
Illness-Promoting Psychological Processes in Children and Adolescents with Functional Neurological Disorder
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Data Acquisition
2.3. Analysis of Clinical Characteristics and Psychological Processes Data
2.4. Missing Data
2.5. Participant Characteristics
2.6. Self-Report Data and Global Assessment of Function
3. Results: Illness-Promoting Psychological Processes Identified during Admission to the Mind–Body Program (FND Group Only)
- −
- Attentional processes: attention to symptoms (n = 61; 80.3%);
- −
- Cognitive processes and expectations related to the functional symptoms: e.g., negative/catastrophic-symptom expectations (n = 40; 52.6%), and experiencing a low sense of control (predictability) in relation to the symptoms (n = 44; 57.9%);
- −
- Cognitive processes (more general and related to the self): e.g., self-critical rumination (n = 42; 55.3%);
- −
- Feeling-related processes: e.g., feeling worried about schoolwork, friendships, or parental wellbeing (n = 64; 84.2), and feeling sad (n = 58; 76.3%);
- −
- Avoidance processes: e.g., pushing difficult thoughts out of mind (n = 44; 57.9%), pushing difficult feelings out of mind (feeling avoidance, n = 37; 48.7%), and avoiding activities (n = 38; 50.0%);
- −
- Disconnecting from the body and inability to sense and track body state (n = 43, 56.6%);
- −
- Unresolved loss, unresolved trauma, and unresolved bad experiences: intrusive thoughts/feelings/memories associated with the event (n = 38; 50.0%)
4. Treatment Interventions Targeting Illness-Promoting Psychological Processes
5. Centrally Important Interventions: Used with All Children and Their Families
5.1. Setting Up Positive Expectations
Vignette: Jack (use of an indirect positive suggestion)
Jack was a 13-year-old boy with functional gait difficulties. The physiotherapist began the process of removing Jack’s wheelchair, beginning with the footboard. She expressed the positive expectation that the wheelchair would soon be parked away—when, not if, Jack’s legs regained strength. Jack’s gait normalized four weeks later.
Vignette: Olga (use of a direct positive suggestion)
Olga, a 12-year-old girl experiencing functional seizures, attended an initial assessment with her distressed parents, who asked about her prognosis, “Will my child get well?” The team doctor explained that treatment outcomes are very positive. She said, “The research shows that children and adolescents do really well. Almost everyone—up to 95% of children—show full resolution of symptoms, especially when they work with a multidisciplinary team and engage in a holistic program: physiotherapy, individual therapy, working with the family, and working with the school. It will be interesting how you will notice this in your body.” Olga and her parents appeared relieved to hear this and expressed hope in the possibility of Olga’s recovery.
Vignette: Nancy (use of humour to shift expectations)
Nancy, a 13-year-old girl with limb weakness, tremors, visual symptoms, headaches, and dizziness, described her admission to her local hospital as traumatic. Her family described the staff’s clinical approach—at Nancy’s local hospital—as “punitive”. As a result, Nancy and the family had a lack of trust in the health system and were uncertain about an admission to the Mind–Body Program. During their assessment, clinicians listened attentively to the family’s story, providing space for them to discuss their difficult experiences. The clinicians also—deliberately—wove humour into the assessment in order to signal safety and play, not fault finding and sanctions. Together with the family, they laughed about the father’s extensive collection of horror figurines, thereby setting up expectations that the mind–body admission would have a light-heartened element and many opportunities for laughter.
Vignette: Meera (use of positive suggestion through hypnosis)
Meera was a 17-year-old adolescent with FND—paralysis of her legs and in one arm, with comorbid postural orthostatic tachycardia syndrome, fatigue, and social anxiety—that had not improved with treatment and that left her wheelchair-bound. On presentation Meera was hopeless and was clear that she did not expect anything to work. She did not expect to get better. To shift these expectations the therapist provided psychoeducation about the treatment outcomes for FND: she made explicit positive predictions about Meera’s likelihood of recovery. The therapists then focused on and amplified small gains that Meera was making, thereby redirecting Meera’s attention away from her perceived failures. The therapist then used hypnosis designed to build positive expectancies for the future (adapted from a Michael Yapko protocol for patients with depression). The work emphasized the idea that past (negative) experiences do not predict the future. Meera’s sense of agency and hope increased as she built the links between her actions today and her future outcome. The therapist used a mixture of general suggestions (e.g., “Every choice you make today will help to contribute to what tomorrow is like for you.”) and concrete suggestions (e.g., “Every time you choose to do your physio exercises you are helping yourself get better and better.”).
Vignette: James (use of direct positive suggestion and scaffolding)
James was an 11-year-old boy with functional seizures. He and his family had noticed a pattern where his functional seizures would subside during the school holidays and then return during school term, making it hard for James to attend school consistently. James and his therapist had worked on a variety of mind–body regulation strategies. During the school holidays James was able to use these strategies to avert a seizure when he noticed the impending warning signs. But he struggled to transfer these skills to the school environment. In a therapy appointment scheduled for the last week of the school term before the holidays, the therapist made the explicit prediction that he would do well in the school holidays, as he had always done so before. When James came for a review at the end of the holidays, he had (as expected) done very well (no functional seizures). The therapist then made a second prediction that, given how well he had done in the school holidays, he would be able to carry these skills through to the new school term. The session then focussed on what skills James had used in the school holidays and how he could carry these through to the school term (i.e., building up a sense of agency alongside positive expectations). At his next appointment, James was proud to report he had spent the last two weeks at school seizure free.
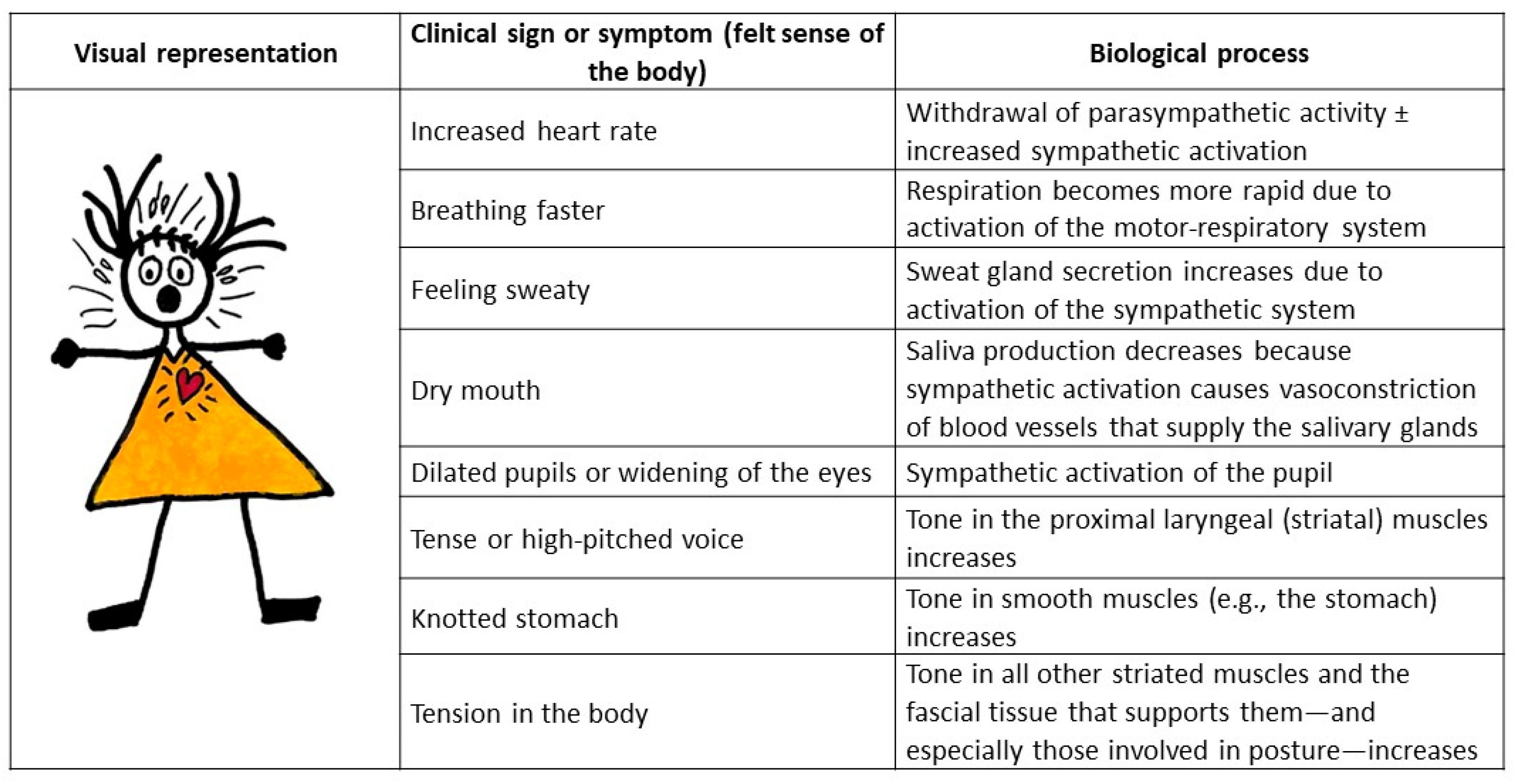
5.2. Working with the Felt Sense of the Body: Noticing and Sequencing Body Sensations
5.3. Working with Focus of Attention
Vignette: Becca (carers stepping back to allow development of regulation strategies)
Becca, a 16-year-old girl, suffered from functional seizures (including drop attacks). These were occurring 20–30 times daily. Becca’s parents would provide physical comfort and support: they cradled and stroked her head, lifted her up onto a chair or bed, and asked how she was feeling. In hospital, a new response to functional seizures was negotiated and was practiced by Becca, her parents, and the nursing staff. The nursing staff were to check that Becca was not injured (e.g., had not hit her head) and that she was safe on the floor. Becca was to practice implementation of the regulation strategies she was learning, and she was to get up from the floor when she was ready (had regained control). Over a two-week period, Becca’s functional seizures (and particularly her drop attacks) reduced to approximately 4–5 daily. She and her parents, as well as school staff, were then able to implement the new approach to managing the functional seizures. Becca continued to build her regulation skills with the support of an outpatient therapist.
