
Outcomes of Multimodal Treatment in Elderly Patients with Localized Non-Small Lung Cancer from a Radiation Oncology Point of View: Special Focus on Low-Dose Cisplatin

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
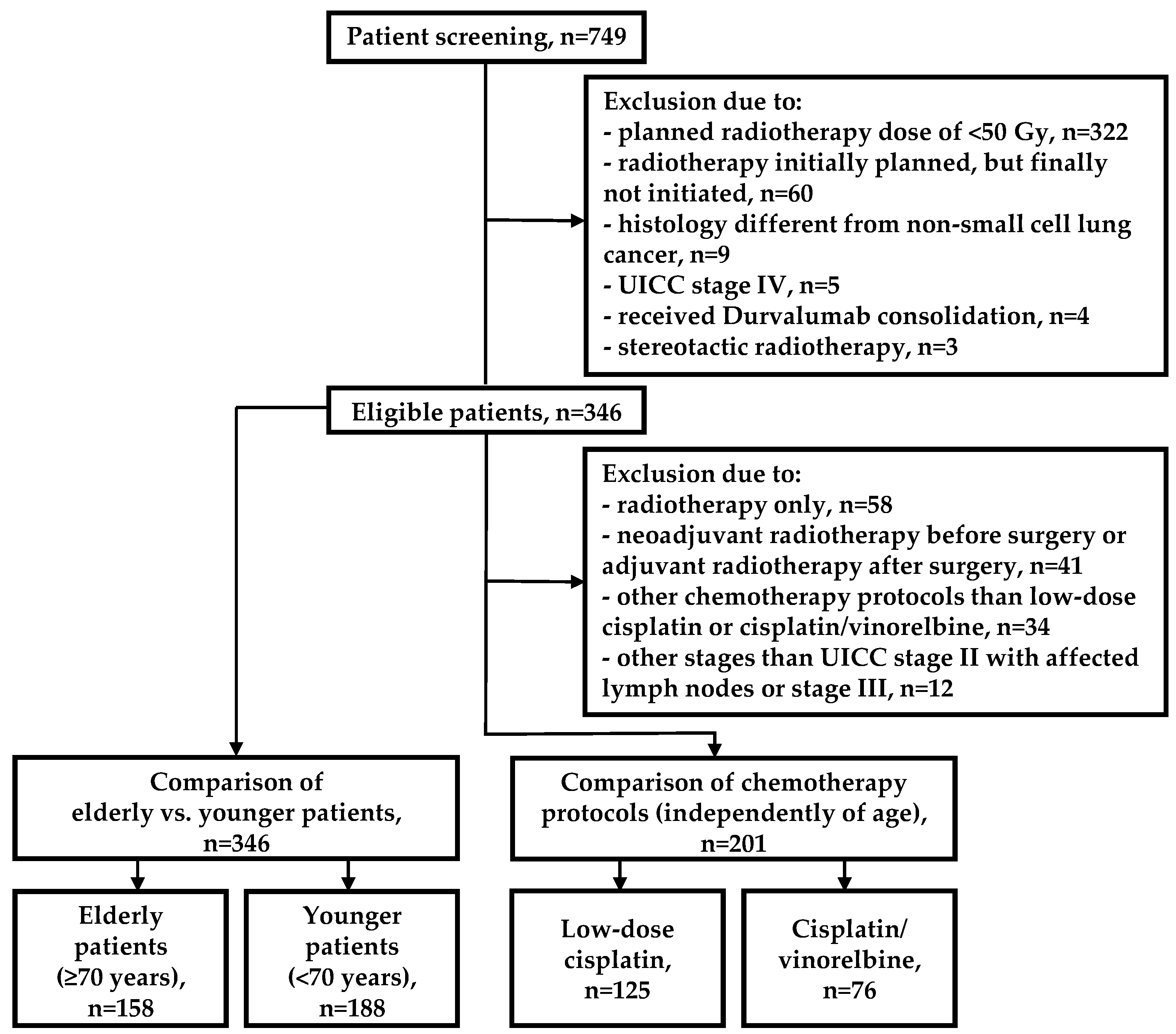
2. Patients and Methods
2.1. Study Design
2.2. Radiochemotherapy
2.3. Endpoints and Statistical Analysis
3. Results
3.1. Clinical and Treatment Characteristics
3.1.1. Elderly vs. Younger Patients
3.1.2. Cisplatin/Vinorelbine vs. Low-Dose Cisplatin in Definitive Radiochemotherapy (Independently of Age)
3.2. Toxicities
3.2.1. Elderly vs. Younger Patients
3.2.2. Cisplatin/Vinorelbine vs. Low-Dose Cisplatin in Definitive Radiochemotherapy (Independently of Age)
3.3. Outcomes
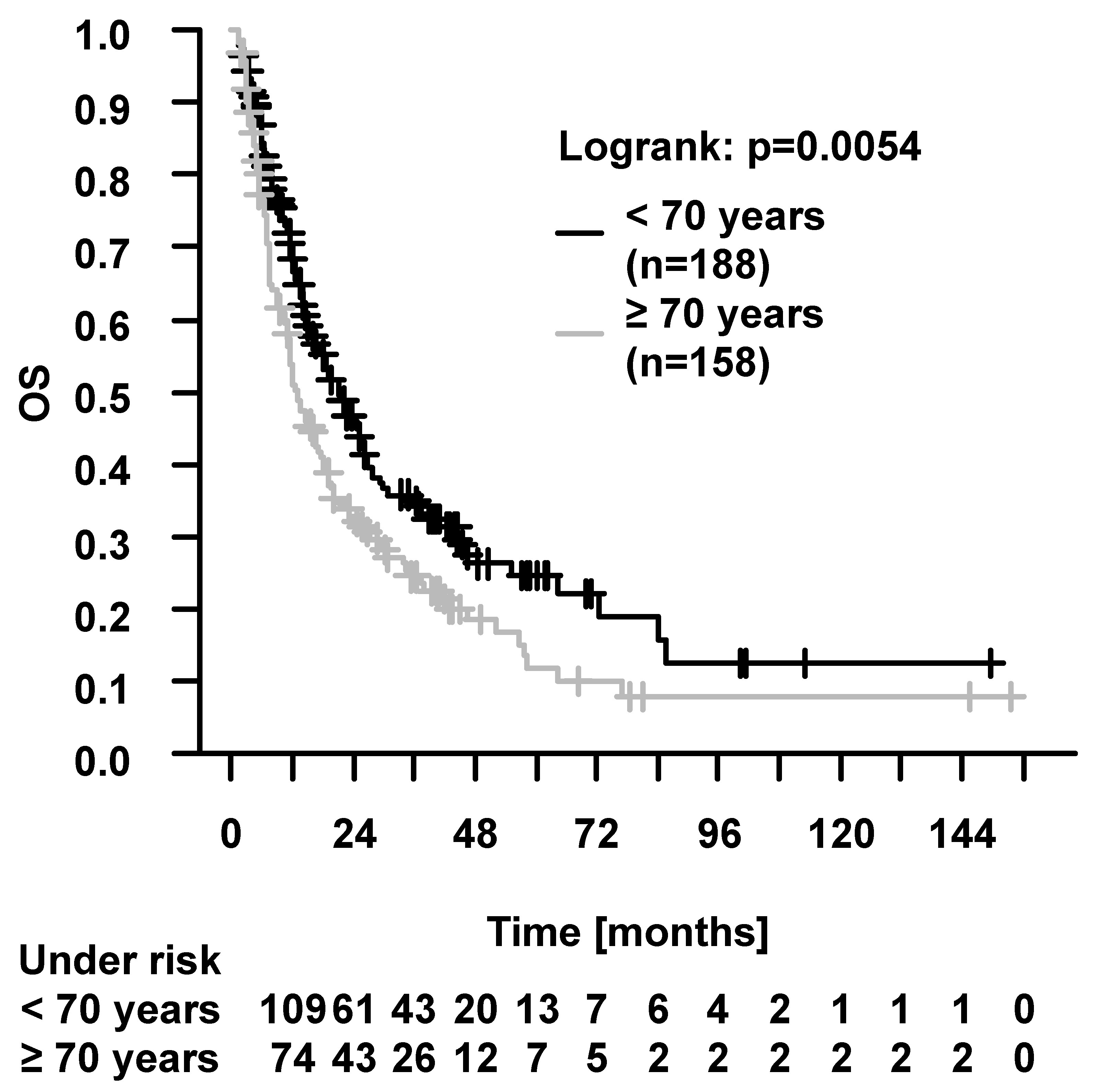
3.3.1. Elderly Patients
Elderly vs. Younger Patients
Prognostic Factors in Elderly Patients
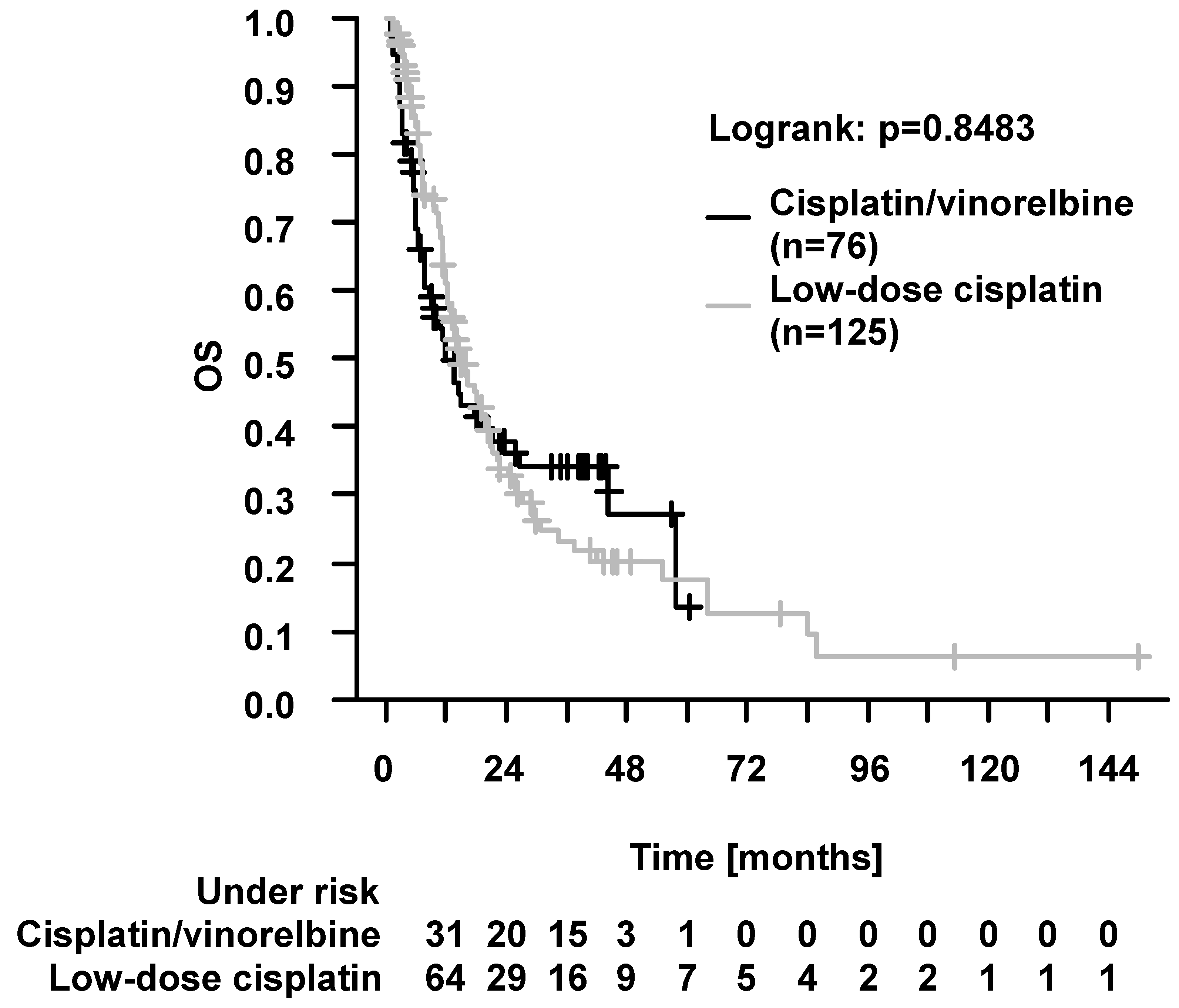
3.3.2. Cisplatin/Vinorelbine vs. Low-Dose Cisplatin in Definitive Radiochemotherapy (Indepently of Age)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malvezzi, M.; Santucci, C.; Boffetta, P.; Collatuzzo, G.; Levi, F.; La Vecchia, C.; Negri, E. European cancer mortality predictions for the year 2023 with focus on lung cancer. Ann. Oncol. 2023, 34, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Frost, N.; Griesinger, F.; Hoffmann, H.; Länger, F.; Nestle, U.; Schütte, W.; Wolf, J.; Reck, M. Lung Cancer in Germany. J. Thorac. Oncol. 2022, 17, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Venuta, F.; Diso, D.; Onorati, I.; Anile, M.; Mantovani, S.; Rendina, E.A. Lung cancer in elderly patients. J. Thorac. Dis. 2016, 8, S908–S914. [Google Scholar] [CrossRef]
