
Maternal Infection and Preterm Birth: From Molecular Basis to Clinical Implications
 , , , , , and
, , , , , and 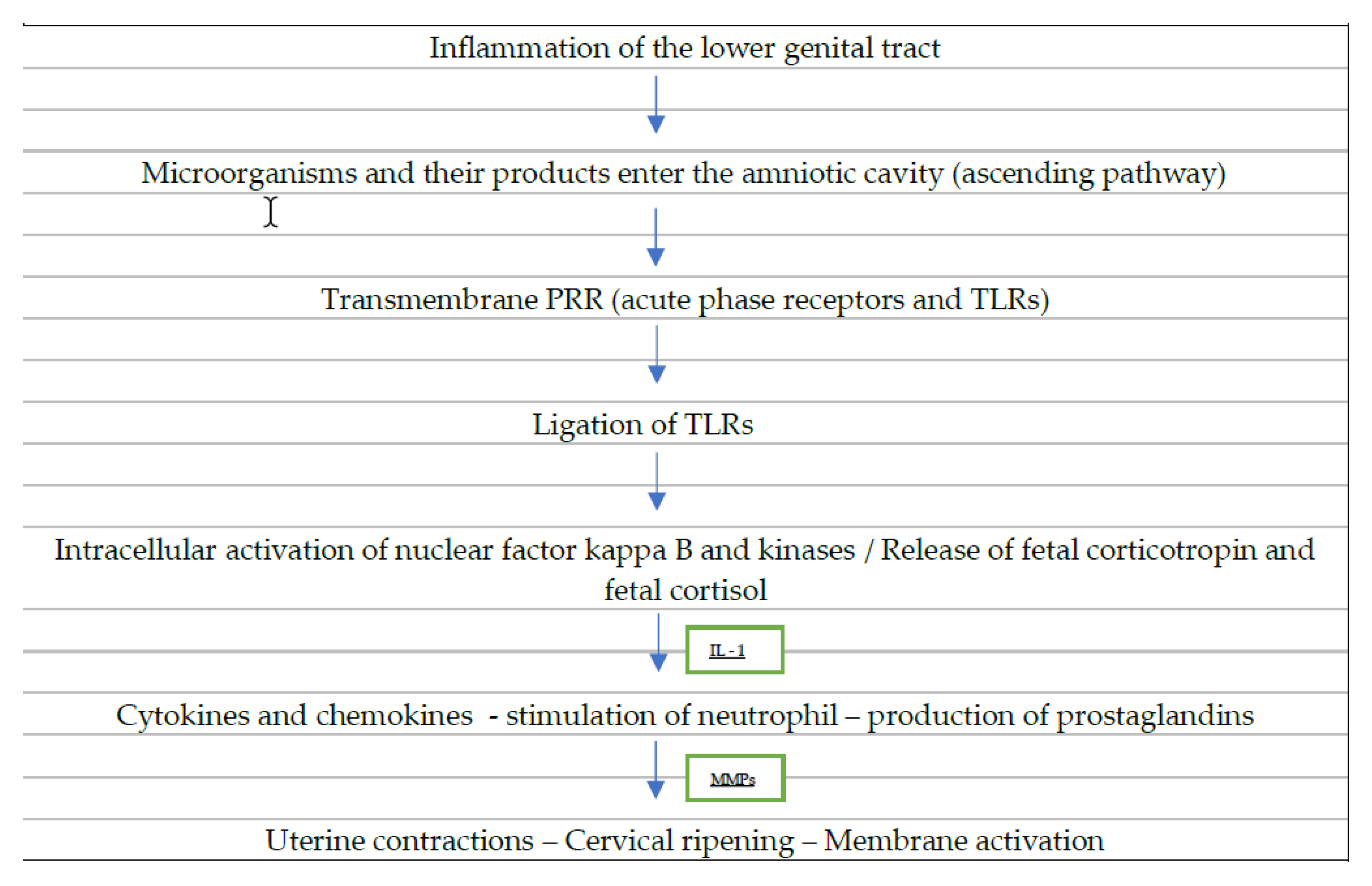{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Inflammation in Labor and Preterm Labor
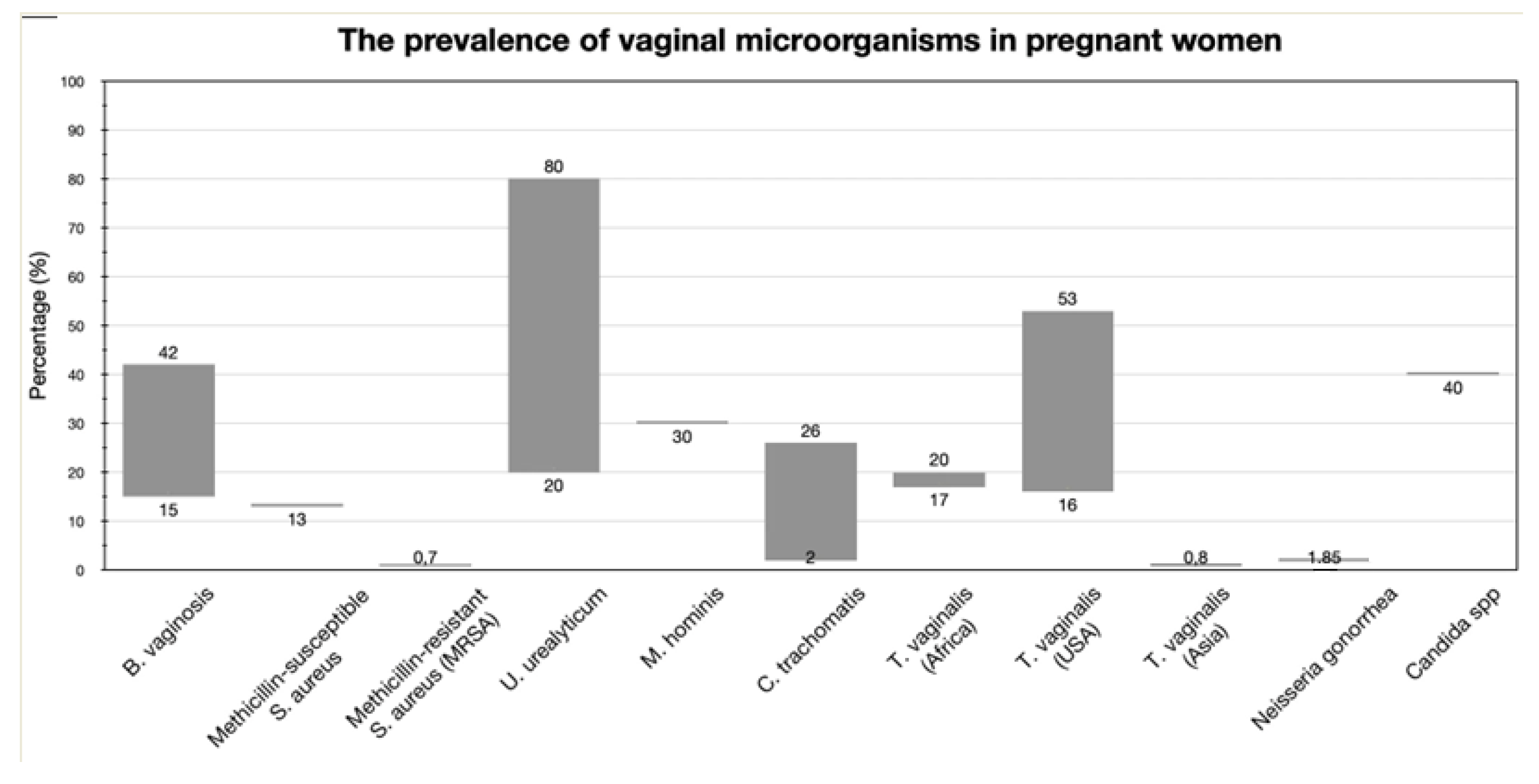
3. Specific Infectious Organisms
3.1. Bacterial Vaginosis (BV)
3.2. Staphylococcus aureus
3.3. Genital Mycoplasmas
Sexually Transmitted Infections
3.4. Chlamydia trachomatis
3.5. Trichomonas vaginalis
3.6. Neisseria gonorrhoeae
3.7. Actinomyces
3.8. Candida Species
3.9. Campylobacter, Salmonella, and Yersinia
3.10. Sneathia
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lawn, J.E.; Cousens, S.; Zupan, J. 4 million neonatal deaths: When? Where? Why? Lancet 2005, 365, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef]
- Jenkins-Manning, S.; Flenady, V.; Dodd, J.; Cincotta, R.; Crowther, C. Care of women at risk of preterm birth: A survey of reported practice in Australia and New Zealand. Aust. N. Z. J. Obstet. Gynaecol. 2006, 46, 546–548. [Google Scholar] [CrossRef]
- Morken, N.H.; Källen, K.; Hagberg, H.; Jacobsson, B. Preterm birth in Sweden 1973–2001: Rate, subgroups, and effect of changing patterns in multiple births, maternal age, and smoking. Acta Obstet. Gynecol. Scand. 2005, 84, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.A.; Hamilton, B.E.; Sutton, P.D.; Ventura, S.J.; Menacker, F.; Kirmeyer, S.; Munson, M.L. Births: Final data for 2005. Natl. Vital Stat. Rep. 2007, 56, 1–103. [Google Scholar] [PubMed]
- Delnord, M.; Blondel, B.; Zeitlin, J. What contributes to disparities in the preterm birth rate in European countries? Curr. Opin. Obstet. Gynecol. 2015, 27, 133. [Google Scholar] [CrossRef]
- Vlachadis, N.; Kornarou, E.; Ktenas, E. The preterm births epidemic in Greece. Acta Obstet. Et Gynecol. Scand. 2013, 92, 1231. [Google Scholar] [CrossRef]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.; Curtin, S.C.; Matthews, T.J. Births: Final data for 2013. Natl. Vital. Stat. Rep. 2015, 64, 1–65. [Google Scholar]
- National Center for Health Statistics. Final Natality Data. 2012. Available online: www.marchofdimes.com/peristats (accessed on 5 April 2023).
- Tucker, J.M.; Goldenberg, R.L.; Davis, R.O.; Copper, R.L.; Winkler, C.L.; Hauth, J.C. Etiologies of preterm birth in an indigent population: Is prevention a logical expectation? Obstet. Gynecol. 1991, 77, 343–347. [Google Scholar]
- Meis, P.J.; Goldenberg, R.L.; Mercer, B.M.; Iams, J.D.; Moawad, A.H.; Miodovnik, M.; Menard, M.K.; Caritis, S.N.; Thurnau, G.R.; Bottoms, S.F.; et al. The preterm prediction study: Risk factors for indicated preterm births. Am. J. Obstet. Gynecol. 1998, 178, 562–567. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Subramaniam, A.; Abramovici, A.; Andrews, W.W.; Tita, A.T. Antimicrobials for preterm birth prevention: An overview. Infect. Dis. Obstet. Gynecol. 2012, 2012, 157159. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, R.L.; Hauth, J.C.; Andrews, W.W. Intrauterine infection and preterm delivery. N. Engl. J. Med. 2000, 342, 1500–1507. [Google Scholar] [CrossRef]
- Tita, A.T.N.; Andrews, W.W. Diagnosis and management of clinical chorioamnionitis. Clin. Perinatol. 2010, 37, 339–354. [Google Scholar] [CrossRef]
- Romero, R.; Espinoza, J.; Gonçalves, L.F.; Kusanovic, J.P.; Friel, L.; Hassan, S. The role of inflammation and infection in preterm birth. Semin. Reprod. Med. 2007, 25, 21–39. [Google Scholar] [CrossRef]
- Pararas, M.V.; Skevaki, C.L.; Kafetzis, D.A. Preterm birth due to maternal infection: Causative pathogens and modes of prevention. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 25, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Gomez, R.; Ghezzi, F.; Yoon, B.H.; Mazor, M.; Edwin, S.S.; Berry, S.M. A fetal systemic inflammatory response is followed by the spontaneous onset of preterm parturition. Am. J. Obstet. Gynecol. 1998, 179, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Sirtori, M.; Oyarzun, E.; Avila, C.; Mazor, M.; Callahan, R.; Sabo, V.; Athanassiadis, A.P.; Hobbins, J.C. Infection and labor V. Prevalence, microbiology, and clinical significance of intraamniotic infection in women with preterm labor and intact membranes. Am. J. Obstet. Gynecol. 1989, 161, 817–824. [Google Scholar] [CrossRef]
- Lamont, R.F.; Rose, M.; Elder, M.G. Effect of bacterial products on prostaglandin E production by amnion cells. Lancet 1985, 2, 1331–1333. [Google Scholar] [CrossRef]
