
New Frontiers in Monoclonal Antibodies for Relapsed/Refractory Diffuse Large B-Cell Lymphoma
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
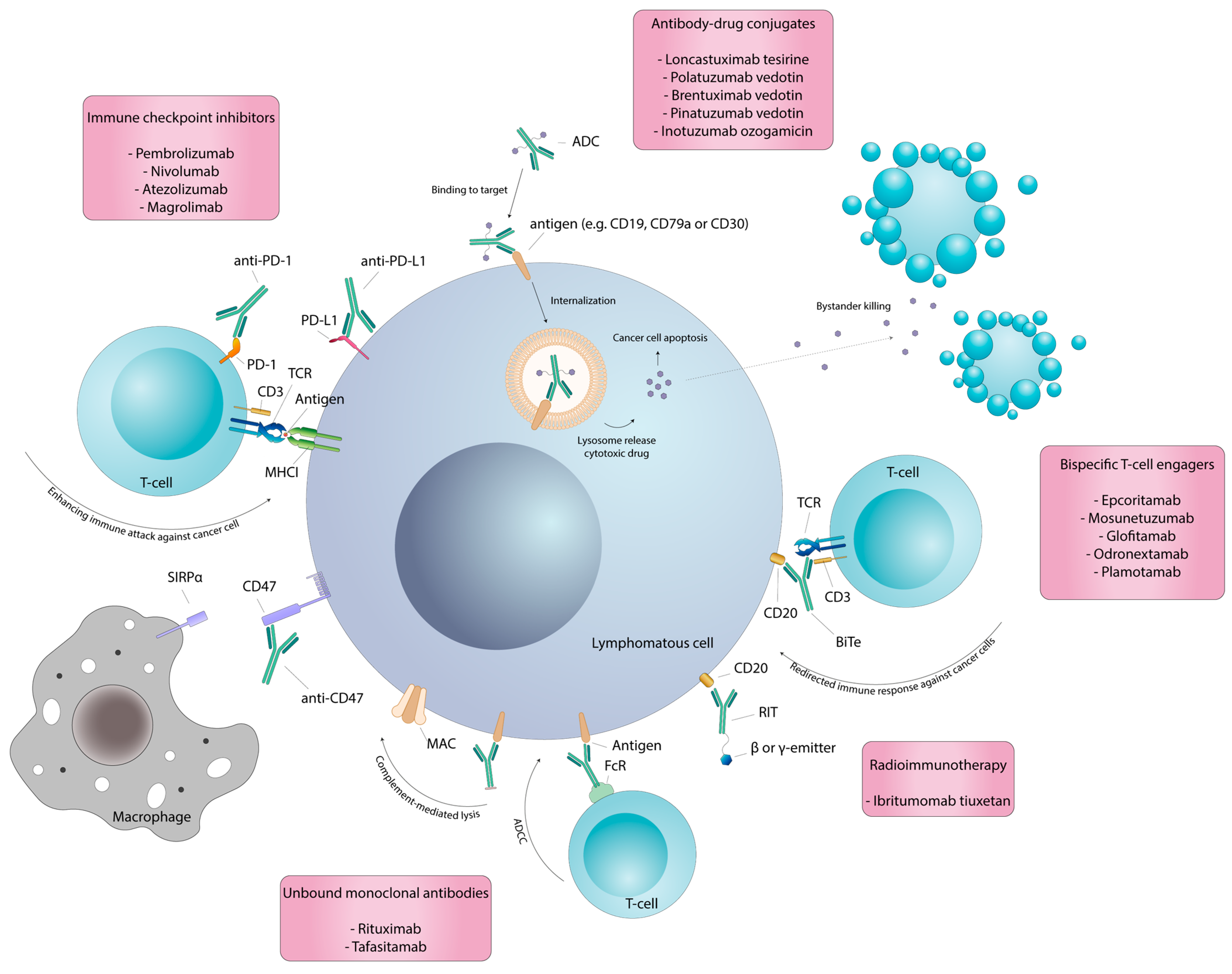
2. Monoclonal Antibodies
3. Unbound Monoclonal Antibodies
4. Bispecific Antibodies
5. Antibody–Drug Conjugates
6. Radioimmunotherapy
7. Immune Checkpoint Inhibitors
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Li, S.; Young, K.H.; Medeiros, L.J. Diffuse Large B-Cell Lymphoma. Pathology 2018, 50, 74–87. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.M.; Diebold, J.; Nathwani, B.N.; Maclennan, K.A.; Müller-Hermelink, H.K.; Bast, M.; Boilesen, E.; Armitage, J.O.; Weisenburger, D.D. Non-Hodgkin Lymphoma in the Developing World: Review of 4539 Cases from the International Non-Hodgkin Lymphoma Classification Project. Haematologica 2016, 101, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.; Crouch, S.; Lax, S.; Li, J.; Painter, D.; Howell, D.; Patmore, R.; Jack, A.; Roman, E. Lymphoma Incidence, Survival and Prevalence 2004–2014: Sub-Type Analyses from the UK’s Haematological Malignancy Research Network. Br. J. Cancer 2015, 112, 1575–1584. [Google Scholar] [CrossRef] [PubMed]
- Coiffier, B.; Lepage, E.; Brière, J.; Herbrecht, R.; Tilly, H.; Bouabdallah, R.; Morel, P.; Van Den Neste, E.; Salles, G.; Gaulard, P.; et al. Chop Chemotherapy plus Rituximab Compared with Chop Alone in Elderly Patients with Diffuse Large-B-Cell Lymphoma. N. Engl. J. Med. 2002, 346, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Barta, S.K. Diffuse Large B-Cell Lymphoma: 2019 Update on Diagnosis, Risk Stratification, and Treatment. Am. J. Hematol. 2019, 94, 604–616. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, D.; Hawkes, E.A.; Jack, A.; Qian, W.; Smith, P.; Mouncey, P.; Pocock, C.; Ardeshna, K.M.; Radford, J.A.; McMillan, A.; et al. Rituximab plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisolone in Patients with Newly Diagnosed Diffuse Large B-Cell Non-Hodgkin Lymphoma: A Phase 3 Comparison of Dose Intensification with 14-Day versus 21-Day Cycles. Lancet 2013, 381, 1817–1826. [Google Scholar] [CrossRef] [PubMed]
- Delarue, R.; Tilly, H.; Mounier, N.; Petrella, T.; Salles, G.; Thieblemont, C.; Bologna, S.; Ghesquières, H.; Hacini, M.; Fruchart, C.; et al. Dose-Dense Rituximab-CHOP Compared with Standard Rituximab-CHOP in Elderly Patients with Diffuse Large B-Cell Lymphoma (the LNH03-6B Study): A Randomised Phase 3 Trial. Lancet Oncol. 2013, 14, 525–533. [Google Scholar] [CrossRef]
- Bartlett, N.L.; Wilson, W.H.; Jung, S.H.; Hsi, E.D.; Maurer, M.J.; Pederson, L.D.; Polley, M.Y.C.; Pitcher, B.N.; Cheson, B.D.; Kahl, B.S.; et al. Dose-Adjusted EPOCH-R Compared with R-CHOP as Frontline Therapy for Diffuse Large B-Cell Lymphoma: Clinical Outcomes of the Phase III Intergroup Trial Alliance/CALGB 50303. J. Clin. Oncol. 2019, 37, 1790–1799. [Google Scholar] [CrossRef]
- Sehn, L.H.; Martelli, M.; Trněný, M.; Liu, W.; Bolen, C.R.; Knapp, A.; Sahin, D.; Sellam, G.; Vitolo, U.; Sehn, L.H. A Randomized, Open-Label, Phase III Study of Obinutuzumab or Rituximab plus CHOP in Patients with Previously Untreated Diffuse Large B-Cell Lymphoma: Final Analysis of GOYA. J. Hematol. Oncol. 2020, 13, 71. [Google Scholar] [CrossRef]
- Jaeger, U.; Trneny, M.; Melzer, H.; Praxmarer, M.; Nawarawong, W.; Ben Yehuda, D.; Goldstein, D.; Mihaljevic, B.; Ilhan, O.; Ballova, V.; et al. Rituximab Maintenance for Patients with Aggressive B-Cell Lymphoma in First Remission: Results of the Randomized NHL13 Trial. Haematologica 2015, 100, 955–963. [Google Scholar] [CrossRef]
- Thieblemont, C.; Tilly, H.; Da Silva, M.G.; Casasnovas, R.O.; Fruchart, C.; Morschhauser, F.; Haioun, C.; Lazarovici, J.; Grosicka, A.; Perrot, A.; et al. Lenalidomide Maintenance Compared with Placebo in Responding Elderly Patients with Diffuse Large B-Cell Lymphoma Treated with First-Line Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone. J. Clin. Oncol. 2017, 35, 2473–2481. [Google Scholar] [CrossRef] [PubMed]
- Witzig, T.E.; Tobinai, K.; Rigacci, L.; Ikeda, T.; Vanazzi, A.; Hino, M.; Shi, Y.; Mayer, J.; Costa, L.J.; Silva, C.D.B.; et al. Adjuvant Everolimus in High-Risk Diffuse Large B-Cell Lymphoma: Final Results from the PILLAR-2 Randomized Phase III Trial. Ann. Oncol. 2018, 29, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Leonard, J.P.; Kolibaba, K.S.; Reeves, J.A.; Tulpule, A.; Flinn, I.W.; Kolevska, T.; Robles, R.; Flowers, C.R.; Collins, R.; DiBella, N.J.; et al. Randomized Phase II Study of R-CHOP with or without Bortezomib in Previously Untreated Patients with Non-Germinal Center B-Cell-like Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. 2017, 35, 3538–3546. [Google Scholar] [CrossRef] [PubMed]
