
The Impact of Statins on the Survival of Patients with Advanced Hepatocellular Carcinoma Treated with Sorafenib or Lenvatinib
 , , , , , , ,
, , , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
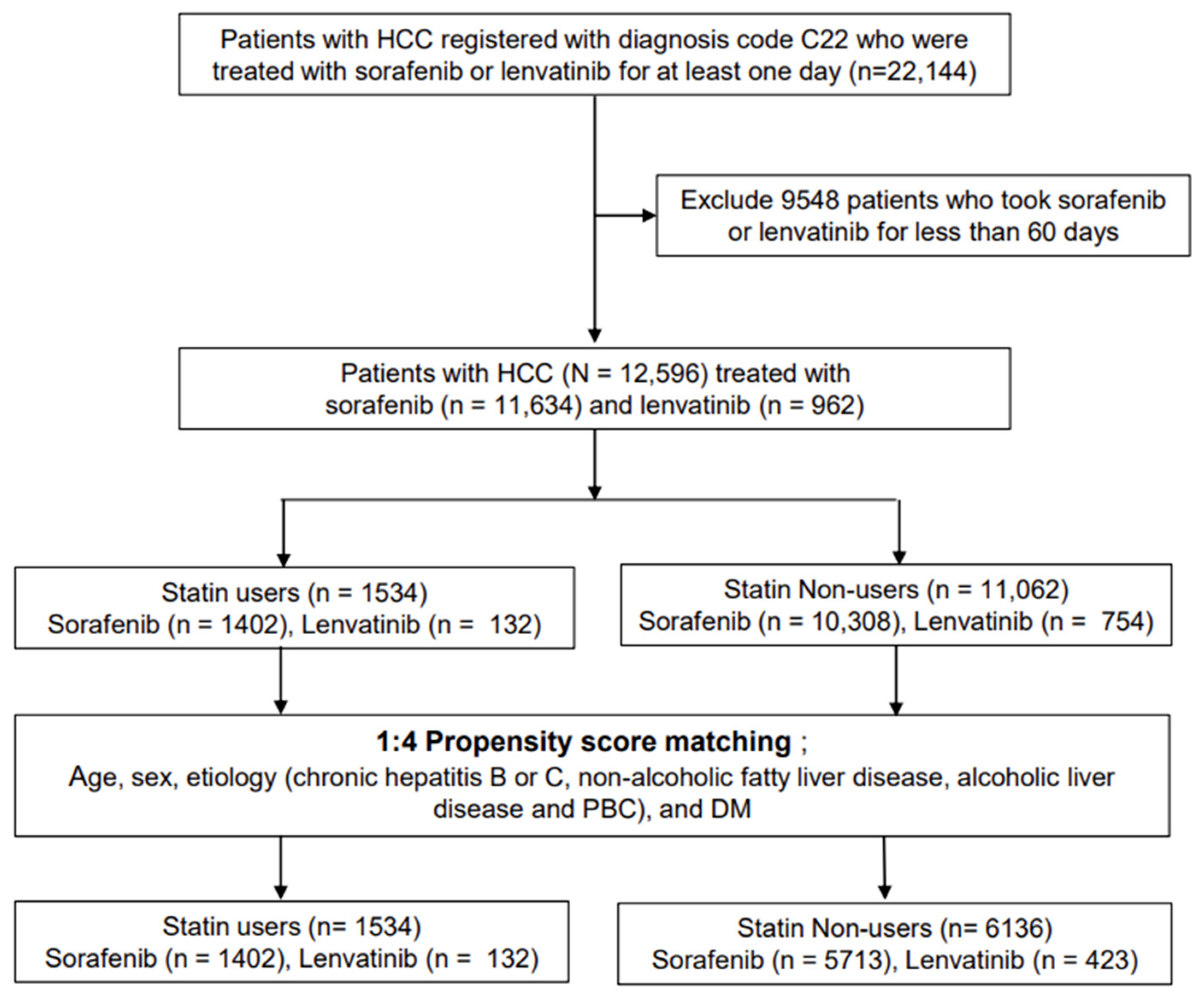
2.2. The Study Population and Definition of Terms

2.3. Data Collection
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Comparing Baseline Characteristics between Statin Users and Nonusers in Unmatched and PS-Matched Cohorts
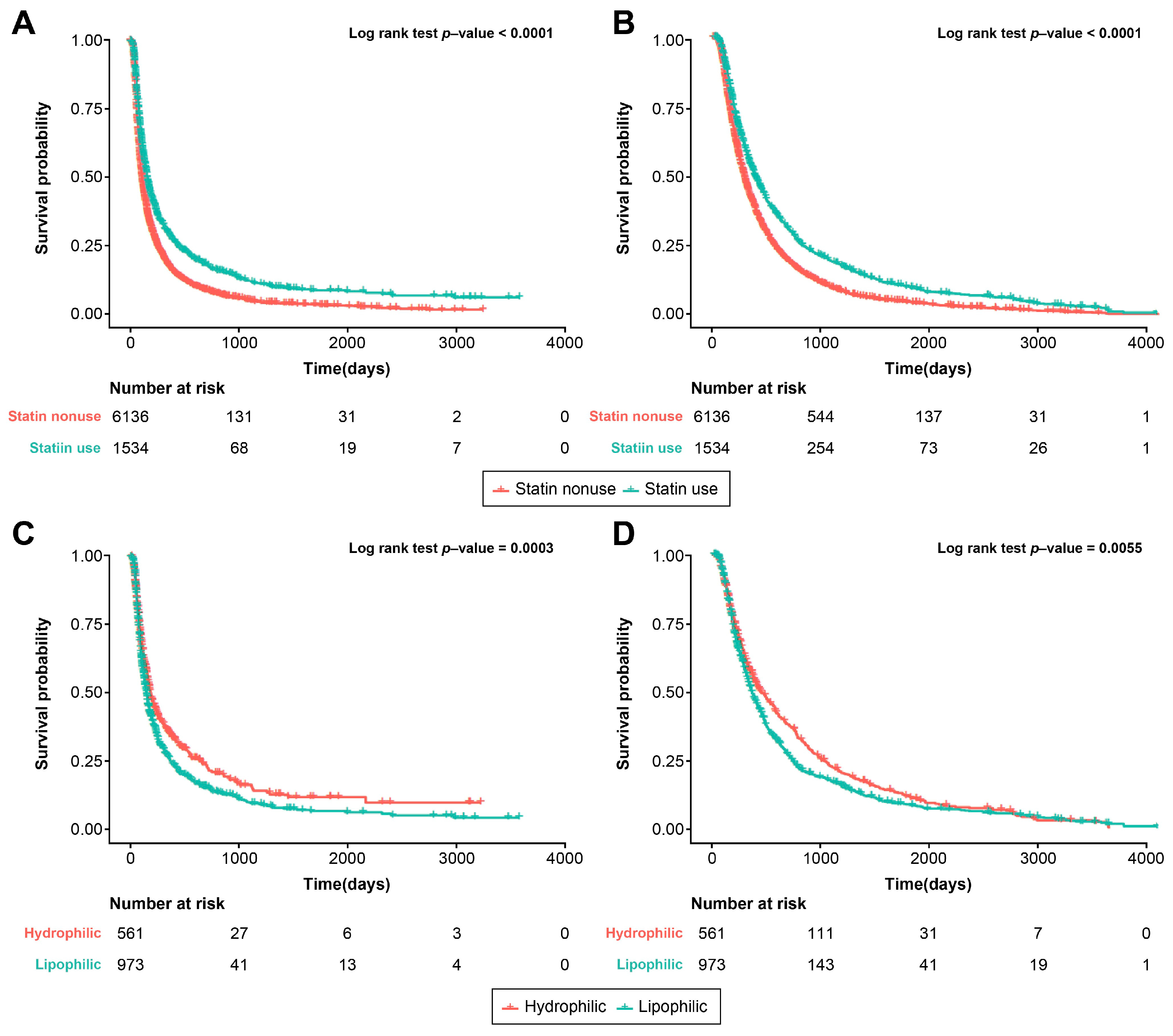
3.2. Statin Use and Survival Outcome
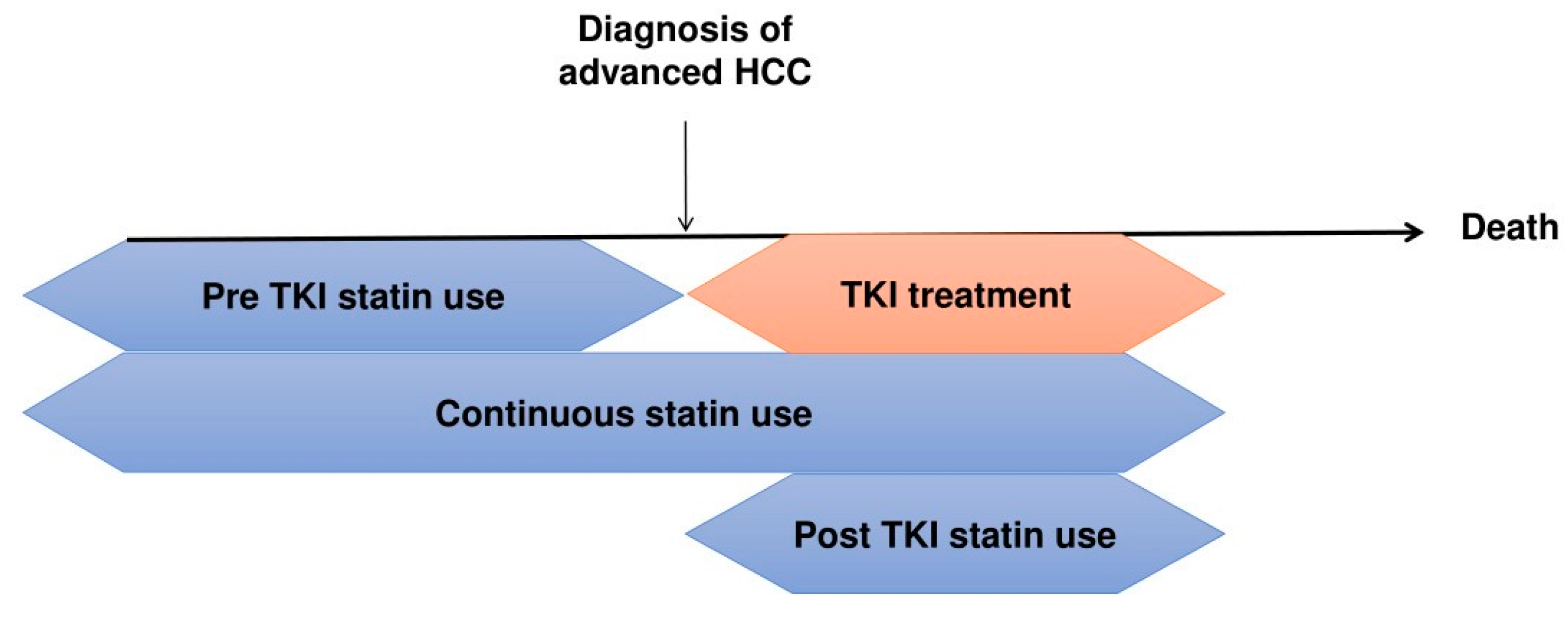
3.3. The Timing of Statin Use and Survival Outcome
3.4. Statin Type and Survival Outcome
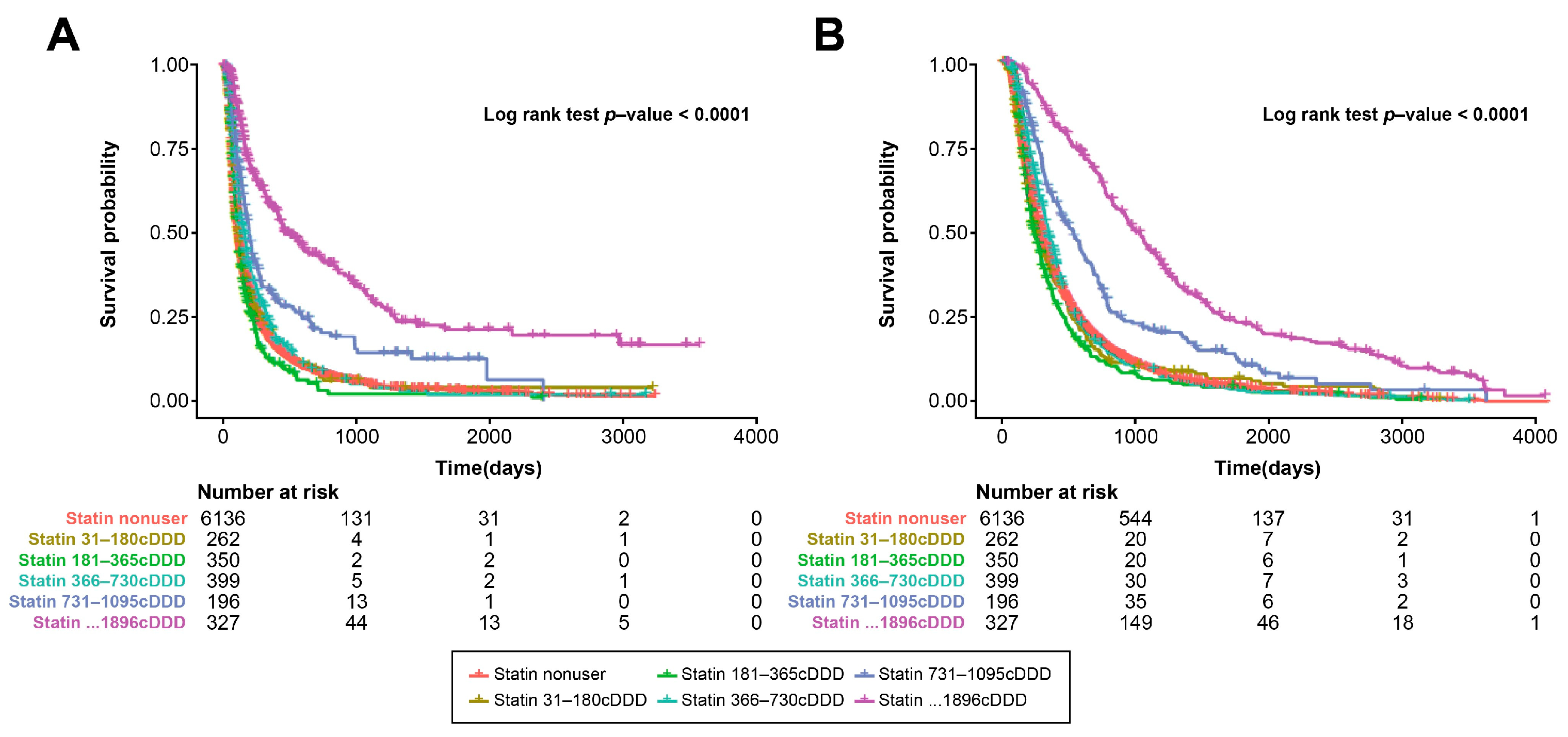
3.5. Statin Dose and Survival Outcome
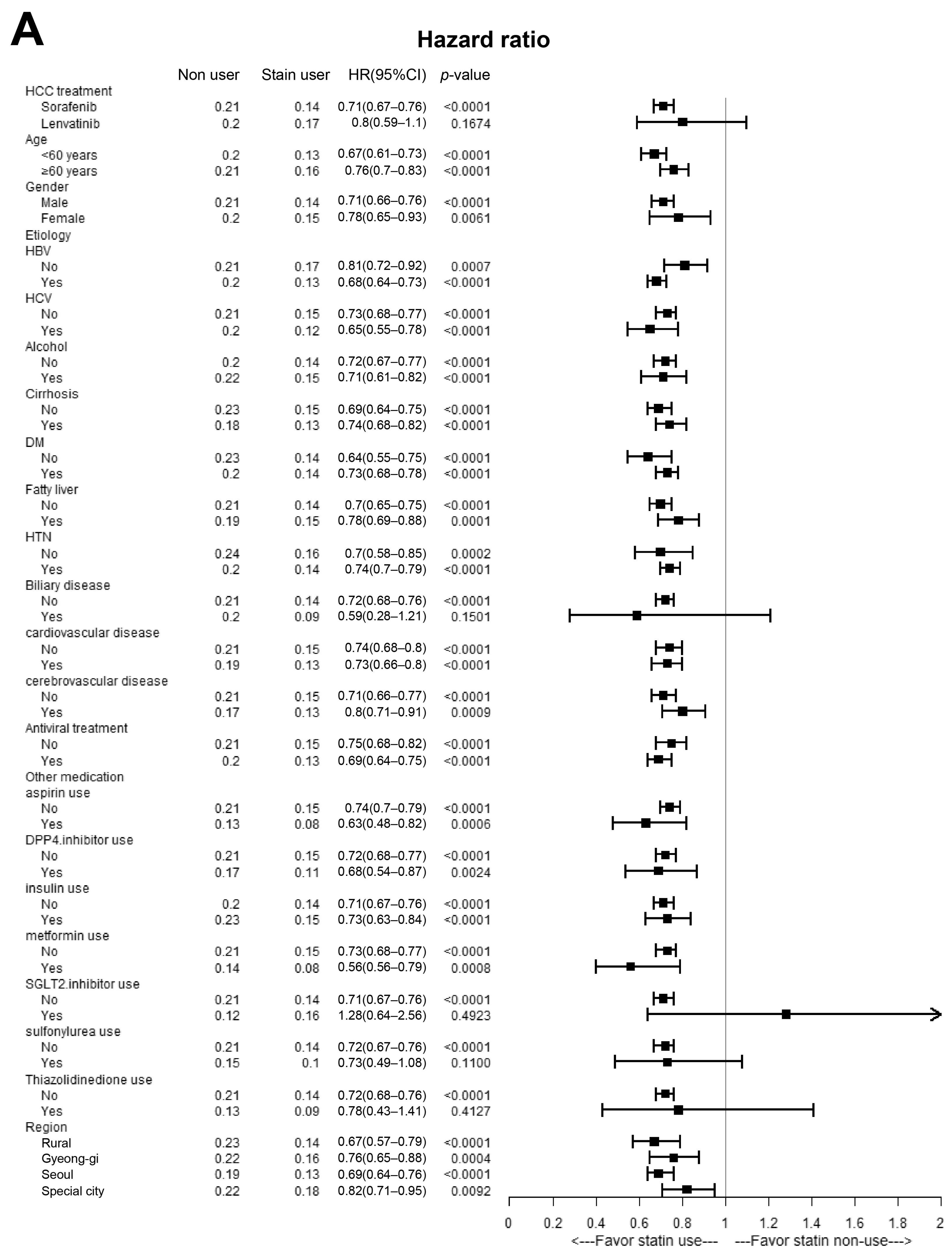
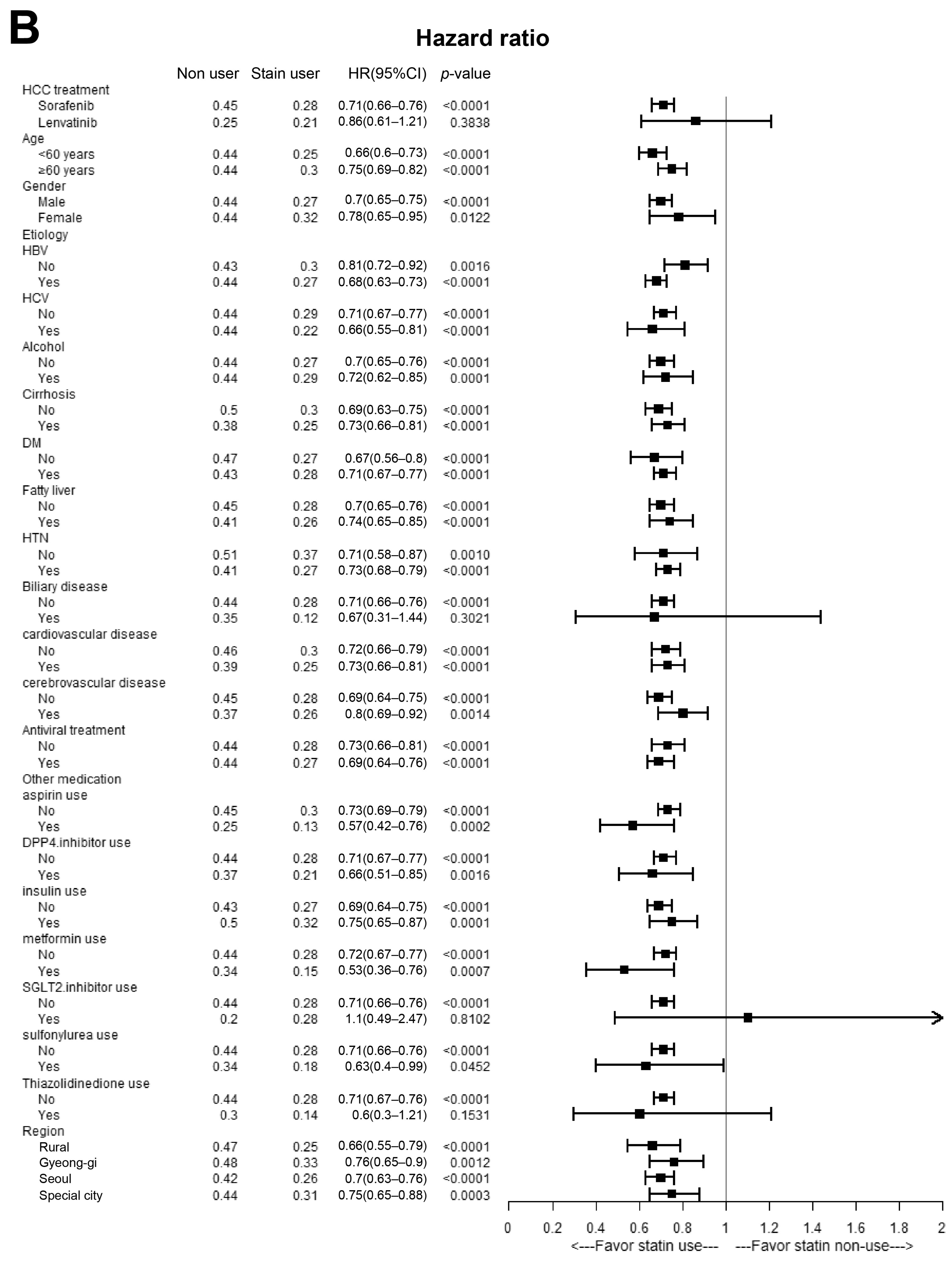
3.6. Multivariate Stratified Analysis
3.7. Subgroup Analysis according to Sorafenib or Lenvatinib Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rumgay, H.; Arnold, M.; Ferlay, J.; Lesi, O.; Cabasag, C.J.; Vignat, J.; Laversanne, M.; McGlynn, K.A.; Soerjomataram, I. Global burden of primary liver cancer in 2020 and predictions to 2040. J. Hepatol. 2022, 77, 1598–1606. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef]
- Cheng, A.L.; Kang, Y.K.; Chen, Z.; Tsao, C.J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Méndez-Blanco, C.; Fondevila, F.; García-Palomo, A.; González-Gallego, J.; Mauriz, J.L. Sorafenib resistance in hepatocarcinoma: Role of hypoxia-inducible factors. Exp. Mol. Med. 2018, 50, 1–9. [Google Scholar] [CrossRef]
- Göbel, A.; Zinna, V.M.; Dell’Endice, S.; Jaschke, N.; Kuhlmann, J.D.; Wimberger, P.; Rachner, T.D. Anti-tumor effects of mevalonate pathway inhibition in ovarian cancer. BMC Cancer 2020, 20, 703. [Google Scholar] [CrossRef]
- Ricco, N.; Flor, A.; Wolfgeher, D.; Efimova, E.V.; Ramamurthy, A.; Appelbe, O.K.; Brinkman, J.; Truman, A.W.; Spiotto, M.T.; Kron, S.J. Mevalonate pathway activity as a determinant of radiation sensitivity in head and neck cancer. Mol. Oncol. 2019, 13, 1927–1943. [Google Scholar] [CrossRef]
- Tan, X.L.; E, J.Y.; Lin, Y.; Rebbeck, T.R.; Lu, S.E.; Shang, M.; Kelly, W.K.; D’Amico, A.; Stein, M.N.; Zhang, L.; et al. Individual and joint effects of metformin and statins on mortality among patients with high-risk prostate cancer. Cancer Med. 2020, 9, 2379–2389. [Google Scholar] [CrossRef]
- Piekuś-Słomka, N.; Mocan, L.P.; Shkreli, R.; Grapă, C.; Denkiewicz, K.; Wesolowska, O.; Kornek, M.; Spârchez, Z.; Słomka, A.; Crăciun, R.; et al. Don’t Judge a Book by Its Cover: The Role of Statins in Liver Cancer. Cancers 2023, 15, 5100. [Google Scholar] [CrossRef]
- Goh, M.J.; Sinn, D.H.; Kim, S.; Woo, S.Y.; Cho, H.; Kang, W.; Gwak, G.Y.; Paik, Y.H.; Choi, M.S.; Lee, J.H.; et al. Statin use and the risk of hepatocellular carcinoma in patients with chronic hepatitis B. Hepatology 2020, 71, 2023–2032. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.Y.; Zhu, G.Q.; Wang, Y.; Zheng, J.N.; Ruan, L.Y.; Cheng, Z.; Hu, B.; Fu, S.W.; Zheng, M.H. Systematic review with network meta-analysis: Statins and risk of hepatocellular carcinoma. Oncotarget 2016, 7, 21753–21762. [Google Scholar] [CrossRef] [PubMed]
