



Examination of Physical Activity Patterns of Children, Reliability and Structural Validity Testing of the Hungarian Version of the PAQ-C Questionnaire
 ,
,  , , and
, , and
Abstract
:
1. Introduction
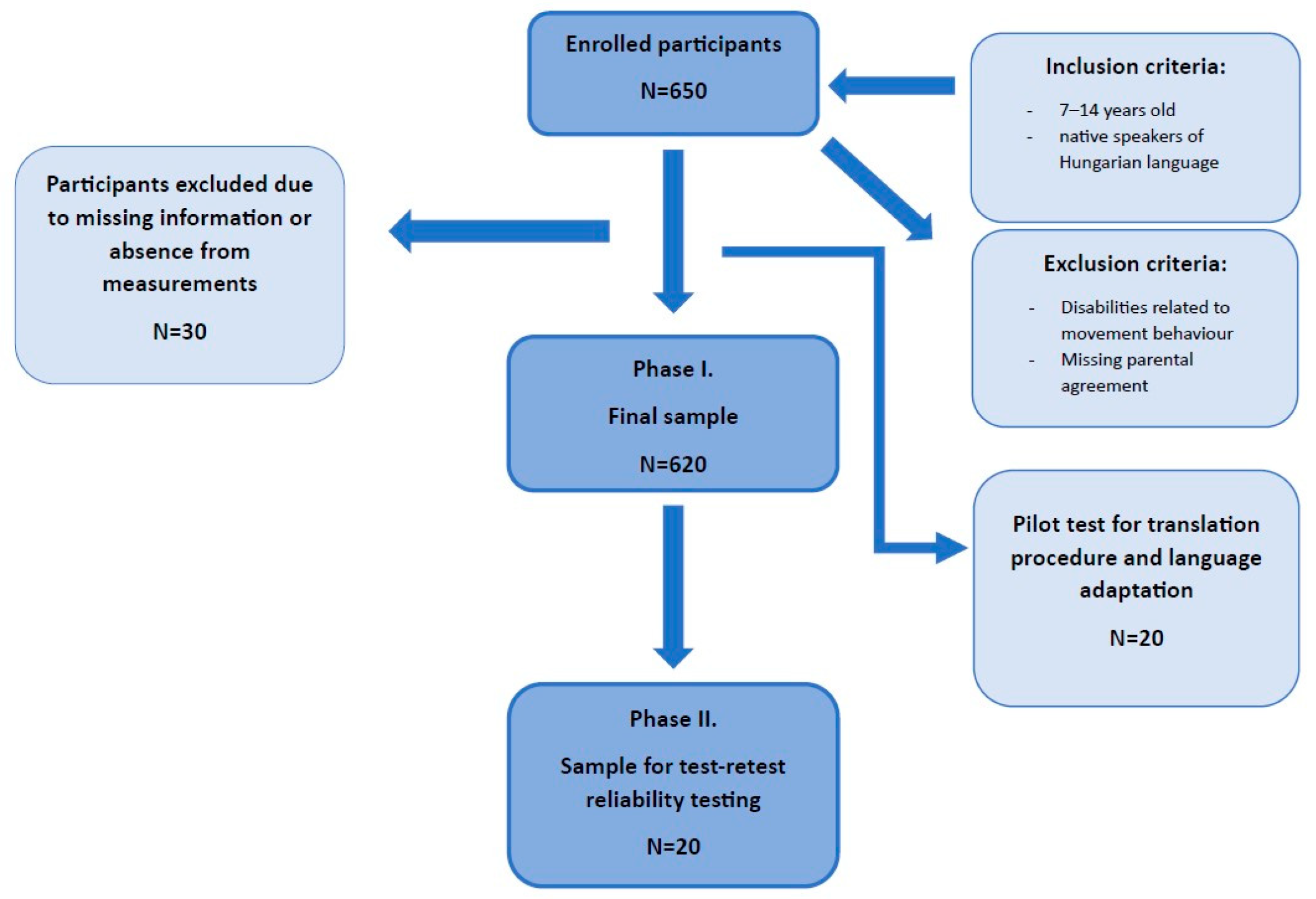
2. Materials and Methods
2.1. Ethical Approval and Consent to Participate
2.1.1. Assessment Tools
PAQ-C
Demographic Questions and Body Composition
2.2. Adaptation and Validation Procedure
2.3. Statistical Analysis
3. Results
3.1. Physical Activity Patterns
3.2. Internal Consistency and Test-Retest Reliability
3.3. Structural Validity of PAQ-C
3.4. Concurrent Validity of PAQ-C Questionnaire
3.5. Discriminant Validity
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Warburton, D.E.; Nicol, C.W.; Bredin, S.S. Health benefits of physical activity: The evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Annual Global Move for Health Initiative: A Concept Paper; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Huotari, P.; Nupponen, H.; Mikkelsson, L.; Laakso, L.; Kujala, U. Adolescent physical fitness and activity as predictors of adulthood activity. J. Sports Sci. 2011, 29, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Itoh, H.; Kitamura, F.; Hagi, N.; Mashiko, T.; Matsukawa, T.; Yokoyama, K. Leisure-time physical activity in youth as a predictor of adult leisure physical activity among Japanese workers: A cross-sectional study. Environ. Health Prev. Med. 2017, 22, 37. [Google Scholar] [CrossRef]
- Telama, R.; Yang, X.; Viikari, J.; Välimäki, I.; Wanne, O.; Raitakari, O. Physical activity from childhood to adulthood. Am. J. Prev. Med. 2005, 28, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Janssen, I.; LeBlanc, A.G. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 40. [Google Scholar] [CrossRef]
- Donnelly, J.E.; Hillman, C.H.; Castelli, D.; Etnier, J.L.; Lee, S.; Tomporowski, P.; Lambourne, K.; Szabo-Reed, A.N. Physical Activity, Fitness, Cognitive Function, and Academic Achievement in Children. Med. Sci. Sports Exerc. 2016, 48, 1197–1222. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Ruiz, J.R.; Ortega, F.B.; Martínez-Gómez, D.; Labayen, I.; Moreno, L.A.; De Bourdeaudhuij, I.; Manios, Y.; Gonzalez-Gross, M.; Mauro, B.; Molnar, D.; et al. Objectively Measured Physical Activity and Sedentary Time in European Adolescents: The HELENA Study. Am. J. Epidemiol. 2011, 174, 173–184. [Google Scholar] [CrossRef]
