
Effects of Rapid Palatal Expansion on the Upper Airway Space in Children with Obstructive Sleep Apnea (OSA): A Case-Control Study
 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Methods
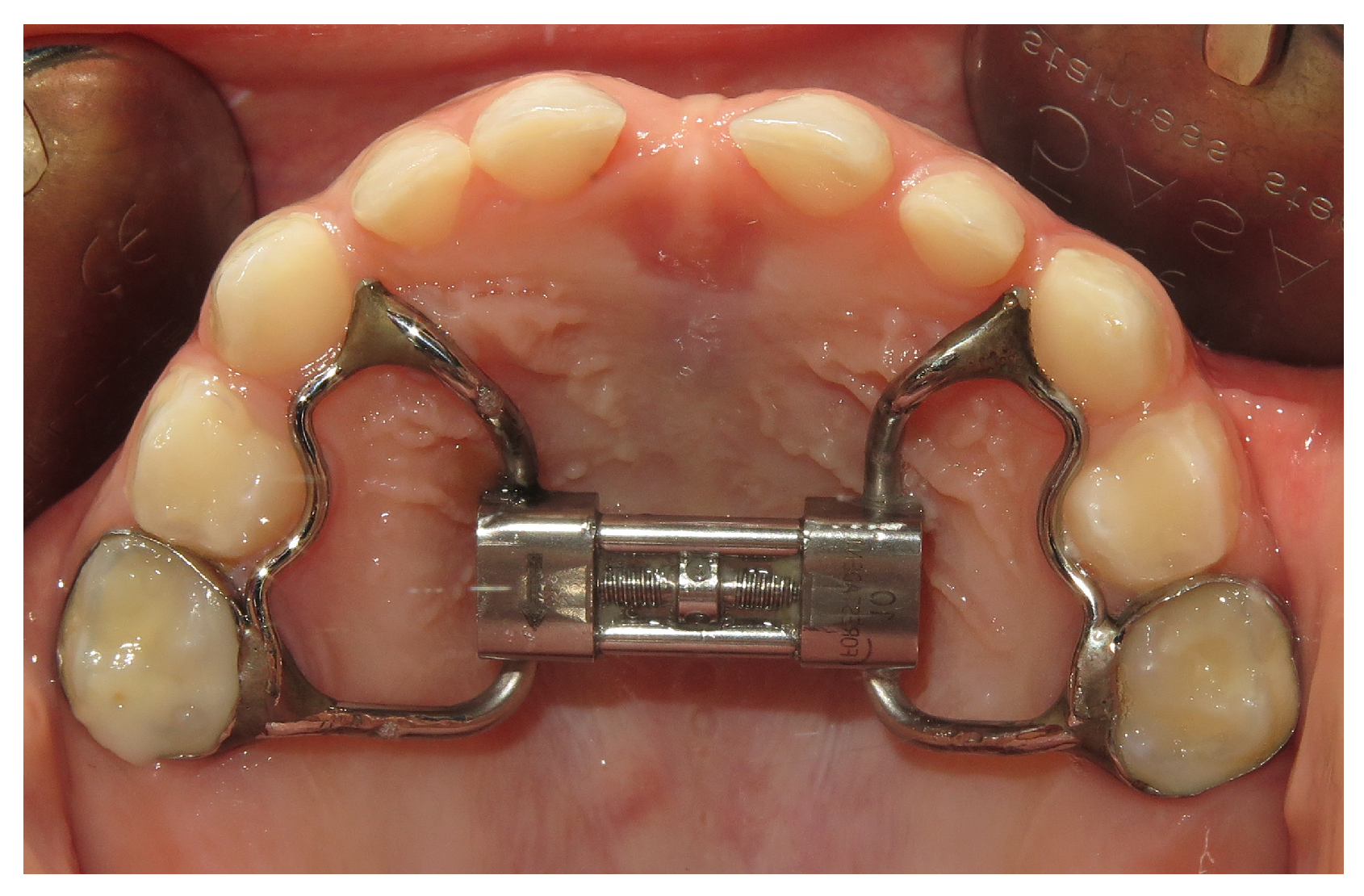
2.2.1. Rapid Palatal Expansion
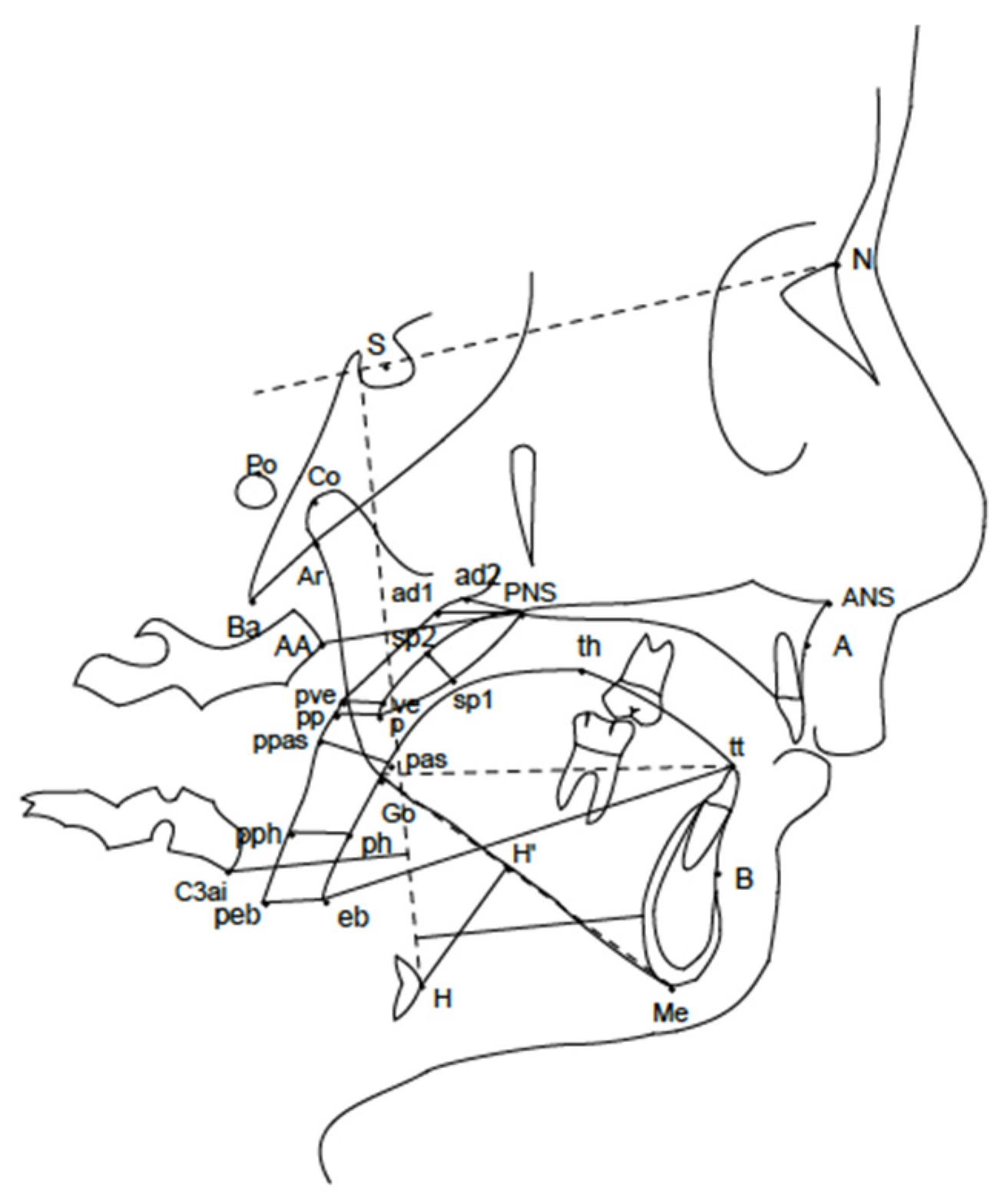
2.2.2. Cephalometric Analysis
2.3. Sample Size Calculation
2.4. Statistical Methods
3. Results
4. Discussion
- The use of a two-dimensional examination, but it was not possible to use a three-dimensional analysis which exposed patients to a massive radiation dose before and after treatment. For this reason, we evaluated the changes in sagittal and vertical direction, but the modifications were not studied in a transverse direction. Nevertheless, we assume that the increase of upper airways in millimeters might be much more substantial with 3D evaluation which analyzes the entire volume, as suggested by other studies [40,41].
- No home sleep study was performed after RPE treatment; therefore, this study does not provide data on the efficacy of orthodontic therapy.