- Lai, S.W.; Liao, K.F.; Lai, H.C.; Muo, C.H.; Sung, F.C.; Chen, P.C. Statin use and risk of hepatocellular carcinoma. Eur. J. Epidemiol. 2013, 28, 485–492. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W.; Joo, Y.S.; Kang, S.C.; Koh, H.B.; Han, S.H.; Yoo, T.H.; Kang, S.W.; Park, J.T. Association of statin treatment with hepatocellular carcinoma risk in end-stage kidney disease patients with chronic viral hepatitis. Sci. Rep. 2022, 12, 10807. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; Duberg, A.S.; Aleman, S.; Hagstrom, H.; Nguyen, L.H.; Khalili, H.; Chung, R.T.; Ludvigsson, J.F. Lipophilic statins and risk for hepatocellular carcinoma and death in patients with chronic viral hepatitis: Results from a nationwide Swedish population. Ann. Intern. Med. 2019, 171, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Singh, P.P.; Roberts, L.R.; Sanchez, W. Chemopreventive strategies in hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2014, 11, 45–54. [Google Scholar] [CrossRef]
- Nishio, T.; Taura, K.; Nakamura, N.; Seo, S.; Yasuchika, K.; Kaido, T.; Okajima, H.; Hatano, E.; Uemoto, S. Impact of statin use on the prognosis of patients with hepatocellular carcinoma undergoing liver resection: A subgroup analysis of patients without chronic hepatitis viral infection. Surgery 2018, 163, 264–269. [Google Scholar] [CrossRef]
- Yang, S.Y.; Wang, C.C.; Chen, K.D.; Liu, Y.W.; Lin, C.C.; Chuang, C.H.; Tsai, Y.C.; Yao, C.C.; Yen, Y.H.; Hsiao, C.C.; et al. Statin use is associated with a lower risk of recurrence after curative resection in BCLC stage 0-A hepatocellular carcinoma. BMC Cancer 2021, 21, 70. [Google Scholar] [CrossRef]
- Su, V.Y.; Yang, K.Y.; Huang, T.Y.; Hsu, C.C.; Chen, Y.M.; Yen, J.C.; Chou, Y.C.; Chang, Y.L.; He, C.H. The efficacy of first-line tyrosine kinase inhibitors combined with co-medications in Asian patients with EGFR mutation non-small cell lung cancer. Sci. Rep. 2020, 10, 14965. [Google Scholar] [CrossRef]
- Matusewicz, L.; Czogalla, A.; Sikorski, A.F. Attempts to use statins in cancer therapy: An update. Tumour Biol. 2020, 42, 1010428320941760. [Google Scholar] [CrossRef]
- Woodard, J.; Joshi, S.; Viollet, B.; Hay, N.; Platanias, L.C. AMPK as a therapeutic target in renal cell carcinoma. Cancer Biol. Ther. 2010, 10, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.J.; Woo, Y.M.; Naka, K.; Park, J.H.; Han, H.J.; Kim, H.J.; Kim, S.H.; Ahn, J.S.; Kim, T.; Kimura, S.; et al. Statins enhance the molecular response in chronic myeloid leukemia when combined with tyrosine kinase inhibitors. Cancers 2021, 13, 5543. [Google Scholar] [CrossRef] [PubMed]
- Hung, M.S.; Chen, I.C.; Lee, C.P.; Huang, R.J.; Chen, P.C.; Tsai, Y.H.; Yang, Y.H. Statin improves survival in patients with EGFR-TKI lung cancer: A nationwide population-based study. PLoS ONE 2017, 12, e0171137. [Google Scholar] [CrossRef] [PubMed]