- Coppinger, T.; Milton, K.; Murtagh, E.; Harrington, D.; Johansen, D.; Seghers, J.; Skovgaard, T.; Chalkley, A. Global Matrix 3.0 physical activity report card for children and youth: A comparison across Europe. Public Health 2020, 187, 150–156. [Google Scholar] [CrossRef]
- Morningstar, B.; Clayborne, Z.; Wong, S.L.; Roberts, K.C.; Prince, S.A.; Gariépy, G.; Goldfield, G.S.; Janssen, I.; Lang, J.J. The association between social media use and physical activity among Canadian adolescents: A Health Behaviour in School-aged Children (HBSC) study. Can. J. Public Health 2023, 114, 642–650. [Google Scholar] [CrossRef]
- Gabriel, K.K.P.; Morrow, J.R.; Woolsey, A.-L.T. Framework for Physical Activity as a Complex and Multidimensional Behavior. J. Phys. Act. Health 2012, 9, S11–S18. [Google Scholar] [CrossRef]
- Marzi, I.; Tcymbal, A.; Gelius, P.; Abu-Omar, K.; Reimers, A.K.; Whiting, S.; Wickramasinghe, K. Monitoring of physical activity promotion in children and adolescents in the EU: Current status and future perspectives. Eur. J. Public Health 2022, 32, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Cuberek, R. Výzkumorientovanýnapohybovouaktivitu: Metodologickéukotvenı; Křížkovského, Palacký University: Olomouc, Czechia, 2019. [Google Scholar]
- Ács, P.; Betlehem, J.; Oláh, A.; Bergier, B.; Morvay-Sey, K.; Makai, A.; Prémusz, V. Cross-cultural adaptation and validationof the Global Physical Activity Questionnaire among healthy Hungarian adults. BMC Public Health 2020, 20 (Suppl. S1), 1056. [Google Scholar] [CrossRef]
- Ács, P.; Betlehem, J.; Oláh, A.; Bergier, J.; Melczer, C.; Prémusz, V.; Makai, A. Measurement of public health benefits of physical activity: Validity and reliability study of the International Physical Activity Questionnaire in Hungary. BMC Public Health 2020, 20 (Suppl. S1), 1198. [Google Scholar] [CrossRef]
- Jakubec, L.; Dygrýn, J.; Šimůnek, A.; Frömel, K. Validity of the original algorithm for assessing physical activity and sedentary behavior from the Youth Activity Profile in Czech children and adolescents. Tělesná Kult. 2020, 42, 62–69. [Google Scholar] [CrossRef]
- Kalman, M.; Hamrik, Z.; Sigmund, E.; Sigmundová, D.; Salonna, F.; Czech National HBSC Team. Physical activity of Czech adolescents: Findings from the HBSC 2010 study. Acta Gymnica 2015, 45, 3–11. [Google Scholar] [CrossRef]