Vignette: Sarah (use of metaphor to shift attention)
Sarah, a 19-year-old young woman with complex pain and functional weakness in her legs, was struggling to manage escalations of pain. Managing pain was important because the escalations of pain were accompanied by a wobbly gait and difficulties in mobilizing, requiring Sarah to use crutches. Sarah’s therapist used the metaphor of a torch with either a narrow or wide beam to talk about the impact of narrowly focusing on her pain (thereby amplifying her pain) versus expanding her focus to other things (thereby decreasing her pain). Sarah practiced expanding and contracting her focus of attention and became skilled at using this pain management strategy.
Vignette: Finn (parents reduce their attention to symptoms)
Finn, a 13-year-old boy, developed functional seizures following the death of his father and a stressful time at high school. The seizures were unpredictable. Finn’s mother had noticed however, that the seizures seemed to come on days when Finn woke up with a headache. The family doctor suggested that paracetamol would potentially be helpful. Thereafter, each morning on waking Finn, his mother would check his headache in case he needed medication. This wake-up procedure—carried out with good intentions—subsequently became an important maintenance factor (daily attention to, and reinforcement of, Finn’s headache) that gave birth to negative expectations of new seizures later the same day. When the wake-up procedure was stopped, Finn’s functional seizures decreased in frequency and finally resolved.
Vignette: Elsa (reducing positive reinforcement)
Elsa, a nine-year-old girl living with both her parents and her little sister, developed acute paralysis in her legs in the aftermath of a serious car accident with her grandparents. Elsa’s parents felt guilty about the accident, and to make up for this, Elsa’s mother made everything nice and cozy at home: fresh baked goods, candlelight, and an endless variety of board games. On getting home from work each day, Elsa’s father was very attentive to her, asking lots of questions about her symptoms. Elsa basked in the attention and told the therapist, “It’s like summer holiday all year around!”.
At first, Elsa’s mother reacted with anger when the therapist explained the role of parental attention and the manner in which this attention reinforced symptoms. However, as the therapeutic relationship grew stronger, Elsa’s parents became “ready” to accept the therapist’s advice. The parents returned to a more everyday-like situation at home. On return home, Elsa’s father found other interests that he and Elsa could discuss together.
Vignette: Tom (carers reduce their attention to symptoms)
Tom, a 12-year-old boy, developed gait difficulties—an uncoordinated gait—when he failed the try out for the elite soccer team in his new school, following a long-distance family relocation. Tom’s symptoms fluctuated. Sometimes he could not stand or walk but could crawl on the floor. At other times—especially when he was alone in his room—the parents noticed that Tom’s legs were functioning. Tom’s physiotherapist had supported the use of a wheelchair, thereby minimizing Tom’s opportunities to mobilize. The paediatrician asked that his parents keep a symptom diary. Several times a day the parents assessed Tom’s symptoms by asking him questions, thereby focusing attention on his symptoms. When the hospital team began to work with Tom, the team asked the parents to stop using the diary, and the physiotherapist in the team began the process of removing the wheelchair.
6. Cognitive Behavioural Therapy Interventions
6.1. Using Sequencing to Identify Illness-Promoting Cognitions
Vignette: Ruth (identifying a sequence)
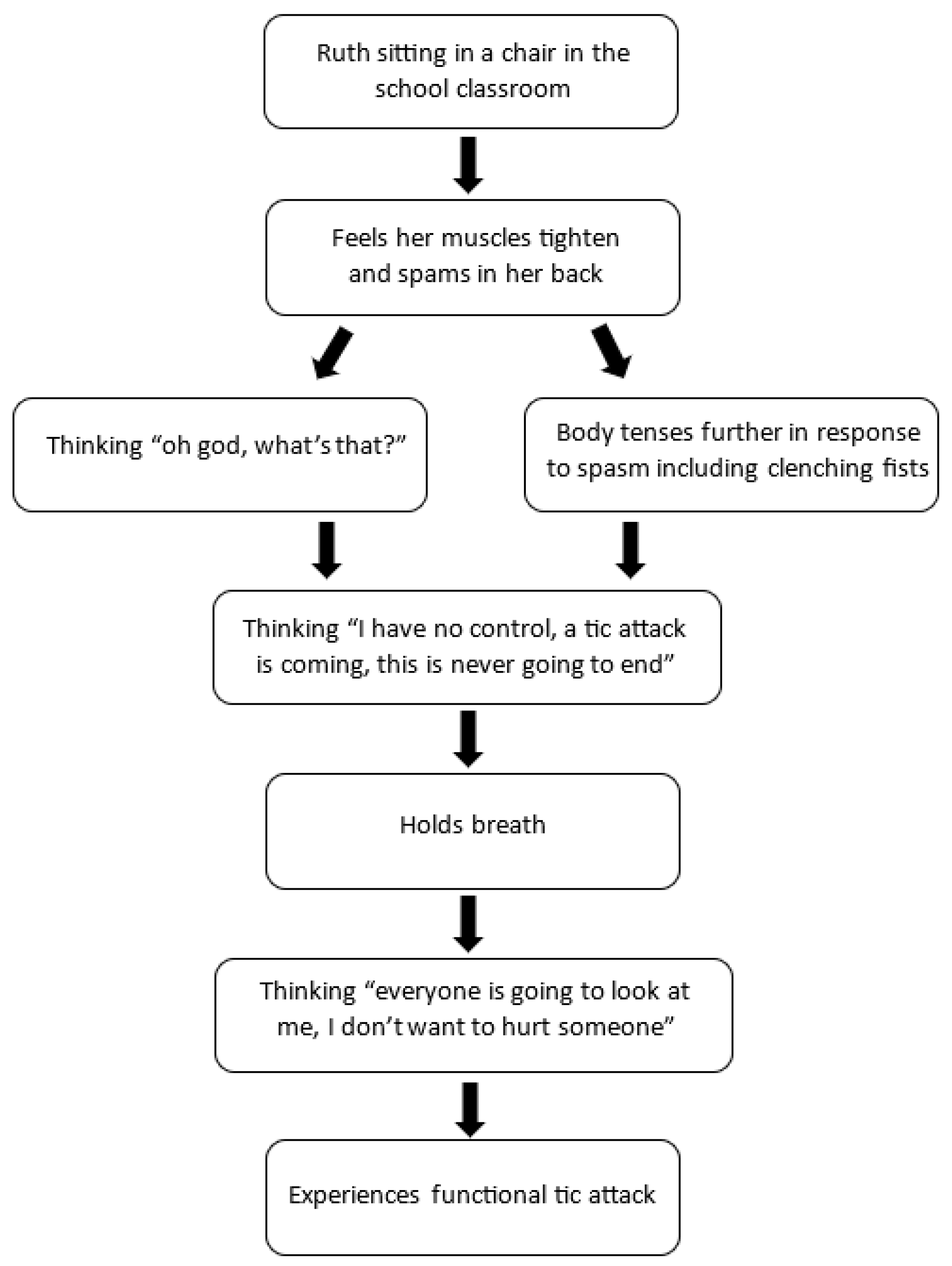
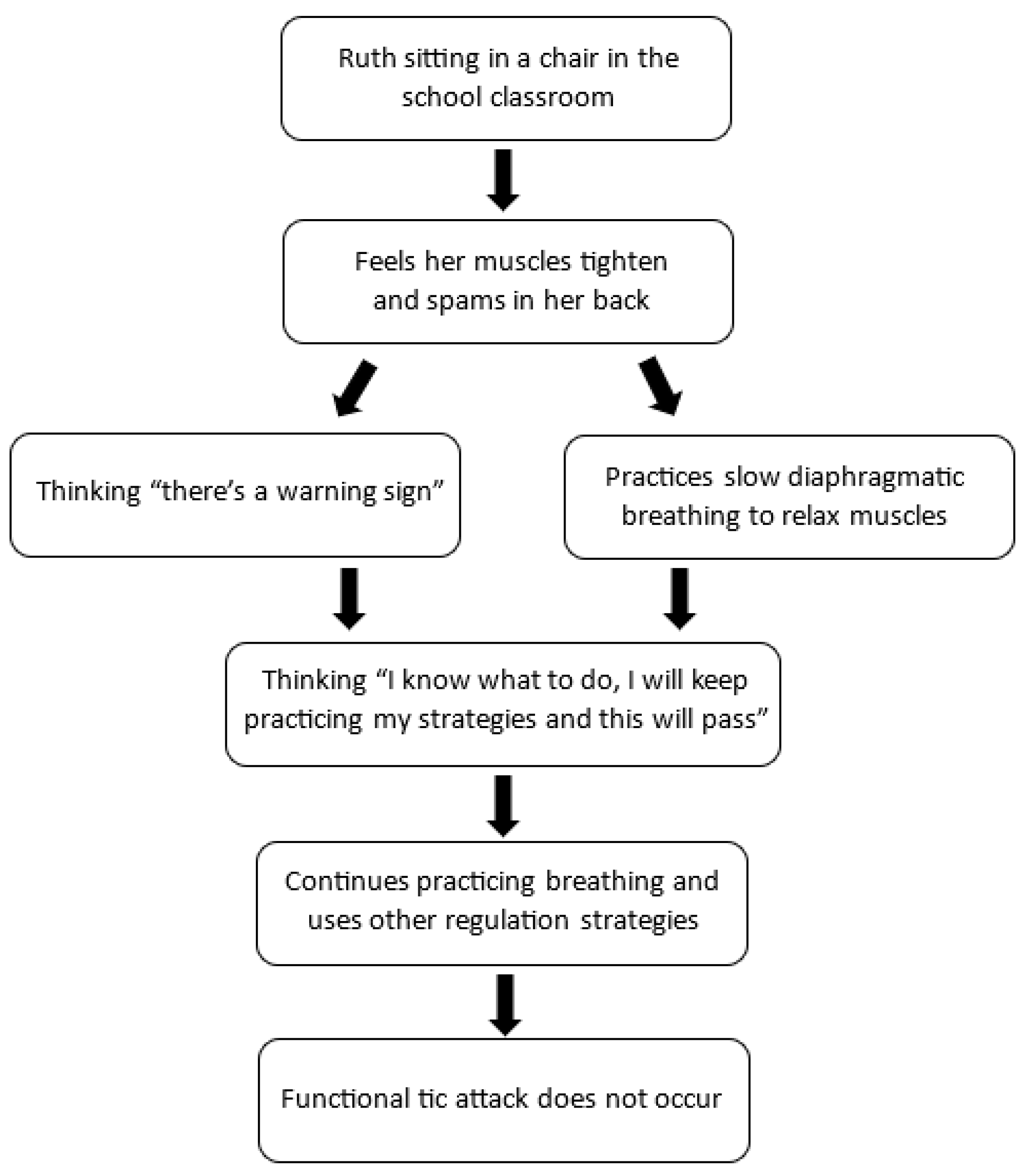
Ruth was a 14-year-old girl with recent-onset functional tics, characterized by noticeable motor movements and loud vocalizations. Ruth reported that she had no control over her tics, and she often noted that they “come out of nowhere”. Through sequencing (illustrated in Figure 8 below), Ruth was able to identify both physiological (felt sense of the body) and cognitive warning signs in the build up to a “tic attack”.