- Lebo, N.L.; Griffiths, R.; Hall, S.; Dimitroulakos, J.; Johnson-Obaseki, S. Effect of statin use on oncologic outcomes in head and neck squamous cell carcinoma. Head Neck 2018, 40, 1697–1706. [Google Scholar] [CrossRef] [PubMed]
- Pose, E.; Trebicka, J.; Mookerjee, R.P.; Angeli, P.; Ginès, P. Statins: Old drugs as new therapy for liver diseases? J. Hepatol. 2019, 70, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, E.; Jacobsen, E.I.; Kalaitzakis, E. Hepatotoxicity associated with statins: Reports of idiosyncratic liver injury post-marketing. J. Hepatol. 2012, 56, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, D.E.; Serper, M.A.; Mehta, R.; Fox, R.; John, B.; Aytaman, A.; Baytarian, M.; Hunt, K.; Albrecht, J.; Njei, B.; et al. Effects of hypercholesterolemia and statin exposure on survival in a large national cohort of patients with cirrhosis. Gastroenterology 2019, 156, 1693–1706.e12. [Google Scholar] [CrossRef]
- Abraldes, J.G.; Villanueva, C.; Aracil, C.; Turnes, J.; Hernandez-Guerra, M.; Genesca, J.; Rodriguez, M.; Castellote, J.; García-Pagán, J.C.; Torres, F.; et al. Addition of simvastatin to standard therapy for the prevention of variceal rebleeding does not reduce rebleeding but increases survival in patients with cirrhosis. Gastroenterology 2016, 150, 1160–1170.e3. [Google Scholar] [CrossRef]
- Mahmud, N.; Chapin, S.; Goldberg, D.S.; Reddy, K.R.; Taddei, T.H.; Kaplan, D.E. Statin exposure is associated with reduced development of acute-on-chronic liver failure in a Veterans Affairs cohort. J. Hepatol. 2022, 76, 1100–1108. [Google Scholar] [CrossRef]
- Kim, J.; Kundu, M.; Viollet, B.; Guan, K.L. AMPK and mTOR regulate autophagy through direct phosphorylation of Ulk1. Nat. Cell Biol. 2011, 13, 132–141. [Google Scholar] [CrossRef]
- Chen, K.F.; Chen, H.L.; Tai, W.T.; Feng, W.C.; Hsu, C.H.; Chen, P.J.; Cheng, A.L. Activation of phosphatidylinositol 3-kinase/Akt signaling pathway mediates acquired resistance to sorafenib in hepatocellular carcinoma cells. J. Pharmacol. Exp. Ther. 2011, 337, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xu, L.; Zhu, X.; Wang, P.; Chi, H.; Meng, Z. Activation of phosphatidylinositol 3-kinase/Akt signaling mediates sorafenib-induced invasion and metastasis in hepatocellular carcinoma. Oncol. Rep. 2014, 32, 1465–1472. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.P.; Ho, R.L.; Chen, G.G.; Lai, P.B. Sorafenib inhibits hypoxia-inducible factor-1α synthesis: Implications for antiangiogenic activity in hepatocellular carcinoma. Clin. Cancer Res. 2012, 18, 5662–5671. [Google Scholar] [CrossRef]
- Zhao, D.; Zhai, B.; He, C.; Tan, G.; Jiang, X.; Pan, S.; Dong, X.; Wei, Z.; Ma, L.; Qiao, H.; et al. Upregulation of HIF-2α induced by sorafenib contributes to the resistance by activating the TGF-α/EGFR pathway in hepatocellular carcinoma cells. Cell. Signal. 2014, 26, 1030–1039. [Google Scholar] [CrossRef] [PubMed]
