
Neuropsychiatric Manifestations, Reduced Self-Esteem and Poor Quality of Life in Children and Adolescents with Neurofibromatosis Type 1 (NF1): The Impact of Symptom Visibility and Bullying Behavior
 ,
,  ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Procedure
2.2. Pediatric and Psychological Assessment
2.3. Statistical Analysis
3. Results
3.1. Sociodemographic and Behavioral Predictors of Psychological Variables and Psychosocial QoL
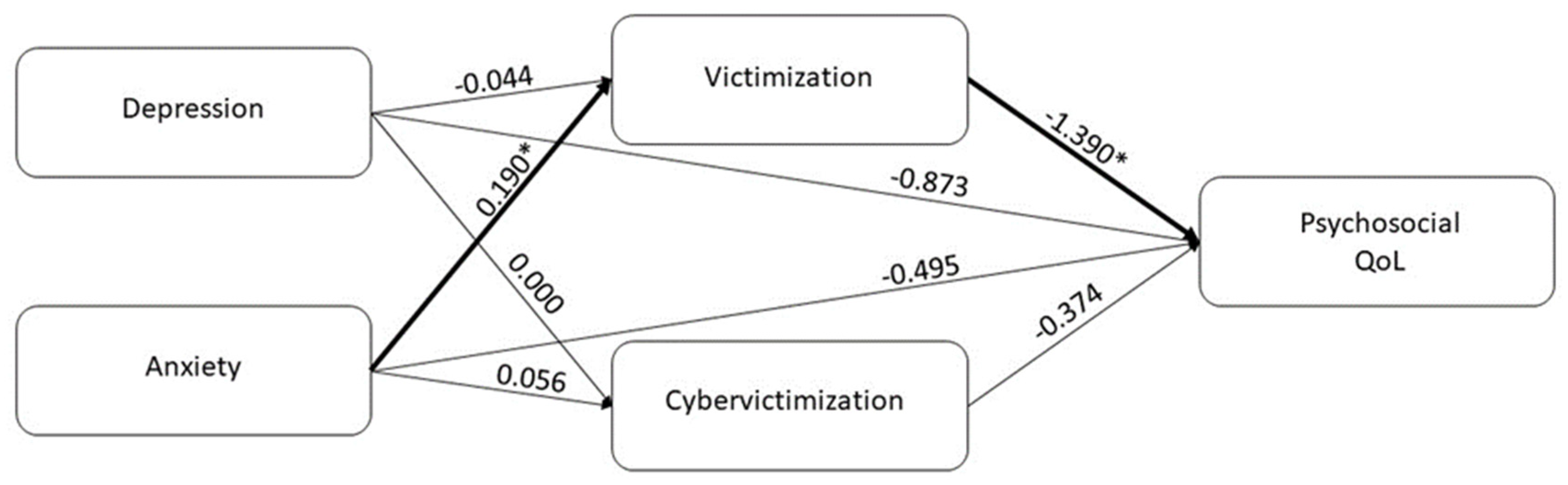
3.2. Mediation Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Legius, E.; Messiaen, L.; Wolkenstein, P.; Pancza, P.; Avery, R.A.; Berman, Y.; Blakeley, J.; Babovic-Vuksanovic, D.; Cunha, K.S.; Ferner, R.; et al. Revised diagnostic criteria for neurofibromatosis type 1 and Legius syndrome: An international consensus recommendation. Genet. Med. 2021, 23, 1506–1513. [Google Scholar] [CrossRef] [PubMed]
- Ozarslan, B.; Russo, T.; Argenziano, G.; Santoro, C.; Piccolo, V. Cutaneous Findings in Neurofibromatosis Type 1. Cancers 2021, 13, 463. [Google Scholar] [CrossRef]
- Kehrer-Sawatzki, H.; Bäzner, U.; Krämer, J.; Lewerenz, J.; Pfeiffer, C. The NF1 microdeletion syndrome: Early genetic diagnosis facilitates the management of a clinically defined disease. J. Dtsch. Dermatol. Ges. 2022, 20, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Lehtonen, A.; Howie, E.; Trump, D.; Huson, S.M. Behaviour in children with neurofibromatosis type 1: Cognition, executive function, attention, emotion, and social competence. Dev. Med. Child Neurol. 2013, 55, 111–125. [Google Scholar] [CrossRef]
- Cutting, L.E.; Clements, A.M.; Lightman, A.D.; Yerby-Hammack, P.D.; Denckla, M.B. Cognitive Profile of Neurofibromatosis Type 1: Rethinking Nonverbal Learning Disabilities. Learn. Disabil. Res. Pract. 2004, 19, 155–165. [Google Scholar] [CrossRef]
- Torres Nupan, M.M.; Velez Van Meerbeke, A.; López Cabra, C.A.; Herrera Gomez, P.M. Cognitive and Behavioral Disorders in Children with Neurofibromatosis Type 1. Front. Pediatr. 2017, 5, 227. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.L.; Smith, K.B.; Esparza, S.; Leigh, F.A.; Muzikansky, A.; Park, E.R.; Plotkin, S.R. Emotional functioning of patients with neurofibromatosis tumor suppressor syndrome. Genet. Med. 2012, 14, 977–982. [Google Scholar] [CrossRef]
- Doser, K.; Andersen, E.W.; Kenborg, L.; Dalton, S.O.; Jepsen, J.R.M.; Krøyer, A.; Østergaard, J.; Hove, H.; Sørensen, S.A.; Johansen, C.; et al. Clinical characteristics and quality of life, depression, and anxiety in adults with neurofibromatosis type 1: A nationwide study. Am. J. Med. Genet. 2020, 182, 1704–1715. [Google Scholar] [CrossRef]
- Hinz, A.; Krauss, O.; Hauss, J.P.; Höckel, M.; Kortmann, R.D.; Stolzenburg, J.U.; Schwarz, R. Anxiety and depression in cancer patients compared with the general population. Eur. J. Cancer Care 2010, 19, 522–529. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Ferguson, D.W.; Gill, J.; Paul, J.; Symonds, P. Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: A systematic review and meta-analysis. Lancet Oncol. 2013, 14, 721–732. [Google Scholar] [CrossRef]
