
Collaborating to Improve Neonatal Care: ParentAl Participation on the NEonatal Ward—Study Protocol of the neoPARTNER Study


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Organisation Involvement
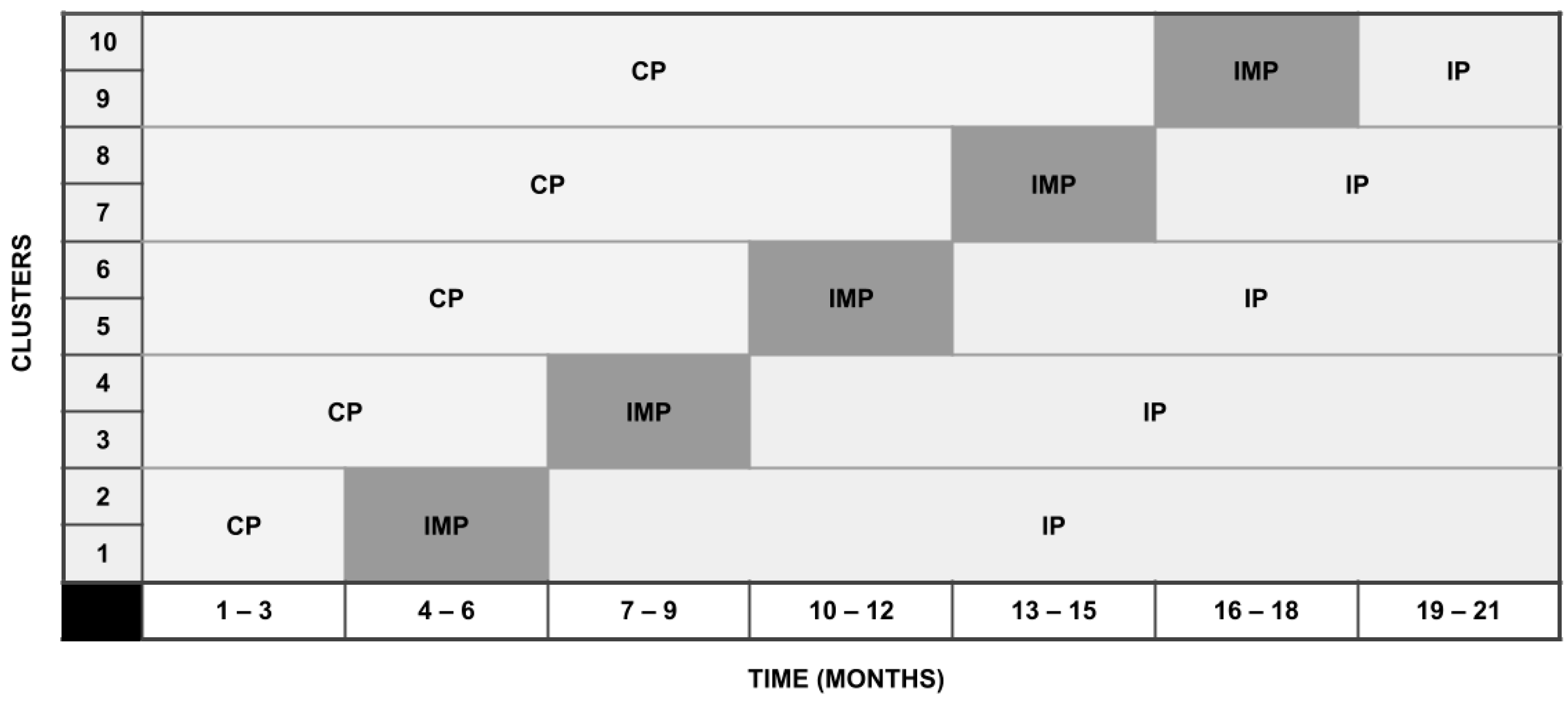
2.2. Design
2.3. Setting
2.4. Study Population
2.4.1. Inclusion Criteria
- −
- Infant requiring hospital admission directly (within 24 h) after birth;
- −
- Parent are 18 years or older;
- −
- Written, informed consent of both parents/legal guardians (compliant to the regulations of the Central Committee on Research Involving Human Subjects).
2.4.2. Exclusion Criteria
- −
- Infant’s hospital stay shorter than 7 days;
- −
- Infant with severe congenital or syndromal anomaly;
- −
- Infant with critical illness who is unlikely to survive;
- −
- Parents with current severe psychosocial problems;
- −
- Involvement of child protective services in the family;
- −
- Parents not able or not willing to fill out questionnaires in English or Dutch.
2.5. Procedures
- Education of parents:
- −
- Information on the hospital admission and care of an infant, including a digital application (NeoZorg application);
- −
- The possibility to keep track of (medical) information in a diary and/or digital application (NeoZorg application, see further);
- −
- Educational and thematic meetings (physical and/or digital) with other parents, led by either healthcare professionals (nurses, paediatricians and/or paramedic staff) or veteran parents.
