
A 5-Year-Old Child with a Deep Neck Abscess Complicated by Laryngeal Obstruction
 , ,
, , 
Abstract
:1. Introduction
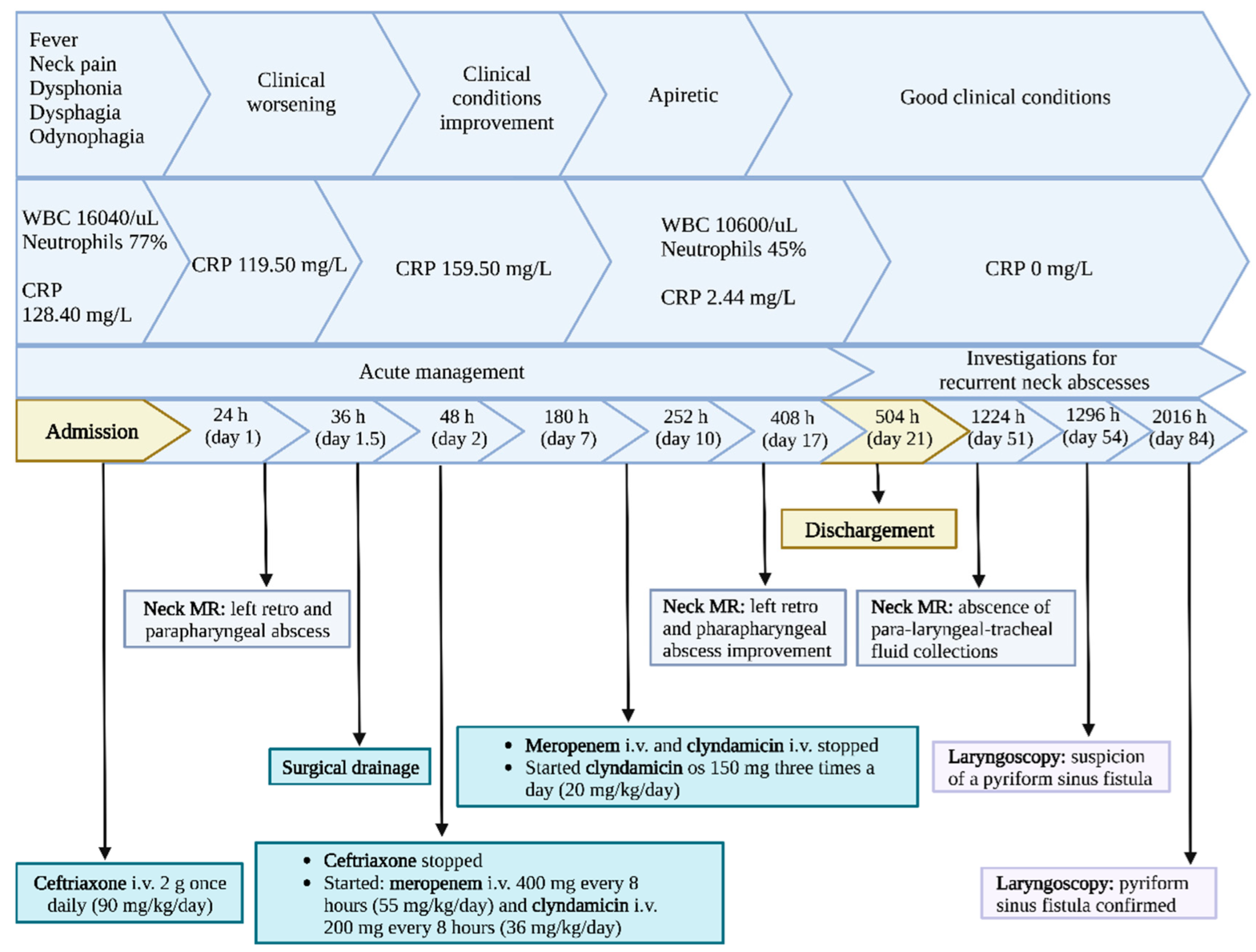
2. Case Report
2.1. Acute Presentation
2.2. Investigations for Recurrent Neck Abscesses
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AP | Antero-posterior |
| CT | Computed Tomography |
| CXR | Chest X-ray |
| DNM | Descending Necrotizing Mediastinitis |
| DNSI | Deep Neck Space Infection |
| EMG | Electromyography |
| ENT | Ear Nose Throat |
| IGRA | Interferon-Gamma Release Assays |
| LL | Latero-lateral |
| MRI | Magnetic Resonance Imaging |
| MRSA | Methicillin-Resistant Staphylococcus aureus |
| PSF | Pyriform Sinus Fistula |
| TID | Ter in Die |
| US | Ultrasound |
References
- Huang, C.M.; Huang, F.L.; Chien, Y.L.; Chen, P.Y. Deep neck infections in children. J. Microbiol. Immunol. Infect. 2017, 50, 627–633. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Gao, B.L.; Xu, G.P.; Xiang, C. Images of deep neck space infection and the clinical significance. Acta Radiol. 2014, 55, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Sansone, F.; Attanasi, M.; Di Filippo, P.; Sferrazza Papa, G.P.; Di Pillo, S.; Chiarelli, F. Usefulness of Lung Ultrasound in Paediatrics Respiratory Diseases. Diagnostics 2021, 28, 1783. [Google Scholar] [CrossRef] [PubMed]
