
Repeated Etching Cycles of Resin Infiltration up to Nine Cycles on Demineralized Enamel: Surface Roughness and Esthetic Outcomes—In Vitro Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
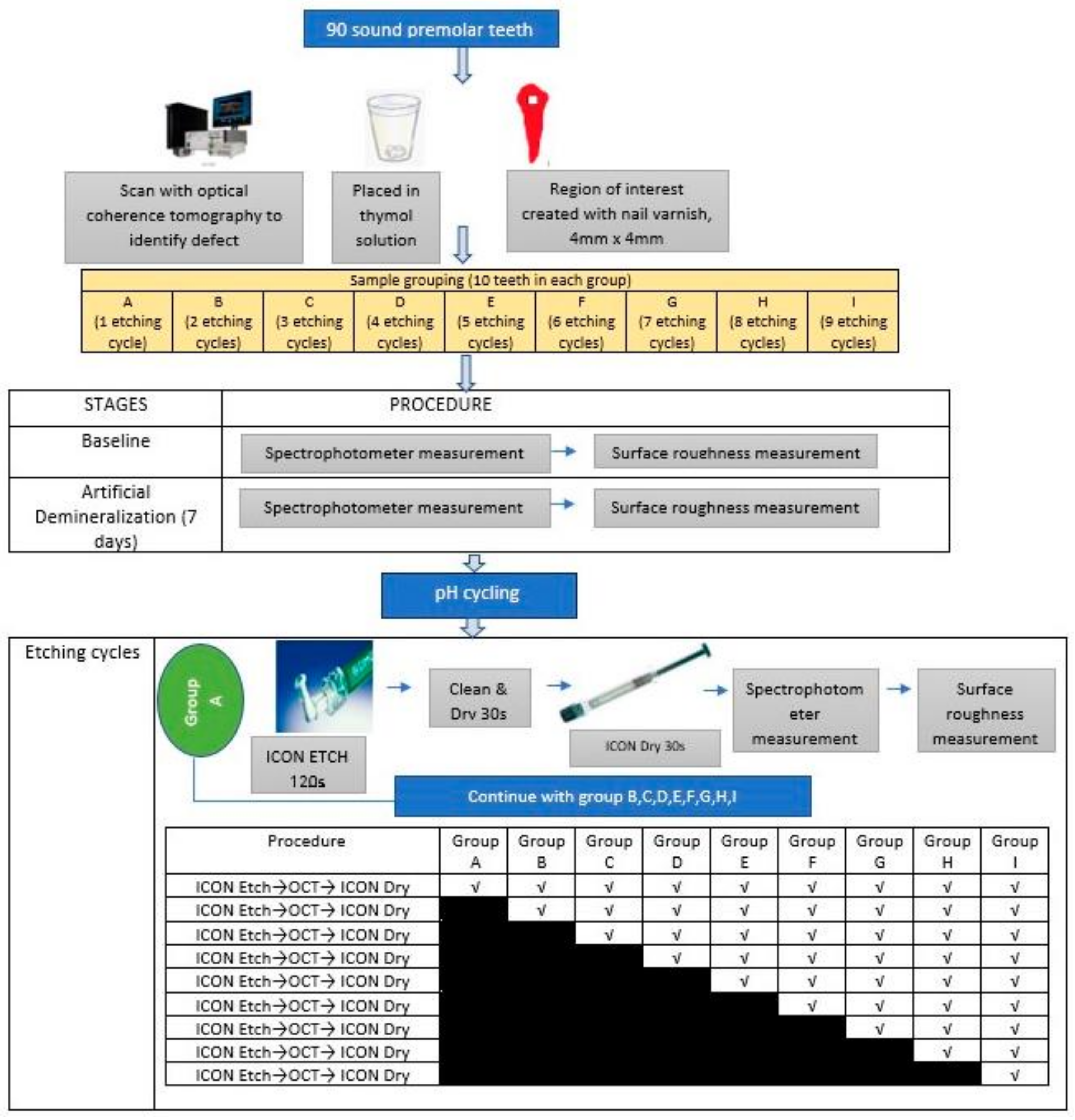
2.1. Study Design and Sample Preparation
2.2. Artificial Demineralization
2.3. pH Cycling
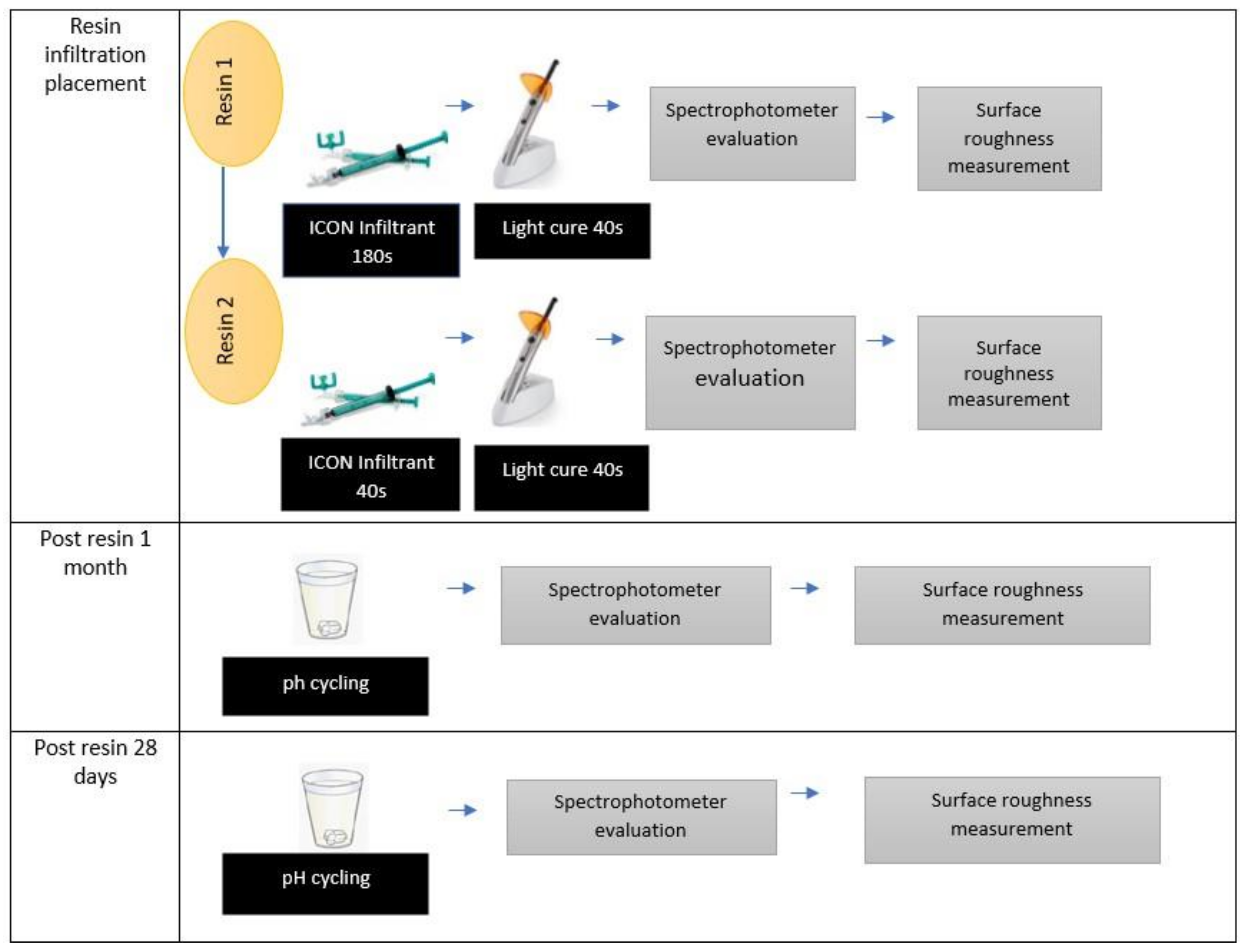
2.4. Resin Infiltration Applications
2.5. Surface Roughness
2.6. Esthetics
2.7. Statistical Analysis
3. Results
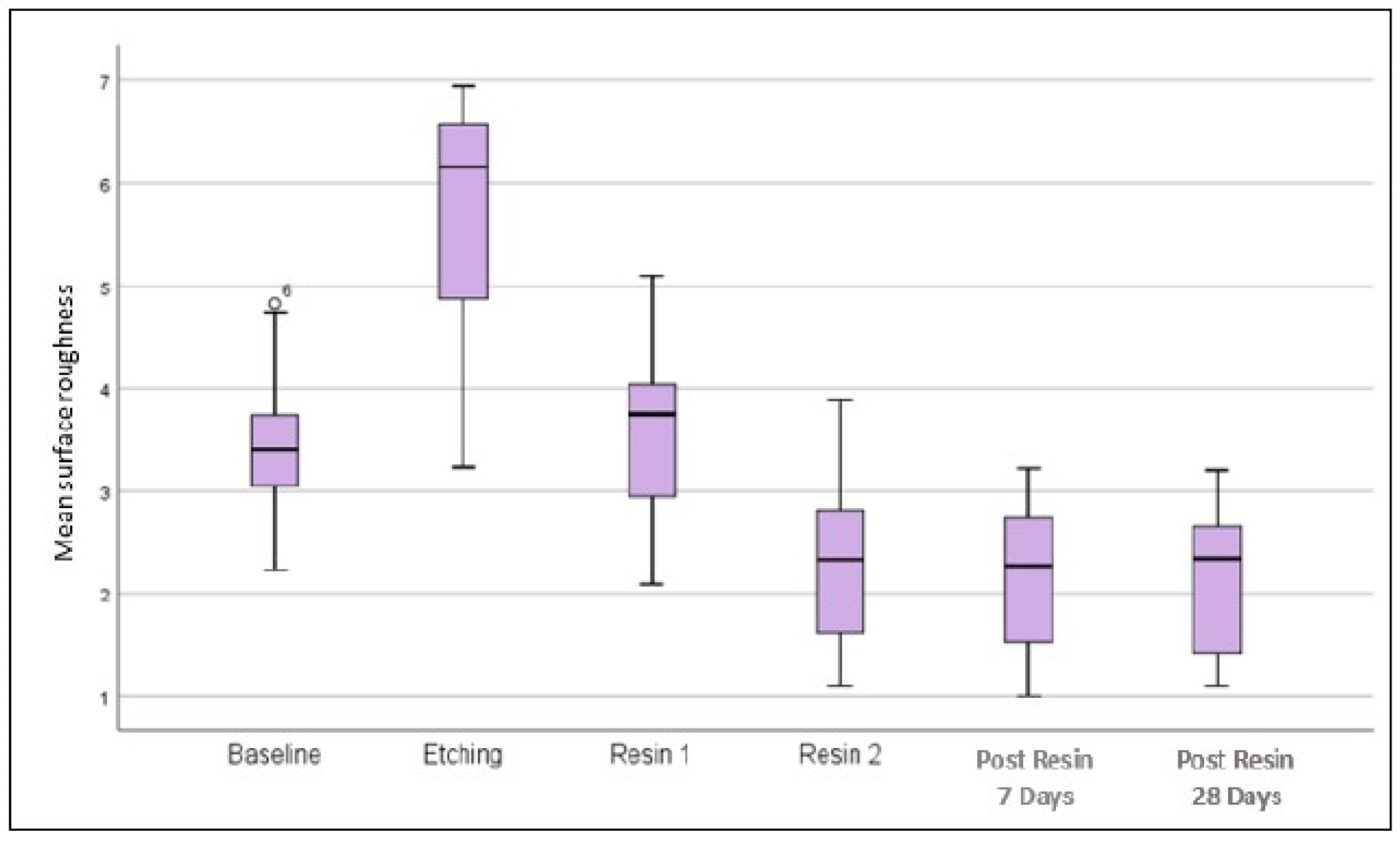
3.1. Surface Roughness
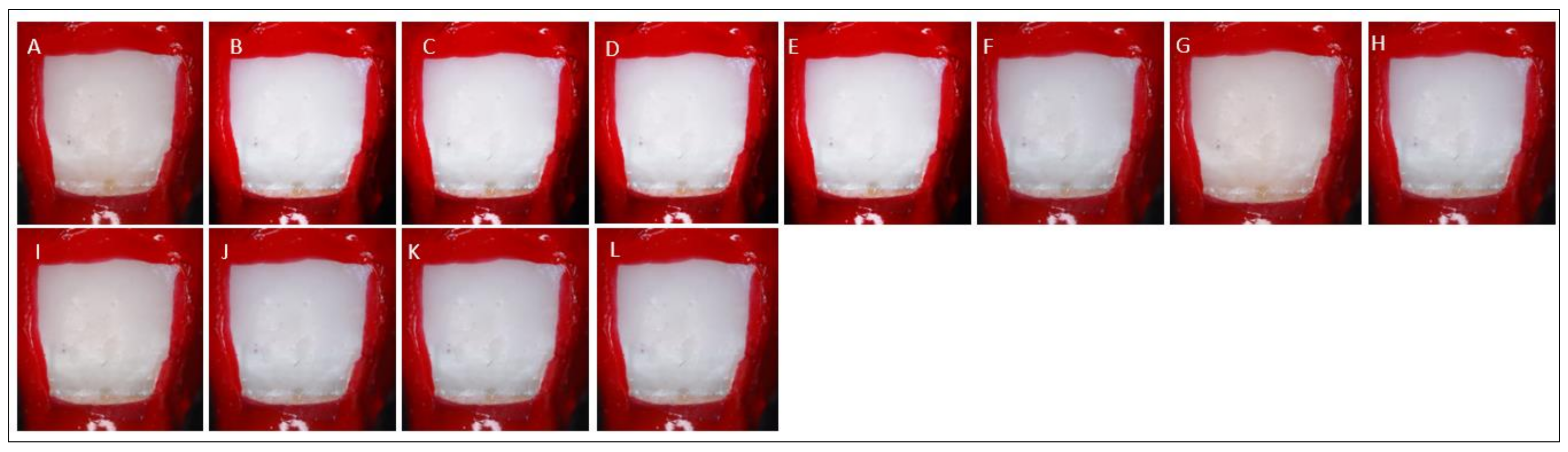
3.2. Esthetic
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Desai, H.; Stewart, C.A.; Finer, Y. Minimally Invasive Therapies for the Management of Dental Caries—A Literature Review. Dent. J. 2021, 9, 147. [Google Scholar] [CrossRef]
- Featherstone, J.D.B.; Crystal, Y.O.; Alston, P.; Chaffee, B.W.; Doméjean, S.; Rechmann, P.; Zhan, L.; Ramos-Gomez, F. Evidence-Based Caries Management for All Ages-Practical Guidelines. Front. Oral Health 2021, 2, 657518. [Google Scholar] [CrossRef] [PubMed]
- Flemming, J.; Hannig, C.; Hannig, M. Caries Management—The Role of Surface Interactions in De- and Remineralization-Processes. J. Clin. Med. 2022, 11, 7044. [Google Scholar] [CrossRef] [PubMed]
- Yu, O.Y.; Lam, W.Y.-H.; Wong, A.W.-Y.; Duangthip, D.; Chu, C.-H. Nonrestorative Management of Dental Caries. Dent. J. 2021, 9, 121. [Google Scholar] [CrossRef]
- Allen, D.N.; Fine, C.M.; Newton, M.N.; Kabani, F.; Muzzin, K.B.; Reed, K.M. Resin Infiltration Therapy: A micro-invasive treatment approach for white spot lesions. J. Dent. Hyg. 2021, 95, 31–35. [Google Scholar]
