
Extra-Capsular Spread of Lymph Node Metastasis in Oral, Oropharyngeal and Hypopharyngeal Cancer: A Comparative Subsite Analysis

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Histopathology Analysis
2.3. Outcome Measurement
2.4. Statistical Analysis
3. Results
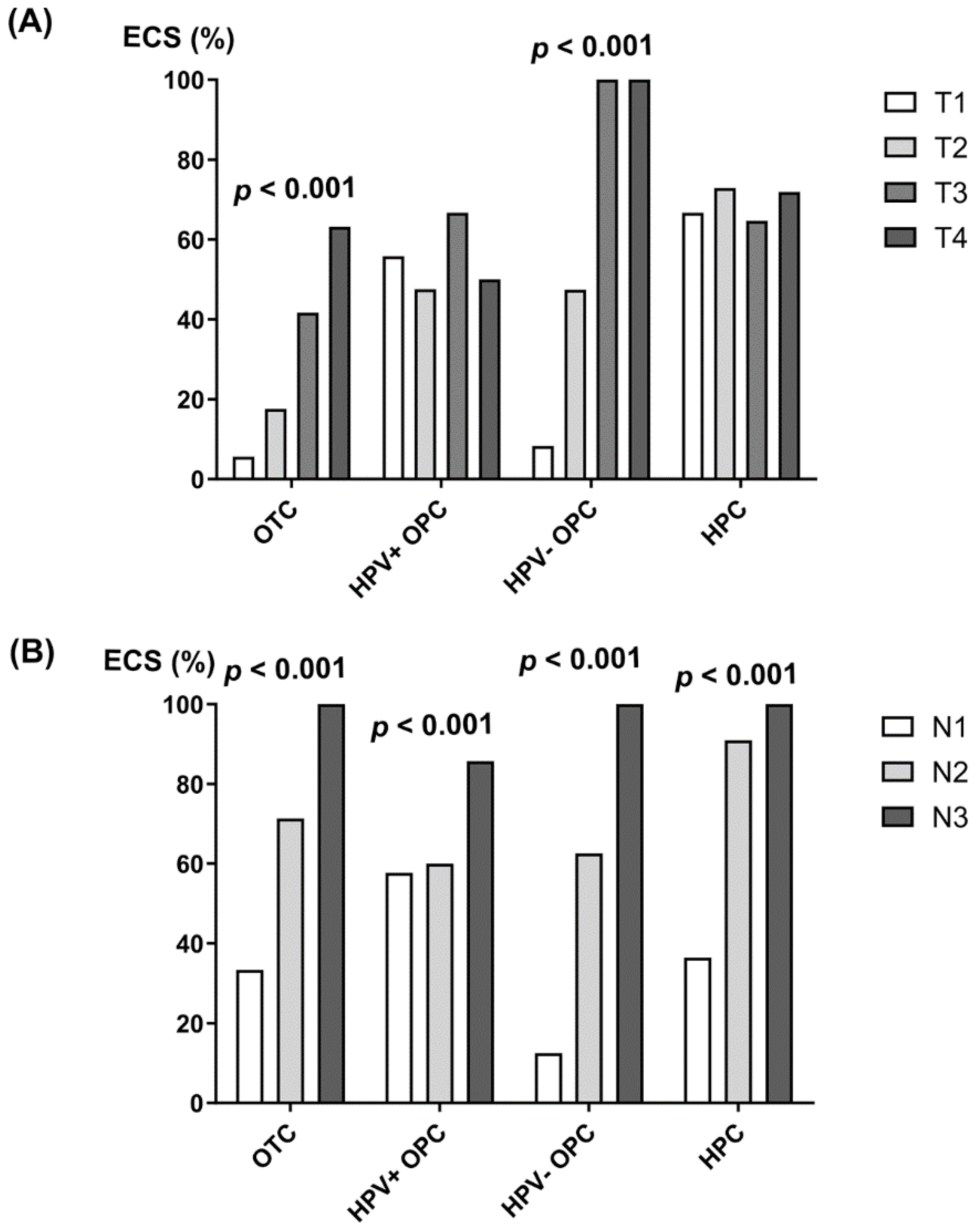
3.1. Clinical and Pathological Differences According to the Presence of ECS and Tumor Subsite
3.2. Univariable and Multivariable Analyses of Risk Factors for ECS
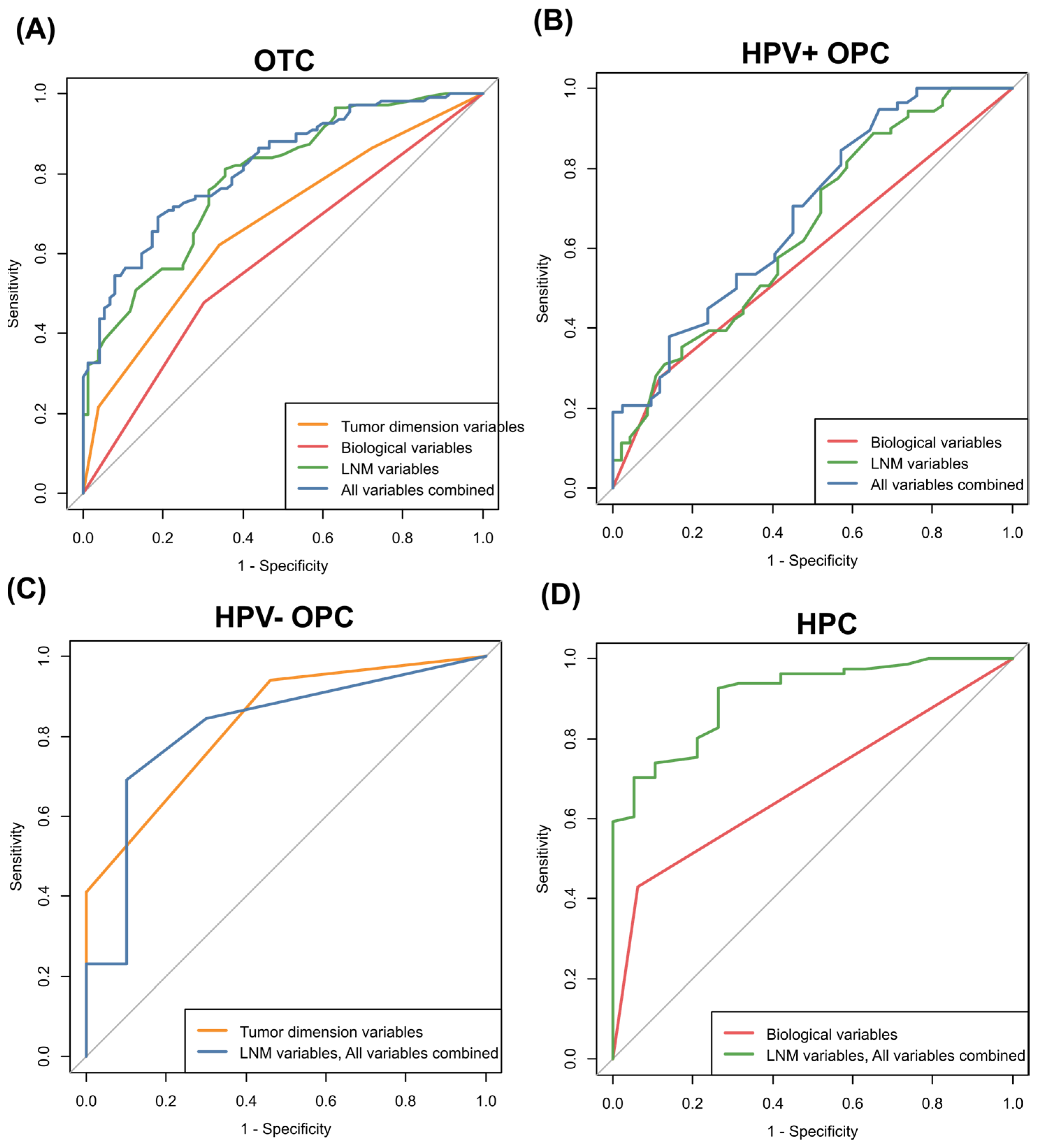
3.3. Predictability of ECS by ROC Curve Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| LNM | Lymph node metastasis |
| ECS | Extra-capsular spread |
| OTC | Oral tongue cancer |
| HPV | Human papillomavirus |
| OPC | Oropharyngeal cancer |
| HPC | Hypopharyngeal cancer |
| DOI | Depth of invasion |
| WPOI | Worst pattern of invasion |
| PNI | Perineural invasion |
| LVI | Lymphovascular invasion |
| ROC | Receiver operating characteristics |
| AUC | Area under the curve |
| LOOCV | Leave-one-out cross-validation |
References
- Abdel-Halim, C.N.; Rosenberg, T.; Larsen, S.R.; Hoilund-Carlsen, P.F.; Sorensen, J.A.; Rohde, M.; Godballe, C. Histopathological Definitions of Extranodal Extension: A Systematic Review. Head Neck Pathol. 2021, 15, 599–607. [Google Scholar] [CrossRef]
- Dobi, E.; Bazan, F.; Dufresne, A.; Demarchi, M.; Villanueva, C.; Chaigneau, L.; Montcuquet, P.; Ivanaj, A.; Sautiere, J.L.; Maisonnette-Escot, Y.; et al. Is extracapsular tumour spread a prognostic factor in patients with early breast cancer? Int. J. Clin. Oncol. 2013, 18, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Alakus, H.; Holscher, A.H.; Grass, G.; Hartmann, E.; Schulte, C.; Drebber, U.; Baldus, S.E.; Bollschweiler, E.; Metzger, R.; Monig, S.P. Extracapsular lymph node spread: A new prognostic factor in gastric cancer. Cancer 2010, 116, 309–315. [Google Scholar] [CrossRef]
- Bhattacharya, P.; Mukherjee, R. Lymph node extracapsular extension as a marker of aggressive phenotype: Classification, prognosis and associated molecular biomarkers. Eur. J. Surg. Oncol. 2021, 47, 721–731. [Google Scholar] [CrossRef] [PubMed]
- Lo, M.; Robinson, A.; Wade, R.; Peach, H.; Dewar, D.; Heaton, M.; Moncrieff, M. Extracapsular Spread in Melanoma Lymphadenopathy: Prognostic Implications, Classification, and Management. Ann. Surg. Oncol. 2021, 28, 1642–1653. [Google Scholar] [CrossRef] [PubMed]
- Alvi, A.; Johnson, J.T. Extracapsular spread in the clinically negative neck (N0): Implications and outcome. Otolaryngol. Head Neck Surg. 1996, 114, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Bernier, J.; Cooper, J.S.; Pajak, T.F.; van Glabbeke, M.; Bourhis, J.; Forastiere, A.; Ozsahin, E.M.; Jacobs, J.R.; Jassem, J.; Ang, K.K.; et al. Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck 2005, 27, 843–850. [Google Scholar] [PubMed]
- Cooper, J.S.; Zhang, Q.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Long-term follow-up of the RTOG 9501/intergroup phase III trial: Postoperative concurrent radiation therapy and chemotherapy in high-risk squamous cell carcinoma of the head and neck. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 1198–1205. [Google Scholar] [CrossRef]
- Morey, T.; Hodge, J.C.; Stern, C.; Krishnan, S.; Foreman, A. Correlation between radiologic and pathologic extranodal extension in HPV-associated oropharyngeal cancer: Systematic review. Head Neck 2022, 44, 2875–2885. [Google Scholar] [CrossRef]
- Matsumoto, F.; Mori, T.; Matsumura, S.; Matsumoto, Y.; Fukasawa, M.; Teshima, M.; Kobayashi, K.; Yoshimoto, S. Prognostic significance of surgical extranodal extension in head and neck squamous cell carcinoma patients. Jpn. J. Clin. Oncol. 2017, 47, 699–704. [Google Scholar] [CrossRef]