- Yellon, R.F.; Bluestone, C.D.; Casselbrant, M.L.; Stool, S.E.; GonzÁAlez-Valdepena, H.; Bluestone, C.D. Head and neck space infections. In Paediatric Otolaryngology, 24th ed.; Saunders: Philadelphia, PA, USA, 2003; pp. 1681–1701. [Google Scholar]
- Gonzalez-Beicos, A.; Nunez, D. Imaging of acute head and neck infections. Radiol. Clin. N. Am. 2012, 50, 73–83. [Google Scholar] [CrossRef] [PubMed]
- Wippold, F.J., 2nd. Head and neck imaging: The role of CT and MRI. J. Magn. Reson. Imaging 2007, 25, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Hansen, B.W.; Ryndin, S.; Mullen, K.M. Infections of Deep Neck Spaces. Semin. Ultrasound CT MR 2020, 41, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Tebruegge, M.; Curtis, N. Infections related to the upper and middle airways. In Principles and Practice of Pediatric Infectious Diseases, 5th ed.; Long, S.S., Prober, C.G., Fischer, M., Eds.; Elsevier Saunders: New York, NY, USA, 2018; p. 208. [Google Scholar]
- Cheng, J.; Elden, L. Children with deep space neck infections: Our experience with 178 children. Otolaryngol. Head Neck Surg. 2013, 148, 1037–1042. [Google Scholar] [CrossRef] [PubMed]
- Carbone, P.N.; Capra, G.G.; Brigger, M.T. Antibiotic therapy for pediatric deep neck abscesses: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2012, 76, 1647–1653. [Google Scholar] [CrossRef] [PubMed]
- Jain, H.; Knorr, T.L.; Sinha, V. Retropharyngeal Abscess. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441873/ (accessed on 12 September 2022).
