
Impact of Targeted Agents on Survival of Chronic Lymphocytic Leukemia Patients Fit for Fludarabine, Cyclophosphamide, and Rituximab (FCR) Relative to Age- and Sex-Matched Population

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
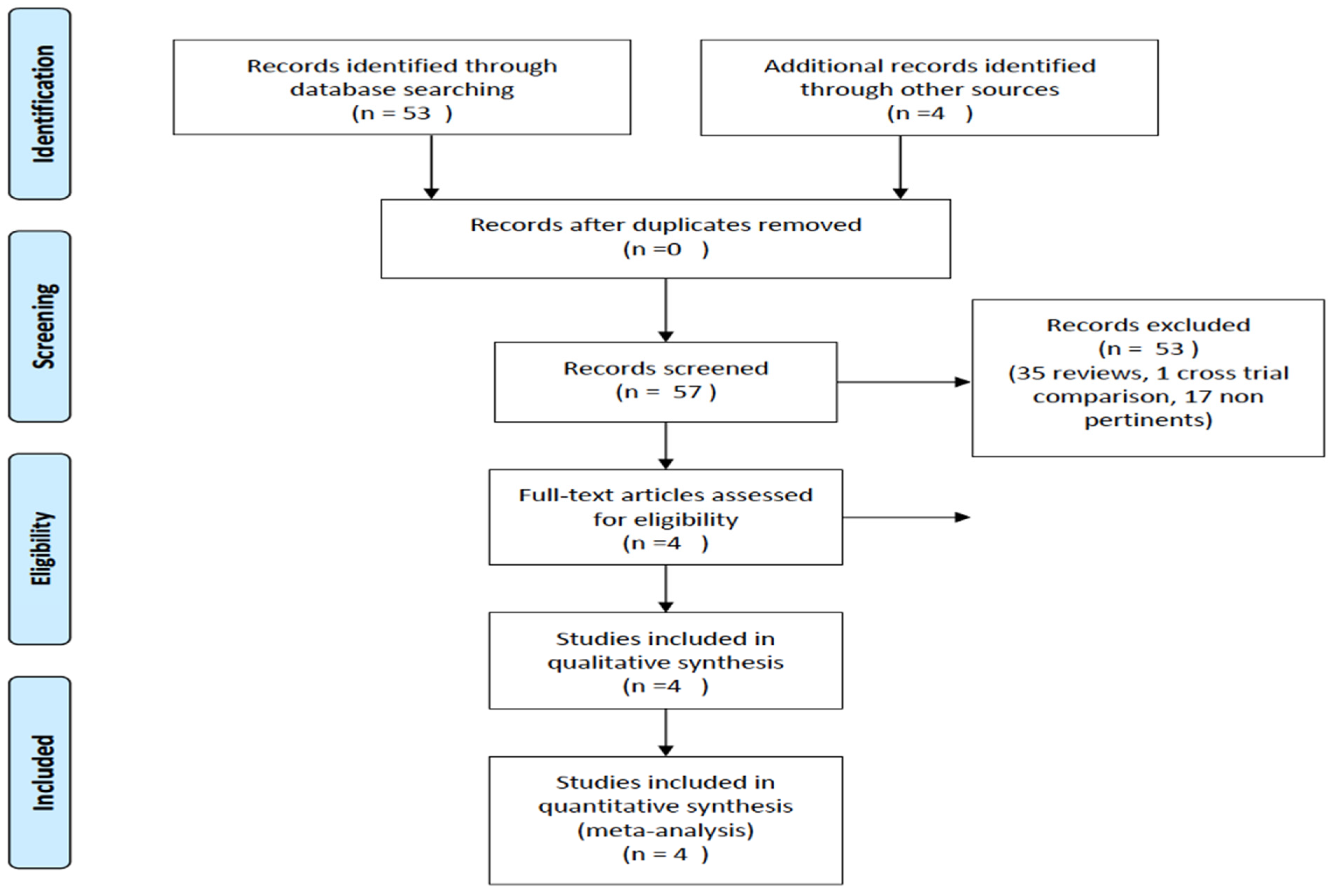
2.1. Search Strategies, Studies’ Eligibility, and Data Extraction
2.2. Statistical Analyses
3. Results
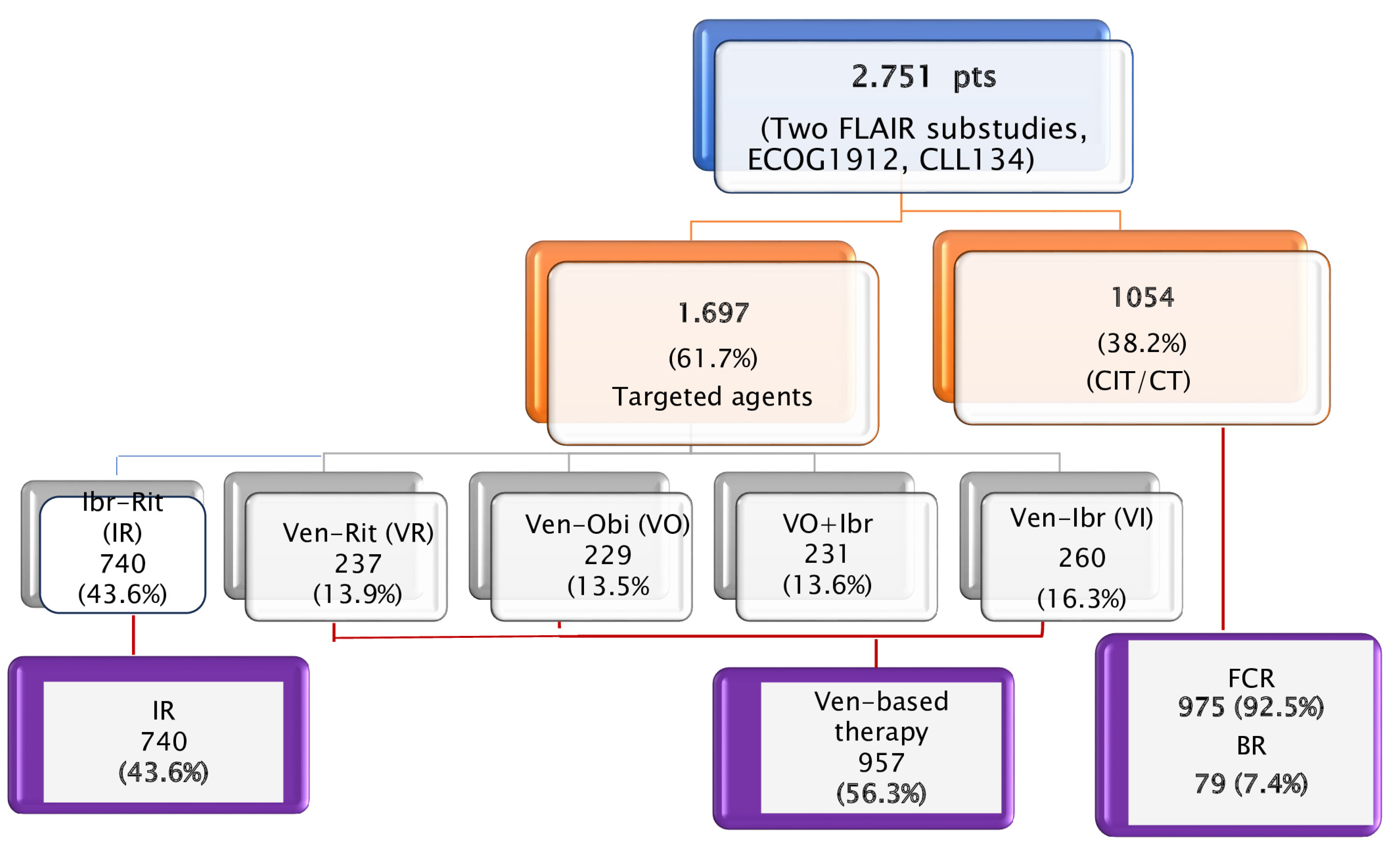
3.1. Studies Selected and Patient Characteristics
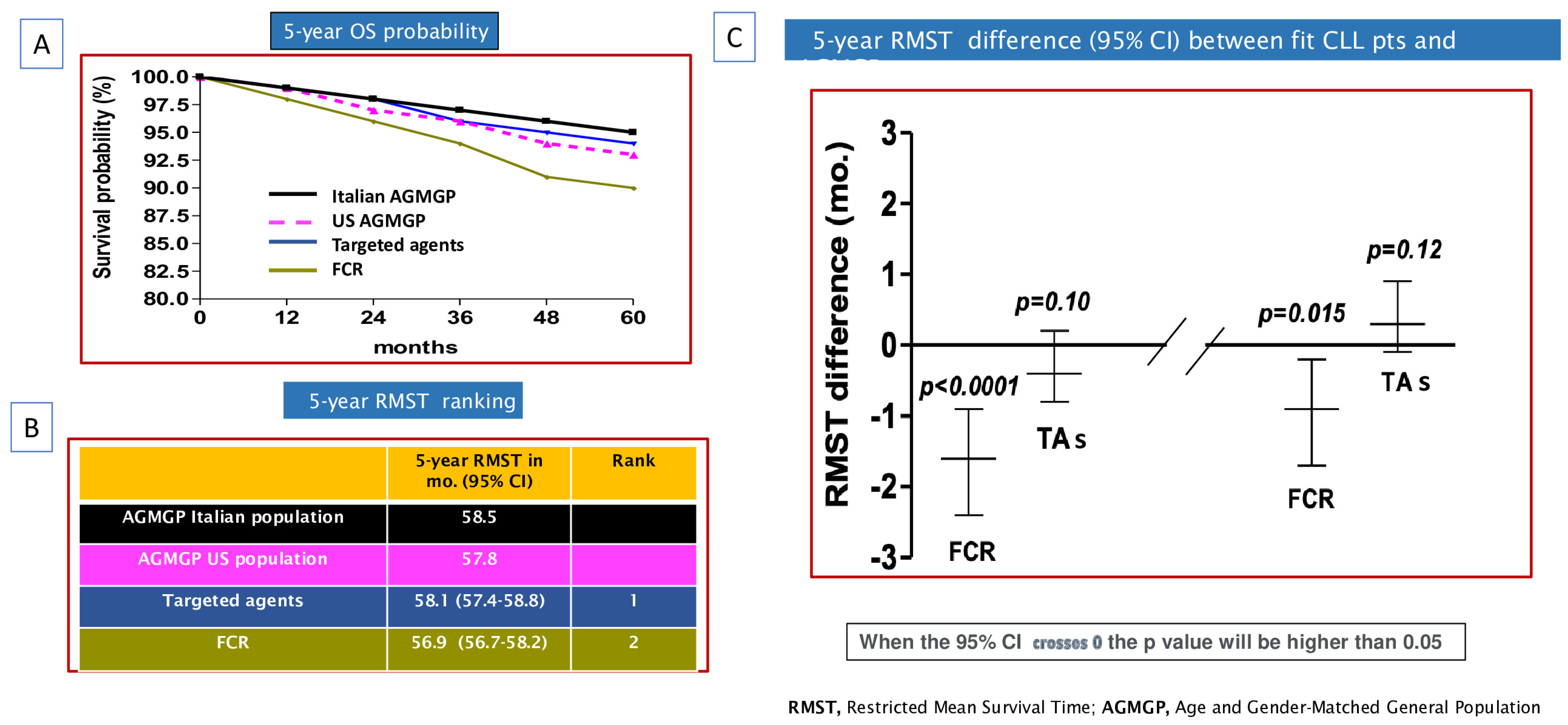
3.2. OS of CLL Patients Treated with TAs or FCR Compared to AGMGP
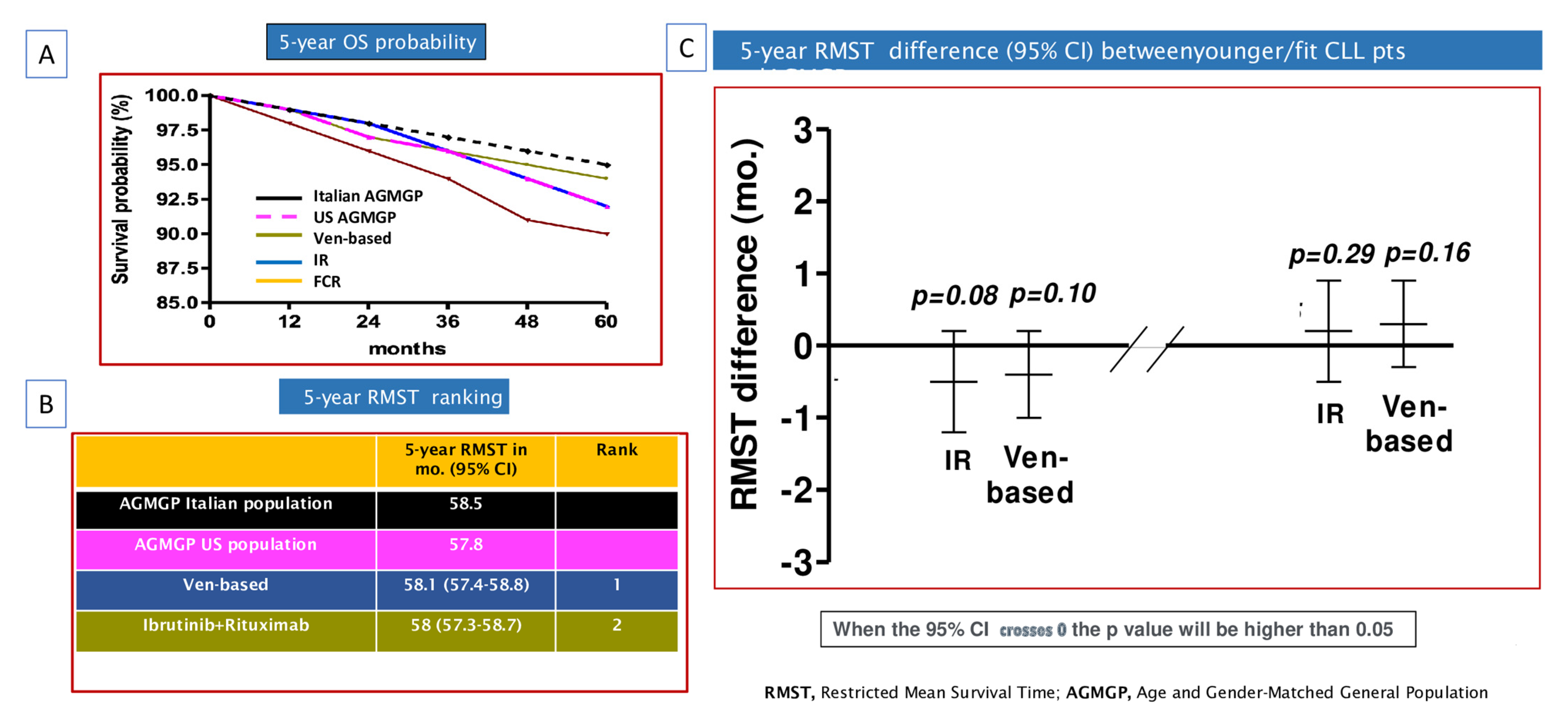
3.3. OS of Patients Treated with Different TAs Compared to the AGMGP
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Bennett, R.; Anderson, M.A.; Seymour, J.F. Unresolved questions in selection of therapies for treatment-naïve chronic lymphocytic leukemia. J. Hematol. Oncol. 2023, 16, 72. [Google Scholar] [CrossRef] [PubMed]
