
Patient-Specific Surgical Correction of Adolescent Idiopathic Scoliosis: A Systematic Review

 ,
,
Abstract
:1. Introduction
- -
- TK planning method;
- -
- Manufacturing: various ways to obtain PSR;
- -
- Comparison between programmed and achieved TK;
- -
- PJK incidence.
2. Materials and Methods
3. Results
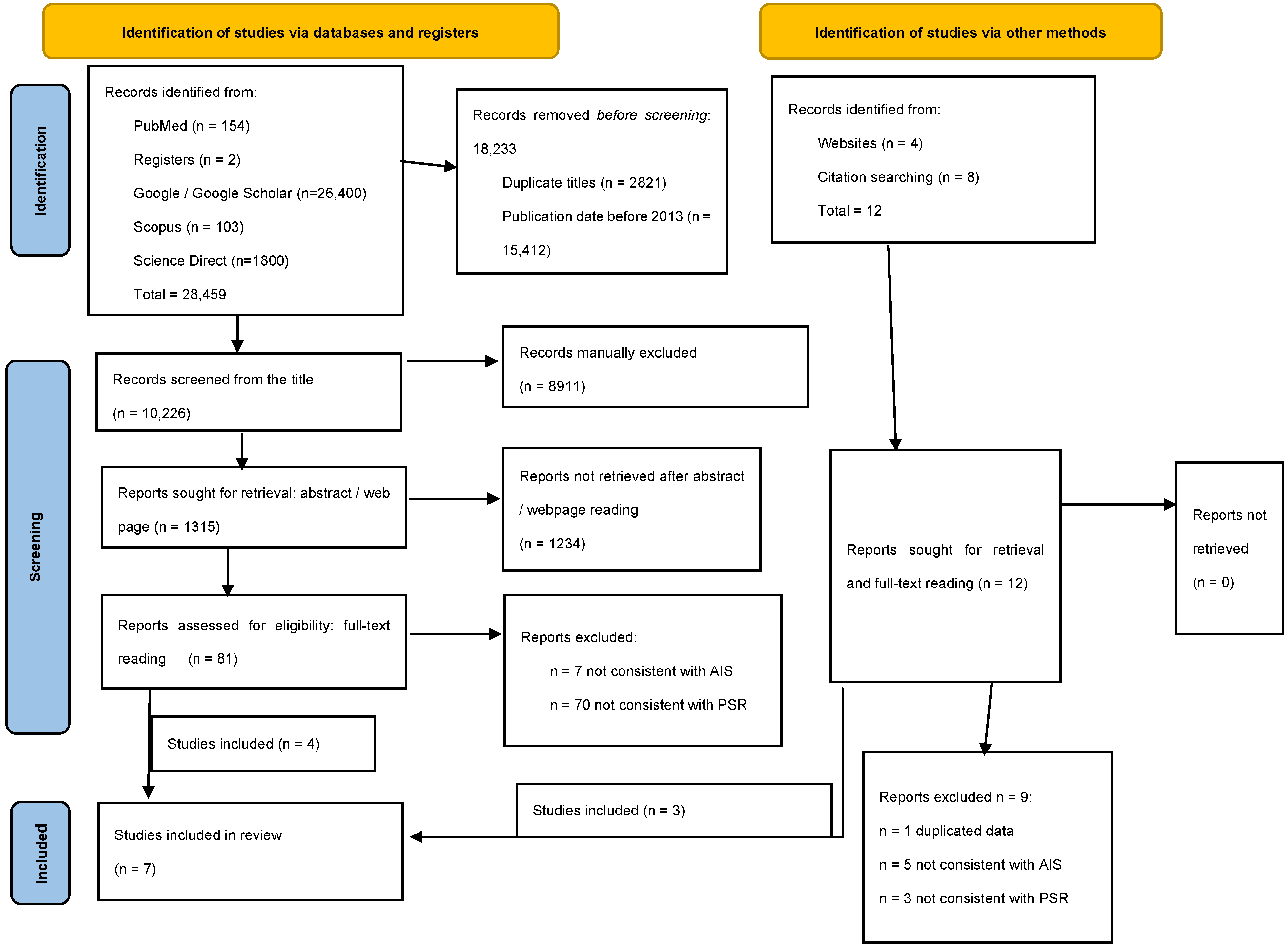
3.1. Literature Search Results
3.2. Radiological Planning and Analysis
3.3. How to Obtain PSR
3.4. Radiological Outcomes
4. Discussion
5. Limitations
6. Future Directions
- -
- How the properties of the rod (diameter, section, material, notched vs. not notched), surgical factors (type and density of implants, type of rod–screw connection, correction and release technique), and baseline variates (spine stiffness, pre-operative TK, patient-related factors, etc.) might influence the relationship between the plan and the achieved alignment;
- -
- If the achieved plan, including the regularity of TK, the position of the apex, and the transition points between TK and adjacent curves, was optimal concerning the postoperative modifications to global alignment, adjacent sagittal curves, and quality of life. For this, TK planning requires a clear definition of the measurement limits, apex, and the number of vertebrae included.
