
Childhood Outcomes in Children with and without Cardiac Echogenic Foci: An Electronic Birth Cohort Study in Wales, UK

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Exposure
2.3. Data Linkage and Outcome Definitions
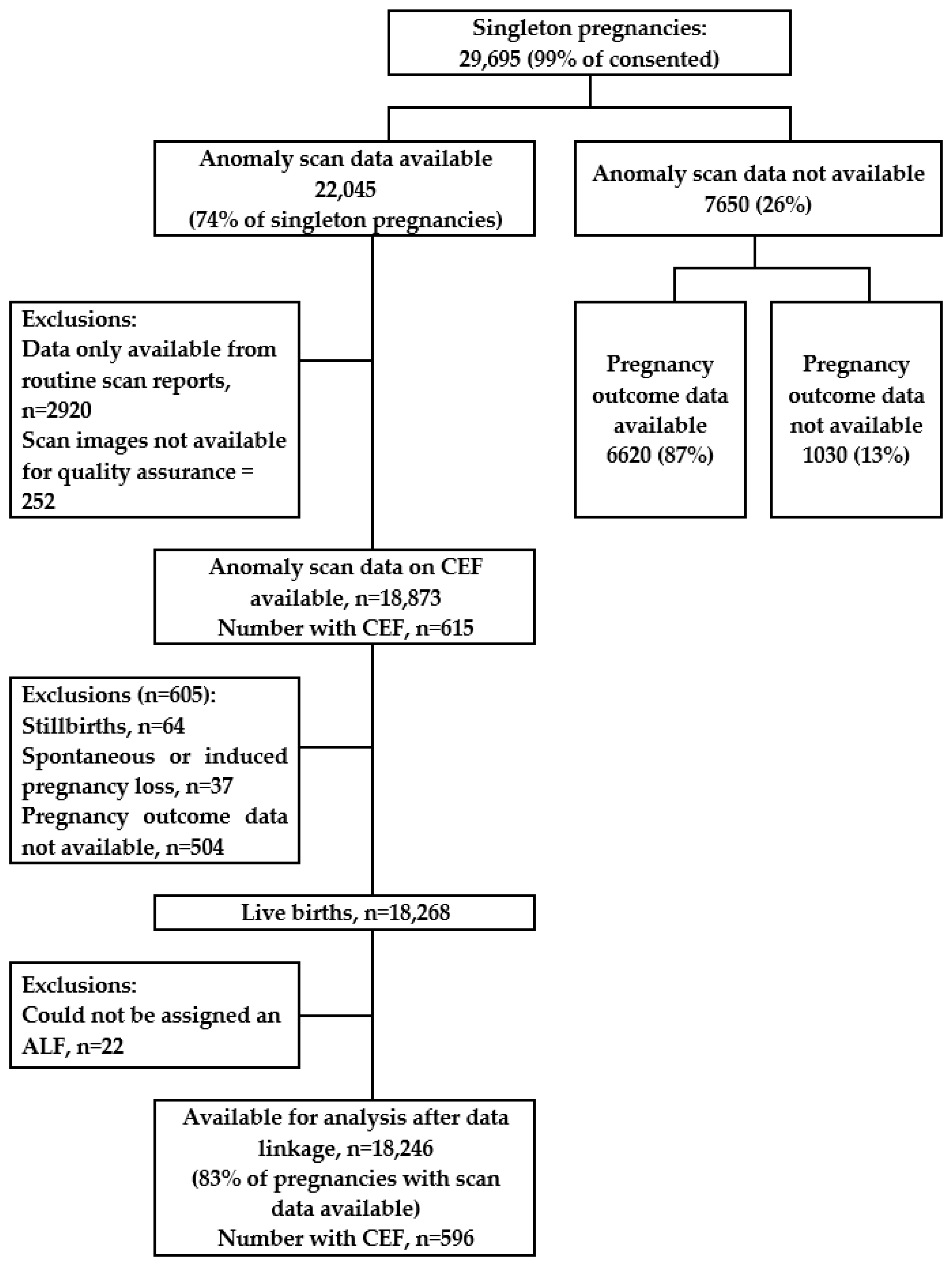
2.4. Statistical Analysis: Inclusion and Exclusion Criteria
2.5. Statistical Analysis: Power Calculations
2.6. Statistical Analysis: Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Calzolari, E.; Barisic, I.; Loane, M.; Morris, J.; Wellesley, D.; Dolk, H.; Addor, M.C.; Arriola, L.; Bianchi, F.; Neville, A.J.; et al. Epidemiology of multiple congenital anomalies in Europe: A EUROCAT population-based registry study. Birth Defects Res. Part A: Clin. Mol. Teratol. 2014, 100, 270–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- British Heart Foundation. Cardiovascular Disease Statistics—British Heart Foundation UK Factsheet. In BHF/Oxford University Analysis of EUROCAT Congenital Anomaly Registers 2010-14; British Heart Foundation: London, UK, 2015. [Google Scholar]
- Van Der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: A systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011, 58, 2241–2247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Bom, T.; Zomer, A.C.; Zwinderman, A.H.; Meijboom, F.J.; Bouma, B.J.; Mulder, B.J.M. The changing epidemiology of congenital heart disease. Nat. Rev. Cardiol. 2011, 8, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Hunter, L.E.; Simpson, J.M. Prenatal screening for structural congenital heart disease. Nat. Rev. Cardiol. 2014, 11, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Salomon, L.J.; Alfirevic, Z.; Berghella, V.; Bilardo, C.M.; Chalouhi, G.E.; Costa, F.D.S.; Hernandez-Andrade, E.; Malinger, G.; Munoz, H.; Paladini, D.; et al. ISUOG Practice Guidelines (updated): Performance of the routine mid-trimester fetal ultrasound scan. Ultrasound Obstet. Gynecol. 2022, 59, 840–856. [Google Scholar] [CrossRef]
- NHS England. 20-Week Screening Scan. Available online: https://www.gov.uk/government/publications/fetal-anomaly-screening-programme-handbook/overview (accessed on 29 May 2023).
- Van Velzen, C.L.; Ket, J.C.; van de Ven, P.M.; Blom, N.A.; Haak, M.C. Systematic review and meta-analysis of the performance of second-trimester screening for prenatal detection of congenital heart defects. Int. J. Gynecol. Obstet. 2018, 140, 137–145. [Google Scholar] [CrossRef]
- Taliento, C.; Salmeri, N.; Greco, P.; Morano, D. Role of sonographic second trimester soft markers in the era of cell-free DNA screening options: A review. Reprod. Med. 2022, 3, 222–234. [Google Scholar] [CrossRef]