- Cipolletta, S.; Spina, G.; Spoto, A. Psychosocial functioning, self-image, and quality of life in children and adolescents with neurofibromatosis type 1. Child Care Health Dev. 2018, 44, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Sanagoo, A.; Jouybari, L.; Koohi, F.; Sayehmiri, F. Evaluation of QoL in neurofibromatosis patients: A systematic review and meta-analysis study. BMC Neurol. 2019, 19, 123. [Google Scholar] [CrossRef] [PubMed]
- Vranceanu, A.M.; Merker, V.L.; Park, E.R.; Plotkin, S.R. Quality of life among children and adolescents with neurofibromatosis 1: A systematic review of the literature. J. Neurooncol. 2015, 122, 219–228. [Google Scholar] [CrossRef] [PubMed]
- Hamoy-Jimenez, G.; Elahmar, H.A.; Mendoza, M.; Kim, R.H.; Bril, V.; Barnett, C. A cross-sectional study of gender differences in quality of life domains in patients with neurofibromatosis type 1. Orphanet J. Rare Dis. 2022, 17, 40. [Google Scholar] [CrossRef] [PubMed]
- Bogadi, M.; Bakija, I.; Kaštelan, S.; Kasun, B. Transdisciplinary Approach in Type I Neurofibromatosis—Review of Psychiatric Disorders. Psychiatr. Danub. 2021, 33, 1254–1260. [Google Scholar]
- Graf, A.; Landolt, M.A.; Mori, A.C.; Boltshauser, E. Quality of life and psychological adjustment in children and adolescents with neurofibromatosis type 1. J. Pediatr. 2006, 149, 348–353. [Google Scholar] [CrossRef]
- Johnson, H.; Wiggs, L.; Stores, G.; Huson, S.M. Psychological disturbance and sleep disorders in children with neurofibromatosis type 1. Dev. Med. Child Neurol. 2005, 47, 237–242. [Google Scholar] [CrossRef]
- Krab, L.C.; Oostenbrink, R.; de Goede-Bolder, A.; Aarsen, F.K.; Elgersma, Y.; Moll, H.A. Health-related quality of life in children with neurofibromatosis type 1: Contribution of demographic factors, disease-related factors, and behavior. J. Pediatr. 2009, 154, 420–425. [Google Scholar] [CrossRef]
- Wolkenstein, P.; Zeller, J.; Revuz, J.; Ecosse, E.; Leplège, A. Quality-of-life impairment in neurofibromatosis type 1: A cross-sectional study of 128 cases. Arch. Dermatol. 2001, 137, 1421–1425. [Google Scholar] [CrossRef]
- Cohen, S.; Rodriguez, R. Pathways Linking Affective Disturbances and Physical Disorders. Health Psychol. 1995, 15, 374–380. [Google Scholar] [CrossRef]
- Bottesi, G.; Spoto, A.; Trevisson, E.; Zuccarello, D.; Vidotto, G.; Cassina, M.; Clementi, M. Dysfunctional coping is related to impaired skin-related quality of life and psychological distress in patients with neurofibromatosis type 1 with major skin involvement. Br. J. Dermatol. 2020, 182, 1449–1457. [Google Scholar] [CrossRef] [PubMed]
- Buono, F.D.; Sprong, M.E.; Paul, E.; Martin, S.; Larkin, K.; Garakani, A. The mediating effects of quality of life, depression, and generalized anxiety on perceived barriers to employment success for people diagnosed with Neurofibromatosis Type 1. Orphanet J. Rare Dis. 2021, 16, 234. [Google Scholar] [CrossRef] [PubMed]