- Dziaruddin, N.; Zakaria, A.S.I. Resin Infiltration of Non-Cavitated Enamel Lesions in Paediatric Dentistry: A Narrative Review. Children 2022, 9, 1893. [Google Scholar] [CrossRef]
- Lin, G.S.S.; Chan, D.Z.K.; Lee, H.Y.; Low, T.T.; Laer, T.S.; Pillai, M.P.M.; Yew, Y.Q.; Wafa, S.W.W.S.S.T. Effectiveness of resin infiltration in caries inhibition and aesthetic appearance improvement of white-spot lesions: An umbrella review. J. Evid. Based Dent. Pract. 2022, 22, 101723. [Google Scholar] [CrossRef]
- Bourouni, S.; Dritsas, K.; Kloukos, D.; Wierichs, R.J. Efficacy of resin infiltration to mask post-orthodontic or non-post-orthodontic white spot lesions or fluorosis—A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 4711–4719. [Google Scholar] [CrossRef]
- Soveral, M.; Machado, V.; Botelho, J.; Mendes, J.J.; Manso, C. Effect of Resin Infiltration on Enamel: A Systematic Review and Meta-Analysis. J. Funct. Biomater. 2021, 12, 48. [Google Scholar] [CrossRef] [PubMed]
- Hasmun, N.; Lawson, J.; Vettore, M.V.; Elcock, C.; Zaitoun, H.; Rodd, H. Change in Oral Health-Related Quality of Life Following Minimally Invasive Aesthetic Treatment for Children with Molar Incisor Hypomineralisation: A Prospective Study. Dent. J. 2018, 6, 61. [Google Scholar] [CrossRef] [Green Version]
- Yazkan, B.; Ermis, R.B. Effect of resin infiltration and microabrasion on the microhardness, surface roughness and morphology of incipient carious lesions. Acta Odontol. Scand. 2018, 76, 473–481. [Google Scholar] [CrossRef]
- Taher, N.M. Atomic force microscopy and tridimensional topography analysis of human enamel after resinous infiltration and storage in water. Saudi Med. J. 2013, 34, 408–414. [Google Scholar]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: Simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Med. 2021, 31, 010502. [Google Scholar] [CrossRef] [PubMed]
