
Lifestyle Factors and Breast Cancer in Females with PTEN Hamartoma Tumor Syndrome (PHTS)

 , , , , , , , , , , , , and add
Show full author list
, , , , , , , , , , , , and add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Clinical, Genetic and Lifestyle Risk Factor Definitions
2.3. Statistical Analyses
3. Results
3.1. Patient Population
3.2. Physical Activity
3.3. Alcohol Consumption
3.4. Tobacco Smoking
3.5. Body Mass Index
3.6. Multiple Lifestyle Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations (Alphabetical Order)
| BMI | Body mass index |
| OR | Odds ratio |
| PHTS | PTEN Hamartoma Tumor Syndrome |
| SD | Standard deviation |
References
- Hendricks, L.A.J.; Hoogerbrugge, N.; Schuurs-Hoeijmakers, J.H.M.; Vos, J.R. A review on age-related cancer risks in PTEN hamartoma tumor syndrome. Clin. Genet. 2021, 99, 219–225. [Google Scholar] [CrossRef]
- Nelen, M.R.; Kremer, H.; Konings, I.B.; Schoute, F.; van Essen, A.J.; Koch, R.; Woods, C.G.; Fryns, J.P.; Hamel, B.; Hoefsloot, L.H.; et al. Novel PTEN mutations in patients with Cowden disease: Absence of clear genotype-phenotype correlations. Eur. J. Hum. Genet. 1999, 7, 267–273. [Google Scholar] [CrossRef]
- Hendricks, L.A.J.; Hoogerbrugge, N.; Mensenkamp, A.R.; Brunet, J.; Lleuger-Pujol, R.; Høberg-Vetti, H.; Haavind, M.T.; Innella, G.; Turchetti, D.; Aretz, S.; et al. Cancer risks by sex and variant type in PTEN Hamartoma Tumor Syndrome. J. Natl. Cancer Inst. 2023, 115, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Wiseman, M.; Cannon, G.; Butrum, R.; Martin, G.; Higginbotham, S.; Heggie, S.; Jones, C.; Fletcher, M. Food, Nutrition, Physical Activity and the Prevention of Cancer: A Global Perspective. Summary; World Cancer Research Fund/Amaerican Institute for Cancer Research: London, UK, 2007. [Google Scholar]
- Thomson, C.A.; McCullough, M.L.; Wertheim, B.C.; Chlebowski, R.T.; Martinez, M.E.; Stefanick, M.L.; Rohan, T.E.; Manson, J.E.; Tindle, H.A.; Ockene, J.; et al. Nutrition and physical activity cancer prevention guidelines, cancer risk, and mortality in the women’s health initiative. Cancer Prev. Res. 2014, 7, 42–53. [Google Scholar] [CrossRef]
- La Vecchia, C.; Giordano, S.H.; Hortobagyi, G.N.; Chabner, B. Overweight, obesity, diabetes, and risk of breast cancer: Interlocking pieces of the puzzle. Oncologist 2011, 16, 726–729. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.E.; Schoemaker, M.J.; Wright, L.B.; Ashworth, A.; Swerdlow, A.J. Smoking and risk of breast cancer in the Generations Study cohort. Breast Cancer Res. 2017, 19, 118. [Google Scholar] [CrossRef]