- This study did not present long-term data.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Thoracic Society. Standards and indications for cardiopulmonary sleep studies in children. Am. J. Respir. Crit. Care Med. 1996, 153, 866–878. [Google Scholar] [CrossRef] [PubMed]
- Gulotta, G.; Iannella, G.; Vicini, C.; Polimeni, A.; Greco, A.; de Vincentiis, M.; Visconti, I.C.; Meccariello, G.; Cammaroto, G.; De Vito, A.; et al. Risk Factors for Obstructive Sleep Apnea Syndrome in Children: State of the Art. Int. J. Environ. Res. Public Health 2019, 16, 3235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paglia, L. Respiratory sleep disorders in children and role of the paediatric dentist. Eur. J. Pediatr. Dent. 2019, 20, 5. [Google Scholar]
- Marino, A.; Ranieri, R.; Chiarotti, F.; Villa, M.P.; Malagola, C. Rapid maxillary expansion in children with Obstructive Sleep Apnoea Syndrome (OSAS). Eur. J. Paediatr. Dent. 2012, 13, 57–63. [Google Scholar]
- Brunetti, L.; Rana, S.; Lospalluti, M.L.; Pietrafesa, A.; Francavilla, R.; Fanelli, M.; Armenio, L. Prevalence of obstructive sleep apnea syndrome in a cohort of 1207 children of southern Italy. Chest 2001, 120, 1930–1935. [Google Scholar] [CrossRef] [Green Version]
- Katyal, V.; Pamula, Y.; Martin, A.J.; Daynes, C.N.; Kennedy, J.D.; Sampson, W.J. Craniofacial and upper airway morphology in pediatric sleep-disordered breathing: Systematic review and meta-analysis. Am. J. Orthod. Dentofacial. Orthop. 2013, 143, 20–30. [Google Scholar] [CrossRef]
- Galeotti, A.; Festa, P.; Viarani, V.; Pavone, M.; Sitzia, E.; Piga, S.; Cutrera, R.; De Vincentis, G.C.; D’Antò, V. Correlation between cephalometric variables and obstructive sleep apnoea severity in children. Eur. J. Paediatr. Dent. 2019, 20, 43–47. [Google Scholar]
- Paradowska-Stolarz, A. MSX1 gene in the etiology orofacial deformities. Postepy Hig. Med. Dosw. 2015, 69, 1499–1504. [Google Scholar]
- Dastan, F.; Ghaffari, H.; Shishvan, H.H.; Zareiyan, M.; Akhlaghian, M.; Shahab, S. Correlation between the upper airway volume and the hyoid bone position, palatal depth, nasal septum deviation, and concha bullosa in different types of malocclusion: A retrospective cone-beam computed tomography study. Dent. Med. Probl. 2021, 58, 509–514. [Google Scholar] [CrossRef]
- Brennan, L.C.; Kirkham, F.J.; Gavlak, J.C. Sleep-disordered breathing and comorbidities: Role of the upper airway and craniofacial skeleton. Nat. Sci. Sleep 2020, 12, 907–936. [Google Scholar] [CrossRef]
- Hill, C.M.; Evans, H.J.; Elphick, H.; Farquhar, M.; Pickering, R.M.; Kingshott, R.; Martin, J.; Reynolds, J.; Joyce, A.; Rush, C.; et al. Prevalence and predictors of obstructive sleep apnoea in young children with Down syndrome. Sleep Med. 2016, 27–28, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Galeotti, A.; Festa, P.; Viarani, V.; D’Antò, V.; Sitzia, E.; Piga, S.; Pavone, M. Prevalence of malocclusion in children with obstructive sleep apnoea. Orthod. Craniofac. Res. 2018, 21, 242–247. [Google Scholar] [CrossRef]
- Bitners, A.C.; Arens, R. Evaluation and Management of Children with Obstructive Sleep Apnea Syndrome. Lung 2020, 198, 257–270. [Google Scholar] [CrossRef] [PubMed]