- Vieira, F.; Allen, S.M.; Stocks, R.M.; Thompson, J.W. Deep neck infection. Otolaryngol. Clin. North Am. 2008, 41, 459–483. [Google Scholar] [CrossRef] [PubMed]
- Songu, M.; Demiray, U.; Adibelli, Z.H.; Adibelli, H. Bilateral deep neck space infection in the paediatric age group: A case report and review of the literature. Acta Otorhinolaryngol. Ital. 2011, 31, 190–193. [Google Scholar] [PubMed]
- Yang, W.; Hu, L.; Wang, Z.; Nie, G.; Li, X.; Lin, D.; Luo, J.; Qin, H.; Wu, J.; Wen, W.; et al. Deep Neck Infection: A Review of 130 Cases in Southern China. Medicine 2015, 94, e994. [Google Scholar] [CrossRef] [PubMed]
- Abbas, P.I.; Roehm, C.E.; Friedman, E.M.; Athanassaki, I.; Kim, E.S.; Brandt, M.L.; Lopez, M.E. Successful endoscopic ablation of a pyriform sinus fistula in a child: Case report and literature review. Pediatr. Surg. Int. 2016, 32, 623–627. [Google Scholar] [CrossRef]
- Madana, J.; Yolmo, D.; Gopalakrishnan, S.; Saxena, S.K. Complete congenital third branchial fistula with left-sided, recurrent, suppurative thyroiditis. J. Laryngol. Otol. 2010, 124, 1025–1029. [Google Scholar] [CrossRef]
- Frisdal, A.; Trainor, P.A. Development and evolution of the pharyngeal apparatus. Wiley Interdiscip Rev. Dev. Biol. 2014, 3, 403–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mou, J.W.; Chan, K.W.; Wong, Y.S.; Houben, C.H.; Tam, Y.H.; Lee, K.H. Recurrent deep neck abscess and piriform sinus tract: A 15-year review on the diagnosis and management. J. Pediatr. Surg. 2014, 49, 1264–1267. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.; Tai, J.; Gao, J.; Wang, S.; Yu, T.; Peng, Y.; Ni, X. MRI in Children With Pyriform Sinus Fistula. J. Magn. Reson. Imaging 2021, 53, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Ge, G.; Chen, J.; Zhao, X.; Sheng, Q.; Zhu, L.; Xu, W.; Liu, J.; Lv, Z. Pyriform Sinus Fistula in Children: Preferred Imaging Modality and Risk Factors for Diagnostic Delay. Front. Pediatr. 2020, 8, 575812. [Google Scholar] [CrossRef] [PubMed]
- Bansal, S.; Jaswal, A.; Gupta, A.K. Complete Pyriform Sinus Fistulas: Case Series and Review of Literature. Int. J. Head Neck Surg. 2011, 2, 134–137. [Google Scholar]
- Chen, W.; Chen, J.; Chen, F.; Wu, J.; Zhao, L.; Xu, H.; Li, X. Endoscopic coblation treatment for congenital pyriform sinus fistula in children. Medicine 2021, 100, e25942. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Diagnosis | Imaging Findings |
|---|---|---|
| Pharyngotonsillitis | Clinical Examination | - |
| Peritonsillar Abscess | Clinical Examination ± Neck Ultrasound | Complex, hypoechoic collection 5–25 mm anteromedial to the internal carotid artery |
| Parapharyngeal Abscess | Neck CT ± MRI | Expansive Process, Airway Compression; Dislocation; Edema, Imbibition and Contrast Impregnation of muscles/fascial planes, “Danger Space” Involvement |
| Retropharyngeal Abscess | Neck CT ± MRI | Expansive Process, Airway Compression; Dislocation; Edema, Imbibition and Contrast Impregnation of muscles/fascial planes, “Danger Space” Involvement |
| Acute Epiglottitis | Clinical Examination ± Neck CT | Marked edema and thickening of the epiglottis and aryepiglottic folds with narrowing of the airway |
| Bacterial Tracheitis/Croup | Clinical Examination | Normal |
| CNS Tumor | Brain CT ± MRI | Expansive Lesions, Cyst/Nodule, Calcifications, Necrosis, Hemorrhage |
| CNS Infection | Brain CT ± MRI | Ring Enhancing Lesions, Basal Ganglia Alterations, White/Gray Matter T2 Hyperintensity |
| Apical Pneumonia | Clinical Examination ± CXR | Upper Lobes Opacity |