Ruth and her therapist used the visual representation of the sequence to develop an intervention (illustrated in Figure 9). First, Ruth practiced noticing and labelling her body sensations (warning signs), thoughts, and feelings in real time, as they occurred prior to a tic attack. Second, she began to practice her calming strategies as soon as she noticed the warning signs, and she would allow the attack to pass (whether the body activation eventuated into a tic attack or not). The calming strategies included diaphragmatic breathing, progressive muscle relaxation, and sensory stimulation, including chewing gum, knitting, spinning fidget toys with her fingers, and placing a weighted blanket on her lap. As part of this process, Ruth was also able to practice challenging unhelpful thinking patterns (catastrophizing and overgeneralization). For instance, she was able to replace her thought of “Oh god, what’s that” with “I can feel my warning signs”, and her thought “I have no control” to “I know what to do, I will practice my strategies, and this will pass.”
6.2. Habit Reversal
Vignette: Mariella (using habit reversal to manage functional seizures)
Mariella, a 17-year-old adolescent, developed chest pain (see Box 1, [19,20,98,99,100,101,102]) and leg tremor, following a series of viral infections. Some weeks later she began to experience full-body tremors, sometimes accompanied by memory loss. A diagnosis of functional seizures (a subtype of FND) was given. Mariella found that loud noises, crowds, and making decisions all triggered the episodes, and she began to avoid situations that presented these triggers. With time, the functional seizures worsened, and Mariella was unable to attend school. Daily, she experienced catastrophic-symptom expectations, “This is going to hurt me! I can’t control this! I am going to have an episode every time I am in a crowd!”
At the first retraining and control therapy session, a plan was developed with Mariella to retrain her FND symptoms. Competing thoughts—“I’m safe. These episodes do not hurt me. I have a good plan to manage my symptoms.”—were developed to counter her catastrophic symptom expectations. Mariella was given opposing responses to each of her symptoms (e.g., moving arms and legs in and out to counter tremors, focusing on items around her and describing them aloud to counter perceived loss of consciousness, speaking or singing to counter vocalizations), and she was instructed to begin these as soon as she felt an episode was about to begin and to continue doing it after the symptoms started, with the aim of preventing or stopping the episode. Mariella’s parents were instructed to ensure her safety during the episodes but to allow her to manage the episode independently. A school reintegration plan was made and initiated.
At the second session, Mariella reported the ability to shorten episodes to about eight minutes. The frequency of her functional seizures had reduced. At the third session, she indicated that she was able to prevent episodes before they started, but she reported the occurrence of a new symptom, head jerking. Rolling her head was added as an additional opposing response for this symptom. Motivators were developed as rewards for meeting the goals that she developed for treatment (e.g., returning to school full time). Over sessions 3–5, Mariella’s symptoms continued to decrease. She returned to school full time. During session 6–9 the cognitive behavioural techniques used to manage the functional symptoms were generalized to other situations, helping her to develop skills for managing general life stressors. At one year follow up, Mariella was still doing well.
6.3. Exposure Interventions to Manage Avoidance of Difficult Thoughts, Feelings, and Situations
Vignette: Safia (using mindfulness to sit with difficult feelings and thoughts)
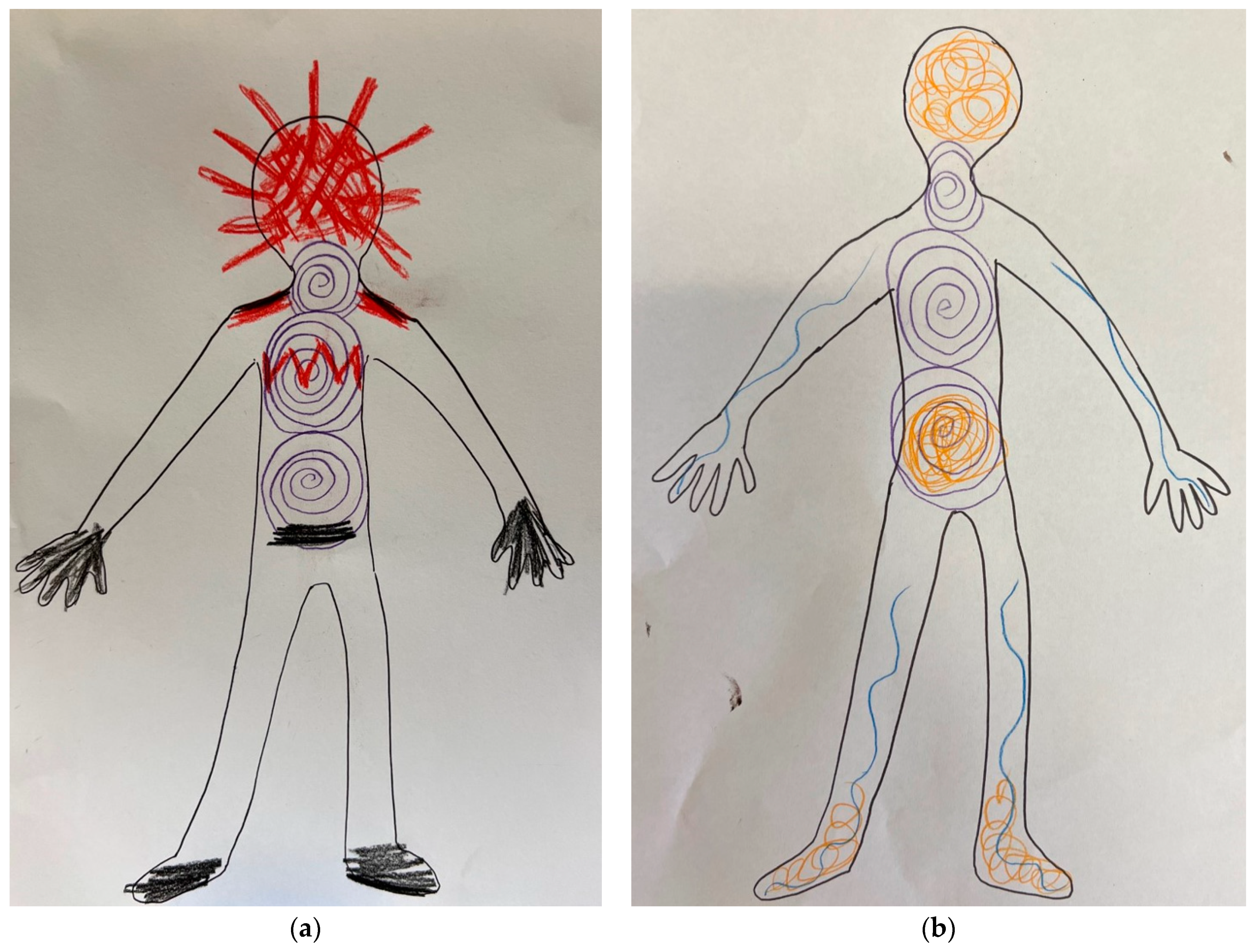
Safia, a 15-year-old girl, started experiencing episodes of sudden twitching and shaking upon return home from school camp, where she had contracted the flu. Safia had great difficulty identifying any warning signs to her functional episodes, often reporting they “came out of nowhere”. She also struggled to identify any of her emotions or thoughts. A number of interventions were implemented to help Safia. A mindful body-scan task was introduced to support Safia to connect with the felt sense of her body and the sensations that she could feel arising and ebbing in her body. A feelings wheel helped Safia identify different feelings. Using coloured pencils, Safia then represented these feelings on a body map. In so doing, she made a link between her feelings and the physiological sense of her body. Finally, a mindfulness task helped Safia to notice her thoughts and feelings as they came into consciousness, to observe them without judgment, and to let them go. With repeated practice, Safia eventually was able build her capacity to notice when her functional twitching and shaking episodes were about to happen. She noticed her triggers included feelings of anger or a negative thought that lingered in her mind, and that her physiological warning signs included an increase in breathing rate, sweaty palms, and a sense of dizziness.