- Bennett, W.A.; Terrone, D.A.; Rinehart, B.K.; Kassab, S.; Martin, J.N.; Granger, J.P. Intrauterine endotoxin infusion in rat pregnancy induces preterm delivery and increases placental prostaglandin F2alpha metabolite levels. Am. J. Obstet. Gynecol. 2000, 182, 1496–1501. [Google Scholar] [CrossRef]
- Ilievski, V.; Hirsch, E. Synergy between viral and bacterial toll-like receptors leads to amplification of inflammatory responses and preterm labor in the mouse. Biol Reprod. 2010, 83, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Gomez, R.; Ghezzi, F.; Romero, R.; Munoz, H.; Tolosa, J.E.; Rojas, I. Premature Labor and Intra-Amniotic Infection: Clinical Aspects and Role of the Cytokines in Diagnosis and Pathophysiology. Clin Perinatol. 1995, 22, 281–342. [Google Scholar] [CrossRef] [PubMed]
- Yoon, B.H.; Oh, S.Y.; Romero, R.; Shim, S.S.; Han, S.Y.; Park, J.S.; Jun, J.K. An elevated amniotic fluid matrix metalloproteinase-8 level at the time of mid-trimester genetic amniocentesis is a risk factor for spontaneous preterm delivery. Am. J. Obstet. Gynecol. 2001, 185, 1162–1167. [Google Scholar] [CrossRef]
- Benedetti, T.J.; Valle, R.; Ledger, W.J. Antepartum pneumonia in pregnancy. Am. J. Obstet. Gynecol. 1982, 144, 413–417. [Google Scholar] [CrossRef]
- Da Fan, Y.; Pastorek, J.G.; Miller, J.M.; Mulvey, J. Acute pyelonephritis in pregnancy. Am. J. Perinatol. 1987, 4, 324–326. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Buekens, P.; Fraser, W.D.; Beck, J.; Offenbacher, S. Periodontal disease and adverse pregnancy outcomes: A systematic review. BJOG 2006, 113, 135–143. [Google Scholar] [CrossRef]
- Hendler, I.; Andrews, W.W.; Carey, C.J.; Klebanoff, M.A.; Noble, W.D.; Sibai, B.M.; Hillier, S.L.; Dudley, D.; Ernest, J.M.; Leveno, K.J.; et al. The relationship between resolution of asymptomatic bacterial vaginosis and spontaneous preterm birth in fetal fibronectin–positive women. Am. J. Obstet. Gynecol. 2007, 197, 488-e1. [Google Scholar] [CrossRef]
- Romero, R.; Avila, C.; Sepulveda, W. The role of systemic and intrauterine infection in preterm labor. In Preterm Birth: Causes, Prevention, and Management; Fuchs, A., Fuchs, F., Stubblefield, P., Eds.; McGraw-Hill: New York, NY, USA, 1993; p. 97. [Google Scholar]
- Romero, R.; Espinoza, J.; Kusanovic, J.P.; Gotsch, F.; Hassan, S.; Erez, O.; Chaiworapongsa, T.; Mazor, M. The preterm parturition syndrome. BJOG: Int. J. Obstet. Gynaecol. 2006, 113, 17–42. [Google Scholar] [CrossRef]
- Khandre, V.; Potdar, J.; Keerti, A.; Khandre, V., Jr. Preterm Birth: An Overview. Cureus 2022, 14, e33006. [Google Scholar] [CrossRef]
- Hodgson, E.J.; Lockwood, C.J. Preterm birth: A complex disease. In Preterm birth: Prevention and management; Wiley-Blackwell: Hoboken, NJ, USA, 2010; pp. 8–16.4. [Google Scholar]
- Mitchell, C.; Johnson, R.; Bisits, A.; Hirst, J.; Zakar, T. PTGS2 (Prostaglandin Endoperoxide Synthase-2) expression in term human amnion in vivo involves rapid mRNA turnover, polymerase 5′-pausing, and glucocorticoid transrepression. Endocrinology 2011, 152, 2113–2122. [Google Scholar] [CrossRef]
- Becher, N.; Hein, M.; Danielsen, C.C.; Uldbjerg, N. Matrix metalloproteinase in the cervical mucus plug in relation to gestational age, plug compartment, and preterm labor. Reprod. Biol. Endocrinol. 2010, 24, 113. [Google Scholar] [CrossRef]
- Madsen, G.; Zakar, T.; Ku, C.Y.; Sanborn, B.M.; Smith, R.; Mesiano, S. Prostaglandins differentially modulate progesterone receptor-A and -B expression in human myometrial cells: Evidence for prostaglandin-induced functional progesterone withdrawal. J. Clin. Endocrinol. Metab. 2004, 89, 1010–1013. [Google Scholar] [CrossRef] [PubMed]
- Oner, C.; Schatz, F.; Kizilay, G.; Murk, W.; Buchwalder, L.F.; Kayisli, U.A.; Arici, A.; Lockwood, C.J. Progestin-inflammatory cytokine interactions affect matrix metalloproteinase-1 and-3 expression in term decidual cells: Implications for treatment of chorioamnionitis-induced preterm delivery. J. Clin. Endocrinol. Metab. 2008, 93, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Lopez, N.; Romero, R.; Galaz, J.; Xu, Y.; Panaitescu, B.; Slutsky, R.; Motomura, K.; Gill, N.; Para, R.; Pacora, P.; et al. Cellular immune responses in amniotic fluid of women with preterm labor and intra-amniotic infection or intra-amniotic inflammation. Am. J. Reprod. Immunol. 2019, 82, e13171. [Google Scholar] [CrossRef] [PubMed]