- Roberts, D.; Genest, D. Cardiac histologic pathology characteristics of trisomies 13 and 21. Hum. Pathol. 1992, 23, 1130–1140. [Google Scholar] [CrossRef]
- Brown, D.; Roberts, D.; Miller, W. Left ventricular echogenic focus in the fetal heart: Pathologic correlation. J. Ultrasound Med. 1994, 13, 613–616. [Google Scholar] [CrossRef]
- Rodriguez, R.; Herrero, B.; Bartha, J. The continuing enigma of the fetal echogenic intracardiac focus in prenatal ultrasound. Curr. Opin. Obstet. Gynecol. 2013, 25, 145–151. [Google Scholar] [CrossRef]
- Sepulveda, W.; Romero, D. Significance of echogenic foci in the fetal heart. Ultrasound Obstet. Gynecol. 1998, 12, 445–449. [Google Scholar] [CrossRef]
- Lamont, R.; Havutcu, E.; Salgia, S.; Adinkra, P.; Nicholl, R. The association between isolated fetal echogenic cardiac foci on second-trimester ultrasound scan and trisomy 21 in low-risk unselected women. Ultrasound Obstet. Gynecol. 2004, 23, 346–351. [Google Scholar] [CrossRef]
- Ahman, A.; Axelsson, O.; Maras, G.; Rubertsson, C.; Sarkadi, A.; Lindgren, P. Ultrasonographic fetal soft markers in a low-risk population: Prevalence, association with trisomies and invasive tests. Acta Obstet. Et Gynecol. Scand. 2014, 93, 367–373. [Google Scholar] [CrossRef]
- Hurt, L.; Wright, M.; Dunstan, F.; Thomas, S.; Brook, F.; Morris, S.; Tucker, D.; Wills, M.; Davies, C.; John, G.; et al. Prevalence of defined ultrasound findings of unknown significance at the second trimester fetal anomaly scan and their association with adverse pregnancy outcomes: The Welsh study of mothers and babies population-based cohort. Prenat. Diagn. 2015, 36, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Sotiriadis, A.; Makrydimas, G.; Ioannidis, J. Diagnostic performance of intracardiac echogenic foci for Down Syndrome: A meta analysis. Obstet. Gynecol. 2003, 101, 1009–1016. [Google Scholar] [CrossRef]
- Lorente, A.; Moreno-Cid, M.; Rodriguez, M.; Bueno, G.; Tenias, J.; Roman, C.; Arias, A.; Pascual, A. Meta-analysis of validity of echogenic intracardiac foci for calculating the risk of Down syndrome in the second trimester of pregnancy. Taiwan. J. Obstet. Gynecol. 2017, 56, 16–22. [Google Scholar] [CrossRef]
- Norton, M.E.; Biggio, J.R.; Kuller, J.A.; Blackwell, S.C.; Society for Maternal-Fetal Medicine (SMFM). The role of ultrasound in women who undergo cell-free DNA screening. Am. J. Obstet. Gynecol. 2017, 216, B2–B7. [Google Scholar] [CrossRef] [Green Version]