- Education of healthcare professionals:
- −
- Comprehensive e-learning on FICare and FCR, developed by the research group. The e-learning comprises the following modules:
- −
- Theoretical background and historical context of FICare and FCR;
- −
- Implementing FCR in practical settings;
- −
- Coaching of parents by healthcare professionals;
- −
- Explanation of the existing (co-)interventions SFR and family-centred care;
- −
- Understanding the principles of FCR and shared decision-making.
- −
- Training in FICare principles: the research group has designed training materials for effective collaboration and communication with parents, parent participation and shared decision-making. These training materials draw from both existing literature and the valuable insights available on the Canadian website dedicated to FICare (www.familyintegratedcare.com, accessed on 22 May 2022).
- −
- The theory and practical application of FICare and FCR;
- −
- The role of healthcare professionals within the context of FICare;
- −
- Emphasizing shared decision-making.
- Psychosocial support:
- −
- Facilitating contact and peer support for parents with veteran parents, both during admission and after discharge;
- −
- Support by paramedical staff (e.g., psychologist, preverbal speech therapist, physiotherapist, social worker).
- Environment of the neonatal ward:
- −
- FICare whiteboard/communication board, at which parents can track for example their participation progress and information on their infant;
- −
- Facilities for skin-to-skin contact and expressing human milk on the ward;
- −
- 24/7 access to the ward;
- −
- Facilities to be (digitally) present during medical rounds (i.e., including video conference or telephone calls).
2.6. Control Treatment: Standard Neonatal Care without FCR
2.7. Interventional Treatment: Family-Centred Rounds Embedded in the FICare Principles
2.8. Primary Outcome
2.9. Secondary Outcomes
2.9.1. Infant Outcomes
2.9.2. Parental Outcomes
2.9.3. Outcomes at Cluster Level
2.9.4. Cost-Effectiveness
2.9.5. Biomarkers
2.10. Statistical Procedures
2.10.1. Sample Size Calculation
2.10.2. Statistical Analysis
3. Results
3.1. Trial Progress
3.2. Reporting and Publication
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flacking, R.; Lehtonen, L.; Thomson, G.; Axelin, A.; Ahlqvist, S.; Moran, V.H.; Ewald, U.; Dykes, F. Closeness and Separation in Neonatal Intensive Care. Acta Paediatr. Int. J. Paediatr. 2012, 101, 1032–1037. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.S. Parents of Critically Ill Premature Infants: Sources of Stress. Crit. Care Nurs. Q. 1989, 12, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Serlachius, A.; Hames, J.; Juth, V.; Garton, D.; Rowley, S.; Petrie, K.J. Parental Experiences of Family-Centred Care from Admission to Discharge in the Neonatal Intensive Care Unit. J. Paediatr. Child Health 2018, 54, 1227–1233. [Google Scholar] [CrossRef] [PubMed]
- Cleveland, L.M. Parenting in the Neonatal Intensive Care Unit. JOGNN J. Obstet. Gynecol. Neonatal Nurs. 2008, 37, 666–691. [Google Scholar] [CrossRef]
- Fenwick, J.; Barclay, L.; Schmied, V. Struggling to Mother: A Consequence of Inhibitive Nursing Interactions in the Neonatal Nursery. J. Perinat. Neonatal Nurs. 2001, 15, 49–64. [Google Scholar] [CrossRef]
- Galarza-Winton, M.E.; Dicky, T.; O’Leary, L.; Lee, S.K.; O’Brien, K. Implementing Family-Integrated Care in the NICU: Educating Nurses. Adv. Neonatal Care 2013, 13, 335–340. [Google Scholar] [CrossRef]
- Lasiuk, G.C.; Comeau, T.; Newburn-Cook, C. Unexpected: An Interpretive Description of Parental Traumas’ Associated with Preterm Birth. BMC Pregnancy Childbirth 2013, 13 (Suppl. 1), S13. [Google Scholar] [CrossRef]
- Woodward, L.J.; Bora, S.; Clark, C.A.C.; Montgomery-Hönger, A.; Pritchard, V.E.; Spencer, C.; Austin, N.C. Very Preterm Birth: Maternal Experiences of the Neonatal Intensive Care Environment. J. Perinatol. 2014, 34, 555–561. [Google Scholar] [CrossRef]