- Sant, M.; Daidone, C.; Innos, K.; Marcos-Gragera, R.; Vanschoenbeek, K.; Barranco, M.R.; Poch, E.O.; Lillini, R. Patterns of care and survival for lung cancer: Results of the European population-based high-resolution study. Front. Epidemiol. 2023, 3, 109853. [Google Scholar] [CrossRef]
- Sharma, G.; Goodwin, J. Effect of aging on respiratory system physiology and immunology. Clin. Interv. Aging 2006, 1, 253–260. [Google Scholar] [CrossRef]
- Weyand, C.M.; Goronzy, J.J. Aging of the Immune System. Mechanisms and Therapeutic Targets. Ann. Am. Thorac. Soc. 2016, 13, S422–S428. [Google Scholar] [CrossRef] [PubMed]
- Stupka, J.E.; Mortensen, E.M.; Anzueto, A.; Restrepo, M.I. Community-acquired pneumonia in elderly patients. Aging health 2009, 5, 763–774. [Google Scholar] [CrossRef]
- Duan, Z.; Cai, G.; Li, J.; Chen, X. Cisplatin-induced renal toxicity in elderly people. Ther. Adv. Med. Oncol. 2020, 12, 1–15. [Google Scholar] [CrossRef]
- Tang, M.; Pearson, S.-A.; Schaffer, A.L.; Lewis, C.R.; John, T.; Simes, R.J.; Lee, C.K. Are clinical trial eligibility criteria representative of older patients with lung cancer? A population-based data linkage study. J. Geriatr. Oncol. 2021, 12, 930–936. [Google Scholar] [CrossRef]
- Nadal, E.; Oré-Arce, M.; Remon, J.; Bernabé-Caro, R.; Covela-Rúa, M.; de Castro-Carpeño, J.; Massutí-Sureda, B.; Guillot-Morales, M.; Majem, M.; Maestu-Maiques, I.; et al. Expert consensus to optimize the management of older adult patients with advanced EGFR-mutated non-small cell lung cancer. Clin. Transl. Oncol. 2023, 25, 3139–3151. [Google Scholar] [CrossRef]
