
Achieving Textbook Outcomes after Laparoscopic Resection in Posterosuperior Segments of the Liver: The Impact of the Learning Curve

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Definitions
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
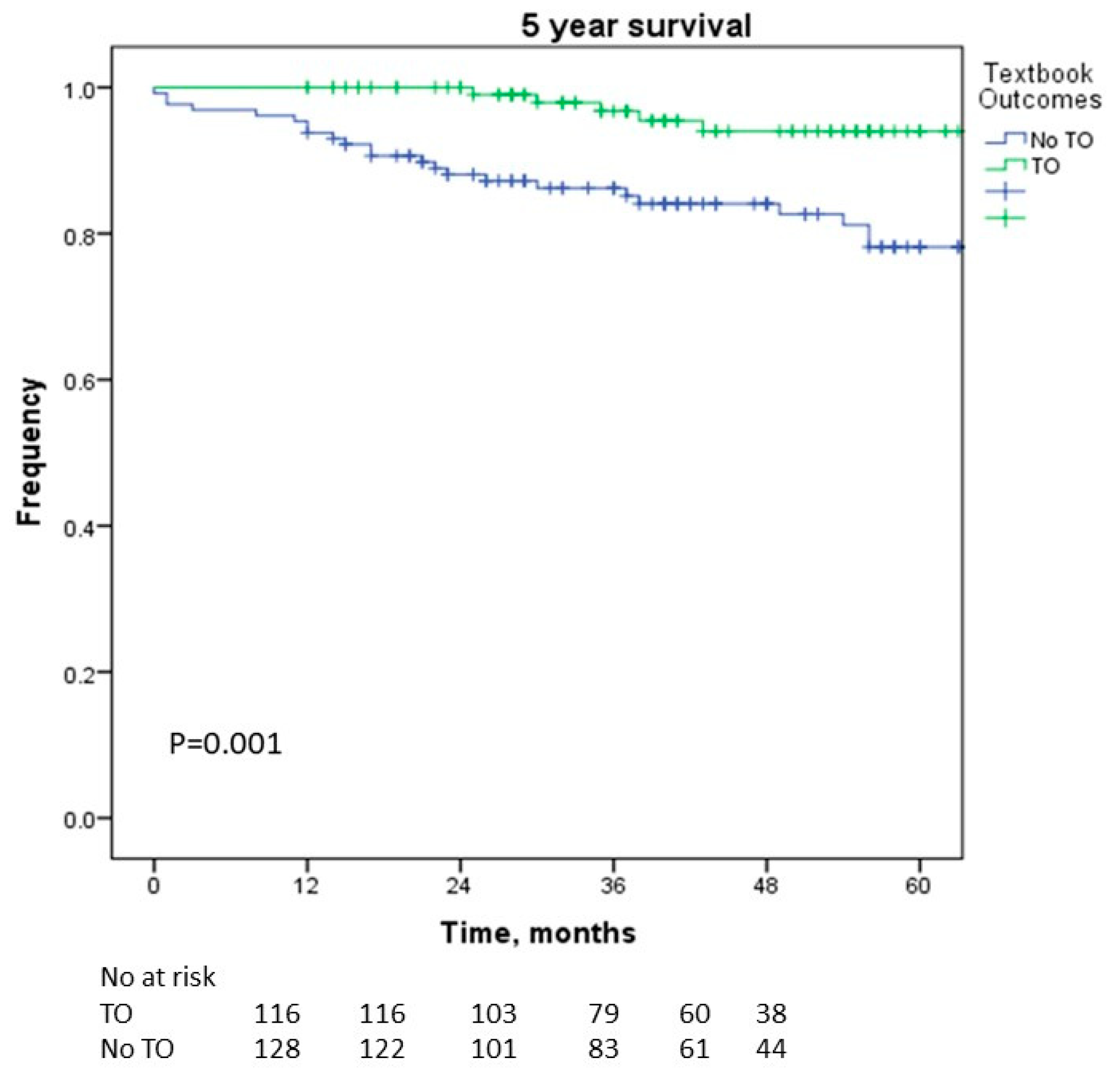
3.2. Factors Associated with Survival
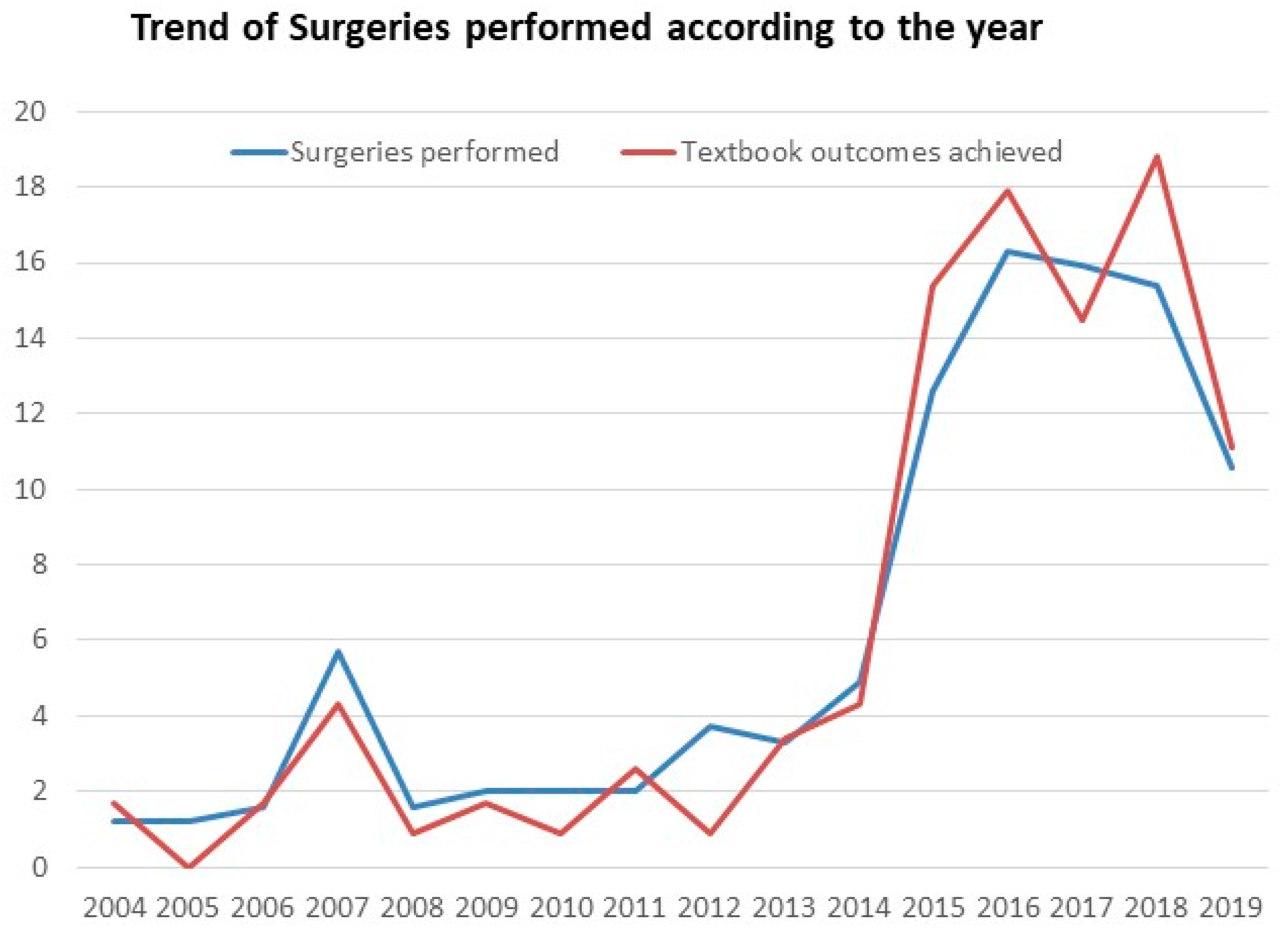
3.3. Learning Curve
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ibrahim, A.M.; Dimick, J.B. What Metrics Accurately Reflect Surgical Quality? Annu. Rev. Med. 2018, 69, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Dimick, J.B.; Birkmeyer, N.J. Measuring the quality of surgical care: Structure, process, or outcomes? J. Am. Coll. Surg. 2004, 198, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Denbo, J.; Anaya, D.A. Textbook Outcomes Following Liver Resection for Cancer: A New Standard for Quality Benchmarking and Patient Decision Making. Ann. Surg. Oncol. 2020, 27, 3118–3120. [Google Scholar] [CrossRef] [PubMed]
- Roemer, M.I.; Moustafa, A.T.; Hopkins, C.E. A proposed hospital quality index: Hospital death rates adjusted for case severity. Health Serv. Res. 1968, 3, 96–118. [Google Scholar]
- Kim, B.H.; Lee, D.; Jung, K.-W.; Won, Y.-J.; Cho, H. Cause of death and cause-specific mortality for primary liver cancer in South Korea: A nationwide population-based study in hepatitis B virus-endemic area. Clin. Mol. Hepatol. 2022, 28, 242–253. [Google Scholar] [CrossRef]
- Rajendran, L.; Ivanics, T.; Claasen, M.P.; Muaddi, H.; Sapisochin, G. The management of post-transplantation recurrence of hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 1–16. [Google Scholar] [CrossRef]
- Hong, S.Y.; Kang, M.J.; Kim, T.; Jung, K.-W.; Kim, B.-W. Incidence, mortality, and survival of liver cancer using Korea central cancer registry database: 1999–2019. Ann. Hepato-Biliary-Pancreat. Surg. 2022, 26, 211–219. [Google Scholar] [CrossRef]
- Morise, Z.; Wakabayashi, G. First quarter century of laparoscopic liver resection. World J. Gastroenterol. 2017, 23, 3581–3588. [Google Scholar] [CrossRef]