Vignette: Corey (using exposure to widen the social context)
Corey was an 11-year-old boy with severe functional seizures that manifest as violent, full-body jerking that sometimes caused him to catapult out of his bed. Corey had been bed bound for many months. Attempts to widen his social context beyond his bed—to enable discharge from the hospital—were met with anxiety that triggered a functional seizure. The graded exposure hierarchy began with trips to the hospital café, where Corey and his father drank milkshakes and played rounds of uno. Despite Corey repeatedly stating “it won’t work” and “I’ll stuff it up”, the exposure hierarchy was extended to cafés outside the hospital. Eventually, it was taken home by the family and integrated into a very gradual transition plan back to school (starting with driving past the schoolground with his parents).
7. Trauma-Processing Interventions
Vignette: Morgan (use of eye movement desensitization and reprocessing)
Morgan was a 14-year-old female with a history of complex PTSD and anxiety stemming from being exposed to chronic and violent domestic abuse perpetrated by her biological mother’s boyfriend while Morgan was 1–4 years of age. Morgan went to live with her grandmother at age 5. Through the loving and stable environment that her grandmother provided, Morgan thrived. When Morgan was 13, she was at a local bakery with her friends when a song came on the radio that the perpetrator of the domestic violence had often played in the home. Morgan became hypervigilant. She responded with panic attacks to any song on the radio that sounded similar. Two weeks after the event, Morgan started experiencing functional seizures, characterized by prolonged periods of unresponsiveness. As part of her treatment, Morgan engaged in EMDR therapy, alongside other mind–body interventions—to assist in down regulating her stress system (so that the functional seizures could resolve).
Vignette: Deepa (use of radical exposure tapping)
Deepa’s first FND episode (weakness in the legs and ataxic gait) was triggered at 14 years of age by the shock of death. First, her rabbit died, and then a few weeks later, her grandfather. Her second FND episode (leg weakness and functional seizures) at 15 years of age was triggered by her father’s near-death experience on the operating table and ten-day admission to intensive care. Her third FND episode (jaw dystonia and functional seizures) was triggered after the family had visited her grandfather’s grave. Her forth FND episode (jaw dystonia) was triggered when she heard that her father needed another hospital admission for a minor procedure. Deepa and her therapist used RET first with the memories of her rabbit, then her grandfather alive, then her grandfather in his coffin, a visual image of the current grave site, and then memories of Deepa’s father, his stay in intensive care, and his coming home, to process Deepa’s loss and trauma memories.
8. Hypnosis
Vignette: Sammy (using hypnosis as calming strategy)
Sammy, a 13-year-old girl who was very reactive in social situations, would become very angry and distressed when her friends did not respond in a way that she perceived to be supportive. This would then activate her stress system and escalate her functional symptoms. Sammy would then blame her friends for making her sick. Sammy’s therapist used a brief hypnosis session in which Sammy practiced being the “eye of the storm” with emotions and reactions swirling around her. Sammy then practiced bringing up imagery that helped to calm the storm. Sammy also found a smooth pebble she liked holding. She would keep this in her pocket at school and touch it as a way to help her remember to visualize water swirling around her—just like difficult emotions would do. Sammy was subsequently able to access this imagery and the associated feelings of calm when she was triggered by her social setting. She used this interval of calming imagery to settle herself before she acted.
Vignette: Malin (using hypnosis to imagine the past and visualize a new future)
Malin, a 16-year-old girl with paralysis in both legs, had lost all hope for recovering and did not believe that a therapist could be of any help. “You see, my body doesn’t remember how it feels to walk, dance, feel energized, or just be happy.” The therapist used hypnosis to help Malin experience how she could use the power of her imagination in the present to remember the past and to sow a seed in her mind about a positive illness outcome. Guided by the therapist, Malin used her imagination to recall in detail a wonderful situation from the past in which her legs were doing their job all by themselves while she just was happy and had a nice feeling of energy and of control. Malin was amazed by how her mind was able to evoke all the pleasant sensations, emotions, and memories in her body. “I wonder if your mind’s power also can reach out to the future?”—the therapist wondered aloud. Malin was curious, and again, guided by the therapist, she used her imagination to create a wonderful future situation where she was at a marvellous party with her friends, dancing, laughing, and feeling happy—while her strong legs were doing their job all by themselves. This contributed to a shift in Malin’s expectation for the future symptom course and made her more open to therapeutic change and eventual recovery from her FND.
9. Family Interventions That Scaffold the Work with the Child
10. School Interventions That Scaffold the Work with the Child
11. Discussion
12. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Leary, P.M. Conversion disorder in childhood-diagnosed too late, investigated too much. J. R. Soc. Med. 2003, 96, 436–438. [Google Scholar]
- Operto, F.F.; Coppola, G.; Mazza, R.; Pastorino, G.M.G.; Campanozzi, S.; Margari, L.; Roccella, M.; Marotta, R.; Carotenuto, M. Psychogenic nonepileptic seizures in pediatric population: A review. Brain Behav. 2019, 9, e01406. [Google Scholar] [CrossRef] [PubMed]
- Jungilligens, J.; Michaelis, R.; Popkirov, S. Misdiagnosis of prolonged psychogenic non-epileptic seizures as status epilepticus: Epidemiology and associated risks. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1341–1345. [Google Scholar] [CrossRef]
- Yong, K.; Chin, R.F.M.; Shetty, J.; Hogg, K.; Burgess, K.; Lindsay, M.; McLellan, A.; Stone, J.; KamathTallur, K.; The Edinburgh Paediatric FND Study Group. Functional neurological disorder in children and young people: Incidence, clinical features, and prognosis. Dev. Med. Child Neurol. 2023, 65, 1238–1246. [Google Scholar] [CrossRef] [PubMed]
- Intergovernmental Panel on Climate Change (IPCC). Climate Change 2021: The Physical Science Basis; Intergovernmental Panel on Climate Change (IPCC): Geneva, Switzerland, 2021. [Google Scholar]
- Samji, H.; Wu, J.; Ladak, A.; Vossen, C.; Stewart, E.; Dove, N.; Long, D.; Snell, G. Review: Mental health impacts of the COVID-19 pandemic on children and youth—A systematic review. Child Adolesc. Ment. Health 2022, 27, 173–189. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Youth Risk Behavior Survey. Data Summary and Trends Report. 2023. Available online: https://www.cdc.gov/healthyyouth/data/yrbs/pdf/YRBS_Data-Summary-Trends_Report2023_508.pdf (accessed on 18 February 2023).
- Heyman, I.; Liang, H.; Hedderly, T. COVID-19 related increase in childhood tics and tic-like attacks. Arch. Dis. Child. 2021, 106, 420–421. [Google Scholar] [CrossRef]
- Hull, M.; Parnes, M. Tics and TikTok: Functional Tics Spread Through Social Media. Mov. Disord. Clin. Pract. 2021, 8, 1248–1252. [Google Scholar] [CrossRef]
- Pringsheim, T.; Ganos, C.; McGuire, J.F.; Hedderly, T.; Woods, D.; Gilbert, D.L.; Piacentini, J.; Dale, R.C.; Martino, D. Rapid Onset Functional Tic-like Behaviors in Young Females during the COVID-19 Pandemic. Mov. Disord. 2021, 36, 2707–2713. [Google Scholar] [CrossRef] [PubMed]
- Pringsheim, T.; Martino, D. Rapid onset of functional tic-like behaviours in young adults during the COVID-19 pandemic. Eur. J. Neurol. 2021, 28, 3805–3808. [Google Scholar] [CrossRef] [PubMed]
- Buts, S.; Duncan, M.; Owen, T.; Martino, D.; Pringsheim, T.; Byrne, S.; McWilliams, A.; Murphy, T.; Malik, O.; Liang, H.; et al. Paediatric tic-like presentations during the COVID-19 pandemic. Arch. Dis. Child. 2022, 107, e17. [Google Scholar] [CrossRef]
- Muller-Vahl, K.R.; Pisarenko, A.; Jakubovski, E.; Fremer, C. Stop that! It’s not Tourette’s but a new type of mass sociogenic illness. Brain 2022, 145, 476–480. [Google Scholar] [CrossRef]
- Paulus, T.; Baumer, T.; Verrel, J.; Weissbach, A.; Roessner, V.; Beste, C.; Munchau, A. Pandemic Tic-like Behaviors Following Social Media Consumption. Mov. Disord. 2021, 36, 2932–2935. [Google Scholar] [CrossRef] [PubMed]
- Han, V.X.; Kozlowska, K.; Kothur, K.; Lorentzos, M.; Wong, W.K.; Mohammad, S.S.; Savage, B.; Chudleigh, C.; Dale, R.C. Rapid onset functional tic-like behaviours in children and adolescents during COVID-19: Clinical features, assessment and biopsychosocial treatment approach. J. Paediatr. Child Health 2022, 58, 1181–1187. [Google Scholar] [CrossRef] [PubMed]
- Nilles, C.; Pringsheim, T.M.; Martino, D. The recent surge of functional movement disorders: Social distress or greater awareness? Curr. Opin. Neurol. 2022, 35, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Martino, D.; Hedderly, T.; Murphy, T.; Muller-Vahl, K.R.; Dale, R.C.; Gilbert, D.L.; Rizzo, R.; Hartmann, A.; Nagy, P.; Anheim, M.; et al. The spectrum of functional tic-like behaviours: Data from an international registry. Eur. J. Neurol. 2023, 30, 334–343. [Google Scholar] [CrossRef]
- Martindale, J.M.; Mink, J.W. The Rise of Functional Tic-like Behaviors: What Do the COVID-19 Pandemic and Social Media Have to Do With It? A Narrative Review. Front. Pediatr. 2022, 10, 863919. [Google Scholar] [CrossRef] [PubMed]
- Kozlowska, K.; Scher, S.; Helgeland, H. Functional Somatic Symptoms in Children and Adolescents: A Stress-System Approach to Assessment and Treatment; Palgrave Macmillan: London, UK, 2020. [Google Scholar]
- Savage, B.; Chudleigh, C.; Hawkes, C.; Scher, S.; Kozlowska, K. Treatment of Functional Seizures in Children and Adolescents: A Mind-Body Manual for Health Professionals; Australian Academic Press: Samford, Australia, 2022. [Google Scholar]
- APA Dictionary of Psychology. Thinking. Available online: https://dictionary.apa.org/thinking (accessed on 12 August 2023).
