
Atomoxetine Treatment of Attention Deficit/Hyperactivity Disorder Symptoms in 3–6-Year-Old Children with Autism Spectrum Disorder: A Retrospective Cohort Study


{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Participants
2.3. Ethics Approval
2.4. Treatment
2.5. Study Outcomes and Analysis
3. Results
3.1. Patient Disposition, Baseline Demographics, and Clinical Characteristics
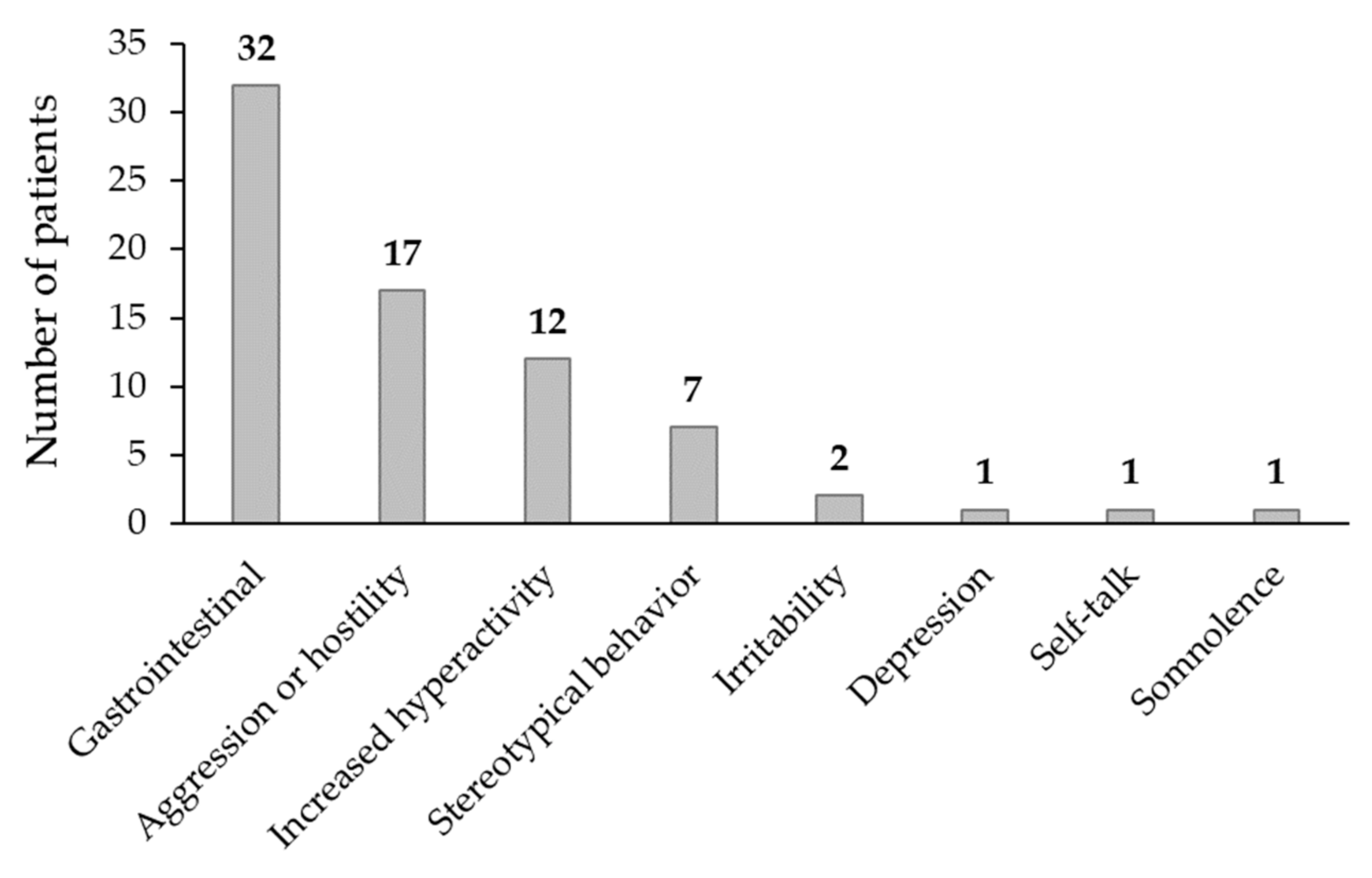
3.2. Safety Outcomes
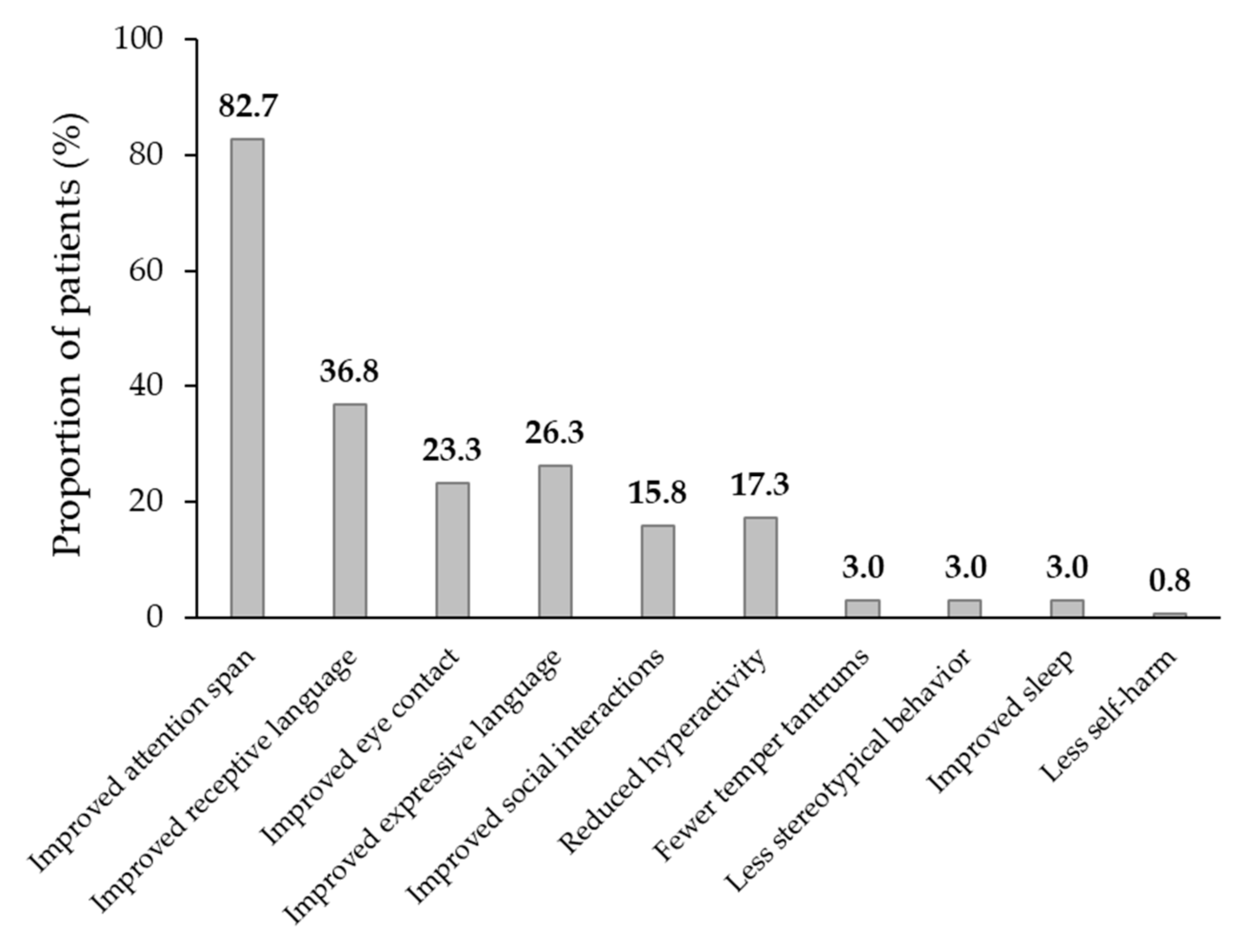
3.3. Effectiveness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schachar, R.J.; Dupuis, A.; Arnold, P.D.; Anagnostou, E.; Kelley, E.; Georgiades, S.; Nicolson, R.; Townes, P.; Burton, C.L.; Crosbie, J. Autism spectrum disorder and attention-deficit/hyperactivity disorder: Shared or unique neurocognitive profiles? Res. Child Adolesc. Psychopathol. 2023, 51, 17–31. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, M.L.; Hagan, J.F., Jr.; Allan, C.; Chan, E.; Davison, D.; Earls, M.; Evans, S.W.; Flinn, S.K.; Froehlich, T.; Frost, J.; et al. Subcommittee on Children and Adolescents with Attention-Deficit/Hyperactive Disorder. Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 2019, 144, e20192528. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Varrasi, S.; Boccaccio, F.M.; Guerrera, C.S.; Platania, G.A.; Pirrone, C.; Castellano, S. Schooling and occupational outcomes in adults with ADHD: Predictors of success and support strategies for effective learning. Educ. Sci. 2023, 13, 37. [Google Scholar] [CrossRef]
- GBD 2019 Mental Disorders Collaborators. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry 2022, 9, 137–150. [Google Scholar] [CrossRef]