- Macacu, A.; Autier, P.; Boniol, M.; Boyle, P. Active and passive smoking and risk of breast cancer: A meta-analysis. Breast Cancer Res. Treat. 2015, 154, 213–224. [Google Scholar] [CrossRef]
- McDonald, J.A.; Goyal, A.; Terry, M.B. Alcohol Intake and Breast Cancer Risk: Weighing the Overall Evidence. Curr. Breast Cancer Rep. 2013, 5, 208–221. [Google Scholar] [CrossRef]
- Lofterød, T.; Frydenberg, H.; Flote, V.; Eggen, A.E.; McTiernan, A.; Mortensen, E.S.; Akslen, L.A.; Reitan, J.B.; Wilsgaard, T.; Thune, I. Exploring the effects of lifestyle on breast cancer risk, age at diagnosis, and survival: The EBBA-Life study. Breast Cancer Res. Treat. 2020, 182, 215–227. [Google Scholar] [CrossRef] [PubMed]
- Hardefeldt, P.J.; Penninkilampi, R.; Edirimanne, S.; Eslick, G.D. Physical Activity and Weight Loss Reduce the Risk of Breast Cancer: A Meta-analysis of 139 Prospective and Retrospective Studies. Clin. Breast Cancer 2018, 18, e601–e612. [Google Scholar] [CrossRef]
- Chlebowski, R.T. Nutrition and physical activity influence on breast cancer incidence and outcome. Breast 2013, 22 (Suppl. S2), S30–S37. [Google Scholar] [CrossRef] [PubMed]
- Pijpe, A.; Manders, P.; Brohet, R.M.; Collée, J.M.; Verhoef, S.; Vasen, H.F.; Hoogerbrugge, N.; van Asperen, C.J.; Dommering, C.; Ausems, M.G.; et al. Physical activity and the risk of breast cancer in BRCA1/2 mutation carriers. Breast Cancer Res. Treat. 2010, 120, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Manders, P.; Pijpe, A.; Hooning, M.J.; Kluijt, I.; Vasen, H.F.; Hoogerbrugge, N.; van Asperen, C.J.; Meijers-Heijboer, H.; Ausems, M.G.; van Os, T.A.; et al. Body weight and risk of breast cancer in BRCA1/2 mutation carriers. Breast Cancer Res. Treat. 2011, 126, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Terry, M.B.; Antoniou, A.C.; Phillips, K.A.; Kast, K.; Mooij, T.M.; Engel, C.; Noguès, C.; Stoppa-Lyonnet, D.; Lasset, C.; et al. Alcohol Consumption, Cigarette Smoking, and Risk of Breast Cancer for BRCA1 and BRCA2 Mutation Carriers: Results from The BRCA1 and BRCA2 Cohort Consortium. Cancer Epidemiol. Biomark. Prev. 2020, 29, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Dennis, J.; Ghadirian, P.; Little, J.; Lubinski, J.; Gronwald, J.; Kim-Sing, C.; Foulkes, W.; Moller, P.; Lynch, H.T.; Neuhausen, S.L.; et al. Alcohol consumption and the risk of breast cancer among BRCA1 and BRCA2 mutation carriers. Breast 2010, 19, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Ko, K.P.; Kim, S.J.; Huzarski, T.; Gronwald, J.; Lubinski, J.; Lynch, H.T.; Armel, S.; Park, S.K.; Karlan, B.; Singer, C.F.; et al. The association between smoking and cancer incidence in BRCA1 and BRCA2 mutation carriers. Int. J. Cancer 2018, 142, 2263–2272. [Google Scholar] [CrossRef] [PubMed]
