
Redox Homeostasis in Muscular Dystrophies
by
 , , , and
, , , and
Nicola Mosca
1,† ,
,
Sara Petrillo
2,†,
Sara Bortolani
1,
Mauro Monforte
1,
Enzo Ricci
1,3,*,
Fiorella Piemonte
2,‡ and
Giorgio Tasca
1,*,‡ 1
Unità Operativa Complessa di Neurologia, Fondazione Policlinico Universitario A. Gemelli IRCCS, 00168 Roma, Italy
2
Unit of Muscular and Neurodegenerative Diseases, Ospedale Pediatrico Bambino Gesù, IRCCS, 00146 Rome, Italy
3
Istituto di Neurologia, Università Cattolica del Sacro Cuore, 00168 Roma, Italy
*
Authors to whom correspondence should be addressed.
†
Shared first authorship.
‡
Shared senior authorship.
Cells 2021, 10(6), 1364; https://doi.org/10.3390/cells10061364
Submission received: 27 April 2021
/
Revised: 27 May 2021
/
Accepted: 28 May 2021
/
Published: 1 June 2021
(This article belongs to the Special Issue The Role of Skeletal Muscle in Neuromuscular Diseases: From Cellular and Molecular Players to Therapeutic Interventions)
{kind=link}
{kind=link}
{kind=link}
Abstract
:In recent years, growing evidence has suggested a prominent role of oxidative stress in the pathophysiology of several early- and adult-onset muscle disorders, although effective antioxidant treatments are still lacking. Oxidative stress causes cell damage by affecting protein function, membrane structure, lipid metabolism, and DNA integrity, thus interfering with skeletal muscle homeostasis and functionality. Some features related to oxidative stress, such as chronic inflammation, defective regeneration, and mitochondrial damage are shared among most muscular dystrophies, and Nrf2 has been shown to be a central player in antagonizing redox imbalance in several of these disorders. However, the exact mechanisms leading to overproduction of reactive oxygen species and deregulation in the cellular antioxidants system seem to be, to a large extent, disease-specific, and the clarification of these mechanisms in vivo in humans is the cornerstone for the development of targeted antioxidant therapies, which will require testing in appropriately designed clinical trials.
1. Introduction
The oxidative damage caused by an overproduction of reactive oxygen species (ROS) to biomolecules may affect skeletal muscle homeostasis and functionality, thus exacerbating pathological conditions in hereditary myopathies and muscular dystrophies [1]. Indeed, muscle degeneration, mitochondrial dysfunction, inflammation, and insufficient muscle regeneration are strictly linked to oxidative stress, which stems from the imbalance between ROS generation and protection provided by antioxidants. When such a disequilibrium of redox homeostasis occurs, the first intracellular defense line is represented by the activation of the transcription factor nuclear factor erythroid 2-related factor 2 (Nrf2), the master regulator of antioxidant response [2]. Many Nrf2 inducers have been reported to counteract oxidative stress in several physiological and pathological conditions, by upregulating the antioxidant defenses, inhibiting inflammation, and improving mitochondrial function [3,4].
Muscular dystrophies are a phenotypically and genotypically heterogeneous group of inherited muscular disorders with common histopathological features that include inflammation, degeneration, necrosis, and fibrosis. In addition to the pathogenic consequence arising from individual gene mutations, oxidative stress has been identified as one of the most relevant causes of muscle damage in these disorders [1,5,6].
This review summarizes the current knowledge about the role of oxidative stress in the pathogenesis of muscular dystrophies and highlights potential new targets for therapies.
2. What Is Oxidative Stress and How Can It Affect Muscles?
ROS are signaling molecules moderately and continuously produced by skeletal muscles as a consequence of their contractile activity and high mitochondrial O2 consumption [6]. The main source of ROS production is located in the cytosol through the activity of nicotinamide adenine dinucleotide phosphate (NADPH) oxidases (NOX enzymes), xanthine oxidase (XO), and nitric oxide synthase (NOS), and by the mitochondrial electron transport chain [1]. When ROS exceed the antioxidant buffering capacity of tissues, oxidative stress occurs [7]. The upregulation of the endogenous antioxidant system is the main response to ROS-induced stress, aiming at scavenging excessive ROS before they cause harm to tissues. ROS can be catalytically neutralized by antioxidant enzymes, including superoxide dismutase (SOD), catalase (CAT), glutathione peroxidase (GPx), and peroxiredoxins (PRDX), and by the action of the tripeptide glutathione (GSH) that directly buffers ROS [1]. High levels of these antioxidants are present in oxidative muscle fibers (type I and IIa in mice) [8,9], and their deficiency is a hallmark of oxidative stress. A secondary antioxidant defense line also exists in cells and is represented by the enzymes belonging to the inducible phase II (i.e., the glutathione S-transferase family enzymes, GST), which are activated by a number of different byproducts, such as xenobiotics, drugs, lipid peroxidation products, and chemical compounds (isothiocyanates and phenols) [10]. In addition, other enzymes, such as heme oxygenase-1 (HO-1), are responsible for the synthesis of nonenzymatic antioxidants present in the skeletal muscle (biliverdin and bilirubin) and play an important role in the regulation of heme catabolism [8]. Lastly, nicotinamide adenine dinucleotide phosphate quinone oxidoreductase 1 (NQO1) is critical in cellular adaptation to stress and is significantly elevated in skeletal muscles in response to aerobic exercise [9].
The balance between production of ROS and antioxidant defenses plays a fundamental role in maintaining redox homeostasis in muscle, while redox imbalance may exacerbate the progression of several muscle diseases. This is particularly true for chronic disorders, such as muscular dystrophies, characterized by the exposure to continuous damage (e.g., due to the lack of dystrophin) and an inappropriate response to injury (e.g., inflammation and profibrotic response).
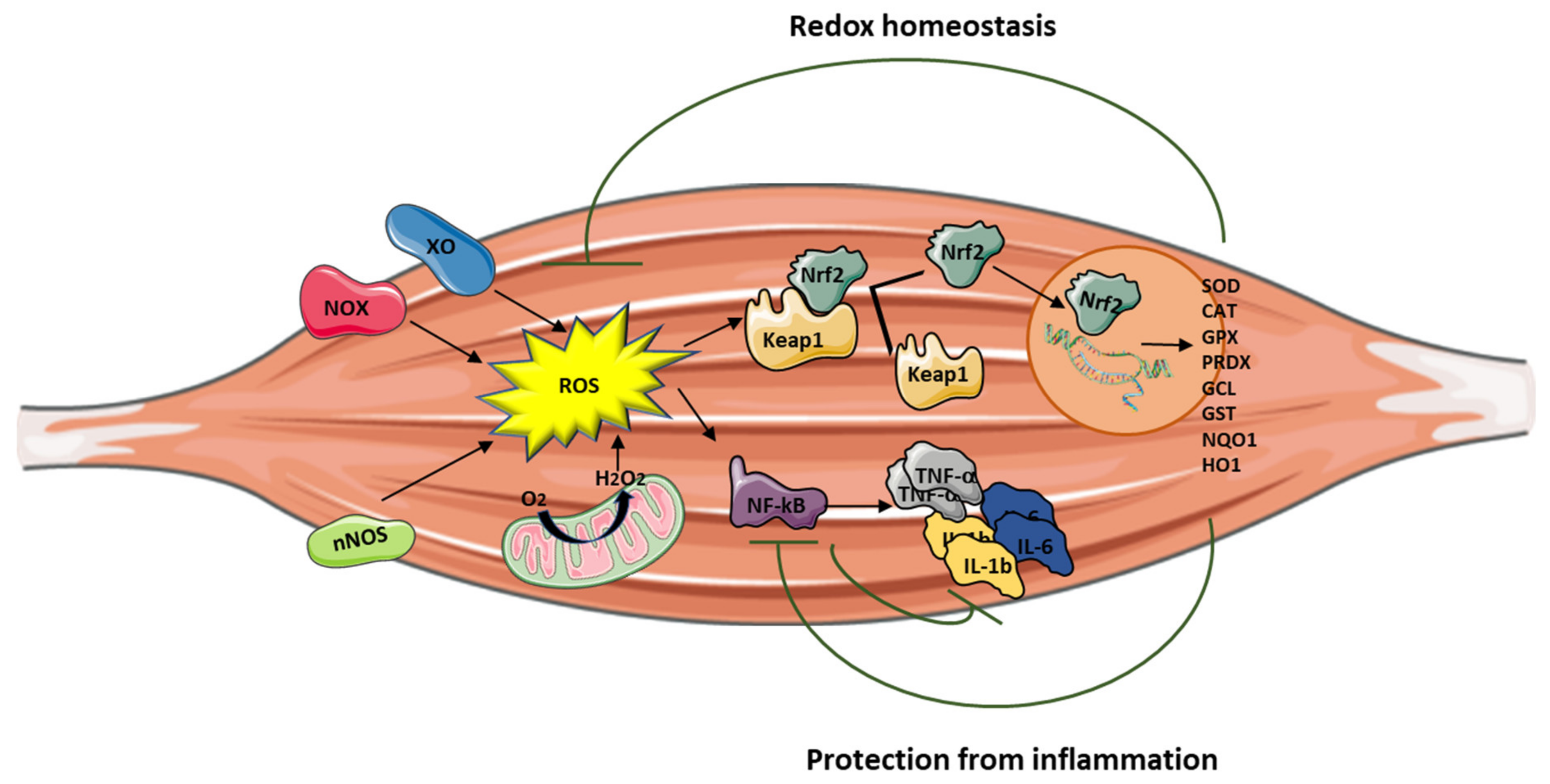
Although ROS have been reported to be mainly harmful, they also play a crucial role in cell signaling by activating Nrf2, which is in turn responsible for regulating the expression of more than 200 cytoprotective redox genes [11,12]. Nrf2 is a member of the basic leucine zipper (bZIP) family of transcription factors and is physiologically repressed through the binding to the protein Keap1 (Kelch-like ECH-associated protein 1) [12]. Upon exposure to ROS, Nrf2 is released from Keap1 and accumulates in the nucleus where it activates many antioxidant and anti-inflammatory target genes [12] (Figure 1). Nrf2 also modulates the NADPH oxidase enzyme activity, which has a central role in the pathophysiology of muscular dystrophies as source of ROS [13,14,15]. Thus, Nrf2 may have a critical role in the development of damage in muscular dystrophies, and its pharmacological activation can contribute to mitigate oxidative stress in muscles and to improve muscle performance [16,17].
3. The Role of Oxidative Stress in Muscle Inflammation
Inflammation can be triggered by an imbalance of cellular oxidative–antioxidant homeostasis. Usually, a moderate ROS production does not stimulate inflammation since ROS are mostly removed by cellular antioxidant systems. However, when ROS production, catalyzed by enzymes including NOX, COX-2, and XO, exceeds the threshold of redox balance, NF-κB is activated, thus triggering inflammation [18,19].
