False Liver Metastasis by Positron Emission Tomography/Computed Tomography Scan after Chemoradiotherapy for Esophageal Cancer—Potential Overstaged Pitfalls of Treatment

Abstract
:Simple Summary
Abstract
1. Introduction
2. Mechanism and Application of FDG PET-CT Scan
2.1. Imaging Principles and Clinical Application
2.2. False Positive and False Negative PET/CT: Causes and Probabilities
2.2.1. Caveats in Interpreting PET-CT in Individuals with Esophageal Cancer
2.2.2. Common Non-Malignant Pathological Conditions Showing Increased Uptake of FDG before Therapy
3. Current Treatment Protocol of Esophageal Cancer Involving True Liver Metastasis and False Liver Metastasis
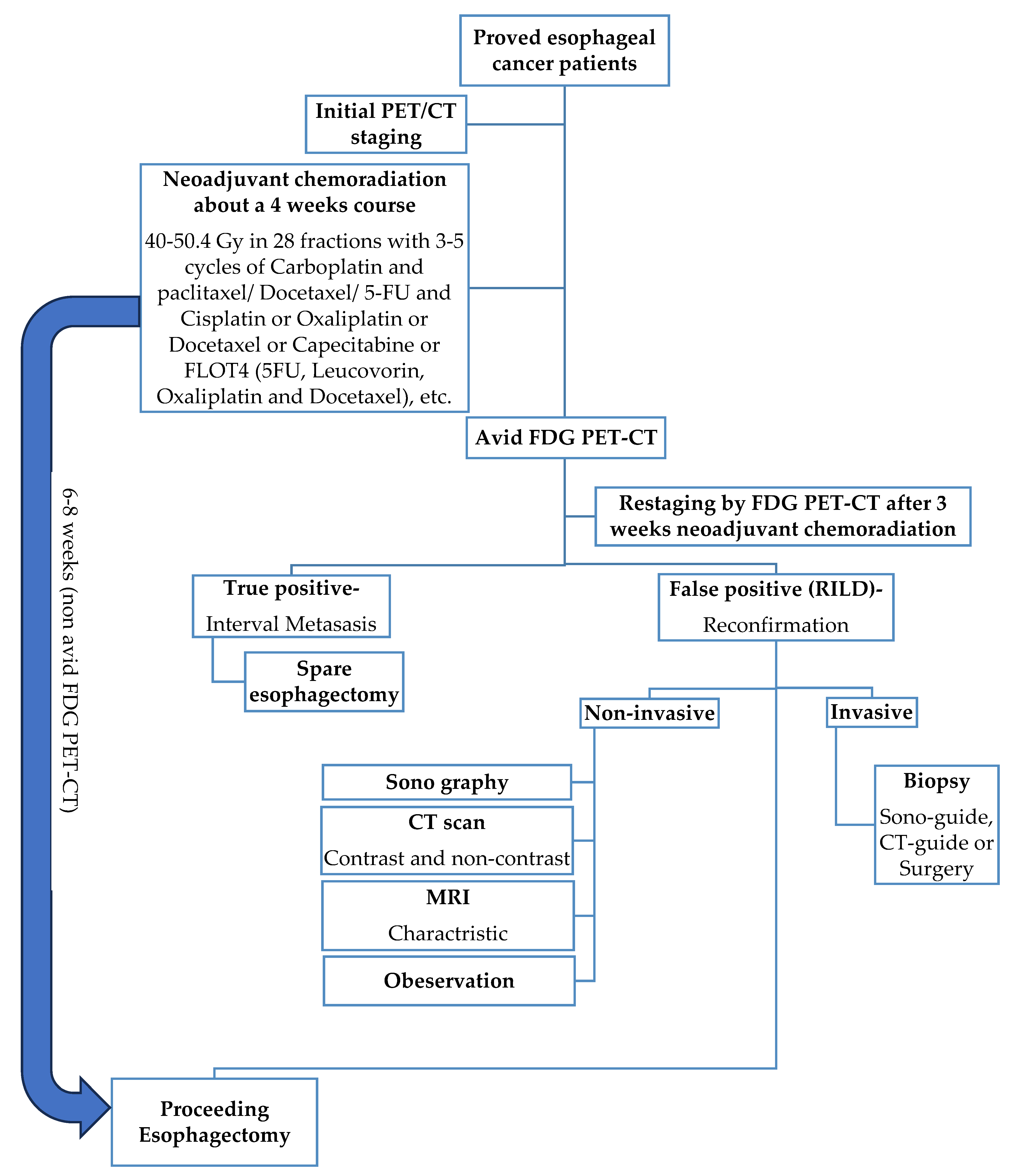
3.1. Current Standard Procedure of Treatment for Esophageal Cancer (Figure 1)

3.2. Reports of the Reference of True and False Metastasis for Restaging after nCRT
Case Reports Series (Table 3) and Cohort Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Age | TNM- Pathology | Chemotherapy | Radiotherapy Dose- Modality | Delay CRT to FDG PET | FDG PET | CT | MR | Biopsy | Liver Tests | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Iyer et al. (2007) [13] | 63 | NA-adeno | NA | 50.4 Gy-3D conformal | 6w | Nodular | Well-defined, low attenuation | - | Perop | AP ↑ | NA |
| Iyer et al. (2007) [13] | NA | NA-NA | NA | 50.4 Gy-3D conformal | 6w | Nodular | Well-defined, low attenuation | - | NA | AP ↑ | NA |
| Nakahara et al. (2008) [5] | 50 | uT3N M2 1(bone)-NA | Docetaxel weekly (20 mg/m2) | 46 Gy + boost 14 Gy-AP-RT | 4w | Wedge-shaped | Well-defined, low attenuation + band-like lesion (≈zone of <40 Gy) | - | NA | AP ↑ | 4 months |
| DeLappe et al. (2009) [44] | 61 | uT3N M1 0-NA | 4 cycli (apirubicine þ oxaliplatin + capcetabine) + 3 cycli (docetaxel þ irinotecan) + concurrent 5-FU | 50.4 Gy-IMRT | 5w | Ill-defined nodular | Patchy defined, mixed attenuation, heterogeneous enhancement of left liver | - | CT-guided + perop | NA | NA |
| Wong et al. (2012) [45] | 58 | NA-NA | NA | 50.4 Gy-AP-RT | 6w | Nodular with linear distribution | Patchy-defined, low attenuation in segment 2 and 3 | - | NA | Normal | NA |
| Rabe et al. (2016) [12] | 53 | uT3N M1 0-squamous | 5 cycli (carboplatin + paclitaxel) | 50.4 Gy-3D conformal | 2w | Nodular | Well-defined, low attenuation | Hyperintens T2-weighted | Perop | AP ↑ | 12 months |
| Demey et al. (2017) [46] | 42 | uT2N M1 0-adeno | Concurrent Oxaliplatin + 5-FU | 45 Gy-3D conformal | 4w | Nodular | Patchy-defined, low attenuation in segment 2 | Hyperintens T2-weighted | Perop | Normal | 18 months |
4. RILD Inducing False FDG PET-CT Interpretations
4.1. Implications of Increased FDG Uptake
4.2. The Formation and Classification of RILD
4.3. Occurrence and Duration of RILD
4.4. Incidence of RILD
4.4.1. Risk Factors for Radiation-Induced Liver Disease (RILD) by Tumor Cell Type
4.4.2. Influence of Gender, Age, and Race on RILD Susceptibility
4.5. Molecule Biology of RILD
4.6. Effects and Implications of RILD
4.6.1. Radiotherapy Dosage
4.6.2. Synergistic Effects with Chemotherapy
4.6.3. Pre-Existing Liver Diseases and Increased RILD Vulnerability
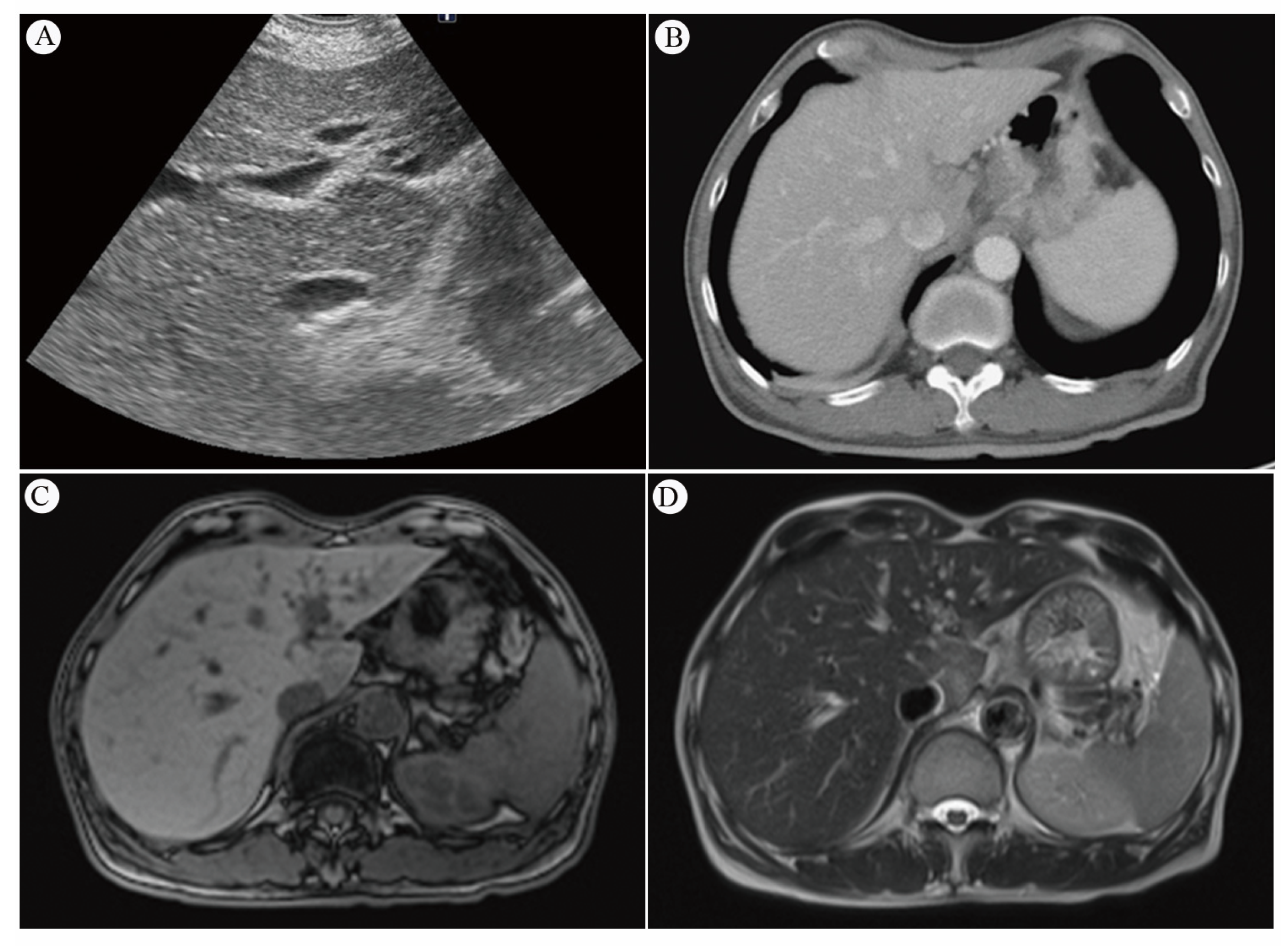
4.7. Challenges in Diagnosing RILD Using Imaging
4.7.1. Sonography of Liver and Its Sensitivity
4.7.2. CT Scan and Its Sensitivity
4.7.3. MRI and Its Sensitivity
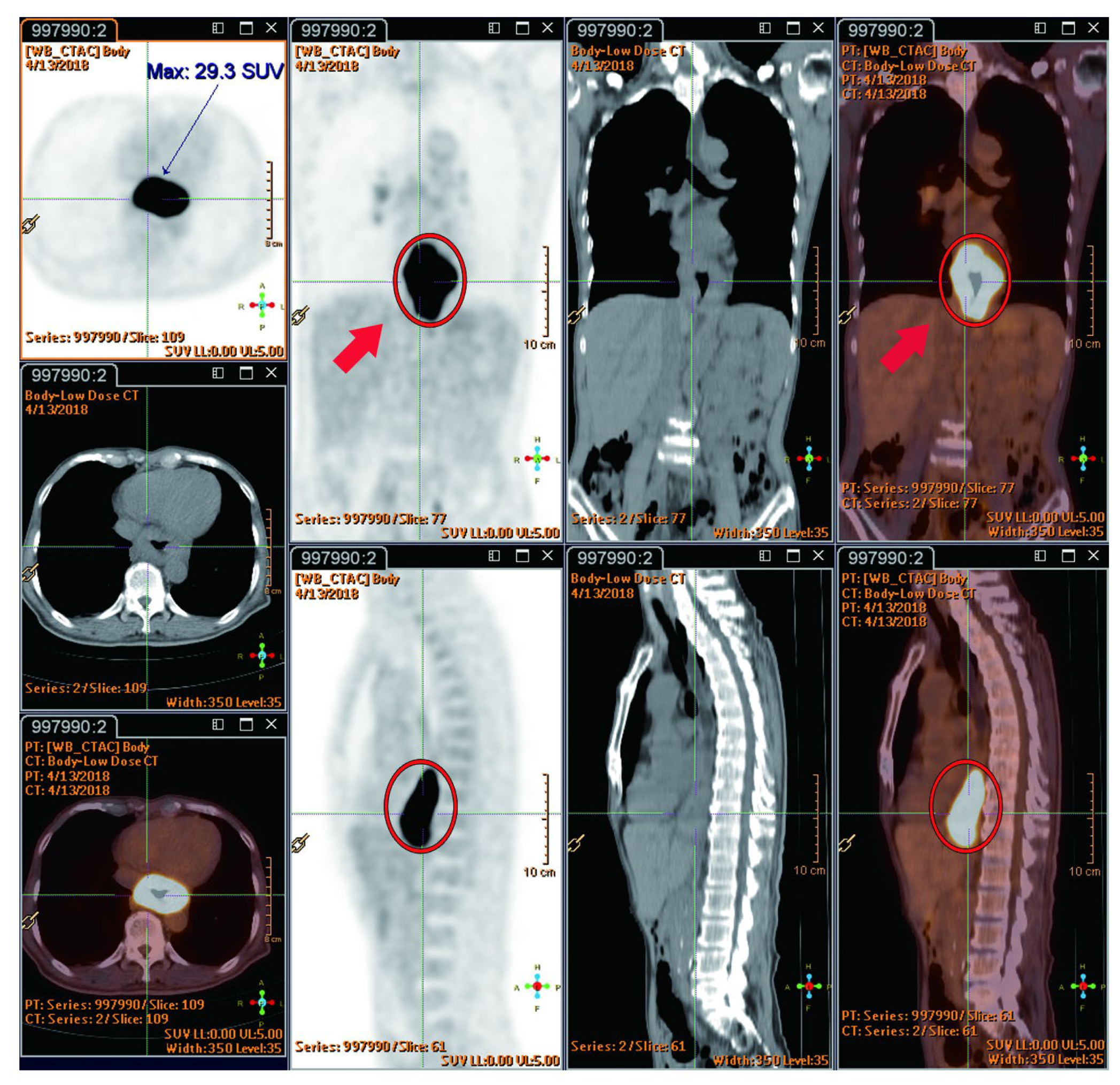
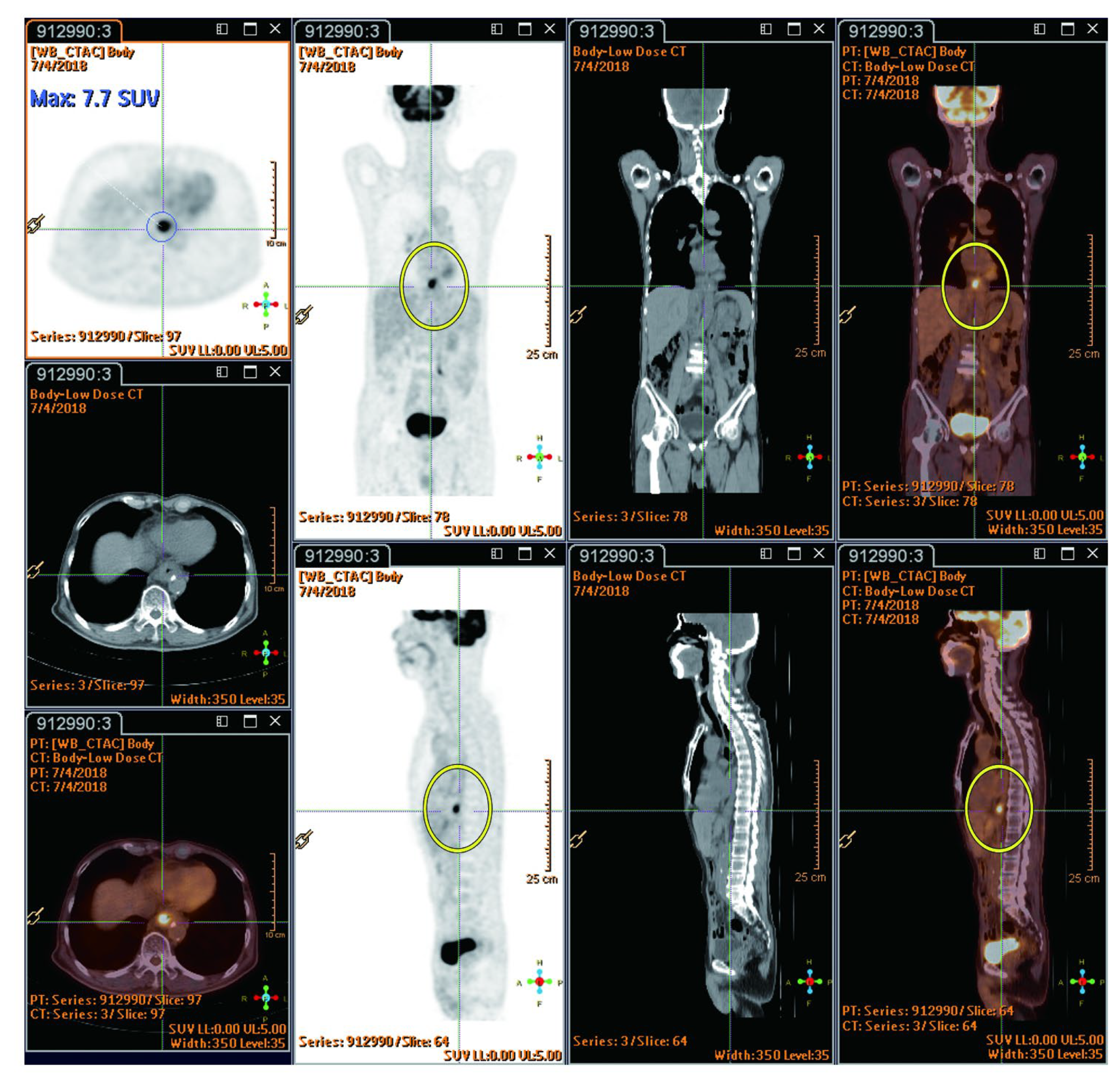
4.7.4. SUVmax (Standardized Uptake Value) Value in FDG PET-CT Serve as Indicators of RILD
4.7.5. Biopsy Options for Diagnosis of Liver lesions—Procedures Guided by Sonography, CT Scan, Mini-laparoscopy, Open Biopsy, or Clinical Observation
Pathological Characteristics of RILD
Gross and Microscopy Appearance of RILD
5. Overview of Literature Review