- Saint-Maurice, P.F.; Kim, Y.; Hibbing, P.; Oh, A.Y.; Perna, F.M.; Welk, G.J. Calibration and Validation of the Youth Activity Profile: The FLASHE Study. Am. J. Prev. Med. 2017, 52, 880–887. [Google Scholar] [CrossRef]
- Sigmund, E.; Baďura, P.; Sigmundová, D.; Csémy, L.; Kalman, M. Methodological Aspects of Trend Studies and Development of the HBSC Study in the Czech Republic. Central Eur. J. Public Health 2017, 25 (Suppl. S1), S4–S9. [Google Scholar] [CrossRef]
- Cuberek, R.; Janíková, M.; Dygrýn, J. Adaptation and validation of the Physical Activity Questionnaire for Older Children (PAQ-C) among Czech children. PLoS ONE 2021, 16, e0245256. [Google Scholar] [CrossRef]
- KKowalski; Crocker, P.; Donen, R.; Honours, B. The Physical Activity Questionnaire for Older Children (PAQ-C) and Adolescents (PAQ-A) Manual. Coll. Kinesiol. Univ. Sask. 2004, 87, 1–38. [Google Scholar]
- Moore, J.B.; Hanes, J.C.; Barbeau, P.; Gutin, B.; Treviño, R.P.; Yin, Z. Validation of the Physical Activity Questionnaire for Older Children in Children of Different Races. Pediatr. Exerc. Sci. 2007, 19, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Benítez-Porres, J.; López-Fernández, I.; Raya, J.F.; Carnero, S.; Alvero-Cruz, J.R.; Carnero, E. Reliability and Validity of the PAQ-C Questionnaire to Assess Physical Activity in Children. J. Sch. Health 2016, 86, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Gobbi, E.; Elliot, C.; Varnier, M.; Carraro, A. Psychometric Properties of the Physical Activity Questionnaire for Older Children in Italy: Testing the Validity among a General and Clinical Pediatric Population. PLoS ONE 2016, 11, e0156354. [Google Scholar] [CrossRef]
- Bervoets, L.; Van Noten, C.; Van Roosbroeck, S.; Hansen, D.; Van Hoorenbeeck, K.; Verheyen, E.; Van Hal, G.; Vankerckhoven, V. Reliability and Validity of the Dutch Physical Activity Questionnaires for Children (PAQ-C) and Adolescents (PAQ-A). Arch. Public Health 2014, 72, 47. [Google Scholar] [CrossRef] [PubMed]
- Jing, W.J.; Tom, B.; Patrick, L.W.; An, C.T.; Jane, P.A. Validation of the Physical Activity Questionnaire for Older Children (PAQ-C) among Chinese Children. Biomed. Environ. Sci. 2016, 29, 177–186. [Google Scholar] [CrossRef]
- Samaržija, D.V.; Mišigoj-Duraković, M. Reliability of Croatian Version of The Questionnaire For Assessment of Overall Level of Physical Activity of Younger School Children. Hrvat. Športskomedicinski Vjesn. 2013, 28, 24. Available online: https://hrcak.srce.hr/106257 (accessed on 9 May 2013).