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mak, T.; Cheung, P.W.H.; Zhang, T.; Cheung, J.P.Y. Patterns of coronal and sagittal deformities in adolescent idiopathic scoliosis. BMC Musculoskelet. Disord. 2021, 22, 44. [Google Scholar] [CrossRef]
- Gardner, A.; Berryman, F.; Pynsent, P. The kyphosis–lordosis difference parameter and its utility in understanding the pathogenesis of adolescent idiopathic scoliosis. BMC Res. Notes 2022, 15, 178. [Google Scholar] [CrossRef] [PubMed]
- Post, M.; Verdun, S.; Roussouly, P.; Abelin-Genevois, K. New sagittal classification of AIS: Validation by 3D characterization. Eur. Spine J. 2019, 28, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Fruergaard, S.; Jain, M.J.; Deveza, L.; Liu, D.; Heydemann, J.; Ohrt-Nissen, S.; Dragsted, C.; Gehrchen, M.; Dahl, B.; Texas Children’s Hospital Spine Study Group. Evaluation of a new sagittal classification system in adolescent idiopathic scoliosis. Eur. Spine J. 2020, 29, 744–753. [Google Scholar] [CrossRef] [PubMed]
- Ritzman, T.F.; Floccari, L.V. The Sagittal Plane in Spinal Fusion for Adolescent Idiopathic Scoliosis. J. Am. Acad. Orthop. Surg. 2022, 30, e957–e967. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.M.; Wang, Y.; Yu, J.; Jin, F.; Zhang, Y.; Zhao, Y.; Fu, Y.; Zhang, K.; Wang, J.; Dai, L.; et al. Analysis of sagittal curvature and its influencing factors in adolescent idiopathic scoliosis. Medicine 2021, 100, e26274. [Google Scholar] [CrossRef]
- Iimura, T.; Ueda, H.; Inami, S.; Moridaira, H.; Takeuchi, D.; Aoki, H.; Taneichi, H. Thoracic kyphosis in light of lumbosacral alignment in thoracic adolescent idiopathic scoliosis: Recognition of thoracic hypokyphosis and therapeutic implications. BMC Musculoskelet. Disord. 2022, 23, 414. [Google Scholar] [CrossRef]
- Pesenti, S.; Clément, J.-L.; Ilharreborde, B.; Morin, C.; Charles, Y.P.; Parent, H.F.; Violas, P.; Szadkowski, M.; Boissière, L.; Jouve, J.-L.; et al. Comparison of four correction techniques for posterior spinal fusion in adolescent idiopathic scoliosis. Eur. Spine J. 2022, 31, 1028–1035. [Google Scholar] [CrossRef]
- Boeckenfoerde, K.; Boevingloh, A.S.; Gosheger, G.; Bockholt, S.; Lampe, L.P.; Lange, T. Risk Factors of Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis—The Spinous Processes and Proximal Rod Contouring. J. Clin. Med. 2022, 11, 6098. [Google Scholar] [CrossRef]
- Pasha, S.; Ilharreborde, B.; Baldwin, K. Sagittal Spinopelvic Alignment After Posterior Spinal Fusion in Adolescent Idiopathic Scoliosis: A Systematic Review and Meta-analysis. Spine 2019, 44, 41–52. [Google Scholar] [CrossRef]
- Bodendorfer, B.M.; Shah, S.A.; Bastrom, T.P.; Lonner, B.S.; Yaszay, B.; Samdani, A.F.; Miyanji, F.; Cahill, P.J.; Sponseller, P.D.; Betz, R.R.; et al. Restoration of Thoracic Kyphosis in Adolescent Idiopathic Scoliosis Over a Twenty-year Period: Are We Getting Better? Spine 2020, 45, 1625–1633. [Google Scholar] [CrossRef] [PubMed]
- Garg, B.; Mehta, N.; Gupta, A.; Sugumar, P.A.A.; Shetty, A.P.; Basu, S.; Jakkepally, S.; Gowda, S.D.; Babu, J.N.; Chhabra, H.S. Cervical sagittal alignment in Lenke 1 adolescent idiopathic scoliosis and assessment of its alteration with surgery: A retrospective, multi-centric study. Spine Deform. 2021, 9, 1559–1568. [Google Scholar] [CrossRef]
- Alzakri, A.; Vergari, C.; Van den Abbeele, M.; Gille, O.; Skalli, W.; Obeid, I. Global Sagittal Alignment and Proximal Junctional Kyphosis in Adolescent Idiopathic Scoliosis. Spine Deform. 2019, 7, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.B.; Skaggs, D.L.M.; Andras, L.M.; Tolo, V.; Tamrazi, B.; Illingworth, K.D. Increasing Cervical Kyphosis Correlates With Cervical Degenerative Disc Disease in Patients With Adolescent Idiopathic Scoliosis. Spine 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Young, E.; Regan, C.; Currier, B.L.; Yaszemski, M.J.; Larson, A.N. At Mean 30-Year Follow-Up, Cervical Spine Disease Is Common and Associated with Thoracic Hypokyphosis after Pediatric Treatment of Adolescent Idiopathic Scoliosis. J. Clin. Med. 2022, 11, 6064. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, P.; Hentschel, S.; Platzek, I.; Hühne, S.; Ettrich, U.; Hartmann, A.; Seifert, J. Thoracal flat back is a risk factor for lumbar disc degeneration after scoliosis surgery. Spine J. 2014, 14, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Lenke, L.G.; Edwards, C.C.I.; Bridwell, K.H. The lenke classification of adolescent idiopathic scoliosis: How it organizes curve patterns as a template to perform selective fusions of the spine. Spine 2003, 28, S199–S207. [Google Scholar] [CrossRef]