- Chatterjee, D.; Bansal, V.; Malik, V.; Bhagat, R.; Punia, R.S.; Handa, U.; Gupta, A.; Dass, A. Tumor Budding and Worse Pattern of Invasion Can Predict Nodal Metastasis in Oral Cancers and Associated with Poor Survival in Early-Stage Tumors. Ear Nose Throat J. 2019, 98, E112–E119. [Google Scholar] [CrossRef]
- Tirelli, G.; Tofanelli, M.; Sacchet, E.; Bussani, R.; Shafiei, V.; Gatto, A.; Boscolo-Rizzo, P.; Gardenal, N. Extranodal extension in head and neck squamous cell cancer: Is there a role for further stratification? Br. J. Oral. Maxillofac. Surg. 2021, 59, 567–572. [Google Scholar] [CrossRef]
- Doescher, J.; Veit, J.A.; Hoffmann, T.K. The 8th edition of the AJCC Cancer Staging Manual: Updates in otorhinolaryngology, head and neck surgery. HNO 2017, 65, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.H.; O’Sullivan, B. Overview of the 8th Edition TNM Classification for Head and Neck Cancer. Curr. Treat. Options Oncol. 2017, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-T.; Lee, L.-Y.; Hsueh, C.; Lin, C.-Y.; Fan, K.-H.; Wang, H.-M.; Hsieh, C.-H.; Ng, S.-H.; Lin, C.-H.; Tsao, C.-K. Pathological risk factors stratification in pN3b oral cavity squamous cell carcinoma: Focus on the number of positive nodes and extranodal extension. Oral. Oncol. 2018, 86, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Puri, S.K.; Fan, C.-Y.; Hanna, E. Significance of extracapsular lymph node metastases in patients with head and neck squamous cell carcinoma. Curr. Opin. Otolaryngol. Head Neck Surg. 2003, 11, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Suton, P.; Salaric, I.; Granic, M.; Mueller, D.; Luksic, I. Prognostic significance of extracapsular spread of lymph node metastasis from oral squamous cell carcinoma in the clinically negative neck. Int. J. Oral. Maxillofac. Surg. 2017, 46, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, J.H.; Ferris, R.L.; Gooding, W.; Cunningham, D.; Mehta, V.; Kim, S.; Myers, E.N.; Johnson, J.; Chiosea, S. Extracapsular spread in head and neck carcinoma: Impact of site and human papillomavirus status. Cancer 2013, 119, 3302–3308. [Google Scholar] [CrossRef] [PubMed]
- Quinton, B.A.; Cabrera, C.I.; Tamaki, A.; Li, S.; Fowler, N.; Rezaee, R.; Lavertu, P.; Teknos, T.; Pan, Q.; Thuener, J. The impact of microscopic versus macroscopic extranodal extension in oral cavity squamous cell carcinoma: National cancer database analysis and review of the literature. Am. J. Otolaryngol. 2022, 43, 103511. [Google Scholar] [CrossRef]
- Kharytaniuk, N.; Molony, P.; Boyle, S.; O’Leary, G.; Werner, R.; Heffron, C.; Feeley, L.; Sheahan, P. Association of Extracapsular Spread With Survival According to Human Papillomavirus Status in Oropharynx Squamous Cell Carcinoma and Carcinoma of Unknown Primary Site. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 683–690. [Google Scholar] [CrossRef]
- An, Y.; Park, H.S.; Kelly, J.R.; Stahl, J.M.; Yarbrough, W.G.; Burtness, B.A.; Contessa, J.N.; Decker, R.H.; Koshy, M.; Husain, Z.A. The prognostic value of extranodal extension in human papillomavirus-associated oropharyngeal squamous cell carcinoma. Cancer 2017, 123, 2762–2772. [Google Scholar] [CrossRef]
- Zhan, K.Y.; Eskander, A.; Kang, S.Y.; Old, M.O.; Ozer, E.; Agrawal, A.A.; Carrau, R.L.; Rocco, J.W.; Teknos, T.N. Appraisal of the AJCC 8th edition pathologic staging modifications for HPV-positive oropharyngeal cancer, a study of the National Cancer Data Base. Oral. Oncol. 2017, 73, 152–159. [Google Scholar] [CrossRef]
- Meyer, M.F.; Meinrath, J.; Seehawer, J.; Lechner, A.; Odenthal, M.; Quaas, A.; Semrau, R.; Huebbers, C.U.; Marnitz, S.; Buttner, R.; et al. The relevance of the lymph node ratio as predictor of prognosis is higher in HPV-negative than in HPV-positive oropharyngeal squamous cell carcinoma. Clin. Otolaryngol. 2018, 43, 192–198. [Google Scholar] [CrossRef]