- Long, Q.; Zou, X.; Song, Y.; Duan, Z.; Liu, L. PFKFB3/HIF-1α feedback loop modulates sorafenib resistance in hepatocellular carcinoma cells. Biochem. Biophys. Res. Commun. 2019, 513, 642–650. [Google Scholar] [CrossRef] [PubMed]
- Liang, C.; Dong, Z.; Cai, X.; Shen, J.; Xu, Y.; Zhang, M.; Li, H.; Yu, W.; Chen, W. Hypoxia induces sorafenib resistance mediated by autophagy via activating FOXO3a in hepatocellular carcinoma. Cell Death Dis. 2020, 11, 1017. [Google Scholar] [CrossRef] [PubMed]
- Blanc, J.F.; Khemissa, F.; Bronowicki, J.P.; Monterymard, C.; Perarnau, J.M.; Bourgeois, V.; Obled, S.; Abdelghani, M.B.; Mabile-Archambeaud, I.; Faroux, R.; et al. Phase 2 trial comparing sorafenib, pravastatin, their combination or supportive care in HCC with Child-Pugh B cirrhosis. Hepatol. Int. 2021, 15, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Dai, W.; Mao, Y.; Wu, L.; Li, J.; Chen, K.; Yu, Q.; Kong, R.; Li, S.; Zhang, J.; et al. Simvastatin re-sensitizes hepatocellular carcinoma cells to sorafenib by inhibiting HIF-1α/PPAR-γ/PKM2-mediated glycolysis. J. Exp. Clin. Cancer Res. 2020, 39, 24. [Google Scholar] [CrossRef]
- Zhang, S.; Doudican, N.A.; Quay, E.; Orlow, S.J. Fluvastatin enhances sorafenib cytotoxicity in melanoma cells via modulation of AKT and JNK signaling pathways. Anticancer Res. 2011, 31, 3259–3265. [Google Scholar]
- Cheng, Y.; Luo, R.; Zheng, H.; Wang, B.; Liu, Y.; Liu, D.; Chen, J.; Xu, W.; Li, A.; Zhu, Y. Synergistic anti-tumor efficacy of sorafenib and fluvastatin in hepatocellular carcinoma. Oncotarget 2017, 8, 23265–23276. [Google Scholar] [CrossRef]
- Hisada, T.; Ayaori, M.; Ohrui, N.; Nakashima, H.; Nakaya, K.; Uto-Kondo, H.; Yakushiji, E.; Takiguchi, S.; Terao, Y.; Miyamoto, Y.; et al. Statin inhibits hypoxia-induced endothelin-1 via accelerated degradation of HIF-1α in vascular smooth muscle cells. Cardiovasc. Res. 2012, 95, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Hijona, E.; Banales, J.M.; Hijona, L.; Medina, J.F.; Arenas, J.; Herreros-Villanueva, M.; Aldazabal, P.; Bujanda, L. Pravastatin inhibits cell proliferation and increased MAT1A expression in hepatocarcinoma cells and in vivo models. Cancer Cell Int. 2012, 12, 5. [Google Scholar] [CrossRef] [PubMed]
- Riaño, I.; Martín, L.; Varela, M.; Serrano, T.; Núñez, O.; Mínguez, B.; Rodrigues, P.M.; Perugorria, M.J.; Banales, J.M.; Arenas, J.I. Efficacy and safety of the combination of pravastatin and sorafenib for the treatment of advanced hepatocellular carcinoma (ESTAHEP clinical trial). Cancers 2020, 12, 1900. [Google Scholar] [CrossRef] [PubMed]
- Jouve, J.L.; Lecomte, T.; Bouché, O.; Barbier, E.; Khemissa Akouz, F.; Riachi, G.; Nguyen Khac, E.; Ollivier-Hourmand, I.; Debette-Gratien, M.; Faroux, R.; et al. Pravastatin combination with sorafenib does not improve survival in advanced hepatocellular carcinoma. J. Hepatol. 2019, 71, 516–522. [Google Scholar] [CrossRef] [PubMed]