- Franco, R.A.; Rosenfeld, R.M.; Rao, M. First place—Resident clinical science award 1999 Quality of life for children with obstructive sleep apnea. Otolaryngol. Head Neck Surg. 2000, 123, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Chervin, R.D.; Hedger, K.; Dillon, J.E.; Pituch, K.J. Pediatric sleep questionnaire (PSQ): Validity and reliability of scales for sleep-disordered breathing, snoring, sleepiness, and behavioral problems. Sleep Med. 2000, 1, 21–32. [Google Scholar] [CrossRef]
- American Academy of Pediatrics. Clinical practice guideline: Diagnosis and managment of childhood obstructive sleep apnea syndrome. Pediatrics 2002, 109, 704–712. [Google Scholar] [CrossRef] [Green Version]
- Villa, M.P.; Pietropaoli, N.; Supino, M.C.; Vitelli, O.; Rabasco, J.; Evangelisti, M.; Del Pozzo, M.; Kaditis, A.G. Diagnosis of Pediatric Obstructive Sleep Apnea Syndrome in Settings With Limited Resources. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Kang, K.T.; Weng, W.C.; Lee, P.L.; Hsu, W.C. Quality of life after adenotonsillectomy in children with obstructive sleep apnea: Short-term and long-term results. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 210–215. [Google Scholar] [CrossRef]
- Katyal, V.; Kennedy, D.; Martin Dreyer, C.; Sampson, W. Paediatric sleep-disorder breathing due to upper airway obstruction in the orthodontic setting: A review. Aust. Orthod. J. 2013, 29, 184–192. [Google Scholar]
- Brouillette, R.T.; Horwood, L.; Constantin, E.; Brown, K.; Ross, N.A. Childhood sleep apnea and neighborhood disadavantage. J. Pediatr. 2011, 158, 789–795. [Google Scholar] [CrossRef]
- Ngiam, J.; Cistulli, P.A. Dental treatment for paediatric obstructive sleep apnea. Paediatr. Respir. Rev. 2015, 16, 174–181. [Google Scholar] [CrossRef]
- Pereira, J.D.S.; Jacob, H.B.; Locks, A.; Brunetto, M.; Ribeiro, G.L.U. Evaluation of the rapid and slow maxillary expansion using cone-beam computed tomography: A randomized clinical trial. Dent. Press J. Orthod. 2017, 22, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buccheri, A.; Chinè, F.; Fratto, G.; Manzon, L. Rapid Maxillary Expansion in Obstructive Sleep Apnea in Young Patients: Cardio-Respiratory Monitoring. J. Clin. Pediatr. Dent. 2017, 41, 312–316. [Google Scholar] [CrossRef] [PubMed]
- Baratieri, C.; Alves, M., Jr.; de Souza, M.G.; de Souza Araùjo, M.T.; Cople Maia, L. Does rapid maxillary expansion have long-term effects on airway dimensions and breathing? Am. J. Orthod. Dentofacial. Orthop. 2011, 140, 146–156. [Google Scholar] [CrossRef]
- Galeotti, A.; Festa, P.; Pavone, M.; De Vincentis, G.C. Effects of simultaneous palatal expansion and mandibular advancement in a child suffering from OSA. Acta Otorhinolaryngol. Ital. 2016, 36, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Pirelli, P.; Fanucci, E.; Giancotti, A.; Di Girolamo, M.; Guilleminault, C. Skeletal changes after rapid maxillary expansion in children with obstructive sleep apnea evaluated by low-dose multi-slice computed tomography. Sleep Med. 2019, 60, 75–80. [Google Scholar] [CrossRef]
- Brouillette, R.T.; Morielli, A.; Leimanis, A.; Waters, K.A.; Luciano, R.; Ducharme, F.M. Nocturnal pulse oximetry as an abbreviated testing modality for pediatric obstructive sleep apnea. Pediatrics 2000, 105, 405–412. [Google Scholar] [CrossRef]
- Kirjavainen, M.; Kirjavainen, T. Upper airway dimensions in class II malocclusion. Effects of headgear treatment. Angle Orthod. 2007, 77, 1046–1053. [Google Scholar] [CrossRef]
- Dahlberg, G. Statistical Methods for Medical and Biological Students; George Allen & Unwin: London, UK, 1940; 232p. [Google Scholar]