- Ghia, P.; Owen, C.; Barrientos, J.C.; Barr, P.M.; Mato, A.R.; Shi, C.; Szoke, A.; Abbazio, C.; Krigsfeld, G.K.; Burger, J.A. Initiating first-line (1L) Ibrutinib (Ibr) in patients with chronic lymphocytic leukemia (CLL) improves overall survival (OS) outcomes to rates approximating an age-matched population of ≥65 years. Blood 2022, 140 (Suppl. S1), 4159–4161. [Google Scholar] [CrossRef]
- Molica, S.; Shanafelt, T.; Allsup, D.; Giannarelli, D. Impact of Targeted Agents on Survival of CLL Patients Age > 65 Relative to Age and Sex Matched Population. Am. J. Hematol. 2023, 99, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Wang, X.V.; Kay, N.E.; Hanson, C.A.; O’Brien, S.; Barrientos, J.; Jelinek, D.F.; Braggio, E.; Leis, J.F.; Zhang, C.C.; et al. Ibrutinib-Rituximab or Chemoimmunotherapy for Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2019, 381, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Wang, X.V.; Hanson, C.A.; Paietta, E.M.; O’Brien, S.; Barrientos, J.; Jelinek, D.F.; Braggio, E.; Leis, J.F.; Zhang, C.C.; et al. Long-term outcomes for ibrutinib-rituximab and chemoimmunotherapy in CLL: Updated results of the E1912 trial. Blood 2022, 140, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Eichhorst, B.; Niemann, C.U.; Kater, A.P.; Fürstenau, M.; von Tresckow, J.; Zhang, C.; Robrecht, S.; Gregor, M.; Juliusson, G.; Thornton, P.; et al. First-Line Venetoclax Combinations in Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2023, 388, 1739–1754. [Google Scholar] [CrossRef] [PubMed]
- Hillmen, P.; Pitchford, A.; Bloor, A.; Broom, A.; Young, M.; Kennedy, B.; Walewska, R.; Furtado, M.; Preston, G.; Neilson, J.R.; et al. Ibrutinib and rituximab versus fludarabine, cyclophosphamide, and rituximab for patients with previously untreated chronic lymphocytic leukaemia (FLAIR): Interim analysis of a multicentre, open-label, randomized, phase 3 trial. Lancet Oncol. 