- Fantaguzzi, C.; Allen, E.; Miners, A.; Christie, D.; Opondo, C.; Sadique, Z.; Fletcher, A.; Grieve, R.; Bonell, C.; Viner, R.M.; et al. Health-related quality of life associated with bullying and aggression: A cross-sectional study in English secondary schools. Eur. J. Health Econ. 2018, 19, 641–651. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, T.; Gaspar de Matos, M.; Ribeiro, J.P.; Leal, I.; Albergaria, F. Psychosocial factors related to bullying and victimization in children and adolescents. Health Behav. Policy Rev. 2014, 1, 452–459. [Google Scholar] [CrossRef]
- Olweus, D. Bully/victim problems among schoolchildren: Basic facts and effects of a school based intervention program. In Book The Development and Treatment of Childhood Aggression, 1st ed.; Pepler, D.J., Rubin, K.H., Eds.; Lawrence Erlbaum Associates, Inc.: Hillsdale, MI, USA, 1991; pp. 411–448. [Google Scholar]
- Younan, B. A systematic review of bullying definitions: How definition and format affect study outcome. J. Aggress. Confl. Peace Res. 2018, 11, 109–115. [Google Scholar] [CrossRef]
- Olweus, D.; Solberg, C. Bullying among Children and Young People. Information and Guidance for Parents; Pedagogisk forum: Oslo, Norway, 1998. [Google Scholar]
- Grindvik, A.S.; Hodøl, J.S.; Vik, T.; Evensen, K.A.; Skranes, J.; Brubakk, A.M.; Indredavik, M.S. Bullying among adolescents with very low birth weight. Acta Paediatr. 2009, 98, 1049–1051. [Google Scholar] [CrossRef]
- Smith, P.K.; Mahdavi, J.; Carvalho, M.; Fisher, S.; Russell, S.; Tippett, N. Cyber-bullying: Its nature and impact in secondary school pupils. J. Child Psychol. Psychiatry 2008, 49, 376–385. [Google Scholar] [CrossRef]
- Kowalski, R.M.; Limber, S.P. Electronic bullying among middle school students. J. Adolesc. Health 2007, 41, 22–30. [Google Scholar] [CrossRef]
- Corcoran, L.; Guckin, C.M.; Prentice, G. Cyberbullying or Cyber Aggression?: A Review of Existing Definitions of Cyber-Based Peer-to-Peer Aggression. Societies 2015, 5, 245–255. [Google Scholar] [CrossRef]
- Wang, J.; Nansel, T.R.; Iannotti, R.J. Cyber and traditional bullying: Differential association with depression. J. Adolesc. Health 2011, 48, 415–417. [Google Scholar] [CrossRef]
- Vieno, A.; Gini, G.; Lenzi, M.; Pozzoli, T.; Canale, N.; Santinello, M. Cybervictimization and somatic and psychological symptoms among Italian middle school students. Eur. J. Public Health 2015, 25, 433–437. [Google Scholar] [CrossRef] [Green Version]
- Holfeld, B.; Sukhawathanakul, P. Associations between Internet Attachment, Cyber Victimization, and Internalizing Symptoms Among Adolescents. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 91–96. [Google Scholar] [CrossRef]
- Holland, A.A.; Stavinoha, P.L.; Swearer, S.M.; Solesbee, C.; Patel, S.; Klesse, L.J. Rate and frequency of bullying victimization in school-age children with neurofibromatosis type 1 (NF1). Sch. Psychol. 2019, 34, 687–694. [Google Scholar] [CrossRef]
- Hummelvoll, G.; Antonsen, K.M. Young adults’ experience of living with neurofibromatosis type 1. J. Genet. Couns. 2013, 22, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Stavinoha, P.L.; Solesbee, C.; Swearer, S.M.; Svoboda, S.; Klesse, L.J.; Holland, A.A. Risk Factors for Bullying Victimization in Children with Neurofibromatosis Type 1 (NF1). Children 2021, 8, 145. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Ablon, J. Gender response to neurofibromatosis 1. Soc. Sci. Med. 1996, 42, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, M. Children’s Depression Inventory, 2nd ed.; Italian Adaptation (Curated by Camuffo M and Cerutti R); Hogrefe: Firenze, Italy, 2018. [Google Scholar]