- Sullivan, T.B.; Bastrom, T.P.; Bartley, C.E.; Dolan, L.A.; Weinstein, S.L.; Newton, P.O. More severe thoracic idiopathic scoliosis is associated with a greater three-dimensional loss of thoracic kyphosis. Spine Deform. 2020, 8, 1205–1211. [Google Scholar] [CrossRef]
- Schlösser, T.P.; Abelin-Genevois, K.; Homans, J.; Pasha, S.; Kruyt, M.; Roussouly, P.; Shah, S.A.; Castelein, R.M. Comparison of different strategies on three-dimensional correction of AIS: Which plane will suffer? Eur. Spine J. 2021, 30, 645–652. [Google Scholar] [CrossRef]
- Winter, R.B.; Lonstein, J.E.; Denis, F. Sagittal spinal alignment: The true measurement, norms, and description of correction for thoracic kyphosis. J. Spinal Disord. Tech. 2009, 22, 311–314. [Google Scholar] [CrossRef]
- Zappalá, M.; Lightbourne, S.; Heneghan, N.R. The relationship between thoracic kyphosis and age, and normative values across age groups: A systematic review of healthy adults. J. Orthop. Surg. Res. 2021, 16, 447. [Google Scholar] [CrossRef] [PubMed]
- Laouissat, F.; Sebaaly, A.; Gehrchen, M.; Roussouly, P. Classification of normal sagittal spine alignment: Refounding the Roussouly classification. Eur. Spine J. 2018, 27, 2002–2011. [Google Scholar] [CrossRef]
- Iyer, S.; Lenke, L.G.; Nemani, V.M.; Albert, T.J.; Sides, B.A.; Metz, L.N.; Cunningham, M.E.; Kim, H.J. Variations in Sagittal Alignment Parameters Based on Age: A Prospective Study of Asymptomatic Volunteers Using Full-Body Radiographs. Spine 2016, 41, 1826–1836. [Google Scholar] [CrossRef] [PubMed]
- Clément, J.-L.; Solla, F.; Amorese, V.; Oborocianu, I.; Rosello, O.; Rampal, V. Lumbopelvic parameters can be used to predict thoracic kyphosis in adolescents. Eur. Spine J. 2020, 29, 2281–2286. [Google Scholar] [CrossRef] [PubMed]
- Solla, F.; Ilharreborde, B.; Blondel, B.; Prost, S.; Bauduin, E.; Laouissat, F.; Riouallon, G.; Wolff, S.; Challier, V.; Obeid, I.; et al. Can Lumbopelvic Parameters Be Used to Predict Thoracic Kyphosis at all Ages? A National Cross-Sectional Study. Glob. Spine J. 2022, 21925682221134039. [Google Scholar] [CrossRef] [PubMed]
- Clément, J.-L.; Pesenti, S.; Ilharreborde, B.; Morin, C.; Charles, Y.-P.; Parent, H.-F.; Violas, P.; Szadkowski, M.; Boissière, L.; Solla, F. Proximal junctional kyphosis is a rebalancing spinal phenomenon due to insufficient postoperative thoracic kyphosis after adolescent idiopathic scoliosis surgery. Eur. Spine J. 2021, 30, 1988–1997. [Google Scholar] [CrossRef] [PubMed]
- Hostin, R.A.; Yeramaneni, S.; Gum, J.L.; Smith, J.S. Clinical and Economic Impact of Proximal Junctional Kyphosis on Pediatric and Adult Spinal Deformity Patients. Int. J. Spine Surg. 2023, 17, S9–S17. [Google Scholar] [CrossRef]
- Erkilinc, M.; Baldwin, K.D.; Pasha, S.; Mistovich, R.J. Proximal junctional kyphosis in pediatric spinal deformity surgery: A systematic review and critical analysis. Spine Deform. 2022, 10, 257–266. [Google Scholar] [CrossRef]
- Ferrero, E.; Bocahut, N.; Lefevre, Y.; Roussouly, P.; Pesenti, S.; Lakhal, W.; Odent, T.; Morin, C.; Clement, J.-L.; Compagnon, R.; et al. Proximal junctional kyphosis in thoracic adolescent idiopathic scoliosis: Risk factors and compensatory mechanisms in a multicenter national cohort. Eur. Spine J. 2018, 27, 2241–2250. [Google Scholar] [CrossRef]
- Cerpa, M.; Sardar, Z.; Lenke, L. Revision surgery in proximal junctional kyphosis. Eur. Spine J. 2020, 29, 78–85. [Google Scholar] [CrossRef]
- Barton, C.; Noshchenko, A.; Patel, V.; Kleck, C.; Burger, E. Early Experience and Initial Outcomes with Patient-Specific Spine Rods for Adult Spinal Deformity. Orthopedics 2016, 39, 79–86. [Google Scholar] [CrossRef] [PubMed]