- Ginsburg, O.; Ghadirian, P.; Lubinski, J.; Cybulski, C.; Lynch, H.; Neuhausen, S.; Kim-Sing, C.; Robson, M.; Domchek, S.; Isaacs, C.; et al. Smoking and the risk of breast cancer in BRCA1 and BRCA2 carriers: An update. Breast Cancer Res. Treat. 2009, 114, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Ghadirian, P.; Lubinski, J.; Lynch, H.; Neuhausen, S.L.; Weber, B.; Isaacs, C.; Baruch, R.G.; Randall, S.; Ainsworth, P.; Friedman, E.; et al. Smoking and the risk of breast cancer among carriers of BRCA mutations. Int. J. Cancer 2004, 110, 413–416. [Google Scholar] [CrossRef]
- Lammert, J.; Grill, S.; Kiechle, M. Modifiable Lifestyle Factors: Opportunities for (Hereditary) Breast Cancer Prevention—A Narrative Review. Breast Care 2018, 13, 109–114. [Google Scholar] [CrossRef]
- World Cancer Research Fund/Amaerican Institute for Cancer Research. Diet, Nutrition, Physical Activity and Breast Cancer; Continuous Update Project Expert Report 2018; World Cancer Research Fund/Amaerican Institute for Cancer Research: Washington, DC, USA, 2018. [Google Scholar]
- Kilian, C.; Manthey, J.; Probst, C.; Brunborg, G.S.; Bye, E.K.; Ekholm, O.; Kraus, L.; Moskalewicz, J.; Sieroslawski, J.; Rehm, J. Why Is Per Capita Consumption Underestimated in Alcohol Surveys? Results from 39 Surveys in 23 European Countries. Alcohol Alcohol. 2020, 55, 554–563. [Google Scholar] [CrossRef]
- Dieterich, M.; Stubert, J.; Reimer, T.; Erickson, N.; Berling, A. Influence of lifestyle factors on breast cancer risk. Breast Care 2014, 9, 407–414. [Google Scholar] [CrossRef]
- Kispert, S.; McHowat, J. Recent insights into cigarette smoking as a lifestyle risk factor for breast cancer. Breast Cancer (Dove. Med. Press) 2017, 9, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; Peralta, M.; Naia, A.; Loureiro, N.; de Matos, M.G. Prevalence of adult overweight and obesity in 20 European countries, 2014. Eur. J. Public Health 2018, 28, 295–300. [Google Scholar] [CrossRef]
- Neuhouser, M.L.; Aragaki, A.K.; Prentice, R.L.; Manson, J.E.; Chlebowski, R.; Carty, C.L.; Ochs-Balcom, H.M.; Thomson, C.A.; Caan, B.J.; Tinker, L.F.; et al. Overweight, Obesity, and Postmenopausal Invasive Breast Cancer Risk: A Secondary Analysis of the Women’s Health Initiative Randomized Clinical Trials. JAMA Oncol. 2015, 1, 611–621. [Google Scholar] [CrossRef]
- Ansari, S.; Haboubi, H.; Haboubi, N. Adult obesity complications: Challenges and clinical impact. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820934955. [Google Scholar] [CrossRef] [PubMed]