| Author (Year) | Gender | Age (Range) | Race | Chemoradiotherapy | Liver Function * | Stage | Esophageal Cancer | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Neoadjuvant | Dose | Medicine | SCC | Adeno | Other | |||||||
| 1 | Rabe et al. (2016) [12] | F | 53 | NA | Yes | 50.4 Gy | Cbp and Ptx | Yes | T3N1M0-->T2-weighted | 1 | 0 | 0 |
| 2 | Iyer et al. (2007) [13] | 24M/2F | 54 (41–78) | NA | Yes | 50.4 Gy | NA | Yes | NA | 2 | 24 | 0 |
| 3 | Daly et al. (2007) [4] | 74.2%M/25.8%F, n = 5044 | 67.3 | 76.8% Non-Hispanic Caucasian, 19.2% African American, 4.0% Hispanic | NA | NA | NA | NA | Clinical stage—0 (2.2%), I (14.1%), II (23.0%), III (22.1%), IV (38.7%) | 51.6% | 41.9% | 0 |
| 4 | Nakahara et al. (2008) [5] | M | 50 | NA | Yes | 46 Gy with an additional boost irradiation of 14 Gy. | Dot | Yes | Diagnosed with esophageal cancer with lymph node and bone metastases | NA | NA | 0 |
| 5 | Voncken et al. (2018) [14] | M | 50 | NA | Yes | 50.4 Gy | Cbp and Ptx | NA | T3N1M0 | 1 | 0 | 0 |
| M | 62 | Not specified | Yes | 41.4 Gy | Cbp and Ptx | No | T3N0M0 | 0 | 62 | 0 | ||
| M | 41 | NA | Yes | 41.4 Gy | Cbp and Ptx | No | T3N1M0 | 0 | 41 | 0 | ||
| M | 59 | NA | Yes | 50 Gy | Cis and 5-FU | No | T3N1M0 | 0 | 1 | 0 | ||
| M | 49 | NA | Yes | 41.4 Gy | Cbp and Ptx | No | T3N1M0 | 0 | 1 | 0 | ||
| 6 | Stiekema et al. (2014) [10] | 60M/16F | 63 (46–80) | NA | Yes | 50 Gy or 50/50.4 Gy | 5-FU and Cis or Cbp and Ptx | NA | NA | 14 | 60 | 2 |
| 24M/2F | 63 (46–80) | NA | Yes | 50 Gy (n= 21) or 41.4 Gy (n = 50) or 50.4 Gy (n = 5) | 5-FU and Cis (n = 21) or Cbp and Ptx (n= 55) | NA | NA | 9 | 39 | 0 | ||
| 7 | Grant et al. (2014) [22] | 93M/19F | 57 (28–81) | NA | Yes | 41.4–50.4 Gy | NA | NA | NA | 21 | 97 | 4 |
| 8 | Wieder et al. (2004) [56] | 27M/11F | 60 (46–73) | NA | Yes | 40 Gy | 5-FU | NA | NA | 38 | 0 | 0 |
| 9 | DeLappe et al. (2009) [44] | M | 61 | NA | Yes | 50.4 Gy | NA | NA | T3N1M0 | 0 | 1 | 0 |
| 10 | Shai et al. (2020) [48] | M | 66 | Asian | Yes | 50 Gy | NA | No | T3N1M0 | 1 | 0 | 0 |
| 11 | Demey et al. (2016) [46] | M | 42 | NA | Yes | 45 Gy | Oxa, levofolinic acid, and 5-FU | No | uT2N1M0 | 0 | 1 | 0 |
| 12 | Anderegg et al. (2015) [72] | 76.3%M, n = 156 | 65 (34–83) | NA | Yes | 41.4 Gy | Cbp and Ptx (n = 139) or Cbp, Ptx, and Vectibix (n = 17) | NA | NA | 29 | 126 | 1 |
| 13 | Voncken et al. (2018) [14] | M | 50 | NA | Yes | 50.4 Gy | Cbp and Ptx | NA | T3N1M0 | 1 | 0 | 0 |
| M | 62 | NA | Yes | 41.4 Gy | Cbp and Ptx | No | T3N0M0 | 0 | 1 | 0 | ||
| M | 41 | NA | Yes | 41.4 Gy | Cbp and Ptx | No | T3N1M0 | 0 | 1 | 0 | ||
| M | 59 | NA | Yes | 50 Gy | Cis and 5-FU | No | T3N1M0 | 0 | 1 | 0 | ||
| M | 49 | NA | Yes | 41.4 Gy | Cbp and Ptx | No | T3N1M0 | 0 | 1 | 0 | ||
| M | 75 | NA | Yes | 50 Gy | Cbp and etoposide | No | T2N1M0 | 0 | 0 | 1 | ||
| 14 | Goense et al. (2018) [11] | 675M/108F | <65, n = 425; ≥65, n = 358 | NA | Yes | 45 Gy or 50.4 Gy | Oxa and 5-FU or Doc and 5-FU or Xeloda and 5-FU or other | NA | NA | 111 | 672 | 0 |
| 15 | Gabriel et al. (2017) [21] | 234M/24F | 61.5 | NA | Yes | 50.4 Gy | Cis and Iri/Cbp and Ptx or Oxa and Xeloda or 5-FU and Cis | NA | NA | 39 | 219 | 0 |
| 16 | Li et al. (2020) [73] | 76M/48F | 56 (25–82) | NA | NA | NA | NA | NA | NA | 20 | 69 | 35 |
| 17 | Blom et al. (2011) [8] | 40M/10F | 61 (56–67) | NA | Yes | 50.4 Gy | Cis and 5-FU | NA | Stages II to IVa | 9 | 40 | 1 |
| 18 | Cerfolio et al. (2005) [40] | 41M/7F | 68 (48–76) | NA | Yes | <50 Gy (n = 22), >50 Gy (n = 26) | NA | NA | Stages I to Ivb | 5 | 43 | 0 |
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
Abbreviations
| nCRT | neoadjuvant chemoradiotherapy |
| CRT | chemoradiotherapy |
| 18F-FDG | F-18-fluorodeoxyglucose |
| PET-CT | positron emission tomography–computed tomography |
