Noninvasive Neurally Adjusted Ventilation versus Nasal Continuous or Intermittent Positive Airway Pressure for Preterm Infants: A Systematic Review and Meta-Analysis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Study Design and Methods
2.1. Eligibility Criteria
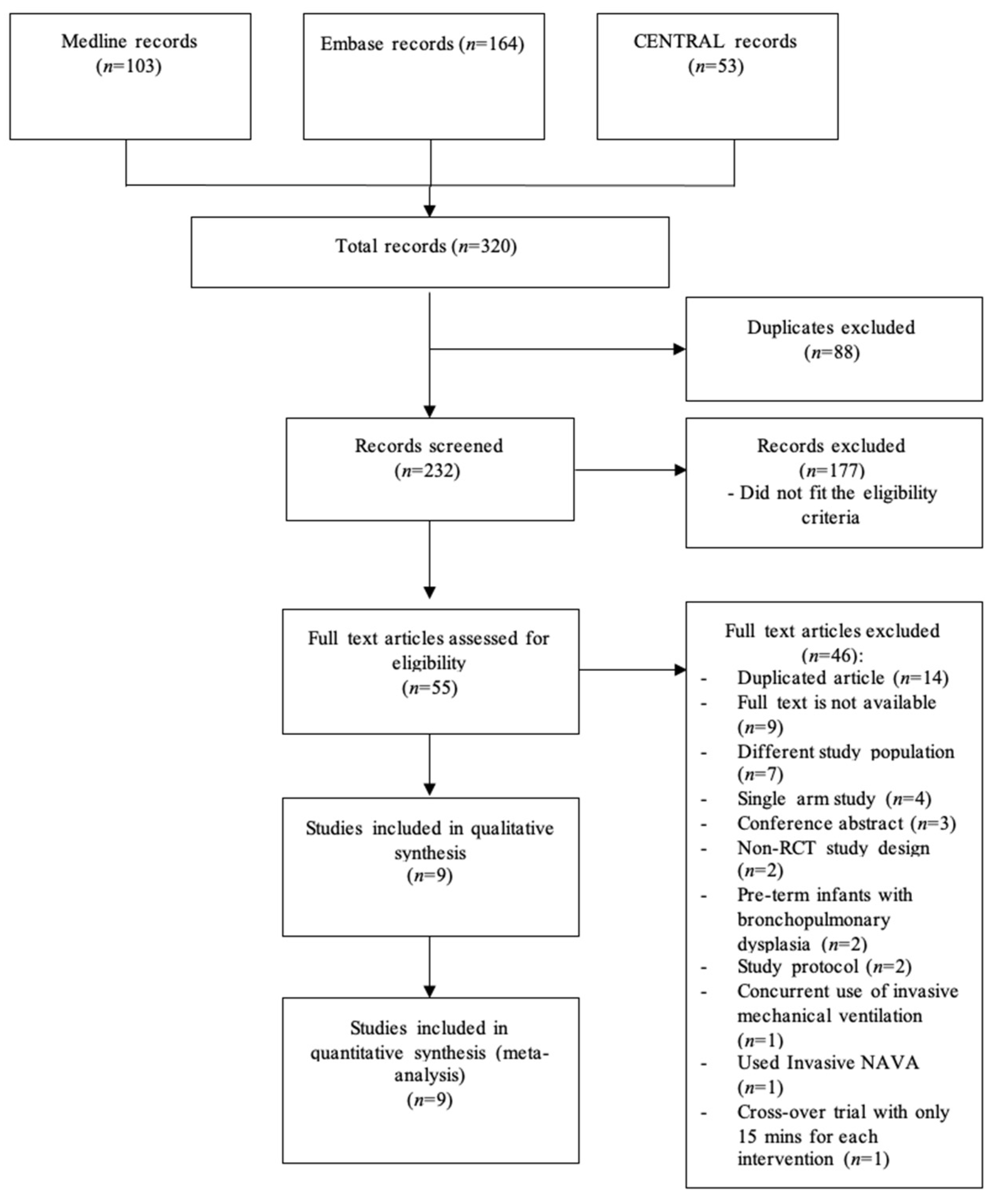
2.2. Search Strategy
2.3. Study Selection and Data Extraction
2.4. Statistical Analysis
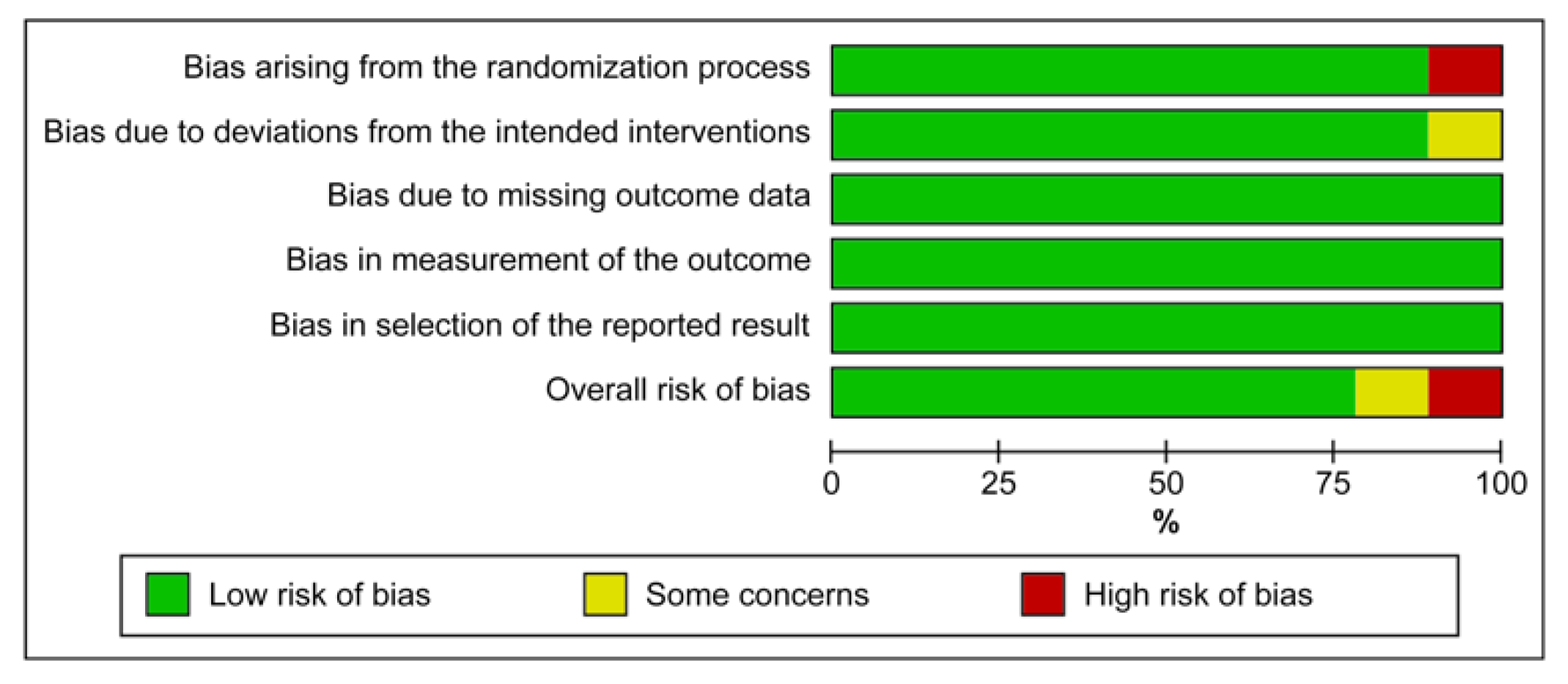
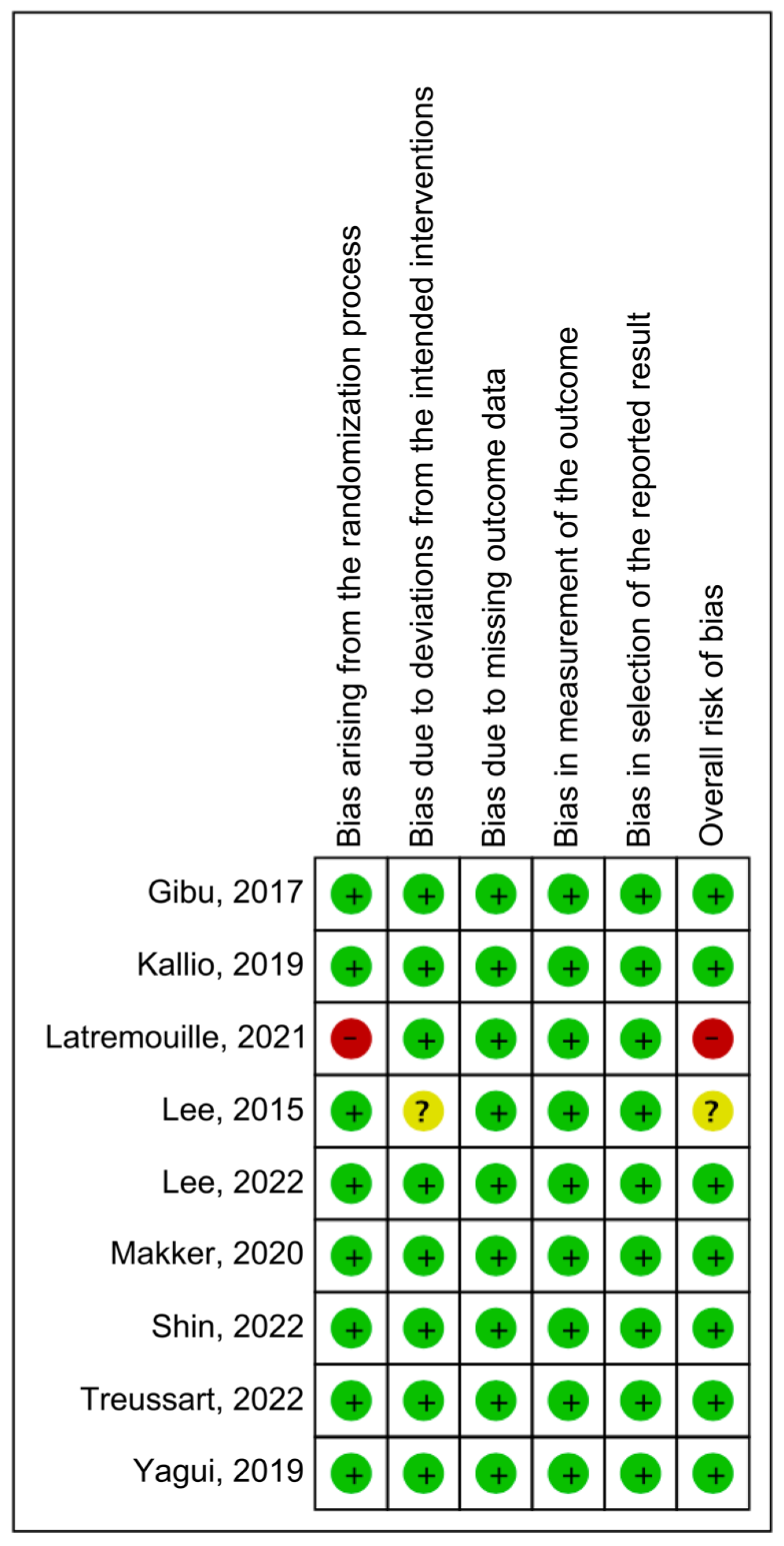
2.5. Risk of Bias Assessment
3. Results
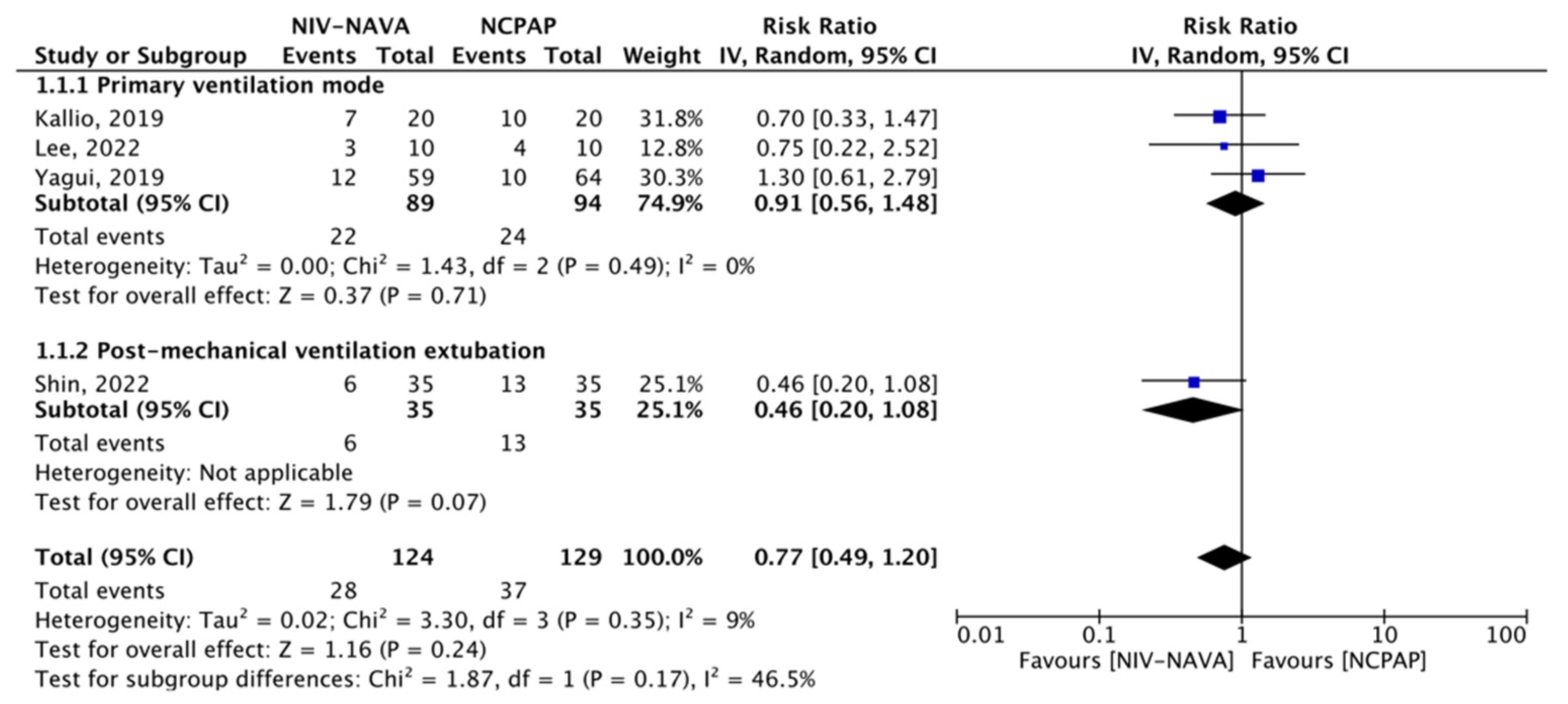
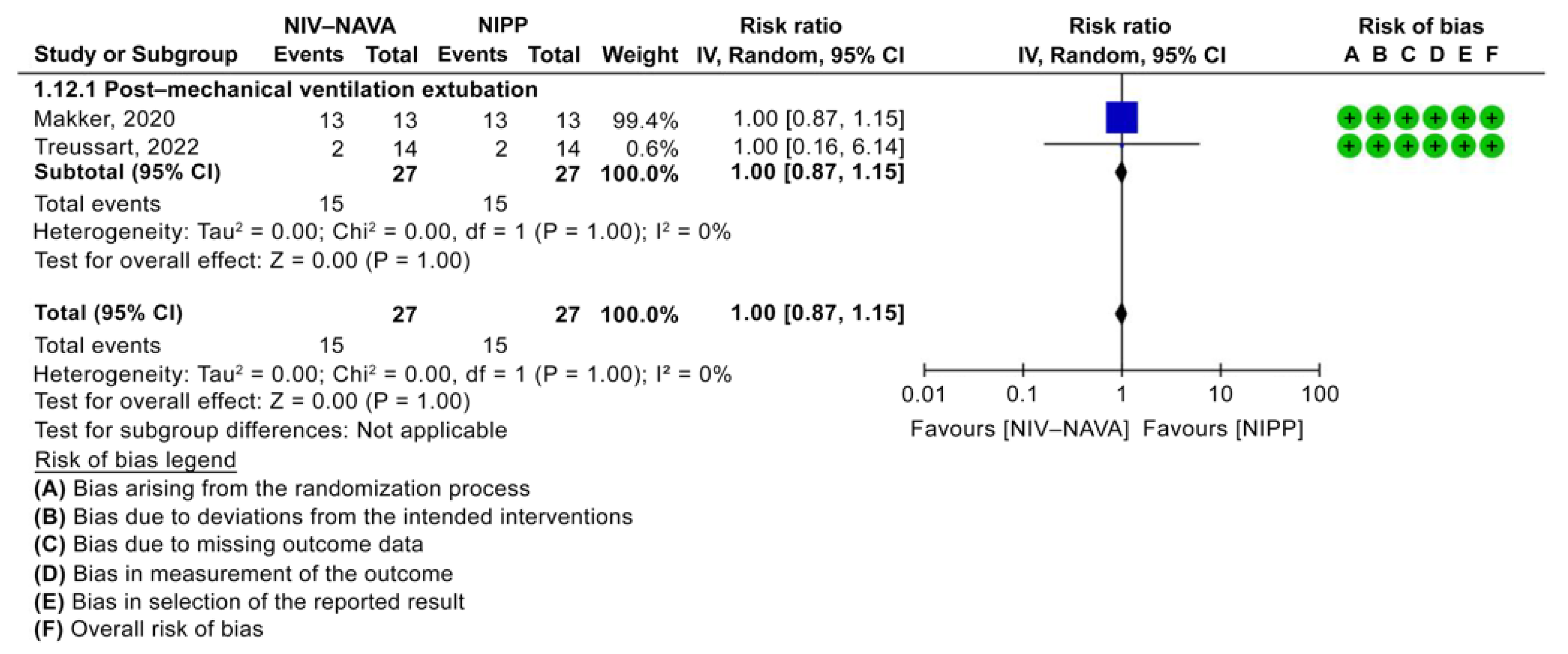
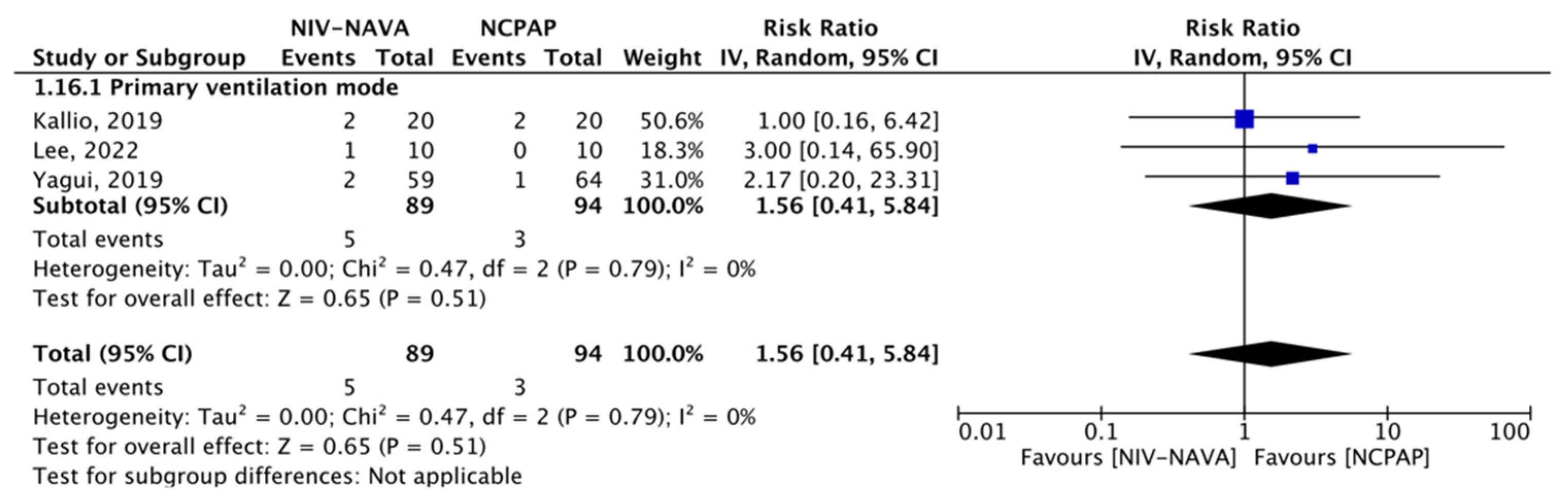
3.1. Noninvasive Modality Failure (Need for Intubation When Used as Primary Mode, and Need for Re-Intubation When Used as Weaning)
3.2. Need for Surfactant Therapy
3.3. Pneumothorax
3.4. Bronchopulmonary Dysplasia
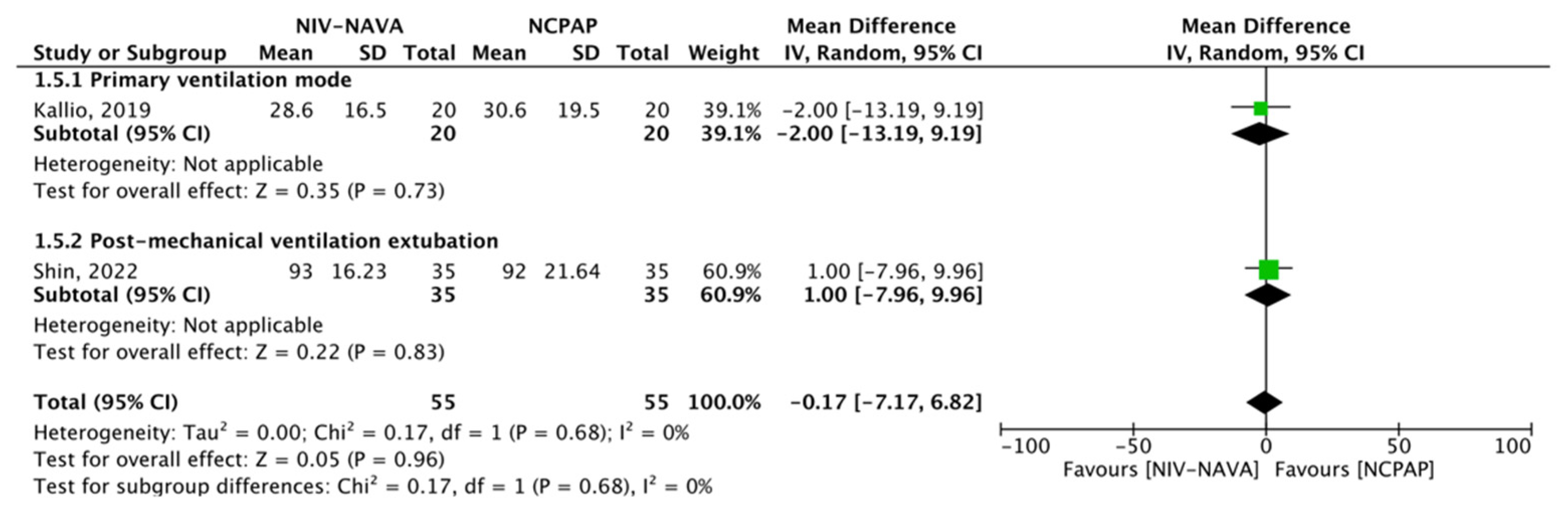
3.5. Length of NICU Stay
3.6. Length of Hospital Stay
3.7. Duration of Invasive Ventilation
3.8. Electrical Activity of the Diaphragm (Edi)
3.9. Other Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dbstet, A. WHO: Recommended definitions, terminology and format for statistical tables related to the perinatal period and use of a new certificate for cause of perinatal deaths. Modifications recommended by Figo as amended October 14, 1976. Acta Obs. Gynecol Scand 1977, 56, 247–253. [Google Scholar]
- Raju, T.N.K.; Higgins, R.D.; Stark, A.R.; Leveno, K.J. Optimizing care and outcome for late-preterm (near-term) infants: A summary of the workshop sponsored by the National Institute of Child Health and Human Development. Pediatrics 2006, 118, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Koivisto, M.; Marttila, R.; Kurkinen-Räty, M.; Saarela, T.; Pokela, M.L.; Jouppila, P.; Hallman, M. Changing incidence and outcome of infants with respiratory distress syndrome in the 1990s: A population-based survey. Acta Paediatr. 2004, 93, 177–184. [Google Scholar] [CrossRef]
- Morley, C.J.; Davis, P.G.; Doyle, L.W.; Brion, L.P.; Hascoet, J.M.; Carlin, J.B. Nasal CPAP or intubation at birth for very preterm infants. N. Engl. J. Med. 2008, 358, 700–708. [Google Scholar] [CrossRef]