- Miles, M.S.; Holditch-Davis, D.; Schwartz, T.A.; Scher, M. Depressive Symptoms in Mothers of Prematurely Born Infants. J. Dev. Behav. Pediatr. 2007, 28, 36–44. [Google Scholar] [CrossRef]
- Nicolaou, M.; Glazebrook, C. Emotional Support for Families of Sick Neonates. Paediatr. Child Health Oxf. 2008, 18, 196–199. [Google Scholar] [CrossRef]
- Maas, A.J.B.M.; Vreeswijk, C.M.J.M.; de Cock, E.S.A.; Rijk, C.H.A.M.; van Bakel, H.J.A. “Expectant Parents”: Study Protocol of a Longitudinal Study Concerning Prenatal (Risk) Factors and Postnatal Infant Development, Parenting, and Parent-Infant Relationships. BMC Pregnancy Childbirth 2012, 12, 46. [Google Scholar] [CrossRef] [PubMed]
- van Veenendaal, N.R.; Labrie, N.H.M.; Mader, S.; van Kempen, A.A.M.W.; van der Schoor, S.R.D.; van Goudoever, J.B.; Bertino, E.; Bhojnagarwala, B.; Bodrogi, E.; Bohlin, K.; et al. An International Study on Implementation and Facilitators and Barriers for Parent-Infant Closeness in Neonatal Units. Pediatr. Investig. 2022, 6, 179–188. [Google Scholar] [CrossRef]
- Franck, L.S.; O’Brien, K. The Evolution of Family-Centered Care: From Supporting Parent-Delivered Interventions to a Model of Family Integrated Care. Birth Defects Res. 2019, 111, 1044–1059. [Google Scholar] [CrossRef]
- O’Brien, K.; Bracht, M.; Robson, K.; Ye, X.Y.; Mirea, L.; Cruz, M.; Ng, E.; Monterrosa, L.; Soraisham, A.; Alvaro, R.; et al. Evaluation of the Family Integrated Care Model of Neonatal Intensive Care: A Cluster Randomized Controlled Trial in Canada and Australia. BMC Pediatr. 2015, 15, 210. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.; Bracht, M.; Macdonell, K.; McBride, T.; Robson, K.; O’Leary, L.; Christie, K.; Galarza, M.; Dicky, T.; Levin, A.; et al. A Pilot Cohort Analytic Study of Family Integrated Care in a Canadian Neonatal Intensive Care Unit. BMC Pregnancy Childbirth 2013, 13 (Suppl. 1), S12. [Google Scholar] [CrossRef] [PubMed]
- Stelwagen, M.; van Kempen, A.; Westmaas, A.; Vet, E.; Scheele, F. Parents’ Experiences With a Model of Integrated Maternity and Neonatal Care Designed to Empower Parents. J. Obstet. Gynecol. Neonatal Nurs. 2021, 50, 181–192. [Google Scholar] [CrossRef]
- Stelwagen, M.; Westmaas, A.; Van Kempen, A.; Scheele, F. In-Hospital Education of Parents of Newborns May Benefit from Competency-Based Education: A Qualitative Focus Group and Interview Study among Health Professionals. J. Clin. Nurs. 2023, 32, 1076–1088. [Google Scholar] [CrossRef]
- Labrie, N.H.M.; van Veenendaal, N.R.; Ludolph, R.A.; Ket, J.C.F.; van der Schoor, S.R.D.; van Kempen, A.A.M.W. Effects of Parent-Provider Communication during Infant Hospitalization in the NICU on Parents: A Systematic Review with Meta-Synthesis and Narrative Synthesis. Patient Educ. Couns. 2021, 104, 1526–1552. [Google Scholar] [CrossRef]
- Axelin, A.; Outinen, J.; Lainema, K.; Lehtonen, L.; Franck, L.S. Neonatologists Can Impede or Support Parents’ Participation in Decision-Making during Medical Rounds in Neonatal Intensive Care Units. Acta Paediatr. Int. J. Paediatr. 2018, 107, 2100–2108. [Google Scholar] [CrossRef]
- Voos, K.C.; Ross, G.; Ward, M.J.; Yohay, A.L.; Osorio, S.N.; Perlman, J.M. Effects of Implementing Family-Centered Rounds (FCRs) in a Neonatal Intensive Care Unit (NICU). J. Matern. Neonatal Med. 2011, 24, 1403–1406. [Google Scholar] [CrossRef]
- Davidson, J.E. Family Presence on Rounds in Neonatal, Pediatric, and Adult Intensive Care Units. Ann. Am. Thorac. Soc. 2013, 10, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Church, P.T.; Grunau, R.E.; Mirea, L.; Petrie, J.; Soraisham, A.S.; Synnes, A.; Ye, Y.; O’brien, K. Family Integrated Care (FICare): Positive Impact on Behavioural Outcomes at 18 Months. Early Hum. Dev. 2020, 151, 105196. [Google Scholar] [CrossRef] [PubMed]
- Moe, A.M.; Kurilova, J.; Afzal, A.R.; Benzies, K.M. Effects of Alberta Family Integrated Care (FICare) on Preterm Infant Development: Two Studies at 2 Months and between 6 and 24 Months Corrected Age. J. Clin. Med. 2022, 11, 1684. [Google Scholar] [CrossRef] [PubMed]