- Beltz, A.; Gosswein, D.; Zimmer, S.; Limburg, I.; Wunsch, D.; Gribko, A.; Deichelbohrer, M.; Hagemann, J.; Stauber, R.H.; Kunzel, J. Staging of oropharyngeal squamous cell carcinoma of the head and neck: Prognostic features and power of the 8th edition of the UICC staging manual. Eur. J. Surg. Oncol. 2019, 45, 1046–1053. [Google Scholar] [CrossRef]
- Beltz, A.; Zimmer, S.; Michaelides, I.; Evert, K.; Psychogios, G.; Bohr, C.; Kunzel, J. Significance of Extranodal Extension in Surgically Treated HPV-Positive Oropharyngeal Carcinomas. Front. Oncol. 2020, 10, 1394. [Google Scholar] [CrossRef]
- Gal, T.J.; O’Brien, K.J.; Chen, Q.; Huang, B. Clinical vs Microscopic Extranodal Extension and Survival in Oropharyngeal Carcinoma in the Human Papillomavirus Era. Otolaryngol. Head Neck Surg. 2020, 162, 693–701. [Google Scholar] [CrossRef] [PubMed]
- Mermod, M.; Tolstonog, G.; Simon, C.; Monnier, Y. Extracapsular spread in head and neck squamous cell carcinoma: A systematic review and meta-analysis. Oral. Oncol. 2016, 62, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Steinhart, H.; Schroeder, H.G.; Buchta, B.; Schmidt, A.; Kleinsasser, O. Prognostic significance of extra-capsular invasion in cervical lymph node metastases of squamous epithelial carcinoma. Laryngorhinootologie 1994, 73, 620–625. [Google Scholar] [CrossRef] [PubMed]
- Imre, K.; Pinar, E.; Oncel, S.; Calli, C.; Tatar, B. Predictors of extracapsular spread in lymph node metastasis. Eur. Arch. Otorhinolaryngol. 2008, 265, 337–339. [Google Scholar] [CrossRef]
- Pinsolle, J.; Pinsolle, V.; Majoufre, C.; Duroux, S.; Demeaux, H.; Siberchicot, F. Prognostic value of histologic findings in neck dissections for squamous cell carcinoma. Arch. Otolaryngol. Head Neck Surg. 1997, 123, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Michikawa, C.; Uzawa, N.; Sato, H.; Ohyama, Y.; Okada, N.; Amagasa, T. Epidermal growth factor receptor gene copy number aberration at the primary tumour is significantly associated with extracapsular spread in oral cancer. Br. J. Cancer 2011, 104, 850–855. [Google Scholar] [CrossRef]
- Coatesworth, A.P.; MacLennan, K. Squamous cell carcinoma of the upper aerodigestive tract: The prevalence of microscopic extracapsular spread and soft tissue deposits in the clinically N0 neck. Head. Neck 2002, 24, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Carter, R.L.; Barr, L.C.; O’Brien, C.J.; Soo, K.C.; Shaw, H.J. Transcapsular spread of metastatic squamous cell carcinoma from cervical lymph nodes. Am. J. Surg. 1985, 150, 495–499. [Google Scholar] [CrossRef]
- Brannan, A.G.; Johnstone, P.A.; Cooper, J. Extracapsular tumor extension in cervical lymph nodes: Reconciling the literature and seer data. Head. Neck 2011, 33, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Noda, Y.; Ishida, M.; Ueno, Y.; Fujisawa, T.; Iwai, H.; Tsuta, K. Novel pathological predictive factors for extranodal extension in oral squamous cell carcinoma: A retrospective cohort study based on tumor budding, desmoplastic reaction, tumor-infiltrating lymphocytes, and depth of invasion. BMC Cancer 2022, 22, 402. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.Y.; Kim, M.J.; Ryu, G.; Choi, N.; Ko, Y.H.; Jeong, H.S. Prediction of Lymph Node Metastasis by Tumor Dimension Versus Tumor Biological Properties in Head and Neck Squamous Cell Carcinomas. Cancer Res. Treat. 2016, 48, 54–62. [Google Scholar] [CrossRef]
- Wenzel, S.; Sagowski, C.; Kehrl, W.; Metternich, F. The prognostic impact of metastatic pattern of lymph nodes in patients with oral and oropharyngeal squamous cell carcinomas. Eur. Arch. Oto-Rhino-Laryngol. Head Neck 2004, 261, 270–275. [Google Scholar]
- Yasuda, M.; Chiodo, C.; Lilley, C.; Mehrotra, S.; Ananthanarayanan, V.; Ziegler, A.; Thorpe, E. Relationship Between Worst Pattern of Invasion and Extranodal Extension in Oral Tongue Squamous Cell Carcinomas. Head Neck Pathol. 2023, 17, 460–466. [Google Scholar] [CrossRef]