- Erdím, L.; Ergün, A. Reliability and validity of the Turkish version of the Physical Activity Questionnaire for Older Children (PAQ-C). Turk. J. Med. Sci. 2019, 49, 162–169. [Google Scholar] [CrossRef]
- Voss, C.; Dean, P.H.; Gardner, R.F.; Duncombe, S.L.; Harris, K.C. Validity and reliability of the Physical Activity Questionnaire for Children (PAQ-C) and Adolescents (PAQ-A) in individuals with congenital heart disease. PLoS ONE 2017, 12, e0175806. [Google Scholar] [CrossRef]
- Isa, T.; Sawa, R.; Torizawa, K.; Murata, S.; Saito, T.; Ebina, A.; Kondo, Y.; Tsuboi, Y.; Fukuta, A.; Misu, S.; et al. Reliability and Validity of the Japanese Version of the Physical Activity Questionnaire for Older Children. Clin. Med. Insights Pediatr. 2019, 13, 117955651983583. [Google Scholar] [CrossRef]
- Sirajudeen, M.S.; Waly, M.; Manzar, D.; Alqahtani, M.; Alzhrani, M.; Alanazi, A.; Unnikrishnan, R.; Muthusamy, H.; Saibannavar, R.; Alrubaia, W. Physical activity questionnaire for older children (PAQ-C): Arabic translation, cross-cultural adaptation, and psychometric validation in school-aged children in Saudi Arabia. PeerJ 2022, 10, e13237. [Google Scholar] [CrossRef]
- Németh, Á. Új Adatok a Magyar Serdülőkorúak Egészséget Befolyásoló Szokásairól És Egészségi Állapotáról. [New Data On The Hungarian Adolescents’ Health-Related Behaviours And Health Status]. Egészségfejlesztés 2020, 61, 84–85. [Google Scholar] [CrossRef]
- Welk, G.J.; Saint-Maurice, P.F.; Csányi, T. Health-Related Physical Fitness in Hungarian Youth: Age, Sex, and Regional Profiles. Res. Q. Exerc. Sport 2015, 86, S45–S57. [Google Scholar] [CrossRef]
- Karsai, I.; Kaj, M.; Csányi, T.; Ihász, F.; Marton, O.; Vass, Z. Magyar 11-19 éves iskolások egészségközpontú fittségi állapotának keresztmetszeti vizsgálata—Első jelentés az Országos Reprezentatív Iskolai Fittségmérési Program eredményeiről. Magy. Sport. Szle. 2013, 14, 9–18. [Google Scholar]
- MacCallum, R.C.; Widaman, K.F.; Zhang, S.; Hong, S. Sample size in factor analysis. Psychol. Methods 1999, 4, 84–99. [Google Scholar] [CrossRef]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Mokkink, L.B.; Terwee, C.B.; Knol, D.L.; Stratford, P.W.; Alonso, J.; Patrick, D.L.; Bouter, L.M.; de Vet, H.C. The COSMIN checklist for evaluating the methodological quality of studies on measurement properties: A clarification of its content. BMC Med. Res. Methodol. 2010, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Kincaid, J.P.; Fishburne, R.P., Jr.; Rogers, R.L.; Chissom, B.S. Derivation of New Readability Formulas (Automated Readability Index, Fog Count and Flesch Reading Ease Formula) for Navy Enlisted Personnel; University of Central Florida: Orlando, FL, USA, 1975. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Shevlin, M.; Miles, J.; Davies, M.; Walker, S. Coefficient alpha: A useful indicator of reliability? Pers. Individ. Differ. 2000, 28, 229–237. [Google Scholar] [CrossRef]