- Guro, H.; Cho, J.Y.; Han, H.-S.; Yoon, Y.-S.; Choi, Y.; Kim, S.; Kim, K.; Hyun, I.G. Outcomes of major laparoscopic liver resection for hepatocellular carcinoma. Surg. Oncol. 2018, 27, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Cherqui, D.; Ciria, R.; Kwon, C.H.D.; Kim, K.-H.; Broering, D.; Wakabayashi, G.; Samstein, B.; Troisi, R.I.; Han, H.S.; Rotellar, F.; et al. Expert Consensus Guidelines on Minimally Invasive Donor Hepatectomy for Living Donor Liver Transplantation From Innovation to Implementation. Ann. Surg. 2021, 273, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Dokmak, S.; Cauchy, F.; Sepulveda, A.; Choinier, P.M.; Dondéro, F.; Aussilhou, B.; Hego, C.; Chopinet, S.; Infantes, P.; Weiss, E.; et al. Laparoscopic Liver Transplantation. Ann. Surg. 2020, 272, 889–893. [Google Scholar] [CrossRef]
- Machairas, N.; Prodromidou, A.; Kostakis, I.D.; Spartalis, E.; Sotiropoulos, G.C. Safety and Efficacy of Laparoscopic Liver Resection for Lesions Located on Posterosuperior Segments: A Meta-Analysis of Short-term Outcomes. Surg. Laparosc. Endosc. Percutaneous Tech. 2018, 28, 203–208. [Google Scholar] [CrossRef]
- Abu Hilal, M.; Tschuor, C.; Kuemmerli, C.; López-Ben, S.; Lesurtel, M.; Rotellar, F. Laparoscopic posterior segmental resections: How I do it: Tips and pitfalls. Int. J. Surg. 2020, 82, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Korean Liver Cancer Association (KLCA) and National Cancer Center (NCC) Korea. 2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma. Clin. Mol. Hepatol. 2022, 28, 583–705. [Google Scholar] [CrossRef]
- Morise, Z. Laparoscopic liver resection for posterosuperior tumors using caudal approach and postural changes: A new technical approach. World J. Gastroenterol. 2016, 22, 10267–10274. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.Y.; Han, H.-S.; Yoon, Y.-S.; Shin, S.-H. Experiences of laparoscopic liver resection including lesions in the posterosuperior segments of the liver. Surg. Endosc. 2008, 22, 2344–2349. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.; Han, H.; Yoon, Y.; Cho, J.Y.; Choi, Y.; Shin, H.K. Role of intercostal trocars on laparoscopic liver resection for tumors in segments 7 and 8. J. Hepato-Biliary-Pancreat. Sci. 2014, 21, E65–E68. [Google Scholar] [CrossRef]
- Troisi, R.I.; Montalti, R.; Van Limmen, J.G.; Cavaniglia, D.; Reyntjens, K.; Rogiers, X.; De Hemptinne, B. Risk factors and management of conversions to an open approach in laparoscopic liver resection: Analysis of 265 consecutive cases. HPB 2014, 16, 75–82. [Google Scholar] [CrossRef]