- González-Barca, E.; Carrillo-Cruz, E.; Grande, C.; Martín, A.; Coronado, M.; Montes-Moreno, S.; Mercadal, S.; Roncero, J.M.; de Oteyza, J.P.; Nicolás, C.; et al. Phase 2 Randomized Trial Comparing Standard RCHOP Versus Brcap (Bortezomib, Rituximab, Cyclophosphamide, Adriamycin and Prednisone) as First Line Treatment in Young Patients with High-Risk Diffuse Large B-Cell Lymphoma (DLBCL). A Study from Spanish Group. Blood 2016, 128, 4201. [Google Scholar] [CrossRef]
- Younes, A.; Sehn, L.H.; Johnson, P.; Zinzani, P.L.; Hong, X.; Zhu, J.; Patti, C.; Belada, D.; Samoilova, O.; Suh, C.; et al. Randomized Phase III Trial of Ibrutinib and Rituximab plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone in Non–Germinal Center B-Cell Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. 2019, 37, 1285–1295. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.; Cummin, T.E.; Barrans, S.; Maishman, T.; Mamot, C.; Novak, U.; Caddy, J.; Stanton, L.; Kazmi-Stokes, S.; McMillan, A.; et al. Gene-Expression Profiling of Bortezomib Added to Standard Chemoimmunotherapy for Diffuse Large B-Cell Lymphoma (REMoDL-B): An Open-Label, Randomised, Phase 3 Trial. Lancet Oncol. 2019, 20, 649–662. [Google Scholar] [CrossRef] [PubMed]
- Nowakowski, G.S.; Hong, F.; Scott, D.W.; Macon, W.R.; King, R.L.; Habermann, T.M.; Wagner-Johnston, N.; Casulo, C.; Wade, J.L.; Nagargoje, G.G.; et al. Addition of Lenalidomide to R-CHOP Improves Outcomes in Newly Diagnosed Diffuse Large B-Cell Lymphoma in a Randomized Phase II US Intergroup Study ECOG-ACRIN E1412. J. Clin. Oncol. 2021, 39, 1329–1338. [Google Scholar] [CrossRef]
- Tilly, H.; Morschhauser, F.; Sehn, L.H.; Friedberg, J.W.; Trněný, M.; Sharman, J.P.; Herbaux, C.; Burke, J.M.; Matasar, M.; Rai, S.; et al. Polatuzumab Vedotin in Previously Untreated Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 386, 351–363. [Google Scholar] [CrossRef]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised Response Criteria for Malignant Lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef]
- Maurer, M.J.; Ghesquières, H.; Jais, J.P.; Witzig, T.E.; Haioun, C.; Thompson, C.A.; Delarue, R.; Micallef, I.N.; Peyrade, F.; Macon, W.R.; et al. Event-Free Survival at 24 Months Is a Robust End Point for Disease-Related Outcome in Diffuse Large B-Cell Lymphoma Treated with Immunochemotherapy. J. Clin. Oncol. 2014, 32, 1066–1073. [Google Scholar] [CrossRef]
- Crump, M.; Neelapu, S.S.; Farooq, U.; Van Den Neste, E.; Kuruvilla, J.; Westin, J.; Link, B.K.; Hay, A.; Cerhan, J.R.; Zhu, L.; et al. Outcomes in Refractory Diffuse Large B-Cell Lymphoma: Results from the International SCHOLAR-1 Study. Blood 2017, 130, 1800–1808. [Google Scholar] [CrossRef]
- Gisselbrecht, C.; Schmitz, N.; Mounier, N.; Gill, D.S.; Linch, D.C.; Trneny, M.; Bosly, A.; Milpied, N.J.; Radford, J.; Ketterer, N.; et al. Rituximab Maintenance Therapy after Autologous Stem-Cell Transplantation in Patients with Relapsed CD20+ Diffuse Large B-Cell Lymphoma: Final Analysis of the Collaborative Trial in Relapsed Aggressive Lymphoma. J. Clin. Oncol. 2012, 30, 4462–4469. [Google Scholar] [CrossRef] [PubMed]
- Köhler, G.; Milstein, C. Continuous Cultures of Fused Cells Secreting Antibody of Predefined Specificity. Nature 1975, 256, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Buss, N.A.P.S.; Henderson, S.J.; McFarlane, M.; Shenton, J.M.; De Haan, L. Monoclonal Antibody Therapeutics: History and Future. Curr. Opin. Pharmacol. 2012, 12, 615–622. [Google Scholar] [CrossRef] [PubMed]
- Goebeler, M.E.; Bargou, R.C. T Cell-Engaging Therapies—BiTEs and Beyond. Nat. Rev. Clin. Oncol. 2020, 17, 418–434. [Google Scholar] [CrossRef] [PubMed]
- Alsaab, H.O.; Sau, S.; Alzhrani, R.; Tatiparti, K.; Bhise, K.; Kashaw, S.K.; Iyer, A.K. PD-1 and PD-L1 Checkpoint Signaling Inhibition for Cancer Immunotherapy: Mechanism, Combinations, and Clinical Outcome. Front. Pharmacol. 2017, 8, 561. [Google Scholar] [CrossRef] [PubMed]
- Jurczak, W.; Zinzani, P.L.; Gaidano, G.; Goy, A.; Provencio, M.; Nagy, Z.; Robak, T.; Maddocks, K.; Buske, C.; Ambarkhane, S.; et al. Phase IIa Study of the CD19 Antibody MOR208 in Patients with Relapsed or Refractory B-Cell Non- Hodgkin’s Lymphoma. Ann. Oncol. 2018, 29, 1266–1272. [Google Scholar] [CrossRef]
- Salles, G.; Duell, J.; Barca, E.G.; Tournilhac, O.; Jurczak, W.; Liberati, A.M.; Nagy, Z.; Obr, A.; Gaidano, G.; André, M.; et al. Tafasitamab plus Lenalidomide in Relapsed or Refractory Diffuse Large B-Cell Lymphoma (L-MIND): A Multicentre, Prospective, Single-Arm, Phase 2 Study. Lancet. Oncol. 2020, 21, 978–988. [Google Scholar] [CrossRef]
- Woyach, J.A.; Awan, F.; Flinn, I.W.; Berdeja, J.G.; Wiley, E.; Mansoor, S.; Huang, Y.; Lozanski, G.; Foster, P.A.; Byrd, J.C. A Phase 1 Trial of the Fc-Engineered CD19 Antibody XmAb5574 (MOR00208) Demonstrates Safety and Preliminary Efficacy in Relapsed CLL. Blood 2014, 124, 3553–3560. [Google Scholar] [CrossRef]
- Gribben, J.G.; Fowler, N.; Morschhauser, F. Mechanisms of Action of Lenalidomide in B-Cell Non-Hodgkin Lymphoma. J. Clin. Oncol. 2015, 33, 2803–2811. [Google Scholar] [CrossRef]