2023, 24, 535–552. [Google Scholar] [CrossRef] [PubMed]
- Munir, T.; Cairns, D.A.; Bloor, A.; Allsup, D.; Cwynarski, K.; Pettitt, A.; Paneesha, S.; Fox, C.P.; Eyre, T.A.; Forconi, F.; et al. Chronic Lymphocytic Leukemia Therapy Guided by Measurable Residual Disease. N. Engl. J. Med. 2024, 390, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Royston, P.; Parmar, M.K. Restricted mean survival time: An alternative to the hazard ratio for the design and analysis of randomized trials with a time-to-event outcome. BMC Med. Res. Methodol. 2013, 13, 152. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Zhou, Y.; Lee, J.J. IPD from KM: Reconstruct individual patient data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2021, 21, 111. [Google Scholar] [CrossRef] [PubMed]
- Syn, N.L.; Cummings, D.E.; Wang, L.Z.; Lin, D.J.; Zhao, J.J.; Loh, M.; Koh, Z.J.; Chew, C.A.; Loo, Y.E.; Tai, B.C.; et al. Association of metabolic-bariatric surgery with long-term survival in adults with and without diabetes: A one-stage meta-analysis of matched cohort and prospective controlled studies with 174,772 participants. Lancet 2021, 397, 1830–1841. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Shao, F.; Chen, K.; Wang, Y.; Wu, Z.; Wang, Y.; Gao, Y.; Cornelius, V.; Li, C.; Jiang, Z. Time to Clinical Benefit of Intensive Blood Pressure Lowering in Patients 60 Years and Older with Hypertension: A Secondary Analysis of Randomized Clinical Trials. JAMA Intern. Med. 2022, 182, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.istat.it/en/archivio/226922 (accessed on 21 January 2024).
- Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr70/nvsr70-19.pdf (accessed on 21 January 2024).