- Mownah, O.A.; Aroori, S. The Pringle maneuver in the modern era: A review of techniques for hepatic inflow occlusion in minimally invasive liver resection. Ann. Hepato-Biliary-Pancreat. Surg. 2023, 27, 131–140. [Google Scholar] [CrossRef]
- Hobeika, C.; Fuks, D.; Cauchy, F.; Goumard, C.; Gayet, B.; Laurent, A.; Soubrane, O.; Salamé, E.; Cherqui, D.; Regimbeau, J.-M.; et al. Benchmark performance of laparoscopic left lateral sectionectomy and right hepatectomy in expert centers. J. Hepatol. 2020, 73, 1100–1108. [Google Scholar] [CrossRef]
- D’Silva, M.; Cho, J.Y.; Han, H.; Yoon, Y.; Lee, H.W.; Lee, J.S.; Lee, B.; Kim, M.; Jo, Y. Association between achieving textbook outcomes and better survival after laparoscopic liver resection in the anterolateral segments in patients with hepatocellular carcinoma. J. Hepato-Biliary-Pancreat. Sci. 2022, 29, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Görgec, B.; Cacciaguerra, A.B.; Lanari, J.; Russolillo, N.; Cipriani, F.; Aghayan, D.; Zimmitti, G.; Efanov, M.; Alseidi, A.; Mocchegiani, F.; et al. Assessment of Textbook Outcome in Laparoscopic and Open Liver Surgery. JAMA Surg. 2021, 156, e212064. [Google Scholar] [CrossRef] [PubMed]
- Sandri, G.B.L.; Spoletini, G.; Vennarecci, G.; Francone, E.; Abu Hilal, M.; Ettorre, G.M. Laparoscopic liver resection for large HCC: Short- and long-term outcomes in relation to tumor size. Surg. Endosc. 2018, 32, 4772–4779. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.Y.; Han, H.-S.; Yoon, Y.-S.; Shin, S.-H. Feasibility of laparoscopic liver resection for tumors located in the posterosuperior segments of the liver, with a special reference to overcoming current limitations on tumor location. Surgery 2008, 144, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Berardi, G.; Aghayan, D.; Fretland, A.; Elberm, H.; Cipriani, F.; Spagnoli, A.; Montalti, R.; Ceelen, W.P.; Aldrighetti, L.; Abu Hilal, M.; et al. Multicentre analysis of the learning curve for laparoscopic liver resection of the posterosuperior segments. Br. J. Surg. 2019, 106, 1512–1522. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.M.; Geller, D.A. What is the Learning Curve for Laparoscopic Major Hepatectomy? J. Gastrointest. Surg. 2016, 20, 1065–1071. [Google Scholar] [CrossRef]