- Miodovnik, A.; Harstad, E.; Sideridis, G.; Huntington, N. Timing of the diagnosis of attention-deficit/hyperactivity disorder and autism spectrum disorder. Pediatrics 2015, 136, e830–e837. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Geier, D.A.; Sykes, L.K.; Geier, M.R.; Deth, R.C. Are ASD and ADHD a continuum? A comparison of pathophysiological similarities between the disorders. J. Atten. Disord. 2015, 19, 805–827. [Google Scholar] [CrossRef] [PubMed]
- Kern, J.K.; Geier, D.A.; King, P.G.; Sykes, L.K.; Mehta, J.A.; Geier, M.R. Shared brain connectivity issues, symptoms, and comorbidities in autism spectrum disorder, attention deficit/hyperactivity disorder, and Tourette syndrome. Brain Connect. 2015, 5, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Hoogman, M.; Van Rooij, D.; Klein, M.; Boedhoe, P.; Ilioska, I.; Li, T.; Patel, Y.; Postema, M.C.; Zhang-James, Y.; Anagnostou, E.; et al. Consortium neuroscience of attention deficit/hyperactivity disorder and autism spectrum disorder: The ENIGMA adventure. Hum. Brain Mapp. 2022, 43, 37–55. [Google Scholar] [CrossRef]
- Eom, T.H.; Kim, Y.H. Clinical practice guidelines for attention-deficit/hyperactivity disorder: Recent updates. Clin. Exp. Pediatr. 2024, 67, 26–34. [Google Scholar] [CrossRef]
- Hyman, S.L.; Levy, S.E.; Myers, S.M.; Council on Children with Disabilities, Section on Developmental and Behavioral Pediatrics. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics 2020, 145, e20193447. [Google Scholar] [CrossRef]
- Egger, H.L.; Angold, A. Common emotional and behavioral disorders in preschool children: Presentation, nosology, and epidemiology. J. Child Psychol. Psychiatry Allied Discipl. 2006, 47, 313–337. [Google Scholar] [CrossRef] [PubMed]
- Sonuga-Barke, E.J.; Koerting, J.; Smith, E.; McCann, D.C.; Thompson, M. Early detection and intervention for attention-deficit/hyperactivity disorder. Expert Rev. Neurother. 2011, 11, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Weyandt, L.L.; Clarkin, C.M.; Holding, E.Z.; May, S.E.; Marraccini, M.E.; Gudmundsdottir, B.G.; Shepard, E.; Thompson, L. Neuroplasticity in children and adolescents in response to treatment intervention: A systematic review of the literature. Clin. Transl. Neurosci. 2020, 4, 21. [Google Scholar] [CrossRef]