- Afshin, A.; Forouzanfar, M.H.; Reitsma, M.B.; Sur, P.; Estep, K.; Lee, A.; Marczak, L.; Mokdad, A.H.; Moradi-Lakeh, M.; Naghavi, M.; et al. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar]
- Sprague, B.L.; Trentham-Dietz, A.; Nichols, H.B.; Hampton, J.M.; Newcomb, P.A. Change in lifestyle behaviors and medication use after a diagnosis of ductal carcinoma in situ. Breast Cancer Res. Treat. 2010, 124, 487–495. [Google Scholar] [CrossRef]
- Irwin, M.L.; Crumley, D.; McTiernan, A.; Bernstein, L.; Baumgartner, R.; Gilliland, F.D.; Kriska, A.; Ballard-Barbash, R. Physical activity levels before and after a diagnosis of breast carcinoma: The Health, Eating, Activity, and Lifestyle (HEAL) study. Cancer 2003, 97, 1746–1757. [Google Scholar] [CrossRef]
- Peila, R.; Arthur, R.S.; Dannenberg, A.J.; Rohan, T.E. Association of a Healthy Lifestyle Index with Risk of Breast Cancer among Women with Normal Body Mass Index in the UK Biobank. Cancer Epidemiol. Biomark. Prev. 2022, 31, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Eriksson, M.; Czene, K.; Lee, A.; Leslie, G.; Lush, M.; Wang, J.; Dennis, J.; Dorling, L.; Carvalho, S.; et al. Prospective validation of the BOADICEA multifactorial breast cancer risk prediction model in a large prospective cohort study. J. Med. Genet. 2022, 59, 1196–1205. [Google Scholar] [CrossRef]


{kind=link}
| Including Breast Cancer Index | Excluding Breast Cancer Index | |
|---|---|---|
| Characteristics | N = 125 | N = 104 |
| Age at questionnaire completion, mean (SD) | 44 (13) | 42 (13) |
| Age at PHTS diagnosis, mean (SD) | 37 (14) | 34 (14) |
| Coding effect, N (%) | 124 (99%) | 103 (99%) |
| Missense | 51 (41%) | 45 (44%) |
| Truncating | 72 (58%) | 57 (55%) |
| Other | 1 (1%) | 1 (1%) |
| Domain, N (%) | 124 (99%) | 103 (99%) |
| C2 | 32 (26%) | 26 (25%) |
| Phosphatase | 77 (62%) | 64 (62%) |
| Other | 15 (12%) | 13 (13%) |
| Breast cancer (invasive or in situ) | ||
| N (%) | 39 (31%) | 18 (17%) |
| Age, mean (SD) | 43 (9) | 44 (8) |
| Preventive bilateral mastectomy b | ||
| N (%) | 16 (13%) | 16 (15%) |
| Age, mean (SD) | 33 (10) | 33 (10) |
| Lifestyle risk factors | ||
| Physical activity, N (%) | ||
| <1 time a week | 11 (9%) | 8 (8%) |
| 1 time a week | 13 (10%) | 10 (10%) |
| 2–3 times a week | 49 (39%) | 43 (41%) |
| 4–5 times a week | 29 (23%) | 25 (24%) |
| >5 times a week | 23 (18%) | 18 (17%) |
| Tobacco smoking, N (%) | ||
| Currently smoking | 6 (5%) | 6 (6%) |
| Smoked in the past | 22 (18%) | 16 (15%) |
| Never smoked | 89 (71%) | 76 (73%) |
| Never smoked, but indoor smoking at home | 8 (6%) | 6 (6%) |
| Smoking amount, N (%) c | ||
| <10 per day | 19 (68%) | 15 (68%) |
| 10-25 per day | 9 (32%) | 7 (32%) |
| >25 per day | 0 (0%) | 0 (0%) |