- Balducci, L. Geriatric oncology: Challenges for the new century. Eur. J. Cancer 2000, 36, 1741–1754. [Google Scholar] [CrossRef] [PubMed]
- Bonanno, L.; Attili, I.; Pavan, A.; Sepulcri, M.; Pasello, G.; Rea, F.; Guarneri, V.; Conte, P. Treatment strategies for locally advanced non-small cell lung cancer in elderly patients: Translating scientific evidence into clinical practice. Crit. Rev. Oncol. Hematol. 2021, 163, 103378. [Google Scholar] [CrossRef]
- Okawara, G.; Mackay, J.A.; Evans, W.K.; Ung, Y.C. Management of Unresected Stage III Non-small Cell Lung Cancer: A Systematic Review. J. Thorac. Oncol. 2006, 1, 377–393. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; He, Z.; Dang, J.; Li, G. Comparative efficacy and safety for different chemotherapy regimens used concurrently with thoracic radiation for locally advanced non-small cell lung cancer: A systematic review and network meta-analysis. Radiat. Oncol. 2019, 14, 55. [Google Scholar] [CrossRef]
- Flentje, M.; Huber, R.M.; Engel-Riedel, W.; Andreas, S.; Kollmeier, J.; Staar, S.; Dickgreber, N.; Vaissiere, N.; de Almeida, C.; Edlich, B.; et al. GILT—A randomised phase III study of oral vinorelbine and cisplatin with concomitant radiotherapy followed by either consolidation therapy with oral vinorelbine and cisplatin or best supportive care alone in stage III non-small cell lung cancer. Strahlenther. Onkol. 2016, 192, 216–222. [Google Scholar] [CrossRef] [PubMed]