- Yu, O.Y.; Zhao, I.S.; Mei, M.L.; Lo, E.C.-M.; Chu, C.-H. A Review of the Common Models Used in Mechanistic Studies on Demineralization-Remineralization for Cariology Research. Dent. J. 2017, 5, 20. [Google Scholar] [CrossRef] [Green Version]
- Amaechi, B.T. Protocols to Study Dental Caries In Vitro: pH Cycling Models. Methods Mol. Biol. 2019, 1922, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Bak, S.Y.; Kim, Y.; Hyun, H.K. Color change of white spot lesions after resin infiltration. COLOR Res. Appl. 2014, 39, 506–510. [Google Scholar] [CrossRef]
- Paris, S.; Bitter, K.; Krois, J.; Meyer-Lueckel, H. Seven-year-efficacy of proximal caries infiltration—Randomized clinical trial. J. Dent. 2020, 93, 103277. [Google Scholar] [CrossRef]
- Mian, M.J.; Razmi, J.; Ladani, L. Grain Scale Investigation of the Mechanical Anisotropic Behavior of Electron Beam Powder Bed Additively Manufactured Ti6Al4V Parts. Metals 2022, 12, 163. [Google Scholar] [CrossRef]
- Saegusa, M.; Kurokawa, H.; Takahashi, N.; Takamizawa, T.; Ishii, R.; Shiratsuchi, K.; Miyazaki, M. Evaluation of Color-matching Ability of a Structural Colored Resin Composite. Oper. Dent. 2021, 46, 306–315. [Google Scholar] [CrossRef]
- Arnold, W.H.; Haddad, B.; Schaper, K.; Hagemann, K.; Lippold, C.; Danesh, G. Enamel surface alterations after repeated conditioning with HCl. Head Face Med. 2015, 11, 32. [Google Scholar] [CrossRef] [Green Version]