- Sawalha, Y. Relapsed/Refractory Diffuse Large B-Cell Lymphoma: A Look at the Approved and Emerging Therapies. J. Pers. Med. 2021, 11, 1345. [Google Scholar] [CrossRef] [PubMed]
- Czuczman, M.S.; Trněný, M.; Davies, A.; Rule, S.; Linton, K.M.; Wagner-Johnston, N.; Gascoyne, R.D.; Slack, G.W.; Brousset, P.; Eberhard, D.A.; et al. A Phase 2/3 Multicenter, Randomized, Open-Label Study to Compare the Efficacy and Safety of Lenalidomide versus Investigator’s Choice in Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma. Clin. Cancer Res. 2017, 23, 4127–4137. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Fowler, N.; Wagner-Bartak, N.; Feng, L.; Romaguera, J.; Neelapu, S.S.; Hagemeister, F.; Fanale, M.; Oki, Y.; Pro, B.; et al. Oral Lenalidomide with Rituximab in Relapsed or Refractory Diffuse Large Cell, Follicular and Transformed Lymphoma: A Phase II Clinical Trial. Leukemia 2013, 27, 1902–1909. [Google Scholar] [CrossRef] [PubMed]
- Wiernik, P.H.; Lossos, I.S.; Tuscano, J.M.; Justice, G.; Vose, J.M.; Cole, C.E.; Lam, W.; McBride, K.; Wride, K.; Pietronigro, D.; et al. Lenalidomide Monotherapy in Relapsed or Refractory Aggressive Non-Hodgkin’s Lymphoma. J. Clin. Oncol. 2008, 26, 4952–4957. [Google Scholar] [CrossRef] [PubMed]
- Duell, J.; Maddocks, K.J.; González-Barca, E.; Jurczak, W.; Liberati, A.M.; de Vos, S.; Nagy, Z.; Obr, A.; Gaidano, G.; Abrisqueta, P.; et al. Long-Term Outcomes from the Phase II L-MIND Study of Tafasitamab (MOR208) plus Lenalidomide in Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma. Haematologica 2021, 106, 2417–2426. [Google Scholar] [CrossRef]
- Duell, J.; Jurczak, W.; Liberati, A.M.; Halka, J.; Carbó, E.P.; Costa, P.A.; Maddocks, K.J.; Dreyling, M.; Rosenwald, A.; Bakuli, A.; et al. L-Mind: A Safety and Efficacy Analysis of Tafasitamab in Patients with Relapsed/Refractory Diffuse Large B-Cell Lymphoma (R/R DLBCL) Receiving Treatment for at Least 2 Years. Blood 2022, 140, 6596–6598. [Google Scholar] [CrossRef]
- Larsen, T.S.; Manzke, O.; Leibovitz, D.; Arbushites, M. A Phase 3 Study of Tafasitamab Plus Lenalidomide in Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma (FirmMIND). Blood 2022, 140, 12077–12078. [Google Scholar] [CrossRef]
- Nowakowski, G.S.; Yoon, D.H.; Mondello, P.; Joffe, E.; Peters, A.; Fleury, I.; Greil, R.; Ku, M.; Marks, R.; Kim, K.; et al. RE-MIND2: Comparative Effectiveness of Tafasitamab plus Lenalidomide versus Polatuzumab Vedotin/Bendamustine/Rituximab (Pola-BR), CAR-T Therapies, and Lenalidomide/Rituximab (R2) Based on Real-World Data in Patients with Relapsed/Refractory Diffuse Large. Ann. Hematol. 2023, 102, 1773–1787. [Google Scholar] [CrossRef]
- Cordoba, R.; Prawitz, T.; Westley, T.; Sharma, A.; Ambarkhane, S.; Kapetanakis, V.; Sabatelli, L. Tafasitamab Plus Lenalidomide Versus 3 Rituximab-Based Treatments for Non-Transplant Eligible Relapsed/Refractory Diffuse Large B-Cell Lymphoma: A Matching-Adjusted Indirect Comparison. Adv. Ther. 2022, 39, 2668–2687. [Google Scholar] [CrossRef]
- Nowakowski, G.S.; Duell, J.; Kopeckova, K.; Trneny, M.; Pott, C.; Khouja, M.; Burke, J.M.; Waldron-Lynch, M.; Wagner, S.; Mukhopadhyay, A.; et al. First-Mind: Final Analysis from a Phase Ib, Open-Label, Randomized Study to Assess Safety of Tafasitamab or Tafasitamab + Lenalidomide in Addition to R-CHOP in Patients with Newly Diagnosed Diffuse Large B-Cell Lymphoma. Blood 2022, 140, 3731–3733. [Google Scholar] [CrossRef]
- Vitolo, U.; Nowakowski, G.S.; Burke, J.M.; Fox, C.P.; Trneny, M.; Chiappella, A.; Waldron-Lynch, M.; Wagner, S.; Pachori, A.; Lenz, G. Frontmind: A Phase III, Multicenter, Randomized, Double-Blind Study of Tafasitamab + Lenalidomide + R-CHOP Versus R-CHOP Alone for Newly Diagnosed High-Intermediate and High-Risk Diffuse Large B-Cell Lymphoma. Blood 2022, 140, 6618–6620. [Google Scholar] [CrossRef]
- Engelberts, P.J.; Hiemstra, I.H.; de Jong, B.; Schuurhuis, D.H.; Meesters, J.; Hernandez, I.B.; Oostindie, S.C.; Neijssen, J.; van den Brink, E.N.; Horbach, G.J.; et al. DuoBody-CD3xCD20 Induces Potent T-Cell-Mediated Killing of Malignant B Cells in Preclinical Models and Provides Opportunities for Subcutaneous Dosing. EBioMedicine 2020, 52, 102625. [Google Scholar] [CrossRef] [PubMed]
- van der Horst, H.J.; de Jonge, A.V.; Hiemstra, I.H.; Gelderloos, A.T.; Berry, D.R.A.I.; Hijmering, N.J.; van Essen, H.F.; de Jong, D.; Chamuleau, M.E.D.; Zweegman, S.; et al. Epcoritamab Induces Potent Anti-Tumor Activity against Malignant B-Cells from Patients with DLBCL, FL and MCL, Irrespective of Prior CD20 Monoclonal Antibody Treatment. Blood Cancer J. 2021, 11, 38. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, M.; Mous, R.; Clausen, M.R.; Johnson, P.; Linton, K.M.; Chamuleau, M.E.D.; Lewis, D.J.; Balari, A.S.; Cunningham, D.; Oliveri, R.S.; et al. Dose Escalation of Subcutaneous Epcoritamab in Patients with Relapsed or Refractory B-Cell Non-Hodgkin Lymphoma: An Open-Label, Phase 1/2 Study. Lancet 2021, 398, 1157–1169. [Google Scholar] [CrossRef] [PubMed]