- Van Kaam, A.H.; Rimensberger, P.C.; Borensztajn, D.; De Jaegere, A.P.; Neovent Study Group. Ventilation practices in the Neonatal Intensive Care Unit: A cross-sectional study. J. Pediatr. 2010, 157, 767–771.e1. [Google Scholar] [CrossRef]
- Mwaniki, M.K.; Atieno, M.; Lawn, J.E.; Newton, C.R. Long-term neurodevelopmental outcomes after intrauterine and neonatal insults: A systematic review. Lancet 2012, 379, 445–452. [Google Scholar] [CrossRef]
- Araújo, B.F.; Zatti, H.; Madi, J.M.; Coelho, M.B.; Olmi, F.B.; Canabarro, C.T. Analysis of neonatal morbidity and mortality in late-preterm newborn infants. J. Pediatr. 2012, 88, 259–266. [Google Scholar] [CrossRef]
- Platt, M.J. Outcomes in preterm infants. Public Health 2014, 128, 399–403. [Google Scholar] [CrossRef]
- Kinsella, J.P.; Greenough, A.; Abman, S.H. Bronchopulmonary dysplasia. Lancet 2006, 367, 1421–1431. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Plavka, R.; Saugstad, O.D.; Simeoni, U.; Speer, C.P.; Vento, M.; et al. European consensus guidelines on the management of respiratory distress syndrome—2016 update. Neonatology 2017, 111, 107–125. [Google Scholar] [CrossRef]
- Huang, L.; Mendler, M.R.; Waitz, M.; Schmid, M.; Hassan, M.A.; Hummler, H.D. Effects of synchronization during noninvasive intermittent mandatory ventilation in preterm infants with respiratory distress syndrome immediately after extubation. Neonatology 2015, 108, 108–114. [Google Scholar] [CrossRef]
- Lemyre, B.; Davis, P.G.; De Paoli, A.G.; Kirpalani, H. Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation. Cochrane Database Syst. Rev. 2017, 2, CD003212. [Google Scholar] [CrossRef]
- Beck, J.; Reilly, M.; Grasselli, G.; Qui, H.; Slutsky, A.S.; Dunn, M.S.; Sinderby, C.A. Characterization of neural breathing pattern in spontaneously breathing preterm infants. Pediatr. Res. 2011, 70, 607–613. [Google Scholar] [CrossRef]
- Stein, H.; Alosh, H.; Ethington, P.; White, D.B. Prospective crossover comparison between Nava and pressure control ventilation in premature neonates less than 1500 grams. J. Perinatol. 2013, 33, 452–456. [Google Scholar] [CrossRef]