- Pace-Schott, E.F.; Amole, M.C.; Aue, T.; Balconi, M.; Bylsma, L.M.; Critchley, H.; Demaree, H.A.; Friedman, B.H.; Gooding, A.E.K.; Gosseries, O.; et al. Physiological Feelings. Neurosci. Biobehav. Rev. 2019, 103, 267–304. [Google Scholar] [CrossRef]
- Damasio, A.R. Of appetites and emotions. In Looking for Spinoza: Joy, Sorrow, and the Feeling Brain; Harcourt: Orlando, FL, USA, 2003; pp. 27–80. [Google Scholar]
- Edwards, M.J.; Adams, R.A.; Brown, H.; Parees, I.; Friston, K.J. A Bayesian account of ‘hysteria’. Brain 2012, 135, 3495–3512. [Google Scholar] [CrossRef]
- Gianaros, P.J.; Wager, T.D. Brain-Body Pathways Linking Psychological Stress and Physical Health. Curr. Dir. Psychol. Sci. 2015, 24, 313–321. [Google Scholar] [CrossRef]
- Barrett, L.F. The theory of constructed emotion: An active inference account of interoception and categorization. Soc. Cogn. Affect. Neurosci. 2017, 12, 1833. [Google Scholar] [CrossRef]
- Jungilligens, J.; Paredes-Echeverri, S.; Popkirov, S.; Barrett, L.F.; Perez, D.L. A new science of emotion: Implications for functional neurological disorder. Brain 2022, 145, 2648–2663. [Google Scholar] [CrossRef] [PubMed]
- Kozlowska, K.; Nunn, K.P.; Rose, D.; Morris, A.; Ouvrier, R.A.; Varghese, J. Conversion disorder in Australian pediatric practice. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Ani, C.; Reading, R.; Lynn, R.; Forlee, S.; Garralda, E. Incidence and 12-month outcome of non-transient childhood conversion disorder in the UK and Ireland. Br. J. Psychiatry 2013, 202, 413–418. [Google Scholar] [CrossRef]
- Sigurdardottir, K.R.; Olafsson, E. Incidence of psychogenic seizures in adults: A population-based study in Iceland. Epilepsia 1998, 39, 749–752. [Google Scholar] [CrossRef]
- Hansen, A.S.; Rask, C.U.; Rodrigo-Domingo, M.; Pristed, S.G.; Christensen, J.; Nielsen, R.E. Incidence rates and characteristics of pediatric onset psychogenic nonepileptic seizures. Pediatr. Res. 2020, 88, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.S.; Rask, C.U.; Christensen, A.E.; Rodrigo-Domingo, M.; Christensen, J.; Nielsen, R.E. Psychiatric Disorders in Children and Adolescents With Psychogenic Nonepileptic Seizures. Neurology 2021, 97, e464–e475. [Google Scholar] [CrossRef]
- Shephard, B. A War of Nerves: Soldiers and Psychiatrists in the Twentieth Century; Harvard University Press: Cambridge, MA, USA, 2001. [Google Scholar]
- Kardiner, A. The Traumatic Neuroses of War; National Research Council: Washington, DC, USA, 1941. [Google Scholar]
- Kardiner, A. War Stress and Neurotic Illness; Hoeber: Edinburgh, UK, 1947. [Google Scholar]
- Kozlowska, K. Stress, Distress, and Bodytalk: Co-constructing Formulations with Patients Who Present with Somatic Symptoms. Harv. Rev. Psychiatry 2013, 21, 314–333. [Google Scholar] [CrossRef]
- Kozlowska, K. A stress-system model for functional neurological symptoms. J. Neurol. Sci. 2017, 383, 151–152. [Google Scholar] [CrossRef]
- Chung, J.; Mukerji, S.; Kozlowska, K. Cortisol and alpha-amylase awakening response in children and adolescents with functional neurological (conversion) disorder. Aust. N. Z. J. Psychiatry 2022, 57, 115–129. [Google Scholar] [CrossRef]
- Rai, S.; Foster, S.; Griffiths, K.R.; Breukelaar, I.A.; Kozlowska, K.; Korgaonkar, M.S. Altered resting-state neural networks in children and adolescents with functional neurological disorder. Neuroimage Clin 2022, 35, 103110. [Google Scholar] [CrossRef]
- Pick, S.; Goldstein, L.H.; Perez, D.L.; Nicholson, T.R. Emotional processing in functional neurological disorder: A review, biopsychosocial model and research agenda. J. Neurol. Neurosurg. Psychiatry 2019, 90, 704–711. [Google Scholar] [CrossRef]
- Sharma, A.A.; Szaflarski, J.P. Neuroinflammation as a pathophysiological factor in the development and maintenance of functional seizures: A hypothesis. Epilepsy Behav. Rep. 2021, 16, 100496. [Google Scholar] [CrossRef] [PubMed]
- Paredes-Echeverri, S.; Maggio, J.; Begue, I.; Pick, S.; Nicholson, T.R.; Perez, D.L. Autonomic, Endocrine, and Inflammation Profiles in Functional Neurological Disorder: A Systematic Review and Meta-Analysis. J. Neuropsychiatry Clin. Neurosci. 2022, 34, 30–43. [Google Scholar] [CrossRef]
- Weber, S.; Buhler, J.; Vanini, G.; Loukas, S.; Bruckmaier, R.; Aybek, S. Identification of biopsychological trait markers in functional neurological disorders. Brain 2022, 146, 2627–2641. [Google Scholar] [CrossRef] [PubMed]
- Tsigos, C.; Stefanaki, C.; Lambrou, G.I.; Boschiero, D.; Chrousos, G.P. Stress and inflammatory biomarkers and symptoms are associated with bioimpedance measures. Eur. J. Clin. Investig. 2015, 45, 126–134. [Google Scholar] [CrossRef]
- Sterling, P.; Eyer, J. Allostatis: A new paradigm to explain arousal pathology. In Handbook of Life Stress, Cognition and Health; Fisher, S., Reason, J., Eds.; Wiley: Chichester, UK, 1988; pp. 629–649. [Google Scholar]
- Kleckner, I.R.; Zhang, J.; Touroutoglou, A.; Chanes, L.; Xia, C.; Simmons, W.K.; Quigley, K.S.; Dickerson, B.C.; Barrett, L.F. Evidence for a Large-Scale Brain System Supporting Allostasis and Interoception in Humans. Nat. Hum. Behav. 2017, 1, 0069. [Google Scholar] [CrossRef] [PubMed]
- Bernard, C. An Introduction to the Study of Experimental Medicine; Dover Publications: New York, NY, USA, 1957. First published 1865. [Google Scholar]
- Chrousos, G.P.; Loriaux, D.L.; Gold, P.W. (Eds.) Preface. In Mechanisms of Physical and Emotional Stress; Advances in Experimental Medicine and Biology; Plenum Press: New York, NY, USA, 1988; Volume 245, pp. vii–viii. [Google Scholar]
- McCraty, R.; Childre, D. Coherence: Bridging personal, social, and global health. Altern. Ther. Health Med. 2010, 16, 10–24. [Google Scholar]
- McCraty, R.; Zayas, M.A. Cardiac coherence, self-regulation, autonomic stability, and psychosocial well-being. Front. Psychol. 2014, 5, 1090. [Google Scholar] [CrossRef]
- Edwards, M.J.; Fotopoulou, A.; Parees, I. Neurobiology of functional (psychogenic) movement disorders. Curr. Opin. Neurol. 2013, 26, 442–447. [Google Scholar] [CrossRef]
- Carson, A.; Lehn, A.; Ludwig, L.; Stone, J. Explaining functional disorders in the neurology clinic: A photo story. Pract. Neurol. 2015, 16, 56–61. [Google Scholar] [CrossRef]
- Stone, J. Functional neurological disorders: The neurological assessment as treatment. Pract. Neurol. 2016, 16, 7–17. [Google Scholar] [CrossRef]
- Kozlowska, K.; Mohammad, S. Functional neurological disorder in children and adolescents: Assessment and Treatment. In Symptom Based Approach to Pediatric Neurology; Sivaswamy, L., Kamat, D., Eds.; Springer Nature: Cham, Switzerland, 2022; pp. 683–724. [Google Scholar] [CrossRef]
- Aybek, S.; Perez, D.L. Diagnosis and management of functional neurological disorder. BMJ 2022, 376, o64. [Google Scholar] [CrossRef] [PubMed]
- Kozlowska, K.; Scher, S.; Williams, L.M. Patterns of emotional-cognitive functioning in pediatric conversion patients: Implications for the conceptualization of conversion disorders. Psychosom. Med. 2011, 73, 775–788. [Google Scholar] [CrossRef]
- Crittenden, P.M.; Landini, A. Assessing Adult Attachment: A Dynamic-Maturational Approach to Discourse Analysis; Norton: New York, NY, USA, 2011. [Google Scholar]
- Crittenden, P.M. School-aged assessment of attachment. Coding manual using the dynamic maturational method. Unpublished manuscript. Available from the author. 1995. [Google Scholar]
- Crittenden, P.M. Transition to Adulthood Attachment Interview. Miami, FL, USA. 2005; unpublished manuscript. [Google Scholar]
- Crittenden, P.M. Attachment theory, information processing, and psychiatric disorder. World J. Psychiatry 2002, 1, 72–75. [Google Scholar]
- Crittenden, P.M.; Heller, M.B. The Roots of Chronic Posttraumatic Stress Disorder: Childhood Trauma, Information Processing, and Self-protective Strategies. Chronic Stress 2017, 1, 2470547016682965. [Google Scholar] [CrossRef] [PubMed]
- Sawchuk, T.; Buchhalter, J. Psychogenic nonepileptic seizures in children—Psychological presentation, treatment, and short-term outcomes. Epilepsy Behav. 2015, 52, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Sawchuk, T.; Buchhalter, J.; Senft, B. Psychogenic nonepileptic seizures in children-Prospective validation of a clinical care pathway & risk factors for treatment outcome. Epilepsy Behav. 2020, 105, 106971. [Google Scholar] [CrossRef]
- Stager, L.; Morriss, S.; Szaflarski, J.P.; Fobian, A.D. Psychiatric and personality factors in pediatric functional seizures: A prospective case-control study. Seizure 2022, 98, 105–112. [Google Scholar] [CrossRef]
- Kozlowska, K.; Cruz, C.; Davies, F.; Brown, K.; Palmer, D.M.; McLean, L.; Scher, S.; Willams, L.M. The Utility (or Not) of Self-Report Instruments in Family Assessment for Child and Adolescent Conversion Disorders? Aust. N. Z. J. Fam. Ther. 2016, 37, 480–499. [Google Scholar] [CrossRef]