- Synnes, A.R.; Petrie, J.; Grunau, R.E.; Church, P.; Kelly, E.; Moddemann, D.; Ye, X.; Lee, S.K.; O’Brien, K. Family Integrated Care: Very Preterm Neurodevelopmental Outcomes at 18 Months. Arch. Dis. Child. Fetal Neonatal Ed. 2022, 107, 76–81. [Google Scholar] [CrossRef]
- Van Veenendaal, N.R.; Van Kempen, A.A.M.W.; Broekman, B.F.P.; De Groof, F.; Van Laerhoven, H.; Van Den Heuvel, M.E.N.; Rijnhart, J.J.M.; Van Goudoever, J.B.; Van Der Schoor, S.R.D. Association of a Zero-Separation Neonatal Care Model With Stress in Mothers of Preterm Infants. JAMA Netw. open 2022, 5, e224514. [Google Scholar] [CrossRef]
- van Veenendaal, N.R.; van der Schoor, S.R.D.; Broekman, B.F.P.; de Groof, F.; van Laerhoven, H.; van den Heuvel, M.E.N.; Rijnhart, J.J.M.; van Goudoever, J.H.B.; van Kempen, A.A.M.W. Association of a Family Integrated Care Model With Paternal Mental Health Outcomes During Neonatal Hospitalization. JAMA Netw. open 2022, 5, E2144720. [Google Scholar] [CrossRef]
- Staniszewska, S.; Brett, J.; Simera, I.; Seers, K.; Mockford, C.; Goodlad, S.; Altman, D.G.; Moher, D.; Barber, R.; Denegri, S.; et al. GRIPP2 Reporting Checklists: Tools to Improve Reporting of Patient and Public Involvement in Research. Res. Involv. Engagem. 2017, 358, j3453. [Google Scholar] [CrossRef]
- Hemming, K.; Taljaard, M.; McKenzie, J.E.; Hooper, R.; Copas, A.; Thompson, J.A.; Dixon-Woods, M.; Aldcroft, A.; Doussau, A.; Grayling, M.; et al. Reporting of Stepped Wedge Cluster Randomised Trials: Extension of the CONSORT 2010 Statement with Explanation and Elaboration. BMJ 2018, 363, k1614. [Google Scholar] [CrossRef]
- Barfield, W.D.; Papile, L.A.; Baley, J.E.; Benitz, W.; Cummings, J.; Carlo, W.A.; Kumar, P.; Polin, R.A.; Tan, R.C.; Watterberg, K.L.; et al. Levels of Neonatal Care. Pediatrics 2012, 130, 587–597. [Google Scholar] [CrossRef]
- Perined, Utrecht, 2022. Available online: www.peristat.nl (accessed on 2 August 2023).
- Schappin, R.; Wijnroks, L.; Uniken Venema, M.M.A.T.; Jongmans, M.J. Rethinking Stress in Parents of Preterm Infants: A Meta-Analysis. PLoS ONE 2013, 8, e54992. [Google Scholar] [CrossRef]
- Miles, M.S.; Funk, S.G.; Carlson, J. Parental Stressor Scale: Neonatal Intensive Care Unit. Nurs. Res. 1993, 42, 148–152. [Google Scholar] [CrossRef]
- Flamant, C.; Branger, B.; Nguyen The Tich, S.; de La Rochebrochard, E.; Savagner, C.; Berlie, I.; Rozé, J.-C. Parent-Completed Developmental Screening in Premature Children: A Valid Tool for Follow-Up Programs. PLoS ONE 2011, 6, e20004. [Google Scholar] [CrossRef]
- Schonhaut, L.; Armijo, I.; Schönstedt, M.; Alvarez, J.; Cordero, M. Validity of the Ages and Stages Questionnaires in Term and Preterm Infants. Pediatrics 2013, 131, e1468–e1474. [Google Scholar] [CrossRef]
- Steenis, L.J.P.; Verhoeven, M.; Hessen, D.J.; van Baar, A.L. Parental and Professional Assessment of Early Child Development: The ASQ-3 and the Bayley-III-NL. Early Hum. Dev. 2015, 91, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Kriston, L.; Scholl, I.; Hölzel, L.; Simon, D.; Loh, A.; Härter, M. The 9-Item Shared Decision Making Questionnaire (SDM-Q-9). Development and Psychometric Properties in a Primary Care Sample. Patient Educ. Couns. 2010, 80, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg-Vandenbussche, S.; Pieterse, A.H.; Kroonenberg, P.M.; Scholl, I.; van der Weijden, T.; Luyten, G.P.M.; Kruitwagen, R.F.P.M.; den Ouden, H.; Carlier, I.V.E.; van Vliet, I.M.; et al. Dutch Translation and Psychometric Testing of the 9-Item Shared Decision Making Questionnaire (SDM-Q-9) and Shared Decision Making Questionnaire-Physician Version (SDM-Q-Doc) in Primary and Secondary Care. PLoS ONE 2015, 10, e0132158. [Google Scholar] [CrossRef]
- Degner, L.F.; Sloan, J.A.; Venkatesh, P. The Control Preferences Scale. Can. J. Nurs. Res. 1997, 29, 21–43. [Google Scholar] [CrossRef] [PubMed]