- Hacker, F.M.; Hersh, A.R.; Shaffer, B.L.; Caughey, A.B. Isolated echogenic intracardiac foci and the role of cell-free fetal DNA: A cost-effectiveness analysis. Prenat. Diagn. 2020, 40, 1517–1524. [Google Scholar] [CrossRef]
- Facio, M.C.; Hervías-Vivancos, B.; Broullón, J.R.; Avila, J.; Fajardo-Expósito, M.A.; Bartha, J.L. Cardiac biometry and function in euploid fetuses with intracardiac echogenic foci. Prenat. Diagn. 2012, 32, 113–116. [Google Scholar] [CrossRef]
- Kurtulmus, S.; Mese, T.; Taner, C.; Oztekin, D.; Okyay, D.; Uysal, A.; Uysal, F.; Cingillioglu, B. Evaluation of tissue Doppler-derived myocardial performance index in fetuses with intracardiac echogenic focus. J. Matern. Fetal Neonatal Med. 2013, 26, 1662–1666. [Google Scholar] [CrossRef]
- Yozgat, Y.; Kilic, A.; Ozdemir, R.; Karadeniz, C.; Kucuk, M.; Karaaslan, U.; Mese, T.; Unal, N. Modified myocardial performance index is not affected in fetuses with an isolated echogenic focus in the left ventricle. J. Matern. Fetal Neonatal Med. 2014, 28, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Degani, S.; Leibovitz, Z.; Shapiro, I.; Gonen, R.; Ohel, G. Cardiac function in fetuses with intracardiac echogenic foci. Ultrasound Obstet. Gynecol. 2001, 18, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Prentice, G.; Welsh, A.; Howat, A.; Ross, D.; Henry, A. Isolated ‘soft signs’ of fetal choroid plexus cysts or echogenic intracardiac focus–consequences of their continued reporting. Australas. J. Ultrasound Med. 2019, 22, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Hurt, L.; Wright, M.; Brook, F.; Thomas, S.; Dunstan, F.; Fone, D.; John, G.; Morris, S.; Tucker, D.; Wills, M.; et al. The Welsh study of mothers and babies: Protocol for a population-based cohort study to investigate the clinical significance of defined ultrasound findings of uncertain significance. BMC Pregnancy Childbirth 2014, 14, 164. [Google Scholar] [CrossRef] [Green Version]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, 1628–1655. [Google Scholar] [CrossRef]
- Ford, D.; Jones, K.; Verplancke, J.; Lyons, R.; John, G.; Brown, G.; Brooks, C.; Thompson, S.; Bodger, O.; Couch, T. The SAIL Databank: Building a national architecture for e-health research and evaluation. BMC Health Serv. Res. 2009, 9, 157. [Google Scholar] [CrossRef] [Green Version]
- Lyons, R.; Jones, K.; John, G.; Brooks, C.; Verplancke, J.; Ford, D.; Brown, G.; Leake, K. The SAIL databank: Linking multiple health and social care datasets. BMC Med Inform. Decis. Mak. 2009, 9, 3. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 10th Revision. Available online: https://apps.who.int/iris/handle/10665/246208 (accessed on 29 May 2023).