- Tandon, S.; Bera, R.N.; Singh, A.K.; Mishra, M. Predictors of Extracapsular Spread in T1/T2 Oral Squamous Cell Carcinoma: A retrospective study. J. Oral Biol. Craniofacial Res. 2022, 12, 449–453. [Google Scholar] [CrossRef]
- Singh, A.K.; Bera, R.N.; Anandkumar, J.; Krishnan, A.; Rajpoot, R. Primary Tumour Characteristics Poorly Correlate with Extracapsular Spread and Cervical Sublevel IIb Metastasis in Patients with Oral Squamous Cell Carcinoma and Clinically N0 Neck: A Retrospective Study. Ann. Maxillofac. Surg. 2021, 11, 274–279. [Google Scholar]
- Caudell, J.J.; Gillison, M.L.; Maghami, E.; Spencer, S.; Pfister, D.G.; Adkins, D.; Birkeland, A.C.; Brizel, D.M.; Busse, P.M.; Cmelak, A.J.; et al. NCCN Guidelines(R) Insights: Head and Neck Cancers, Version 1.2022. J. Natl. Compr. Canc Netw. 2022, 20, 224–234. [Google Scholar] [CrossRef]
- Machiels, J.P.; Rene Leemans, C.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef]
- Huang, S.H.; Chernock, R.; O’Sullivan, B.; Fakhry, C. Assessment Criteria and Clinical Implications of Extranodal Extension in Head and Neck Cancer. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, 265–278. [Google Scholar] [CrossRef]
- Almangush, A.; Bello, I.O.; Keski-Santti, H.; Makinen, L.K.; Kauppila, J.H.; Pukkila, M.; Hagstrom, J.; Laranne, J.; Tommola, S.; Nieminen, O.; et al. Depth of invasion, tumor budding, and worst pattern of invasion: Prognostic indicators in early-stage oral tongue cancer. Head. Neck 2014, 36, 811–818. [Google Scholar] [CrossRef]
- Mamic, M.; Lucijanic, M.; Manojlovic, L.; Muller, D.; Suton, P.; Luksic, I. Prognostic significance of extranodal extension in oral cavity squamous cell carcinoma with occult neck metastases. Int. J. Oral Maxillofac. Surg. 2021, 50, 309–315. [Google Scholar] [CrossRef]
- Peng, C.H.; Liao, C.T.; Peng, S.C.; Chen, Y.J.; Cheng, A.J.; Juang, J.L.; Tsai, C.Y.; Chen, T.C.; Chuang, Y.J.; Tang, C.Y.; et al. A novel molecular signature identified by systems genetics approach predicts prognosis in oral squamous cell carcinoma. PLoS ONE 2011, 6, e23452. [Google Scholar] [CrossRef] [PubMed]
- Jithesh, P.V.; Risk, J.M.; Schache, A.G.; Dhanda, J.; Lane, B.; Liloglou, T.; Shaw, R.J. The epigenetic landscape of oral squamous cell carcinoma. Br. J. Cancer 2013, 108, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.M.; Kim, H.J.; Koo, B.S.; Rha, K.S.; Yoon, Y.H. Expression of matrix metalloproteinase-12 is correlated with extracapsular spread of tumor from nodes with metastasis in head and neck squamous cell carcinoma. Eur. Arch. Otorhinolaryngol. 2013, 270, 1137–1142. [Google Scholar] [CrossRef]
- Chien, C.Y.; Chuang, H.C.; Chen, C.H.; Fang, F.M.; Chen, W.C.; Huang, C.C.; Huang, H.Y. The expression of activin receptor-like kinase 1 among patients with head and neck cancer. Otolaryngol. Head Neck Surg. 2013, 148, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Dhanda, J.; Triantafyllou, A.; Liloglou, T.; Kalirai, H.; Lloyd, B.; Hanlon, R.; Shaw, R.J.; Sibson, D.R.; Risk, J.M. SERPINE1 and SMA expression at the invasive front predict extracapsular spread and survival in oral squamous cell carcinoma. Br. J. Cancer 2014, 111, 2114–2121. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Lim, W.K.; Leong, H.S.; Chong, F.T.; Lim, T.K.; Tan, D.S.; Teh, B.T.; Iyer, N.G. An eleven gene molecular signature for extra-capsular spread in oral squamous cell carcinoma serves as a prognosticator of outcome in patients without nodal metastases. Oral Oncol. 2015, 51, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.; Chang, K.P.; OuYang, C.N.; Kao, H.K.; Hsueh, C.; Chen, L.C.; Cheng, H.Y.; Liang, Y.; Liou, W.; Liang, C.L.; et al. ASC contributes to metastasis of oral cavity squamous cell carcinoma. Oncotarget 2016, 7, 50074–50085. [Google Scholar] [CrossRef]
- Liao, C.T.; Chen, S.J.; Lee, L.Y.; Hsueh, C.; Yang, L.Y.; Lin, C.Y.; Fan, K.H.; Wang, H.M.; Ng, S.H.; Lin, C.H.; et al. An Ultra-Deep Targeted Sequencing Gene Panel Improves the Prognostic Stratification of Patients With Advanced Oral Cavity Squamous Cell Carcinoma. Medicine 2016, 95, e2751. [Google Scholar] [CrossRef]