- Kasper, J.; Heesen, C.; Köpke, S.; Fulcher, G.; Geiger, F. Patients’ and Observers’ Perceptions of Involvement Differ. Validation Study on Inter-Relating Measures for Shared Decision Making. PLoS ONE 2011, 6, 26255. [Google Scholar] [CrossRef]
- van Veenendaal, N.R.; Auxier, J.N.; van der Schoor, S.R.D.; Franck, L.S.; Stelwagen, M.A.; de Groof, F.; van Goudoever, J.B.; Eekhout, I.E.; de Vet, H.C.W.; Axelin, A.; et al. Development and Psychometric Evaluation of the CO-PARTNER Tool for Collaboration and Parent Participation in Neonatal Care. PLoS ONE 2021, 16, e0252074. [Google Scholar] [CrossRef]
- Condon, J.T.; Corkindale, C.J. The Assessment of Parent-to-Infant Attachment: Development of a Self-Report Questionnaire Instrument. J. Reprod. Infant Psychol. 1998, 16, 57–76. [Google Scholar] [CrossRef]
- van Bussel, J.C.H.; Spitz, B.; Demyttenaere, K. Three Self-Report Questionnaires of the Early Mother-to-Infant Bond: Reliability and Validity of the Dutch Version of the MPAS, PBQ and MIBS. Arch. Women’s Ment. Health 2010, 13, 373–384. [Google Scholar] [CrossRef]
- Scopesi, A.; Viterbori, P.; Sponza, S.; Zucchinetti, P. Assessing Mother-to-infant Attachment: The Italian Adaptation of a Self-report Questionnaire. J. Reprod. Infant Psychol. 2010, 22, 99–109. [Google Scholar] [CrossRef]
- Condon, J.T.; Corkindale, C.J.; Boyce, P. Assessment of Postnatal Paternal–Infant Attachment: Development of a Questionnaire Instrument. J. Reprod. Infant Psychol. 2008, 26, 195–210. [Google Scholar] [CrossRef]
- Blevins, C.A.; Weathers, F.W.; Davis, M.T.; Witte, T.K.; Domino, J.L. The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5): Development and Initial Psychometric Evaluation. J. Trauma. Stress 2015, 28, 489–498. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (PCL-5)—Standard [Measurement Instrument]. Available online: https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp (accessed on 2 September 2021).
- Sveen, J.; Bondjers, K.; Willebrand, M. Psychometric Properties of the PTSD Checklist for Dsm-5: A Pilot Study. Eur. J. Psychotraumatol. 2016, 7, 30165. [Google Scholar] [CrossRef]
- Boeschoten, M.A.; Bakker, A.; Jongedijk, R.A.; Olff, M. PTSD Checklist for DSM-5—Nederlandstalige Versie. In Uitgave: Stichting Centrum ‘45; Arq Psychotrauma Expert Groep: Diemen, The Netherlands, 2014. [Google Scholar]
- van Praag, D.L.G.; Fardzadeh, H.E.; Covic, A.; Maas, A.I.R.; von Steinbüchel, N. Preliminary Validation of the Dutch Version of the Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5) after Traumatic Brain Injury in a Civilian Population. PLoS ONE 2020, 15, e0231857. [Google Scholar] [CrossRef]
- Terwee, C.B.; Roorda, L.D.; de Vet, H.C.; Dekker, J.; Westhovens, R.; van Leeuwen, J.; Cella, D.; Correia, H.; Arnold, B.; Perez, B.; et al. Dutch-Flemish Translation of 17 Item Banks from the Patient-Reported Outcomes Measurement Information System (PROMIS). Qual. Life Res. 2014, 23, 1733–1741. [Google Scholar] [CrossRef]
- Pilkonis, P.A.; Choi, S.W.; Reise, S.P.; Stover, A.M.; Riley, W.T.; Cella, D. Item Banks for Measuring Emotional Distress from the Patient-Reported Outcomes Measurement Information System (PROMIS®): Depression, Anxiety, and Anger. Assessment 2011, 18, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Hake-Brooks, S.J.; Anderson, G.C. Kangaroo Care and Breastfeeding of Mother-Preterm Infant Dyads 0-18 Months: A Randomized, Controlled Trial. Neonatal Netw. 2008, 27, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Labbok, M.; Krasovec, K. Toward Consistency in Breastfeeding Definitions. Stud. Fam. Plann. 1990, 21, 226. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.L.; Engstrom, J.L.; Meier, P.P.; Kimura, R.E. Accuracy of Methods for Calculating Postnatal Growth Velocity for Extremely Low Birth Weight Infants. Pediatrics 2005, 116, 1466–1473. [Google Scholar] [CrossRef] [PubMed]
- Kantake, M.; Yoshitake, H.; Ishikawa, H.; Araki, Y.; Shimizu, T. Postnatal Epigenetic Modification of Glucocorticoid Receptor Gene in Preterm Infants: A Prospective Cohort Study. BMJ Open 2014, 4, e005318. [Google Scholar] [CrossRef]