| RILI | radiation-induced liver injury |
| RILD | radiation-induced liver disease |
| TB | tuberculosis |
| IMRT | intensity-modulated therapy |
| RT | radiation therapy |
| RH | radiation hepatitis |
| VOD | Veno Occlusive Disease |
| SCC | squamous-cell carcinoma |
| KC | Kupffer cells |
| HSC | Hepatic stellate cell |
| SEC | sinusoidal endothelial cell |
| IMRT | intensity modulated therapy |
| SUV | standardized uptake value |
| FLOT4 | 5FU, Leucovorin, Oxaliplatin, Docetaxel |
References
- Pennathur, A.; Gibson, M.K.; Jobe, B.A.; Luketich, J.D. Oesophageal carcinoma. Lancet 2013, 381, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Sjoquist, K.M.; Burmeister, B.H.; Smithers, B.M.; Zalcberg, J.R.; Simes, R.J.; Barbour, A.; Gebski, V. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: An updated meta-analysis. Lancet Oncol. 2011, 12, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, J.; van Lanschot, J.J.B.; Hulshof, M.; van Hagen, P.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.L.; van Laarhoven, H.W.M.; Nieuwenhuijzen, G.A.P.; Hospers, G.A.P.; Bonenkamp, J.J.; et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): Long-term results of a randomised controlled trial. Lancet Oncol. 2015, 16, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.M.; Fry, W.A.; Little, A.G.; Winchester, D.P.; McKee, R.F.; Stewart, A.K.; Fremgen, A.M. Esophageal cancer: Results of an American College of Surgeons Patient Care Evaluation Study. J. Am. Coll. Surg. 2000, 190, 562–572; discussion 563–572. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, T.; Takagi, Y.; Takemasa, K.; Mitsui, Y.; Tsuyuki, A.; Shigematsu, N.; Kubo, A. Dose-related fluorodeoxyglucose uptake in acute radiation-induced hepatitis. Eur. J. Gastroenterol. Hepatol. 2008, 20, 1040–1044. [Google Scholar] [CrossRef] [PubMed]
- Monjazeb, A.M.; Riedlinger, G.; Aklilu, M.; Geisinger, K.R.; Mishra, G.; Isom, S.; Clark, P.; Levine, E.A.; Blackstock, A.W. Outcomes of patients with esophageal cancer staged with [18F]fluorodeoxyglucose positron emission tomography (FDG-PET): Can postchemoradiotherapy FDG-PET predict the utility of resection? J. Clin. Oncol. 2010, 28, 4714–4721. [Google Scholar] [CrossRef] [PubMed]
- Smithers, B.M.; Couper, G.C.; Thomas, J.M.; Wong, D.; Gotley, D.C.; Martin, I.; Harvey, J.A.; Thomson, D.B.; Walpole, E.T.; Watts, N.; et al. Positron emission tomography and pathological evidence of response to neoadjuvant therapy in adenocarcinoma of the esophagus. Dis. Esophagus 2008, 21, 151–158. [Google Scholar] [CrossRef]
- Blom, R.L.; Schreurs, W.M.; Belgers, H.J.; Oostenbrug, L.E.; Vliegen, R.F.; Sosef, M.N. The value of post-neoadjuvant therapy PET-CT in the detection of interval metastases in esophageal carcinoma. Eur. J. Surg. Oncol. 2011, 37, 774–778. [Google Scholar] [CrossRef]
- Bruzzi, J.F.; Munden, R.F.; Truong, M.T.; Marom, E.M.; Sabloff, B.S.; Gladish, G.W.; Iyer, R.B.; Pan, T.S.; Macapinlac, H.A.; Erasmus, J.J. PET/CT of esophageal cancer: Its role in clinical management. Radiographics 2007, 27, 1635–1652. [Google Scholar] [CrossRef]
- Stiekema, J.; Vermeulen, D.; Vegt, E.; Voncken, F.E.; Aleman, B.M.; Sanders, J.; Boot, H.; van Sandick, J.W. Detecting interval metastases and response assessment using 18F-FDG PET/CT after neoadjuvant chemoradiotherapy for esophageal cancer. Clin. Nucl. Med. 2014, 39, 862–867. [Google Scholar] [CrossRef]
- Goense, L.; Ruurda, J.P.; Carter, B.W.; Fang, P.; Ho, L.; Meijer, G.J.; van Hillegersberg, R.; Hofstetter, W.L.; Lin, S.H. Prediction and diagnosis of interval metastasis after neoadjuvant chemoradiotherapy for oesophageal cancer using (18)F-FDG PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1742–1751. [Google Scholar] [CrossRef] [PubMed]