- Radmanesh, M.; Jalili, M.; Kozlowska, K. Activation of Functional Brain Networks in Children and Adolescents with Psychogenic Non-epileptic Seizures. Front. Hum. Neurosci. 2020, 14, 339. [Google Scholar] [CrossRef]
- Fobian, A.D.; Long, D.M.; Szaflarski, J.P. Retraining and control therapy for pediatric psychogenic non-epileptic seizures. Ann. Clin. Transl. Neurol. 2020, 7, 1410–1419. [Google Scholar] [CrossRef] [PubMed]
- Fobian, A.D.; Szaflarski, J.P. Identifying and evaluating novel treatment targets for the development of evidence-based interventions for Functional Neurological Disorder. Epilepsy Behav. Rep. 2021, 16, 100479. [Google Scholar] [CrossRef]
- Stager, L.; Morriss, S.; McKibben, L.; Grant, M.; Szaflarski, J.P.; Fobian, A.D. Sense of control, selective attention and cognitive inhibition in pediatric functional seizures: A prospective case-control study. Seizure 2022, 98, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Stager, L.; Szaflarski, J.P.; Fobian, A.D. One-year follow-up of treatment outcomes and patient opinions of Retraining and Control Therapy (ReACT) for pediatric functional seizures. Epilepsy Behav. Rep. 2021, 16, 100503. [Google Scholar] [CrossRef]
- Stager, L.; Mueller, C.; Morriss, S.; Szaflarski, J.P.; Fobian, A.D. Sense of control, selective attention, cognitive inhibition, and psychosocial outcomes after Retraining and Control Therapy (ReACT) in pediatric functional seizures. Epilepsy Behav. 2023, 142, 109143. [Google Scholar] [CrossRef]
- Kozlowska, K.; Chudleigh, C.; Savage, B.; Hawkes, C.; Scher, S.; Nunn, K.P. Evidence-Based Mind-Body Interventions for Children and Adolescents with Functional Neurological Disorder. Harv. Rev. Psychiatry 2023, 31, 60–82. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 4th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scale; The Psychological Foundation of Australia, Inc.: Sydney, Australia, 1995. [Google Scholar]
- Patrick, J.; Dyck, M.; Bramston, P. Depression anxiety stress scale: Is it valid for children and adolescents? J. Clin. Psychol. 2010, 66, 996–1007. [Google Scholar] [CrossRef]
- Cohen, R.A.; Hitsman, B.L.; Paul, R.H.; McCaffery, J.; Stroud, L.; Sweet, L.; Gunstad, J.; Niaura, R.; MacFarlane, A.; Bryant, R.A.; et al. Early life stress and adult emotional experience: An international perspective. Int. J. Psychiatry Med. 2006, 36, 35–52. [Google Scholar] [CrossRef]
- Kozlowska, K.; Sawchuk, T.; Waugh, J.L.; Helgeland, H.; Baker, J.; Scher, S.; Fobian, A. Changing the Culture of Care for Children and Adolescents with Functional Neurological Disorder. Epilepsy Behav. Rep. 2021, 16, 1004486. [Google Scholar] [CrossRef]
- Helgeland, H.; Gjone, I.H.; Diseth, T.H. The biopsychosocial board—A conversation tool for broad diagnostic assessment and identification of effective treatment of children with functional somatic disorders. Hum. Syst. 2022, 2, 144–157. [Google Scholar] [CrossRef]
- Førde, S.; Herner, L.B.; Helland, I.B.; Diseth, T.H. The biopsychosocial model in paediatric clinical practice-An interdisciplinary approach to somatic symptom disorders. Acta Paediatr. 2022, 111, 2115–2124. [Google Scholar] [CrossRef]
- Benedetti, F. The Patient’s Brain; Oxford University Press: Oxford, UK, 2011. [Google Scholar]
- Kabat-Zinn, J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: Theoretical considerations and preliminary results. Gen. Hosp. Psychiatry 1982, 4, 33–47. [Google Scholar] [CrossRef]
- Kain, K.L.; Terrell, S.J. Nurturing Resilience: Helping Clients Move forward from Developmental Trauma: An Integrative Somatic Approach; North Atlantic Books: Berkeley, CA, USA, 2018. [Google Scholar]
- Ogden, P.; Fisher, J. Sensorimotor Psychotherapy. Interventions for Trauma and Attachment; Norton: New York, NY, USA, 2015. [Google Scholar]
- Levine, P. Waking the Tiger: Healing Trauma; North Atlantic Books: Berkeley, CA, USA, 1997. [Google Scholar]
- Gray, N.; Savage, B.; Scher, S.; Kozlowska, K. Psychologically Informed Physical Therapy for Children and Adolescents With Functional Neurological Symptoms: The Wellness Approach. J. Neuropsychiatry Clin. Neurosci. 2020, 32, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.N.; Gray, N.; Jones, A.; Scher, S.; Kozlowska, K. The Role of Physiotherapy in the Management of Functional Neurological Disorder in Children and Adolescents. Semin. Pediatr. Neurol. 2022, 41, 100947. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C. Acceptance and commitment therapy, relational frame theory, and the third wave of behavioral and cognitive therapies. Behav. Ther. 2004, 35, 639–665. [Google Scholar] [CrossRef]
- Brown, L.A.; Gaudiano, B.A.; Miller, I.W. Investigating the similarities and differences between practitioners of second- and third-wave cognitive-behavioral therapies. Behav. Modif. 2011, 35, 187–200. [Google Scholar] [CrossRef]
- Hayes, S.C.; Hofmann, S.G. Process-Based CBT: The Science and Core Clinical Competencies of Cognitive Behavioral Therapy; Context Press: Oakland, CA, USA, 2018. [Google Scholar]
- Kozlowska, K.; Chudleigh, C.; Cruz, C.; Lim, M.; McClure, G.; Savage, B.; Shah, U.; Cook, A.; Scher, S.; Carrive, P.; et al. Psychogenic non-epileptic seizures in children and adolescents: Part II—Explanations to families, treatment, and group outcomes. Clin. Child Psychol. Psychiatry 2018, 23, 160–176. [Google Scholar] [CrossRef]
- Vassilopoulos, A.; Mohammad, S.; Dure, L.; Kozlowska, K.; Fobian, A.D. Treatment Approaches for Functional Neurological Disorders in Children. Curr. Treat. Options Neurol. 2022, 24, 77–97. [Google Scholar] [CrossRef]
- Arnsten, A.F. Stress weakens prefrontal networks: Molecular insults to higher cognition. Nat. Neurosci. 2015, 18, 1376–1385. [Google Scholar] [CrossRef]
- Rathus, J.H.; Miller, A.L. Dialectical behavior therapy adapted for suicidal adolescents. Suicide Life Threat. Behav. 2002, 32, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Linehan, M.M. Cognitive-Behavioral Treatment of Borderline Personality Disorder; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Minuchin, S. Families and Family Therapy; Harvard University Press: Cambridge, MA, USA, 1974. [Google Scholar]
- Lappin, J. Family Therapy: A Structural Approach. In Paradigms of Clinical Social Work; Dorfman, R.A., Ed.; Brunner/Maze: New York, NY, USA, 1988; pp. 220–252. [Google Scholar]
- Engel, G.L.; Ferris, E.B.; Logan, M. Hyperventilation: Analysis of clinical symptomatology. Ann. Intern. Med. 1947, 27, 683–704. [Google Scholar] [PubMed]
- Lum, L.C. Hyperventilation: The tip and the iceberg. J. Psychosom. Res. 1975, 19, 375–383. [Google Scholar] [CrossRef]
- Huffman, J.C.; Pollack, M.H.; Stern, T.A. Panic Disorder and Chest Pain: Mechanisms, Morbidity, and Management. Prim. Care Companion J. Clin. Psychiatry 2002, 4, 54–62. [Google Scholar] [CrossRef]
- Kozlowska, K.; Rampersad, R.; Cruz, C.; Shah, U.; Chudleigh, C.; Soe, S.; Gill, D.; Scher, S.; Carrive, P. The respiratory control of carbon dioxide in children and adolescents referred for treatment of psychogenic non-epileptic seizures. Eur. Child Adolesc. Psychiatry 2017, 26, 1207–1217. [Google Scholar] [CrossRef] [PubMed]
- Sawchuk, T.; Buchhalter, J.; Senft, B. Psychogenic non-epileptic seizures in children—Psychophysiology & dissociative characteristics. Psychiatry Res. 2020, 294, 113544. [Google Scholar] [CrossRef] [PubMed]
- Raissouni, M.; Benhammou, S.; Belbachir, S. The place of EMDR in children: A review of the literature. Eur. Psychiatry 2023, 66, S734. [Google Scholar] [CrossRef]
- Burkhart, K.; Agarwal, N.; Kim, S.; Neudecker, M.; Ievers-Landis, C.E. A Scoping Review of Trauma-Informed Pediatric Interventions in Response to Natural and Biologic Disasters. Children 2023, 10, 1017. [Google Scholar] [CrossRef]
- MacKinnon, L. Deactivating the Buttons: Integrating Radical Exposure Tapping with a Family Therapy Framework. Aust. N. Z. J. Fam. Ther. 2014, 35, 244–260. [Google Scholar] [CrossRef]
- Waits, W.; Marumoto, M.; Weaver, J. Accelerated Resolution Therapy (ART): A Review and Research to Date. Curr. Psychiatry Rep. 2017, 19, 18. [Google Scholar] [CrossRef]
- Terhune, D.B.; Cleeremans, A.; Raz, A.; Lynn, S.J. Hypnosis and top-down regulation of consciousness. Neurosci. Biobehav. Rev. 2017, 81, 59–74. [Google Scholar] [CrossRef]
- Yapko, M.D. Trancework. An Introduction to the Practice of Clinical Hypnosis, 5th ed.; Routledge: New York, NY, USA, 2019. [Google Scholar]
- Helgeland, H.; Savage, B.; Kozlowska, K. Hypnosis in the Treatment of Functional Somatic Symptoms in Children and Adolescents. In The Routledge International Handbook of Clinical Hypnosis; Linden, J.H., De Benedittis, G., Sugarman, L.I., Varga, K., Eds.; Routledge Taylor & Francis: Oxfordshire, UK, forthcoming.