NF-κB is, therefore, the primary redox-sensitive signaling pathway of inflammation. The activation of protein kinase C (PKC) and NF-κB-induced kinase, a member of the MAPK family, is known to activate IKK, which phosphorylates the IκB subunit of the NF-κB complex and unleashes p50/p65 for nuclear binding [18,20]. As a result of NF-κB activation, proinflammatory cytokines, such as TNF-α, IL-1β, and IL-6, are produced by immune cells and/or damaged muscle tissues, thus further promoting the expression of adhesion molecules, including vascular cell adhesion molecule 1 (VCAM-1), cytokine-induced neutrophil chemoattractant-1 (CINC-1), and monocyte chemoattractant protein-1 (MCP-1), together with NOS upregulation [21]. Moreover, the NO production contributes to increase blood flow and the chemotactic effects of adhesion molecules, facilitating the infiltration of inflammatory cells into the affected area.
Mitochondria are also involved in the inflammatory process, and high levels of proinflammatory cytokines affect mitochondrial ROS generation and metabolic function. PGC-1α, which is a key regulator of muscle metabolism and mitochondrial biogenesis, also plays a role as an anti-inflammatory agent. Studies performed on PGC-1α KO mice models demonstrated high basal mRNA expression of TNF-α and IL-6 in skeletal muscle and in serum, showing that PGC-1α is able to effectively modulate local and systemic inflammation [22]. In addition, mice overexpressing PGC-1α showed low expression of TNF-α and IL-6 [23], suggesting that PGC-1α may play a protective role in the inflammatory response by reducing the generation of proinflammatory cytokines.
Nrf2 activation can attenuate inflammation by modulating the expression of NF-κB [16,24] (Figure 1). Thus, Nrf2 and NF-κB are interrelated in the inflammatory response [25]. Nrf2 exerts its anti-inflammatory function via the activation of HO-1 that catalyzes the degradation of heme into carbon monoxide (CO), free iron (Fe2+), and biliverdin, before being converted to the antioxidant bilirubin [25,26,27]. Muscle damage and inflammation worsened after ablation of HO-1 in the mdx mouse [28], while pharmacological induction of HO-1 exerted a protective effect on skeletal muscle through the inhibition of NF-κB [29].
It is important to note that Nrf2 binds DNA in proximity of the genes encoding IL-1β and IL-18 to modulate their transcription [30], thereby supporting its direct inhibitory effect on NOD-like receptor protein 3 (NLRP3) inflammasome priming.
4. Oxidative Stress in Early Onset Myopathies
Early-onset myopathies are inherited muscle diseases occurring during infancy or early childhood. These can be further classified into congenital muscular dystrophies (CMDs) and congenital myopathies (CMs) [31,32]. They are typically associated with muscle weakness and hypotonia, delayed motor development, and difficult or absent ambulation, sometimes with orthopedic complications, respiratory and cardiac failure, and, in the most severe forms, premature death [31].
CMDs and CMs have been classified on the basis of their major muscle morphological features. Patients with CMDs present dystrophic lesions on muscle biopsies, with or without necrotic fibers and regeneration, whereas, in congenital myopathies, muscles are generally not dystrophic but show characteristic structural changes in the internal fiber architecture [33]. CMDs and CMs share several pathophysiological pathways, involving proteins essential for the embryonic muscle development, the complex architectural structure of muscle fibers, the excitation/contraction coupling, and the redox regulation system [33].
The deregulation of redox homeostasis is a mechanism implicated in the pathogenesis of early-onset myopathies, and significant progress has been reached in the understanding of these diseases through the analysis of oxidative-mediated processes [34,35,36,37]. Proteins involved in redox regulation represent hallmarks and potential therapeutic targets in several early-onset myopathies, including RYR1- and SEPN1-related myopathies, and in Duchenne muscular dystrophy (DMD) [38,39,40,41].
RYR1-related myopathies are a group of skeletal muscle disorders caused by mutations in the ryanodine receptor gene, RYR1 [42]. They are clinically characterized by a wide spectrum of symptoms ranging from slowly progressive hip and axial muscle proximal weakness, to malignant hyperthermia [43,44]. RYR1, also known as skeletal muscle calcium release channel, is an essential component of the excitation–contraction coupling apparatus and contains many redox-sensitive reactive cysteines, strongly involved in calcium handling [45,46,47,48,49]. Mitochondrial dysfunction and redox imbalance have been associated with RYR1 primary defects, thus emerging as promising therapeutic targets for the disease. The use of N-acetylcysteine (NAC), the precursor of the antioxidant glutathione (GSH), improved muscle function and restored myotube phenotype in RYR1 mutated cell cultures and in the Y522S mouse model, opening the way to clinical trials in patients [50,51,52,53].
Defects in redox homeostasis have also been described in SEPN1-related myopathy, an inherited muscle disease caused by mutations in gene encoding selenoprotein-N (SELENON), which displays clinical and pathological overlap with RYR1-related myopathies [39]. Selenoproteins are a family of proteins containing several selenocysteine residues involved in modulating redox calcium homeostasis and protecting against oxidative stress [39]. In addition, the SEPN1 gene promoter contains sequences for NF-κB, the primary redox-sensitive signaling pathway in inflammation [39]. SEPN1-mutated patients often show a severe weakness of neck and trunk muscle, leading to scoliosis, spinal rigidity, and life-threatening respiratory insufficiency [54]. Limited motility and body rigidity after forced swimming test were reported in Sepn1-deficient mouse models [55], and increased protein oxidation, abrogated after pretreating cells with NAC, was described in myoblasts primary cultures from patients [56], leading to NAC clinical trials (SELNAC, clinicaltrials.gov, identifier: NCT02505087).
Increasing evidence shows a central role for oxidative stress in DMD and Becker muscular dystrophy (BMD), the most common muscular dystrophies in childhood. DMD is a severe X-linked recessive neuromuscular disorder affecting one in 3600 boys [57]. Muscle degeneration results in weakness, delayed motor milestones, and, eventually, loss of ambulation. DMD is caused by mutations in the gene encoding for dystrophin, a membrane protein whose absence is responsible for increased susceptibility to damage, with myofiber necrosis and secondary inflammation as a result of skeletal muscle contraction [57,58,59]. Dystrophin is also expressed in cardiomyocytes, and patients also develop cardiomyopathy. Mutations in the same gene may also result in a mildly defective dystrophin protein production, clinically corresponding to BMD, characterized by a less severe phenotype [57].
Oxidative stress makes the dystrophin-deficient heart and skeletal muscle highly susceptible to injury, exacerbating the pathological features of the disease [60,61,62,63,64]. NOX is the main source of ROS in dystrophin-deficient models, contributing to enhanced Ca2+ influx and activation of the Src kinase [65]. Furthermore, decreased levels of the antioxidant GSH, with a concomitant increase of its oxidized form GSSG and a reduced activity of the protective enzyme GPX, have been found in dystrophic muscles and in peripheral blood of patients with DMD [66,67]. Notably, preclinical studies using antioxidant drugs have evidenced beneficial effects on dystrophin-deficient mouse models, such as reduced muscle damage, decreased necrosis, inflammation, and fibrosis [68,69,70,71,72,73].
5. Oxidative Stress in Adult-Onset Muscular Dystrophies
Adult-onset muscular dystrophies are inherited disorders with different severity, age of onset, and type of muscle involvement. Among them, the most prevalent are myotonic dystrophy type 1 (Steinert disease), facioscapulohumeral muscular dystrophy, and limb girdle muscular dystrophies.
5.1. Facioscapulohumeral Muscular Dystrophy
Facioscapulohumeral muscular dystrophy (FSHD) is one of the most common forms of muscular dystrophy. It is characterized by a distinctive pattern of skeletal muscle weakness and a wide spectrum of disease severity. FSHD type 1 was mapped to chromosome 4q35 and is associated with a contraction in a macrosatellite repeat array known as D4Z4 [74,75]. This contraction, together with a polyadenylation signal distal to the repeats, allows the stable transcription of the DUX4 retrogene that is normally repressed in somatic tissues including skeletal muscle. The DUX4 protein is highly toxic and can induce apoptosis, through activation of caspase-3. Moreover, DUX4 expression in skeletal muscle can also lead to activation of different genes involved in atrophy, protein degradation, and innate immunity, and it negatively regulates myogenesis [76,77].
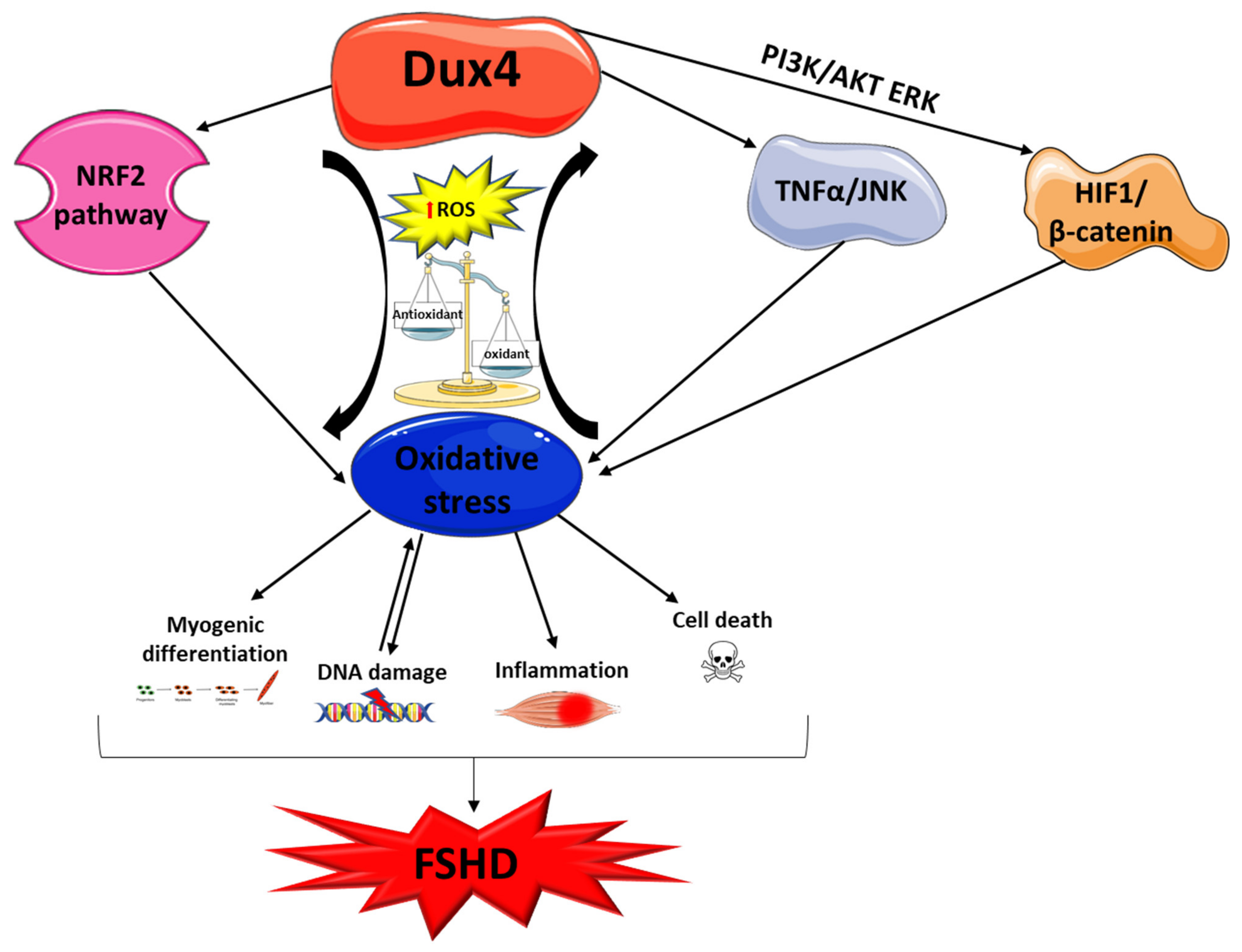
Since DUX4 is a central player in FSHD pathogenesis, different authors focused their attention on its role in the development of oxidative stress (Figure 2). Bosnakovski and colleagues showed that DUX4 alters the expression of genes implicated in redox balance and enhances the sensitivity of C2C12 myoblasts to pro-oxidant compounds, while antioxidant treatment reduced DUX4 toxicity [78,79]. Interestingly, oxidative stress induced by DUX4 is a direct cause of DNA damage, and both DNA damage and oxidative stress can also affect the myogenic differentiation process contributing to aberrant myotube formation [80]. Noteworthy is that DNA damage caused by moderate doses of oxidants is efficiently repaired in FSHD myoblasts, suggesting the capacity of handling oxidative stress up to a certain level [81]. On the other hand, the treatment of patient-derived induced pluripotent stem cells (iPSC) with H2O2 significantly increases the transcription of DUX4 and its targets. In this case, the DNA damage induced by oxidative stress occurs prior to DUX4 increase and this effect seems to be mediated by ataxia telangiectasia mutated serine/threonine kinase (ATM) activation [82]. This evidence shows that a feedback loop regulation may occur between DUX4 and oxidative stress contributing to muscle damage in FSHD. Furthermore, DUX4 can activate TNF-α and JNK pathways, increasing susceptibility to oxidative stress-induced cell death, as well as regulate hypoxia-inducible factor 1α (HIF1A) expression, which, upon interacting with β-catenin, inhibits cell proliferation and induces transcription of hypoxic response genes [83]. Interestingly, it is known that high levels of ROS can induce HIF-1α stabilization via PI3K/ATK and ERK pathways [84].