- Reynolds, C.R.; Richmond, B.O. RCMAS-2 Revised Children’s Manifest Anxiety Scale, 2nd ed.; Scozzari, S., Sella, F., Di Pietro, M., Eds.; Giunti O.S.: Firenze, Italy, 2012. [Google Scholar]
- Prezza, M.; Trombaccia, F.R.; Armento, L. The Rosenberg Self-Esteem Scale: Italian translation and validation. Giunti Organ. Spec. 1997, 223, 35–44. [Google Scholar]
- Varni, J.W.; Seid, M.; Rode, C.A. The PedsQL™: Measurement model for the pediatric quality of life inventory. Med. Care 1999, 37, 126–139. [Google Scholar] [CrossRef]
- Menesini, E.; Giannetti, E. The Bully-Victim Questionnaire for the Italian Popularion: Theoretic and Methodological Problems. In Il Bullismo in Italia, 1st ed.; Fonzi, A., Ed.; Giunti Gruppo Editoriale: Firenze, Italy, 1997. [Google Scholar]
- Willard, N.E. Cyberbullying and Cyberthreats: Responding to the Challenge of Online Social Aggression, Threats, and Distress, 1st ed.; Research Press: Champaign, IL, USA, 2007; pp. 209–216. [Google Scholar]
- Preacher, K.J.; Hayes, A.F. Asymptotic and Resampling Strategies for Assessing and Comparing Indirect Effects in Multiple Mediator Models. Behav. Res. Methods 2008, 40, 879–891. [Google Scholar] [CrossRef]
- Solberg, M.F.; Olweus, D. Prevalence estimation of school bullying with the Olweus bully/victim questionnaire. Aggress. Behav. 2003, 29, 239–268. [Google Scholar] [CrossRef]
- Nocentini, A.; Menesini, E.; Salmivalli, C. Level and change of bullying behavior during high school: A multilevel growth curve analysis. J. Adolesc. 2013, 36, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, A.; Baldry, A.C.; Farrington, D.P.; Blaya, C. Epidemiology of cyberbullying across Europe: Differences between countries and genders. Educ. Sci. Theory Pract. 2019, 19. [Google Scholar] [CrossRef]
- Baldry, A.C.; Farrington, D.P.; Sorrentino, A. School bullying and cyberbullying among boys and girls: Roles and overlap. J. Aggress. Maltreat. Trauma 2017, 26, 937–951. [Google Scholar] [CrossRef]
- Garwood, M.M.; Bernacki, J.M.; Fine, K.M.; Hainsworth, K.R.; Davies, W.H.; Klein-Tasman, B.P. Physical, cognitive, and psychosocial predictors of functional disability and health-related quality of life in adolescents with neurofibromatosis-1. Pain Res. Treat. 2012, 2012, 975364. [Google Scholar] [CrossRef] [PubMed]
- Rosnau, K.; Hashmi, S.S.; Northrup, H.; Slopis, J.; Noblin, S.; Ashfaq, M. Knowledge and Self-Esteem of Individuals with Neurofibromatosis Type 1 (NF1). J. Genet. Couns. 2017, 26, 620–627. [Google Scholar] [CrossRef] [PubMed]
- Wolkenstein, P.; Rodriguez, D.; Ferkal, S.; Gravier, H.; Buret, V.; Algans, N.; Simeoni, M.C.; Bastuji-Garin, S. Impact of neurofibromatosis 1 upon quality of life in childhood: A cross-sectional study of 79 cases. Br. J. Dermatol. 2009, 160, 844–848. [Google Scholar] [CrossRef]