- Houston, W.J. The analysis of errors in orthodontic measurements. Am. J. Orthod. 1983, 83, 382–390. [Google Scholar] [CrossRef]
- Sakai, R.H.; de Assumpção, M.S.; Ribeiro, J.D.; Sakano, E. Impact of rapid maxillary expansion on mouth-breathing children and adolescents: A systematic review. J. Clin. Exp. Dent. 2021, 13, 1258–1270. [Google Scholar] [CrossRef]
- Bucci, R.; Montanaro, D.; Rongo, R.; Valletta, R.; Michelotti, A.; D’Antò, V. Effects of maxillary expansion on the upper airways. Evidence from systematic reviews and meta-analyses. J. Oral Rehabil. 2019, 46, 377–387. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Henriquez, C.; Capasso, R.; Chiesa-Estomba, C.; Yung Liu, S.; Martins-Neves, S.; Castedo, E.; O’Connor-Reina, C.; Ruano-Ravina, A.; Kahn, S. The role of pediatric maxillary expansion on nasal breathing. A systematic review and metanalysis. Int. J. Pediatr. Otorhinolaryngol. 2020, 135, 110139. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Di Carlo, G.; Cornelis, M.A.; Cattaneo, P.M. Three-dimensional analyses of short- and long-term effects of rapid maxillary expansion on nasal cavity and upper airway: A systematic review and meta-analysis. Orthod. Craniofac. Res. 2020, 23, 250–276. [Google Scholar] [PubMed]
- Radescu, O.D.; Colosi, H.A.; Albu, S. Effects of rapid palatal expansion (RPE) and twin block mandibular advancement device (MAD) on pharyngeal structures in Class II pediatric patients from Cluj-Napoca, Romania. Cranio 2020, 38, 22–29. [Google Scholar] [CrossRef]
- Aljawad, H.; Lee, K.M.; Lim, H.J. Three-dimensional evaluation of upper airway changes following rapid maxillary expansion: A retrospective comparison with propensity score matched controls. PLoS ONE 2021, 16, e0261579. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.C.; Tu, Y.K.; Chen, R.; Fu, M.W.; Fu, E. Pharyngeal airway changes following maxillary expansion or protraction: A meta-analysis. Orthod. Craniofac. Res. 2018, 21, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Aloufi, F.; Preston, C.B.; Zawawi, K.H. Changes in the upper and lower pharyngeal airway spaces associated with rapid maxillary expansion. ISRN Dent. 2012, 2012, 290964. [Google Scholar] [CrossRef] [Green Version]
- Iwasaki, T.; Saitoh, I.; Takemoto, Y.; Inada, E.; Kakuno, E.; Kanomi, R.; Hayasaki, H.; Yamasaki, Y. Tongue posture improvement and pharyngeal airway enlargement as secondary effects of rapid maxillary expansion: A cone-beam computed tomography study. Am. J. Orthod. Dentofacial. Orthop. 2013, 143, 235–245. [Google Scholar] [CrossRef]
- Ribeiro, A.N.; de Paiva, J.B.; Rino-Neto, J.; Illipronti-Filho, E.; Trivino, T.; Fantini, S.M. Upper airway expansion after rapid maxillary expansion evaluated with cone beam computed tomography. Angle Orthod. 2012, 82, 458–463. [Google Scholar] [CrossRef] [Green Version]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Ward, S.D.; Sheldon, S.H.; Shiffman, R.N.; et al. American Academy of Pediatrics. Diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2012, 130, 714–755. [Google Scholar] [CrossRef] [Green Version]