- Taber, K.S. The Use of Cronbach’s Alpha When Developing and Reporting Research Instruments in Science Education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Beckerman, H.; Roebroeck, M.; Lankhorst, G.; Becher, J.; Bezemer, P.; Verbeek, A. Smallest real difference, a link between reproducibility and responsiveness. Qual. Life Res. 2001, 10, 571–578. [Google Scholar] [CrossRef]
- Cronbach, L.J.; Meehl, P.E. Construct validity in psychological tests. Psychol. Bull. 1955, 52, 281–302. [Google Scholar] [CrossRef] [PubMed]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice, 3rd ed.; Prentice Hall: Hoboken, NJ, USA, 2007. [Google Scholar]
- George, D.; Mallery, P. SPSS for Windows Step by Step a Simple Guide and Reference 11.0 Update, 4th ed.; Allyn & Bacon: Boston, MA, USA, 2003. [Google Scholar]
- Uvacsek, M.; Soós, I. A V4 országokban élő gyermekek és fiatalok fizikai aktivitására vonatkozó eredmények a Global Matrix 4.0 alapján. Magy. Sport. Szle. 2023, 24, 124. [Google Scholar]
- Lang, J.J.; Zhang, K.; Agostinis-Sobrinho, C.; Andersen, L.B.; Basterfield, L.; Berglind, D.; Blain, D.O.; Cadenas-Sanchez, C.; Cameron, C.; Carson, V.; et al. Top 10 International Priorities for Physical Fitness Research and Surveillance Among Children and Adolescents: A Twin-Panel Delphi Study. Sports Med. 2022, 53, 549–564. [Google Scholar] [CrossRef] [PubMed]
- MKaj; Kälbli, K.; Király, A.; Karsai, I.; Marton, O.; Csányi, T. Kézikönyv a Nemzeti Egységes Tanulói Fittségi Teszt (NETFIT®) Alkalmazásához. Második, Bővített Kiadás; Magyar Diáksport Szövetség: Budapest, Hungary, 2019. [Google Scholar]
- Pogrmilovic, B.K.; Varela, A.R.; Pratt, M.; Milton, K.; Bauman, A.; Biddle, S.J.H.; Pedisic, Z. National physical activity and sedentary behaviour policies in 76 countries: Availability, comprehensiveness, implementation, and effectiveness. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 116. [Google Scholar] [CrossRef]
- Premelč, J.; Meh, K.; Vähä-Ypyä, H.; Sember, V.; Jurak, G. Do Fitter Children Better Assess Their Physical Activity with Questionnaire Than Less Fit Children? Int. J. Environ. Res. Public Health 2022, 19, 1304. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Items | N | % |
|---|---|---|---|
| Gender | male | 338 | 54.52 |
| female | 282 | 45.48 | |
| Mothers’ education | 8 classes | 53 | 8.55 |
| secondary school, vocational school | 165 | 31.29 | |
| college, university | 373 | 60.16 | |
| Fathers’ education | 8 classes | 25 | 4.03 |
| secondary school, vocational school | 280 | 45.16 | |
| college, university | 315 | 50.81 | |
| Place of living | capital/county seats | 446 | 71.94 |
| city | 76 | 12.26 | |
| village | 98 | 15.81 |
| Male (N = 338) | Female (N = 282) | Total (N = 620) | Gender Differences | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | p | |
| Weight (kg) | 43.19 | 15.29 | 41.79 | 15.01 | 42.55 | 15.17 | 0.240 |
| Body Fat (kg) | 8.18 | 6.56 | 9.48 | 6.27 | 8.77 | 6.46 | <0.001 |
| Skeletal Muscle Mass (kg) | 18.72 | 6.94 | 17.06 | 6.01 | 17.97 | 6.58 | 0.005 |
| Body Mass Index (kg/m2) | 18.56 | 3.78 | 18.34 | 3.64 | 18.46 | 3.71 | 0.503 |