DUX4 is also able to modulate the Nrf2-mediated oxidative stress response pathway. Sharma and colleagues, in a transcriptomic study conducted on human rhabdomyosarcoma cells overexpressing DUX4, identified 31 out of the 86 transcripts known to function in the Nrf2 pathway as differentially expressed, with the majority of these changes potentially inducing or contributing to oxidative stress [85]. The study confirms the link between Nrf2 and DUX4, and it further highlights the role of DUX4 in the induction of oxidative stress.
Lastly, DUX4 seems to be negatively involved in the plasma membrane repair pathways. Indeed, Bittel and colleagues demonstrated, using a cellular and animal model, that DUX4 inhibition, as well as antioxidant treatment, is able to improve plasma membrane repair by reducing mitochondrial ROS levels [86].
Further evidence coming from earlier studies supports additional roles for oxidative stress in the development of muscle wasting in FSHD. Winokur and colleagues demonstrated that FSHD myoblasts are sensitive to oxidative stress upon exposure to paraquat and that this susceptibility is no longer seen upon differentiation to myotubes [87]. They also showed an alteration of several genes involved in oxidative stress, particularly a glutathione S-transferase theta-2 (GSTT2) downregulation, suggesting a reduced capacity to buffer oxidative stress [87]. Furthermore, ANT1, one of the most abundant mitochondrial inner membrane proteins, is reported to be increased in FSHD muscles with the highest level of protein detected in the clinically unaffected muscles, suggesting that this upregulation may be an early phenomenon in FSHD pathogenesis. Overexpression of ANT1 is associated with altered expression of different enzymes related to oxidative stress, such as SOD1, GST, and thioredoxin peroxidase [88,89,90]. Moreover, increased expression of ANT1 leads to recruitment of the IκBa/NF-κB complex into mitochondria, with a decrease in nuclear NF-κB DNA-binding activity. In this scenario, genes with antioxidant and antiapoptotic activity are downregulated and, consequently, muscle cells are sensitized to oxidative stress and apoptosis [91]. Another potential link between oxidative stress and FSHD muscle wasting is the mitochondria ultrastructure alteration in affected muscles. In FSHD, the mitochondrial ultrastructure of myofibers is altered, and mitochondria accumulate. In these regions, mitochondria present badly formed cristae or inner and outer membrane separation. These structural alterations are associated with mitochondrial dysfunctions, such as reduced COX activity and ATP production, as well as oxidative stress imbalance [92]. More recently, Banerji and colleagues, using a dynamic transcriptomic analysis that combines high-throughput time course imaging and transcriptomics, showed a downregulation of the ERRα/PGC1α pathway in immortalized FSHD human myoblast cell lines. PGC1α, which is critical for mitochondria biogenesis, is directly involved in defense against oxidative stress, upregulating different antioxidant enzymes such as Manganese superoxide dismutase (MnSOD) [93].
Lastly, it is intriguing that inflammation seems to be involved in the development of muscle damage in FSHD with a progression that can be followed using muscle imaging [94,95]. Although its role is not completely understood, in vivo evidence suggests that it constitutes an active process in muscles undergoing early damage [96] and significantly involves cytokines and mediators of the innate immunity arm [97]. The inappropriate expression of cancer testis and other autoantigens has been evoked as a possible trigger of the inflammatory response, but conclusive evidence is currently lacking. The possible interplay between inflammation and oxidative stress in FSHD also needs clarification, as preliminary evidence suggests a redox imbalance in muscles showing signs of early damage. In these muscles, proteomic analysis of the interstitial fluid analyzed by mass spectrometry identified a downregulation of SOD1 and upregulation of GPx3 and CAT [98]. Taken together, these data suggest that targeting specific players in these pathways may serve as a therapeutic approach to reduce oxidative stress in FSHD.
5.2. Myotonic Dystrophy Type 1
Oxidative stress is also a player in the pathophysiology of myotonic dystrophy type 1 (DM1). DM1 is the most common form of muscular dystrophy in the adult and is caused by an expansion of CTG repeats in the 3′-untranslated region of the myotonic dystrophy protein kinase (DMPK) gene [99]. In 1995, Ihara and colleagues proposed a role for oxidative stress in DM1 on the basis of the discovery in patients’ blood of an increased level of free radicals and lipid peroxides, as well as a decrease in antioxidants such as α-tocopherol, coenzyme Q10, selenium, and albumin [100]. Usaki and colleagues, using the C2C12 cell model, demonstrated that the susceptibility to oxidative stress is CTG-repeat number-dependent, suggesting that it could be involved in the pathogenesis of the disease. Furthermore, using the same model, they found that the induction of apoptosis by oxidative stress is related to the activation of the SAPK/JNK pathway and the inhibition of the ERK pathway [101]. DM1 is a multisystemic disorder with an involvement also of the central nervous system. In a mouse model of DM1, the chronic administration of methylphenidate (MPH) was able to reduce the reactive microglia and proinflammatory cytokine IL-1β levels [102]. The treatment increased the NRF2 gene expression in the hippocampus of the DM1 mice by modulating the brain-derived neurotrophic factor (BDNF) levels, which regulates Nrf2 nuclear translocation [103]. These findings support a role for Nrf2 in mediating the reduction of oxidative stress and inflammation in DM1 and address the pharmacological Nrf2 induction as a promising therapy in this disease [104].
Moreover, evidence indicates that mitochondrial dysfunction is involved in the pathophysiology of DM1. In this regard, signs of mitochondrial alteration in muscle biopsy and oxidative stress markers have been detected in different DM1 patient cohorts [105,106]. Lastly, recent studies focused the attention on antioxidant system deregulation showing the downregulation of several proteins such as GPx, Gst, and GSH in DM1 patients [107,108].
5.3. Limb Girdle Muscular Dystrophies
Limb girdle muscular dystrophies (LGMDs) constitute a group of genetic disorders characterized by progressive weakness and wasting of the proximal limb muscles, with onset by definition after the acquisition of autonomous ambulation. Several studies showed the involvement of oxidative stress in calpainopathy (LGMDR1, previously named LGMD2A). LGMDR1 is caused by mutations in the gene encoding calpain-3 (CAPN3), a non-lysosomal calcium-dependent cysteine protease, and Capn3 KO mice show abnormalities in mitochondrial structure, distribution, and function, suggesting that energy production deficits, along with increased oxidative stress, are pathogenic features of LGMDR1 [109]. Moreover, oxidative and nitrosative stress occurring in LGMDR1 activate different pathways such as the NF-κB one that is involved in muscle wasting [110].
Redox imbalance has also been detected in LGMDR1 patients [111], where reductions in antioxidant defense mechanisms (SOD1 and Nrf2), coupled with increased lipid peroxidation and protein ubiquitination, were found. The redox imbalance primarily affected nonmitochondrial compartments, since the enzyme activities of citrate synthase, cytochrome c oxidase, and complex I + III were comparable to controls.
Lastly, a relevant upregulation of oxidative stress and NF-κB signaling has also been identified in dysferlinopathy or LGMDR2. Analyses on human precursor and differentiated cultured muscle cells demonstrated that a reduction in dysferlin induces oxidative stress with the mitochondria as a source of ROS [112].