- Taher, N.M.; Alkhamis, H.A.; Dowaidi, S.M. The influence of resin infiltration system on enamel microhardness and surface roughness: An in vitro study. Saudi Dent. J. 2012, 24, 79–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Risnes, S.; Li, C. On the method of revealing enamel structure by acid etching. Aspects of optimization and interpretation. Microsc. Res. Tech. 2019, 82, 1668–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aswani, R.; Chandrappa, V.; Uloopi, K.S.; Chandrasekhar, R.; RojaRamya, K.S. Resin Infiltration of Artificial Enamel Lesions: Evaluation of Penetration Depth, Surface Roughness and Color Stability. Int. J. Clin. Pediatr. Dent. 2019, 12, 520–523. [Google Scholar] [CrossRef]
- Harsha, L.; Subramanian, A.K. Comparative Assessment of pH and Degree of Surface Roughness of Enamel When Etched with Five Commercially Available Etchants: An In Vitro Study. J. Contemp. Dent. Pract. 2022, 23, 181–185. [Google Scholar]
- Tsai, M.-T.; Wang, Y.-L.; Yeh, T.-W.; Lee, H.-C.; Chen, W.-J.; Ke, J.-L.; Lee, Y.-J. Early detection of enamel demineralization by optical coherence tomography. Sci. Rep. 2019, 9, 17154. [Google Scholar] [CrossRef] [Green Version]
- El Meligy, O.A.E.S.; Alamoudi, N.M.; Eldin Ibrahim, S.T.; Felemban, O.M.; Al-Tuwirqi, A.A. Effect of resin infiltration application on early proximal caries lesions in vitro. J. Dent. Sci. 2021, 16, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Saccucci, M.; Corridore, D.; Di Carlo, G.; Bonucci, E.; Cicciù, M.; Vozza, I. Assessment of Enamel Color Stability of Resins Infiltration Treatment in Human Teeth: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 11269. [Google Scholar] [CrossRef]