- Hollanders, J.J.; van der Voorn, B.; de Goede, P.; Toorop, A.A.; Dijkstra, L.R.; Honig, A.; Rotteveel, J.; Dolman, K.M.; Kalsbeek, A.; Finken, M.J.J. Biphasic Glucocorticoid Rhythm in One-Month-Old Infants: Reflection of a Developing HPA-Axis? J. Clin. Endocrinol. Metab. 2020, 105, e544. [Google Scholar] [CrossRef]
- Romijn, M.; Tilburg, L.J.L.; van Hollanders, J.J.; van der Voorn, B.; de Goede, P.; Dolman, K.M.; Heijboer, A.C.; Broekman, B.F.P.; Rotteveel, J.; Finken, M.J.J. The Association between Maternal Stress and Glucocorticoid Rhythmicity in Human Milk. Nutrients 2021, 13, 1608. [Google Scholar] [CrossRef]
- Bouwmans, C.; Hakkaart-van Roijen, L.; Koopmanschap, M.; Krol, M.; Severens, H.; Brouwer, W. Handleiding iMTA Medical Cost Questionnaire (iMCQ); iMTA: Rotterdam, The Netherlands; Erasmus Universiteit Rotterdam: Rotterdam, The Netherlands, 2013. [Google Scholar]
- Bouwmans, C.; Krol, M.; Severens, H.; Koopmanschap, M.; Brouwer, W.; Hakkaart-van Roijen, L. The IMTA Productivity Cost Questionnaire: A Standardized Instrument for Measuring and Valuing Health-Related Productivity Losses. Value Health 2015, 18, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Scholl, I.; Kriston, L.; Dirmaier, J.; Buchholz, A.; Härter, M. Development and Psychometric Properties of the Shared Decision Making Questionnaire—Physician Version (SDM-Q-Doc). Patient Educ. Couns. 2012, 88, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.; Bakker, A. Uwes Utrecht Work Engagement Scale Preliminary Manual. Available online: https://www.wilmarschaufeli.nl/publications/Schaufeli/Test%20Manuals/Test_manual_UWES_English.pdf (accessed on 2 September 2021).
- Schaufeli, W.B.; Bakker, A.B.; Salanova, M. The Measurement of Work Engagement With a Short Questionnaire: A Cross-National Study. Educ. Psychol. Meas. 2016, 66, 701–716. [Google Scholar] [CrossRef]
- Van Berkel, J.; Boot, C.R.L.; Proper, K.I.; Bongers, P.M.; Van Der Beek, A.J. Effectiveness of a Worksite Mindfulness-Related Multi-Component Health Promotion Intervention on Work Engagement and Mental Health: Results of a Randomized Controlled Trial. PLoS ONE 2014, 9, e84118. [Google Scholar] [CrossRef] [PubMed]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An Instrument for Internationally Comparative Assessments of Psychosocial Job Characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef] [PubMed]
- Hollanders, J.J.; van der Voorn, B.; Kieviet, N.; Dolman, K.M.; de Rijke, Y.B.; van den Akker, E.L.T.; Rotteveel, J.; Honig, A.; Finken, M.J.J. Interpretation of Glucocorticoids in Neonatal Hair: A Reflection of Intrauterine Glucocorticoid Regulation? Endocr. Connect. 2017, 6, 692–699. [Google Scholar] [CrossRef]
- Kaan, A.M.; Buijs, M.J.; Brandt, B.W.; Crielaard, W.; Keijser, B.J.F.; de Ruyter, J.C.; Zaura, E. Home Sampling Is a Feasible Method for Oral Microbiota Analysis for Infants and Mothers. J. Dent. 2020, 100, 103428. [Google Scholar] [CrossRef] [PubMed]
- Sauvé, B.; Koren, G.; Walsh, G.; Tokmakejian, S.; Van Uum, S.H.M. Measurement of Cortisol in Human Hair as a Biomarker of Systemic Exposure. Clin. Investig. Med. 2007, 30, E183–E191. [Google Scholar] [CrossRef]
- Wennig, R. Potential Problems with the Interpretation of Hair Analysis Results. Forensic Sci. Int. 2000, 107, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Abell, J.G.; Stalder, T.; Ferrie, J.E.; Shipley, M.J.; Kirschbaum, C.; Kivimäki, M.; Kumari, M. Assessing Cortisol from Hair Samples in a Large Observational Cohort: The Whitehall II Study. Psychoneuroendocrinology 2016, 73, 148–156. [Google Scholar] [CrossRef]
- Jolani, S.; Debray, T.P.A.; Koffijberg, H.; van Buuren, S.; Moons, K.G.M. Imputation of Systematically Missing Predictors in an Individual Participant Data Meta-Analysis: A Generalized Approach Using MICE. Stat. Med. 2015, 34, 1841–1863. [Google Scholar] [CrossRef]