- Thieblemont, C.; Phillips, T.; Ghesquieres, H.; Cheah, C.Y.; Clausen, M.R.; Cunningham, D.; Do, Y.R.; Feldman, T.; Gasiorowski, R.; Jurczak, W.; et al. Epcoritamab, a Novel, Subcutaneous CD3 × CD20 Bispecific T-Cell-Engaging Antibody, in Relapsed or Refractory Large B-Cell Lymphoma: Dose Expansion in a Phase I/II Trial. J. Clin. Oncol. 2023, 41, 2238–2247. [Google Scholar] [CrossRef] [PubMed]
- Abrisqueta, P.; Cordoba, R.; Falchi, L.; de Vos, S.; Nijland, M.; Offner, F.; Wu, J.; Bykhovski, I.; Wang, L.; Rana, A.; et al. Subcutaneous Epcoritamab + R-Dhax/C in Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma Eligible for Autologous Stem Cell Transplant: Updated Phase 1/2 Results. Blood 2022, 140, 1068–1069. [Google Scholar] [CrossRef]
- Budde, L.E.; Assouline, S.; Sehn, L.H.; Schuster, S.J.; Yoon, S.-S.; Yoon, D.H.; Matasar, M.J.; Bosch, F.; Kim, W.S.; Nastoupil, L.J.; et al. Single-Agent Mosunetuzumab Shows Durable Complete Responses in Patients with Relapsed or Refractory B-Cell Lymphomas: Phase I Dose-Escalation Study. J. Clin. Oncol. 2021, 40, 481–491. [Google Scholar] [CrossRef]
- Schuster, S.J.; Bartlett, N.L.; Assouline, S.; Yoon, S.-S.; Bosch, F.; Sehn, L.H.; Cheah, C.Y.; Shadman, M.; Gregory, G.P.; Ku, M.; et al. Mosunetuzumab Induces Complete Remissions in Poor Prognosis Non-Hodgkin Lymphoma Patients, Including Those Who Are Resistant to or Relapsing After Chimeric Antigen Receptor T-Cell (CAR-T) Therapies, and Is Active in Treatment through Multiple Lines. Blood 2019, 134, 6. [Google Scholar] [CrossRef]
- Bartlett, N.L.; Giri, P.; Budde, L.E.; Schuster, S.J.; Assouline, S.; Matasar, M.J.; Yoon, S.-S.; Canales, M.; Gutierrez, N.C.; Fay, K.; et al. Subcutaneous (SC) Administration of Mosunetuzumab with Cycle 1 Step-up Dosing Is Tolerable and Active in Patients with Relapsed/Refractory B-Cell Non-Hodgkin Lymphomas (R/R B-NHL): Initial Results from a Phase I/II Study. Blood 2021, 138, 3573. [Google Scholar] [CrossRef]
- Matasar, M.J.; Cheah, C.Y.; Yoon, D.H.; Assouline, S.E.; Bartlett, N.L.; Ku, M.; Giri, P.; Johnston, A.; Flinn, I.W.; Goy, A.H.; et al. Subcutaneous Mosunetuzumab in Relapsed or Refractory B-Cell Lymphoma: Promising Safety and Encouraging Efficacy in Dose Escalation Cohorts. Blood 2020, 136, 45–46. [Google Scholar] [CrossRef]
- Budde, E.L.; Bartlett, N.L.; Giri, P.; Schuster, S.J.; Assouline, S.; Yoon, S.-S.; Fay, K.; Matasar, M.J.; Gutierrez, N.C.; Marlton, P.; et al. Subcutaneous Mosunetuzumab Is Active with a Manageable Safety Profile in Patients (Pts) with Relapsed/Refractory (R/R) B-Cell Non-Hodgkin Lymphomas (B-NHLs): Updated Results from a Phase I/II Study. Blood 2022, 140, 3753–3755. [Google Scholar] [CrossRef]
- Olszewski, A.J.; Budde, L.E.; Chavez, J.; Ghosh, N.; Kamdar, M.; Lossos, I.S.; Diefenbach, C.; Sabry, W.; Dorritie, K.; Huw, L.-Y.; et al. Mosunetuzumab with Polatuzumab Vedotin Is Effective and Has a Manageable Safety Profile in Patients Aged <65 and ≥65 Years with Relapsed/Refractory Diffuse Large B-Cell Lymphoma (R/R DLBCL) and ≥1 Prior Therapy: Subgroup Analysis of a Phase Ib/II Study. Blood 2022, 140, 3757–3759. [Google Scholar] [CrossRef]
- Bacac, M.; Colombetti, S.; Herter, S.; Sam, J.; Perro, M.; Chen, S.; Bianchi, R.; Richard, M.; Schoenle, A.; Nicolini, V.; et al. CD20-TCB with Obinutuzumab Pretreatment as next-Generation Treatment of Hematologic Malignancies. Clin. Cancer Res. 2018, 24, 4785–4797. [Google Scholar] [CrossRef] [PubMed]
- Hutchings, M.; Morschhauser, F.; Iacoboni, G.; Carlo-Stella, C.; Offner, F.C.; Sureda, A.; Salles, G.; Martínez-Lopez, J.; Crump, M.; Thomas, D.N.; et al. Glofitamab, a Novel, Bivalent CD20-Targeting T-Cell-Engaging Bispecific Antibody, Induces Durable Complete Remissions in Relapsed or Refractory B-Cell Lymphoma: A Phase I Trial. J. Clin. Oncol. 2021, 39, 1959–1970. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, M.J.; Carlo-Stella, C.; Morschhauser, F.; Bachy, E.; Corradini, P.; Iacoboni, G.; Khan, C.; Wróbel, T.; Offner, F.; Trněný, M.; et al. Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Engl. J. Med. 2022, 387, 2220–2231. [Google Scholar] [CrossRef] [PubMed]
- Ferhanoglu, B.; Gulbas, Z.; Uzay, A.; Özcan, M.; Ozkalemkas, F.; Dal, M.S.; Kalyon, H.; Akay, O.M.; Deveci, B.; Bekoz, H.; et al. Glofitamab in Relapsed/Refractory Diffuse Large B Cell Lymphoma: Real World Data. Blood 2022, 140, 6704–6705. [Google Scholar] [CrossRef]
- Hutchings, M.; Carlo-Stella, C.; Morschhauser, F.; Bachy, E.; Corradini, P.; Iacoboni, G.; Khan, C.; Patel, K.; Hertzberg, M.; Falchi, L.; et al. Relapse Is Uncommon in Patients with Large B-Cell Lymphoma Who Are in Complete Remission at the End of Fixed-Course Glofitamab Treatment. Blood 2022, 140, 1062–1064. [Google Scholar] [CrossRef]