- El Rahal, A.; Solla, F.; Fière, V.; Toquart, A.; Barrey, C.Y. Spine Surgery. Case-Based Approach; Sagittal balance and preoperative planning; Springer Nature: Berlin, Germany, 2019; pp. 447–458. [Google Scholar]
- Branche, K.; Netsanet, R.; Noshchenko, A.; Burger, E.; Patel, V.; Ou-Yang, D.; Kleck, C.J. Radius of Curvature in Patient-Specific Short Rod Constructs Versus Standard Pre-Bent Rods. Int. J. Spine Surg. 2020, 14, 944–948. [Google Scholar] [CrossRef]
- Sardi, J.P.; Ames, C.P.; Coffey, S.; Good, C.; Dahl, B.; Kraemer, P.; Gum, J.; Devito, D.; Brayda-Bruno, M.; Lee, R.; et al. Accuracy of Rod Contouring to Desired Angles with and without a Template: Implications for Achieving Desired Spinal Alignment and Outcomes. Glob. Spine J. 2023, 13, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Solla, F.; Barrey, C.Y.; Burger, E.; Kleck, C.J.; Fière, V. Patient-specific Rods for Surgical Correction of Sagittal Imbalance in Adults: Technical Aspects and Preliminary Results. Clin. Spine Surg. 2019, 32, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Prost, S.; Farah, K.; Pesenti, S.; Tropiano, P.; Fuentes, S.; Blondel, B. “Patient-specific” rods in the management of adult spinal deformity. One-year radiographic results of a prospective study about 86 patients. Neurochirurgie 2020, 66, 162–167. [Google Scholar] [CrossRef]
- Prost, S.; Pesenti, S.; Farah, K.; Tropiano, P.; Fuentes, S.; Blondel, B. Adult Spinal Deformities: Can Patient-Specific Rods Change the Preoperative Planning into Clinical Reality? Feasibility Study and Preliminary Results about 77 Cases. Adv. Orthop. 2020, 2020, 6120580. [Google Scholar] [CrossRef] [PubMed]
- Sadrameli, S.S.; Boghani, Z.; Iii, W.J.S.; Holman, P.J. Utility of Patient-Specific Rod Instrumentation in Deformity Correction: Single Institution Experience. Spine Surg. Relat. Res. 2020, 4, 256–260. [Google Scholar] [CrossRef]
- Alijanipour, P.; Heffernan, M.J.; Baldwin, N.K.; King, A.G. Radiographic comparison of patient-specific (ps) and manually contoured conventional (c) rods in adolescent idiopathic scoliosis (ais) surgery. Eur. Spine J. 2017, 26 (Suppl. S2), S251–S291. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Ferrero, E.; Mazda, K.; Simon, A.-L.; Ilharreborde, B. Preliminary experience with SpineEOS, a new software for 3D planning in AIS surgery. Eur. Spine J. 2018, 27, 2165–2174. [Google Scholar] [CrossRef]
- Marya, S.; Elmalky, M.; Schroeder, A.; Tambe, A. Correction of Thoracic Hypokyphosis in Adolescent Scoliosis Using Patient-Specific Rod Templating. Healthcare 2023, 11, 980. [Google Scholar] [CrossRef] [PubMed]
- Thomas, E.S.; Boyer, N.; Meyers, A.; Aziz, H.; Aminian, A. Restoration of thoracic kyphosis in adolescent idiopathic scoliosis with patient-specific rods: Did the preoperative plan match postoperative sagittal alignment? Eur. Spine J. 2023, 32, 190–201. [Google Scholar] [CrossRef] [PubMed]
- Grobost, P.; Chevillotte, T.; Verdun, S.; Abelin Genevois, K. Tiges sur Mesure pour la Correction Chirurgicale des ais- Application des Principes de la Nouvelle Classification ais Sagittale. In Proceedings of SFCR Congress, Strasbourg. 2019. Available online: https://www.sfcr.fr/uploads/media/default/0001/04/recueil-des-resumes-ok-20190709092413.pdf (accessed on 15 October 2023).
- Solla, F.; Clément, J.-L.; Cunin, V.; Bertoncelli, C.M.; Fière, V.; Rampal, V. Patient-specific rods for thoracic kyphosis correction in adolescent idiopathic scoliosis surgery: Preliminary results. Orthop. Traumatol. Surg. Res. 2020, 106, 159–165. [Google Scholar] [CrossRef]
- Solla, F.; Cunin, V.; Haddad, E.; Laquièvre, A.; Fière, V.; Dohin, B.; Clément, J.L. Analysis of 85 adolescent idiopathic scoliosis patients corrected with patient specific rods with a minimum of 1 year follow-up. Eur. Spine J. 2021, 30, 237–277. [Google Scholar] [CrossRef]
- Marx, R.G.; Wilson, S.M.; Swiontkowski, M.F. Updating the Assignment of Levels of Evidence. J. Bone Jt. Surg. Am. 2015, 97, 1–2. [Google Scholar] [CrossRef]
- Surgimap. Available online: https://www.surgimap.com/ (accessed on 5 December 2023).