- Goepfert, A.R.; Jeffcoat, M.K.; Andrews, W.W.; Faye-Petersen, O.; Cliver, S.P.; Goldenberg, R.L.; Hauth, J.C. Periodontal disease and upper genital tract inflammation in early spontaneous preterm birth. Obstet. Gynecol. 2004, 104, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Macones, G.A.; Parry, S.; Elkousy, M.; Clothier, B.; Ural, S.; Strauss, J.F., 3rd. A polymorphism in the promoter region of TNF and bacterial vaginosis: Preliminary evidence of gene-enviroment interaction in the etiology of spontaneous preterm birth. Am. J. Obstet. Gynecol. 2004, 190, 1504–1508. [Google Scholar] [CrossRef]
- Berghella, V. (Ed.) Preterm Birth: Prevention and Management; John Wiley & Sons: Hoboken, NJ, USA, 2010. [Google Scholar]
- Tsai, H.J.; Yu, Y.; Zhang, S.; Pearson, C.; Ortiz, K.; Xu, X.; Bauchner, H.; Zuckerman, B.; Wang, X. Association of genetic ancestry with preterm delivery and related traits among African American mothers. Am. J. Obstet. Gynecol. 2009, 201, 94-e1. [Google Scholar] [CrossRef]
- Gao, Y.; Mi, N.; Zhang, Y.; Li, X.; Guan, W.; Bai, C. Uterine macrophages as treatment targets for therapy of premature rupture of membranes by modified ADSC-EVs through a circRNA/miRNA/NF-κB pathway. J. Nanobiotechnology 2022, 20, 487. [Google Scholar] [CrossRef]
- Bashiri, A.; Burstein, E.; Mazor, M. Cerebral palsy and fetal inflammatory response syndrome: A review. J. Perinat. Med. 2006, 34, 5–12. [Google Scholar] [CrossRef]
- Lee, J.; Oh, K.J.; Yang, H.J.; Park, J.S.; Romero, R.; Yoon, B.H. The importance of intra-amniotic inflammation in the subsequent development of atypical chronic lung disease. J. Matern. Fetal Neonatal Med. 2009, 22, 917–923. [Google Scholar] [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef]
- Parthiban, P.; Mahendra, J. Toll-Like Receptors: A Key Marker for Periodontal Disease and Preterm Birth—A Contemporary Review. J. Clin. Diagn. Res. 2015, 9, ZE14-7. [Google Scholar] [CrossRef]
- Boyle, A.K.; Rinaldi, S.F.; Norman, J.E.; Stock, S.J. Preterm birth: Inflammation, fetal injury and treatment strategies. J. Reprod. Immunol. 2017, 119, 62–66. [Google Scholar] [CrossRef]
- Gruber, E.J.; Leifer, C.A. Molecular regulation of TLR signaling in health and disease: Mechano-regulation of macrophages and TLR signaling. Innate Immun. 2020, 26, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; He, J.; Qin, L.; Chen, Y.; Chen, L.; Li, R.; Zeng, Y.; Zhu, C.; You, X.; Wu, Y. Mycoplasma pneumoniae lipids license TLR-4 for activation of NLRP3 inflammasome and autophagy to evoke a proinflammatory response. Clin. Exp. Immunol. 2021, 203, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Robertson, S.A.; Hutchinson, M.R.; Rice, K.C.; Chin, P.Y.; Moldenhauer, L.M.; Stark, M.J.; Olson, D.M.; Keelan, J.A. Targeting Toll-like receptor-4 to tackle preterm birth and fetal inflammatory injury. Clin. Transl. Immunol. 2020, 9, e1121. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, K.A.; Kagan, J.C. Toll-like receptors and the control of immunity. Cell 2020, 180, 1044–1066. [Google Scholar] [CrossRef]
- Boros-Rausch, A.J. Preventing Infection-Induced Myometrial Inflammation by a Broad-Spectrum Chemokine Inhibitor. Ph.D. Thesis, University of Toronto, Toronto, ON, Canada, 2021. [Google Scholar]
- Parris, K.M.; Amabebe, E.; Cohen, M.C.; Anumba, D.O. Placental microbial–metabolite profiles and inflammatory mechanisms associated with preterm birth. J. Clin. Pathol. 2021, 74, 10–18. [Google Scholar] [CrossRef]
- Chatterjee, P.; Chiasson, V.L.; Bounds, K.R.; Mitchell, B.M. Regulation of the Anti-Inflammatory Cytokines Interleukin-4 and Interleukin-10 during Pregnancy. Front. Immunol. 2014, 5, 1. [Google Scholar] [CrossRef]
- Gómez-Chávez, F.; Correa, D.; Navarrete-Meneses, P.; Cancino-Diaz, J.C.; Cancino-Diaz, M.E.; Rodríguez-Martínez, S. NF-κB and its regulators during pregnancy. Front. Immunol. 2021, 12, 679106. [Google Scholar] [CrossRef]
- Galinsky, R.; Polglase, G.R.; Hooper, S.B.; Black, M.J.; Moss, T.J.M. The consequences of chorioamnionitis: Preterm birth and effects on development. J. Pregnancy 2013, 2013, 412831. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Norwitz, G.A.; Pavlicev, M.; Tilburgs, T.; Simón, C.; Norwitz, E.R. Endometrial decidualization: The primary driver of pregnancy health. Int. J. Mol. Sci. 2020, 21, 4092. [Google Scholar] [CrossRef] [PubMed]
- Sinkey, R.G.; Guzeloglu-Kayisli, O.; Arlier, S.; Guo, X.; Semerci, N.; Moore, R.; Ozmen, A.; Larsen, K.; Nwabuobi, C.; Kumar, D.; et al. Thrombin-induced decidual colony-stimulating factor-2 promotes abruption-related preterm birth by weakening fetal membranes. Am. J. Pathol. 2020, 190, 388–399. [Google Scholar] [CrossRef] [PubMed]