- Molica, S. Redefining efficacy and safety endpoints for chronic lymphocytic leukemia in the era of targeted therapy. Expert Rev. Hematol. 2023, 16, 803–806. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Uno, H.; Wei, L.J. Restricted Mean Survival Time as a Measure to Interpret Clinical Trial Results. JAMA Cardiol. 2017, 2, 1179–1180. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; Brown, J.R.; Kahl, B.S.; Ghia, P.; Giannopoulos, K.; Jurczak, W.; Šimkovič, M.; Shadman, M.; Österborg, A.; Laurenti, L.; et al. Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and small lymphocytic lymphoma (SEQUOIA): A andomized, controlled, phase 3 trial. Lancet Oncol. 2022, 23, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, A.; Ferrant, E.; Flinn, I.W.; Tam, C.S.; Ghia, P.; Robak, T.; Brown, J.R.; Ramakrishnan, V.; Tian, T.; Kuwahara, S.B.; et al. Zanubrutinib in Combination with Venetoclax for Patients with Treatment-Naïve (TN) Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Lymphoma (SLL) with del(17p): Early Results from Arm D of the SEQUOIA (BGB-3111-304) Trial. In Proceedings of the American Society of Hematology Annual Meeting, Atlanta, GA, USA, 11–14 December 2021. [Google Scholar]
- Soumerai, J.D.; Mato, A.R.; Dogan, A.; Seshan, V.E.; Joffe, E.; Flaherty, K.; Hochberg, E.; Barnes, J.A.; Hamilton, A.M.; Abramson, J.S.; et al. Zanubrutinib, obinutuzumab, and venetoclax with minimal residual disease-driven discontinuation in previously untreated patients with chronic lymphocytic leukaemia or small lymphocytic lymphoma: A multicentre, single-arm, phase 2 trial. Lancet Haematol. 2021, 8, e879–e890. [Google Scholar] [CrossRef] [PubMed]
- Davids, M.S.; Lampson, B.L.; Tyekucheva, S.; Wang, Z.; Lowney, J.C.; Pazienza, S.; Montegaard, J.; Patterson, V.; Weinstock, M.; Crombie, J.L.; et al. Acalabrutinib, venetoclax, and binutuzumab as frontline treatment for chronic lymphocytic leukaemia: A single-arm, open-label, phase 2 study. Lancet Oncol. 2021, 22, 1391–1402. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Study | Recruiting from | Inclusion Criteria | Experimental Arm | Control Arm | Randomization Ratio | |
|---|---|---|---|---|---|---|
| 1° FLAIR sub-study [7] | RCT | UK Institutions | Pts. fit for FCR | IR | FCR | 1:1 |
| 2° FLAIR sub-study [8] | RCT | UK Institutions | Pts. fit for FCR | IR or I | FCR | 1:1:1 |
| ECOG1912 [4,5] | RCT | ECOG Centers | Pts. fit for FCR | IR | FCR | 2:1 |
| CLL13 [6] | RCT | GCLLSG/HOVON centers | CIRS score < 6/Cr Cl > 70 | VR/VO/VOI | FCR * | 1:1:1:1 |
| Study | Experimental Arm | No Pts. in Experimental Arm | Pts Median Age in Years, (Range) | Male | Median Follow-Up (Mo) | Pts. with U-IGHV | Pts. with 11q (Del) | Pts with TP53 Aberrations |
|---|---|---|---|---|---|---|---|---|
| First FLAIR sub-study [7] | Ibrutinib + Rituximab | 386 | 63 (55–67) | 73.0% | 53.0 | 50.0% | 15% | <1% |
| CLL13 [6] | VR VO VO + Ibrutinib | 237 229 231 | 62 (27–84) 62 (31–83) 60 (30–84) | 73.8% 74.7% 68.4% | 38.8 | 56.5% 57.0% 53.2% | 19.0% 19.2% 13.9% | NR |
| ECOG1912 [4,5] | Ibrutinib + Rituximab | 354 | 56.7 (±7.5) * | 62.0% | 69.7 | 75.0% | 22.0 % | <1% |
| Second FLAIR sub-study [8] | Ibrutinib +Venetoclax | 260 | 62 (56–67) | 71.3% | 43.7 | 49.9% | 18.2% | <1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molica, S.; Shanafelt, T.D.; Allsup, D.; Giannarelli, D. Impact of Targeted Agents on Survival of Chronic Lymphocytic Leukemia Patients Fit for Fludarabine, Cyclophosphamide, and Rituximab (FCR) Relative to Age- and Sex-Matched Population. Cancers 2024, 16, 1085. https://doi.org/10.3390/cancers16061085
Molica S, Shanafelt TD, Allsup D, Giannarelli D. Impact of Targeted Agents on Survival of Chronic Lymphocytic Leukemia Patients Fit for Fludarabine, Cyclophosphamide, and Rituximab (FCR) Relative to Age- and Sex-Matched Population. Cancers. 2024; 16(6):1085. https://doi.org/10.3390/cancers16061085
Chicago/Turabian StyleMolica, Stefano, Tait D. Shanafelt, David Allsup, and Diana Giannarelli. 2024. "Impact of Targeted Agents on Survival of Chronic Lymphocytic Leukemia Patients Fit for Fludarabine, Cyclophosphamide, and Rituximab (FCR) Relative to Age- and Sex-Matched Population" Cancers 16, no. 6: 1085. https://doi.org/10.3390/cancers16061085