- Lee, J.; Kim, H.S.; Jung, Y.H.; Shin, S.H.; Choi, C.W.; Kim, E.K.; Kim, B.I.; Choi, J.H. Non-invasive neurally adjusted ventilatory assist in preterm infants: A randomised phase II crossover trial. Arch. Dis. Child Fetal. Neonatal. Ed. 2015, 100, F507–F513. [Google Scholar] [CrossRef]
- Colaizy, T.T.; Kummet, G.J.; Kummet, C.M.; Klein, J.M. Noninvasive neurally adjusted ventilatory assist in premature infants postextubation. Am. J. Perinatol. 2017, 34, 593–598. [Google Scholar] [CrossRef]
- Beck, J.; Brander, L.; Slutsky, A.S.; Reilly, M.C.; Dunn, M.S.; Sinderby, C. Non-invasive neurally adjusted ventilatory assist in rabbits with acute lung injury. Intensive Care Med. 2008, 34, 316–323. [Google Scholar] [CrossRef]
- Sinderby, C.; Navalesi, P.; Beck, J.; Skrobik, Y.; Comtois, N.; Friberg, S.; Gottfried, S.B.; Lindström, L. Neural control of mechanical ventilation in respiratory failure. Nat. Med. 1999, 5, 1433–1436. [Google Scholar] [CrossRef]
- Sinderby, C.; Beck, J. Neurally adjusted ventilatory assist in non-invasive ventilation. Minerva Anestesiol. 2013, 79, 915–925. [Google Scholar]
- Gibu, C.K.; Cheng, P.Y.; Ward, R.J.; Castro, B.; Heldt, G.P. Feasibility and physiological effects of noninvasive neurally adjusted ventilatory assist in preterm infants. Pediatr. Res. 2017, 82, 650–657. [Google Scholar] [CrossRef]
- Kallio, M.; Mahlman, M.; Koskela, U.; Aikio, O.; Suo-Palosaari, M.; Pokka, T.; Saarela, T.; Hallman, M. NIV NAVA versus nasal CPAP in premature infants: A randomized clinical trial. Neonatology 2019, 116, 380–384. [Google Scholar] [CrossRef]
- Latremouille, S.; Bhuller, M.; Shalish, W.; Sant’Anna, G. Cardiorespiratory effects of NIV-NAVA, NIPPV, and NCPAP shortly after extubation in extremely preterm infants: A randomized crossover trial. Pediatr. Pulmonol. 2021, 56, 3273–3282. [Google Scholar] [CrossRef]
- Goel, D.; Oei, J.L.; Smyth, J.; Schindler, T. Diaphragm-triggered non-invasive respiratory support in preterm infants. Cochrane Database Syst. Rev. 2020, 3, CD012935. [Google Scholar] [CrossRef]