- Eisenberger, N.I.; Lieberman, M.D.; Williams, K.D. Does rejection hurt? An FMRI study of social exclusion. Science 2003, 302, 290–292. [Google Scholar] [CrossRef] [PubMed]
- Eisenberger, N.I.; Lieberman, M.D. Why rejection hurts: A common neural alarm system for physical and social pain. Trends Cogn. Sci. 2004, 8, 294–300. [Google Scholar] [CrossRef]
- Dermendzhiyskais, E. Rejection Kills. The Brain Makes No Distinction between a Broken Bone and an Aching Heart. That’s Why Social Exclusion Needs a Health Warning. Aeon. 2019. Available online: https://aeon.co/essays/health-warning-social-rejection-doesnt-only-hurt-it-kills (accessed on 30 April 2019).
- Kozlowska, K.; Spooner, C.J.; Palmer, D.M.; Harris, A.; Korgaonkar, M.S.; Scher, S.; Williams, L.M. “Motoring in idle”: The default mode and somatomotor networks are overactive in children and adolescents with functional neurological symptoms. Neuroimage Clin 2018, 18, 730–743. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.D.; Azzi, M.; White, S.; Salter, D.; Trieu, T.; Morgan, G.; Rahman, M.; Watt, S.; Riley, M.; Chang, L.T.; et al. The Summer 2019-2020 Wildfires in East Coast Australia and Their Impacts on Air Quality and Health in New South Wales, Australia. Int. J. Environ. Res. Public Health 2021, 18, 3538. [Google Scholar] [CrossRef]
- Audit Office of New South Wales. Natural Disasters (1 June 2023). 2023. Available online: https://www.audit.nsw.gov.au/our-work/reports/natural-disasters (accessed on 11 August 2023).
- Diez, I.; Larson, A.G.; Nakhate, V.; Dunn, E.C.; Fricchione, G.L.; Nicholson, T.R.; Sepulcre, J.; Perez, D.L. Early-life trauma endophenotypes and brain circuit-gene expression relationships in functional neurological (conversion) disorder. Mol. Psychiatry 2020, 26, 3817–3828. [Google Scholar] [CrossRef]
- Felitti, V.J. Adverse childhood experiences and adult health. Acad. Pediatr. 2009, 9, 131–132. [Google Scholar] [CrossRef] [PubMed]
- Hertzman, C. The biological embedding of early experience and its effects on health in adulthood. Ann. N. Y. Acad. Sci. 1999, 896, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Perez, D.L.; Edwards, M.J.; Nielsen, G.; Kozlowska, K.; Hallett, M.; LaFrance, W.C., Jr. Decade of progress in motor functional neurological disorder: Continuing the momentum. J. Neurol. Neurosurg. Psychiatry 2021, 16, 668–677. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measure | Description |
|---|---|
| RAHC-GAF | The Royal Alexandra Hospital for Children Global Assessment of Function is the DSM-IV-TR Global Assessment of Functioning modified to include functional impairment secondary to physical illness [74]. The scale has 100 points and 10 categories (10 points each). Healthy controls fall into the upper two brackets “superior in all areas” (score 91−100) or “good in all areas” (score 81−90). Lower values (and brackets) mark functional impairment of increasing severity. Patients with physical or psychological impairment fall into the lower brackets (score < 81). |
| DASS-21 | The Depression Anxiety and Stress Scales are a validated measure of perceived distress in paediatric populations [75,76]. |
| ELSQ | The Early Life Stress Questionnaire is a checklist of 19 stress items—and an option for elaboration—based on the Child Abuse and Trauma Scale [77]. Twelve of the items pertain to relational stressors: bullying, physical abuse, sexual abuse, emotional abuse, neglect, parental separation, loss by separation, loss by death, family conflict, severe illness of a family member, domestic violence, and other. Other items pertain to birth complications, life-threatening/severe illness, war trauma, and natural disasters. Participants record if they have or have not experienced the given stressor and the age period during which the stressor has been experienced. |
| Comorbid Medical Conditions | ||
| Any comorbid medical condition a | 30 | 39.5% |
| 8 | 10.5% |
| 7 | 9.2% |
| 5 | 6.6% |
| 3 | 3.9% |
| 2 | 2.6% |
| 2 | 7.6% |
| 2 | 7.6% |
| 8 | 10.1% |
| Comorbid Functional Syndromes | ||
| Any complex (functional) pain | 51 | 67.1% |
| 26 | 34.2% |
| 14 | 18.2.0% |
| 12 | 15.8% |
| 12 | 15.8% |
| 6 | 7.9% |
| Any comorbid functional syndrome (excluding pain) | 23 | 30.3.8% |
| 18 | 23.7% |
| 8 | 10.5% |
| 2 | 2.6% |
| Comorbid Nonspecific Somatic Symptoms | ||
| Any comorbid nonspecific somatic symptom | 68 | 89.5% |
| 42 | 55.3% |
| 41 | 53.9% |
| 36 | 47.4% |
| 29 | 38.2% |
| 22 | 28.9% |
| 18 | 23.7% |
| Comorbid Nonspecific Symptoms Other | ||
| Sleep (difficulties falling asleep, waking, unrefreshing sleep) | 61 | 80.3% |
| Concentration difficulties | 52 | 68.4% |
| Comorbid Mental Health Disorders And Symptoms | ||
| Any mental health disorder (DSM-5) | 66 | 86.8% |
| 61 | 80.3% |
| 33 | 43.4% |
| 10 | 13.2% |
| 5 | 6.6% |
| 8 | 10.5% |
| 7 | 9.2% |
| 1 | 1.3% |
| Common Adverse Childhood Experiences (ACEs) Reported by the Child and Family (Maltreatment-Related Events Are Denoted by an Asterisk) | ||
| One or more ACEs (range = 1–12; mean = 5.79; median = 6.00) | 76 | 100% |
| 47 | 61.8% |
| 41 | 53.9% |
| 36 | 47.4% |
| 33 | 43.4% |
| 26 | 34.2% |
| 25 | 32.9% |
| 20 | 26.3% |
| 17 | 22.4% |
| 16 | 21.1% |
| 15 | 19.7% |
| 17 | 22.4% |
| 11 | 14.5% |
| 7 | 9.2% |
| 7 | 9.2% |
| 5 | 6.6% |
| 5 | 6.6% |
| 3 | 3.9% |
| Socioeconomic Status of the Family | ||
| Professional | 5 | 6.6% |
| White collar | 18 | 23.7% |
| Blue collar | 25 | 32.9% |
| Unemployed | 2 | 6.5% |
| Family Constellation | ||
| Biological parents | 47 | 61.8% |
| Blended family | 25 | 32.9% |
| Lives with one parent (single mother in these cases) | 3 | 3.9% |
| Foster care | 1 | 1.3% |
| Intelligence Quota Estimated from School Reports (or Formal Testing) | ||
| Superior range (120+) | 20 | 26.3% |
| Average range (80−119) | 44 | 57.9% |
| Borderline range (70−79) | 9 | 11.8% |
| Delayed (<70) | 3 | 3.9% |
| Measure | FND Group (n = 76): a Mean Value/Total Score (Range) | Healthy-Control Group (n = 47): Mean Value/Total Score (Range) | t/χ2 (p) |
|---|---|---|---|
| GAF | 32.04 (10–51) | 89.66 (75–99) | −42.40 (<0.001) |
| DASS-21 Total Score | 26.82 (2–52) | 5.68 0–30 | 12.18 (<0.001) |
| ELSQ | 3.64 (0–10) | 0.51 (0–3) | 9.38 (<0.001) |
| Item (19 Items) | Number (n = 73) | Percentage |
|---|---|---|
| Prematurity/birth complications | 21 | 27.6 |
| Adopted | 0 | 0 |
| Major surgery or repeated hospitalization | 20 | 26.3 |
| Life-threatening illness/injury (self) | 5 | 6.6 |
| Sustained bullying of rejection by school mates | 41 | 53.9 |
| Physical abuse | 11 | 14.5 |
| Sexual abuse | 6 | 7.9 |
| Emotional abuse | 20 | 26.3 |
| Extreme poverty | 4 | 5.3 |
| Witness natural disaster first-hand | 15 | 19.7 |
| House destroyed by fire or other means | 5 | 6.6 |
| Witness warfare | 0 | 0 |
| Parents divorced or separated | 27 | 35.5 |
| Separated long time from a parent, brother, or sister | 12 | 15.8 |
| Sustained conflict within family | 23 | 30.3 |
| Death of a parent, brother, or sister | 7 | 9.2 |
| Life-threatening illness (parents, brother, or sister) | 10 | 13.2 |
| Witness domestic violence in family | 14 | 18.4 |
| Witness of experience some other traumatic event | 25 | 32.9 |
| Psychological Process | Explanation/Example of the Psychological Process | Number (%) (n = 76) |
|---|---|---|
| Attentional processes | ||
| Attention to symptoms | Attention to symptoms—by the child or the parents—worsens FND symptoms and amplifies pain. | 61 (80.3%) |
| Cognitive processes and expectations (a subset relates to symptoms and treatment, and a subset to the self or other situations) | ||
| Negative/catastrophic a-symptom expectations | Thoughts about the symptom lead to a negative or catastrophic outcome. For example, in response to a muscle spasm and a new pattern of pain in the back—in a boy with motor weakness in the legs and left arm—thinking over and over again, “What is wrong now? How bad is it going to get?” coupled with a visual image of his body being completely paralyzed. | 40 (52.6%) |
| Low sense of control (predictability) over symptoms | Thoughts—coupled with feelings of helplessness—that highlight the child perceived lack of control. For example, “It just happens out of the blue.” or “There is nothing I can do.” | 44 (57.9%) |
| Negative expectations pertaining to treatment interventions | Negative expectations (nocebo effect) are set up in the context of catastrophic-symptom expectations and thoughts/feelings associated with a low sense of control. Negative expectations can undermine the efficacy of strategies that the child needs to learn to manage the symptoms. | 30 (39.5%) |
| Low sense of control (and predictability) with regard to events or expectations in the home or school setting | Thoughts that underline the child’s perceived lack of control. For example, “It’s too hard. I can’t do it. I hate school. They all think I am stupid.”—coupled with feelings of helplessness. | 26 (34.2%) |
| Catastrophic thinking (pertaining to self [symptoms excluded]) | “If I don’t get everything right now (in the upcoming test), I’ll never be able to become a surgeon.” | 33 (43.4%) |