| Weekday alcohol consumption, N (%) | ||
| 0 glasses a day | 115 (92%) | 96 (92%) |
| 1 glass a day d | 1 (1%) | 1 (1%) |
| 2 glasses a day | 8 (6%) | 6 (5%) |
| ≥3 glasses a day | 1 (1%) | 1 (1%) |
| Weekend alcohol consumption, N (%) | ||
| 0 glasses a day | 80 (64%) | 65 (63%) |
| 1 glass a day d | 0 (0%) | 0 (0%) |
| 2 glasses a day | 35 (28%) | 30 (29%) |
| ≥3 glasses a day | 10 (8%) | 9 (9%) |
| BMI (kg/m2), N (%) | ||
| <18.5 (underweight) | 2 (2%) | 2 (2%) |
| 18.5–24.9 (normal weight) | 32 (26%) | 27 (26%) |
| 25.0–29.9 (overweight) | 38 (31%) | 34 (33%) |
| ≥30.0 (obesity) | 50 (41%) | 39 (38%) |
| Unknown | 3 | 2 |
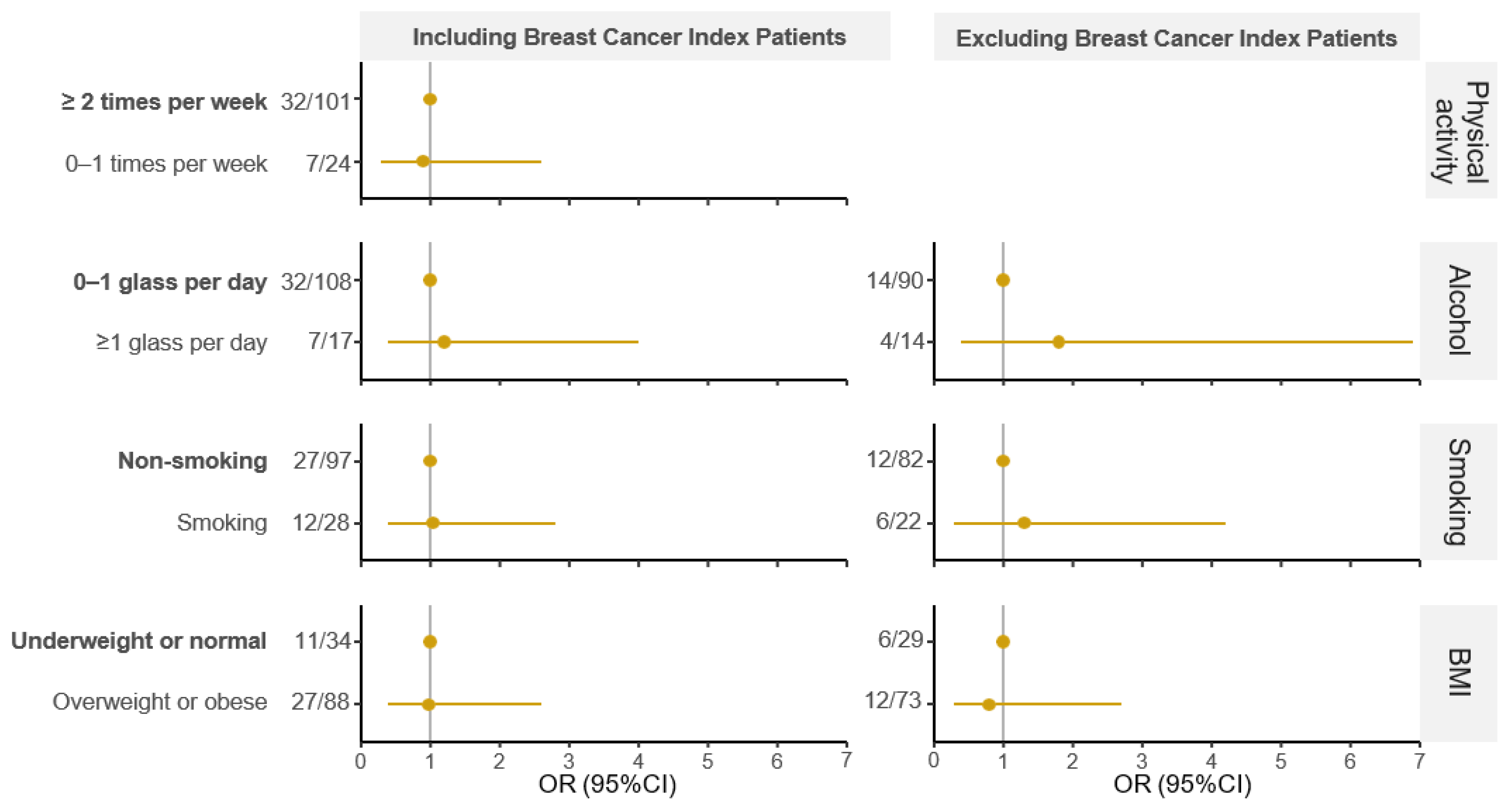
| Including Breast Cancer Index Patients | Excluding Breast Cancer Index Patients | |||||
|---|---|---|---|---|---|---|
| Lifestyle Factor | n/N | OR (95%CI) | ORadj (95%CI) | n/N | OR (95%CI) | ORadj (95%CI) |
| Physical activity | ||||||
| ≥2 times per week | 32/101 | - | - | 17/86 | - | - |
| 0–1 times per week | 7/24 | 0.9 (0.3–2.3) | 0.9 (0.3–2.6) | 1/18 | n/a | n/a |
| Alcohol consumption | ||||||
| 0–1 glass per day | 32/108 | - | - | 14/90 | - | - |
| ≥1 glass per day | 7/17 | 1.7 (0.6–4.7) | 1.2 (0.4–4.0) | 4/14 | 2.2 (0.5–7.6) | 1.8 (0.4–6.9) |
| Smoking | ||||||
| Non-smoking | 27/97 | - | - | 12/82 | - | - |
| Smoking | 12/28 | 1.9 (0.8–4.6) | 1.04 (0.4–2.8) | 6/22 | 2.2 (0.7–6.6) | 1.3 (0.3–4.2) |
| BMI | ||||||
| Underweight or normal | 11/34 | - | - | 6/29 | - | - |
| Overweight or obese | 27/88 | 0.9 (0.4–2.2) | 0.98 (0.4–2.6) | 12/73 | 0.8 (0.3–2.4) | 0.8 (0.3–2.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendricks, L.A.J.; Verbeek, K.C.J.; Schuurs-Hoeijmakers, J.H.M.; Mensenkamp, A.R.; Brems, H.; de Putter, R.; Anastasiadou, V.C.; Villy, M.-C.; Jahn, A.; Steinke-Lange, V.; et al. Lifestyle Factors and Breast Cancer in Females with PTEN Hamartoma Tumor Syndrome (PHTS). Cancers 2024, 16, 953. https://doi.org/10.3390/cancers16050953
Hendricks LAJ, Verbeek KCJ, Schuurs-Hoeijmakers JHM, Mensenkamp AR, Brems H, de Putter R, Anastasiadou VC, Villy M-C, Jahn A, Steinke-Lange V, et al. Lifestyle Factors and Breast Cancer in Females with PTEN Hamartoma Tumor Syndrome (PHTS). Cancers. 2024; 16(5):953. https://doi.org/10.3390/cancers16050953
Chicago/Turabian StyleHendricks, Linda A. J., Katja C. J. Verbeek, Janneke H. M. Schuurs-Hoeijmakers, Arjen R. Mensenkamp, Hilde Brems, Robin de Putter, Violetta C. Anastasiadou, Marie-Charlotte Villy, Arne Jahn, Verena Steinke-Lange, and et al. 2024. "Lifestyle Factors and Breast Cancer in Females with PTEN Hamartoma Tumor Syndrome (PHTS)" Cancers 16, no. 5: 953. https://doi.org/10.3390/cancers16050953