- Puram, S.V.; Tirosh, I.; Parikh, A.S.; Patel, A.P.; Yizhak, K.; Gillespie, S.; Rodman, C.; Luo, C.L.; Mroz, E.A.; Emerick, K.S.; et al. Single-Cell Transcriptomic Analysis of Primary and Metastatic Tumor Ecosystems in Head and Neck Cancer. Cell 2017, 171, 1611–1624.e1624. [Google Scholar] [CrossRef]
- Lyons, A.J.; Bateman, A.C.; Spedding, A.; Primrose, J.N.; Mandel, U. Oncofetal fibronectin and oral squamous cell carcinoma. Br. J. Oral Maxillofac. Surg. 2001, 39, 471–477. [Google Scholar] [CrossRef] [PubMed]
- Brennan, P.A.; Dennis, S.; Poller, D.; Quintero, M.; Puxeddu, R.; Thomas, G.J. Inducible nitric oxide synthase: Correlation with extracapsular spread and enhancement of tumor cell invasion in head and neck squamous cell carcinoma. Head Neck 2008, 30, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Mermod, M.; Bongiovanni, M.; Petrova, T.V.; Dubikovskaya, E.A.; Simon, C.; Tolstonog, G.; Monnier, Y. Correlation between podoplanin expression and extracapsular spread in squamous cell carcinoma of the oral cavity using subjective immunoreactivity scores and semiquantitative image analysis. Head Neck 2017, 39, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Temam, S.; Oh, M.; Pungpravat, N.; Huang, B.L.; Mao, L.; Wong, D.T. Global expression-based classification of lymph node metastasis and extracapsular spread of oral tongue squamous cell carcinoma. Neoplasia 2006, 8, 925–932. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.H.; Kuo, H.K.; Chang, K.W. The evolving transcriptome of head and neck squamous cell carcinoma: A systematic review. PLoS ONE 2008, 3, e3215. [Google Scholar] [CrossRef] [PubMed]
- Mroz, E.A.; Rocco, J.W. Gene expression analysis as a tool in early-stage oral cancer management. J. Clin. Oncol. 2012, 30, 4053–4055. [Google Scholar] [CrossRef] [PubMed]
- van Hooff, S.R.; Leusink, F.K.; Roepman, P.; Baatenburg de Jong, R.J.; Speel, E.J.; van den Brekel, M.W.; van Velthuysen, M.L.; van Diest, P.J.; van Es, R.J.; Merkx, M.A.; et al. Validation of a gene expression signature for assessment of lymph node metastasis in oral squamous cell carcinoma. J. Clin. Oncol. 2012, 30, 4104–4110. [Google Scholar] [CrossRef]
- Lee, H.R.; Roh, J.; Gu, G.Y.; Lee, J.H.; Shin, Y.S.; Jang, J.Y.; Kim, C.H. Differential expression of podoplanin in metastatic lymph node is associated with extranodal extension in oropharyngeal cancer. Sci. Rep. 2022, 12, 3665. [Google Scholar] [CrossRef]
- Pilborough, A.E.; Lambert, D.W.; Khurram, S.A. Extranodal extension in oral cancer: A role for the nodal microenvironment? J. Oral Pathol. Med. 2019, 48, 863–870. [Google Scholar] [CrossRef]
- Adel, M.; Kao, H.K.; Hsu, C.L.; Huang, J.J.; Lee, L.Y.; Huang, Y.; Browne, T.; Tsang, N.M.; Chang, Y.L.; Chang, K.P. Evaluation of Lymphatic and Vascular Invasion in Relation to Clinicopathological Factors and Treatment Outcome in Oral Cavity Squamous Cell Carcinoma. Medicine 2015, 94, e1510. [Google Scholar] [CrossRef] [PubMed]
- Pavlidis, N.; Pentheroudakis, G.; Plataniotis, G. Cervical lymph node metastases of squamous cell carcinoma from an unknown primary site: A favourable prognosis subset of patients with CUP. Clin. Transl. Oncol. 2009, 11, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Strojan, P.; Ferlito, A.; Medina, J.E.; Woolgar, J.A.; Rinaldo, A.; Robbins, K.T.; Fagan, J.J.; Mendenhall, W.M.; Paleri, V.; Silver, C.E.; et al. Contemporary management of lymph node metastases from an unknown primary to the neck: I. A review of diagnostic approaches. Head Neck 2013, 35, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Eskander, A.; Ghanem, T.; Agrawal, A.; Education Committee of American Head and Neck Society. AHNS Series: Do you know your guidelines? Guideline recommendations for head and neck cancer of unknown primary site. Head Neck 2018, 40, 614–621. [Google Scholar] [CrossRef] [PubMed]