- Taljaard, M.; Donner, A.; Klar, N. Imputation Strategies for Missing Continuous Outcomes in Cluster Randomized Trials. Biom. J. 2008, 50, 29–345. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.B. Inference and Missing Data. Biometrika 1976, 63, 581–592. [Google Scholar] [CrossRef]
- Fiero, M.H.; Huang, S.; Oren, E.; Bell, M.L. Statistical Analysis and Handling of Missing Data in Cluster Randomized Trials: A Systematic Review. Trials 2016, 17, 72. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, K.; Robson, K.; Bracht, M.; Cruz, M.; Lui, K.; Alvaro, R.; da Silva, O.; Monterrosa, L.; Narvey, M.; Ng, E.; et al. Effectiveness of Family Integrated Care in Neonatal Intensive Care Units on Infant and Parent Outcomes: A Multicentre, Multinational, Cluster-Randomised Controlled Trial. Lancet Child Adolesc. Health 2018, 2, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Toivonen, M.; Lehtonen, L.; Löyttyniemi, E.; Ahlqvist-Björkroth, S.; Axelin, A. Close Collaboration with Parents Intervention Improves Family-Centered Care in Different Neonatal Unit Contexts: A Pre–Post Study. Pediatr. Res. 2020, 88, 421–428. [Google Scholar] [CrossRef]
- Benzies, K.M.; Aziz, K.; Shah, V.; Faris, P.; Isaranuwatchai, W.; Scotland, J.; Larocque, J.; Mrklas, K.J.; Naugler, C.; Stelfox, H.T.; et al. Effectiveness of Alberta Family Integrated Care on Infant Length of Stay in Level II Neonatal Intensive Care Units: A Cluster Randomized Controlled Trial. BMC Pediatr. 2020, 20, 535. [Google Scholar] [CrossRef] [PubMed]
- Hoeben, H.; Obermann-Borst, S.A.; Stelwagen, M.A.; van Kempen, A.A.M.W.; van Goudoever, J.B.; van der Schoor, S.R.D.; van Veenendaal, N.R. Parent’s Experience in Participation in Different Settings of Dutch Neonatal Care: A Cross-Sectional Survey Study; OLVG: Amsterdam, The Netherlands, 2023. [Google Scholar]
- Ziomkiewicz, A.; Babiszewska, M.; Apanasewicz, A.; Piosek, M.; Wychowaniec, P.; Cierniak, A.; Barbarska, O.; Szołtysik, M.; Danel, D.; Wichary, S. Psychosocial Stress and Cortisol Stress Reactivity Predict Breast Milk Composition. Sci. Rep. 2021, 11, 11576. [Google Scholar] [CrossRef] [PubMed]
- di Benedetto, M.G.; Bottanelli, C.; Cattaneo, A.; Pariante, C.M.; Borsini, A. Nutritional and Immunological Factors in Breast Milk: A Role in the Intergenerational Transmission from Maternal Psychopathology to Child Development. Brain. Behav. Immun. 2020, 85, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, M.; Browne, P.D.; Hechler, C.; Beijers, R.; Rodríguez, J.M.; de Weerth, C.; Fernández, L. Human Milk Cortisol and Immune Factors over the First Three Postnatal Months: Relations to Maternal Psychosocial Distress. PLoS ONE 2020, 15, e0233554. [Google Scholar] [CrossRef]
- Mohd Shukri, N.H.; Wells, J.; Eaton, S.; Mukhtar, F.; Petelin, A.; Jenko-Pražnikar, J.; Fewtrell, M. Randomized Controlled Trial Investigating the Effects of a Breastfeeding Relaxation Intervention on Maternal Psychological State, Breast Milk Outcomes, and Infant Behavior and Growth. Am. J. Clin. Nutr. 2019, 110, 121–130. [Google Scholar] [CrossRef]
- Hei, M.; Gao, X.; Li, Y.; Gao, X.; Li, Z.; Xia, S.; Zhang, Q.; Han, S.; Gao, H.; Nong, S.; et al. Family Integrated Care for Preterm Infants in China: A Cluster Randomized Controlled Trial. J. Pediatr. 2020, 228, 36–43.e2. [Google Scholar] [CrossRef]
- Broom, M.; Parsons, G.; Carlisle, H.; Kecskes, Z.; Dowling, D.; Thibeau, S. Exploring Parental and Staff Perceptions of the Family-Integrated Care Model: A Qualitative Focus Group Study. Adv. Neonatal Care 2017, 17, E12–E19. [Google Scholar] [CrossRef]
- Moreno-Sanz, B.; Montes, M.T.; Antón, M.; Serrada, M.T.; Cabrera, M.; Pellicer, A. Scaling Up the Family Integrated Care Model in a Level IIIC Neonatal Intensive Care Unit: A Systematic Approach to the Methods and Effort Taken for Implementation. Front. Pediatr. 2021, 9, 682097. [Google Scholar] [CrossRef]
- Statistics Netherlands. Talen en Dialecten in Nederland. Available online: https://www.cbs.nl/nl-nl/longread/statistische-trends/2021/talen-en-dialecten-in-nederland?onepage=true (accessed on 28 July 2023).