- Hutchings, M.; Carlo-Stella, C.; Gritti, G.; Bosch, F.; Morschhauser, F.; Townsend, W.; Offner, F.; Walter, H.S.; Ghesquieres, H.; Houot, R.; et al. CD19 4-1BBL (RO7227166) a Novel Costimulatory Bispecific Antibody Can Be Safely Combined with the T-Cell-Engaging Bispecific Antibody Glofitamab in Relapsed or Refractory B-Cell Non-Hodgkin Lymphoma. Blood 2022, 140, 9461–9463. [Google Scholar] [CrossRef]
- Topp, M.S.; Tani, M.; Dickinson, M.; Ghosh, N.; Santoro, A.; Pinto, A.; Bosch, F.; Fox, C.P.; López-Guillermo, A.; Carlucci, C.; et al. Glofitamab Plus R-CHOP Induces High Response Rates and a Favorable Safety Profile in Patients with Previously Untreated Diffuse Large B-Cell Lymphoma (DLBCL): Results from a Phase Ib Study. Blood 2022, 140, 1775–1777. [Google Scholar] [CrossRef]
- Smith, E.J.; Olson, K.; Haber, L.J.; Varghese, B.; Duramad, P.; Tustian, A.D.; Oyejide, A.; Kirshner, J.R.; Canova, L.; Menon, J.; et al. A Novel, Native-Format Bispecific Antibody Triggering T-Cell Killing of B-Cells Is Robustly Active in Mouse Tumor Models and Cynomolgus Monkeys. Sci. Rep. 2015, 5, 17943. [Google Scholar] [CrossRef]
- Bannerji, R.; Arnason, J.E.; Advani, R.H.; Brown, J.R.; Allan, J.N.; Ansell, S.M.; Barnes, J.A.; O’Brien, S.M.; Chávez, J.C.; Duell, J.; et al. Odronextamab, a Human CD20 × CD3 Bispecific Antibody in Patients with CD20-Positive B-Cell Malignancies (ELM-1): Results from the Relapsed or Refractory Non-Hodgkin Lymphoma Cohort in a Single-Arm, Multicentre, Phase 1 Trial. Lancet Haematol. 2022, 9, e327–e339. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.-S.; Kim, T.M.; Cho, S.-G.; Jarque, I.; Iskierka-Jażdżewska, E.; Poon, M.L.; Prince, H.M.; Oh, S.Y.; Lim, F.; Carpio, C.; et al. Odronextamab in Patients with Relapsed/Refractory (R/R) Diffuse Large B-Cell Lymphoma (DLBCL): Results from a Prespecified Analysis of the Pivotal Phase II Study ELM-2. Blood 2022, 140, 1070–1071. [Google Scholar] [CrossRef]
- Wei, J.; Montalvo-Ortiz, W.; Yu, L.; Krasco, A.; Olson, K.; Rizvi, S.; Fiaschi, N.; Coetzee, S.; Wang, F.; Ullman, E.; et al. CD22-Targeted CD28 Bispecific Antibody Enhances Antitumor Efficacy of Odronextamab in Refractory Diffuse Large B Cell Lymphoma Models. Sci. Transl. Med. 2022, 14, eabn1082. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Michot, J.-M.; Chanan-Khan, A.A.; Salles, G.A.; Cartron, G.; Peyrade, F.; Bouabdallah, R.; Reid, E.G.; Thomas, S.K.; Wierda, W.G.; et al. Preliminary Safety and Anti-Tumor Activity of XmAb13676, an Anti-CD20 × Anti-CD3 Bispecific Antibody, in Patients with Relapsed/Refractory Non-Hodgkin’s Lymphoma and Chronic Lymphocytic Leukemia. Blood 2019, 134, 4079. [Google Scholar] [CrossRef]
- Patel, K.; Riedell, P.A.; Tilly, H.; Ahmed, S.; Michot, J.-M.; Ghesquieres, H.; de Collela, J.M.S.; Chanan-Khan, A.; Bouabdallah, K.; Tessoulin, B.; et al. A Phase 1 Study of Plamotamab, an Anti-CD20 × Anti-CD3 Bispecific Antibody, in Patients with Relapsed/Refractory Non-Hodgkin’s Lymphoma: Recommended Dose Safety/Efficacy Update and Escalation Exposure-Response Analysis. Blood 2022, 140, 9470–9472. [Google Scholar] [CrossRef]
- Thomas, A.; Teicher, B.A.; Hassan, R. Antibody–Drug Conjugates for Cancer Therapy. Lancet. Oncol. 2016, 17, e254. [Google Scholar] [CrossRef] [PubMed]
- Staudacher, A.H.; Brown, M.P. Antibody Drug Conjugates and Bystander Killing: Is Antigen-Dependent Internalisation Required? Br. J. Cancer 2017, 117, 1736–1742. [Google Scholar] [CrossRef]
- Chu, Y.; Zhou, X.; Wang, X. Antibody-Drug Conjugates for the Treatment of Lymphoma: Clinical Advances and Latest Progress. J. Hematol. Oncol. 2021, 14, 88. [Google Scholar] [CrossRef]
- Dornan, D.; Bennett, F.; Chen, Y.; Dennis, M.; Eaton, D.; Elkins, K.; French, D.; Go, M.A.T.; Jack, A.; Junutula, J.R.; et al. Therapeutic Potential of an Anti-CD79b Antibody–Drug Conjugate, Anti–CD79b-vc-MMAE, for the Treatment of Non-Hodgkin Lymphoma. Blood 2009, 114, 2721–2729. [Google Scholar] [CrossRef]
- Palanca-Wessels, M.C.A.; Czuczman, M.; Salles, G.; Assouline, S.; Sehn, L.H.; Flinn, I.; Patel, M.R.; Sangha, R.; Hagenbeek, A.; Advani, R.; et al. Safety and Activity of the Anti-CD79B Antibody–Drug Conjugate Polatuzumab Vedotin in Relapsed or Refractory B-Cell Non-Hodgkin Lymphoma and Chronic Lymphocytic Leukaemia: A Phase 1 Study. Lancet Oncol. 2015, 16, 704–715. [Google Scholar] [CrossRef]
- Morschhauser, F.; Flinn, I.W.; Advani, R.; Sehn, L.H.; Diefenbach, C.; Kolibaba, K.; Press, O.W.; Salles, G.; Tilly, H.; Chen, A.I.; et al. Polatuzumab Vedotin or Pinatuzumab Vedotin plus Rituximab in Patients with Relapsed or Refractory Non-Hodgkin Lymphoma: Final Results from a Phase 2 Randomised Study (ROMULUS). Lancet Haematol. 2019, 5, e254–e265. [Google Scholar] [CrossRef] [PubMed]
- Sehn, L.H.; Herrera, A.F.; Flowers, C.R.; Kamdar, M.K.; McMillan, A.; Hertzberg, M.; Assouline, S.; Kim, T.M.; Kim, W.S.; Ozcan, M.; et al. Polatuzumab Vedotin in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. J. Clin. Oncol. 2020, 38, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Sehn, L.H.; Hertzberg, M.; Opat, S.; Herrera, A.F.; Assouline, S.; Flowers, C.R.; Kim, T.M.; McMillan, A.; Ozcan, M.; Safar, V.; et al. Polatuzumab Vedotin plus Bendamustine and Rituximab in Relapsed/Refractory DLBCL: Survival Update and New Extension Cohort Data. Blood Adv. 2022, 6, 533–543. [Google Scholar] [CrossRef] [PubMed]