6. Potential Targets for Therapy
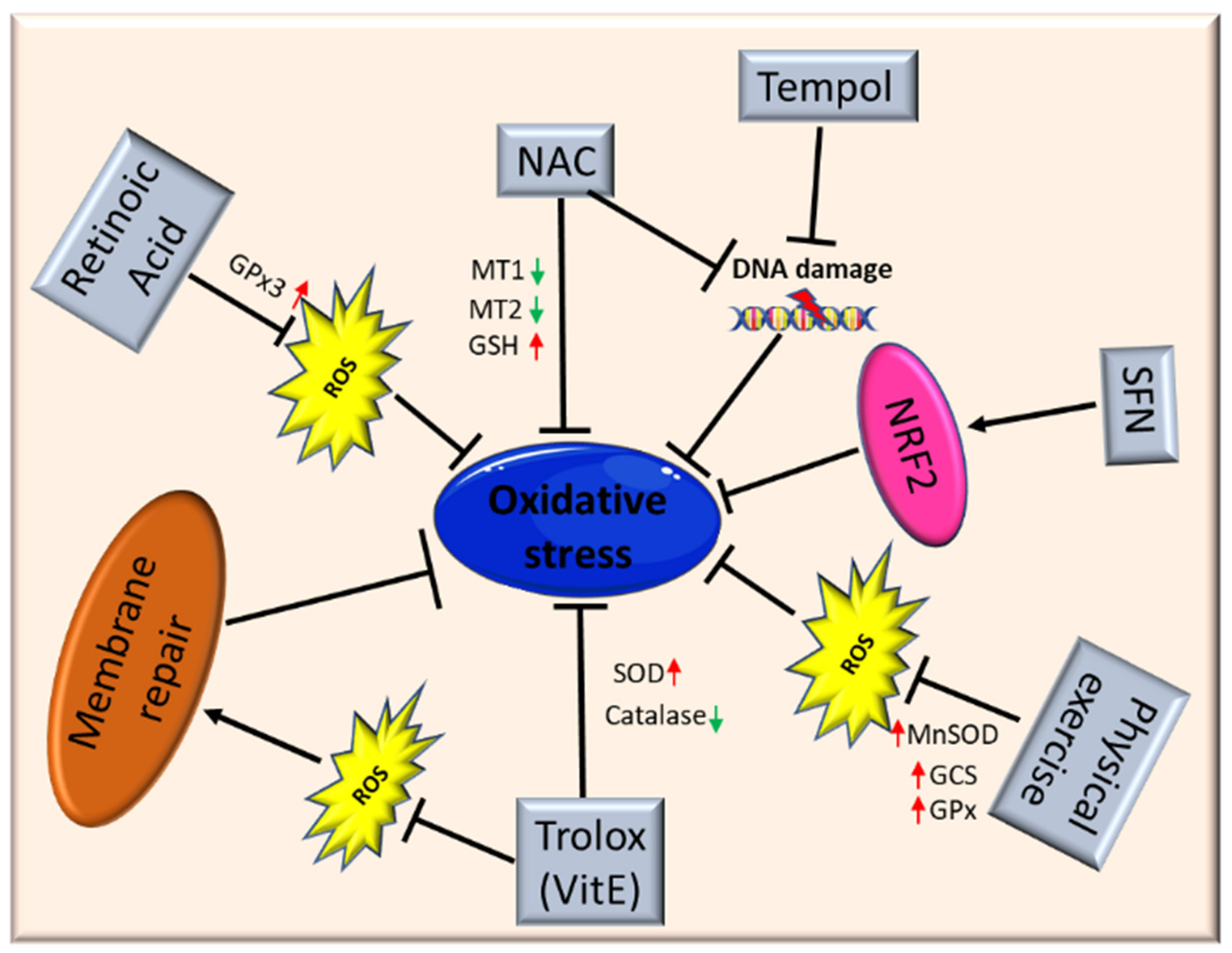
As oxidative stress is involved in muscle homeostasis and functionality, antioxidant treatment may be a potential therapeutic option, alone or as an adjuvant, to treat myopathies and muscular dystrophies. To date, different studies have shown the ability of antioxidants to improve muscle health, reducing ROS levels through the modulation of different genes involved in oxidative stress response (Figure 3).
El Haddad and colleagues reported that treatment with retinoic acid, a metabolite of vitamin A, reduced ROS level in human myoblasts derived from both healthy subjects and FSHD patients and improved cell survival in transplantation assays. Moreover, they underlined the molecular mechanism involved, further demonstrating that retinoic acid is able to induce expression and increase activity of GPx3 [113].
Another study demonstrated that treatment with tempol, a powerful antioxidant, of DUX4-transfected myoblasts, as well as myoblasts derived from FSHD patients, efficiently reduced the level of ROS and DNA breaks.
Similar findings were obtained using NAC [80]. Moreover, deferoxamine (DFX) was able to improve the antioxidant effects of NAC on primary cultures from mdx mice mainly reducing H2O2 production and NF-κB levels [71]. NAC treatment also decreased oxidative stress-responsive genes metallothionein1 and 2 (Mt1 and Mt2), ameliorating myopathic phenotypes in a mouse model of GNE myopathy, one of the most prevalent distal myopathies [114].
Vitamin E is commonly used as an antioxidant to limit oxidative damage and inflammatory disease. Bittel and colleagues reported that treatment with Trolox, a water-soluble analogue of vitamin E, significantly improved membrane repair capacity by reducing mitochondrial ROS levels in FSHD myoblasts [86]. Furthermore, vitamin E is able to significantly increase the level of SOD and decrease the catalase level in mdx mice, suggesting that it may contribute to counteract the deleterious effects of oxidative damage, including lipid peroxidation and free-radical generation [68]. Bosnakovski and colleagues identified 52 compounds that can inhibit DUX4-induced toxicity in FSHD myoblasts. Two-thirds of these compounds have been shown to reduce oxidative stress in FSHD muscle, along with slowing disease processes [79].
Several studies also highlighted the role of physical exercise to counteract oxidative stress in muscle. Increasing evidence suggests that the continued presence of a small stimulus, such as low concentrations of ROS, can induce a compensatory increase of antioxidant defenses. For instance, Gomez-Cabrera and colleagues demonstrated that exhaustive exercise in animals resulted in reduced oxidative damage due to the upregulation of endogenous antioxidant enzymes such as MnSOD, GPx, and γ-glutamylcysteine synthetase (GCS), along with an enhanced NF-κB pathway [115]. Therefore, physical exercise should be considered beneficial in patients with muscular dystrophies.
It is important to underline once again that Nrf2 is the primary regulator of the endogenous antioxidant response, and that Nrf2 induction is a more efficient alternative to the use of a single antioxidant. Indeed, unlike other strategies, targeting Nrf2 activation has the potential to simultaneously modulate separate pathological features and amplify therapeutic benefits in muscular dystrophies [2]. Nrf2 may ensure a durable benefit in chronic disease states via upstream regulation of several antioxidant and anti-inflammatory pathways. Many Nrf2 activators have been identified, some of those are either already in clinical practice or tested in interventional trials (e.g., the fumaric acid esters, oltipraz and ursodiol) [116,117,118]. For instance, the use of the isothiocyanate sulforaphane (SFN), a well-known Nrf2 inducer [119], was able to attenuate muscle inflammation and fibrosis in mdx mice [16]. A recent study further confirmed the importance of targeting Nrf2 to amplify the therapeutic benefits and open the way to new drugs for treating chronic muscle diseases [2].
However, despite the amount of preclinical evidence about the central role of oxidative stress in development of muscle damage in muscular dystrophies, early clinical trials using antioxidants such as nicotinamide (vitamin B) and tocopherols (vitamin E) have so far failed to bring significant clinical benefits [37]. Nevertheless, a double-blind randomized controlled clinical trial with antioxidant supplementation (vitamin C, vitamin E, zinc gluconate, and selenium) in FSHD patients was shown to minimize some adverse effects related to oxidative damage (particularly lipid peroxidation) resulting in an improvement of muscle strength [120]. Furthermore, more recently, Sitzia and colleagues, in a single-center randomized double-blind placebo-controlled study, reported clinical benefit on 29 patients with DMD, FSHD, or LGMD after the supplementation with flavonoids/omega3 (FLAVOMEGA) [121].
7. Conclusions
Evidence coming from the literature suggests that oxidative stress is an important modulator of skeletal muscle homeostasis and functionality. Because of their contractile activity, as well as their high oxygen consumption, and metabolic rate, skeletal muscles continuously produce moderate levels of ROS. Under normal conditions, there is a balance between pro-oxidative and antioxidative factors to allow the proper functioning of metabolic pathways, as well as cellular integrity [6,122,123]. If this balance is disrupted, the accumulation of oxidative agents may lead to cellular dysfunction and death, resulting in chronic tissue degeneration and inflammation [124]. As discussed, oxidative stress is one of the most relevant causes of muscle damage, and it is not surprising that an impairment of redox homeostasis has been evidenced in several muscle disorders.
Since redox homeostasis is drug-targetable, the implementation of pharmacological trials with antioxidants can pave the way for novel promising preclinical studies. Nevertheless, many questions need further investigation, such as the exact mechanism underlying oxidative stress in patients with muscle disorders and the effective benefits of antioxidant supplementation in specific forms of muscular dystrophies.
Author Contributions
Conceptualization: F.P. and G.T.; methodology: N.M., S.P. and M.M.; formal analysis, investigation, and data curation: N.M., S.P., and S.B.; writing—original draft preparation: N.M., S.P.; writing—review and editing: S.B., M.M., F.P., and G.T.; supervision: E.R., F.P. and G.T.; funding acquisition G.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was Funded by Italian Ministry of Health (GR-2018-12366350).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Le Moal, E.; Pialoux, V.; Juban, G.; Groussard, C.; Zouhal, H.; Chazaud, B.; Mounier, R. Redox Control of Skeletal Muscle Regeneration. Antioxid. Redox Signal. 2017, 27, 276–310. [Google Scholar] [CrossRef]
- Kourakis, S.; Timpani, C.A.; de Haan, J.B.; Gueven, N.; Fischer, D.; Rybalka, E. Targeting Nrf2 for the Treatment of Duchenne Muscular Dystrophy. Redox Biol. 2021, 38, 101803. [Google Scholar] [CrossRef]
- Rojo de la Vega, M.; Dodson, M.; Chapman, E.; Zhang, D.D. NRF2-Targeted Therapeutics: New Targets and Modes of NRF2 Regulation. Curr. Opin. Toxicol. 2016, 1, 62–70. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, M.; Kensler, T.W.; Motohashi, H. The KEAP1-NRF2 System: A Thiol-Based Sensor-Effector Apparatus for Maintaining Redox Homeostasis. Physiol. Rev. 2018, 98, 1169–1203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serra, A.J.; Pinto, J.R.; Prokić, M.D.; Arsa, G.; Vasconsuelo, A. Oxidative Stress in Muscle Diseases: Current and Future Therapy. Oxid. Med. Cell. Longev. 2020, 2020, 6030417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbieri, E.; Sestili, P. Reactive Oxygen Species in Skeletal Muscle Signaling. J. Signal Transduct. 2012, 2012, 982794. [Google Scholar] [CrossRef] [Green Version]
- Betteridge, D.J. What Is Oxidative Stress? Metabolism 2000, 49, 3–8. [Google Scholar] [CrossRef]
- Vesely, M.J.; Exon, D.J.; Clark, J.E.; Foresti, R.; Green, C.J.; Motterlini, R. Heme Oxygenase-1 Induction in Skeletal Muscle Cells: Hemin and Sodium Nitroprusside Are Regulators in Vitro. Am. J. Physiol. 1998, 275, C1087–C1094. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Criswell, D.; Lawler, J.; Ji, L.L.; Martin, D.; Herb, R.A.; Dudley, G. Influence of Exercise and Fiber Type on Antioxidant Enzyme Activity in Rat Skeletal Muscle. Am. J. Physiol. 1994, 266, R375–R380. [Google Scholar] [CrossRef]