- Xu, Y.; Zhu, X.; Kong, X.; Li, J. Outcomes of noninvasive neurally adjusted ventilatory assist and nasal continuous positive airway pressure in preterm infants: A systematic review and meta-analysis. Arch. Argent. Pediatr. 2022, 120, 89–98. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Higgins, J.P.; Eldridge, S.; Li, T. Including variants on randomized trials. In Cochrane Handbook for Systematic Reviews of Interventions; Wiley: Hoboken, NJ, USA, 2019; pp. 569–593. [Google Scholar]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Lee, J.; Parikka, V.; Oda, A.; Wallström, L.; Lehtonen, L.; Soukka, H. NIV-NAVA versus NCPAP immediately after birth in premature infants: A randomized controlled trial. Respir. Physiol. Neurobiol. 2022, 302, 103916. [Google Scholar] [CrossRef]
- Makker, K.; Cortez, J.; Jha, K.; Shah, S.; Nandula, P.; Lowrie, D.; Smotherman, C.; Gautam, S.; Hudak, M.L. Comparison of extubation success using noninvasive positive pressure ventilation (NIPPV) versus noninvasive neurally adjusted ventilatory assist (NI-NAVA). J. Perinatol. 2020, 40, 1202–1210. [Google Scholar] [CrossRef]
- Shin, S.H.; Shin, S.H.; Kim, S.H.; Song, I.G.; Jung, Y.H.; Kim, E.K.; Kim, H.S. Noninvasive neurally adjusted ventilation in postextubation stabilization of preterm infants: A randomized controlled study. J. Pediatr. 2022, 247, 53–59.e1. [Google Scholar] [CrossRef]
- Treussart, C.; Decobert, F.; Tauzin, M.; Bourgoin, L.; Danan, C.; Dassieu, G.; Carteaux, G.; Mekontso-Dessap, A.; Louis, B.; Durrmeyer, X. Patient-ventilator synchrony in extremely premature neonates during non-invasive neurally adjusted ventilatory assist or synchronized intermittent positive airway pressure: A randomized crossover pilot trial. Neonatology 2022, 119, 386–393. [Google Scholar] [CrossRef]
- Yagui, A.C.; Meneses, J.; Zólio, B.A.; Brito, G.M.G.; da Silva, R.J.; Rebello, C.M. Nasal continuous positive airway pressure (NCPAP) or noninvasive neurally adjusted ventilatory assist (NIV-NAVA) for preterm infants with respiratory distress after birth: A randomized controlled trial. Pediatr. Pulmonol. 2019, 54, 1704–1711. [Google Scholar] [CrossRef]
- Shalish, W.; Kanbar, L.; Kovacs, L.; Chawla, S.; Keszler, M.; Rao, S.; Panaitescu, B.; Laliberte, A.; Precup, D.; Brown, K.; et al. The impact of time interval between extubation and reintubation on death or bronchopulmonary dysplasia in extremely preterm infants. J. Pediatr. 2019, 205, 70–76.e2. [Google Scholar] [CrossRef]