- Sultana, A.; Nightingale, P.; Marudanayagam, R.; Sutcliffe, R.P. Evaluating the learning curve for laparoscopic liver resection: A comparative study between standard and learning curve CUSUM. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2019, 21, 1505–1512. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Sahara, K.; Moris, D.; Mehta, R.; Paredes, A.Z.; Ratti, F.; Marques, H.P.; Soubrane, O.; Lam, V.; Poultsides, G.A.; et al. Assessing Textbook Outcomes Following Liver Surgery for Primary Liver Cancer Over a 12-Year Time Period at Major Hepatobiliary Centers. Ann. Surg. Oncol. 2020, 27, 3318–3327. [Google Scholar] [CrossRef]
- Tsilimigras, D.I.; Mehta, R.; Merath, K.; Bagante, F.; Paredes, A.Z.; Farooq, A.; Ratti, F.; Marques, H.P.; Silva, S.; Soubrane, O.; et al. Hospital variation in Textbook Outcomes following curative-intent resection of hepatocellular carcinoma: An international multi-institutional analysis. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2020, 22, 1305–1313. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| TO a Achieved (n = 117) | TO Not Achieved (n = 129) | p-Value | |
|---|---|---|---|
| Age | 0.026 | ||
| ≤65 years | 84 (71.8) | 75 (58.1) | |
| >65 years | 33 (28.2) | 54 (41.9) | |
| Sex | 0.860 | ||
| Male | 90 (76.9) | 98 (76) | |
| Female | 27 (23.1) | 31 (24) | |
| BMI b | 0.006 | ||
| <25 kg/m2 | 51 (43.6) | 79 (61.2) | |
| ≥25 kg/m2 | 66 (56.4) | 50 (38.8) | |
| Hypertension | 53 (45.3) | 58 (45) | 0.958 |
| Diabetes mellitus | 32 (27.4) | 36 (27.9) | 0.922 |
| Alcohol | 50 (42.7) | 39 (30.2) | 0.042 |
| Smoking | 43 (36.8) | 31 (24.0) | 0.031 |
| Child—Pugh | 0.057 | ||
| A | 114 (97.4) | 118 (91.5) | |
| B | 3 (2.6) | 11 (8.5) | |
| MELD c | 5 (4.3) | 11 (8.5) | 0.198 |
| Tumor size | 0.001 | ||
| ≤3 cm | 85 (72.6) | 67 (51.9) | |
| >3 cm | 32 (27.4) | 62 (48.1) | |
| T stage | 0.013 | ||
| T1–2 | 112 (95.7) | 111 (86) | |
| T3–4 | 5 (4.3) | 18 (14) | |
| Pathological cirrhosis | 66 (56.4) | 78 (60.5) | 0.519 |
| Operation time | <0.001 | ||
| ≤280 min | 84 (71.8) | 42 (32.6) | |
| >280 min | 33 (28.2) | 87 (67.4) | |
| EBL d | <0.001 | ||
| ≤500 mL | 89 (76.1) | 47 (36.4) | |