- Wierichs, R.J.; Langer, F.; Kobbe, C.; Abou-Ayash, B.; Esteves-Oliveira, M.; Wolf, M.; Knaup, I.; Meyer-Lueckel, H. Aesthetic caries infiltration—Long-term masking efficacy after 6 years. J. Dent. 2023, 132, 104474. [Google Scholar] [CrossRef]
- Abbas, B.A.; Marzouk, E.S.; Zaher, A.R. Treatment of various degrees of white spot lesions using resin infiltration-in vitro study. Prog. Orthod. 2018, 19, 27. [Google Scholar] [CrossRef] [Green Version]
- de Oliveira Correia, A.M.; Bühler Borges, A.; Torres, C.R.G. Color masking prediction of posterior white spot lesions by resin infiltration in vitro. J. Dent. 2020, 95, 103308. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Stages (Mean ± SD) | |||||
|---|---|---|---|---|---|---|
| Baseline | Etching | Resin 1 | Resin 2 | Post Resin 7 Days | Post Resin 28 Days | |
| 1 | 2.31 ± 0.064 | 3.64 ± 0.612 | 3.03 ± 0.664 | 1.53 ± 0.22 | 1.37 ± 0.195 | 1.34 ± 0.073 |
| 2 | 3.37 ± 0.225 | 4.37 ± 0.225 | 3.39 ± 0.492 | 1.54 ± 0.626 | 1.44 ± 0.569 | 1.49 ± 0.332 |
| 3 | 3.29 ± 0.153 | 4.96 ± 0.992 | 3.57 ± 0.216 | 1.74 ± 0.419 | 1.74 ± 0.467 | 1.74 ± 0.607 |
| 4 | 3.17 ± 0.737 | 5.51 ± 0.208 | 4.39 ± 0.367 | 1.95 ± 0.367 | 1.86 ± 0.467 | 1.96 ± 0.417 |
| 5 | 4.09 ± 0.429 | 6.21 ± 0.413 | 5.06 ± 0.724 | 2.54 ± 0.182 | 2.2 ± 0.049 | 2.62 ± 0.01 |
| 6 | 4.09 ± 1.364 | 6.31 ± 0.246 | 5.39 ± 0.63 | 2.67 ± 0.968 | 2.71 ± 0.968 | 2.64 ± 0.968 |
| 7 | 4.43 ± 0.238 | 6.44 ± 0.203 | 6.39 ± 0.358 | 2.87 ± 0.09 | 2.62 ± 0.395 | 2.81 ± 0.13 |
| 8 | 4.77 ± 0.737 | 6.56 ± 0.391 | 7.39 ± 0.196 | 2.44 ± 0.408 | 2.63 ± 0.075 | 2.26 ± 0.122 |
| 9 | 5.11 ± 0.537 | 6.59 ± 0.379 | 2.69 ± 0.313 | 3.44 ± 0.725 | 2.85 ± 0.458 | 2.77 ± 0.575 |
| Source | SS | df | MS | f | p-Value |
|---|---|---|---|---|---|