- Pirelli, P.; Fiaschetti, V.; Fanucci, E.; Giancotti, A.; Saccomanno, S.; Mampieri, G. Cone beam CT evaluation of skeletal and nasomaxillary complex volume changes after rapid maxillary expansion in OSA children. Sleep Med. 2021, 86, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Vogler, R.C.; Ii, F.J.; Pilgram, T.K. Age-specific size of the normal adenoid pad on magnetic resonance imaging. Clin. Otolaryngol. Allied Sci. 2000, 25, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Arens, R.; Marcus, C.L. Patophysiology of upper airway obstruction: A developmental perspective. Sleep 2004, 27, 997–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, J.B.; Anselmo-Lima, W.T.; Valera, F.C.; Gallego, A.J.; Matsumoto, M.A. Cephalometric assessment of the mandibular growth pattern in mouth-breathing children. J. Pediatr. Otorhinolaryngol. 2005, 69, 311–317. [Google Scholar] [CrossRef]
- Cozza, P.; Giancotti, A.; Petrosino, A. Rapid palatal expansion in mixed dentition using a modified expander: A cephalometric investigation. J. Orthod. 2001, 28, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Lineberger, M.W.; McNamara, J.A.; Baccetti, T.; Herberger, T.; Franchi, L. Effects of rapid maxillary expansion in hyperdivergent patients. Am. J. Orthod. Dentofacial. Orthop. 2012, 142, 60–69. [Google Scholar] [CrossRef]
- Machado-Júnior, A.J.; Zancanella, E.; Crespo, A.N. Rapid maxillary expansion and obstructive sleep apnea: A review and meta-analysis. Med. Oral Patol. Oral Cir. Bucal 2016, 21, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Vale, F.; Albergaria, M.; Carrilho, E.; Francisco, I.; Guimarães, A.; Caramelo, F.; Maló, L. Efficacy of Rapid Maxillary Expansion in the Treatment of Obstructive Sleep Apnea Syndrome: A Systematic Review With Meta-analysis. J. Evid. Based Dent. Pract. 2017, 17, 159–168. [Google Scholar] [CrossRef]
- Guilleminault, C.; Quo, S.; Huynh, N.T.; Li, K. Orthodontic expansion treatment and adenotonsillectomy in the treatment of obstructive sleep apnea in prepubertal children. Sleep 2008, 31, 953–957. [Google Scholar]



{kind=link}
{kind=link}
| Nasopharynx | |
| ad1-PNS | The distance of ad1 point to PNS (posterior nasal spine). Ad1 is the intersection point of posterior pharyngeal wall and the line from PNS to Basion (Ba) |
| ad2-PNS | The distance of ad2 point to PNS. Ad2 is the intersection point of posterior pharyngeal wall and the line from the midpoint of the line from sella (S) to basion (Ba) to PNS |
| Oropharynx | |
| p-pp | The distance of the tip of soft palate (p) to horizontal counterpoint on posterior pharyngeal wall (pp) |
| pa | The distance of the intersection points on anterior and posterior pharyngeal wall of the line from supramentale (B) to gonion (Go) |
| Hyoid bone | |
| H-H′ | The distance from the most anterior and superior point of hyoid bone (H) perpendicular to mandibular plane (MP). |
| Maxilla | |
| SNA | The angle sella (S) to nasion (N) to subspinale (A) |
| Mandible | |
| SNB | The angle sella (S) to nasion (N) to supramentale (B) |
| ANB | The angle subspinale (A) to nasion (N) to supramentale (B) |
| Facial heights | |
| S-Go | The distance from sella (S) to gonion (Go) |
| N-Me | The distance from nasion (N) to menton (Me) |
| P-A face height (S-Go/N-Me)% | The ratio between S-Go/N-Me |
| Typology | |
| SN-MP | The angle nasion (N) to sella (S) to mandibular plane (MP). |
| PP-MP | The angle PP to MP. PP is the line from anterior nasal spine (ANS) to PNS |
| Cranial base | |
| SN | The distance from sella (S) to nasion (N) |
| Cephalometric Variables | Time | Mean Difference by Time | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T1–T0 | ||||||