| >500 mL | 28 (23.9) | 82 (63.6) | |
| Thrombocytopenia | 7 (6.0) | 17 (13.2) | 0.064 |
| Hypoalbuminemia | 8 (6.8) | 23 (17.8) | 0.012 |
| Pringle maneuver | 61 (52.1) | 62 (48.1) | 0.523 |
| Type of resection | 0.002 | ||
| Minor | 103 (88.0) | 93 (72.1) | |
| Major | 14 (12.0) | 36 (27.9) | |
| Anatomical resection | 48 (41.0) | 80 (62.0) | 0.001 |
| Mortality | 6 (5.1) | 30 (23.3) | <0.001 |
| p-Value | OR a | 95% CI b | |
|---|---|---|---|
| Obesity | 0.001 | 2.933 | 1.516–5.677 |
| Operation time | <0.001 | 3.870 | 1.900–7.881 |
| EBLc | <0.001 | 5.663 | 2.743–11.691 |
| Hypoalbuminemia | 0.003 | 4.903 | 1.737–13.843 |
| Major resection | 0.046 | 2.424 | 1.016–5.785 |
| p-Value | OR a | 95.0% CI b | ||
|---|---|---|---|---|
| Lower | Upper | |||
| BMI c > 25 kg/m2 | 0.020 | 2.889 | 1.182 | 7.062 |
| Age > 65 years | 0.049 | 2.046 | 1.004 | 4.172 |
| TO d not achieved | 0.024 | 3.009 | 1.154 | 7.841 |
| Factor | Before 2015 | After 2015 | p-Value |
|---|---|---|---|
| Transfusion | 21 (29.2) | 41 (23.6) | 0.358 |
| Readmission | 3 (4.2) | 8 (4.6) | 0.882 |
| R1 margins | 2 (2.8) | 10 (5.7) | 0.336 |
| LOS a > 7 days | 43 (59.7) | 59 (33.9) | <0.001 |
| Major complication | 10 (13.9) | 28 (16.1) | 0.664 |
| 30-day mortality | 0 | 3 (1.7) | 0.999 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Silva, M.; Cho, J.-Y.; Han, H.-S.; Yoon, Y.-S.; Lee, H.-W.; Lee, B.-R.; Kang, M.-Y.; Park, Y.-S.; Kim, J.-J. Achieving Textbook Outcomes after Laparoscopic Resection in Posterosuperior Segments of the Liver: The Impact of the Learning Curve. Cancers 2024, 16, 930. https://doi.org/10.3390/cancers16050930
D’Silva M, Cho J-Y, Han H-S, Yoon Y-S, Lee H-W, Lee B-R, Kang M-Y, Park Y-S, Kim J-J. Achieving Textbook Outcomes after Laparoscopic Resection in Posterosuperior Segments of the Liver: The Impact of the Learning Curve. Cancers. 2024; 16(5):930. https://doi.org/10.3390/cancers16050930
Chicago/Turabian StyleD’Silva, Mizelle, Jai-Young Cho, Ho-Seong Han, Yoo-Seok Yoon, Hae-Won Lee, Bo-Ram Lee, Mee-Young Kang, Ye-Shong Park, and Jin-Ju Kim. 2024. "Achieving Textbook Outcomes after Laparoscopic Resection in Posterosuperior Segments of the Liver: The Impact of the Learning Curve" Cancers 16, no. 5: 930. https://doi.org/10.3390/cancers16050930