- Zammarchi, F.; Corbett, S.; Adams, L.; Tyrer, P.C.; Kiakos, K.; Janghra, N.; Marafioti, T.; Britten, C.E.; Havenith, C.E.G.; Chivers, S.; et al. ADCT-402, a PBD Dimer–Containing Antibody Drug Conjugate Targeting CD19-Expressing Malignancies. Blood 2018, 131, 1094–1105. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wei, G.; Liu, D. CD19: A Biomarker for B Cell Development, Lymphoma Diagnosis and Therapy. Exp. Hematol. Oncol. 2012 11 2012, 1, 36. [Google Scholar] [CrossRef] [PubMed]
- Caimi, P.F.; Ai, W.; Alderuccio, J.P.; Ardeshna, K.M.; Hamadani, M.; Hess, B.; Kahl, B.S.; Radford, J.; Solh, M.; Stathis, A.; et al. Loncastuximab Tesirine in Relapsed or Refractory Diffuse Large B-Cell Lymphoma (LOTIS-2): A Multicentre, Open-Label, Single-Arm, Phase 2 Trial. Lancet Oncol. 2021, 22, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Hamadani, M.; Radford, J.; Carlo-Stella, C.; Caimi, P.F.; Reid, E.; O’Connor, O.A.; Feingold, J.M.; Ardeshna, K.M.; Townsend, W.; Solh, M.; et al. Final Results of a Phase 1 Study of Loncastuximab Tesirine in Relapsed/Refractory B-Cell Non-Hodgkin Lymphoma. Blood 2021, 137, 2634–2645. [Google Scholar] [CrossRef]
- Connors, J.M.; Jurczak, W.; Straus, D.J.; Ansell, S.M.; Kim, W.S.; Gallamini, A.; Younes, A.; Alekseev, S.; Illés, Á.; Picardi, M.; et al. Brentuximab Vedotin with Chemotherapy for Stage III or IV Hodgkin’s Lymphoma. N. Engl. J. Med. 2018, 378, 331–344. [Google Scholar] [CrossRef]
- Jacobsen, E.D.; Sharman, J.P.; Oki, Y.; Advani, R.H.; Winter, J.N.; Bello, C.M.; Spitzer, G.; Palanca-Wessels, M.C.; Kennedy, D.A.; Levine, P.; et al. Brentuximab Vedotin Demonstrates Objective Responses in a Phase 2 Study of Relapsed/Refractory DLBCL with Variable CD30 Expression. Blood 2015, 125, 1394–1402. [Google Scholar] [CrossRef]
- Ward, J.P.; Berrien-Elliott, M.M.; Gomez, F.; Luo, J.; Becker-Hapak, M.; Cashen, A.F.; Wagner-Johnston, N.D.; Maddocks, K.; Mosior, M.; Foster, M.; et al. Phase 1/Dose Expansion Trial of Brentuximab Vedotin and Lenalidomide in Relapsed or Refractory Diffuse Large B-Cell Lymphoma. Blood 2022, 139, 1999–2010. [Google Scholar] [CrossRef]
- Advani, R.H.; Lebovic, D.; Chen, A.; Brunvand, M.; Goy, A.; Chang, J.E.; Hochberg, E.; Yalamanchili, S.; Kahn, R.; Lu, D.; et al. Phase i Study of the Anti-CD22 Antibody-Drug Conjugate Pinatuzumab Vedotin with/without Rituximab in Patients with Relapsed/Refractory B-Cell Non-Hodgkin Lymphoma. Clin. Cancer Res. 2017, 23, 1167–1176. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.A.; Smith, K.G.C. CD22: An Inhibitory Enigma. Immunology 2008, 123, 314–325. [Google Scholar] [CrossRef] [PubMed]
- Fayad, L.; Offner, F.; Smith, M.R.; Verhoef, G.; Johnson, P.; Kaufman, J.L.; Rohatiner, A.; Advani, A.; Foran, J.; Hess, G.; et al. Safety and Clinical Activity of a Combination Therapy Comprising Two Antibody-Based Targeting Agents for the Treatment of Non-Hodgkin Lymphoma: Results of a Phase I/II Study Evaluating the Immunoconjugate Inotuzumab Ozogamicin with Rituximab. J. Clin. Oncol. 2013, 31, 573–583. [Google Scholar] [CrossRef] [PubMed]
- Wagner-Johnston, N.D.; Goy, A.; Rodriguez, M.A.; Ehmann, W.C.; Hamlin, P.A.; Radford, J.; Thieblemont, C.; Suh, C.; Sweetenham, J.; Huang, Y.; et al. A Phase 2 Study of Inotuzumab Ozogamicin and Rituximab, Followed by Autologous Stem Cell Transplant in Patients with Relapsed/Refractory Diffuse Large B-Cell Lymphoma. Leuk. Lymphoma 2015, 56, 2863–2869. [Google Scholar] [CrossRef] [PubMed]
- Sangha, R.; Davies, A.; Dang, N.H.; Ogura, M.; MacDonald, D.A.; Ananthakrishnan, R.; Paccagnella, M.L.; Vandendries, E.; Boni, J.; Goh, Y.T. Phase 1 Study of Inotuzumab Ozogamicin Combined with R-GDP for the Treatment of Patients with Relapsed/Refractory CD22+ B-Cell Non-Hodgkin Lymphoma. J. Drug Assess. 2017, 6, 10. [Google Scholar] [CrossRef] [PubMed]
- Rizzieri, D. Zevalin® (Ibritumomab Tiuxetan): After More than a Decade of Treatment Experience, What Have We Learned? Crit. Rev. Oncol. Hematol. 2016, 105, 5–17. [Google Scholar] [CrossRef] [PubMed]
- Morschhauser, F.; Illidge, T.; Huglo, D.; Martinelli, G.; Paganelli, G.; Zinzani, P.L.; Rule, S.; Liberati, A.M.; Milpied, N.; Hess, G.; et al. Efficacy and Safety of Yttrium-90 Ibritumomab Tiuxetan in Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma Not Appropriate for Autologous Stem-Cell Transplantation. Blood 2007, 110, 54–58. [Google Scholar] [CrossRef]
- Shimoni, A.; Avivi, I.; Rowe, J.M.; Yeshurun, M.; Levi, I.; Or, R.; Patachenko, P.; Avigdor, A.; Zwas, T.; Nagler, A. A Randomized Study Comparing Yttrium-90 Ibritumomab Tiuxetan (Zevalin) and High-Dose BEAM Chemotherapy versus BEAM Alone as the Conditioning Regimen before Autologous Stem Cell Transplantation in Patients with Aggressive Lymphoma. Cancer 2012, 118, 4706–4714. [Google Scholar] [CrossRef]