| Interaction stages and etching group | 46.334 | 48 | 0.965 | 3.48 | <0.001 * |
| Stages | 53.633 | 8 | 6.704 | 24.17 | <0.001 * |
| Etching group | 277.881 | 6 | 46.313 | 166.974 | <0.001 * |
| Group | Stages (Mean ± SD) | |||||
|---|---|---|---|---|---|---|
| Baseline | Etching | Resin 1 | Resin 2 | Post Resin 7 Days | Post Resin 28 Days | |
| 1 | 2.95 ± 0.06 | 3.64 ± 0.306 | 2.56 ± 0.905 | 1.83 ± 0.577 | 1.82 ± 0.811 | 1.72 ± 0.639 |
| 2 | 2.49 ± 0.81 | 4.37 ± 0.026 | 2.34 ± 0.279 | 1.74 ± 1.671 | 1.68 ± 0.446 | 1.72 ± 0.537 |
| 3 | 2.31 ± 0.104 | 4.96 ± 0.002 | 2.06 ± 0.329 | 1.68 ± 0.032 | 1.61 ± 0.272 | 1.69 ± 0.499 |
| 4 | 1.97 ± 0.012 | 5.51 ± 0.034 | 1.89 ± 0.974 | 1.63 ± 0.758 | 1.58 ± 0.375 | 1.67 ± 2.67 |
| 5 | 2.14 ± 1.209 | 6.21 ± 0.046 | 1.71 ± 0.172 | 1.58 ± 0.117 | 1.55 ± 0.484 | 1.64 ± 0.23 |
| 6 | 2.04 ± 0.353 | 6.51 ± 0.06 | 1.56 ± 0.095 | 1.53 ± 0.608 | 1.51 ± 0.305 | 1.64 ± 0.029 |
| 7 | 2.27 ± 0.196 | 6.52 ± 1.306 | 1.65 ± 0.057 | 1.48 ± 0.305 | 1.46 ± 0.703 | 1.54 ± 0.029 |
| 8 | 2.5 ± 0.433 | 6.53 ± 0.007 | 1.56 ± 0.046 | 1.44 ± 0.561 | 1.4 ± 0.34 | 1.14 ± 0.573 |
| 9 | 1.89 ± 0.234 | 6.54 ± 0.052 | 1.34 ± 0.833 | 1.3 ± 0.23 | 1.32 ± 0.499 | 1.19 ± 1.508 |
| Source | SS | df | MS | f | p-Value |
|---|---|---|---|---|---|
| Interaction stages and etching group | 46.334 | 4 | 0.965 | 1.177 | 0.045 * |
| Stages | 53.974 | 8 | 6.704 | 12.32 | <0.001 * |
| Etching group | 24.17 | 6 | 46.313 | 122.17 | <0.001 * |
| Etching Cycle (I) | Etching Cycle (J) | Mean (I − J) | Std. Error | p-Value |
|---|---|---|---|---|
| 1 | 2 | 3.557 | 0.272 | <0.0001 * |
| 3 | 5.162 | 0.272 | <0.0001 * | |
| 4 | 3.883 | 0.272 | <0.0001 * | |
| 5 | 3.751 | 0.272 | <0.0001 * | |