- S3-Leitlinie: Prävention, Diagnostik, Therapie und Nachsorge des Lungenkarzinoms. Available online: https://www.leitlinienprogramm-onkologie.de/fileadmin/user_upload/Downloads/Leitlinien/Lungenkarzinom/Version_2/LL_Lungenkarzinom_Langversion_2.2.pdf (accessed on 7 November 2023).
- Schaake-Koning, C.; van den Bogaert, W.; Dalesio, O.; Festen, J.; Hoogenhout, J.; van Houtte, P.; Kirkpatrick, A.; Koolen, M.; Maat, B.; Nijs, A. Effects of concomitant cisplatin and radiotherapy on inoperable non-small-cell lung cancer. N. Engl. J. Med. 1992, 326, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Koning, C.C.; Wouterse, S.J.; Daams, J.G.; Uitterhoeve, L.L.; van den Heuvel, M.M.; Belderbos, J.S. Toxicity of concurrent radiochemotherapy for locally advanced non--small-cell lung cancer: A systematic review of the literature. Clin. Lung Cancer 2013, 14, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Overall Survival with Durvalumab after Chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Non-Small Cell Lung Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (accessed on 7 November 2023).
- Nestle, U.; de Ruysscher, D.; Ricardi, U.; Geets, X.; Belderbos, J.; Pöttgen, C.; Dziadiuszko, R.; Peeters, S.; Lievens, Y.; Hurkmans, C.; et al. ESTRO ACROP guidelines for target volume definition in the treatment of locally advanced non-small cell lung cancer. Radiother. Oncol. 2018, 127, 1–5. [Google Scholar] [CrossRef]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (accessed on 8 November 2023).