- Su, Z.; Duan, Z.; Pan, W.; Wu, C.; Jia, Y.; Han, B.; Li, C. Predicting extracapsular spread of head and neck cancers using different imaging techniques: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Surg. 2016, 45, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Lewis Jr, J.S.; Carpenter, D.H.; Thorstad, W.L.; Zhang, Q.; Haughey, B.H. Extracapsular extension is a poor predictor of disease recurrence in surgically treated oropharyngeal squamous cell carcinoma. Mod. Pathol. 2011, 24, 1413–1420. [Google Scholar] [CrossRef]
- Greenberg, J.S.; Fowler, R.; Gomez, J.; Mo, V.; Roberts, D.; El Naggar, A.K.; Myers, J.N. Extent of extracapsular spread: A critical prognosticator in oral tongue cancer. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2003, 97, 1464–1470. [Google Scholar] [CrossRef]
- Wreesmann, V.B.; Katabi, N.; Palmer, F.L.; Montero, P.H.; Migliacci, J.C.; Goenen, M.; Carlson, D.; Ganly, I.; Shah, J.P.; Ghossein, R. Influence of extracapsular nodal spread extent on prognosis of oral squamous cell carcinoma. Head. Neck 2016, 38, E1192–E1199. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, J.P.; Kane, S.; Ghosh-Laskar, S.; Pilar, A.; Manik, V.; Oza, N.; Wagle, P.; Gupta, T.; Budrukkar, A.; Murthy, V. Extranodal extension in resected oral cavity squamous cell carcinoma: More to it than meets the eye. Laryngoscope 2019, 129, 1130–1136. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| OTC (n = 190) | HPV-Positive OPC (n = 118) | |||||
|---|---|---|---|---|---|---|
| No. (%) | ECS(+) (n = 113) | ECS(−) (n = 77) | p-value | ECS(+) (n = 72) | ECS(−) (n = 46) | p-value |
| Age (mean ± SD) | 55.0 ± 14.9 | 55.7 ± 13.6 | 0.534 | 57.0 ± 9.4 | 55.9 ± 9.4 | 0.577 |
| Sex (M:F) | 62:51 (54.9:45.1) | 46:31 (59.7: 40.3) | 0.605 | 63:9 (87.5:12.5) | 36:10 (78.3:21.7) | 0.282 |
| Tumor diameter (cm) | 3.0 | 2.8 | 0.010 | 2.1 | 2.1 | 0.650 |
| (median, [Q1–Q3]) | [2.2–4.5] | [1.8–3.3] | [1.5–2.9] | [1.4–2.6] | ||
| Tumor volume (cm3) (median, [Q1–Q3]) | 7.0 [2.0–11.6] | 3.2 [1.4–6.4] | 0.003 | 1.6 [0.5–4.8] | 1.3 [0.4–3.8] | 0.422 |
| DOI (mm) | (n = 111) | (n = 76) | 0.003 | (n = 37) | (n = 20) | 0.786 |
| DOI ≤ 5 | 30 (27.0) | 39 (51.3) | 10 (24.4) | 7 (29.2) | ||
| 5 < DOI ≤ 10 | 21 (18.9) | 12 (15.8) | 12 (29.3) | 6 (25.0) | ||
| 10 < DOI | 60 (54.1) | 25 (32.9) | 15 (36.6) | 7 (29.2) | ||
| T status | (n = 111) | (n = 76) | <0.001 | (n = 69) | (n = 45) | 0.720 |
| T0 | 4 (5.8) | 4 (8.9) | ||||
| T1 | 15 (13.5) | 21 (27.6) | 29 (42.0) | 16 (35.6) | ||
| T2 | 27 (24.3) | 29 (38.2) | 29 (42.0) | 23 (51.1) | ||
| T3 | 45 (40.5) | 23 (30.3) | 4 (5.8) | 1 (2.2) | ||
| T4 | 24 (21.6) | 3 (3.9) | 3 (4.3) | 1 (2.2) | ||
| LVI | (n = 110) | (n = 76) | 0.028 | (n = 58) | (n = 42) | 0.057 |
| Present | 38 (34.5) | 15 (19.7) | 16 (27.6) | 5 (11.9) | ||
| PNI | (n = 109) | (n = 76) | 0.017 | (n = 60) | (n = 42) | 0.078 |
| Present | 52 (47.7) | 23 (30.3) | 8 (13.3) | 1 (2.4) | ||
| WPOI | (n = 37) | (n = 25) | 0.880 | |||
| Present | 17 (45.9) | 11 (44.0) | ||||
| Histologic grade | (n = 107) | (n = 76) | 0.297 | (n = 36) | (n = 21) | 0.844 |
| WD | 39 (36.4) | 36 (47.4) | 1 (2.8) | 0 (0.0) | ||
| MD | 48 (44.9) | 30 (39.5) | 27 (75.0) | 15 (71.4) | ||
| PD | 20 (18.7) | 10 (13.2) | 8 (22.2) | 6 (28.6) | ||
| N status | <0.001 | 0.431 | ||||
| N1 | 23 (20.4) | 46 (10.1) | 15 (20.8) | 11 (23.9) | ||
| N2 | 77 (68.1) | 31 (6.8) | 51 (70.8) | 34 (73.9) | ||
| N3 | 13 (11.5) | 0 (0.0) | 6 (8.3) | 1 (2.2) | ||
| LNM number (median, [Q1–Q3]) | 2.0 [1.0–4.0] | 1.0 [1.0–2.0] | <0.001 | 2.0 [1.0–4.0] | 2.0 [1.0–3.0] | 0.068 |
| LNM largest node size (cm) (median, [Q1–Q3]) | 1.3 [0.9–1.9] | 0.9 [0.4–1.4] | <0.001 | 3.0 [2.3–4.5] | 2.5 [1.3–3.4] | 0.008 |
| HPV-negative OPC (n = 30) | HPC (n = 100) | |||||