- Kawata, S.; Yamasaki, E.; Nagase, T.; Inui, Y.; Ito, N.; Matsuda, Y.; Inada, M.; Tamura, S.; Noda, S.; Imai, Y.; et al. Effect of pravastatin on survival in patients with advanced hepatocellular carcinoma. A randomized controlled trial. Br. J. Cancer 2001, 84, 886–891. [Google Scholar] [CrossRef]
- Thrift, A.P.; Natarajan, Y.; Liu, Y.; El-Serag, H.B. Statin use after diagnosis of hepatocellular carcinoma is associated with decreased mortality. Clin. Gastroenterol. Hepatol. 2019, 17, 2117–2125.e3. [Google Scholar] [CrossRef]
- Lauschke, V.M.; Ingelman-Sundberg, M. The importance of patient-specific factors for hepatic drug response and toxicity. Int. J. Mol. Sci. 2016, 17, 1714. [Google Scholar] [CrossRef]
- Goh, M.J.; Sinn, D.H. Statin and aspirin for chemoprevention of hepatocellular carcinoma: Time to use or wait further? Clin. Mol. Hepatol. 2022, 28, 380–395. [Google Scholar] [CrossRef]
- Zeng, R.W.; Yong, J.N.; Tan, D.J.H.; Fu, C.E.; Lim, W.H.; Xiao, J.; Chan, K.E.; Tan, C.; Goh, X.L.; Chee, D.; et al. Meta-analysis: Chemoprevention of hepatocellular carcinoma with statins, aspirin and metformin. Aliment. Pharmacol. Ther. 2023, 57, 600–609. [Google Scholar] [CrossRef]
- Hsu, W.H.; Sue, S.P.; Liang, H.L.; Tseng, C.W.; Lin, H.C.; Wen, W.L.; Lee, M.Y. Dipeptidyl peptidase 4 inhibitors decrease the risk of hepatocellular carcinoma in patients with chronic hepatitis C infection and type 2 diabetes mellitus: A nationwide study in Taiwan. Front. Public. Health 2021, 9, 711723. [Google Scholar] [CrossRef]
- Nishina, S.; Yamauchi, A.; Kawaguchi, T.; Kaku, K.; Goto, M.; Sasaki, K.; Hara, Y.; Tomiyama, Y.; Kuribayashi, F.; Torimura, T.; et al. Dipeptidyl peptidase 4 inhibitors reduce hepatocellular carcinoma by activating lymphocyte chemotaxis in mice. Cell. Mol. Gastroenterol. Hepatol. 2019, 7, 115–134. [Google Scholar] [CrossRef] [PubMed]
- Shan, Y.; Lu, C.; Wang, J.; Li, M.; Ye, S.; Wu, S.; Huang, J.; Bu, S.; Wang, F. IGF-1 contributes to liver cancer development in diabetes patients by promoting autophagy. Ann. Hepatol. 2022, 27, 100697. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before PS-Matching | After PS-Matching | |||||
|---|---|---|---|---|---|---|
| Non-Users (n = 11,062) | Statin Users (n = 1534) | p-Value | Non-Users (n = 6136) | Statin Users (n = 1534) | p-Value | |
| Age | 56.48 (8.28) | 59.87 (7.29) | <0.001 | 59.363 (7.013) | 59.870 (7.290) | 0.012 |
| Sex, male, No. (%) | 9652 (87.3%) | 1359 (88.6%) | 0.139 | 5439 (88.6%) | 1359 (88.6%) | 0.957 |
| Region, No. (%) | 0.033 | 0.004 | ||||
| Rural | 1542 (13.9%) | 202 (13.2%) | 912 (14.9%) | 202 (13.2%) | ||
| Gyeong-gi | 1721 (15.6%) | 242 (15.8%) | 906 (14.8%) | 242 (15.8%) | ||
| Seoul | 5590 (50.5%) | 826 (53.8%) | 3066 (50.0%) | 826 (53.8%) | ||
| Special city | 2209 (20.0%) | 264 (17.2%) | 1252 (20.4%) | 264 (17.2%) | ||
| HCC treatment, No. (%) | 0.010 | 0.021 | ||||
| Sorafenib | 10,308 (93.2%) | 1402 (91.4%) | 5713 (93.1%) | 1402 (91.4%) | ||
| Lenvatinib | 754 (6.8%) | 132 (8.6%) | 423 (6.9%) | 132 (8.6%) | ||