- American Joint Committee on Cancer. AJCC Cancer Staging Manual, 7th ed.; Springer: New York, NY, USA, 2010; ISBN 978-0-387-88440-0. [Google Scholar]
- Wittekind, C.; Asamura, H.; Sobin, L.H. (Eds.) TNM Atlas: Illustrated Guide to the TNM Classification of Malignant Tumours, 6th ed.; Wiley-Blackwell: Chichester, UK, 2014; ISBN 978-1-118-69564-7. [Google Scholar]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V. The IASLC Lung Cancer Staging Project: Proposals for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Lung Cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Niehoff, J.; Diederich, S.; Höink, A. Staging des Lungenkarzinoms nach der revidierten TNM-Klassifikation. Radiol. up2date 2017, 17, 347–359. [Google Scholar] [CrossRef]
- Gross, A.; Ziepert, M.; Scholz, M. KMWin—A convenient tool for graphical presentation of results from Kaplan-Meier survival time analysis. PLoS ONE 2012, 7, e38960. [Google Scholar] [CrossRef] [PubMed]
- Stinchcombe, T.E.; Zhang, Y.; Vokes, E.E.; Schiller, J.H.; Bradley, J.D.; Kelly, K.; Curran, W.J., Jr.; Schild, S.E.; Movsas, B.; Clamon, G.; et al. Pooled Analysis of Individual Patient Data on Concurrent Chemoradiotherapy for Stage III Non-Small-Cell Lung Cancer in Elderly Patients Compared With Younger Patients Who Participated in US National Cancer Institute Cooperative Group Studies. J. Clin. Oncol. 2017, 35, 2885–2892. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.F.; Lin, F.P.; Epstein, R.J. How aging of the global population is changing oncology. Ecancermedicalscience 2021, 15, ed119. [Google Scholar] [CrossRef] [PubMed]
- Zaborowska-Szmit, M.; Olszyna-Serementa, M.; Kowalski, D.M.; Szmit, S.; Krzakowski, M. Elderly Patients with Locally Advanced and Unresectable Non-Small-Cell Lung Cancer May Benefit from Sequential Chemoradiotherapy. Cancers 2021, 13, 4534. [Google Scholar] [CrossRef]
- Jolly, T.A.; Deal, A.M.; Nyrop, K.A.; Williams, G.R.; Pergolotti, M.; Wood, W.A.; Alston, S.M.; Gordon, B.-B.E.; Dixon, S.A.; Moore, S.G.; et al. Geriatric Assessment-Identified Deficits in Older Cancer Patients With Normal Performance Status. Oncologist 2015, 20, 379–385. [Google Scholar] [CrossRef]
- Antonio, M.; Saldaña, J.; Linares, J.; Ruffinelli, J.C.; Palmero, R.; Navarro, A.; Arnaiz, M.D.; Brao, I.; Aso, S.; Padrones, S.; et al. Geriatric assessment may help decision-making in elderly patients with inoperable, locally advanced non-small-cell lung cancer. Br. J. Cancer 2018, 118, 639–647. [Google Scholar] [CrossRef]
- Owusu, C.; Koroukian, S.M.; Schluchter, M.; Bakaki, P.; Berger, N.A. Screening older cancer patients for a Comprehensive Geriatric Assessment: A comparison of three instruments. J. Geriatr. Oncol. 2011, 2, 121–129. [Google Scholar] [CrossRef]
- Wang, S.; Wong, M.L.; Hamilton, N.; Davoren, J.B.; Jahan, T.M.; Walter, L.C. Impact of age and comorbidity on non-small-cell lung cancer treatment in older veterans. J. Clin. Oncol. 2012, 30, 1447–1455. [Google Scholar] [CrossRef]
- Cacicedo, J.; Casquero, F.; Navarro, A.; Martinez-Indart, L.; Del Hoyo, O.; Frías, A.; de Zarate, R.O.; Büchser, D.; Gómez-Iturriaga, A.; San Miguel, I.; et al. Prospective multicentre analysis of the therapeutic approach and prognostic factors determining overall survival in elderly patients with non-small-cell lung carcinoma treated with curative intent. BJR Open 2022, 4, 20210058. [Google Scholar] [CrossRef]
- Driessen, E.J.M.; Bootsma, G.P.; Hendriks, L.E.L.; van den Berkmortel, F.W.P.J.; Bogaarts, B.A.H.A.; van Loon, J.G.M.; Dingemans, A.-M.C.; Janssen-Heijnen, M.L.G. Stage III Non-Small Cell Lung Cancer in the elderly: Patient characteristics predictive for tolerance and survival of chemoradiation in daily clinical practice. Radiother. Oncol. 2016, 121, 26–31. [Google Scholar] [CrossRef]