| No. (%) | ECS(+) (n = 17) | ECS(−) (n = 13) | p-value | ECS(+) (n = 81) | ECS(−) (n = 19) | p-value |
| Age (mean ± SD) | 57.7 ± 10.1 | 60.6 ± 8.4 | 0.414 | 63.8 ± 9.0 | 65.2 ± 9.2 | 0.657 |
| Sex (M:F) | 16:1 (94.1:5.9) | 12:1 (92.3:7.7) | 0.999 | 79:2 (97.5:2.5) | 17:2 (89.5:10.5) | 0.336 |
| Tumor diameter (cm) | 2.9 | 2.5 | 0.395 | 3.0 | 2.7 | 0.692 |
| (median, [Q1–Q3]) | [2.2–3.5] | [1.6–2.9] | [2.2–4.5] | [2.2–4.1] | ||
| Tumor volume (cm3) (median, [Q1–Q3]) | 6.5 [0.7–11.4] | 3.2 [1.0–9.1] | 0.702 | 4.5 [1.3–12.5] | 4.4 [2.8–11.3] | 0.983 |
| DOI (mm) | (n = 11) | (n = 8) | 0.589 | (n = 33) | (n = 11) | 0.622 |
| DOI ≤ 5 | 2 (18.2) | 2 (25.0) | 11 (33.3) | 4 (36.4) | ||
| 5 < DOI ≤ 10 | 4 (36.4) | 1 (12.5) | 11 (33.3) | 5 (45.5) | ||
| 10 < DOI | 5 (45.5) | 5 (62.5) | 11 (33.3) | 2 (18.2) | ||
| T status | (n = 17) | (n = 13) | 0.004 | (n = 81) | (n = 18) | 0.570 |
| T0 | ||||||
| T1 | 1 (5.9) | 7 (53.8) | 12 (14.8) | 5 (27.8) | ||
| T2 | 9 (52.9) | 6 (46.2) | 35 (43.2) | 7 (38.9) | ||
| T3 | 6 (35.3) | 0 (0.0) | 11 (13.6) | 1 (5.6) | ||
| T4 | 1 (5.9) | 0 (0.0) | 23 (28.4) | 5 (27.8) | ||
| LVI | (n = 13) | (n = 10) | 0.402 | (n = 65) | (n = 16) | 0.006 |
| Present | 7 (53.8) | 3 (30.0) | 28 (43.1) | 1 (6.3) | ||
| PNI | (n = 14) | (n = 10) | 0.341 | (n = 65) | (n = 16) | 0.171 |
| Present | 5 (35.7) | 1 (10.0) | 16 (24.6) | 1 (6.3) | ||
| WPOI | ||||||
| Present | ||||||
| Histologic grade | (n = 13) | (n = 9) | 0.448 | (n = 71) | (n = 16) | 0.202 |
| WD | 1 (7.7) | 0 (0.0) | 9 (12.7) | 0 (0.0) | ||
| MD | 8 (61.5) | 8 (88.9) | 50 (70.4) | 15 (93.8) | ||
| PD | 4 (30.8) | 1 (11.1) | 12 (16.9) | 1 (6.3) | ||
| N status | 0.002 | <0.001 | ||||
| N1 | 1(5.9) | 7 (53.8) | 8 (9.9) | 14 (73.7) | ||
| N2 | 10 (58.8) | 6 (46.2) | 50 (61.7) | 5 (26.3) | ||
| N3 | 6 (35.3) | 0 (0.0) | 23 (28.4) | 0 (0.0) | ||
| LNM number (median, [Q1–Q3]) | 3.0 [1.0–6.5] | 1.0 [1.0–3.0] | 0.034 | 3.0 [2.0–5.0] | 1.0 [1.0–2.0] | <0.001 |
| LNM largest node size (cm) (median, [Q1–Q3)) | 2.1 [1.3–3.1) | 1.3 [0.9–2.4] | 0.156 | 2.5 [1.7–4.4] | 1.4 [0.8–2.0] | 0.002 |
| Univariable Analyses | Multivariable Analyses | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Tumor dimension variables | ||||||
| Tumor diameter (cm) | 1.325 | 1.074–1.636 | 0.009 | |||
| Tumor volume (cm3) | 1.058 | 1.015–1.103 | 0.008 | |||
| DOI (mm) | ||||||
| DOI ≤ 5 | 1 | |||||
| 5 < DOI ≤ 10 | 2.275 | 0.968–5.345 | 0.059 | |||
| 10 < DOI | 3.119 | 1.602–6.075 | <0.001 | |||
| T status | ||||||
| T1 | 1 | 1 | ||||
| T2 | 1.303 | 0.560–3.034 | 0.539 | 1.215 | 0.465–3.175 | 0.692 |
| T3 | 2.739 | 1.193–6.291 | 0.018 | 1.905 | 0.732–4.953 | 0.186 |
| T4 | 11.200 | 2.843–44.119 | <0.001 | 6.483 | 1.544–27.225 | 0.011 |
| Tumor biological variables | ||||||
| LVI | 2.146 | 1.078–4.269 | 0.030 | |||
| PNI | 2.102 | 1.134–3.896 | 0.018 | |||
| WPOI | 1.082 | 0.390–3.002 | 0.880 | |||
| Histologic grade | ||||||
| WD | 1 | |||||
| MD | 1.477 | 0.777–2.809 | 0.235 | |||
| PD | 1.846 | 0.763–4.469 | 0.174 | |||
| LNM variables | ||||||
| LNM number | 1.681 | 1.292–2.186 | <0.001 | |||
| LNM largest size (cm) | 3.223 | 1.899–5.470 | <0.001 | 2.288 | 1.328–3.942 | 0.003 |
| N status | ||||||
| N1 | 1 | 1 | ||||
| N2 | 4.868 | 2.541–9.327 | <0.001 | 3.192 | 1.549–6.581 | 0.002 |
| N3 | 53.415 | 2.737–1042.499 | 0.009 | 35.870 | 1.808–711.619 | 0.019 |
| Univariable Analyses | Multivariable Analyses | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Tumor dimension variables | ||||||
| Tumor diameter (cm) | 1.164 | 0.830–1.631 | 0.380 | |||
| Tumor volume (cm3) | 1.050 | 0.970–1.136 | 0.225 | |||
| DOI (mm) | ||||||
| DOI = 0 | 1 | |||||
| 0 < DOI ≤ 5 | 1.429 | 0.267–7.736 | 0.679 | |||
| 5 < DOI ≤ 10 | 2.000 | 0.366–10.919 | 0.424 | |||
| 10 < DOI | 2.143 | 0.411–11.168 | 0.366 | |||
| T status | ||||||
| T0 | 1 | |||||
| T1 | 1.812 | 0.399–8.241 | 0.442 | |||