| Statin use pattern, No. (%) | - | - | ||||
| Pre-TKI use | - | 218 (14.2%) | - | 218 (14.2%) | ||
| Continuous use from TKI treatment | - | 950 (61.9%) | - | 950 (61.9%) | ||
| Post-TKI use | - | 366 (23.9%) | - | 366 (23.9%) | ||
| Etiology, No. (%) | ||||||
| HBV | 9363 (84.6%) | 1109 (72.3%) | <0.001 | 4818 (78.5%) | 1109 (72.3%) | <0.001 |
| HCV | 1368 (12.4%) | 185 (12.1%) | 0.732 | 793 (12.9%) | 185 (12.1%) | 0.364 |
| Alcoholic | 1472 (13.3%) | 263 (17.1%) | <0.001 | 972 (15.8%) | 263 (17.1%) | 0.214 |
| History of comorbidities | ||||||
| History of DM, No. (%) | 6413 (58.0%) | 1303 (84.9%) | <0.001 | 5163 (84.1%) | 1303 (84.9%) | 0.442 |
| History of fatty liver, No. (%) | 1735 (15.7%) | 415 (27.1%) | <0.001 | 1352 (22.0%) | 415 (27.1%) | <0.001 |
| History of cirrhosis, No. (%) | 4832 (43.7%) | 713 (46.5%) | 0.0385 | 2892(47.1%) | 713(46.5%) | 0.647 |
| History of HTN, No. (%) | 7067 (63.9%) | 1397 (91.1%) | <0.001 | 4433 (72.2%) | 1397 (91.1%) | <0.001 |
| History of PBC, No. (%) | 52 (0.5%) | 17 (1.1%) | 0.002 | 45 (0.7%) | 17 (1.1%) | 0.143 |
| History of cardiovascular disease, No. (%) | 2448 (22.1%) | 717 (46.7%) | <0.001 | 1614 (26.3%) | 717 (46.7%) | <0.001 |
| History of cerebrovascular disease, No. (%) | 970 (8.8%) | 437 (28.5%) | <0.001 | 718 (11.7%) | 437 (28.5%) | <0.001 |
| Antiviral treatment, No. (%) | ||||||
| HBV treatment | 7752 (70.1%) | 842 (54.9%) | <0.001 | 3905 (63.6%) | 842 (54.9%) | <0.001 |
| HCV treatment | 248 (2.2%) | 47 (3.1%) | 0.046 | 793 (12.9%) | 185 (12.1%) | 0.364 |
| Other medication, No. (%) | ||||||
| Aspirin use | 264 (2.4%) | 106 (6.9%) | <0.001 | 158 (2.6%) | 106 (6.9%) | <0.001 |
| DPP-4 inhibitor use | 279 (2.5%) | 109 (7.1%) | <0.001 | 241 (3.9%) | 109 (7.1%) | <0.001 |
| Insulin use | 1717 (15.5%) | 285 (18.6%) | 0.002 | 1010 (16.5%) | 285 (18.6%) | 0.048 |
| Metformin use | 229 (2.1%) | 54 (3.5%) | <0.001 | 173 (2.8%) | 54 (3.5%) | 0.147 |
| SGLT-2 inhibitor use | 27 (0.2%) | 18 (1.2%) | <0.001 | 25 (0.4%) | 18 (1.2%) | <0.001 |
| Sulfonylurea use | 131 (1.2%) | 38 (2.5%) | <0.001 | 109 (1.8%) | 38 (2.5%) | 0.073 |
| Thiazolidinedione use | 43 (0.4%) | 21 (1.4%) | <0.001 | 36 (0.6%) | 21 (1.4%) | 0.001 |
| Median treatment duration (days) | 260.00 (149.00, 498.00) | 337.00 (180.00, 708.00) | <0.001 | 269.00 (152.00, 512.00) | 337.00 (180.00, 708.00) | <0.001 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Statin use, yes | 0.71 | 0.66–0.76 | <0.001 | 0.77 | 0.72–0.82 | <0.001 |
| Age, ≥60 years | 0.99 | 0.94–1.04 | 0.624 | 1.00 | 1.00–1.01 | 0.469 |
| Sex, female | 0.93 | 0.86–1.01 | 0.080 | 0.95 | 0.88–1.03 | 0.205 |
| Region, urban | 0.96 | 0.89–1.03 | 0.249 | |||
| DM, yes | 0.92 | 0.86–0.99 | 0.022 | 0.94 | 0.87–1.01 | 0.086 |
| HTN, yes | 0.80 | 0.75–0.85 | <0.001 | 0.87 | 0.82–0.92 | <0.001 |
| Cardiovascular disease, yes | 0.86 | 0.81–0.91 | <0.001 | 0.93 | 0.88–0.98 | 0.010 |
| Cerebrovascular disease, yes | 0.86 | 0.80–0.92 | <0.001 | |||
| Fatty liver, yes | 0.90 | 0.84–0.96 | 0.001 | 0.95 | 0.89–1.01 | 0.081 |