- Zazuli, Z.; Kos, R.; Veltman, J.D.; Uyterlinde, W.; Longo, C.; Baas, P.; Masereeuw, R.; Vijverberg, S.J.H.; Maitland-van der Zee, A.-H. Comparison of Myelotoxicity and Nephrotoxicity Between Daily Low-Dose Cisplatin With Concurrent Radiation and Cyclic High-Dose Cisplatin in Non-Small Cell Lung Cancer Patients. Front. Pharmacol. 2020, 11, 975. [Google Scholar] [CrossRef] [PubMed]
- Weiling, M.J.; Losensky, W.; Wächter, K.; Schilling, T.; Frank, F.; Haas, M.; Fietkau, R.; Distel, L.V.; Weiss, S. Older Patients Are Less Affected by Radiochemotherapeutic Treatment than Younger. Biomed. Res. Int. 2018, 2018, 5471054. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Balducci, L. Anemia of aging: The role of chronic inflammation and cancer. Semin. Hematol. 2008, 45, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, M.; Rajta, P.N.; Khatana, J. Anemia in Chronic obstructive pulmonary disease: Prevalence, pathogenesis, and potential impact. Lung India 2015, 32, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Durham, A.L.; Adcock, I.M. The relationship between COPD and lung cancer. Lung Cancer 2015, 90, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Dawe, D.E.; Christiansen, D.; Swaminath, A.; Ellis, P.M.; Rothney, J.; Rabbani, R.; Abou-Setta, A.M.; Zarychanski, R.; Mahmud, S.M. Chemoradiotherapy versus radiotherapy alone in elderly patients with stage III non-small cell lung cancer: A systematic review and meta-analysis. Lung Cancer 2016, 99, 180–185. [Google Scholar] [CrossRef]
- Blanco, R.; Maestu, I.; de La Torre, M.G.; Cassinello, A.; Nunez, I. A review of the management of elderly patients with non-small-cell lung cancer. Ann. Oncol. 2015, 26, 451–463. [Google Scholar] [CrossRef]
- Owonikoko, T.K.; Ragin, C.C.; Belani, C.P.; Oton, A.B.; Gooding, W.E.; Taioli, E.; Ramalingam, S.S. Lung cancer in elderly patients: An analysis of the surveillance, epidemiology, and end results database. J. Clin. Oncol. 2007, 25, 5570–5577. [Google Scholar] [CrossRef]
- May, L.; Shows, K.; Nana-Sinkam, P.; Li, H.; Landry, J.W. Sex Differences in Lung Cancer. Cancers 2023, 15, 3111. [Google Scholar] [CrossRef]
- Miller, E.D.; Fisher, J.L.; Haglund, K.E.; Grecula, J.C.; Xu-Welliver, M.; Bertino, E.M.; He, K.; Shields, P.G.; Carbone, D.P.; Williams, T.M.; et al. The Addition of Chemotherapy to Radiation Therapy Improves Survival in Elderly Patients with Stage III Non-Small Cell Lung Cancer. J. Thorac. Oncol. 2018, 13, 426–435. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, J.; Klinkhammer-Schalke, M.; Bierbaum, V.; Gerken, M.; Bobeth, C.; Rößler, M.; Dröge, P.; Ruhnke, T.; Günster, C.; Kleihues-van Tol, K.; et al. Initial Cancer Treatment in Certified Versus Non-Certified Hospitals. Dtsch. Arztebl. Int. 2023, 120, 647–654. [Google Scholar] [CrossRef] [PubMed]
- Walter, J.; Moeller, C.; Resuli, B.; Kauffmann-Guerrero, D.; Manapov, F.; Dinkel, J.; Neumann, J.; Kovacs, J.; Schneider, C.; Huber, R.M.; et al. Guideline adherence of tumor board recommendations in lung cancer and transfer into clinical practice. J. Cancer Res. Clin. Oncol. 2023, 149, 11679–11688. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | ≥70 Years, n = 158 | <70 Years, n = 188 | p-Value |
|---|---|---|---|
| Age (years, median (min–max)) | 75.8 (70.1–89.2) | 61.2 (32.5–69.9) | <0.01 5 |
| Gender | 0.02 6 | ||
| Male (number (%)) | 123 (77.8) | 126 (67.0) | |
| Female (number (%)) | 35 (22.2) | 62 (33.0) | |
| Follow-up (months, median, min–max) | 11.4 (1.4–153.8) | 14.2 (1.2–149.7) | 0.04 5 |
| Karnofsky index (median, min–max) | 80 (50–90) | 90 (20–90) | 0.03 5 |
| Charlson comorbidity index (median, min–max) | 7 (4–14) | 5 (2–12) | <0.01 5 |
| Histology, numbers (%) | 0.07 5 | ||
| Squamous cell carcinoma | 100 (63.3) | 102 (54.2) | |