- Kline, J.; Godfrey, J.; Ansell, S.M. The Immune Landscape and Response to Immune Checkpoint Blockade Therapy in Lymphoma. Blood 2020, 135, 523–533. [Google Scholar] [CrossRef]
- Pasqualucci, L.; Dalla-Favera, R. Genetics of Diffuse Large B-Cell Lymphoma. Blood 2018, 131, 2307–2319. [Google Scholar] [CrossRef]
- Georgiou, K.; Chen, L.; Berglund, M.; Ren, W.; De Miranda, N.F.C.C.; Lisboa, S.; Fangazio, M.; Zhu, S.; Hou, Y.; Wu, K.; et al. Genetic Basis of PD-L1 Overexpression in Diffuse Large B-Cell Lymphomas. Blood 2016, 127, 3026–3034. [Google Scholar] [CrossRef] [PubMed]
- Chao, M.P.; Alizadeh, A.A.; Tang, C.; Myklebust, J.H.; Varghese, B.; Gill, S.; Jan, M.; Cha, A.C.; Chan, C.K.; Tan, B.T.; et al. Anti-CD47 Antibody Synergizes with Rituximab to Promote Phagocytosis and Eradicate Non-Hodgkin Lymphoma. Cell 2010, 142, 699–713. [Google Scholar] [CrossRef] [PubMed]
- Freeman, G.J.; Long, A.J.; Iwai, Y.; Bourque, K.; Chernova, T.; Nishimura, H.; Fitz, L.J.; Malenkovich, N.; Okazaki, T.; Byrne, M.C.; et al. Engagement of the PD-1 Immunoinhibitory Receptor by a Novel B7 Family Member Leads to Negative Regulation of Lymphocyte Activation. J. Exp. Med. 2000, 192, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Twa, D.D.W.; Chan, F.C.; Ben-Neriah, S.; Woolcock, B.W.; Mottok, A.; Tan, K.L.; Slack, G.W.; Gunawardana, J.; Lim, R.S.; McPherson, A.W.; et al. Genomic Rearrangements Involving Programmed Death Ligands Are Recurrent in Primary Mediastinal Large B-Cell Lymphoma. Blood 2014, 123, 2062–2065. [Google Scholar] [CrossRef] [PubMed]
- Ansell, S.M.; Minnema, M.C.; Johnson, P.; Timmerman, J.M.; Armand, P.; Shipp, M.A.; Rodig, S.J.; Ligon, A.H.; Roemer, M.G.M.; Reddy, N.; et al. Nivolumab for Relapsed/Refractory Diffuse Large B-Cell Lymphoma in Patients Ineligible for or Having Failed Autologous Transplantation: A Single-Arm, Phase II Study. J. Clin. Oncol. 2019, 37, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Qian, B.Z.; Pollard, J.W. Macrophage Diversity Enhances Tumor Progression and Metastasis. Cell 2010, 141, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Tsai, R.K.; Discher, D.E. Inhibition of “Self” Engulfment through Deactivation of Myosin-II at the Phagocytic Synapse between Human Cells. J. Cell Biol. 2008, 180, 989–1003. [Google Scholar] [CrossRef]
- Liu, J.; Wang, L.; Zhao, F.; Tseng, S.; Narayanan, C.; Shura, L.; Willingham, S.; Howard, M.; Prohaska, S.; Volkmer, J.; et al. Pre-Clinical Development of a Humanized Anti-CD47 Antibody with Anti-Cancer Therapeutic Potential. PLoS ONE 2015, 10, e0137345. [Google Scholar] [CrossRef]
- Tseng, D.; Volkmer, J.P.; Willingham, S.B.; Contreras-Trujillo, H.; Fathman, J.W.; Fernhoff, N.B.; Seita, J.; Inlay, M.A.; Weiskopf, K.; Miyanishi, M.; et al. Anti-CD47 Antibody-Mediated Phagocytosis of Cancer by Macrophages Primes an Effective Antitumor T-Cell Response. Proc. Natl. Acad. Sci. USA 2013, 110, 11103–11108. [Google Scholar] [CrossRef]
- Advani, R.; Flinn, I.; Popplewell, L.; Forero, A.; Bartlett, N.L.; Ghosh, N.; Kline, J.; Roschewski, M.; LaCasce, A.; Collins, G.P.; et al. CD47 Blockade by Hu5F9-G4 and Rituximab in Non-Hodgkin’s Lymphoma. N. Engl. J. Med. 2018, 379, 1711–1721. [Google Scholar] [CrossRef]
- de Vos, S.; Reagan, P.M.; Patel, M.R.; Saba, N.S.; Mortlock, A.; Cerec, V.; Munugalavadla, V.; Acar, M.; Nuttall, B.; Jenkins, D.; et al. Magrolimab, Rituximab and Acalabrutinib for Relapsed/Refractory (R/R) Diffuse Large B-Cell Lymphoma (DLBCL): Results from the Phase 1 PRISM Trial. Blood 2022, 140, 6635–6637. [Google Scholar] [CrossRef]
- Maakaron, J.; Asch, A.S.; Popplewell, L.L.; Collins, G.P.; Flinn, I.W.; Ghosh, N.; Keane, C.; Ku, M.; Mehta, A.; Roschewski, M.; et al. Magrolimab in Combination with Rituximab + Chemotherapy in Patients with Relapsed or Refractory (R/R) Diffuse Large B-Cell Lymphoma (DLBCL). Blood 2022, 140, 3728–3730. [Google Scholar] [CrossRef]


{kind=link}
| NCT | Phase | Targets | Drugs | Results |
|---|---|---|---|---|
| NCT05626322 | phase II | CD47, CD19 | maplirpacept-tafasitamab-lenalidomide | NA |
| NCT01685008 | phase IIa | CD19 | tafasitamab | ORR 26%, CR 6%; mPFS 2.7 months, mDOR 20.1 months |
| NCT02399085 | phase II | CD19 | tafasitamab-lenalidomide | ORR 60%, CR 40%; mPFS 18 months in 46%, mDOR 21.7 months |
| NCT05429268 | phase III | CD19 | tafasitamab-lenalidomide | NA |
| NCT04697160 | real world | CD19 | tafasitamab-lenalidomide vs. other therapies (R2, pola-BR, CAR-T) | ORR 62.5% vs. 58.3% (pola-BR); 63.6% vs. 30.3% (R2); 59.5% vs. 75.7% (CAR-T) |
| NCT02763319 | phase II/III | CD19 | tafasitamab-bendamustine vs. rituximab-bendamustine | NA |
| NCT05328102 | phase II | CD19, CD20/CD3 | tafasitamab-lenalidomide-plamotamab vs. tafasitamab-lenalidomide | NA |