- Dalsgaard, S.; Thorsteinsson, E.; Trabjerg, B.B.; Schullehner, J.; Plana-Ripoll, O.; Brikell, I.; Wimberley, T.; Thygesen, M.; Madsen, K.B.; Timmerman, A.; et al. Incidence Rates and Cumulative Incidences of the Full Spectrum of Diagnosed Mental Disorders in Childhood and Adolescence. JAMA Psychiatry 2020, 77, 155–164. [Google Scholar] [CrossRef]
- Perou, R.; Bitsko, R.H.; Blumberg, S.J.; Pastor, P.; Ghandour, R.M.; Gfroerer, J.C.; Hedden, S.L.; Crosby, A.E.; Visser, S.N.; Schieve, L.A.; et al. Mental health surveillance among children—United States, 2005–2011. Morb. Mortal. Wkly. Rep. Suppl. 2013, 62, 1–35. [Google Scholar]
- Martin, S.; Wolters, P.; Baldwin, A.; Gillespie, A.; Dombi, E.; Walker, K.; Widemann, B. Social-emotional functioning of children and adolescents with neurofibromatosis type 1 and plexiform neurofibromas: Relationships with cognitive, disease, and environmental variables. J. Pediatr. Psychol. 2012, 37, 713–724. [Google Scholar] [CrossRef]
- Huang, Y.Y.; Chou, C. An analysis of multiple factors of cyberbullying among junior high school students in Taiwan. Comput. Hum. Behav. 2010, 26, 1581–1590. [Google Scholar] [CrossRef]
- Ma, X.; Stewin, L.L.; Mah, D.L. Bullying in school: Nature, effects and remedies. Res. Pap. Educ. 2001, 16, 247–270. [Google Scholar] [CrossRef]
- Smith, P.K.; López-Castro, L.; Robinson, S.; Görzig, A. Consistency of gender differences in bullying in cross-cultural surveys. Aggress. Violent Behav. 2019, 45, 33–40. [Google Scholar] [CrossRef]
- Piccinelli, M.; Wilkinson, G. Gender differences in depression. Critical review. Br. J. Psychiatry 2000, 177, 486–492. [Google Scholar] [CrossRef]
- Zeigler-Hill, V.; Myers, E.M. A review of gender differences in self-esteem. In Psychology of Gender Differences, 1st ed.; McGeown, S.P., Ed.; Nova Science Publishers: Hauppauge, NY, USA, 2012; pp. 131–143. [Google Scholar]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Li, S.H.; Graham, B.M. Why are women so vulnerable to anxiety, trauma-related and stress-related disorders? The potential role of sex hormones. Lancet Psychiatry 2017, 4, 73–82. [Google Scholar] [CrossRef]
- Maggi, G.; Baldassarre, I.; Barbaro, A.; Cavallo, N.D.; Cropano, M.; Nappo, R.; Santangelo, G. Age- and gender-related differences in the evolution of psychological and cognitive status after the lockdown for the COVID-19 outbreak: A follow-up study. Neurol. Sci. 2022, 43, 1521–1532. [Google Scholar] [CrossRef] [PubMed]
- Belzeaux, R.; Lançon, C. Neurofibromatose de type 1. Troubles psychiatriques et altération de la qualité de vie [Neurofibromatosis type 1: Psychiatric disorders and quality of life impairment]. Presse Med. 2006, 35, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Pasini, A.; Lo-Castro, A.; Di Carlo, L.; Pitzianti, M.; Siracusano, M.; Rosa, C.; Galasso, C. Detecting anxiety symptoms in children and youths with neurofibromatosis type I. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2012, 159, 869–873. [Google Scholar] [CrossRef]