| Fractures/Dislocations | Cervical X-ray (AP + LL Projection) | Irregular and Non-corticated Vertebral Line Vertebral Disk Space Widening Bilateral Interfacetal Dislocation |
| Neck Muscle Hematomas | Neck MRI | Soft Tissue/Muscle Swelling |
| Cervical Dystonia | Clinical Examination ± EMG ± MRI | Possible Structural Brain Alterations |
| Foreign Body Ingestion | CXR + Abdomen X-ray (if Radiopaque) | Radiopaque Foreign Body within Gastro-Intestinal Tract |
| Acute Esophagitis | History + Clinical Examination ± Endoscopy ± Esophageal pH Monitoring | - |
| Malignant Etiology | CT/MRI + Biopsy Confirmation | Expansive Lesions with Earlier and Faster Uptake of Contrast Material |
| Ocular Dysfunction | Eye Examination + Vision Testing | - |
| Temporomandibular Arthritis in Juvenile Idiopathic Arthritis | Clinical Examination | - |
| Kawasaki Disease | Clinical Examination | - |
| Autoimmune Granulomatous Diseases | Clinical Examination + Laboratory studies | - |
| Thyroiditis | Clinical Examination + Laboratory studies + Thyroid US | Nodular lesions, nonnodular lesions |
| Pediatric Thyroid Cancer | History + Clinical Examination + Laboratory studies + Thyroid US + Neck CT +Fine Needle Aspiration | Solid nodules, cystic lesions, lesions with a thick irregular halo |
| Pneumomediastinum | Clinical Examination + CXR | Thymic sail sign, “ring around the artery” sign, tubular artery sign, double bronchial wall sign, extrapleural sign |
| Child abuse | History + Clinical Examination ± CXR ± Neck US | Bone or soft tissue lesions |
| Acute Management Additional Exams | Results |
|---|---|
| Serology for Epstein-Barr virus | Negative |
| Serology for Cytomegalovirus | Negative |
| Serology for Toxoplasma gondii | Negative |
| Serology for Bartonella henselae | Negative |
| Serology for Adenovirus | Negative |
| Anti-streptolysin O | Negative |
| Pharyngeal swab for Group A Beta-Hemolitic Streptococcus | Negative |
| Culture for Staphylococcus Aureus | Negative |
| Culture for Streptococcus viridans | Negative |
| Culture for Escherichia coli | Negative |
| Culture for Klebsiella pneumoniae | Negative |
| Culture for Veilonella | Negative |
| Culture for Haemofilus influenzae | Negative |
| Culture for Enterobacter | Negative |
| Blood culture | Negative |
| Interferon gamma release assay (IGRA test) | Negative |
| Peripheral venous blood smear | Negative for blood and blood-related diseases |
| Investigations for recurrent neck abscesses | Results |
| Serum immunoglobulin level (IgM, IgA, IgG) | Normal level |
| B cell phenotyping profile | No humoral and B-cell immunity abnormality |
| T cell surface markers by flow cytometry | No cellular immunodeficiency |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Ludovico, A.; Raso, M.; Di Filippo, P.; Di Pillo, S.; Zappacosta, R.; Parruti, G.; Zingariello, P.; Chiarelli, F.; Attanasi, M. A 5-Year-Old Child with a Deep Neck Abscess Complicated by Laryngeal Obstruction. Children 2023, 10, 17. https://doi.org/10.3390/children10010017
Di Ludovico A, Raso M, Di Filippo P, Di Pillo S, Zappacosta R, Parruti G, Zingariello P, Chiarelli F, Attanasi M. A 5-Year-Old Child with a Deep Neck Abscess Complicated by Laryngeal Obstruction. Children. 2023; 10(1):17. https://doi.org/10.3390/children10010017
Chicago/Turabian StyleDi Ludovico, Armando, Massimiliano Raso, Paola Di Filippo, Sabrina Di Pillo, Roberta Zappacosta, Giustino Parruti, Pasquale Zingariello, Francesco Chiarelli, and Marina Attanasi. 2023. "A 5-Year-Old Child with a Deep Neck Abscess Complicated by Laryngeal Obstruction" Children 10, no. 1: 17. https://doi.org/10.3390/children10010017