- Lockwood, C.J.; Toti, P.; Arcuri, F.; Paidas, M.; Buchwalder, L.; Krikun, G.; Schatz, F. Mechanisms of abruption-induced premature rupture of the fetal membranes: Thrombin-enhanced interleukin-8 expression in term decidua. Am. J. Pathol. 2005, 167, 1443–1449. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, C.R.; Gao, L.; Montalbano, A.P. Multifactorial regulation of myometrial contractility during pregnancy and parturition. Front. Endocrinol. 2019, 10, 714. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.; McDonald, S.D.; Mundle, W.R.; Farine, D. Guideline No. 398: Progesterone for prevention of spontaneous preterm birth. J. Obstet. Gynaecol. Can. 2020, 42, 806–812. [Google Scholar] [CrossRef] [PubMed]
- Haas, D.M.; Caldwell, D.M.; Kirkpatrick, P.; McIntosh, J.J.; Welton, N.J. Tocolytic therapy for preterm delivery: Systematic review and network meta-analysis. BMJ 2012, 345, e6226. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Conde-Agudelo, A.; Da Fonseca, E.; O′Brien, J.M.; Cetingoz, E.; Creasy, G.W.; Hassan, S.S.; Nicolaides, K.H. Vaginal progesterone in women with an asymptomatic sonographic short cervix in the midtrimester decreases preterm delivery and neonatal morbidity: A systematic review and metaanalysis of individual patient data. Am. J. Obstet. Gynecol. 2012, 206, 124.e1–124.e9. [Google Scholar] [CrossRef]
- Berghella, V.; Odibo, A.O.; Tolosa, J.E. Cerclage for prevention of preterm birth in women with a short cervix found on transvaginal ultrasound examination: A randomized trial. Am. J. Obstet. Gynecol. 2016, 214, S12. [Google Scholar] [CrossRef] [PubMed]
- Duhig, K.E.; Chandiramani, M.; Seed, P.T.; Briley, A.L.; Kenyon, A.P.; Shennan, A.H. Fetal fibronectin as a predictor of spontaneous preterm labour in asymptomatic women with a cervical cerclage. BJOG 2009, 116, 799–803. [Google Scholar] [CrossRef] [PubMed]
- Saccone, G.; Ciardulli, A.; Xodo, S.; Dugoff, L.; Ludmir, J.; Locci, M.; Biondi, A.; Visentin, S.; Di Tommaso, M.; Rizzo, G.; et al. Cervical pessary for preventing preterm birth in singleton pregnancies with short cervical length: A systematic review and meta-analysis. J. Ultrasound Med. 2017, 36, 2053–2063. [Google Scholar] [CrossRef] [PubMed]
- Stanfield, Z.; Amini, P.; Wang, J.; Yi, L.; Tan, H.; Chance, M.R.; Koyutürk, M.; Mesiano, S. Interplay of transcriptional signaling by progesterone, cyclic AMP, and inflammation in myometrial cells: Implications for the control of human parturition. Mol. Hum. Reprod. 2019, 25, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.S.; Romero, R.; Vidyadhari, D.; Fusey, S.; Baxter, J.K.; Khandelwal, M.; Vijayaraghavan, J.; Trivedi, Y.; Soma-Pillay, P.; Sambarey, P.; et al. Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: A multicenter, randomized, double-blind, placebo-controlled trial. Ultrasound Obstet Gynecol. 2011, 38, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Fettweis, J.M.; Serrano, M.G.; Brooks, J.P.; Edwards, D.J.; Girerd, P.H.; Parikh, H.I.; Huang, B.; Arodz, T.J.; Edupuganti, L.; Glascock, A.L.; et al. The vaginal microbiome and preterm birth. Nat. Med. 2019, 25, 1012–1021. [Google Scholar] [CrossRef] [PubMed]
- Muzny, C.A.; Taylor, C.M.; Swords, W.E.; Tamhane, A.; Chattopadhyay, D.; Cerca, N.; Schwebke, J.R. An updated conceptual model on the pathogenesis of bacterial vaginosis. J. Infect. Dis. 2019, 220, 1399–1405. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G. Definition and classification of abnormal vaginal flora. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 355–373. [Google Scholar] [CrossRef] [PubMed]
- Donati, L.; Di Vico, A.; Nucci, M.; Quagliozzi, L.; Spagnuolo, T.; Labianca, A.; Bracaglia, M.; Ianniello, F.; Caruso, A.; Paradisi, G. Vaginal microbial flora and outcome of pregnancy. Arch. Gynecol. Obstet. 2010, 281, 589–600. [Google Scholar] [CrossRef]
- Guaschino, S.; De Seta, F.; Piccoli, M.; Maso, G.; Alberico, S. Aetiology of preterm labour: Bacterial vaginosis. BJOG 2006, 113, 46–51. [Google Scholar] [CrossRef]
- Colonna, C. and Steelman, M. Amsel criteria. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- van den Munckhof, E.H.; van Sitter, R.L.; Lamont, R.F.; le Cessie, S.; Kuijper, E.J.; Knetsch, C.W.; Molijn, A.; Quint, W.G.; Boers, K.E.; Leverstein-van Hall, M.A. Developing an algorithm for the diagnosis of abnormal vaginal discharge in a dutch clinical setting: A pilot study. Diagn. Microbiol. Infect. Dis. 2021, 101, 115431. [Google Scholar] [CrossRef]