| Adenocarcinoma | 54 (34.2) | 77 (41.0) | |
| Other histology 1 | 4 (2.5) | 9 (4.8) | |
| T stage 0–2 2, numbers (%) | 52 (32.9) | 60 (31.9) | 0.84 6 |
| T stage 3–4, numbers (%) | 106 (67.1) | 128 (68.1) | |
| N stage 0–1, numbers (%) | 48 (30.4) | 42 (22.3) | 0.08 6 |
| N stage 2–3, numbers (%) | 110 (69.6) | 146 (77.7) | |
| UICC stage IIA-IIIA, numbers (%) | 89 (56.3) | 70 (27.2) | <0.01 6 |
| UICC stage IIIB-IIIC, numbers (%) | 69 (43.7) | 118 (62.8) | |
| Treatment concept, numbers (%) 3 | <0.01 5 | ||
| Trimodality therapy | 10 (6.3) | 19 (10.1) | |
| Bimodality therapy | 100 (63.3) | 154 (81.9) | |
| RT only | 48 (30.4) | 15 (8.0) | |
| Radiotherapy, applied dose [Gy] (median, min–max) | 60 (8–70) | 60 (2–70) | 0.57 5 |
| Completion of radiotherapy as planned, numbers (%) | 129 (81.6) | 159 (84.6) | 0.47 6 |
| Definitive radiotherapy or radiochemotherapy | 144 (91.1) | 161 (85.6) | 0.11 6 |
| Radiotherapy only | 48 (33.3) | 15 (9.3) | <0.01 6 |
| Radiochemotherapy | 96 (66.7) | 146 (90.7) | |
| Sequential chemotherapy | 7 (7.3) | 7 (4.8) | 0.42 6 |
| Concurrent chemotherapy | 89 (92.7) | 139 (95.2) | |
| Cisplatin/vinorelbine | 20 (22.5) | 62 (44.6) | 0.03 5 |
| Low-dose cisplatin | 68 (76.4) | 72 (51.8) | |
| Other 4 | 1 (1.1) | 5 (3.6) |
| Parameter | Low-Dose Cisplatin, n = 125 | Cisplatin/Vinorelbine, n = 76 | p-Value |
|---|---|---|---|
| Age (years, median (min–max)) | 68.5 (32.5–85.0) | 62.6 (39.2–77.8) | <0.01 2 |
| Gender | |||
| Male (number (%)) | 95 (76.0) | 55 (72.4) | 0.57 3 |
| Female (number (%)) | 30 (24.0) | 21 (27.6) | |
| Follow-up (months, median (min–max)) | 12.3 (1.5–149.7) | 9.4 (1.2–60.4) | 0.28 2 |
| Karnofsky index (median, min–max) | 90 (50–90) | 90 (20–90) | 0.17 2 |
| Charlson comorbidity index (median, min-max) | 6 (2–13) | 5 (2–9) | <0.01 2 |
| T stage 0–2 1, numbers (%) | 35 (28.0) | 25 (32.9) | 0.46 3 |
| T stage 3–4, numbers (%) | 90 (72.0) | 51 (67.1) | |
| N stage 0–1, numbers (%) | 33 (26.4) | 7 (9.2) | <0.01 3 |
| N stage 2–3, numbers (%) | 92 (73.6) | 69 (90.8) | |
| UICC stage IIB-IIIA, numbers (%) | 51 (40.8) | 23 (30.2) | 0.13 3 |
| UICC stage IIIB-IIIC, numbers (%) | 74 (59.2) | 53 (69.8) | |
| Radiotherapy, applied dose [Gy] (median, min-max) | 60 (4–66.6) | 65 (10–66) | 0.37 2 |
| Completion of radiotherapy as planned, numbers (%) | 111 (88.8) | 60 (78.9) | 0.06 3 |
| Completion of concomitant chemotherapy as planned, numbers (%) | 98 (78.4) | 49 (64.5) | 0.03 3 |
| Parameter | Elderly Patients (≥70 Years, n = 158) | Younger Patients (<70 Years, n = 188) | p-Value |
|---|---|---|---|
| Dermatitis, ≥grade 1 | 46 (29.1) | 88 (46.8) | <0.01 |
| Dermatitis, ≥grade 2 | 2 (1.3) | 1 (0.5) | 0.46 |
| Dysphagia, ≥grade 1 | 90 (57.0) | 130 (69.1) | <0.02 |
| Dysphagia, ≥grade 2 | 29 (18.4) | 48 (25.5) | 0.11 |
| Dysphagia, ≥grade 3 | 8 (5.1) | 17 (9.0) | 0.15 |
| Nausea, ≥grade 1 | 45 (28.5) | 65 (34.6) | 0.23 |
| Nausea, ≥grade 2 | 12 (7.6) | 18 (9.6) | 0.51 |
| Pneumonitis, ≥grade 1 | 43 (27.2) | 48 (25.5) | 0.72 |
| Pneumonitis, ≥grade 2 | 19 (12.0) | 16 (8.5) | 0.28 |
| Pneumonitis, ≥grade 3 | 4 (2.5) | 3 (1.6) | 0.54 |
| Lung infection, ≥grade 2 | 19 (12.0) | 29 (15.4) | 0.36 |
| Dyspnea, ≥grade 1 | 108 (68.4) | 126 (67.0) | 0.79 |
| Dyspnea, ≥grade 2 | 56 (35.5) | 59 (31.4) | 0.42 |
| Dyspnea, ≥grade 3 | 30 (19.0) | 24 (12.8) | 0.11 |
| Myocardial infarction, ≥grade 2 | 4 (2.5) | 2 (1.1) | 0.30 |
| Anemia, ≥grade 1 | 147 (93.0) | 158 (84.0) | 0.01 |
| Anemia, ≥grade 2 | 52 (32.9) | 51 (27.1) | 0.24 |
| Anemia, ≥grade 3 | 12 (7.6) | 13 (6.9) | 0.81 |
| Leukopenia, ≥grade 1 | 86 (54.4) | 107 (56.9) | 0.64 |
| Leukopenia, ≥grade 2 | 54 (34.2) | 69 (36.7) | 0.63 |
| Leukopenia, ≥grade 3 | 31 (19.6) | 39 (20.7) | 0.80 |