{kind=link}
| Timing | Subject | Outcome | Tool/Unit |
|---|---|---|---|
| Admission 1 | Parents | Parental stress levels 2 | PSS:NICU [31,32] |
| Depression | PROMIS [50,51] | ||
| Anxiety | PROMIS [50,51] | ||
| PTSD | PCL-5 [45,46,48] | ||
| Infant | Baseline characteristics | N/A | |
| Discharge | Parents | Demographics | General questionnaire |
| Parental stress levels | PSS:NICU [31,32] | ||
| SDM | SDM-Q-9 [36,37] | ||
| SDM preference | CPS [39] | ||
| Depression | PROMIS [50,51] | ||
| Anxiety | PROMIS [50,51] | ||
| PTSD | PCL-5 [45,46,48] | ||
| Mothers | Human milk biofactors | See text | |
| Infant | Breastfeeding rates | Index of breastfeeding [52,53] | |
| Length of stay | days | ||
| Growth | Weight gain velocity [54] | ||
| Glucocorticoid receptor methylation rate in buccal mucosal cells | Mquant method [55] | ||
| CA of 3 months of the infant | Parents | Follow-up characteristics | General questionnaire |
| Depression | PROMIS [50,51] | ||
| Anxiety | PROMIS [50,51] | ||
| PTSD | PCL-5 [45,46,48] | ||
| Hair cortisol | LC-MS/MS [56,57] | ||
| Salivary cortisol | LC-MS/MS [56,57] | ||
| Mothers | Human milk biofactors | See text | |
| Infant | Glucocorticoid receptor methylation rate in buccal mucosal cells | Mquant method [55] | |
| Salivary cortisol | LC-MS/MS [56,57] | ||
| CA of 6 months of the infant | Parents | Follow-up characteristics | General questionnaire |
| Depression | PROMIS [50,51] | ||
| Anxiety | PROMIS [50,51] | ||
| PTSD | PCL-5 [45,46,48] | ||
| CA of 12 months of the infant | Infant | Neurodevelopment | ASQ [33,35] |
| Medical costs | iMTA MCQ [58] | ||
| Parents | Follow-up characteristics | General questionnaire | |
| Productivity costs | iMTA PCQ [59] | ||
| Medical costs | iMTA MCQ [58] | ||
| Depression | PROMIS [50,51] | ||
| Anxiety | PROMIS [50,51] | ||
| PTSD | PCL-5 [45,46,48] |
| Timing | Subject | Outcome | Tool/Unit |
|---|---|---|---|
| At start, halfway through and end of study | HCP | Demographics | General questionnaire |
| Work engagement | UWES-9 [61] | ||
| Autonomy | Subscale of JCQ [64] | ||
| SDM | SDM-Q-Doc [37,60] | ||
| Productivity costs | iMTA PCQ [59] | ||
| Organisation | Work absence | Percentages of absenteeism | |
| Parental presence at rounds | No. of parents present, no. of rounds | ||
| Duration of rounds | Minutes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoeben, H.; Alferink, M.T.; van Kempen, A.A.M.W.; van Goudoever, J.B.; van Veenendaal, N.R.; van der Schoor, S.R.D.; on behalf of the neoPARTNER Study Group. Collaborating to Improve Neonatal Care: ParentAl Participation on the NEonatal Ward—Study Protocol of the neoPARTNER Study. Children 2023, 10, 1482. https://doi.org/10.3390/children10091482
Hoeben H, Alferink MT, van Kempen AAMW, van Goudoever JB, van Veenendaal NR, van der Schoor SRD, on behalf of the neoPARTNER Study Group. Collaborating to Improve Neonatal Care: ParentAl Participation on the NEonatal Ward—Study Protocol of the neoPARTNER Study. Children. 2023; 10(9):1482. https://doi.org/10.3390/children10091482
Chicago/Turabian StyleHoeben, Hannah, Milène T. Alferink, Anne A. M. W. van Kempen, Johannes B. van Goudoever, Nicole R. van Veenendaal, Sophie R. D. van der Schoor, and on behalf of the neoPARTNER Study Group. 2023. "Collaborating to Improve Neonatal Care: ParentAl Participation on the NEonatal Ward—Study Protocol of the neoPARTNER Study" Children 10, no. 9: 1482. https://doi.org/10.3390/children10091482