- Stinson, L.F.; Payne, M.S. Infection-mediated preterm birth: Bacterial origins and avenues for intervention. Aust. New Zealand J. Obstet. Gynaecol. 2019, 59, 781–790. [Google Scholar] [CrossRef]
- Bennett, P.R.; Brown, R.G.; MacIntyre, D.A. Vaginal microbiome in preterm rupture of membranes. Obstet. Gynecol. Clin. 2020, 47, 503–521. [Google Scholar] [CrossRef] [PubMed]
- Leitich, H.; Kiss, H. Asymptomatic bacterial vaginosis and intermediate flora as risk factors for adverse pregnancy outcome. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 375–390. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Andrews, W.W.; Goepfert, A.R.; Faye-Petersen, O.; Cliver, S.P.; Carlo, W.A.; Hauth, J.C. The Alabama Preterm Birth Study: Umbilical cord blood Ureaplasma urealyticum and Mycoplasma hominis cultures in very preterm newborn infants. Am. J. Obstet. Gynecol. 2008, 198, 43-e1. [Google Scholar] [CrossRef] [PubMed]
- Waters, T.P.; Denney, J.M.; Mathew, L.; Goldenberg, R.L.; Culhane, J.F. Longitudinal trajectory of bacterial vaginosis during pregnancy. Am. J. Obstet. Gynecol. 2008, 199, 431.e1–431.e5. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, U.; Misra, D.; Marazita, M.L.; Foxman, B. Vaginal and oral microbes, host genotype and preterm birth. Med. Hypotheses 2009, 73, 963–975. [Google Scholar] [CrossRef]
- Ryckman, K.K.; Simhan, H.N.; Krohn, M.A.; Williams, S.M. Cervical cytokine network patterns during pregnancy: The role of bacterial vaginosis and geographic ancestry. J. Reprod. Immunol. 2009, 79, 174–182. [Google Scholar] [CrossRef]
- Klebanoff, M.A.; Schuit, E.; Lamont, R.F.; Larsson, P.G.; Odendaal, H.J.; Ugwumadu, A.; Kiss, H.; Petricevic, L.; Andrews, W.W.; Hoffman, M.K.; et al. Antibiotic treatment of bacterial vaginosis to prevent preterm delivery: Systematic review and individual participant data meta-analysis. Paediatr. Perinat. Epidemiol. 2023, 37, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Yadufashije, C.; Umugwaneza, J.; Izere, C.; Munyeshyaka, E.; Habyarimana, T. Study of chorioamnionitis among women with preterm birth at Ruhengeri referral hospital. Afr. J. Biol. Sci. 2019, 1, 32–39. [Google Scholar] [CrossRef]
- Flannery, D.D.; Edwards, E.M.; Coggins, S.A.; Horbar, J.D.; Puopolo, K.M. Late-Onset Sepsis Among Very Preterm Infants. Pediatrics 2022, 150, e2022058813. [Google Scholar] [CrossRef]
- Farooqi, H.M.U.; Kim, K.H.; Kausar, F.; Muhammad, J.; Bukhari, H.; Choi, K.H. Frequency and molecular characterization of Staphylococcus aureus from placenta of mothers with term and preterm deliveries. Life 2022, 12, 257. [Google Scholar] [CrossRef]
- Top, K.A.; Buet, A.; Whittier, S.; Ratner, A.J.; Saiman, L. Predictors of Staphylococcus aureus Rectovaginal Colonization in Pregnant Women and Risk for Maternal and Neonatal Infections. J. Pediatric Infect. Dis. Soc. 2012, 1, 7. [Google Scholar] [CrossRef] [PubMed]
- Eleje, G.U.; Adinma, J.I.; Ghasi, S.; Ikechebelu, J.I.; Igwegbe, A.O.; Okonkwo, J.E.; Okafor, C.I.; Ezeama, C.O.; Ezebialu, I.U.; Ogbuagu, C.N. Antibiotic susceptibility pattern of genital tract bacteria in pregnant women with preterm premature rupture of membranes in a resource-limited setting. Int. J. Gynecol. Obstet. 2014, 127, 10–14. [Google Scholar] [CrossRef]
- Geisler, J.P.; Horlander, K.M.; Hiett, A.K. Methicillin resistant Staphylococcus aureus as a cause of chorioamnionitis. Clin. Exp. Obstet. Gynecol. 1998, 25, 119–120. [Google Scholar] [PubMed]
- Scherr, T.D.; Heim, C.E.; Morrison, J.M.; Kielian, T. Hiding in Plain Sight: Interplay between Staphylococcal Biofilms and Host Immunity. Front. Immunol. 2014, 5, 37. [Google Scholar] [CrossRef]
- McCarthy, H.; Rudkin, J.K.; Black, N.S.; Gallagher, L.; O’Neill, E.; O’Gara, J.P. Methicillin resistance and the biofilm phenotype in Staphylococcus aureus. Front. Cell Infect. Microbiol. 2015, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.J.; Lin, Y.C.; Gillman, A.N.; Parks, P.J.; Schlievert, P.M.; Peterson, M.L. Alpha-toxin promotes Staphylococcus aureus mucosal biofilm formation. Front. Cell Infect. Microbiol. 2012, 2, 64. [Google Scholar] [CrossRef]
- Hoang, M.; Potter, J.A.; Gysler, S.M.; Han, C.S.; Guller, S.; Norwitz, E.R.; Abrahams, V.M. Human fetal membranes generate distinct cytokine profiles in response to bacterial Toll-like receptor and nod-like receptor agonists. Biol. Reprod. 2014, 90, 39. [Google Scholar] [CrossRef] [PubMed]