- Rabe, T.M.; Yokoo, T.; Meyer, J.; Kernstine, K.H., Sr.; Wang, D.; Khatri, G. Radiation-Induced Liver Injury Mimicking Metastatic Disease in a Patient With Esophageal Cancer: Correlation of Positron Emission Tomography/Computed Tomography With Magnetic Resonance Imaging and Literature Review. J. Comput. Assist. Tomogr. 2016, 40, 560–563. [Google Scholar] [CrossRef] [PubMed]
- Iyer, R.B.; Balachandran, A.; Bruzzi, J.F.; Johnson, V.; Macapinlac, H.A.; Munden, R.F. PET/CT and hepatic radiation injury in esophageal cancer patients. Cancer Imaging 2007, 7, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Voncken, F.E.M.; Aleman, B.M.P.; van Dieren, J.M.; Grootscholten, C.; Lalezari, F.; van Sandick, J.W.; Steinberg, J.D.; Vegt, E. Radiation-induced liver injury mimicking liver metastases on FDG-PET-CT after chemoradiotherapy for esophageal cancer: A retrospective study and literature review. Strahlenther. Onkol. 2018, 194, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Reed, G.B., Jr.; Cox, A.J., Jr. The human liver after radiation injury. A form of veno-occlusive disease. Am. J. Pathol. 1966, 48, 597–611. [Google Scholar] [PubMed]
- Benson, R.; Madan, R.; Kilambi, R.; Chander, S. Radiation induced liver disease: A clinical update. J. Egypt. Natl. Canc Inst. 2016, 28, 7–11. [Google Scholar] [CrossRef]
- Kim, J.; Jung, Y. Radiation-induced liver disease: Current understanding and future perspectives. Exp. Mol. Med. 2017, 49, e359. [Google Scholar] [CrossRef]
- Lawrence, T.S.; Robertson, J.M.; Anscher, M.S.; Jirtle, R.L.; Ensminger, W.D.; Fajardo, L.F. Hepatic toxicity resulting from cancer treatment. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1237–1248. [Google Scholar] [CrossRef]
- Ogata, K.; Hizawa, K.; Yoshida, M.; Kitamuro, T.; Akagi, G.; Kagawa, K.; Fukuda, F. Hepatic Injury Following Irradiation—A Morphologic Study. Tokushima J. Exp. Med. 1963, 10, 240–251. [Google Scholar]
- Chou, C.H.; Chen, P.J.; Lee, P.H.; Cheng, A.L.; Hsu, H.C.; Cheng, J.C. Radiation-induced hepatitis B virus reactivation in liver mediated by the bystander effect from irradiated endothelial cells. Clin. Cancer Res. 2007, 13, 851–857. [Google Scholar] [CrossRef]
- Gabriel, E.; Alnaji, R.; Du, W.; Attwood, K.; Kukar, M.; Hochwald, S. Effectiveness of Repeat 18F-Fluorodeoxyglucose Positron Emission Tomography Computerized Tomography (PET-CT) Scan in Identifying Interval Metastases for Patients with Esophageal Cancer. Ann. Surg. Oncol. 2017, 24, 1739–1746. [Google Scholar] [CrossRef]
- Grant, M.J.; Didier, R.A.; Stevens, J.S.; Beyder, D.D.; Hunter, J.G.; Thomas, C.R.; Coakley, F.V. Radiation-induced liver disease as a mimic of liver metastases at serial PET/CT during neoadjuvant chemoradiation of distal esophageal cancer. Abdom. Imaging 2014, 39, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Som, P.; Atkins, H.L.; Bandoypadhyay, D.; Fowler, J.S.; MacGregor, R.R.; Matsui, K.; Oster, Z.H.; Sacker, D.F.; Shiue, C.Y.; Turner, H.; et al. A fluorinated glucose analog, 2-fluoro-2-deoxy-D-glucose (F-18): Nontoxic tracer for rapid tumor detection. J. Nucl. Med. 1980, 21, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ghesani, N.V.; Zuckier, L.S. Physiology and pathophysiology of incidental findings detected on FDG-PET scintigraphy. Semin. Nucl. Med. 2010, 40, 294–315. [Google Scholar] [CrossRef] [PubMed]
- von Schulthess, G.K.; Steinert, H.C.; Hany, T.F. Integrated PET/CT: Current applications and future directions. Radiology 2006, 238, 405–422. [Google Scholar] [CrossRef] [PubMed]
- Blodgett, T.M.; Meltzer, C.C.; Townsend, D.W. PET/CT: Form and function. Radiology 2007, 242, 360–385. [Google Scholar] [CrossRef] [PubMed]