- Medtronic Unid Hub. Available online: https://platformous.medicrea.com/Account/ (accessed on 5 December 2023).
- Langlais, T.; Bouy, A.; Eloy, G.; Mainard, N.; Skalli, W.; Vergari, C.; Vialle, R. Sagittal plane assessment of manual concave rod bending for posterior correction in adolescents with idiopathic thoracic scoliosis (Lenke 1 and 3). Orthop. Traumatol. Surg. Res. 2023, 109, 103654. [Google Scholar] [CrossRef]
- Sudo, H.; Tachi, H.; Kokabu, T.; Yamada, K.; Iwata, A.; Endo, T.; Takahata, M.; Abe, Y.; Iwasaki, N. In vivo deformation of anatomically pre-bent rods in thoracic adolescent idiopathic scoliosis. Sci. Rep. 2021, 11, 12622. [Google Scholar] [CrossRef]
- Tachi, H.; Kato, K.; Abe, Y.; Kokabu, T.; Yamada, K.; Iwasaki, N.; Sudo, H. Surgical Outcome Prediction Using a Four-Dimensional Planning Simulation System with Finite Element Analysis Incorporating Pre-bent Rods in Adolescent Idiopathic Scoliosis: Simulation for Spatiotemporal Anatomical Correction Technique. Front. Bioeng. Biotechnol. 2021, 9, 746902. [Google Scholar] [CrossRef]
- Sudo, H. Four-Dimensional Anatomical Spinal Reconstruction in Thoracic Adolescent Idiopathic Scoliosis. JBJS Essent. Surg. Tech. 2022, 12, e21.00038. [Google Scholar] [CrossRef]
- Robert Reid. Available online: https://www.robert-reid.co.jp/english/ (accessed on 21 December 2023).
- Nuvasive. Available online: https://www.nuvasive.com/procedures/featured-offerings/bendini/ (accessed on 5 December 2023).
- SMAIO and KEOPS. Available online: https://smaio.com/e-ifu/archives/rev_a/KROD-IMP-IFU-UE-EN_Rev_a.pdf (accessed on 5 December 2023).
- Gutman, G.; Labelle, H.; Barchi, S.; Roussouly, P.; Berthonnaud, E.; Mac-Thiong, J.-M. Normal sagittal parameters of global spinal balance in children and adolescents: A prospective study of 646 asymptomatic subjects. Eur. Spine J. 2016, 25, 3650–3657. [Google Scholar] [CrossRef] [PubMed]
- Rothenfluh, D.A.; Stratton, A.; Nnadi, C.; Beresford-Cleary, N. A Critical Thoracic Kyphosis Is Required to Prevent Sagittal Plane Deterioration in Selective Thoracic Fusions in Lenke I and II AIS. Eur. Spine J. 2019, 28, 3066–3075. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.W.; Samdani, A.F.; Tantorski, M.; Cahill, P.; Nydick, J.; Fine, A.; Betz, R.R.; Antonacci, M.D. Cervical Sagittal Plane Decompensation after Surgery for Adolescent Idiopathic Scoliosis: An Effect Imparted by Postoperative Thoracic Hypokyphosis. J. Neurosurg. Spine 2011, 15, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Abelin-Genevois, K.; Estivalezes, E.; Briot, J.; Sévely, A.; De Gauzy, J.S.; Swider, P. Spino-pelvic alignment influences disc hydration properties after AIS surgery: A prospective MRI-based study. Eur. Spine J. 2015, 24, 1183–1190. [Google Scholar] [CrossRef]
- Clément, J.-L.; Pelletier, Y.; Solla, F.; Rampal, V. Surgical increase in thoracic kyphosis increases unfused lumbar lordosis in selective fusion for thoracic adolescent idiopathic scoliosis. Eur. Spine J. 2019, 28, 581–589. [Google Scholar] [CrossRef]
- Basu, S.; Solanki, A.; Patel, D.; Lenke, L.G.; Silva, F.E.; Biswas, A. Normal spino-pelvic parameters and correlation between lumbar lordosis (LL) and pelvic incidence (PI) in children and adolescents in Indian population. Spine Deform. 2021, 9, 941–948. [Google Scholar] [CrossRef]
- Ignasiak, D. A novel method for prediction of postoperative global sagittal alignment based on full-body musculoskeletal modeling and posture optimization. J. Biomech. 2020, 102, 109324. [Google Scholar] [CrossRef]
- Clement, J.-L.; Le Goff, L.; Oborocianu, I.; Rosello, O.; Bertoncelli, C.; Solla, F.; Rampal, V. Surgical increase in thoracic kyphosis predicts increase of cervical lordosis after thoracic fusion for adolescent idiopathic scoliosis. Eur. Spine J. 2021, 30, 3550–3556. [Google Scholar] [CrossRef]
- Matsumoto, H.; Colacchio, N.D.; Schwab, F.J.; Lafage, V.; Roye, D.P.; Vitale, M.G. Flatback Revisited: Reciprocal Loss of Lumbar Lordosis Following Selective Thoracic Fusion in the Setting of Adolescent Idiopathic Scoliosis. Spine Deform. 2015, 3, 345–351. [Google Scholar] [CrossRef]
- Sebaaly, A.; Silvestre, C.; Rizkallah, M.; Grobost, P.; Chevillotte, T.; Kharrat, K.; Roussouly, P. Revisiting thoracic kyphosis: A normative description of the thoracic sagittal curve in an asymptomatic population. Eur. Spine J. 2021, 30, 1184–1189. [Google Scholar] [CrossRef]
- Maillot, C.; Ferrero, E.; Fort, D.; Heyberger, C.; Le Huec, J.-C. Reproducibility and repeatability of a new computerized software for sagittal spinopelvic and scoliosis curvature radiologic measurements: Keops®. Eur. Spine J. 2015, 24, 1574–1581. [Google Scholar] [CrossRef]
- SpineEOS. Available online: https://www.eos-imaging.com/us/our-expertise/advanced-orthopedic-solutions/3d-surgical-planning-tools (accessed on 5 December 2023).