| 6 | 5.952 | 0.27 | <0.0001 * | |
| 7 | 5.717 | 0.272 | <0.0001 * | |
| 8 | 6.345 | 0.272 | <0.0001 * | |
| 9 | 6.908 | 0.272 | <0.0001 * | |
| 2 | 3 | 1.605 | 0.272 | 0.001 * |
| 4 | 0.327 | 0.272 | <0.0001 * | |
| 5 | 0.194 | 0.272 | <0.0001 * | |
| 6 | 2.395 | 0.272 | <0.0001 * | |
| 7 | 2.161 | 0.27 | <0.0001 * | |
| 8 | 2.789 | 0.272 | <0.0001 * | |
| 9 | 3.352 | 0.272 | <0.0001 * | |
| 3 | 4 | −1.278 | 0.272 | 0.007 * |
| 5 | −1.411 | 0.272 | 0.002 * | |
| 6 | 0.79 | 0.272 | <0.0001 * | |
| 7 | 0.555 | 0.272 | <0.0001 * | |
| 8 | 1.183 | 0.272 | <0.0001 * | |
| 9 | 1.746 | 0.272 | <0.0001 * | |
| 4 | 7 | 1.834 | 0.272 | <0.0001 * |
| 8 | 2.462 | 0.272 | <0.0001 * | |
| 9 | 3.025 | 0.272 | <0.0001 * | |
| 5 | 1 | 1.966 | 0.272 | <0.0001 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ibrahim, D.F.A.; Hasmun, N.N.; Liew, Y.M.; Venkiteswaran, A. Repeated Etching Cycles of Resin Infiltration up to Nine Cycles on Demineralized Enamel: Surface Roughness and Esthetic Outcomes—In Vitro Study. Children 2023, 10, 1148. https://doi.org/10.3390/children10071148
Ibrahim DFA, Hasmun NN, Liew YM, Venkiteswaran A. Repeated Etching Cycles of Resin Infiltration up to Nine Cycles on Demineralized Enamel: Surface Roughness and Esthetic Outcomes—In Vitro Study. Children. 2023; 10(7):1148. https://doi.org/10.3390/children10071148
Chicago/Turabian StyleIbrahim, Dayang Fadzlina Abang, Noren Nor Hasmun, Yih Miin Liew, and Annapurny Venkiteswaran. 2023. "Repeated Etching Cycles of Resin Infiltration up to Nine Cycles on Demineralized Enamel: Surface Roughness and Esthetic Outcomes—In Vitro Study" Children 10, no. 7: 1148. https://doi.org/10.3390/children10071148