- Hillner, B.E.; Siegel, B.A.; Liu, D.; Shields, A.F.; Gareen, I.F.; Hanna, L.; Stine, S.H.; Coleman, R.E. Impact of positron emission tomography/computed tomography and positron emission tomography (PET) alone on expected management of patients with cancer: Initial results from the National Oncologic PET Registry. J. Clin. Oncol. 2008, 26, 2155–2161. [Google Scholar] [CrossRef]
- Poeppel, T.D.; Krause, B.J.; Heusner, T.A.; Boy, C.; Bockisch, A.; Antoch, G. PET/CT for the staging and follow-up of patients with malignancies. Eur. J. Radiol. 2009, 70, 382–392. [Google Scholar] [CrossRef]
- Metser, U.; Miller, E.; Lerman, H.; Even-Sapir, E. Benign nonphysiologic lesions with increased 18F-FDG uptake on PET/CT: Characterization and incidence. Am. J. Roentgenol. 2007, 189, 1203–1210. [Google Scholar] [CrossRef]
- Beatty, J.S.; Williams, H.T.; Aldridge, B.A.; Hughes, M.P.; Vasudeva, V.S.; Gucwa, A.L.; David, G.S.; Lind, D.S.; Kruse, E.J.; McLoughlin, J.M. Incidental PET/CT findings in the cancer patient: How should they be managed? Surgery 2009, 146, 274–281. [Google Scholar] [CrossRef]
- Culverwell, A.D.; Scarsbrook, A.F.; Chowdhury, F.U. False-positive uptake on 2-[18F]-fluoro-2-deoxy-D-glucose (FDG) positron-emission tomography/computed tomography (PET/CT) in oncological imaging. Clin. Radiol. 2011, 66, 366–382. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, F.U.; Sheerin, F.; Bradley, K.M.; Gleeson, F.V. Sarcoid-like reaction to malignancy on whole-body integrated (18)F-FDG PET/CT: Prevalence and disease pattern. Clin. Radiol. 2009, 64, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Jacene, H.A.; Stearns, V.; Wahl, R.L. Lymphadenopathy resulting from acute hepatitis C infection mimicking metastatic breast carcinoma on FDG PET/CT. Clin. Nucl. Med. 2006, 31, 379–381. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Steliarova-Foucher, E.; Lortet-Tieulent, J.; Rosso, S.; Coebergh, J.W.; Comber, H.; Forman, D.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries in 2012. Eur. J. Cancer 2013, 49, 1374–1403. [Google Scholar] [CrossRef] [PubMed]
- Heeren, P.A.; Jager, P.L.; Bongaerts, F.; van Dullemen, H.; Sluiter, W.; Plukker, J.T. Detection of distant metastases in esophageal cancer with (18)F-FDG PET. J. Nucl. Med. 2004, 45, 980–987. [Google Scholar] [PubMed]
- Nijkamp, J.; Rossi, M.; Lebesque, J.; Belderbos, J.; van den Heuvel, M.; Kwint, M.; Uyterlinde, W.; Vogel, W.; Sonke, J.J. Relating acute esophagitis to radiotherapy dose using FDG-PET in concurrent chemo-radiotherapy for locally advanced non-small cell lung cancer. Radiother. Oncol. 2013, 106, 118–123. [Google Scholar] [CrossRef] [PubMed]
- Ulaner, G.A.; Lyall, A. Identifying and distinguishing treatment effects and complications from malignancy at FDG PET/CT. Radiographics 2013, 33, 1817–1834. [Google Scholar] [CrossRef]
- Bruzzi, J.F.; Swisher, S.G.; Truong, M.T.; Munden, R.F.; Hofstetter, W.L.; Macapinlac, H.A.; Correa, A.M.; Mawlawi, O.; Ajani, J.A.; Komaki, R.R.; et al. Detection of interval distant metastases: Clinical utility of integrated CT-PET imaging in patients with esophageal carcinoma after neoadjuvant therapy. Cancer 2007, 109, 125–134. [Google Scholar] [CrossRef]
- Flamen, P.; Van Cutsem, E.; Lerut, A.; Cambier, J.P.; Haustermans, K.; Bormans, G.; De Leyn, P.; Van Raemdonck, D.; De Wever, W.; Ectors, N.; et al. Positron emission tomography for assessment of the response to induction radiochemotherapy in locally advanced oesophageal cancer. Ann. Oncol. 2002, 13, 361–368. [Google Scholar] [CrossRef]
- Cerfolio, R.J.; Bryant, A.S.; Ohja, B.; Bartolucci, A.A.; Eloubeidi, M.A. The accuracy of endoscopic ultrasonography with fine-needle aspiration, integrated positron emission tomography with computed tomography, and computed tomography in restaging patients with esophageal cancer after neoadjuvant chemoradiotherapy. J. Thorac. Cardiovasc. Surg. 2005, 129, 1232–1241. [Google Scholar] [CrossRef]