- Akbar, M.; Terran, J.; Ames, C.P.; Lafage, V.; Schwab, F. Use of surgimap spine in sagittal plane analysis, osteotomy planning, and correction calculation. Neurosurg. Clin. N. Am. 2013, 24, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Pu, J.J.M.; I Lo, A.W.; Wong, M.C.M.; Choi, W.-S.M.; Ho, G.M.; Yang, W.-F.M.; Su, Y.-X. A quantitative comparison of bone resection margin distances in virtual surgical planning versus histopathology: A prospective study. Int. J. Surg. 2023. online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Jia, S.; Weng, Y.; Wang, K.; Qi, H.; Yang, Y.; Ma, C.; Lu, W.W.; Wu, H. Performance evaluation of an AI-based preoperative planning software application for automatic selection of pedicle screws based on computed tomography images. Front. Surg. 2023, 10, 1247527. [Google Scholar] [CrossRef] [PubMed]
- Pasha, S.; Shah, S.; Newton, P.; Group, H.S. Machine Learning Predicts the 3D Outcomes of Adolescent Idiopathic Scoliosis Surgery Using Patient–Surgeon Specific Parameters. Spine 2021, 46, 579–587. [Google Scholar] [CrossRef]
- Bruschi, A.; Donati, D.M.; Di Bella, C. What to choose in bone tumour resections? Patient specific instrumentation versus surgical navigation: A systematic review. J. Bone Oncol. 2023, 42, 100503. [Google Scholar] [CrossRef]
- Schlager, B.; Großkinsky, M.; Ruf, M.; Wiedenhöfer, B.; Akbar, M.; Wilke, H.-J. Range of surgical strategies for individual adolescent idiopathic scoliosis cases: Evaluation of a multi-centre survey. Spine Deform. 2023, 12, 1–12. [Google Scholar] [CrossRef]
- Sakai, D.; Tanaka, M.; Takahashi, J.; Taniguchi, Y.; Schol, J.; Hiyama, A.; Misawa, H.; Kuraishi, S.; Oba, H.; Matsubayashi, Y.; et al. Cobalt-chromium versus titanium alloy rods for correction of adolescent idiopathic scoliosis based on 1-year follow-up: A multicenter randomized controlled clinical trial. J. Neurosurg. Spine 2021, 34, 897–906. [Google Scholar] [CrossRef]
- Wang, F.; Chen, K.; Ji, T.; Ma, Y.; Huang, H.; Zhou, P.; Wei, X.; Chen, Z.; Bai, Y. Do hypokyphotic adolescent idiopathic scoliosis patients treated with Ponte osteotomy obtain a better clinical efficacy? A preliminary retrospective study. J. Orthop. Surg. Res. 2022, 17, 491. [Google Scholar] [CrossRef]
- Wang, X.; Aubin, C.-E.; Crandall, D.; Labelle, H. Biomechanical comparison of force levels in spinal instrumentation using monoaxial versus multi degree of freedom postloading pedicle screws. Spine 2011, 36, E95–E104. [Google Scholar] [CrossRef]
- Prost, S.; Pesenti, S.; Farah, K.; Tropiano, P.; Fuentes, S.; Blondel, B. Sagittal reduction of spinal deformity: Superior versus lateral screw-rod connection. Orthop. Traumatol. Surg. Res. 2021, 107, 102954. [Google Scholar] [CrossRef] [PubMed]
- Yao, W.; Zhou, T.; Huang, K.; Dai, M.; Mo, F.; Xu, J.; Cao, Z.; Lai, Q.; Xie, B.; Guo, R.; et al. A comparison of monoaxial pedicle screw versus polyaxial pedicle screw in short-segment posterior fixation for the treatment of thoracolumbar fractured vertebra. Ann. Transl. Med. 2021, 9, 669. [Google Scholar] [CrossRef] [PubMed]
- Cidambi, K.R.; Glaser, D.A.; Bastrom, T.P.; Nunn, T.N.; Ono, T.; Newton, P.O. Postoperative changes in spinal rod contour in adolescent idiopathic scoliosis: An in vivo deformation study. Spine 2012, 37, 1566–1572. [Google Scholar] [CrossRef] [PubMed]
- Abe, Y.; Ito, M.; Abumi, K.; Sudo, H.; Salmingo, R.; Tadano, S. Scoliosis corrective force estimation from the implanted rod deformation using 3D-FEM analysis. Scoliosis 2015, 10, S2. [Google Scholar] [CrossRef]
- Kluck, D.; Newton, P.O.; Sullivan, T.B.; Yaszay, B.; Jeffords, M.; Bastrom, T.P.M.; Bartley, C.E.M. A 3D Parameter Can Guide Concave Rod Contour for the Correction of Hypokyphosis in Adolescent Idiopathic Scoliosis. Spine 2020, 45, E1264–E1271. [Google Scholar] [CrossRef]