- Molero, M.M.; Martos, Á.; Barragán, A.B.; Pérez-Fuentes, M.C.; Gázquez, J.J. Anxiety and depression from cybervictimization in adolescents: A metaanalysis and meta-regression study. Eur. J. Psychol. Appl. Leg. Context 2022, 14, 42–50. [Google Scholar] [CrossRef]
- Wright, M.F. Cyber Victimization on College Campuses: Longitudinal Associations with Suicidal Ideation, Depression, and Anxiety. Crim. Justice Rev. 2016, 41, 190–203. [Google Scholar] [CrossRef]
- Lee, J. Pathways from Childhood Bullying Victimization to Young Adult Depressive and Anxiety Symptoms. Child Psychiatry Hum. Dev. 2021, 52, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Rose, C.A.; Tynes, B.M. Longitudinal Associations between Cybervictimization and Mental Health among U.S. Adolescents. J. Adolesc. Health 2015, 57, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Van Cleave, J.; Davis, M.M. Bullying and peer victimization among children with special health care needs. Pediatrics 2006, 118, 1212–1219. [Google Scholar] [CrossRef] [PubMed]
- Frisén, A.; Bjarnelind, S. Health-related quality of life and bullying in adolescence. Acta Paediatr. 2010, 99, 597–603. [Google Scholar] [CrossRef]
- Wilkins-Shurmer, A.; O’Callaghan, M.J.; Najman, J.M.; Bor, W.; Williams, G.M.; Anderson, M.J. Association of bullying with adolescent health-related quality of life. J. Paediatr. Child Health 2003, 39, 436–441. [Google Scholar] [CrossRef]
- Sigurdson, J.F.; Wallander, J.; Sund, A.M. Is involvement in school bullying associated with general health and psychosocial adjustment outcomes in adulthood? Child Abuse Negl. 2014, 10, 1607–1617. [Google Scholar] [CrossRef]
- Takizawa, R.; Maughan, B.; Arseneault, L. Adult health outcomes of childhood bullying victimization: Evidence from a five-decade longitudinal British birth cohort. Am. J. Psychiatry 2014, 171, 777–784. [Google Scholar] [CrossRef]
- Ferner, R.E.; Huson, S.M.; Thomas, N.; Moss, C.; Willshaw, H.; Evans, D.G.; Upadhyaya, M.; Towers, R.; Gleeson, M.; Steiger, C.; et al. Guidelines for the diagnosis and management of individuals with neurofibromatosis 1. J. Med. Genet. 2007, 44, 81–88. [Google Scholar] [CrossRef]
- Gupta, M.A.; Gupta, A.K.; Ellis, C.N.; Koblenzer, C.S. Psychiatric evaluation of the dermatology patient. Dermatol. Clin. 2005, 23, 591–599. [Google Scholar] [CrossRef]
- Picardi, A.; Abeni, D.; Melchi, C.F.; Puddu, P.; Pasquini, P. Psychiatric morbidity in dermatological outpatients: An issue to be recognized. Br. J. Dermatol. 2000, 143, 983–991. [Google Scholar] [CrossRef]
- Rumsey, N.; Harcourt, D. Body image and disfigurement: Issues and interventions. Body Image 2004, 1, 83–97. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, J.A. Body image and self-esteem. In Encyclopedia of Body Image and Human Appearance, 1st ed.; Cash, T.F., Ed.; Academic Press: Waltham, MA, USA, 2012; pp. 141–147. [Google Scholar]
- Johnson, N.S.; Saal, H.M.; Lovell, A.M.; Schorry, E.K. Social and emotional problems in children with neurofibromatosis type 1: Evidence and proposed interventions. J. Pediatr. 1999, 134, 767–772. [Google Scholar] [CrossRef] [PubMed]
- Sebold, C.D.; Lovell, A.; Hopkin, R.; Noll, R.; Schorry, E. Perception of disease severity in adolescents diagnosed with neurofibromatosis type 1. J. Adolesc. Health 2004, 35, 297–302. [Google Scholar] [CrossRef]