- Weber, W.A.; Ott, K.; Becker, K.; Dittler, H.J.; Helmberger, H.; Avril, N.E.; Meisetschläger, G.; Busch, R.; Siewert, J.R.; Schwaiger, M.; et al. Prediction of response to preoperative chemotherapy in adenocarcinomas of the esophagogastric junction by metabolic imaging. J. Clin. Oncol. 2001, 19, 3058–3065. [Google Scholar] [CrossRef] [PubMed]
- Findlay, J.M.; Gillies, R.S.; Franklin, J.M.; Teoh, E.J.; Jones, G.E.; di Carlo, S.; Gleeson, F.V.; Maynard, N.D.; Bradley, K.M.; Middleton, M.R. Restaging oesophageal cancer after neoadjuvant therapy with (18)F-FDG PET-CT: Identifying interval metastases and predicting incurable disease at surgery. Eur. Radiol. 2016, 26, 3519–3533. [Google Scholar] [CrossRef] [PubMed]
- Levine, E.A.; Farmer, M.R.; Clark, P.; Mishra, G.; Ho, C.; Geisinger, K.R.; Melin, S.A.; Lovato, J.; Oaks, T.; Blackstock, A.W. Predictive value of 18-fluoro-deoxy-glucose-positron emission tomography (18F-FDG-PET) in the identification of responders to chemoradiation therapy for the treatment of locally advanced esophageal cancer. Ann. Surg. 2006, 243, 472–478. [Google Scholar] [CrossRef] [PubMed]
- DeLappe, E.M.; Truong, M.T.; Bruzzi, J.F.; Swisher, S.G.; Rohren, E.M. Hepatic radiation injury mimicking a metastasis on positron-emission tomography/computed tomography in a patient with esophageal carcinoma. J. Thorac. Oncol. 2009, 4, 1442–1444. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.J.; Anthony, M.P.; Lan Khong, P. Hepatic radiation injury in distal esophageal carcinoma: A case report. Clin. Nucl. Med. 2012, 37, 709–711. [Google Scholar] [CrossRef]
- Demey, K.; Van Veer, H.; Nafteux, P.; Deroose, C.M.; Haustermans, K.; Coolen, J.; Vandecaveye, V.; Coosemans, W.; Van Cutsem, E. Hepatic radiation injury mimicking metastasis in distal esophageal cancer. Acta Chir. Belg. 2017, 117, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Luk, W.H.; Au-Yeung, A.W.; Loke, T.K. Imaging patterns of liver uptakes on PET scan: Pearls and pitfalls. Nucl. Med. Rev. Cent. East. Eur. 2013, 16, 75–81. [Google Scholar] [CrossRef]
- Shai, S.E.; Lin, Y.H.; Lai, Y.L.; Tang, H.W.; Hsieh, Y.W.; Hung, S.C. Phantom simulation of liver metastasis on a positron emission tomography with computed tomography scan after neoadjuvant chemoradiotherapy for distal esophageal cancer: A case report. J. Med. Case Rep. 2020, 14, 106. [Google Scholar] [CrossRef]
- Fajardo, L.F.; Colby, T.V. Pathogenesis of veno-occlusive liver disease after radiation. Arch. Pathol. Lab. Med. 1980, 104, 584–588. [Google Scholar]
- Dawson, L.A.; Normolle, D.; Balter, J.M.; McGinn, C.J.; Lawrence, T.S.; Ten Haken, R.K. Analysis of radiation-induced liver disease using the Lyman NTCP model. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 810–821. [Google Scholar] [CrossRef]
- Dawson, L.A.; Ten Haken, R.K. Partial volume tolerance of the liver to radiation. Semin. Radiat. Oncol. 2005, 15, 279–283. [Google Scholar] [CrossRef]
- Yamasaki, S.A.; Marn, C.S.; Francis, I.R.; Robertson, J.M.; Lawrence, T.S. High-dose localized radiation therapy for treatment of hepatic malignant tumors: CT findings and their relation to radiation hepatitis. Am. J. Roentgenol. 1995, 165, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Munden, R.F.; Erasmus, J.J.; Smythe, W.R.; Madewell, J.E.; Forster, K.M.; Stevens, C.W. Radiation injury to the liver after intensity-modulated radiation therapy in patients with mesothelioma: An unusual CT appearance. Am. J. Roentgenol. 2005, 184, 1091–1095. [Google Scholar] [CrossRef] [PubMed]
- Enzinger, P.C.; Mayer, R.J. Esophageal cancer. N. Engl. J. Med. 2003, 349, 2241–2252. [Google Scholar] [CrossRef] [PubMed]