| Cirrhosis, yes | 0.80 | 0.76-0.84 | <0.001 | |||
| Aspirin, yes | 0.61 | 0.53–0.70 | <0.001 | 0.64 | 0.55–0.74 | <0.001 |
| DPP-4 inhibitor use, yes | 0.85 | 0.75–0.95 | 0.006 | |||
| Insulin use, yes | 1.14 | 1.07–1.22 | <0.001 | 1.24 | 1.16–1.33 | <0.001 |
| Metformin use, yes | 0.75 | 0.65–0.87 | <0.001 | 0.78 | 0.67–0.91 | 0.002 |
| SGLT-2 inhibitor use, yes | 0.60 | 0.41–0.88 | 0.01 | 0.67 | 0.45–0.99 | 0.044 |
| Sulfonylurea use, yes | 0.76 | 0.63–0.91 | 0.003 | 0.81 | 0.67–0.99 | 0.037 |
| Thiazolidinedione use, yes | 0.65 | 0.47–0.89 | 0.007 | 0.79 | 0.57–1.09 | 0.150 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Statin use, yes | 0.72 | 0.67–0.76 | <0.001 | 0.78 | 0.74–0.84 | <0.001 |
| Age, ≥60 years | 1.04 | 0.99–1.09 | 0.156 | 1.01 | 1.00–1.01 | 0.006 |
| Sex, female | 0.98 | 0.91–1.06 | 0.603 | 1.01 | 0.94–1.09 | 0.825 |
| Region, urban | 0.88 | 0.82–0.94 | <0.001 | 0.87 | 0.81–0.93 | <0.001 |
| DM, yes | 0.91 | 0.85–0.98 | 0.007 | 0.95 | 0.88–1.01 | 0.104 |
| Fatty liver, yes | 0.94 | 0.89–1.00 | 0.054 | |||
| Cirrhosis, yes | 0.82 | 0.79-0.86 | <0.001 | |||
| HTN, yes | 0.80 | 0.75–0.84 | <0.001 | 0.86 | 0.81–0.91 | <0.001 |
| Cardiovascular disease, yes | 0.84 | 0.79–0.88 | <0.001 | 0.90 | 0.86–0.96 | <0.001 |
| Cerebrovascular disease, yes | 0.81 | 0.76–0.87 | <0.001 | 0.90 | 0.84–0.97 | 0.004 |
| Aspirin use, yes | 0.57 | 0.50–0.65 | <0.001 | 0.63 | 0.55–0.73 | <0.001 |
| DPP-4 inhibitor use, yes | 0.78 | 0.70–0.88 | <0.001 | 0.90 | 0.80–1.01 | 0.085 |
| Insulin use, yes | 1.13 | 1.06–1.20 | <0.001 | 1.26 | 1.18–1.35 | <0.001 |
| Metformin use, yes | 0.68 | 0.59–0.78 | <0.001 | 0.72 | 0.62–0.84 | <0.001 |
| SGLT-2 inhibitor use, yes | 0.70 | 0.50–0.98 | 0.038 | 0.77 | 0.54–1.07 | 0.123 |
| Sulfonylurea use, yes | 0.73 | 0.61–0.86 | <0.001 | 0.83 | 0.69–1.00 | 0.049 |
| Thiazolidinedione use, yes | 0.64 | 0.49–0.85 | 0.002 | 0.80 | 0.60–1.06 | 0.114 |
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Statin use pattern | ||||||
| Non-user | reference | reference | ||||
| Pre-TKI use | 1.31 | 1.13–1.52 | <0.001 | 1.33 | 1.14–1.54 | <0.001 |
| Continuous use from TKI treatment | 0.80 | 0.74–0.87 | <0.001 | 0.87 | 0.80–0.95 | 0.002 |
| Post-TKI use | 0.40 | 0.35–0.46 | <0.001 | 0.43 | 0.38–0.50 | <0.001 |
| Age, ≥60 years | 0.99 | 0.94–1.04 | 0.624 | 1.00 | 1.00–1.00 | 0.767 |
| Sex, female | 0.93 | 0.86–1.01 | 0.080 | 0.95 | 0.88–1.03 | 0.246 |
| Region, urban | 0.96 | 0.89–1.03 | 0.249 | |||
| DM, yes | 0.92 | 0.86–0.99 | 0.022 | 0.93 | 0.87–1.00 | 0.048 |
| Fatty liver, yes | 0.90 | 0.84–0.96 | <0.001 | 0.94 | 0.88–1.00 | 0.050 |
| Cirrhosis, yes | 0.80 | 0.76-0.84 | <0.001 | |||
| HTN, yes | 0.80 | 0.75–0.85 | <0.001 | 0.87 | 0.82–0.92 | <0.001 |
| Cardiovascular disease, yes | 0.86 | 0.81–0.91 | <0.001 | 0.93 | 0.88–0.99 | 0.016 |
| Cerebrovascular disease, yes | 0.86 | 0.80–0.92 | <0.001 | |||
| Aspirin use, yes | 0.61 | 0.53–0.70 | <0.001 | 0.69 | 0.59–0.79 | <0.001 |