- Shalish, W.; Kanbar, L.; Keszler, M.; Chawla, S.; Kovacs, L.; Rao, S.; Panaitescu, B.A.; Laliberte, A.; Precup, D.; Brown, K.; et al. Patterns of reintubation in extremely preterm infants: A longitudinal cohort study. Pediatr. Res. 2018, 83, 969–975. [Google Scholar] [CrossRef]
- Kirpalani, H.; Millar, D.; Lemyre, B.; Yoder, B.A.; Chiu, A.; Roberts, R.S.; Roberts, R.S.; NIPPV Study Group. A trial comparing noninvasive ventilation strategies in preterm infants. N. Engl. J. Med. 2013, 369, 611–620. [Google Scholar] [CrossRef]
- Lemyre, B.; Deguise, M.O.; Benson, P.; Kirpalani, H.; Ekhaguere, O.A.; Davis, P.G. Early nasal intermittent positive pressure ventilation (NIPPV) versus early nasal continuous positive airway pressure (NCPAP) for preterm infants. Cochrane Database Syst. Rev. 2023, 7, CD005384. [Google Scholar] [CrossRef]
- Lee, B.K.; Shin, S.H.; Jung, Y.H.; Kim, E.K.; Kim, H.S. Comparison of NIV-NAVA and NCPAP in facilitating extubation for very preterm infants. BMC Pediatr. 2019, 19, 298. [Google Scholar] [CrossRef]
- Yagui, A.C.; Gonçalves, P.A.; Murakami, S.H.; Santos, A.Z.; Zacharias, R.S.B.; Rebello, C.M. Is noninvasive neurally adjusted ventilatory assistance (NIV-NAVA) an alternative to NCPAP in preventing extubation failure in preterm infants? J. Matern. Fetal. Neonatal. Med. 2021, 34, 3756–3760. [Google Scholar] [CrossRef]
- Al-Hindi, M.; Alshamrani, Z.; Alkhotani, W.; Albassam, A.; Amin Tashkandi, A.; AlQurashi, M. Utilization of health-care resources of preterm infants during their first 2 years of life after discharge from neonatal intensive care unit. J. Clin. Neonatol. 2021, 10, 37. [Google Scholar] [CrossRef]
- Alharbi, A.S.; Alqwaiee, M.; Al-Hindi, M.Y.; Mosalli, R.; Al-Shamrani, A.; Alharbi, S.; Yousef, A.; Al Aidaroos, A.; Alahmadi, T.; Alshammary, A.; et al. Bronchiolitis in children: The Saudi initiative of bronchiolitis diagnosis, management, and prevention (SIBRO). Ann. Thorac. Med. 2018, 13, 127–143. [Google Scholar] [CrossRef]
- Al-Hindi, M.Y.; Almahdi, B.H.; Alasmari, D.A.; Alwagdani, R.K.; Hunjur, W.M.; Khalel, A.F.; AlQurashi, M.A. Screening for neurodevelopmental delay for preterm very low birth weight infants at Tertiary Care Center in Saudi Arabia. Cureus 2021, 13, e20092. [Google Scholar] [CrossRef]