- Leffa, D.T.; Caye, A.; Rohde, L.A. ADHD in children and adults: Diagnosis and prognosis. Curr. Top Behav. Neurosci. 2022, 57, 1–18. [Google Scholar]
- Sonuga-Barke, E.J.; Halperin, J.M. Developmental phenotypes and causal pathways in attention deficit/hyperactivity disorder: Potential targets for early intervention? J. Child Psychol. Psychiatry 2010, 51, 368–389. [Google Scholar] [CrossRef]
- Cortese, S.; Kelly, C.; Chabernaud, C.; Proal, E.; Di Martino, A.; Milham, M.P.; Castellanos, F.X. Toward systems neuroscience of ADHD: A meta-analysis of 55 fMRI studies. Am. J. Psychiatry 2012, 169, 1038–1055. [Google Scholar] [CrossRef]
- Mahajan, R.; Bernal, M.P.; Panzer, R.; Whitaker, A.; Roberts, W.; Handen, B.; Hardan, A.; Anagnostou, E.; Veenstra-VanderWeele, J.; Autism Speaks Autism Treatment Network Psychopharmacology Committee. Clinical practice pathways for evaluation and medication choice for attention-deficit/hyperactivity disorder symptoms in autism spectrum disorders. Pediatrics 2012, 130 (Suppl. 2), S125–S138. [Google Scholar] [CrossRef]
- Galvez-Contreras, A.Y.; Vargas-de la Cruz, I.; Beltran-Navarro, B.; Gonzalez-Castaneda, R.E.; Gonzalez-Perez, O. Therapeutic approaches for ADHD by developmental stage and clinical presentation. Int. J. Environ. Res. Public Health 2022, 19, 12880. [Google Scholar] [CrossRef]
- Newcorn, J.H.; Krone, B.; Dittmann, R.W. Nonstimulant treatments for ADHD. Child Adolesc. Psychiatr. Clin. N Am. 2022, 31, 417–435. [Google Scholar] [CrossRef]
- Eli Lilly and Company. Strattera® (Atomoxetine Hydrochloride)—Prescribing Information. 2020. Available online: http://pi.lilly.com/us/strattera-pi.pdf (accessed on 9 October 2023).