| Body Fat % | 17.71 | 9.58 | 21.06 | 8.04 | 19.24 | 9.06 | <0.001 |
| Male | Female | Total | ||||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | |
| 1. Spare time activity | 1.01 | 0.12 | 1.02 | 0.13 | 1.01 | 0.13 |
| 2. Physical education | 4.17 | 0.99 | 4.17 | 0.83 | 4.17 | 0.92 |
| 3. Recess | 2.03 | 1.08 | 1.69 | 0.86 | 1.88 | 1.00 |
| 4. Lunch | 1.04 | 0.26 | 1.03 | 0.28 | 1.04 | 0.27 |
| 5. After school | 3.23 | 1.26 | 2.96 | 1.31 | 3.11 | 1.29 |
| 6. Evenings | 1.78 | 1.13 | 1.73 | 1.20 | 1.75 | 1.16 |
| 7. Weekends | 1.85 | 0.90 | 1.78 | 0.91 | 1.82 | 0.91 |
| 8. Describes you best | 2.85 | 1.01 | 2.63 | 1.04 | 2.75 | 1.03 |
| 9. Activity frequency | 3.11 | 0.98 | 2.86 | 1.02 | 3.00 | 1.00 |
| Study | Internal Consistency (Cronbach Alpha) | Test-Retest Reliability (ICC, 95% CI) |
|---|---|---|
| Phase I (N = 620) | 0.729 | 0.772 (0.373–0.841) |
| Phase II (N = 20) | 0.736 |
| PAQ-C | CFI | GFI | TLI | RMSEA | χ2 | df | p | χ2/df |
|---|---|---|---|---|---|---|---|---|
| Model 1 | 0.921 | 0.957 | 0.891 | 0.077 | 120.56 | 26 | <0.001 | 4.637 |
| Model 2 | 0.922 | 0.957 | 0.896 | 0.075 | 120.61 | 27 | <0.001 | 4.467 |
| Model 3 | 0.973 | 0.980 | 0.961 | 0.046 | 57.79 | 25 | <0.001 | 2.311 |
| Male (N = 338) | Female (N = 282 | Total (N = 620) | ||||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| Body Fat (kg) | −0.150 | 0.006 | 0.029 | 0.632 | −0.084 | 0.036 |
| Skeletal Muscle Mass (kg) | 0.262 | <0.001 | 0.289 | <0.001 | 0.281 | <0.001 |
| Body Mass Index | −0.027 | 0.627 | 0.075 | 0.206 | 0.026 | 0.520 |
| Body Fat % | −0.275 | <0.001 | −0.135 | 0.023 | −0.225 | <0.001 |
| Authors | Sample Size | Internal Consistency | ICC | Discriminant Validity—Gender Differences |
|---|---|---|---|---|
| Italian [26] | 1116 | 0.74 | - | Boys significantly higher than girls p < 0.001 |
| tCanada [31] | 84—congenital heart disease | 0.837 | 0.73 | - |
| Japanese [32] | 210 | 0.80 | 0.83 | Significantly higher in active subgroup p < 0.01 |
| Turkish [30] | 784 | 0.77 | 0.91 | - |
| Chech [22] | Phase 1 = 169 Phase 2 = 63 | 0.77 | 0.73–0.94 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makai, A.; Prémusz, V.; Dózsa-Juhász, O.; Fodor-Mazzag, K.; Melczer, C.; Ács, P. Examination of Physical Activity Patterns of Children, Reliability and Structural Validity Testing of the Hungarian Version of the PAQ-C Questionnaire. Children 2023, 10, 1547. https://doi.org/10.3390/children10091547
Makai A, Prémusz V, Dózsa-Juhász O, Fodor-Mazzag K, Melczer C, Ács P. Examination of Physical Activity Patterns of Children, Reliability and Structural Validity Testing of the Hungarian Version of the PAQ-C Questionnaire. Children. 2023; 10(9):1547. https://doi.org/10.3390/children10091547
Chicago/Turabian StyleMakai, Alexandra, Viktória Prémusz, Olívia Dózsa-Juhász, Kitti Fodor-Mazzag, Csaba Melczer, and Pongrác Ács. 2023. "Examination of Physical Activity Patterns of Children, Reliability and Structural Validity Testing of the Hungarian Version of the PAQ-C Questionnaire" Children 10, no. 9: 1547. https://doi.org/10.3390/children10091547