| Catastrophic thinking (pertaining to non-self) | For example, ruminating thoughts about the ecological stress that the earth is under, as in “When the glacier melts, we shall have no water, and we shall all die.” | 27 (35.5%) |
| Perfectionistic thinking | For example, “I did not reply to my brother’s text because I could not get my text right.” or “I only got 98% in the math exam” (associated with a feeling of disappointment and sadness). | 27 (35.5%) |
| Self-critical rumination b | Beating oneself up over what one could or should have done. For example, when a child with FND says, “I haven’t tried hard enough. It is my fault I am in hospital. I should have tried harder and done better.” or “The money my parents are spending on my treatment means my family is missing out.” | 42 (55.3%) |
| Obsessive thinking | Unable to switch thought processes away from a certain idea or worry. For example, an adolescent girl with FND was obsessed with the accuracy of her diagnosis. Each morning at ward rounds she grilled her team about her diagnosis, including the pros and cons of formally including other diagnoses on her chart: fibromyalgia, postural orthostatic tachycardia syndrome, complex/chronic pain, irritable bowel syndrome, and so on. | 34 (44.7%) |
| An exclusively negative focus regarding the future, coupled with the inability to be in the present and to celebrate progress in the here and now | For example, an adolescent girl who had presented with leg paralysis, cognitive impairment, and functional seizures complained that everything was getting worse, that her occasional drop attacks made life impossible. She forgot to mention—or celebrate—that she was now dancing around the house and that her cognitive capacities had returned. | 30 (39.5%) |
| Feeling-related processes (especially feelings that are unacceptable to the self or in the family system) | ||
| Feeling overly responsible | For example, feeling compelled to act as a confidant and mediator in the school setting to settle distress felt by others or to sort out disputes between friends. Or taking responsibility to keep younger siblings safe while an older sibling is out of control or while parents engage in conflict. | 25 (32.9%) |
| Feeling worried | For example, chronic worries about schoolwork, friendships, or parental wellbeing. | 64 (84.2%) |
| Feeling sad | For example, experiencing sadness or a low mood but not being able to admit and share these feelings with attachment figures. | 58 (76.3%) |
| Feeling anger | For example, experiencing anger but not being able to admit and share feelings of anger. | 39 (51.3%) |
| Feeling guilt | For example, feeling guilt about asking for help or for taking up a hospital bed, or about feeling sad or worried. | 26 (34.2%) |
| Feeling helpless/hopeless about the situation | Nothing will work. No point trying. And so on. | 30 (39.5%) |
| Avoidance processes | ||
| Pushing difficult thoughts out of mind (cognition avoidance) | Attempting to manage worries and difficult thoughts—and the associated emotions—by pushing them out of mind. For example, an adolescent girl did not tick the questionnaire item pertaining to family conflict. When asked why, she explained that her father—with whom she was in sharp conflict—was no longer part of her family. | 44 (57.9%) |
| Pushing difficult feelings out of mind (feeling avoidance) | For example (and most commonly), pushing anger out of mind. | 37 (48.7%) |
| Avoidance of activities | For example, avoidance of exercise because it exacerbates pain and can trigger autonomic system activation (such as a panic attack). | 38 (50.0%) |
| Feeling-related processes related to body state (feeling homeostatic emotions) | ||
| Disconnecting and the inability to track body states (homeostatic emotions) | Inability to track any change in body state marking increased arousal or distress (e.g., respiratory rate, butterflies in the stomach, changes in tension). For example, an adolescent with leg weakness and panic attacks repetitively stated that she loved school and that school was not stressful despite a relapse of symptoms every time reintegration to school was attempted. | 43 (56.6%) |
| Attachment-related processes and behavioural processes | ||
| Being unable to tell parents that not all is well. | For example, not being able to tell parents about feelings of sadness or anger, or about the experience of being worried, overwhelmed. | 27 (35.5%) |
| Not telling parents about what is happening to the child to protect (not burden) parents. | For example, not telling parents about bullying, and trying to manage it all by oneself (but being unable to) in an effort to protect parents from becoming too stressed. | 22 (28.9%) |
| Not being able to ask for help. | For example, from the teacher, thereby perpetuating problems at school. | 25 (32.9%) |
| Amplify signals of distress to activate caregiving behaviour from parents (others) | For example, a boy with an abnormal gait coupled with back pain who signals his distress via loud, lingering wails as he laboriously makes his way to the hospital schoolroom. | 32 (42.1%) |
| Unresolved loss, unresolved trauma, and unresolved bad experiences | ||
| Intrusive thoughts/feelings/memories of the adverse event | For example, FND symptoms triggered on the anniversary of a parent’s death or past hospitalization, or when memories of an unresolved trauma are brought to mind in some other way. | 38 (50.0%) |
| Wave 1: Behaviour Therapy |
| In the first wave, behaviour therapy methods focus on changing overt behaviour by observing, predicting, and modifying behaviour to promote health and wellbeing. Behaviour therapy involves learning through association and utilizing reinforcement and punishment to modify behaviours. This wave is based on the work of Ivan Pavlov, Burrhus Frederic Skinner, and John Watson. |
| Wave 2: Classic CBT |
| The second wave of CBT—based on the work of Albert Ellis and Aaron Beck—focuses on the top-down link between maladaptive cognitions and behaviours; the goal is to detect and alter these existing maladaptive patterns and to develop more adaptive ones by identifying, labelling, and reframing cognitive distortions. This wave of CBT also acknowledges the role of behaviour in reinforcing cognitions and feelings, and incorporates bottom-up techniques such as exposure and habit reversal. |
| Wave 3: Acceptance CBT |
| The third wave of CBT is focused on the person’s relationship to thought and emotion more than the content itself. It emphasizes mindfulness (beginning with the work of Jon Kabat-Zinn), emotions, acceptance, values, and meta-cognition. This wave involves top-down, mindfulness-based, emotion-regulation strategies in which the child utilizes intentional efforts to increase attention and awareness capacities for better control of thoughts and feelings. The objective in third-wave CBT is to help the individual learn to live with painful or unpleasant sensations and with pain in the world, and to accept how things are instead of suffering by trying to change them. |
| CBT for FND |
| Each of the CBT-based interventions for FND utilizes different techniques selected from the above three waves. For example, retraining and control therapy (ReACT) uses bottom-up strategies, such as principles of habit reversal and mindfulness, to develop opposing responses to FS symptoms, and it challenges catastrophic symptoms expectations [67]. Children are asked to attend to their immediate experience (e.g., what they see and hear, and their physical sensations) immediately prior to the onset of an FS episode, and then to remain aware and conscious of their current experience while engaging in their opposing responses to prevent or stop FS symptoms. Other interventions [63,91] use bottom-up regulation strategies (e.g., slow-breathing techniques, heart rate variability biofeedback, and grounding techniques [similar to those described for retraining and control therapy] [19]) to increase capacity for neuroregulation before implementing other CBT strategies to target specific symptoms. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozlowska, K.; Schollar-Root, O.; Savage, B.; Hawkes, C.; Chudleigh, C.; Raghunandan, J.; Scher, S.; Helgeland, H. Illness-Promoting Psychological Processes in Children and Adolescents with Functional Neurological Disorder. Children 2023, 10, 1724. https://doi.org/10.3390/children10111724
Kozlowska K, Schollar-Root O, Savage B, Hawkes C, Chudleigh C, Raghunandan J, Scher S, Helgeland H. Illness-Promoting Psychological Processes in Children and Adolescents with Functional Neurological Disorder. Children. 2023; 10(11):1724. https://doi.org/10.3390/children10111724
Chicago/Turabian StyleKozlowska, Kasia, Olivia Schollar-Root, Blanche Savage, Clare Hawkes, Catherine Chudleigh, Jyoti Raghunandan, Stephen Scher, and Helene Helgeland. 2023. "Illness-Promoting Psychological Processes in Children and Adolescents with Functional Neurological Disorder" Children 10, no. 11: 1724. https://doi.org/10.3390/children10111724