- Amorim, L.D.; Cai, J. Modelling recurrent events: A tutorial for analysis in epidemiology. Int. J. Epidemiol. 2015, 44, 324–333. [Google Scholar] [CrossRef]
- Townsend, P.; Phillimore, P.; Beattie, A. Health and Deprivation: Inequality and the North; Croom Helm: London, UK, 1988. [Google Scholar]
- White, I.; Royston, P.; Wood, A. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 2011, 30, 377–399. [Google Scholar] [CrossRef]
- White, I.; Royston, P. Imputing missing covariate values for the Cox model. Stat. Med. 2009, 28, 1982–1998. [Google Scholar] [CrossRef] [Green Version]
- StataCorp. Stata Statistical Software: Release 16; StataCorp LLC: College Station, TX, USA, 2019. [Google Scholar]
- Chiu, G.; Zhao, A.; Zhang, B.; Zhang, T. Clinical value of isolated intracardiac echogenic focus in the fetal heart: A retrospective study in Chinese women. Clin. Exp. Obstet. Gynecol. 2019, 46, 972–976. [Google Scholar] [CrossRef]
- Hu, T.; Tian, T.; Zhang, Z.; Wang, J.; Hu, R.; Xiao, L.; Zhu, H.; Lai, Y.; Wang, H.; Liu, S. Prenatal chromosomal microarray analysis in 2466 fetuses with ultrasonographic soft markers: A prospective cohort study. Am. J. Obstet. Gynecol. 2021, 224, 516.e1–516.e16. [Google Scholar] [CrossRef]
- Rose, N.C.; Kaimal, A.J.; Dugoff, L.; Norton, M.E.; American College of Obstetricians and Gynecologists. Screening for fetal chromosomal abnormalities: ACOG practice bulletin, number 226. Obstet. Gynecol. 2020, 136, e48–e69. [Google Scholar]
- Guo, Y.; He, Y.; Gu, X.; Zhang, Y.; Sun, L.; Liu, X.; Zhao, Y.; Han, J. Echogenic intracardiac foci and fetal cardiac anomalies: A review of cases from a tertiary care center in China. J. Clin. Ultrasound 2018, 46, 103–107. [Google Scholar] [CrossRef]
- Bronshtein, M.; Jakobi, P.; Ofir, C. Multiple fetal intracardiac echogenic foci: Not always a benign sonographic finding. Prenat. Diagn. 1996, 16, 131–135. [Google Scholar] [CrossRef]


{kind=link}
| Total | Cardiac Echogenic Foci at the Fetal Anomaly Scan | ||
| No | Yes | ||
| N | N (%) | N (%) | |
| 18,246 | 17,650 (96.7) | 596 (3.3) | |
| Sex | |||
| Female | 8845 (48.5%) | 8559 (48.5) | 286 (48.0) |
| Male | 9401 (51.5%) | 9091 (51.5) | 310 (52.0) |
| Maternal age (years) | |||
| <25 | 5384 (29.5%) | 5169 (29.3) | 215 (36.0) |
| 25–34 | 10,075 (55.2%) | 9779 (55.4) | 296 (49.7) |
| 35+ | 2787 (15.3%) | 2702 (15.3) | 85 (14.3) |
| Townsend Score * | |||
| 1 | 2962 (16.4%) | 2878 (16.4) | 84 (14.1) |
| 2 | 2964 (16.4%) | 2880 (16.5) | 84 (14.1) |
| 3 | 3586 (19.8%) | 3466 (19.8) | 120 (20.1) |
| 4 | 4248 (23.5%) | 4117 (23.5) | 131 (22.0) |
| 5 | 4342 (24.0%) | 4165 (23.8) | 177 (29.7) |
| Birth by Caesarean Section ** | |||
| Yes | 4517 (25.0%) | 4383 (25.1) | 134 (22.5) |
| No | 13,558 (75.0%) | 13,097 (74.9) | 461 (77.5) |
| Preterm birth † | |||
| Yes | 966 (5.3%) | 922 (5.2) | 44 (7.4) |
| No | 17,237 (94.7%) | 16,687 (94.8) | 550 (92.6) |
| Conditional HR, Any Admission * (95% CI) | p Value | Conditional HR, Multiple Admissions ** (95% CI) | p Value | |
|---|---|---|---|---|
| Hospital admissions with all cardiac codes | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 0.82 (0.44, 1.55) | 0.547 | 0.87 (0.33, 2.25) | 0.768 |
| No CEF | No cardiac admissions in multiple marker group | |||
| Isolated CEF | ||||
| CEF with another marker | ||||
| Congenital Cardiac Anomaly and All Congenital Anomaly Cases | ||||
| Univariate OR (95% CI) | p Value | Conditional OR (95% CI) * | p Value | |