| Mean | SD | 95% CI | Mean | SD | 95% CI | |||
| SNA (°) | 80.9 | 4.43 | 79.4–82.4 | 80.81 | 4.76 | 79.2–82.4 | −0.07 | 0.866 |
| SNB (°) | 75.6 | 3.97 | 74.3–76.9 | 75.8 | 3.9 | 74.5–77.2 | 0.26 | 0.492 |
| ANB (°) | 5.29 | 3.1 | 4.2–6.3 | 4.96 | 2.3 | 4.2–5.7 | −0.32 | 0.381 |
| SN (mm) | 58.3 | 5.8 | 56.4–60.3 | 59.96 | 4.3 | 58.5–61.4 | 1.63 | 0.136 |
| SN/MP (°) | 38.3 | 5.8 | 36.4–40.3 | 37.9 | 6.0 | 35.9–39.9 | −0.46 | 0.320 |
| PP/MP (°) | 32.1 | 5.6 | 30.2–33.9 | 30.9 | 5.3 | 29.2–32.7 | −1.14 | 0.043 * |
| P-A face height (S-Go/N-Me) (%) | 61.5 | 5.2 | 59.8–63.2 | 61.9 | 5.3 | 60.2–63.7 | 0.47 | 0.299 |
| ad1-PNS (mm) | AD | 5.6 | 9.2–12.9 | 14.6 | 5.6 | 12.7–16.5 | 3.48 | <0.001 * |
| ad2-PNS (mm) | 7.5 | 3.6 | 6.3–8.6 | 9.1 | 3.9 | 7.8–10.5 | 1.67 | 0.003 * |
| p-pp (mm) | 13.3 | 4.2 | 11.9–14.7 | 13.0 | 4.3 | 11.6–14.5 | −0.25 | 0.795 |
| pas-ppas (mm) | 14.3 | 3.6 | 13.1–15.5 | 14.1 | 3.5 | 12.9–15.2 | −0.21 | 0.760 |
| eb-peb (mm) | 15.2 | 5.0 | 13.6–16.9 | 14.5 | 5.4 | 12.7–16.3 | −0.7 | 0.539 |
| H-H′ (GnGo-H) (mm) | 13.9 | 4.9 | 12.2–15.5 | 14.0 | 5.3 | 12.2–15.8 | 0.14 | 0.873 |
| Cephalometric Variables | Time | Mean Difference by Time | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T1–T0 | ||||||
| Mean | SD | 95% CI | Mean | SD | 95% CI | |||
| SNA (°) | 81.2 | 4.1 | 80.5–83.1 | 81.0 | 5.0 | 79.9–83.2 | 0.2 | 0.639 |
| SNB (°) | 78.4 | 4.3 | 77.0–79.7 | 78.3 | 4.7 | 77.6–79.8 | 0.1 | 0.809 |
| ANB (°) | 3.4 | 2.4 | 2.7–4.2 | 3.3 | 2.2 | 2.6–4.0 | 0.1 | 0.663 |
| SN (mm) | 61.3 | 5.1 | 59.6–62.9 | 63.2 | 7.0 | 60.9–65.4 | −1.9 | 0.038 |
| SN/MP (°) | 34.5 | 5.5 | 32.7–36.3 | 35.4 | 7.2 | 33.1–37.7 | −0.9 | 0.375 |
| PP/MP (°) | 28.4 | 5.4 | 26.6–30.1 | 27.7 | 4.8 | 26.1–29.3 | 0.6 | 0.260 |
| P-A face height (S-Go/N-Me) (%) | 63.8 | 4.9 | 62.2–65.4 | 64.0 | 4.3 | 62.6–65.4 | −0.2 | 0.746 |
| ad1-pns (mm) | 15.6 | 6.5 | 13.5–17.7 | 16.7 | 5.0 | 15.1–18.3 | −1.1 | 0.108 |
| ad2-pns (mm) | 8.6 | 4.0 | 7.3–9.9 | 9.2 | 3.2 | 8.1–10.2 | −0.5 | 0.267 |
| p-pp (mm) | 11.3 | 4.6 | 9.9–12.8 | 10.7 | 4.6 | 9.2–12.1 | 0.7 | 0.281 |
| pas-ppas (mm) | 12.5 | 3.8 | 11.3–13.7 | 12.1 | 4.0 | 10.8–13.4 | 0.4 | 0.396 |
| eb-peb (mm) | 16.5 | 4.7 | 15.0–18.0 | 17.0 | 4.9 | 15.4–18.6 | −0.4 | 0.624 |
| H-H’ (GnGo-H) (mm) | 11.0 | 5.1 | 9.4–12.7 | 10.3 | 5.5 | 8.5–12.1 | 0.7 | 0.299 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galeotti, A.; Gatto, R.; Caruso, S.; Piga, S.; Maldonato, W.; Sitzia, E.; Viarani, V.; Bompiani, G.; Aristei, F.; Marzo, G.; et al. Effects of Rapid Palatal Expansion on the Upper Airway Space in Children with Obstructive Sleep Apnea (OSA): A Case-Control Study. Children 2023, 10, 244. https://doi.org/10.3390/children10020244
Galeotti A, Gatto R, Caruso S, Piga S, Maldonato W, Sitzia E, Viarani V, Bompiani G, Aristei F, Marzo G, et al. Effects of Rapid Palatal Expansion on the Upper Airway Space in Children with Obstructive Sleep Apnea (OSA): A Case-Control Study. Children. 2023; 10(2):244. https://doi.org/10.3390/children10020244
Chicago/Turabian StyleGaleotti, Angela, Roberto Gatto, Silvia Caruso, Simone Piga, Wanda Maldonato, Emanuela Sitzia, Valeria Viarani, Gaia Bompiani, Francesco Aristei, Giuseppe Marzo, and et al. 2023. "Effects of Rapid Palatal Expansion on the Upper Airway Space in Children with Obstructive Sleep Apnea (OSA): A Case-Control Study" Children 10, no. 2: 244. https://doi.org/10.3390/children10020244