- Busner, J.; Targum, S.D. The Clinical Global Impressions Scale: Applying a research tool in clinical practice. Psychiatry (Edgmont) 2007, 4, 28–37. [Google Scholar] [PubMed]
- Dawkins, T.; Meyer, A.T.; Van Bourgondien, M.E. The relationship between the Childhood Autism Rating Scale: Second Edition and clinical diagnosis utilizing the DSM-IV-TR and the DSM-5. J. Autism Dev. Disord. 2016, 46, 3361–3368. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, M.L.; Lambert, W.; Doffing, M.A.; Bickman, L.; Simmons, T.; Worley, K. Psychometric properties of the Vanderbilt ADHD diagnostic parent rating scale in a referred population. J. Pediatr. Psychol. 2003, 28, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Nachshen, J.; Garcin, N.; Moxness, K.; Tremblay, Y.; Hutchinson, P.; Lachance, A.; Beaurivage, M.; Breitenbach, M.; Bryson, S.; Burack, J.; et al. Screening, Assessment, and Diagnosis of Autism Spectrum Disorders in Young Children: Canadian Best Practice Guidelines; Miriam Foundation: Montreal, QC, Canada, 2008; Available online: https://www.researchgate.net/publication/274960728_Screening_Assessment_and_Diagnosis_of_Autism_Spectrum_Disorders_in_Young_Children_Canadian_Best_Practice_Guidelines (accessed on 20 January 2024).
- Yilmaz, S.; Serdaroglu, G.; Akcay, A.; Gokben, S. Clinical characteristics and outcome of children with electrical status epilepticus during slow wave sleep. J. Pediatr. Neurosci. 2014, 9, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Hergüner, M.O.; Incecik, F.; Altunbaşak, S.; Kiriş, N. Clinical characteristics of 10 patients with continuous spikes and waves during slow sleep syndrome. Pediatr. Neurol. 2008, 38, 411–414. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Holtmann, M.; Banaschewski, T.; Buitelaar, J.; Coghill, D.; Danckaerts, M.; Dittmann, R.W.; Graham, J.; Taylor, E.; Sergeant, J.; et al. Practitioner review: Current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents. J. Child Psychol. Psychiatry 2013, 54, 227–246. [Google Scholar] [CrossRef] [PubMed]
- Kratochvil, C.J.; Vaughan, B.S.; Mayfield-Jorgensen, M.L.; March, J.S.; Kollins, S.H.; Murray, D.W.; Ravi, H.; Greenhill, L.L.; Kotler, L.A.; Paykina, N.; et al. A pilot study of atomoxetine in young children with attention-deficit/hyperactivity disorder. J. Child Adolesc. Psychopharmacol. 2007, 17, 175–185. [Google Scholar] [CrossRef]
- Ghuman, J.K.; Aman, M.G.; Ghuman, H.S.; Reichenbacher, T.; Gelenberg, A.; Wright, R.; Rice, S.; Fort, C. Prospective, naturalistic, pilot study of open-label atomoxetine treatment in preschool children with attention-deficit/hyperactivity disorder. J. Child Adolesc. Psychopharmacol. 2009, 19, 155–166. [Google Scholar] [CrossRef]
- Kratochvil, C.J.; Vaughan, B.S.; Stoner, J.A.; Daughton, J.M.; Lubberstedt, B.D.; Murray, D.W.; Chrisman, A.K.; Faircloth, M.A.; Itchon-Ramos, N.B.; Kollins, S.H.; et al. A double-blind, placebo-controlled study of atomoxetine in young children with ADHD. Pediatrics 2011, 127, e862–e868. [Google Scholar] [CrossRef]
