmström, G.; Kaul, A.; Böhm, B.; Hellström-Westas, L. Visual tracking in very preterm infants at 4 mo predicts neurodevelopment at 3 y of age. Pediatr. Res. 2016, 80, 35–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huurneman, B.; Cox, R.F.; Vlaskamp, B.N.; Boonstra, F.N. Crowded visual search in children with normal vision and children with visual impairment. Vis. Res. 2014, 96, 65–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franz, A.P.; Bolat, G.U.; Bolat, H.; Matijasevich, A.; Santos, I.S.; Silveira, R.C.; Procianoy, R.S.; Rohde, L.A.; Moreira-Maia, C.R. Attention-Deficit/Hyperactivity Disorder and Very Preterm/Very Low Birth Weight: A Meta-analysis. Pediatrics 2017, 141, e20171645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gori, M. Multisensory Integration and Calibration in Children and Adults with and without Sensory and Motor Disabilities. Multisens. Res. 2015, 28, 71–99. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.; Pease, A.; Warnes, P.; Harrison, S.; Pilon, F.; Hyvarinen, L.; West, S.; Self, J.; Ferris, J.; Goodenough, T.; et al. Cerebral visual impairment-related vision problems in primary school children: A cross-sectional survey. Dev. Med. Child Neurol. 2021, 63, 683–689. [Google Scholar] [CrossRef]
- Merabet, L.B.; Mayer, D.L.; Bauer, C.M.; Wright, D.; Kran, B.S. Disentangling How the Brain is “Wired” in Cortical (Cerebral) Visual Impairment. In Seminars in Pediatric Neurology; Elsevier: Amsterdam, The Netherlands, 2017; Volume 24, pp. 83–91. [Google Scholar]
- Morelli, F.; Aprile, G.; Cappagli, G.; Luparia, A.; Decortes, F.; Gori, M.; Signorini, S. A Multidimensional, Multisensory and Comprehensive Rehabilitation Intervention to Improve Spatial Functioning in the Visually Impaired Child: A Community Case Study. Front. Neurosci. 2020, 14, 768. [Google Scholar] [CrossRef]
- Chokron, S.; Kovarski, K.; Dutton, G.N. Cortical Visual Impairments and Learning Disabilities. Front. Hum. Neurosci. 2021, 15, 713316. [Google Scholar] [CrossRef]
- Van Waelvelde, H.; De Weerdt, W.; De Cock, P.; Smits-Engelsman, B.C.M. Association between visual perceptual deficits and motor deficits in children with developmental coordination disorder. Dev. Med. Child Neurol. 2004, 46, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Fazzi, E.; Micheletti, S.; Calza, S.; Merabet, L.; Rossi, A.; Galli, J.; Accorsi, P.; Alessandrini, A.; Bertoletti, A.; Campostrini, E.; et al. Early visual training and environmental adaptation for infants with visual impairment. Dev. Med. Child Neurol. 2021, 63, 1180–1193. [Google Scholar] [CrossRef] [PubMed]

| Parameter | Category | N (%) |
|---|---|---|
| Near visual acuity | Normal (>7/10) | 32 (63) |
| Near-normal (3–7/10) | 12 (32) | |
| Mild low vision (2–3/10) | 2 (4) | |
| Moderate low vision (1–2/10) | 1 (2) | |
| Severe low vision (0.05–1/10) | 0 (0) | |
| Partial blindness (<0.05/10) | 0 (0) | |
| Blindness | 0 (0) | |
| Missing data | 4 (8) | |
| Far visual acuity | Normal (>7/10) | 29 (57) |
| Near-normal (3–7/10) | 12 (33) | |
| Mild low vision (2–3/10) | 3 (6) | |
| Moderate low vision (1–2/10) | 2 (4) | |
| Severe low vision (0.05–1/10) | 0 (0) | |
| Partial blindness (<0.05/10) | 0 (0) | |
| Blindness | 0 (0) | |
| Missing data | 5 (10) | |
| Contrast sensitivity | Normal | 33 (65) |
| Altered | 15 (29) | |
| Missing data | 3 (6) | |
| Fixation | Normal (stable, durable, binocular) | 23 (45) |
| Mildly altered (durable, but alternating or slight difference between the two eyes) | 21 (41) | |
| Slightly instable and/or discontinuous | 6 (12) | |
| Instable and/or discontinuous | 0 (0) | |