- Watkins, R.L.; Pallister, K.B.; Voyich, J.M. The SaeR/S gene regulatory system induces a pro-inflammatory cytokine response during Staphylococcus aureus infection. PLoS ONE 2011, 6, e19939. [Google Scholar] [CrossRef] [PubMed]
- Murtha, A.P.; Edwards, J.M. The role of Mycoplasma and Ureaplasma in adverse pregnancy outcomes. Obstet. Gynecol. Clin. North Am. 2014, 41, 615–627. [Google Scholar] [CrossRef]
- Aparicio, D.; Scheffer, M.P.; Marcos-Silva, M.; Vizarraga, D.; Sprankel, L.; Ratera, M.; Weber, M.S.; Seybert, A.; Torres-Puig, S.; Gonzalez-Gonzalez, L.; et al. Structure and mechanism of the Nap adhesion complex from the human pathogen Mycoplasma genitalium. Nat. Commun. 2020, 11, 2877. [Google Scholar] [CrossRef]
- Cox, C.; Saxena, N.; Watt, A.P.; Gannon, C.; McKenna, J.P.; Fairley, D.J.; Sweet, D.; Shields, M.D.; LCosby, S.; Coyle, P.V. The common vaginal commensal bacterium Ureaplasma parvum is associated with chorioamnionitis in extreme preterm labor. J. Matern. -Fetal Neonatal Med. 2016, 29, 3646–3651. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.J.; Lee, S.E.; Jung, H.; Kim, G.; Romero, R.; Yoon, B.H. Detection of ureaplasmas by the polymerase chain reaction in the amniotic fluid of patients with cervical insufficiency. J. Perinat. Med. 2010, 38, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Kacerovský, M.; Pavlovský, M.; Tosner, J. Preterm premature rupture of the membranes and genital mycoplasmas. Acta Med. 2009, 52, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Noda-Nicolau, N.M.; Tantengco, O.A.G.; Polettini, J.; Silva, M.C.; Bento, G.F.; Cursino, G.C.; Marconi, C.; Lamont, R.F.; Taylor, B.D.; Silva, M.G.; et al. Genital mycoplasmas and biomarkers of inflammation and their Association with spontaneous Preterm Birth and Preterm Prelabor rupture of membranes: A systematic review and Meta-analysis. Front. Microbiol. 2022, 13, 859732. [Google Scholar] [CrossRef] [PubMed]
- Moridi, K.; Hemmaty, M.; Azimian, A.; Fallah, M.H.; Khaneghahi Abyaneh, H.; Ghazvini, K. Epidemiology of genital infections caused by Mycoplasma hominis, M. genitalium and Ureaplasma urealyticum in Iran; a systematic review and meta-analysis study (2000–2019). BMC Public Health 2020, 20, 1020. [Google Scholar] [CrossRef]
- Rumyantseva, T.; Khayrullina, G.; Guschin, A.; Donders, G. Prevalence of Ureaplasma spp. and Mycoplasma hominis in healthy women and patients with flora alterations. Diagn. Microbiol. Infect. Dis. 2019, 93, 227–231. [Google Scholar] [CrossRef]
- Choi, S.J.; Park, S.D.; Jang, I.H.; Uh, Y.; Lee, A. The prevalence of vaginal microorganisms in pregnant women with preterm labor and preterm birth. Ann. Lab. Med. 2012, 32, 194–200. [Google Scholar] [CrossRef]
- Paramel Jayaprakash, T.; Wagner, E.C.; van Schalkwyk, J.; Albert, A.Y.; Hill, J.E.; Money, D.M.; PPROM Study Group. High diversity and variability in the vaginal microbiome in women following preterm premature rupture of membranes (PPROM): A prospective cohort study. PloS ONE 2016, 11, p.e0166794. [Google Scholar] [CrossRef]
- Kataoka, S.; Yamada, T.; Chou, K.; Nishida, R.; Morikawa, M.; Minami, M.; Yamada, H.; Sakuragi, N.; Minakami, H. Association between preterm birth and vaginal colonization by mycoplasmas in early pregnancy. J. Clin. Microbiol. 2006, 44, 51–55. [Google Scholar] [CrossRef]
- Ahmed, J.; Rawre, J.; Dhawan, N.; Khanna, N.; Dhawan, B. Mycoplasma hominis: An under recognized pathogen. Indian J. Med. Microbiol. 2021, 39, 88–97. [Google Scholar] [CrossRef]
- Payne, M.S.; Ireland, D.J.; Watts, R.; Nathan, E.A.; Furfaro, L.L.; Kemp, M.W.; Keelan, J.A.; Newnham, J.P. Ureaplasma parvum genotype, combined vaginal colonisation with Candida albicans, and spontaneous preterm birth in an Australian cohort of pregnant women. BMC Pregnancy Childbirth 2016, 16, 1–13. [Google Scholar] [CrossRef]
- Jonduo, M.E.; Vallely, L.M.; Wand, H.; Sweeney, E.L.; Egli-Gany, D.; Kaldor, J.; Vallely, A.J.; Low, N. Adverse pregnancy and birth outcomes associated with Mycoplasma hominis, Ureaplasma urealyticum and Ureaplasma parvum: A systematic review and meta-analysis. BMJ Open 2022, 12, e062990. [Google Scholar] [CrossRef] [PubMed]
- Olaleye, A.O.; Babah, O.A.; Osuagwu, C.S.; Ogunsola, F.T.; Afolabi, B.B. Sexually transmitted infections in pregnancy–An update on Chlamydia trachomatis and Neisseria gonorrhoeae. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 255, 1–12. [Google Scholar] [CrossRef]
- Smolarczyk, K.; Mlynarczyk-Bonikowska, B.; Rudnicka, E.; Szukiewicz, D.; Meczekalski, B.; Smolarczyk, R.; Pieta, W. The impact of selected bacterial sexually transmitted diseases on pregnancy and female fertility. Int. J. Mol. Sci. 2021, 22, 2170. [Google Scholar] [CrossRef]