| NCT04607772 | phase I/II | CD19, XPO1 | selinexor-tafasitamab-lenalidomide vs. selinexor-other therapies | NA |
| NCT | Phase | Target | Drug | Results |
|---|---|---|---|---|
| NCT03625037 | phase I/II | CD20/CD3 | epcoritamab | ORR 88%, CR 38% Expansion cohort: ORR 63.1%, CR 38.9% |
| NCT04663347 | phase Ib/2 | CD20/CD3 | epcoritamab + other therapies | NA |
| NCT05852717 | phase II | CD20/CD3 | epcoritamab + GDP | NA |
| NCT04628494 | phase III | CD20/CD3 | epcoritamab vs. investigator choice therapy | NA |
| NCT02500407 | phase I/Ib | CD20/CD3 | mosunetuzumab | ORR 34.9%, CR 19.4% |
| phase I/II | CD20/CD3 | mosunetuzumab | ORR 42%, CR 23.9%; mPFS 3.2 months | |
| phase I/II | CD20/CD3 | subcutaneous mosunetuzumab | ORR 36%, CR 20% | |
| NCT03671018 | phase Ib | CD20/CD3, CD79b | mosunetuzumab-polatuzumab | ORR: ≥65 years 72% vs. <65 years 54%; CR: ≥65 years 56% vs. <65 years 38% |
| NCT04889716 | phase II | CD20/CD3, CD19 | CAR-T followed by mosunetuzumab or glofitamab | NA |
| NCT05672251 | phase II | CD20/CD3, CD19 | mosunetuzumab-loncastuximab | NA |
| NCT05464329 | phase Ib | CD20/CD3 | DHAP or ICE + mosunetuzumab and ASCT | NA |
| NCT03075696 | phase I | CD20/CD3, CD20 | glofitamab-obinutuzumab | ORR 71.4%, CR 64.3% |
| phase II | CD20/CD3, CD20 | glofitamab-obinutuzumab fixed duration | ORR 95%, CR 39%; estimated 12 months OS 50% | |
| NCT04408638 | phase III | CD20/CD3, CD20 | glofitamab-GemOx vs. rituximab-GemOx | NA |
| NCT05364424 | phase Ib | CD20/CD3, CD20 | glofitamab -R-ICE | NA |
| NCT05335018 | phase II | CD20/CD3, BTK | glofitamab-poseltinib-lenalidomide | ORR 100%, CR 50%, PR 50%; mDOR 4 months |
| NCT02290951 | phase I | CD20/CD3 | odronextamab | not CAR-T exposed: ORR and CR 53%; CAR-T exposed: ORR 33%, CR 27%; mDOR NR |
| NCT03888105 | phase II | CD20/CD3 | odronextamab | ORR 53%, CR 37%; mDOR NR |
| NCT02924402 | phase I | CD20/CD3 | plamotamab | ORR 47.4%, CR 26.3% |
| NCT05328102 | phase II | CD20/CD3, CD19 | plamotamab-tafasitamab-lenalidomide | NA |
| NCT | Phase | Targets | Drugs | Results |
|---|---|---|---|---|
| NCT01290549 | phase I | CD79b | polatuzumab vedotin | ORR 56%, CR 16%; mPFS 5.0 months, mDOR 5.2 months |
| NCT01209130 | phase I | CD79b | pinatuzumab vedotin | ORR 36%, CR 16%; mPFS 4.0 months, mDOR 3.0 months |
| NCT01691898 | phase II | CD79b, CD20 | rituximab-polatuzumab | ORR 54%, CR 21%; mPFS 5.6 months, mDOR 13.4 months |
| rituximab-pinatuzumab | ORR 60%, CR 26%; mPFS 5.4 months, mDOR 6.2 months | |||
| NCT02257567 | phase Ib/II | CD79b, CD20 | polatuzumab-BR | ORR 45%, CR 40%; mPFS 9.5 months, mDOR 12.6 months |
| NCT04665765 | phase II | CD79b, CD20 | polatuzumab-R-ICE | NA |
| NCT02611323 | phase Ib/II | CD79b, CD20 | polatuzumab-obinutuzumab-venetoclax | NA |
| polatuzumab-rituximab-venetoclax | NA | |||
| NCT02729896 | phase Ib | CD79b, CD20, PD-L1 | rituximab-atezolizumab-polatuzumab | ORR 25%, CR 13% |
| NCT03589469 | phase II | CD19 | loncastuximab tesirine | ORR 48.3%, CR 24.1%; mPFS 4.9 months, mDOR 10.3 months |
| NCT04384484 | phase III | CD19, CD20 | loncastuximab-rituximab | ORR 75%, CR 40%, PR 35% |
| NCT03685344 | phase I | CD19, PD-L1 | loncastuximab-durvalumab | NA |
| NCT01421667 | phase II | CD30 | brentuximab vedotin | ORR 44%, CR 17%; mPFS 4.0 months, mDOR 5.6 months |
| NCT02086604 | phase I | CD30 | BV-lenalidomide | ORR 57%, CR 35%; mPFS 10.2 months, mDOR 13.1 months |
| NCT04404283 | phase III | CD30, CD20 | rituximab-BV-lenalidomide | ORR 70%, CR 4 patients, PR 2 patients |
| NCT00299494 | phase I/II | CD22, CD20 | rituximab-inotuzumab | ORR 74%, CR 50%; mPFS 17.1 months, mDOR 17.7 months |
| NCT | Phase | Targets | Drugs | Results |
|---|---|---|---|---|
| NCT02038933 | phase II | PD-1 | nivolumab | ORR 3–10%, CR 0–3%; mDOR 8–11.4 months |
| NCT02953509 | phase Ib | CD47, CD20 | magrolimab-rituximab | ORR 40%, CR 33% |
| NCT03527147 | phase I | CD47, CD20, BTK | magrolimab-rituximab-acalabrutinib | ORR 28.6%, CR 28.6% |
| NCT02953509 | phase Ib | CD47, CD20 | magrolimab-rituximab-GemOx | ORR 51.5%, CR 39.4%; mPFS 3.9 months, mDOR 18.0 months |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schipani, M.; Rivolta, G.M.; Margiotta-Casaluci, G.; Mahmoud, A.M.; Al Essa, W.; Gaidano, G.; Bruna, R. New Frontiers in Monoclonal Antibodies for Relapsed/Refractory Diffuse Large B-Cell Lymphoma. Cancers 2024, 16, 187. https://doi.org/10.3390/cancers16010187
Schipani M, Rivolta GM, Margiotta-Casaluci G, Mahmoud AM, Al Essa W, Gaidano G, Bruna R. New Frontiers in Monoclonal Antibodies for Relapsed/Refractory Diffuse Large B-Cell Lymphoma. Cancers. 2024; 16(1):187. https://doi.org/10.3390/cancers16010187
Chicago/Turabian StyleSchipani, Mattia, Giulia Maria Rivolta, Gloria Margiotta-Casaluci, Abdurraouf Mokhtar Mahmoud, Wael Al Essa, Gianluca Gaidano, and Riccardo Bruna. 2024. "New Frontiers in Monoclonal Antibodies for Relapsed/Refractory Diffuse Large B-Cell Lymphoma" Cancers 16, no. 1: 187. https://doi.org/10.3390/cancers16010187