- Lee, U.E.; Friedman, S.L. Mechanisms of hepatic fibrogenesis. Best. Pract. Res. Clin. Gastroenterol. 2011, 25, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Wieder, H.A.; Brücher, B.L.; Zimmermann, F.; Becker, K.; Lordick, F.; Beer, A.; Schwaiger, M.; Fink, U.; Siewert, J.R.; Stein, H.J.; et al. Time course of tumor metabolic activity during chemoradiotherapy of esophageal squamous cell carcinoma and response to treatment. J. Clin. Oncol. 2004, 22, 900–908. [Google Scholar] [CrossRef] [PubMed]
- King, P.D.; Perry, M.C. Hepatotoxicity of chemotherapy. Oncologist 2001, 6, 162–176. [Google Scholar] [CrossRef] [PubMed]
- Guha, C.; Kavanagh, B.D. Hepatic radiation toxicity: Avoidance and amelioration. Semin. Radiat. Oncol. 2011, 21, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Jeffrey, R.B., Jr.; Moss, A.A.; Quivey, J.M.; Federle, M.P.; Wara, W.M. CT of radiation-induced hepatic injury. Am. J. Roentgenol. 1980, 135, 445–448. [Google Scholar] [CrossRef]
- Unger, E.C.; Lee, J.K.; Weyman, P.J. CT and MR imaging of radiation hepatitis. J. Comput. Assist. Tomogr. 1987, 11, 264–268. [Google Scholar] [CrossRef]
- Kwek, J.W.; Iyer, R.B.; Dunnington, J.; Faria, S.; Silverman, P.M. Spectrum of imaging findings in the abdomen after radiotherapy. Am. J. Roentgenol. 2006, 187, 1204–1211. [Google Scholar] [CrossRef] [PubMed]
- Itai, Y.; Murata, S.; Kurosaki, Y. Straight border sign of the liver: Spectrum of CT appearances and causes. Radiographics 1995, 15, 1089–1102. [Google Scholar] [CrossRef] [PubMed]
- Vernuccio, F.; Cannella, R.; Bartolotta, T.V.; Galia, M.; Tang, A.; Brancatelli, G. Advances in liver US, CT, and MRI: Moving toward the future. Eur. Radiol. Exp. 2021, 5, 52. [Google Scholar] [CrossRef] [PubMed]
- Viswanathan, C.; Truong, M.T.; Sagebiel, T.L.; Bronstein, Y.; Vikram, R.; Patnana, M.; Silverman, P.M.; Bhosale, P.R. Abdominal and pelvic complications of nonoperative oncologic therapy. Radiographics 2014, 34, 941–961. [Google Scholar] [CrossRef] [PubMed]
- Jelvehgaran, P.; Steinberg, J.D.; Khmelinskii, A.; Borst, G.; Song, J.Y.; de Wit, N.; de Bruin, D.M.; van Herk, M. Evaluation of acute esophageal radiation-induced damage using magnetic resonance imaging: A feasibility study in mice. Radiat. Oncol. 2019, 14, 188. [Google Scholar] [CrossRef] [PubMed]
- Seidensticker, M.; Burak, M.; Kalinski, T.; Garlipp, B.; Koelble, K.; Wust, P.; Antweiler, K.; Seidensticker, R.; Mohnike, K.; Pech, M.; et al. Radiation-induced liver damage: Correlation of histopathology with hepatobiliary magnetic resonance imaging, a feasibility study. Cardiovasc. Intervent Radiol. 2015, 38, 213–221. [Google Scholar] [CrossRef]
- Umezawa, R.; Ota, H.; Takanami, K.; Ichinose, A.; Matsushita, H.; Saito, H.; Takase, K.; Jingu, K. MRI findings of radiation-induced myocardial damage in patients with oesophageal cancer. Clin. Radiol. 2014, 69, 1273–1279. [Google Scholar] [CrossRef]
- Machann, W.; Beer, M.; Breunig, M.; Störk, S.; Angermann, C.; Seufert, I.; Schwab, F.; Kölbl, O.; Flentje, M.; Vordermark, D. Cardiac magnetic resonance imaging findings in 20-year survivors of mediastinal radiotherapy for Hodgkin’s disease. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1117–1123. [Google Scholar] [CrossRef]
- Yankelevitz, D.F.; Henschke, C.I.; Knapp, P.H.; Nisce, L.; Yi, Y.; Cahill, P. Effect of radiation therapy on thoracic and lumbar bone marrow: Evaluation with MR imaging. Am. J. Roentgenol. 1991, 157, 87–92. [Google Scholar] [CrossRef]
- Daldrup-Link, H.E.; Henning, T.; Link, T.M. MR imaging of therapy-induced changes of bone marrow. Eur. Radiol. 2007, 17, 743–761. [Google Scholar] [CrossRef]
- Sempoux, C.; Horsmans, Y.; Geubel, A.; Fraikin, J.; Van Beers, B.E.; Gigot, J.F.; Lerut, J.; Rahier, J. Severe radiation-induced liver disease following localized radiation therapy for biliopancreatic carcinoma: Activation of hepatic stellate cells as an early event. Hepatology 1997, 26, 128–134. [Google Scholar] [CrossRef]