- Blas, M.M.; Canchihuaman, F.A.; Alva, I.E.; Hawes, S.E. Pregnancy outcomes in women infected with Chlamydia trachomatis: A population-based cohort study in Washington State. Sex. Transm. Infect. 2007, 83, 314–318. [Google Scholar] [CrossRef] [PubMed]
- Johnson, H.L.; Ghanem, K.G.; Zenilman, J.M.; Erbelding, E.J. Sexually transmitted infections and adverse pregnancy outcomes among women attending inner city public sexually transmitted diseases clinics. Sex. Transm. Dis. 2011, 38, 167–171. [Google Scholar] [CrossRef]
- Paavonen, J. Chlamydia trachomatis infections of the female genital tract: State of the art. Ann. Med. 2012, 44, 18–28. [Google Scholar] [CrossRef]
- Andrews, W.W.; Goldenberg, R.L.; Mercer, B.; Iams, J.; Meis, P.; Moawad, A.; Das, A.; VanDorsten, J.P.; Caritis, S.N.; Thurnau, G.; et al. The Preterm Prediction Study: Association of second-trimester genitourinary chlamydia infection with subsequent spontaneous preterm birth. Am. J. Obstet. Gynecol. 2000, 183, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Olson-Chen, C.; Balaram, K.; Hackney, D.N. Chlamydia trachomatis and Adverse Pregnancy Outcomes: Meta-analysis of Patients with and without Infection. Matern. Child Health J. 2018, 22, 812–821. [Google Scholar] [CrossRef]
- Walker, G. Interventions for Trichomoniasis in Pregnancy: RHL Commentary. In The WHO Reproductive Health Library; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Hobbs, M.M.; Seña, A.C. Modern diagnosis of Trichomonas vaginalis infection. Sex. Transm. Infect. 2013, 89, 434–438. [Google Scholar] [CrossRef]
- Cotch, M.F.; Pastorek, J.G.; Nugent, R.P.; Hillier, S.L.; Gibbs, R.S.; Martin, D.H.; Eschenbach, D.A.; Edelman, R.; Carey, J.C.; Regan, J.A.; et al. Trichomonas vaginalis associated with low birth weight and preterm delivery. The Vaginal Infections and Prematurity Study Group. Sex. Transm. Dis. 1997, 24, 353–360. [Google Scholar] [CrossRef]
- Silver, B.J.; Guy, R.J.; Kaldor, J.M.; Jamil, M.S.; Rumbold, A.R. Trichomonas vaginalis as a cause of perinatal morbidity: A systematic review and meta-analysis. Sex Transm. Dis. 2014, 41, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Mabaso, N.; Abbai, N.S. A review on Trichomonas vaginalis infections in women from Africa. S. Afr. J. Infect. Dis. 2021, 36, 254. [Google Scholar] [CrossRef]
- Klebanoff, M.A.; Carey, J.C.; Hauth, J.C.; Hillier, S.L.; Nugent, R.P.; Thom, E.A.; Ernest, J.M.; Heine, R.P.; Wapner, R.J.; Trout, W.; et al. Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection. New Engl. J. Med. 2001, 345, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Heumann, C.L.; Quilter, L.A.S.; Eastment, M.C.; Heffron, R.; Hawes, S.E. Adverse Birth Outcomes and Maternal Neisseria gonorrhoeae Infection: A Population-Based Cohort Study in Washington State. Sex. Transm. Dis. 2017, 44, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Donders, G.G.G.; Desmyter, J.; De Wet, D.H.; Van Assche, F.A. The association of gonorrhoea and syphilis with premature birth and low birthweight. Genitourin. Med. 1993, 69, 98–101. [Google Scholar] [CrossRef]
- Nakubulwa, S.; Kaye, D.K.; Bwanga, F.; Tumwesigye, N.M.; Mirembe, F.M. Genital infections and risk of premature rupture of membranes in Mulago Hospital, Uganda: A case control study. BMC Res. Notes 2015, 8, 573. [Google Scholar] [CrossRef]
- Flores-Herrera, H.; Garcia-Lopez, G.; Diaz, N.F.; Molina-Hernandez, A.; Osorio-Caballero, M.; Soriano-Becerril, D.; Zaga-Clavellina, V. An experimental mixed bacterial infection induced differential secretion of proinflammatory cytokines (IL-1β, TNFα) and proMMP-9 in human fetal membranes. Placenta 2012, 33, 271–277. [Google Scholar] [CrossRef]
- French, J.I.; McGregor, J.A.; Parker, R. Readily treatable reproductive tract infections and preterm birth among black women. Am. J. Obstet. Gynecol. 2006, 194, 1717–1726. [Google Scholar] [CrossRef]
- Vaezzadeh, K.; Sepidarkish, M.; Mollalo, A.; As′adi, N.; Rouholamin, S.; Rezaeinejad, M.; Mojtahedi, M.F.; Hosseini, S.M.M.; Taheri, M.; Mahjour, S.; et al. Global prevalence of Neisseria gonorrhoeae infection in pregnant women: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2023, 29, 22–31. [Google Scholar] [CrossRef]
- Fitzhugh, V.; Pompeo, L.; Heller, D. Placental invasion by actinomyces resulting in preterm delivery: A case report. J. Reprod. Med. 2008, 53, 302–304. [Google Scholar]