- Holtzclaw, W.D.; Dinkova-Kostova, A.T.; Talalay, P. Protection against Electrophile and Oxidative Stress by Induction of Phase 2 Genes: The Quest for the Elusive Sensor That Responds to Inducers. Adv. Enzyme Regul. 2004, 44, 335–367. [Google Scholar] [CrossRef]
- Suzuki, T.; Yamamoto, M. Molecular Basis of the Keap1-Nrf2 System. Free Radic. Biol. Med. 2015, 88, 93–100. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, T.; Yamamoto, M. Stress-Sensing Mechanisms and the Physiological Roles of the Keap1-Nrf2 System during Cellular Stress. J. Biol. Chem. 2017, 292, 16817–16824. [Google Scholar] [CrossRef] [Green Version]
- Whitehead, N.P.; Yeung, E.W.; Froehner, S.C.; Allen, D.G. Skeletal Muscle NADPH Oxidase Is Increased and Triggers Stretch-Induced Damage in the Mdx Mouse. PLoS ONE 2010, 5, e15354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, I.A.; Allen, D.G. The Role of Reactive Oxygen Species in the Hearts of Dystrophin-Deficient Mdx Mice. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H1969–H1977. [Google Scholar] [CrossRef] [Green Version]
- Kovac, S.; Angelova, P.R.; Holmström, K.M.; Zhang, Y.; Dinkova-Kostova, A.T.; Abramov, A.Y. Nrf2 Regulates ROS Production by Mitochondria and NADPH Oxidase. Biochim. Biophys. Acta 2015, 1850, 794–801. [Google Scholar] [CrossRef] [Green Version]
- Sun, C.-C.; Li, S.-J.; Yang, C.-L.; Xue, R.-L.; Xi, Y.-Y.; Wang, L.; Zhao, Q.-L.; Li, D.-J. Sulforaphane Attenuates Muscle Inflammation in Dystrophin-Deficient Mdx Mice via NF-E2-Related Factor 2 (Nrf2)-Mediated Inhibition of NF-ΚB Signaling Pathway. J. Biol. Chem. 2015, 290, 17784–17795. [Google Scholar] [CrossRef] [Green Version]
- Zhang, M.; Xu, Y.; Qiu, Z.; Jiang, L. Sulforaphane Attenuates Angiotensin II-Induced Vascular Smooth Muscle Cell Migration via Suppression of NOX4/ROS/Nrf2 Signaling. Int. J. Biol. Sci. 2019, 15, 148–157. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, S.; Karin, M. Missing Pieces in the NF-ΚB Puzzle. Cell 2002, 109, S81–S96. [Google Scholar] [CrossRef] [Green Version]
- Jiang, B.; Xu, S.; Hou, X.; Pimentel, D.R.; Brecher, P.; Cohen, R.A. Temporal Control of NF-ΚB Activation by ERK Differentially Regulates Interleukin-1β-Induced Gene Expression. J. Biol. Chem. 2004, 279, 1323–1329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Engelhardt, J.F. Interleukin-1β Induction of NFκB Is Partially Regulated by H2O2-Mediated Activation of NFκB-Inducing Kinase. J. Biol. Chem. 2006, 281, 1495–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luo, G.; Hershko, D.D.; Robb, B.W.; Wray, C.J.; Hasselgren, P.-O. IL-1β Stimulates IL-6 Production in Cultured Skeletal Muscle Cells through Activation of MAP Kinase Signaling Pathway and NF-ΚB. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2003, 284, R1249–R1254. [Google Scholar] [CrossRef]
- Aoi, W.; Naito, Y.; Takanami, Y.; Kawai, Y.; Sakuma, K.; Ichikawa, H.; Yoshida, N.; Yoshikawa, T. Oxidative Stress and Delayed-Onset Muscle Damage after Exercise. Free Radic. Biol. Med. 2004, 37, 480–487. [Google Scholar] [CrossRef]
- Hanai, J.; Cao, P.; Tanksale, P.; Imamura, S.; Koshimizu, E.; Zhao, J.; Kishi, S.; Yamashita, M.; Phillips, P.S.; Sukhatme, V.P.; et al. The Muscle-Specific Ubiquitin Ligase Atrogin-1/MAFbx Mediates Statin-Induced Muscle Toxicity. J. Clin. Investig. 2007, 117, 3940–3951. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, N.; Slocum, S.L.; Skoko, J.J.; Shin, S.; Kensler, T.W. When NRF2 Talks, Who’s Listening? Antioxid. Redox Signal. 2010, 13, 1649–1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, S.M.U.; Luo, L.; Namani, A.; Wang, X.J.; Tang, X. Nrf2 Signaling Pathway: Pivotal Roles in Inflammation. Biochim. Biophys. Acta BBA Mol. Basis Dis. 2017, 1863, 585–597. [Google Scholar] [CrossRef] [PubMed]
- Seldon, M.P.; Silva, G.; Pejanovic, N.; Larsen, R.; Gregoire, I.P.; Filipe, J.; Anrather, J.; Soares, M.P. Heme Oxygenase-1 Inhibits the Expression of Adhesion Molecules Associated with Endothelial Cell Activation via Inhibition of NF-ΚB RelA Phosphorylation at Serine. J. Immunol. 2007, 179, 7840–7851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.-H.; Chou, P.-C.; Chung, F.-T.; Lin, H.-C.; Huang, K.-H.; Kuo, H.-P. Heat Shock Protein70 Is Implicated in Modulating NF-ΚB Activation in Alveolar Macrophages of Patients with Active Pulmonary Tuberculosis. Sci. Rep. 2017, 7, 1214. [Google Scholar] [CrossRef]
- Pietraszek-Gremplewicz, K.; Kozakowska, M.; Bronisz-Budzynska, I.; Ciesla, M.; Mucha, O.; Podkalicka, P.; Madej, M.; Glowniak, U.; Szade, K.; Stępniewski, J.; et al. Heme Oxygenase-1 Influences Satellite Cells and Progression of Duchenne Muscular Dystrophy in Mice. Antioxid. Redox Signal. 2018, 29, 128–148. [Google Scholar] [CrossRef]
- Chan, M.C.; Ziegler, O.; Liu, L.; Rowe, G.C.; Das, S.; Otterbein, L.E.; Arany, Z. Heme Oxygenase and Carbon Monoxide Protect from Muscle Dystrophy. Skelet. Muscle 2016, 6, 41. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, E.H.; Suzuki, T.; Funayama, R.; Nagashima, T.; Hayashi, M.; Sekine, H.; Tanaka, N.; Moriguchi, T.; Motohashi, H.; Nakayama, K.; et al. Nrf2 Suppresses Macrophage Inflammatory Response by Blocking Proinflammatory Cytokine Transcription. Nat. Commun. 2016, 7, 11624. [Google Scholar] [CrossRef]
- Gilbreath, H.R.; Castro, D.; Iannaccone, S.T. Congenital Myopathies and Muscular Dystrophies. Neurol. Clin. 2014, 32, 689–703. [Google Scholar] [CrossRef]
- Shieh, P.B. Muscular Dystrophies and Other Genetic Myopathies. Neurol. Clin. 2013, 31, 1009–1029. [Google Scholar] [CrossRef]
- Bönnemann, C.G.; Wang, C.H.; Quijano-Roy, S.; Deconinck, N.; Bertini, E.; Ferreiro, A.; Muntoni, F.; Sewry, C.; Béroud, C.; Mathews, K.D.; et al. Diagnostic Approach to the Congenital Muscular Dystrophies. Neuromuscul. Disord. NMD 2014, 24, 289–311. [Google Scholar] [CrossRef] [PubMed]
- Canton, M.; Menazza, S.; Di Lisa, F. Oxidative Stress in Muscular Dystrophy: From Generic Evidence to Specific Sources and Targets. J. Muscle Res. Cell Motil. 2014, 35, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Terrill, J.R.; Radley-Crabb, H.G.; Iwasaki, T.; Lemckert, F.A.; Arthur, P.G.; Grounds, M.D. Oxidative Stress and Pathology in Muscular Dystrophies: Focus on Protein Thiol Oxidation and Dysferlinopathies. FEBS J. 2013, 280, 4149–4164. [Google Scholar] [CrossRef] [PubMed]
- Kozakowska, M.; Pietraszek-Gremplewicz, K.; Jozkowicz, A.; Dulak, J. The Role of Oxidative Stress in Skeletal Muscle Injury and Regeneration: Focus on Antioxidant Enzymes. J. Muscle Res. Cell Motil. 2015, 36, 377–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, M.H.; Ow, J.R.; Yang, N.-D.; Taneja, R. Oxidative Stress-Mediated Skeletal Muscle Degeneration: Molecules, Mechanisms, and Therapies. Oxid. Med. Cell. Longev. 2016, 2016, 6842568. [Google Scholar] [CrossRef] [Green Version]
- Michelucci, A.; De Marco, A.; Guarnier, F.A.; Protasi, F.; Boncompagni, S. Antioxidant Treatment Reduces Formation of Structural Cores and Improves Muscle Function in RYR1Y522S/WT Mice. Oxid. Med. Cell. Longev. 2017, 2017, 6792694. [Google Scholar] [CrossRef] [Green Version]
- Arbogast, S.; Ferreiro, A. Selenoproteins and Protection against Oxidative Stress: Selenoprotein N as a Novel Player at the Crossroads of Redox Signaling and Calcium Homeostasis. Antioxid. Redox Signal. 2010, 12, 893–904. [Google Scholar] [CrossRef]
- Grounds, M.D.; Terrill, J.R.; Al-Mshhdani, B.A.; Duong, M.N.; Radley-Crabb, H.G.; Arthur, P.G. Biomarkers for Duchenne Muscular Dystrophy: Myonecrosis, Inflammation and Oxidative Stress. Dis. Model. Mech. 2020, 13. [Google Scholar] [CrossRef]
- Can, B.; Kara, O.; Kizilarslanoglu, M.C.; Arik, G.; Aycicek, G.S.; Sumer, F.; Civelek, R.; Demirtas, C.; Ulger, Z. Serum Markers of Inflammation and Oxidative Stress in Sarcopenia. Aging Clin. Exp. Res. 2017, 29, 745–752. [Google Scholar] [CrossRef]
- Morrison, L. Unraveling RYR1 Mutations and Muscle Biopsies. Neurology 2008, 70, 99–100. [Google Scholar] [CrossRef]
- Snoeck, M.; van Engelen, B.G.M.; Küsters, B.; Lammens, M.; Meijer, R.; Molenaar, J.P.F.; Raaphorst, J.; Verschuuren-Bemelmans, C.C.; Straathof, C.S.M.; Sie, L.T.L.; et al. RYR1-Related Myopathies: A Wide Spectrum of Phenotypes throughout Life. Eur. J. Neurol. 2015, 22, 1094–1112. [Google Scholar] [CrossRef]