| Thrombocytopenia, ≥grade 1 | 80 (50.6) | 73 (38.8) | 0.03 |
| Thrombocytopenia, ≥grade 2 | 18 (11.4) | 15 (8.0) | 0.28 |
| Thrombocytopenia, ≥grade 3 | 7 (4.4) | 7 (3.7) | 0.74 |
| Parameter | Low-Dose Cisplatin, n = 125 | Cisplatin/Vinorelbine, n = 76 | p-Value |
|---|---|---|---|
| Dermatitis, ≥grade 1 | 51 (40.8) | 31 (40.8) | 1.00 |
| Dermatitis, ≥grade 2 | 1 (0.8) | 0 (0.0) | 0.43 |
| Dysphagia, ≥grade 1 | 78 (62.4) | 51 (67.1) | 0.50 |
| Dysphagia, ≥grade 2 | 24 (19.2) | 24 (31.6) | <0.05 |
| Dysphagia, ≥grade 3 | 6 (4.8) | 11 (14.4) | 0.02 |
| Nausea, ≥grade 1 | 33 (26.4) | 32 (42.1) | 0.02 |
| Nausea, ≥grade 2 | 5 (4.0) | 12 (15.8) | <0.01 |
| Pneumonitis, ≥grade 1 | 33 (26.4) | 15 (19.7) | 0.28 |
| Pneumonitis, ≥grade 2 | 13 (10.4) | 4 (5.3) | 0.20 |
| Pneumonitis, ≥grade 3 | 2 (1.6) | 0 (0.0) | 0.27 |
| Lung infection, ≥grade 2 | 21 (16.8) | 11 (14.5) | 0.66 |
| Dyspnea, ≥grade 1 | 79 (63.2) | 48 (63.2) | 1.00 |
| Dyspnea, ≥grade 2 | 41 (32.8) | 22 (29.0) | 0.57 |
| Dyspnea, ≥grade 3 | 20 (16.0) | 7 (9.2) | 0.17 |
| Myocardial infarction, ≥grade 2 | 2 (1.6) | 0 (0.0) | 0.27 |
| Anemia, ≥grade 1 | 108 (86.4) | 67 (88.2) | 0.72 |
| Anemia, ≥grade 2 | 34 (27.2) | 22 (28.9) | 0.79 |
| Anemia, ≥grade 3 | 7 (5.6) | 7 (9.2) | 0.33 |
| Leukopenia, ≥grade 1 | 78 (62.4) | 58 (76.3) | 0.04 |
| Leukopenia, ≥grade 2 | 45 (36.0) | 47 (61.8) | <0.01 |
| Leukopenia, ≥grade 3 | 18 (14.4) | 31 (40.8) | <0.01 |
| Thrombocytopenia, ≥grade 1 | 69 (55.2) | 34 (44.7) | 0.15 |
| Thrombocytopenia, ≥grade 2 | 11 (8.8) | 9 (11.8) | 0.52 |
| Thrombocytopenia, ≥grade 3 | 2 (1.6) | 4 (5.3) | 0.14 |
| Parameter (Numbers of Patients) | OS | PFS | LPFS | DPFS | ||||
|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Gender (female, 35; male, 123) | 0.60 (0.37–0.97) | 0.04 | 0.61 (0.39–0.95) | 0.03 | 0.60 (0.39–0.94) | 0.03 | 0.6 (0.38–0.96) | 0.03 |
| T stage (T0–2, 52; T3–4, 106) | 1.53 (1.03–2.27) | 0.04 | 1.47 (1.01–2.13) | 0.04 | 1.41 (0.97–2.06) | 0.07 | 1.47 (1.00–2.15) | <0.05 |
| Histology (adenocarcinoma, 54; other histology, 104) | 0.90 (0.60–1.37) | 0.64 | 0.87 (0.58–1.29) | 0.48 | 0.82 (0.55–1.22) | 0.33 | 0.92 (0.61–1.38) | 0.68 |
| Treatment concept, RT only (48) vs. bi- and trimodality therapy (110) | 1.66 (1.12–2.46) | 0.01 | 1.69 (1.17–2.44) | <0.01 | 1.67 (1.15–2.41) | <0.01 | 1.51 (1.04–2.21) | 0.03 |
| Karnofsky index, ≥median (75) vs. <median (83), median = 80 | 0.56 (0.39–0.81) | <0.01 | 0.64 (0.45–0.9) | 0.01 | 0.6 (0.42–0.85) | <0.01 | 0.59 (0.41–0.84) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alt, N.J.; Muster, J.; Ziegler, D.A.; Bendrich, S.; Donath, S.; Hille, A.; Anczykowski, M.Z.; Zwerenz, C.M.; Braulke, F.; von Hammerstein-Equord, A.; et al. Outcomes of Multimodal Treatment in Elderly Patients with Localized Non-Small Lung Cancer from a Radiation Oncology Point of View: Special Focus on Low-Dose Cisplatin. Cancers 2024, 16, 327. https://doi.org/10.3390/cancers16020327
Alt NJ, Muster J, Ziegler DA, Bendrich S, Donath S, Hille A, Anczykowski MZ, Zwerenz CM, Braulke F, von Hammerstein-Equord A, et al. Outcomes of Multimodal Treatment in Elderly Patients with Localized Non-Small Lung Cancer from a Radiation Oncology Point of View: Special Focus on Low-Dose Cisplatin. Cancers. 2024; 16(2):327. https://doi.org/10.3390/cancers16020327
Chicago/Turabian StyleAlt, Niklas Josua, Julian Muster, David Alexander Ziegler, Stephanie Bendrich, Sandra Donath, Andrea Hille, Mahalia Zoe Anczykowski, Carla Marie Zwerenz, Friederike Braulke, Alexander von Hammerstein-Equord, and et al. 2024. "Outcomes of Multimodal Treatment in Elderly Patients with Localized Non-Small Lung Cancer from a Radiation Oncology Point of View: Special Focus on Low-Dose Cisplatin" Cancers 16, no. 2: 327. https://doi.org/10.3390/cancers16020327