| Fluctuating/eccentric | 0 (0) | |
| Occasionally erratic | 0 (0) | |
| Absent response | 0 (0) | |
| Missing data | 1 (2) | |
| Smooth Pursuit | Durable, complete, and binocular | 0 (0) |
| Durable but incomplete/asymmetric/non binocular | 6 (12) | |
| Slightly discontinuous in all or great parts of directions | 19 (37) | |
| Clearly discontinuous/augmented latency | 22 (43) | |
| Inconstant/eccentric/fragmented | 3 (6) | |
| Only for small angle | 0 (0) | |
| Absent/no response | 0 (0) | |
| Missing information | 1 (2) | |
| Saccades | Fluid, complete, normal latency, conjugacy and precision, no evident hypo- or hypermetria | 0 (0) |
| Fluid but incomplete and/or asymmetric and/or not binocular | 4 (8) | |
| Slight alteration (metria, fluidity, latency) | 15 (29) | |
| Moderate alteration (metria, fluidity, latency) | 27 (53) | |
| Severe alteration/difficult to elicit (metria, fluidity, latency) | 4 (8) | |
| Absent/no response | 0 (0) | |
| Missing information | 1 (2) | |
| Extrinsic ocular motility | Normal | 24 (47) |
| Hyperfunction/limitation | 19 (37) | |
| Paralytic limitation | 6 (12) | |
| Missing data | 2 (4) |
| Cognitive Assessment | N (%) | |
|---|---|---|
| WPPSI-III | VCI | 9 (90) |
| PI | 9 (90) | |
| PSI | 4 (40) | |
| TIQ | 8 (80) | |
| GLI | 3 (30) | |
| WISC-IV | VCI | 36 (87) |
| PRI | 32 (78) | |
| WMI | 37 (90) | |
| PSI | 35 (85) | |
| TIQ | 29 (71) | |
| Visuo-Cognitive Assessment | Category | N | |
|---|---|---|---|
| VMI 1 | VMI a | normal (>16°p) | 18 |
| frailty (5°–16°p) | 4 | ||
| deficit (<5°p) | 20 | ||
| total | 42 | ||
| VMI-V b | normal (>16°p) | 20 | |
| frailty (5°–16°p) | 10 | ||
| deficit (<5°p) | 11 | ||
| total | 41 | ||
| VMI-M c | normal (>16°p) | 10 | |
| frailty (5°–16°p) | 9 | ||
| deficit (<5°p) | 21 | ||
| total | 40 | ||
| DTVP 2 | DTVP-GVP a | normal (>16°p) | 14 |
| frailty (5–16°p) | 6 | ||
| deficit (<5°p) | 14 | ||
| total | 34 | ||
| DTVP-NMVP b | normal (>16°p) | 15 | |
| frailty (5°–16°p) | 14 | ||
| deficit (<5°p) | 12 | ||
| total | 41 | ||
| DTVP-VMI c | normal (>16°p) | 8 | |
| frailty (5°–16°p) | 13 | ||
| deficit (<5°p) | 13 | ||
| total | 34 | ||
| Leaning Abilities Assessment | Category | N | ||
|---|---|---|---|---|
| DDE-2 1 | MF a | VEL | normal | 18 |
| deficit | 14 | |||
| total | 32 | |||
| ERR | normal | 26 | ||
| deficit | 5 | |||
| total | 31 | |||
| NMF b | VEL | normal | 12 | |
| deficit | 14 | |||
| total | 26 | |||
| ERR | normal | 22 | ||
| deficit | 6 | |||
| total | 28 | |||
| MT-3 2 | COMP a | normal | 22 | |
| deficit | 13 | |||
| total | 35 | |||
| RCOR b | normal | 21 | ||
| deficit | 5 | |||
| total | 26 | |||
| RVEL c | normal | 16 | ||
| deficit | 12 | |||
| total | 28 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morelli, F.; Aprile, G.; Martolini, C.; Ballante, E.; Olivier, L.; Ercolino, E.; Perotto, E.; Signorini, S. Visual Function and Neuropsychological Profile in Children with Cerebral Visual Impairment. Children 2022, 9, 921. https://doi.org/10.3390/children9060921
Morelli F, Aprile G, Martolini C, Ballante E, Olivier L, Ercolino E, Perotto E, Signorini S. Visual Function and Neuropsychological Profile in Children with Cerebral Visual Impairment. Children. 2022; 9(6):921. https://doi.org/10.3390/children9060921
Chicago/Turabian StyleMorelli, Federica, Giorgia Aprile, Chiara Martolini, Elena Ballante, Lucrezia Olivier, Elisa Ercolino, Eleonora Perotto, and Sabrina Signorini. 2022. "Visual Function and Neuropsychological Profile in Children with Cerebral Visual Impairment" Children 9, no. 6: 921. https://doi.org/10.3390/children9060921