- Anderegg, M.C.; de Groof, E.J.; Gisbertz, S.S.; Bennink, R.J.; Lagarde, S.M.; Klinkenbijl, J.H.; Dijkgraaf, M.G.; Bergman, J.J.; Hulshof, M.C.; van Laarhoven, H.W.; et al. 18F-FDG PET-CT after Neoadjuvant Chemoradiotherapy in Esophageal Cancer Patients to Optimize Surgical Decision Making. PLoS ONE 2015, 10, e0133690. [Google Scholar] [CrossRef]
- Li, Y.; Li, F.; Li, X.; Qu, L.; Han, J. Value of 18F-FDG PET/CT in patients with hepatic metastatic carcinoma of unknown primary. Medicine 2020, 99, e23210. [Google Scholar] [CrossRef]





| Causes of False-Positive Findings | Causes of False-Negative Findings |
|---|---|
| Infections/inflammatory lesions | Lesion dependent |
| Radiation-induced liver disease (RILD) | Small tumors (<8–10 mm) |
| Radiation pneumonitis | Low metabolic activity of the tumor |
| (Postobstructive) pneumonia/abscess | The presence of a treatment-induced decrease in tumor metabolism |
| Mycobacterial or fungal infection | Technique limitation |
| Granulomatous disorders (sarcoidosis, Wegener) | Hyperglycemia |
| Chronic nonspecific lymphadenitis | Paravenous FDG injection |
| (Rheumatoid) arthritis | Excessive time between injection and scanning |
| Occupational exposure (anthracosilicosis) | Low resolution or motion artifacts |
| Bronchiectasis | |
| Organizing pneumonia | |
| Reflux esophagitis | |
| Iatrogenic causes | |
| Invasive procedure (puncture, biopsy) | |
| Talc pleurodesis | |
| Radiation esophagitis and pneumonitis | |
| Bone marrow expansion postchemotherapy | |
| Colony-stimulating factors | |
| Thymic hyperplasia postchemotherapy | |
| Benign mass lesions | |
| Salivary gland adenoma (Whartin) | |
| Thyroid adenoma | |
| Adrenal adenoma | |
| Colorectal dysplastic polyps | |
| Focal physiological FDG uptake | |
| Gastrointestinal tract | |
| Muscle activity | |
| Brown fat | |
| Unilateral vocal cord activity | |
| Arherosclerotic plaques |
| Parameter | 18F-FDG PET-CT |
|---|---|
| Sensitivity (%) [95%CI] | 65/87 (74.7%) [64.3–83.4] |
| Specificity (%) [95%CI] | 652/696 (93.7%) [91.6–95.4] |
| Positive predictive value (%) [95%CI] | 65/109 (59.6%) [52.0–66.9] |
| Negative predictive value (%) [95%CI] | 652/674 (96.7%) [95.4–97.7] |
| Diagnostic accuracy | 91.6% |
| Risk Factor | Squamous Cell Carcinoma | Adenocarcinoma |
|---|---|---|
| Tobacco use | +++ | ++ |
| Alcohol use | +++ | - |
| Barrett’s esophagus | - | ++++ |
| Weekly reflux symptoms | - | +++ |
| Obesity | - | ++ |
| Poverty | ++ | - |
| Achalasia | +++ | - |
| Caustic injury to the esophagus | ++++ | - |
| Nonepidermolytic palmoplantar keratoderma (tylosis) | ++++ | - |
| Plummer–Vinson syndrome | ++++ | - |
| History of head and neck cancer | ++++ | - |
| Frequent consumption of extremely hot beverages | + | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shai, S.-E.; Lai, Y.-L.; Chang, C.-I.; Hsieh, C.-W. False Liver Metastasis by Positron Emission Tomography/Computed Tomography Scan after Chemoradiotherapy for Esophageal Cancer—Potential Overstaged Pitfalls of Treatment. Cancers 2024, 16, 948. https://doi.org/10.3390/cancers16050948
Shai S-E, Lai Y-L, Chang C-I, Hsieh C-W. False Liver Metastasis by Positron Emission Tomography/Computed Tomography Scan after Chemoradiotherapy for Esophageal Cancer—Potential Overstaged Pitfalls of Treatment. Cancers. 2024; 16(5):948. https://doi.org/10.3390/cancers16050948
Chicago/Turabian StyleShai, Sen-Ei, Yi-Ling Lai, Chen-I Chang, and Chi-Wei Hsieh. 2024. "False Liver Metastasis by Positron Emission Tomography/Computed Tomography Scan after Chemoradiotherapy for Esophageal Cancer—Potential Overstaged Pitfalls of Treatment" Cancers 16, no. 5: 948. https://doi.org/10.3390/cancers16050948