- Al-Hindi, M.Y.; Al Sayari, T.A.; Al Solami, R.; Al Baiti, A.K.; Alnemri, J.A.; Mirza, I.M.; Alattas, A.; Faden, Y.A. Association of antenatal risk score with maternal and neonatal mortality and morbidity. Cureus 2020, 12, e12230. [Google Scholar] [CrossRef]
- Al-Hindi, M.Y.; Aljuhani, H.; Alnajjar, A.R.; Alessa, S.; Alqurashi, M.; Faden, Y.A. Examining the association between parental socioeconomic status and preterm birth using multidomain social determinants scale in a Tertiary Care Center in Saudi Arabia. Cureus 2020, 12, e10506. [Google Scholar] [CrossRef]
- Bolisetty, S.; Legge, N.; Bajuk, B.; Lui, K. Preterm infant outcomes in New South Wales and the Australian Capital Territory. J. Paediatr. Child Health 2015, 51, 713–721. [Google Scholar] [CrossRef]
- Darnall, R.A. The role of CO2 and central chemoreception in the control of breathing in the fetus and the neonate. Respir. Physiol. Neurobiol. 2010, 173, 201–212. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study, Year (Sample Size) (Type of Trial) | Gender | Mean Gestational Age (Weeks) | Mean Birth Weight (g) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| NIV-NAVA | NCPAP | NIPP | NIV-NAVA | NCPAP | NIPP | NIV-NAVA | NCPAP | NIPP | ||
| M/F | M/F | M/F | ||||||||
| Primary Mode | Kallio, 2019 (n = 40) (RCT) | 1:1 | 1.86:1 | - | 33.1 (±2.0) * | 33.0 (±1.8) * | - | 2140 (±766) * | 2122 (±776) * | - |
| Lee, 2022 (n = 10) (RCT) | 1:1.5 | 1:1.5 | - | 29.57 (±2) * | 29.9 (±1.29) * | - | 1331 (±370) * | 1346 (±379) * | - | |
| Yagui, 2019 (n = 123) (RCT) | 1:1.68 | 1.13:1 | - | 29.6 (±2.1) * | 29.8 (±2.1) * | - | 1077.8 (±259) * | 1130 (±258.4) * | - | |
| Secondary (weaning) Mode | Shin, 2022 (n = 70) (RCT) | 1.5:1 | 1.9:1 | - | 26.6 (25.4–28.3) ** | 27.1 (26–29) ** | - | 880 (740–1110) ** | 970 (740–1120) ** | - |
| Lee, 2015 (n = 15) (C/O) | 1.5:1 | - | 1.5:1 | 27.1 (26–28.29) *** | - | 27.1 (26–28.29) *** | 790 (675–1215) *** | - | 790 (675–1215) *** | |
| Treussart, 2022 (n = 14) (C/O) | 1.3:1 | - | 1.3:1 | 25.6 (25.3–26.4) ** | - | 25.6 (25.3–26.4) ** | 755 (686–824) ** | - | 755 (686–824) ** | |