- Lopez, R.J.; Byrne, S.; Vukcevic, M.; Sekulic-Jablanovic, M.; Xu, L.; Brink, M.; Alamelu, J.; Voermans, N.; Snoeck, M.; Clement, E.; et al. An RYR1 Mutation Associated with Malignant Hyperthermia Is Also Associated with Bleeding Abnormalities. Sci. Signal. 2016, 9, ra68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treves, S.; Jungbluth, H.; Muntoni, F.; Zorzato, F. Congenital Muscle Disorders with Cores: The Ryanodine Receptor Calcium Channel Paradigm. Curr. Opin. Pharmacol. 2008, 8, 319–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meissner, G. The Structural Basis of Ryanodine Receptor Ion Channel Function. J. Gen. Physiol. 2017, 149, 1065–1089. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, S.L.; Reid, M.B. RyR1 Modulation by Oxidation and Calmodulin. Antioxid. Redox Signal. 2000, 2, 41–45. [Google Scholar] [CrossRef]
- Aracena-Parks, P.; Goonasekera, S.A.; Gilman, C.P.; Dirksen, R.T.; Hidalgo, C.; Hamilton, S.L. Identification of Cysteines Involved in S-Nitrosylation, S-Glutathionylation, and Oxidation to Disulfides in Ryanodine Receptor Type. J. Biol. Chem. 2006, 281, 40354–40368. [Google Scholar] [CrossRef] [Green Version]
- Andersson, D.C.; Betzenhauser, M.J.; Reiken, S.; Meli, A.C.; Umanskaya, A.; Xie, W.; Shiomi, T.; Zalk, R.; Lacampagne, A.; Marks, A.R. Ryanodine Receptor Oxidation Causes Intracellular Calcium Leak and Muscle Weakness in Aging. Cell Metab. 2011, 14, 196–207. [Google Scholar] [CrossRef] [Green Version]
- Durham, W.J.; Aracena-Parks, P.; Long, C.; Rossi, A.E.; Goonasekera, S.A.; Boncompagni, S.; Galvan, D.L.; Gilman, C.P.; Baker, M.R.; Shirokova, N.; et al. RyR1 S-Nitrosylation Underlies Environmental Heat Stroke and Sudden Death in Y522S RyR1 Knockin Mice. Cell 2008, 133, 53–65. [Google Scholar] [CrossRef] [Green Version]
- Todd, J.J.; Lawal, T.A.; Witherspoon, J.W.; Chrismer, I.C.; Razaqyar, M.S.; Punjabi, M.; Elliott, J.S.; Tounkara, F.; Kuo, A.; Shelton, M.O.; et al. Randomized Controlled Trial of N-Acetylcysteine Therapy for RYR1-Related Myopathies. Neurology 2020, 94, e1434–e1444. [Google Scholar] [CrossRef] [Green Version]
- Dowling, J.J.; Arbogast, S.; Hur, J.; Nelson, D.D.; McEvoy, A.; Waugh, T.; Marty, I.; Lunardi, J.; Brooks, S.V.; Kuwada, J.Y.; et al. Oxidative Stress and Successful Antioxidant Treatment in Models of RYR1-Related Myopathy. Brain J. Neurol. 2012, 135, 1115–1127. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.S.; Hanna, A.D.; Wang, H.; Dagnino-Acosta, A.; Joshi, A.D.; Knoblauch, M.; Xia, Y.; Georgiou, D.K.; Xu, J.; Long, C.; et al. A Chemical Chaperone Improves Muscle Function in Mice with a RyR1 Mutation. Nat. Commun. 2017, 8, 14659. [Google Scholar] [CrossRef] [Green Version]
- Flanigan, K.M.; Kerr, L.; Bromberg, M.B.; Leonard, C.; Tsuruda, J.; Zhang, P.; Gonzalez-Gomez, I.; Cohn, R.; Campbell, K.P.; Leppert, M. Congenital Muscular Dystrophy with Rigid Spine Syndrome: A Clinical, Pathological, Radiological, and Genetic Study. Ann. Neurol. 2000, 47, 152–161. [Google Scholar] [CrossRef]
- Rederstorff, M.; Castets, P.; Arbogast, S.; Lainé, J.; Vassilopoulos, S.; Beuvin, M.; Dubourg, O.; Vignaud, A.; Ferry, A.; Krol, A.; et al. Increased Muscle Stress-Sensitivity Induced by Selenoprotein N Inactivation in Mouse: A Mammalian Model for SEPN1-Related Myopathy. PLoS ONE 2011, 6, e23094. [Google Scholar] [CrossRef] [PubMed]
- Arbogast, S.; Beuvin, M.; Fraysse, B.; Zhou, H.; Muntoni, F.; Ferreiro, A. Oxidative Stress in SEPN1-Related Myopathy: From Pathophysiology to Treatment. Ann. Neurol. 2009, 65, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Bushby, K.; Finkel, R.; Birnkrant, D.J.; Case, L.E.; Clemens, P.R.; Cripe, L.; Kaul, A.; Kinnett, K.; McDonald, C.; Pandya, S.; et al. Diagnosis and Management of Duchenne Muscular Dystrophy, Part 1: Diagnosis, and Pharmacological and Psychosocial Management. Lancet Neurol. 2010, 9, 77–93. [Google Scholar] [CrossRef]
- Matsumura, K.; Campbell, K.P. Dystrophin-Glycoprotein Complex: Its Role in the Molecular Pathogenesis of Muscular Dystrophies. Muscle Nerve 1994, 17, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Serra, F.; Quarta, M.; Canato, M.; Toniolo, L.; De Arcangelis, V.; Trotta, A.; Spath, L.; Monaco, L.; Reggiani, C.; Naro, F. Inflammation in Muscular Dystrophy and the Beneficial Effects of Non-Steroidal Anti-Inflammatory Drugs. Muscle Nerve 2012, 46, 773–784. [Google Scholar] [CrossRef]
- Prosser, B.L.; Ward, C.W.; Lederer, W.J. X-ROS Signaling: Rapid Mechano-Chemo Transduction in Heart. Science 2011, 333, 1440–1445. [Google Scholar] [CrossRef] [Green Version]
- Rando, T.A.; Disatnik, M.H.; Yu, Y.; Franco, A. Muscle Cells from Mdx Mice Have an Increased Susceptibility to Oxidative Stress. Neuromuscul. Disord. NMD 1998, 8, 14–21. [Google Scholar] [CrossRef]
- Niebrój-Dobosz, I.; Hausmanowa-Petrusewicz, I. The Involvement of Oxidative Stress in Determining the Severity and Progress of Pathological Processes in Dystrophin-Deficient Muscles. Acta Biochim. Pol. 2005, 52, 449–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaczor, J.J.; Hall, J.E.; Payne, E.; Tarnopolsky, M.A. Low Intensity Training Decreases Markers of Oxidative Stress in Skeletal Muscle of Mdx Mice. Free Radic. Biol. Med. 2007, 43, 145–154. [Google Scholar] [CrossRef]
- Kim, J.-H.; Kwak, H.-B.; Thompson, L.V.; Lawler, J.M. Contribution of Oxidative Stress to Pathology in Diaphragm and Limb Muscles with Duchenne Muscular Dystrophy. J. Muscle Res. Cell Motil. 2013, 34, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Pal, R.; Palmieri, M.; Loehr, J.A.; Li, S.; Abo-Zahrah, R.; Monroe, T.O.; Thakur, P.B.; Sardiello, M.; Rodney, G.G. Src-Dependent Impairment of Autophagy by Oxidative Stress in a Mouse Model of Duchenne Muscular Dystrophy. Nat. Commun. 2014, 5, 4425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrillo, S.; Pelosi, L.; Piemonte, F.; Travaglini, L.; Forcina, L.; Catteruccia, M.; Petrini, S.; Verardo, M.; D’Amico, A.; Musarò, A.; et al. Oxidative Stress in Duchenne Muscular Dystrophy: Focus on the NRF2 Redox Pathway. Hum. Mol. Genet. 2017, 26, 2781–2790. [Google Scholar] [CrossRef] [PubMed]
- Almeida-Becerril, T.; Rodríguez-Cruz, M.; Raúl Sánchez-González, J.; Antonio Villaldama-Soriano, M.; Atilano-Miguel, S.; Villa-Morales, J.; Cárdenas-Conejo, A.; Cárdenas-Vázquez, R. Circulating Markers of Oxidative Stress Are Associated with a Muscle Injury in Patients with Muscular Dystrophy Duchenne. Brain Dev. 2021, 43, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Mâncio, R.D.; Hermes, T.d.A.; Macedo, A.B.; Mizobuti, D.S.; Valduga, A.H.; Rupcic, I.F.; Minatel, E. Vitamin E Treatment Decreases Muscle Injury in Mdx Mice. Nutrition 2017, 43–44, 39–46. [Google Scholar] [CrossRef]
- Mizobuti, D.S.; Fogaça, A.R.; Moraes, F.D.S.R.; Moraes, L.H.R.; Mâncio, R.D.; Hermes, T.d.A.; Macedo, A.B.; Valduga, A.H.; de Lourenço, C.C.; Pereira, E.C.L.; et al. Coenzyme Q10 Supplementation Acts as Antioxidant on Dystrophic Muscle Cells. Cell Stress Chaperones 2019, 24, 1175–1185. [Google Scholar] [CrossRef] [PubMed]
- Burns, D.P.; Drummond, S.E.; Bolger, D.; Coiscaud, A.; Murphy, K.H.; Edge, D.; O’Halloran, K.D. N-Acetylcysteine Decreases Fibrosis and Increases Force-Generating Capacity of Mdx Diaphragm. Antioxidants 2019, 8, 581. [Google Scholar] [CrossRef] [Green Version]
- Moraes, L.H.R.; Bollineli, R.C.; Mizobuti, D.S.; Silveira, L.D.R.; Marques, M.J.; Minatel, E. Effect of N-Acetylcysteine plus Deferoxamine on Oxidative Stress and Inflammation in Dystrophic Muscle Cells. Redox Rep. Commun. Free Radic. Res. 2015, 20, 109–115. [Google Scholar] [CrossRef]
- Pinniger, G.J.; Terrill, J.R.; Assan, E.B.; Grounds, M.D.; Arthur, P.G. Pre-Clinical Evaluation of N-Acetylcysteine Reveals Side Effects in the Mdx Mouse Model of Duchenne Muscular Dystrophy. J. Physiol. 2017, 595, 7093–7107. [Google Scholar] [CrossRef] [PubMed]
- Gamberi, T.; Fiaschi, T.; Valocchia, E.; Modesti, A.; Mantuano, P.; Rolland, J.-F.; Sanarica, F.; De Luca, A.; Magherini, F. Proteome Analysis in Dystrophic Mdx Mouse Muscle Reveals a Drastic Alteration of Key Metabolic and Contractile Proteins after Chronic Exercise and the Potential Modulation by Anti-Oxidant Compounds. J. Proteomics 2018, 170, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Wijmenga, C.; Padberg, G.W.; Moerer, P.; Wiegant, J.; Liem, L.; Brouwer, O.F.; Milner, E.C.; Weber, J.L.; van Ommen, G.B.; Sandkuyl, L.A. Mapping of Facioscapulohumeral Muscular Dystrophy Gene to Chromosome 4q35-Qter by Multipoint Linkage Analysis and in Situ Hybridization. Genomics 1991, 9, 570–575. [Google Scholar] [CrossRef]
- Van Deutekom, J.C.; Wijmenga, C.; van Tienhoven, E.A.; Gruter, A.M.; Hewitt, J.E.; Padberg, G.W.; van Ommen, G.J.; Hofker, M.H.; Frants, R.R. FSHD Associated DNA Rearrangements Are Due to Deletions of Integral Copies of a 3.2 Kb Tandemly Repeated Unit. Hum. Mol. Genet. 1993, 2, 2037–2042. [Google Scholar] [CrossRef]