| Congenital cardiac anomalies | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 1.32 (0.69, 2.49) | 0.400 | 1.19 (0.62, 2.28) | 0.593 |
| No CEF | No congenital cardiac anomalies in the multiple marker group | |||
| Isolated CEF | ||||
| CEF with another marker | ||||
| Any congenital anomalies | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 1.14 (0.82, 1.59) | 0.440 | 1.08 (0.77, 1.51) | 0.671 |
| No CEF | Cannot be presented because n < 5 in some cells | 1.00 | ||
| Isolated CEF | 1.01 (0.71, 1.44) | 0.958 | ||
| CEF with another marker ** | 5.03 (1.26, 20.10) | 0.022 | ||
| Hospital admissions with congenital cardiac anomaly and all congenital anomaly codes | ||||
| Conditional HR, | p value | Conditional HR, multiple admissions †† (95% CI) | p value | |
| any admission † | ||||
| (95% CI) | ||||
| Hospital admissions with congenital cardiac anomaly codes ‡ | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 1.06 (0.50, 2.26) | 0.886 | 1.16 (0.38, 3.52) | 0.793 |
| No CEF | No congenital cardiac admissions in multiple marker group | |||
| Isolated CEF | ||||
| CEF with another marker | ||||
| Hospital admissions with any congenital anomaly codes ‡‡ | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 1.13 (0.80, 1.60) | 0.491 | 0.93 (0.55, 1.58) | 0.803 |
| No CEF | 1.00 | 1.00 | ||
| Isolated CEF | 1.08 (0.76, 1.55) | 0.661 | 0.90 (0.52, 1.56) | 0.707 |
| CEF with another marker | 3.39 (0.84, 13.61) | 0.085 | 2.63 (0.72, 9.65) | 0.143 |
| Conditional HR, Any Admission * (95% CI) | p Value | Conditional HR, Multiple Admissions ** (95% CI) | p Value | |
|---|---|---|---|---|
| Hospital admissions with a code for respiratory illnesses † | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 1.08 (0.93, 1.26) | 0.325 | 1.27 (1.04, 1.54) | 0.020 |
| No CEF | 1.00 | 1.00 | ||
| Isolated CEF | 1.10 (0.94, 1.28) | 0.244 | 1.27 (1.05, 1.56) | 0.015 |
| CEF with another marker | 0.31 (0.04, 2.23) | 0.248 | 0.56 (0.10, 3.22) | 0.520 |
| Hospital admissions with a code for any neoplasms (benign and malignant) †† | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 0.60 (0.15, 2.43) | 0.472 | 0.32 (0.05, 1.98) | 0.220 |
| No CEF | No neoplasm admissions in multiple marker group | |||
| Isolated CEF | ||||
| CEF with another marker | ||||
| Hospital admissions with a code for benign neoplasms ‡ | ||||
| No CEF | 1.00 | 1.00 | ||
| CEF | 0.70 (0.17, 2.85) | 0.619 | 1.15 (0.17, 7.79) | 0.885 |
| No CEF | No neoplasm admissions in multiple marker group | |||
| Isolated CEF | ||||
| CEF with another marker | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hurt, L.; Uzun, O.; Morris, S.; Bethel, J.; Evans, A.; Seaborne, M.; Daniel, R.; Brophy, S.; Paranjothy, S. Childhood Outcomes in Children with and without Cardiac Echogenic Foci: An Electronic Birth Cohort Study in Wales, UK. Children 2023, 10, 1233. https://doi.org/10.3390/children10071233
Hurt L, Uzun O, Morris S, Bethel J, Evans A, Seaborne M, Daniel R, Brophy S, Paranjothy S. Childhood Outcomes in Children with and without Cardiac Echogenic Foci: An Electronic Birth Cohort Study in Wales, UK. Children. 2023; 10(7):1233. https://doi.org/10.3390/children10071233
Chicago/Turabian StyleHurt, Lisa, Orhan Uzun, Susan Morris, Jackie Bethel, Annette Evans, Michael Seaborne, Rhian Daniel, Sinead Brophy, and Shantini Paranjothy. 2023. "Childhood Outcomes in Children with and without Cardiac Echogenic Foci: An Electronic Birth Cohort Study in Wales, UK" Children 10, no. 7: 1233. https://doi.org/10.3390/children10071233