| T2 | 1.261 | 0.284–5.595 | 0.760 | |||
| T3 | 4.000 | 0.299–53.467 | 0.295 | |||
| T4 | 3.000 | 0.211–42.624 | 0.417 | |||
| Tumor biological variables | ||||||
| LVI | 2.819 | 0.941–8.445 | 0.064 | 1.553 | 1.123–2.149 | 0.008 |
| PNI | 6.308 | 0.758–0.088 | 0.088 | |||
| Histologic grade | ||||||
| WD | 1 | |||||
| MD | 0.591 | 0.006–57.099 | 0.822 | |||
| PD | 0.436 | 0.004–45.507 | 0.726 | |||
| LNM variables | ||||||
| LNM number | 1.190 | 0.992–1.428 | 0.061 | |||
| LNM largest size (cm) | 1.488 | 1.117–1.983 | 0.007 | 3.004 | 0.945–9.542 | 0.062 |
| N status | ||||||
| N1 | 1 | |||||
| N2 | 1.108 | 0.455–2.697 | 0.822 | |||
| N3 | 3.215 | 0.414–25.03 | 0.264 | |||
| Univariable Analyses | Multivariable Analyses | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Tumor dimension variables | ||||||
| Tumor diameter (cm) | 1.441 | 0.788–2.634 | 0.236 | |||
| Tumor volume (cm3) | 1.046 | 0.959–1.142 | 0.312 | |||
| DOI (mm) | ||||||
| DOI ≤ 5 | 1 | |||||
| 5 < DOI ≤ 10 | 4.000 | 0.211–75.658 | 0.355 | |||
| 10 mm < DOI | 1.000 | 0.098–10.166 | 0.999 | |||
| T status | ||||||
| T1 | 1 | |||||
| T2 | 7.307 | 0.872–61.222 | 0.067 | |||
| T3 | 64.991 | 1.739–2428.451 | 0.024 | |||
| T4 | 17.800 | 0.110–0.268 | 0.268 | |||
| Tumor biological variables | ||||||
| LVI | 2.722 | 0.479–15.463 | 0.259 | |||
| PNI | 4.999 | 0.483–51.762 | 0.177 | |||
| Histologic grade | ||||||
| WD | 1 | |||||
| MD | 0.332 | 0.332–34.232 | 0.641 | |||
| PD | 0.995 | 0.007–142.386 | 0.998 | |||
| LNM variables | ||||||
| LNM number | 1.648 | 0.963–2.822 | 0.068 | |||
| LNM largest size (cm) | 1.463 | 0.799–2.681 | 0.218 | |||
| N status | ||||||
| N1 | 1 | 1 | ||||
| N2 | 8.077 | 0.974–66.965 | 0.053 | 8.077 | 0.974–66.965 | 0.053 |
| N3 | 65.009 | 1.739–2429.666 | 0.024 | 65.009 | 1.739–2429.666 | 0.024 |
| Univariable Analyses | Multivariable Analyses | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Tumor dimension variables | ||||||
| Tumor diameter (cm) | 1.074 | 0.798–1.445 | 0.639 | |||
| Tumor volume (cm3) | 1.023 | 0.978–1.069 | 0.320 | |||
| DOI (mm) | ||||||
| DOI ≤ 5 | 1 | |||||
| 5 < DOI ≤ 10 | 0.800 | 0.168–3.799 | 0.779 | |||
| 10 < DOI | 2.000 | 0.302–13.265 | 0.473 | |||
| T status | ||||||
| T1 | 1 | |||||
| T2 | 2.083 | 0.565–7.672 | 0.270 | |||
| T3 | 3.373 | 0.434–26.196 | 0.245 | |||
| T4 | 1.880 | 0.464–7.617 | 0.377 | |||
| Tumor biological variables | ||||||
| LVI | 7.854 | 1.333–46.278 | 0.023 | |||
| PNI | 3.444 | 0.562–21.119 | 0.181 | |||
| Histologic grade | ||||||
| WD | 1 | |||||
| MD | 0.172 | 0.008–3.628 | 0.258 | |||
| PD | 0.439 | 0.014–14.163 | 0.642 | |||
| LNM variables | ||||||
| LNM number | 2.025 | 1.214–3.379 | 0.007 | |||
| LNM largest size (cm) | 2.636 | 1.442–4.817 | 0.002 | 2.158 | 1.104–4.218 | 0.025 |
| N status | ||||||
| N1 | 1 | 1 | ||||
| N2 | 15.663 | 4.532–54.136 | <0.001 | 12.754 | 3.470–46.880 | <0.001 |
| N3 | 80.176 | 4.034–1593.502 | 0.004 | 35.989 | 1.617–775.018 | 0.022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, Y.J.; Park, G.; Park, S.Y.; Kim, T.; Kim, E.; Heo, Y.; Lee, C.; Jeong, H.-S. Extra-Capsular Spread of Lymph Node Metastasis in Oral, Oropharyngeal and Hypopharyngeal Cancer: A Comparative Subsite Analysis. Cancers 2024, 16, 659. https://doi.org/10.3390/cancers16030659
Kang YJ, Park G, Park SY, Kim T, Kim E, Heo Y, Lee C, Jeong H-S. Extra-Capsular Spread of Lymph Node Metastasis in Oral, Oropharyngeal and Hypopharyngeal Cancer: A Comparative Subsite Analysis. Cancers. 2024; 16(3):659. https://doi.org/10.3390/cancers16030659
Chicago/Turabian StyleKang, Yung Jee, Goeun Park, Sung Yool Park, Taehwan Kim, Eunhye Kim, Yujin Heo, Changhee Lee, and Han-Sin Jeong. 2024. "Extra-Capsular Spread of Lymph Node Metastasis in Oral, Oropharyngeal and Hypopharyngeal Cancer: A Comparative Subsite Analysis" Cancers 16, no. 3: 659. https://doi.org/10.3390/cancers16030659