- Estrada, S.M.; Magann, E.F.; Napolitano, P.G. Actinomyces in Pregnancy: A Review of the Literature. Obstet. Gynecol. Surv. 2017, 72, 242–247. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.; Czeizel, A.E. Asymptomatic trichomonas and candida colonization and pregnancy outcome. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 403–409. [Google Scholar] [CrossRef]
- Ito, F.; Okubo, T.; Yasuo, T.; Mori, T.; Iwasa, K.; Iwasaku, K.; Kitawaki, J. Premature delivery due to intrauterine Candida infection that caused neonatal congenital cutaneous candidiasis: A case report. J. Obstet. Gynaecol. Res. 2013, 39, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Asemota, O.A.; Nyirjesy, P.; Fox, R.; Sobel, J.D. Candida glabrata complicating in vitro pregnancy: Successful management of subsequent pregnancy. Fertil. Steril. 2011, 95, 803.e1–803.e2. [Google Scholar] [CrossRef]
- Kim, S.K.; Romero, R.; Kusanovic, J.P.; Erez, O.; Vaisbuch, E.; Mazaki-Tovi, S.; Gotsch, F.; Mittal, P.; Chaiworapongsa, T.; Pacora, P.; et al. The prognosis of pregnancy conceived despite the presence of an intrauterine device (IUD). J. Perinat. Med. 2010, 38, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Özer, E.; Ünlü, M.; Erşen, A.; Gülekli, B. Intrauterine fetal loss associated with Candida glabrata chorioamnionitis: Report of two cases. Turk. Patoloji Derg. 2013, 29, 77–79. [Google Scholar]
- Whyte, R.K.; Hussain, Z.; DeSa, D. Antenatal infections with Candida species. Arch. Dis. Child. 1982, 57, 528–535. [Google Scholar] [CrossRef]
- Qureshi, F.; Jacques, S.M.; Bendon, R.W.; Faye-Peterson, O.M.; Heifetz, S.A.; Redline, R.; Sander, C.M. Candida funisitis: A clinicopathologic study of 32 cases. Pediatr. Dev. Pathol. 1998, 1, 118–124. [Google Scholar] [CrossRef]
- Maki, Y.; Fujisaki, M.; Sato, Y.; Sameshima, H. Candida Chorioamnionitis Leads to Preterm Birth and Adverse Fetal-Neonatal Outcome. Infect. Dis. Obstet. Gynecol. 2017, 2017, 9060138. [Google Scholar] [CrossRef]
- O’Sullivan, A.M.; Dore, C.J.; Coid, C.R. Campylobacters and impaired fetal development in mice. J. Med. Microbiol. 1988, 25, 7–12. [Google Scholar] [CrossRef]
- Denton, K.J.; Clarke, T. Role of Campylobacter jejuni as a placental pathogen. J. Clin. Pathol. 1992, 45, 171–172. [Google Scholar] [CrossRef]
- Sauerwein, R.W.; Horrevorts, A.M.; Bisseling, J. Septic abortion associated with Campylobacter fetus subspecies fetus infection: Case report and review of the literature. Infection 1993, 21, 331–333. [Google Scholar] [CrossRef]
- Steinkraus, G.E.; Wright, B.D. Septic abortion with intact fetal membranes caused by Campylobacter fetus subsp. fetus. J. Clin. Microbiol. 1994, 32, 1608–1609. [Google Scholar] [CrossRef] [PubMed]
- Heuvelink, A.E.; Valkenburgh, S.M.; Tilburg, J.J.H.C.; Van Heerwaarden, C.; Zwartkruis-Nahuis, J.T.M.; De Boer, E. Public farms: Hygiene and zoonotic agents. Epidemiol. Infect. 2007, 135, 1174–1183. [Google Scholar] [CrossRef] [PubMed]
- Kantsø, B.; Andersen, A.M.N.; Mølbak, K.; Krogfelt, K.A.; Henriksen, T.B.; Nielsen, S.Y. Campylobacter, Salmonella, and Yersinia antibodies and pregnancy outcome in Danish women with occupational exposure to animals. Int. J. Infect. Dis. 2014, 28, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Theis, K.R.; Florova, V.; Romero, R.; Borisov, A.B.; Winters, A.D.; Galaz, J.; Gomez-Lopez, N. Sneathia: An emerging pathogen in female reproductive disease and adverse perinatal outcomes. Crit. Rev. Microbiol. 2021, 47, 517–542. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daskalakis, G.; Psarris, A.; Koutras, A.; Fasoulakis, Z.; Prokopakis, I.; Varthaliti, A.; Karasmani, C.; Ntounis, T.; Domali, E.; Theodora, M.; et al. Maternal Infection and Preterm Birth: From Molecular Basis to Clinical Implications. Children 2023, 10, 907. https://doi.org/10.3390/children10050907
Daskalakis G, Psarris A, Koutras A, Fasoulakis Z, Prokopakis I, Varthaliti A, Karasmani C, Ntounis T, Domali E, Theodora M, et al. Maternal Infection and Preterm Birth: From Molecular Basis to Clinical Implications. Children. 2023; 10(5):907. https://doi.org/10.3390/children10050907
Chicago/Turabian StyleDaskalakis, George, Alexandros Psarris, Antonios Koutras, Zacharias Fasoulakis, Ioannis Prokopakis, Antonia Varthaliti, Christina Karasmani, Thomas Ntounis, Ekaterini Domali, Marianna Theodora, and et al. 2023. "Maternal Infection and Preterm Birth: From Molecular Basis to Clinical Implications" Children 10, no. 5: 907. https://doi.org/10.3390/children10050907