| Makker, 2020 (n = 26) (RCT) | 1:1.17 | - | 1:1.6 | 27 (25–28) ** | - | 27 (26–30) ** | 1000 (840–1120) ** | - | 990 (690–1370) ** | |
| Gibu, 2017 (n = 8) (C/O) | - | - | - | 25.48 (±1.48) * | - | 25.48 (±1.48) * | 791.125 (±209.35) * | - | 791.125 (±209.35) * | |
| Latremouille, 2021 (n = 23) (C/O) | 1:1.09 | 1:1.09 | 1:1.09 | 25.9 (25.2–26.4) ** | 760 (595–900) ** | |||||
| Outcome (Comparison) | Certainty Assessment | ||||||
|---|---|---|---|---|---|---|---|
| Participants (Studies) | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Certainty of Evidence | |
| Modality Failure (NIV-NAVA VS. NCPAP) | 253 (4 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| Length of hospital stay (NIV-NAVA VS. NCPAP) | 110 (2 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| Mean time to full enteral feeding (NIV-NAVA VS. NCPAP) | 110 (2 RCTs) | not serious | not serious | not serious | serious b | none | Moderate |
| Duration of invasive ventilation after intubation (NIV-NAVA VS. NCPAP) | 183 (3 RCTs) | not serious | serious c | not serious | serious a | none | Low |
| Need for surfactant therapy (NIV-NAVA VS. NCPAP) | 183 (3 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| Need for surfactant therapy (NIV-NAVA VS. NIPP) | 54 (2 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| Desaturation (NIV-NAVA VS. NCPAP) | 116 (2 RCTs) | serious b | not serious | not serious | serious a | none | Low |
| Desaturation (NIV-NAVA VS. NIPP) | 76 (2 RCTs) | serious b | serious d | not serious | serious a | none | Very low |
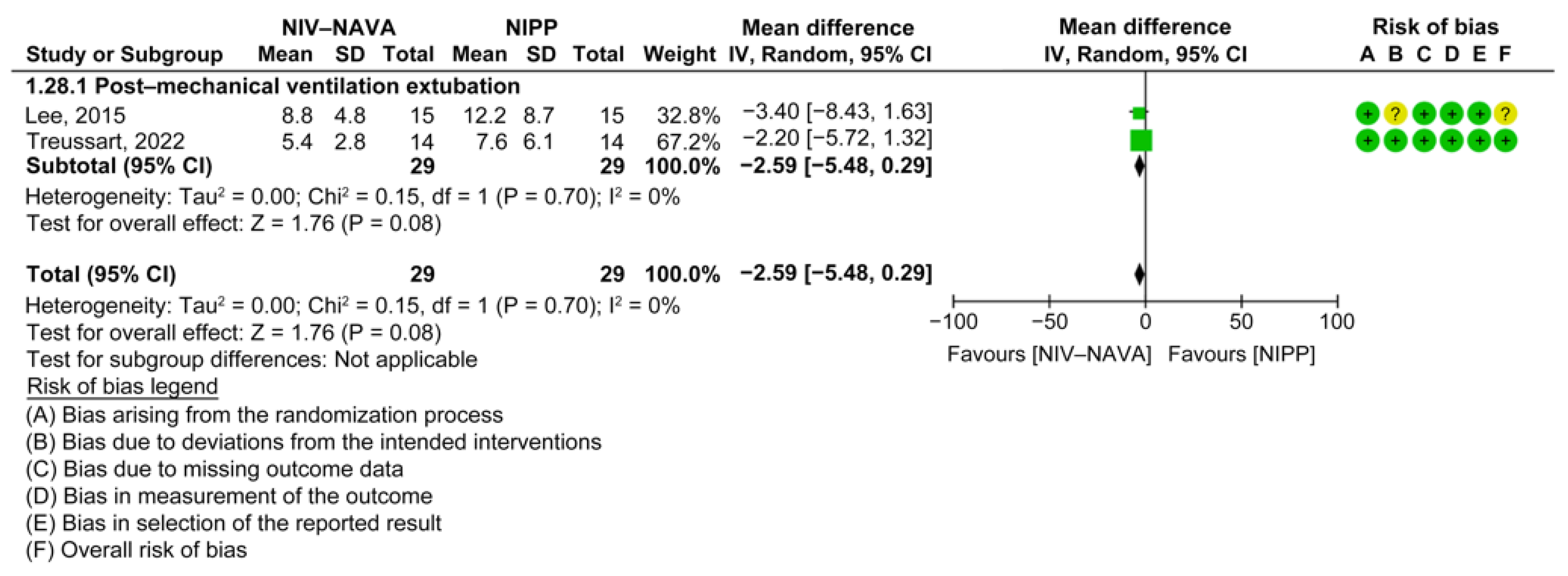
| Bradycardia (NIV-NAVA VS. NIPP) | 76 (2 RCTs) | serious b | not serious | not serious | serious a | none | Low |
| Pneumothorax (NIV-NAVA VS. NCPAP) | 183 (3 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| Apnea (NIV-NAVA VS. NCPAP) | 193 (2 RCTs) | not serious | serious d | not serious | serious a | none | Low |
| Patent ductus arteriosus (NIV-NAVA VS. NCPAP) | 175 (2 RCTs) | not serious | serious d | not serious | serious a | none | Low |