- Handen, B.L.; Aman, M.G.; Arnold, L.E.; Hyman, S.L.; Tumuluru, R.V.; Lecavalier, L.; Corbett-Dick, P.; Pan, X.; Hollway, J.A.; Buchan-Page, K.A.; et al. Atomoxetine, parent training, and their combination in children with autism spectrum disorder and attention-deficit/hyperactivity disorder. J. Am. Acad Child Adolesc. Psychiatry 2015, 54, 905–915. [Google Scholar] [CrossRef]
- Harfterkamp, M.; Buitelaar, J.K.; Minderaa, R.B.; van de Loo-Neus, G.; van der Gaag, R.J.; Hoekstra, P.J. Long-term treatment with atomoxetine for attention-deficit/hyperactivity disorder symptoms in children and adolescents with autism spectrum disorder: An open-label extension study. J. Child Adolesc. Psychopharmacol. 2013, 23, 194–199. [Google Scholar] [CrossRef]
- Savill, N.C.; Buitelaar, J.K.; Anand, E.; Day, K.A.; Treuer, T.; Upadhyaya, H.P.; Coghill, D. The efficacy of atomoxetine for the treatment of children and adolescents with attention-deficit/hyperactivity disorder: A comprehensive review of over a decade of clinical research. CNS Drugs 2015, 29, 131–151. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.; Wu, D.D.; Guo, H.L.; Hu, Y.H.; Xia, Y.; Ji, X.; Fang, W.R.; Li, Y.M.; Xu, J.; Chen, F.; et al. The mechanism, clinical efficacy, safety, and dosage regimen of atomoxetine for ADHD therapy in children: A narrative review. Front. Psychiatry 2022, 12, 780921. [Google Scholar] [CrossRef] [PubMed]
- Bangs, M.E.; Tauscher-Wisniewski, S.; Polzer, J.; Zhang, S.; Acharya, N.; Desaiah, D.; Allen, A.J. Meta-analysis of suicide-related events in atomoxetine-treated patients. In Proceedings of the 52nd Annual Meeting of the American Academy of Child and Adolescent Psychiatry, Toronto, ON, Canada, 18–23 October 2005. [Google Scholar]
- Davies, M.; Coughtrie, A.; Layton, D.; Shakir, S.A. Use of atomoxetine and suicidal ideation in children and adolescents: Results of an observational cohort study within general practice in England. Eur. Psychiatry 2017, 39, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Fu, D.; Guo, H.L.; Hu, Y.H.; Fang, W.R.; Liu, Q.Q.; Xu, J.; Wu, D.D.; Chen, F. Personalizing atomoxetine dosing in children with ADHD: What can we learn from current supporting evidence. Eur. J. Clin. Pharmacol. 2023, 79, 349–370. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alsayouf, H.A.; Alsarhan, O.; Khreisat, W.; Daoud, A. Atomoxetine Treatment of Attention Deficit/Hyperactivity Disorder Symptoms in 3–6-Year-Old Children with Autism Spectrum Disorder: A Retrospective Cohort Study. Children 2024, 11, 163. https://doi.org/10.3390/children11020163
Alsayouf HA, Alsarhan O, Khreisat W, Daoud A. Atomoxetine Treatment of Attention Deficit/Hyperactivity Disorder Symptoms in 3–6-Year-Old Children with Autism Spectrum Disorder: A Retrospective Cohort Study. Children. 2024; 11(2):163. https://doi.org/10.3390/children11020163
Chicago/Turabian StyleAlsayouf, Hamza A., Osama Alsarhan, Wael Khreisat, and Azhar Daoud. 2024. "Atomoxetine Treatment of Attention Deficit/Hyperactivity Disorder Symptoms in 3–6-Year-Old Children with Autism Spectrum Disorder: A Retrospective Cohort Study" Children 11, no. 2: 163. https://doi.org/10.3390/children11020163