- Sia, U.; Tan, B.; Teo, Y.; Wong, C. Post-implantation Deformation of Titanium Rod and Cobalt Chrome Rod in Adolescent Idiopathic Scoliosis. Malays. Orthop. J. 2019, 13, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Le Navéaux, F.; Aubin, C.-E.; Parent, S.; Newton, P.O.; Labelle, H. 3D rod shape changes in adolescent idiopathic scoliosis instrumentation: How much does it impact correction? Eur. Spine J. 2017, 26, 1676–1683. [Google Scholar] [CrossRef]
- Gay, M.; Wang, X.; Ritzman, T.; Floccari, L.; Schwend, R.M.; Aubin, C.-E. Biomechanical analysis of rod contouring in posterior spinal instrumentation and fusion for 3D correction of adolescent idiopathic scoliosis. Spine Deform. 2023, 11, 1–8. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhou, Q.; Zhu, C.; Liu, L.-M.; Song, Y.-M.; Yang, X. Restoring the ideal Roussouly sagittal alignment in Lenke 5 adolescent idiopathic scoliosis patients: A method for decreasing the risk of proximal junctional kyphosis. Eur. Spine J. 2023. Online ahead of print. [Google Scholar] [CrossRef]
- Ogura, Y.; Glassman, S.D.; Sucato, D.; Hresko, M.T.; Carreon, L.Y. Incidence of Proximal Junctional Kyphosis with Pedicle Screws at Upper Instrumented Vertebrae in Posterior Spinal Fusion for Adolescent Idiopathic Scoliosis. Glob. Spine J. 2021, 11, 1019–1024. [Google Scholar] [CrossRef]
- Tsirikos, A.I.; McMillan, T.E. All Pedicle Screw versus Hybrid Hook–Screw Instrumentation in the Treatment of Thoracic Adolescent Idiopathic Scoliosis (AIS): A Prospective Comparative Cohort Study. Healthcare 2022, 10, 1455. [Google Scholar] [CrossRef] [PubMed]
- Erkilinc, M.; Coathup, M.; Liska, M.G.; Lovevoy, J. Can placement of hook at the upper instrumented level decrease the proximal junctional kyphosis risk in adolescent idiopathic scoliosis? Eur. Spine J. 2023, 32, 3113–3117. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| General Informations | MINORS Sub-Score | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Main Author | Type of Study * | Minimum Follow-Up (Months) | Type of Paper ** | A Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Collection of Data | Appropriate Endpoints | Unbiased Assessment of the Endpoint | Follow-Up Period | Loss to Follow Up < 5% | Adequate Statistical Analyses | Total | Out of | Quality |
| Thomas | 1 | 24 | A | 2 | 2 | 1 | 2 | 0 | 2 | 1 | 2 | 12 | 16 | Good |
| Marya | 1 | 6 | A | 2 | 2 | 1 | 2 | 1 | 1 | 0 | 2 | 11 | 16 | Good |
| Solla (OTSR) | 1 | 12 | A | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 13 | 16 | Excellent |
| Solla (ESJ) | 2 | 12 | P | 2 | 0 | 1 | 2 | 1 | 1 | 0 | 2 | 9 | 16 | Good |
| Alijanipour | 1 | 12 | P | 2 | 2 | 1 | 2 | 0 | 1 | 0 | 2 | 15 *** | 24 | Good |
| Grobost/Abelin | 1 | 6 | P | 1 | 2 | 2 | 2 | 1 | 1 | 0 | 1 | 10 | 16 | Good |
| Ferrero | 1 | 4 | A | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 12 | 16 | Good |
| Average | 10.86 | 1.86 | 1.71 | 1.43 | 2.00 | 0.86 | 1.00 | 0.29 | 1.86 | 11.17 | 16 | |||
| Modal value | 1 | 12 | A | 2 | 2 | 1 | 2 | 1 | 1 | 0 | 2 | 12 | Good | |
| Program | Online/Downolad? | Free/Suscription | Owner | Link to Spine Companies | Planning Author | Pros | Cons |
|---|---|---|---|---|---|---|---|
| Surgimap | Download | Basic version is free | Independent | Stryker, Globus, various | Surgeon | Free version | |
| Keops | Online | Subscription (but usually free for SMAIO clients) | Smaio | Smaio | SMAIO Company | Possible data sharing for scientifc studies; Radiological analysis by a third part | |
| Unid hub | Online | Free for Medtronic clients | Medtronic | Medtronic only | Surgeon and/or Medtronic team | Radiological analysis by a third part | Hard password; only for medtronic planning |
| SpineEOS | Online | Subscription | Alphatec | None | Surgeon | Link to EOS imaging | Need for EOS imaging |
| Company (Country) | Type of Technology | Type of Rods | Rod–Screw Connection | Fixation Implants |
|---|---|---|---|---|