| BPD (NIV-NAVA VS. NCPAP) | 175 (2 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| Intraventricular hemorrhage (NIV-NAVA VS. NCPAP) | 215 (3 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| FiO2 (NIV-NAVA VS. NCPAP) | 110 (2 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
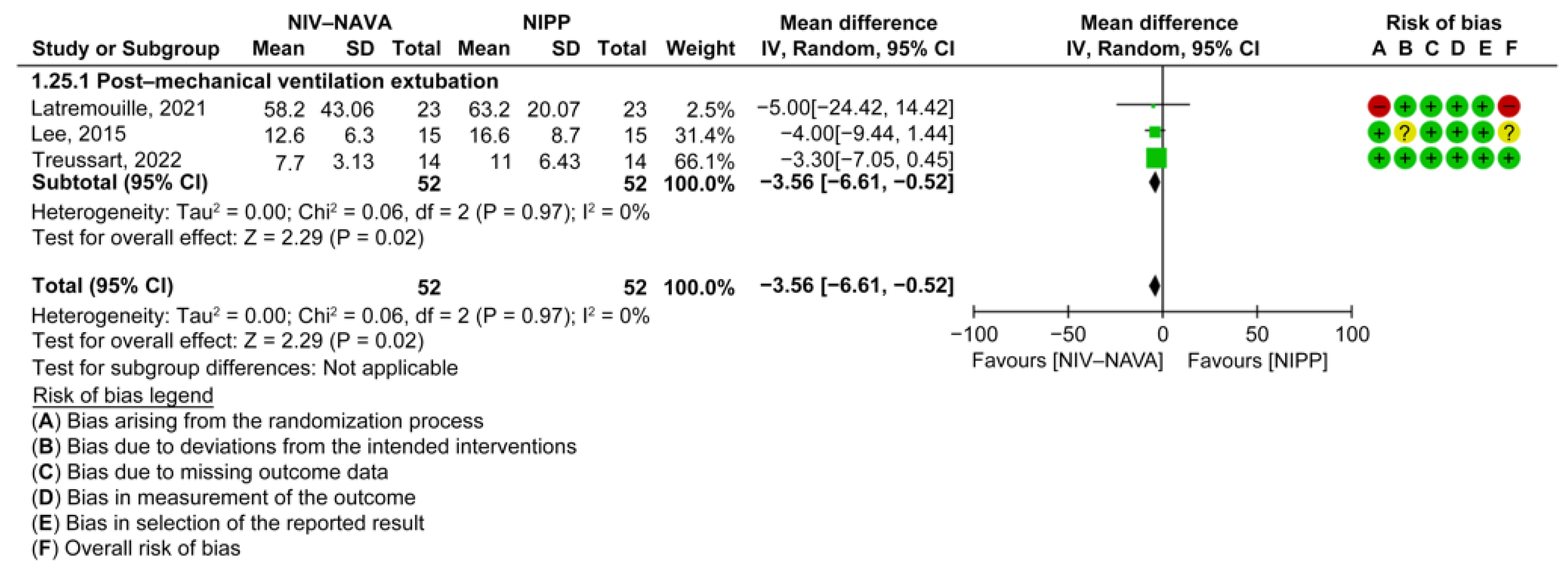
| FiO2 (NIV-NAVA VS. NIPP) | 88 (3 RCTs) | not serious | very serious c | not serious | serious a | none | Very low |
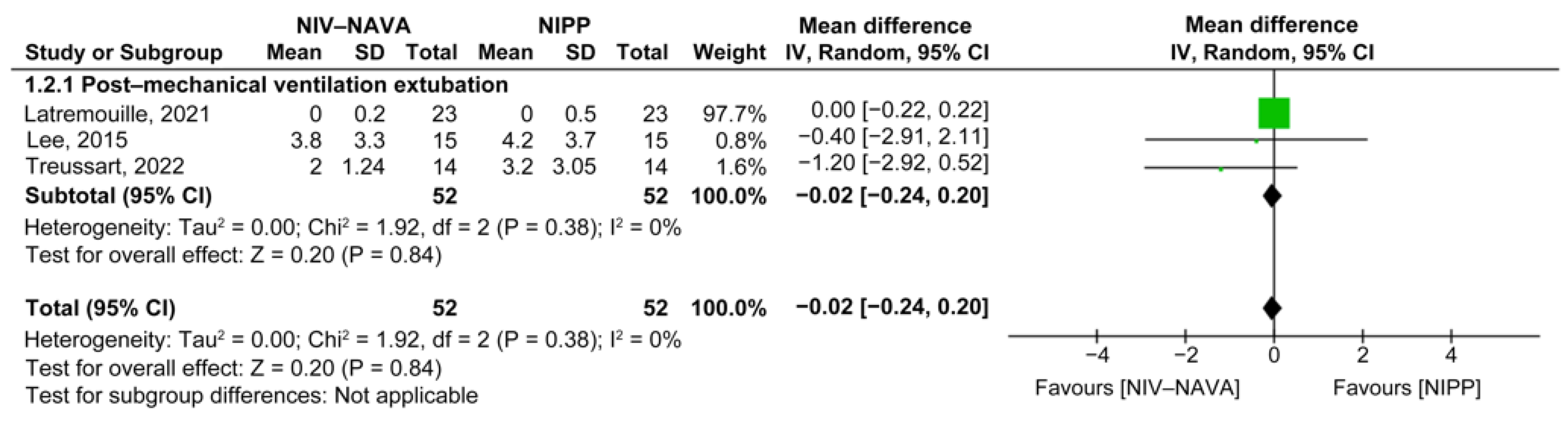
| Respiratory rate (NIV-NAVA VS. NIPP) | 44 (2 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| maximum Edi (NIV-NAVA VS. NIPP) | 104 (3 RCTs) | serious b | not serious | not serious | serious a | none | Low |
| swing Edi (NIV-NAVA VS. NIPP) | 58 (2 RCTs) | not serious | not serious | not serious | very serious a | none | Low |
| minimum Edi (NIV-NAVA VS. NIPP) | 104 (3 RCTs) | serious b | not serious | not serious | serious a | none | Low |
| Mean pH NIV-NAVA VS. NCPAP) | 110 (2 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
| Mean pCO2 (NIV-NAVA VS. NCPAP) | 110 (2 RCTs) | not serious | not serious | not serious | serious a | none | Moderate |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhader, M.; Al-Hindi, M.; Ghaddaf, A.; Alamoudi, A.; Abualola, A.; Kalantan, R.; AlKhulifi, N.; Halawani, I.; Al-Qurashi, M. Noninvasive Neurally Adjusted Ventilation versus Nasal Continuous or Intermittent Positive Airway Pressure for Preterm Infants: A Systematic Review and Meta-Analysis. Children 2023, 10, 1935. https://doi.org/10.3390/children10121935
Bhader M, Al-Hindi M, Ghaddaf A, Alamoudi A, Abualola A, Kalantan R, AlKhulifi N, Halawani I, Al-Qurashi M. Noninvasive Neurally Adjusted Ventilation versus Nasal Continuous or Intermittent Positive Airway Pressure for Preterm Infants: A Systematic Review and Meta-Analysis. Children. 2023; 10(12):1935. https://doi.org/10.3390/children10121935
Chicago/Turabian StyleBhader, Mohammed, Mohammed Al-Hindi, Abdullah Ghaddaf, Anas Alamoudi, Amal Abualola, Renad Kalantan, Norah AlKhulifi, Ibrahim Halawani, and Mansour Al-Qurashi. 2023. "Noninvasive Neurally Adjusted Ventilation versus Nasal Continuous or Intermittent Positive Airway Pressure for Preterm Infants: A Systematic Review and Meta-Analysis" Children 10, no. 12: 1935. https://doi.org/10.3390/children10121935