- Lemmers, R.J.L.F.; van der Vliet, P.J.; Klooster, R.; Sacconi, S.; Camaño, P.; Dauwerse, J.G.; Snider, L.; Straasheijm, K.R.; van Ommen, G.J.; Padberg, G.W.; et al. A Unifying Genetic Model for Facioscapulohumeral Muscular Dystrophy. Science 2010, 329, 1650–1653. [Google Scholar] [CrossRef] [Green Version]
- Hamel, J.; Tawil, R. Facioscapulohumeral Muscular Dystrophy: Update on Pathogenesis and Future Treatments. Neurother. J. Am. Soc. Exp. Neurother. 2018, 15, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Bosnakovski, D.; Xu, Z.; Ji Gang, E.; Galindo, C.L.; Liu, M.; Simsek, T.; Garner, H.R.; Agha-Mohammadi, S.; Tassin, A.; Coppée, F.; et al. An Isogenetic Myoblast Expression Screen Identifies DUX4-Mediated FSHD-Associated Molecular Pathologies. EMBO J. 2008, 27, 2766–2779. [Google Scholar] [CrossRef] [Green Version]
- Bosnakovski, D.; Choi, S.; Strasser, J.M.; Toso, E.A.; Walters, M.A.; Kyba, M. High-Throughput Screening Identifies Inhibitors of DUX4-Induced Myoblast Toxicity. Skelet. Muscle 2014, 4, 4. [Google Scholar] [CrossRef] [Green Version]
- Dmitriev, P.; Bou Saada, Y.; Dib, C.; Ansseau, E.; Barat, A.; Hamade, A.; Dessen, P.; Robert, T.; Lazar, V.; Louzada, R.A.N.; et al. DUX4-Induced Constitutive DNA Damage and Oxidative Stress Contribute to Aberrant Differentiation of Myoblasts from FSHD Patients. Free Radic. Biol. Med. 2016, 99, 244–258. [Google Scholar] [CrossRef]
- Bou Saada, Y.; Dib, C.; Dmitriev, P.; Hamade, A.; Carnac, G.; Laoudj-Chenivesse, D.; Lipinski, M.; Vassetzky, Y.S. Facioscapulohumeral Dystrophy Myoblasts Efficiently Repair Moderate Levels of Oxidative DNA Damage. Histochem. Cell Biol. 2016, 145, 475–483. [Google Scholar] [CrossRef]
- Sasaki-Honda, M.; Jonouchi, T.; Arai, M.; Hotta, A.; Mitsuhashi, S.; Nishino, I.; Matsuda, R.; Sakurai, H. A Patient-Derived IPSC Model Revealed Oxidative Stress Increases Facioscapulohumeral Muscular Dystrophy-Causative DUX. Hum. Mol. Genet. 2018, 27, 4024–4035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerji, C.R.S.; Knopp, P.; Moyle, L.A.; Severini, S.; Orrell, R.W.; Teschendorff, A.E.; Zammit, P.S. β– Catenin Is Central to DUX4 -Driven Network Rewiring in Facioscapulohumeral Muscular Dystrophy. J. R. Soc. Interface 2015, 12, 20140797. [Google Scholar] [CrossRef] [Green Version]
- Movafagh, S.; Crook, S.; Vo, K. Regulation of Hypoxia-Inducible Factor-1a by Reactive Oxygen Species: New Developments in an Old Debate: Regulation of Hypoxia-Inducible Factor-1a. J. Cell. Biochem. 2015, 116, 696–703. [Google Scholar] [CrossRef]
- Sharma, V.; Harafuji, N.; Belayew, A.; Chen, Y.-W. DUX4 Differentially Regulates Transcriptomes of Human Rhabdomyosarcoma and Mouse C2C12 Cells. PLoS ONE 2013, 8, e64691. [Google Scholar] [CrossRef] [Green Version]
- Bittel, A.J.; Sreetama, S.C.; Bittel, D.C.; Horn, A.; Novak, J.S.; Yokota, T.; Zhang, A.; Maruyama, R.; Rowel, Q.; Lim, K.; et al. Membrane Repair Deficit in Facioscapulohumeral Muscular Dystrophy. Int. J. Mol. Sci. 2020, 21, 5575. [Google Scholar] [CrossRef]
- Winokur, S.T.; Barrett, K.; Martin, J.H.; Forrester, J.R.; Simon, M.; Tawil, R.; Chung, S.-A.; Masny, P.S.; Figlewicz, D.A. Facioscapulohumeral Muscular Dystrophy (FSHD) Myoblasts Demonstrate Increased Susceptibility to Oxidative Stress. Neuromuscul. Disord. 2003, 13, 322–333. [Google Scholar] [CrossRef]
- Gabellini, D.; Green, M.R.; Tupler, R. Inappropriate Gene Activation in FSHD: A Repressor Complex Binds a Chromosomal Repeat Deleted in Dystrophic Muscle. Cell 2002, 110, 339–348. [Google Scholar] [CrossRef] [Green Version]
- Laoudj-Chenivesse, D.; Carnac, G.; Bisbal, C.; Hugon, G.; Bouillot, S.; Desnuelle, C.; Vassetzky, Y.; Fernandez, A. Increased Levels of Adenine Nucleotide Translocator 1 Protein and Response to Oxidative Stress Are Early Events in Facioscapulohumeral Muscular Dystrophy Muscle. J. Mol. Med. 2005, 83, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Masny, P.S.; Chan, O.Y.A.; de Greef, J.C.; Bengtsson, U.; Ehrlich, M.; Tawil, R.; Lock, L.F.; Hewitt, J.E.; Stocksdale, J.; Martin, J.H.; et al. Analysis of Allele-Specific RNA Transcription in FSHD by RNA-DNA FISH in Single Myonuclei. Eur. J. Hum. Genet. 2010, 18, 448–456. [Google Scholar] [CrossRef] [Green Version]
- Macaione, V.; Aguennouz, M.; Rodolico, C.; Mazzeo, A.; Patti, A.; Cannistraci, E.; Colantone, L.; Di Giorgio, R.M.; De Luca, G.; Vita, G. RAGE-NF-?B Pathway Activation in Response to Oxidative Stress in Facioscapulohumeral Muscular Dystrophy. Acta Neurol. Scand. 2007, 115, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Turki, A.; Hayot, M.; Carnac, G.; Pillard, F.; Passerieux, E.; Bommart, S.; de Mauverger, E.R.; Hugon, G.; Pincemail, J.; Pietri, S.; et al. Functional Muscle Impairment in Facioscapulohumeral Muscular Dystrophy Is Correlated with Oxidative Stress and Mitochondrial Dysfunction. Free Radic. Biol. Med. 2012, 53, 1068–1079. [Google Scholar] [CrossRef]
- Banerji, C.R.S.; Panamarova, M.; Pruller, J.; Figeac, N.; Hebaishi, H.; Fidanis, E.; Saxena, A.; Contet, J.; Sacconi, S.; Severini, S.; et al. Dynamic Transcriptomic Analysis Reveals Suppression of PGC1α/ERRα Drives Perturbed Myogenesis in Facioscapulohumeral Muscular Dystrophy. Hum. Mol. Genet. 2019, 28, 1244–1259. [Google Scholar] [CrossRef] [PubMed]
- Frisullo, G.; Frusciante, R.; Nociti, V.; Tasca, G.; Renna, R.; Iorio, R.; Patanella, A.K.; Iannaccone, E.; Marti, A.; Rossi, M.; et al. CD8(+) T Cells in Facioscapulohumeral Muscular Dystrophy Patients with Inflammatory Features at Muscle MRI. J. Clin. Immunol. 2011, 31, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Monforte, M.; Laschena, F.; Ottaviani, P.; Bagnato, M.R.; Pichiecchio, A.; Tasca, G.; Ricci, E. Tracking Muscle Wasting and Disease Activity in Facioscapulohumeral Muscular Dystrophy by Qualitative Longitudinal Imaging. J. Cachexia Sarcopenia Muscle 2019, 10, 1258–1265. [Google Scholar] [CrossRef] [PubMed]
- Tasca, G.; Monforte, M.; Iannaccone, E.; Laschena, F.; Ottaviani, P.; Leoncini, E.; Boccia, S.; Galluzzi, G.; Pelliccioni, M.; Masciullo, M.; et al. Upper Girdle Imaging in Facioscapulohumeral Muscular Dystrophy. PLoS ONE 2014, 9, e100292. [Google Scholar] [CrossRef] [Green Version]
- Tasca, G.; Monforte, M.; Corbi, M.; Granata, G.; Lucchetti, D.; Sgambato, A.; Ricci, E. Muscle Microdialysis to Investigate Inflammatory Biomarkers in Facioscapulohumeral Muscular Dystrophy. Mol. Neurobiol. 2018, 55, 2959–2966. [Google Scholar] [CrossRef]
- Corasolla Carregari, V.; Monforte, M.; Di Maio, G.; Pieroni, L.; Urbani, A.; Ricci, E.; Tasca, G. Proteomics of Muscle Microdialysates Identifies Potential Circulating Biomarkers in Facioscapulohumeral Muscular Dystrophy. Int. J. Mol. Sci. 2020, 22, 290. [Google Scholar] [CrossRef] [PubMed]
- Udd, B.; Krahe, R. The Myotonic Dystrophies: Molecular, Clinical, and Therapeutic Challenges. Lancet Neurol. 2012, 11, 891–905. [Google Scholar] [CrossRef]
- Ihara, Y.; Mori, A.; Hayabara, T.; Namba, R.; Nobukuni, K.; Sato, K.; Miyata, S.; Edamatsu, R.; Liu, J.; Kawai, M. Free Radicals, Lipid Peroxides and Antioxidants in Blood of Patients with Myotonic Dystrophy. J. Neurol. 1995, 242, 119–122. [Google Scholar] [CrossRef]
- Usuki, F.; Takahashi, N.; Sasagawa, N.; Ishiura, S. Differential Signaling Pathways Following Oxidative Stress in Mutant Myotonin Protein Kinase CDNA-Transfected C2C12 Cell Lines. Biochem. Biophys. Res. Commun. 2000, 267, 739–743. [Google Scholar] [CrossRef]
- Ramon-Duaso, C.; Gener, T.; Consegal, M.; Fernández-Avilés, C.; Gallego, J.J.; Castarlenas, L.; Swanson, M.S.; de la Torre, R.; Maldonado, R.; Puig, M.V.; et al. Methylphenidate Attenuates the Cognitive and Mood Alterations Observed in Mbnl2 Knockout Mice and Reduces Microglia Overexpression. Cereb. Cortex 2019, 29, 2978–2997. [Google Scholar] [CrossRef] [PubMed]
- Bruna, B.; Lobos, P.; Herrera-Molina, R.; Hidalgo, C.; Paula-Lima, A.; Adasme, T. The Signaling Pathways Underlying BDNF-Induced Nrf2 Hippocampal Nuclear Translocation Involve ROS, RyR-Mediated Ca2+ Signals, ERK and PI3K. Biochem. Biophys. Res. Commun. 2018, 505, 201–207. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, P.; Petrillo, S.; Bertini, E.S.; Piemonte, F. Oxidative Stress in DNA Repeat Expansion Disorders: A Focus on NRF2 Signaling Involvement. Biomolecules 2020, 10, 702. [Google Scholar] [CrossRef] [PubMed]
- Toscano, A.; Messina, S.; Campo, G.M.; Leo, R.D.; Rodolico, C.; Aguennouz, M.; Annesi, G.; Vita, G. Oxidative Stress in Myotonic Dystrophy Type 1. Free Radic. Res. 2005, 39, 771–776. [Google Scholar] [CrossRef]