- Wei, G.; Farooq, J.; Kumar, A. Impact of mind-body treatment interventions on quality of life in neurofibromatosis patients: A systematic review and meta-analysis. Dermatol. Ther. 2021, 34, e14613. [Google Scholar] [CrossRef] [PubMed]
- Taylor, L.A.; Lewis, V.L., Jr. Neurofibromatosis Type 1: Review of Cutaneous and Subcutaneous Tumor Treatment on Quality of Life. Plast. Reconstr. Surg. Glob. Open 2019, 7, e1982. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Males (n = 21) | Females (n = 17) | U Mann–Whitney/X² | p-Value | |
|---|---|---|---|---|
| Age, years mean (SD) | 13.80 (3.00) | 13.94 (3.02) | 172.00 | 0.84 |
| OV, mean (SD) | 9.61 (9.73) | 12.29 (15.74) | 173.00 | 0.86 |
| DHV, mean (SD) | 0.04 (0.21) | 1.4 (2.98) | 132.50 | 0.06 * |
| SU-T, mean (%) | 7 (35) | 5 (29.4) | 0.13 | 0.71 |
| PH-T, n (%) | 0 | 3 (17.6) | 4.02 | 0.04 * |
| NP, n (%) | 8 (38.1) | 4 (23.5) | 0.92 | 0.33 |
| Severity, mean (SD) | 1.71 (0.64) | 1.82 (0.72) | 165.00 | 0.66 |
| Visibility, mean (SD) | 1.42 (0.87) | 1.70 (.091) | 144.00 | 0.25 |
| Familiarity, n (%) | 8 (38.1) | 8 (47.1) | 0.31 | 0.57 |
| School support, n (%) | 5 (23.8) | 2 (11.8) | 0.90 | 0.34 |
| VICT, n (%) | 2 (9.5) | 7 (41.2) | 5.20 | 0.02 * |
| BUL, n (%) | 1 (4.8) | 2 (11.8) | 0.63 | 0.42 |
| CV, n (%) | 5 (23.8) | 7 (41.2) | 1.31 | 0.25 |
| CB, n (%) | 4 (19) | 2 (11.8) | 0.73 | 0.54 |
| CDI, mean (SD) | 5.38 (4.09) | 10.24 (6.67) | 94.50 | 0.01 * |
| CDI, n (%) | 0 | 2 (11.7) | 2.60 | 0.10 |
| RCMAS, mean (SD) | 6.14 (4.17) | 18.35 (8.50) | 41.00 | <0.01 * |
| RCMAS, n (%) | 0 | 7 (41.1) | 10.60 | <0.01 * |
| RSES, mean (SD) | 23.52 (14.17) | 16.41 (4.54) | 26.00 | 0.00 * |
| RSES, n (%) | 0 | 5 (29.4) | 7.11 | <0.01 * |
| PedsQoL-PS, mean (SD) | 79.31 (12.64) | 68.03 (15.37) | 101.00 | 0.02 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cavallo, N.D.; Maggi, G.; Ferraiuolo, F.; Sorrentino, A.; Perrotta, S.; Carotenuto, M.; Santangelo, G.; Santoro, C. Neuropsychiatric Manifestations, Reduced Self-Esteem and Poor Quality of Life in Children and Adolescents with Neurofibromatosis Type 1 (NF1): The Impact of Symptom Visibility and Bullying Behavior. Children 2023, 10, 330. https://doi.org/10.3390/children10020330
Cavallo ND, Maggi G, Ferraiuolo F, Sorrentino A, Perrotta S, Carotenuto M, Santangelo G, Santoro C. Neuropsychiatric Manifestations, Reduced Self-Esteem and Poor Quality of Life in Children and Adolescents with Neurofibromatosis Type 1 (NF1): The Impact of Symptom Visibility and Bullying Behavior. Children. 2023; 10(2):330. https://doi.org/10.3390/children10020330
Chicago/Turabian StyleCavallo, Nicola Davide, Gianpaolo Maggi, Francesco Ferraiuolo, Anna Sorrentino, Silverio Perrotta, Marco Carotenuto, Gabriella Santangelo, and Claudia Santoro. 2023. "Neuropsychiatric Manifestations, Reduced Self-Esteem and Poor Quality of Life in Children and Adolescents with Neurofibromatosis Type 1 (NF1): The Impact of Symptom Visibility and Bullying Behavior" Children 10, no. 2: 330. https://doi.org/10.3390/children10020330