| DPP-4 inhibitor use, yes | 0.85 | 0.75–0.95 | 0.006 | 0.90 | 0.80–1.03 | 0.119 |
| Insulin use, yes | 1.14 | 1.07–1.22 | <0.001 | 1.23 | 1.15–1.32 | <0.001 |
| Metformin use, yes | 0.68 | 0.59–0.78 | <0.001 | 0.83 | 0.71–0.97 | 0.022 |
| SGLT-2 inhibitor use, yes | 0.60 | 0.41–0.88 | 0.010 | 0.66 | 0.45–0.98 | 0.038 |
| Sulfonylurea use, yes | 0.76 | 0.63–0.91 | 0.003 | 0.79 | 0.65–0.96 | 0.020 |
| Thiazolidinedione use, yes | 0.65 | 0.47–0.89 | 0.007 | |||
| Variables | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Statin use pattern | ||||||
| Non-user | reference | reference | ||||
| Pre-TKI use | 1.53 | 1.33–1.77 | <0.001 | 1.56 | 1.35–1.80 | <0.001 |
| Continuous use from TKI treatment | 0.86 | 0.80–0.93 | <0.001 | 0.94 | 0.87–1.02 | 0.122 |
| Post-TKI use | 0.38 | 0.34–0.43 | <0.001 | 0.42 | 0.38–0.48 | <0.001 |
| Age ≥60 years | 1.04 | 0.99–1.09 | 0.156 | 1.00 | 1.00–1.01 | 0.032 |
| Sex, female | 0.98 | 0.91–1.06 | 0.603 | 1.02 | 0.95–1.10 | 0.571 |
| Region, urban | 0.88 | 0.82–0.94 | <0.001 | 0.86 | 0.80–0.92 | <0.001 |
| DM, yes | 0.91 | 0.85–0.98 | 0.007 | 0.92 | 0.86–0.99 | 0.023 |
| Fatty liver, yes | 0.94 | 0.89–1.00 | 0.054 | |||
| Cirrhosis, yes | 0.82 | 0.79-0.86 | <0.001 | |||
| HTN, yes | 0.80 | 0.75–0.84 | <0.001 | 0.86 | 0.81–0.91 | <0.001 |
| Cardiovascular disease, yes | 0.84 | 0.79–0.88 | <0.001 | 0.91 | 0.86–0.96 | 0.001 |
| Cerebrovascular disease, yes | 0.81 | 0.76–0.87 | <0.001 | 0.91 | 0.85–0.98 | 0.012 |
| Aspirin use, yes | 0.57 | 0.50–0.65 | <0.001 | 0.68 | 0.59–0.77 | <0.001 |
| DPP-4 inhibitor use, yes | 0.78 | 0.70–0.88 | <0.001 | 0.88 | 0.78–0.99 | 0.035 |
| Insulin use, yes | 1.13 | 1.06–1.20 | <0.001 | 1.25 | 1.17–1.33 | <0.001 |
| Metformin use, yes | 0.68 | 0.59–0.78 | <0.001 | 0.75 | 0.64–0.87 | <0.001 |
| SGLT-2 inhibitor use, yes | 0.70 | 0.50–0.98 | 0.038 | 0.74 | 0.53–1.03 | 0.077 |
| Sulfonylurea use, yes | 0.73 | 0.61–0.86 | <0.001 | 0.81 | 0.67–0.97 | 0.022 |
| Thiazolidinedione use, yes | 0.64 | 0.49–0.85 | 0.002 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, J.E.; Kim, J.; Cheong, J.Y.; Kim, S.S.; Lim, S.G.; Yang, M.J.; Noh, C.-K.; Lee, G.H.; Eun, J.W.; Park, B.; et al. The Impact of Statins on the Survival of Patients with Advanced Hepatocellular Carcinoma Treated with Sorafenib or Lenvatinib. Cancers 2024, 16, 249. https://doi.org/10.3390/cancers16020249
Han JE, Kim J, Cheong JY, Kim SS, Lim SG, Yang MJ, Noh C-K, Lee GH, Eun JW, Park B, et al. The Impact of Statins on the Survival of Patients with Advanced Hepatocellular Carcinoma Treated with Sorafenib or Lenvatinib. Cancers. 2024; 16(2):249. https://doi.org/10.3390/cancers16020249
Chicago/Turabian StyleHan, Ji Eun, Jisu Kim, Jae Youn Cheong, Soon Sun Kim, Sun Gyo Lim, Min Jae Yang, Choong-Kyun Noh, Gil Ho Lee, Jung Woo Eun, Bumhee Park, and et al. 2024. "The Impact of Statins on the Survival of Patients with Advanced Hepatocellular Carcinoma Treated with Sorafenib or Lenvatinib" Cancers 16, no. 2: 249. https://doi.org/10.3390/cancers16020249