- Gramegna, L.L.; Giannoccaro, M.P.; Manners, D.N.; Testa, C.; Zanigni, S.; Evangelisti, S.; Bianchini, C.; Oppi, F.; Poda, R.; Avoni, P.; et al. Mitochondrial Dysfunction in Myotonic Dystrophy Type. Neuromuscul. Disord. 2018, 28, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Kumar, V.; Singh, S.K.; Muthuswamy, S.; Agarwal, S. Imbalanced Oxidant and Antioxidant Ratio in Myotonic Dystrophy Type. Free Radic. Res. 2014, 48, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Koc, F.; Atli, G.; Menziletoglu, S.Y.; Kose, S. Antioxidant Imbalance in the Erythrocytes of Myotonic Dystrophy Type 1 Patients. Arch. Biochem. Biophys. 2020, 680, 108230. [Google Scholar] [CrossRef]
- Kramerova, I.; Kudryashova, E.; Wu, B.; Germain, S.; Vandenborne, K.; Romain, N.; Haller, R.G.; Verity, M.A.; Spencer, M.J. Mitochondrial Abnormalities, Energy Deficit and Oxidative Stress Are Features of Calpain 3 Deficiency in Skeletal Muscle. Hum. Mol. Genet. 2009, 18, 3194–3205. [Google Scholar] [CrossRef] [Green Version]
- Rajakumar, D.; Alexander, M.; Oommen, A. Oxidative Stress, NF-ΚB and the Ubiquitin Proteasomal Pathway in the Pathology of Calpainopathy. Neurochem. Res. 2013, 38, 2009–2018. [Google Scholar] [CrossRef]
- Nilsson, M.I.; Macneil, L.G.; Kitaoka, Y.; Alqarni, F.; Suri, R.; Akhtar, M.; Haikalis, M.E.; Dhaliwal, P.; Saeed, M.; Tarnopolsky, M.A. Redox State and Mitochondrial Respiratory Chain Function in Skeletal Muscle of LGMD2A Patients. PLoS ONE 2014, 9, e102549. [Google Scholar] [CrossRef]
- Rajakumar, D.; Senguttuvan, S.; Alexander, M.; Oommen, A. Involvement of Oxidative Stress, Nuclear Factor Kappa B and the Ubiquitin Proteasomal Pathway in Dysferlinopathy. Life Sci. 2014, 8, 54–61. [Google Scholar] [CrossRef] [PubMed]
- El Haddad, M.; Jean, E.; Turki, A.; Hugon, G.; Vernus, B.; Bonnieu, A.; Passerieux, E.; Hamade, A.; Mercier, J.; Laoudj-Chenivesse, D.; et al. Glutathione Peroxidase 3, a New Retinoid Target Gene, Is Crucial for Human Skeletal Muscle Precursor Cell Survival. J. Cell Sci. 2012, 125, 6147–6156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, A.; Christine, M.; Malicdan, V.; Miyakawa, M.; Nonaka, I.; Nishino, I.; Noguchi, S. Sialic Acid Deficiency Is Associated with Oxidative Stress Leading to Muscle Atrophy and Weakness in GNE Myopathy. Hum. Mol. Genet. 2017, 26, 3081–3093. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Cabrera, M.-C.; Domenech, E.; Viña, J. Moderate Exercise Is an Antioxidant: Upregulation of Antioxidant Genes by Training. Free Radic. Biol. Med. 2008, 44, 126–131. [Google Scholar] [CrossRef]
- Scuderi, S.A.; Ardizzone, A.; Paterniti, I.; Esposito, E.; Campolo, M. Antioxidant and Anti-Inflammatory Effect of Nrf2 Inducer Dimethyl Fumarate in Neurodegenerative Diseases. Antioxidants 2020, 9, 630. [Google Scholar] [CrossRef]
- Michaličková, D.; Hrnčíř, T.; Canová, N.K.; Slanař, O. Targeting Keap1/Nrf2/ARE Signaling Pathway in Multiple Sclerosis. Eur. J. Pharmacol. 2020, 873, 172973. [Google Scholar] [CrossRef]
- Robledinos-Antón, N.; Fernández-Ginés, R.; Manda, G.; Cuadrado, A. Activators and Inhibitors of NRF2: A Review of Their Potential for Clinical Development. Oxid. Med. Cell. Longev. 2019, 2019, 9372182. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, C.; Chio, I.I.C.; Tuveson, D.A. Transcriptional Regulation by Nrf. Antioxid. Redox Signal. 2018, 29, 1727–1745. [Google Scholar] [CrossRef] [Green Version]
- Passerieux, E.; Hayot, M.; Jaussent, A.; Carnac, G.; Gouzi, F.; Pillard, F.; Picot, M.-C.; Böcker, K.; Hugon, G.; Pincemail, J.; et al. Effects of Vitamin C, Vitamin E, Zinc Gluconate, and Selenomethionine Supplementation on Muscle Function and Oxidative Stress Biomarkers in Patients with Facioscapulohumeral Dystrophy: A Double-Blind Randomized Controlled Clinical Trial. Free Radic. Biol. Med. 2015, 81, 158–169. [Google Scholar] [CrossRef]
- Sitzia, C.; Meregalli, M.; Belicchi, M.; Farini, A.; Arosio, M.; Bestetti, D.; Villa, C.; Valenti, L.; Brambilla, P.; Torrente, Y. Preliminary Evidences of Safety and Efficacy of Flavonoids- and Omega 3-Based Compound for Muscular Dystrophies Treatment: A Randomized Double-Blind Placebo Controlled Pilot Clinical Trial. Front. Neurol. 2019, 10, 755. [Google Scholar] [CrossRef] [Green Version]
- Davies, K.J. Oxidative Stress, Antioxidant Defenses, and Damage Removal, Repair, and Replacement Systems. IUBMB Life 2000, 50, 279–289. [Google Scholar] [CrossRef] [PubMed]
- Musarò, A.; Fulle, S.; Fanò, G. Oxidative Stress and Muscle Homeostasis. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Mensch, A.; Zierz, S. Cellular Stress in the Pathogenesis of Muscular Disorders—From Cause to Consequence. Int. J. Mol. Sci. 2020, 21, 5830. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Central role of Nrf2 in protecting muscle from oxidative stress and inflammation. Abbreviations: XO: xanthine oxidase; NOS: nitric oxide synthase; NOX: nicotinamide adenine dinucleotide phosphate oxidases, ROS: reactive oxygen species; Nrf2: nuclear factor erythroid 2-related factor 2; Keap1: Kelch-like ECH-associated protein 1; NF-κB: nuclear factor kappa-light-chain-enhancer of activated B cells; TNF-α: tumor necrosis factor alpha, IL-6: interleukin-6, IL-1β: interleukin-1β; SOD: superoxide dismutase; CAT: catalase; GPx: glutathione peroxidase; PRDX: peroxiredoxin; GCL: glutamate cysteine ligase; GST: glutathione S-transferase; NQO1: nicotinamide adenine dinucleotide phosphate quinone oxidoreductase 1; HO1: heme oxygenase-1.
Figure 1.
Central role of Nrf2 in protecting muscle from oxidative stress and inflammation. Abbreviations: XO: xanthine oxidase; NOS: nitric oxide synthase; NOX: nicotinamide adenine dinucleotide phosphate oxidases, ROS: reactive oxygen species; Nrf2: nuclear factor erythroid 2-related factor 2; Keap1: Kelch-like ECH-associated protein 1; NF-κB: nuclear factor kappa-light-chain-enhancer of activated B cells; TNF-α: tumor necrosis factor alpha, IL-6: interleukin-6, IL-1β: interleukin-1β; SOD: superoxide dismutase; CAT: catalase; GPx: glutathione peroxidase; PRDX: peroxiredoxin; GCL: glutamate cysteine ligase; GST: glutathione S-transferase; NQO1: nicotinamide adenine dinucleotide phosphate quinone oxidoreductase 1; HO1: heme oxygenase-1.

Figure 2.
Interplay between DUX4 and oxidative stress in FSHD. This schematic highlights the role of DUX4 in oxidative stress induction during FSHD development and progression. Abbreviations: DUX4: double homeobox 4; Nrf2: nuclear factor erythroid 2-related factor 2; ROS: reactive oxygen species; PI3K: phosphatidylinositol 3-kinase; ATK: protein kinase B; ERK: mitogen-activated protein kinase, TNF-α: tumor necrosis factor alpha; JNK: c-Jun N-terminal kinase; HIF-1: hypoxia-inducible factor 1.
Figure 2.
Interplay between DUX4 and oxidative stress in FSHD. This schematic highlights the role of DUX4 in oxidative stress induction during FSHD development and progression. Abbreviations: DUX4: double homeobox 4; Nrf2: nuclear factor erythroid 2-related factor 2; ROS: reactive oxygen species; PI3K: phosphatidylinositol 3-kinase; ATK: protein kinase B; ERK: mitogen-activated protein kinase, TNF-α: tumor necrosis factor alpha; JNK: c-Jun N-terminal kinase; HIF-1: hypoxia-inducible factor 1.

Figure 3.
Schematic illustration of antioxidant therapy targets in muscular dystrophies. Abbreviations: ROS: reactive oxygen species; NAC: N-acetylcysteine; MT1: metallothionein 1; MT2: metallothionein 2; GSH: glutathione; SFN: isothiocyanate sulforaphane; Nrf2: nuclear factor erythroid 2-related factor 2; MnSOD: manganese superoxide dismutase; GCS: γ-glutamylcysteine synthetase; GPx: glutathione peroxidase; SOD: superoxide dismutase.
Figure 3.
Schematic illustration of antioxidant therapy targets in muscular dystrophies. Abbreviations: ROS: reactive oxygen species; NAC: N-acetylcysteine; MT1: metallothionein 1; MT2: metallothionein 2; GSH: glutathione; SFN: isothiocyanate sulforaphane; Nrf2: nuclear factor erythroid 2-related factor 2; MnSOD: manganese superoxide dismutase; GCS: γ-glutamylcysteine synthetase; GPx: glutathione peroxidase; SOD: superoxide dismutase.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Mosca, N.; Petrillo, S.; Bortolani, S.; Monforte, M.; Ricci, E.; Piemonte, F.; Tasca, G. Redox Homeostasis in Muscular Dystrophies. Cells 2021, 10, 1364. https://doi.org/10.3390/cells10061364
AMA Style
Mosca N, Petrillo S, Bortolani S, Monforte M, Ricci E, Piemonte F, Tasca G. Redox Homeostasis in Muscular Dystrophies. Cells. 2021; 10(6):1364. https://doi.org/10.3390/cells10061364
Chicago/Turabian StyleMosca, Nicola, Sara Petrillo, Sara Bortolani, Mauro Monforte, Enzo Ricci, Fiorella Piemonte, and Giorgio Tasca. 2021. "Redox Homeostasis in Muscular Dystrophies" Cells 10, no. 6: 1364. https://doi.org/10.3390/cells10061364
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.