| Medicrea (Fr)/Medtronic (US) | Planning and manufacture | Ti or CoCr, 6 or 5.5 or 3.5 mm, round or derotation rod with baseball-field section (2 plate faces and 2/3 of circus) | -Top connection (tulip screws) | Polyaxial, monoaxial or uniplanar pedicle screws; |
| -Side connection (dome screws) with polyaxial/derotation/realignment connectors | Hooks, claws, sublaminar bands | |||
| SMAIO (Fr) | Planning and manufacture | Ti 6 or 5.5 mm, round section | Side connection | Monoaxial; |
| screws, hooks and claws. | ||||
| Nuvasive (US) | Planning and measured bending with a connected bender | Ti or CrCo, 6 or 5 mm, round section | Top connection | Polyaxial or monoaxial; screws, hooks, sublaminar bands |
| Robert Reid (Japan) | Manufacturing of pre-bent rods | CrCo 5.5, round section | Side connection | Polyaxial screws |
| Main Author | Year | Planning Software | Rods Material and Technology | Pre-Bent or Manually Bent | Surgical Technique and Construct | Number of Patients | Coronal Cobb Angle | TK Increase | TK Increase in Hypo-TK | Planned TK | Planned–Achieved TK | % Patients with Normal TK at Last Follow-Up | Postoperative TL Angle |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Thomas [44] | 2022 | Unid hub | 6 mm Ti, identical, Unid | Pre-bent | ST2R with Ponte osteotomies, apical sublaminar bands (n = 4) | 48 | 63 | 6.4 | 19 | 30 to 40° | −3° | 8° lordosis | |
| Marya [43] | 2023 | Surgimap | 5.5 mm Ti, asymetrical (+20° on concave side), manually bent according to a paper template; rail on concave side, round on convex | Manually bent | Cantilever, multiple pedicle screws construct | 61 | 68 | −1 | 14 | 5° ± 4 | |||
| Solla [46] | 2018 | Surgimap | 6 mm CoCr, asymetrical, diamond section, Unid (+10° for concave side rod) | Pre-bent | ST2R, multiple pedicle screws construct, concave derotation | 37 | 53 | 14 | 20 | 34 | 0°: −4 in normoK, +5 in hypo K | 97% (1 patient with TK = 56°) | |
| Solla [47] | 2020 | Surgimap or Unid Hub | Unid, various: 5.5 or 6 mm, Ti or CoCr | Pre-bent | ST2R, multiple pedicle screws construct ± concave de-rotation or sublaminar bands | 85 | - | 12 | 19 | 1°: −4 in normoK, +6 in hypo K | 96% (2 patients with TK between 10 and 20°) | ||
| Alijanipour [39] | 2017 | Surgimap | Mostly 6 mm Ti, identical, Unid vs. conventional “unplanned” rods | Pre-bent | ST2R with multiple pedicle screws construct | 28 vs. 28 | 57 | −2 vs. −3 | significantly lordotic in C group (−7.3_) compared to PS group (−0.3_, p\0.001). | ||||
| Grobost/ Abelin [45] | 2019 | Keops | 5.5 mm CoCr or 6 mm Ti, identical, Unid | Pre-bent | ST2R with multiple pedicle screws construct + sublaminar bands at the apex | 49 | 54 ± 10 | 10 | 30 ± 8 | 0 | 95% | significantly improved after surgery | |
| Ferrero/ Ilharreborde [42] | 2018 | SpineEOS | 5.5 mm CoCr identical manually bent according to a paper template | Manually bent | Translation on 1 rod; lumbar pedicle screws and thoracic sublaminar bands | 47 | 59 ± 13 | 9 | 38 | 1 | 100% | ||
| Sum | 355 | ||||||||||||
| Average | 2020 | 5.8 | 51 | 59 | 7 | 18 | 34 | 0.67 | 97 | ||||
| Modal value | Surgimap | Pre-bent | ST2R |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solla, F.; Ilharreborde, B.; Clément, J.-L.; Rose, E.O.; Monticone, M.; Bertoncelli, C.M.; Rampal, V. Patient-Specific Surgical Correction of Adolescent Idiopathic Scoliosis: A Systematic Review. Children 2024, 11, 106. https://doi.org/10.3390/children11010106
Solla F, Ilharreborde B, Clément J-L, Rose EO, Monticone M, Bertoncelli CM, Rampal V. Patient-Specific Surgical Correction of Adolescent Idiopathic Scoliosis: A Systematic Review. Children. 2024; 11(1):106. https://doi.org/10.3390/children11010106
Chicago/Turabian StyleSolla, Federico, Brice Ilharreborde, Jean-Luc Clément, Emma O. Rose, Marco Monticone, Carlo M. Bertoncelli, and Virginie Rampal. 2024. "Patient-Specific Surgical Correction of Adolescent Idiopathic Scoliosis: A Systematic Review" Children 11, no. 1: 106. https://doi.org/10.3390/children11010106