
Utilising Pancreatic Exocrine Insufficiency in the Detection of Resectable Pancreatic Ductal Adenocarcinoma
 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Interventions
2.4. Sample Size Considerations
2.5. Statistical Methods
3. Results
3.1. Participant Demographics
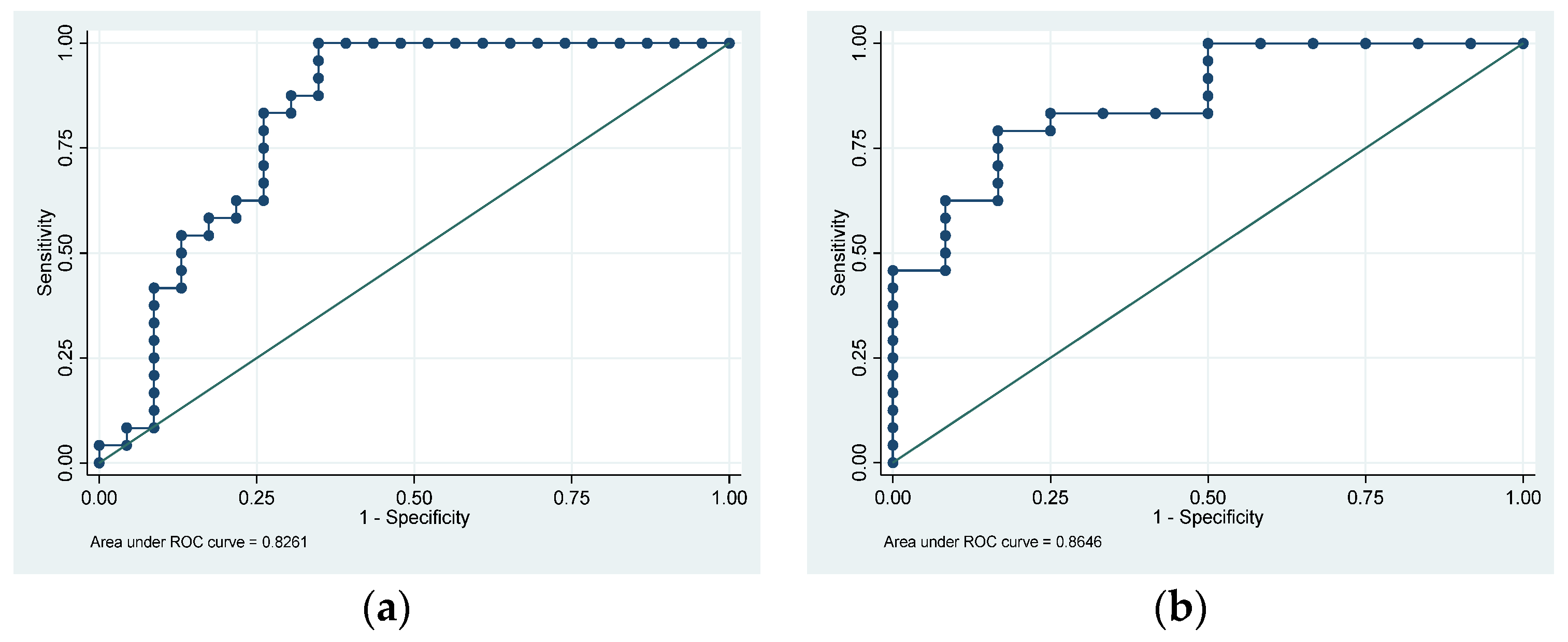
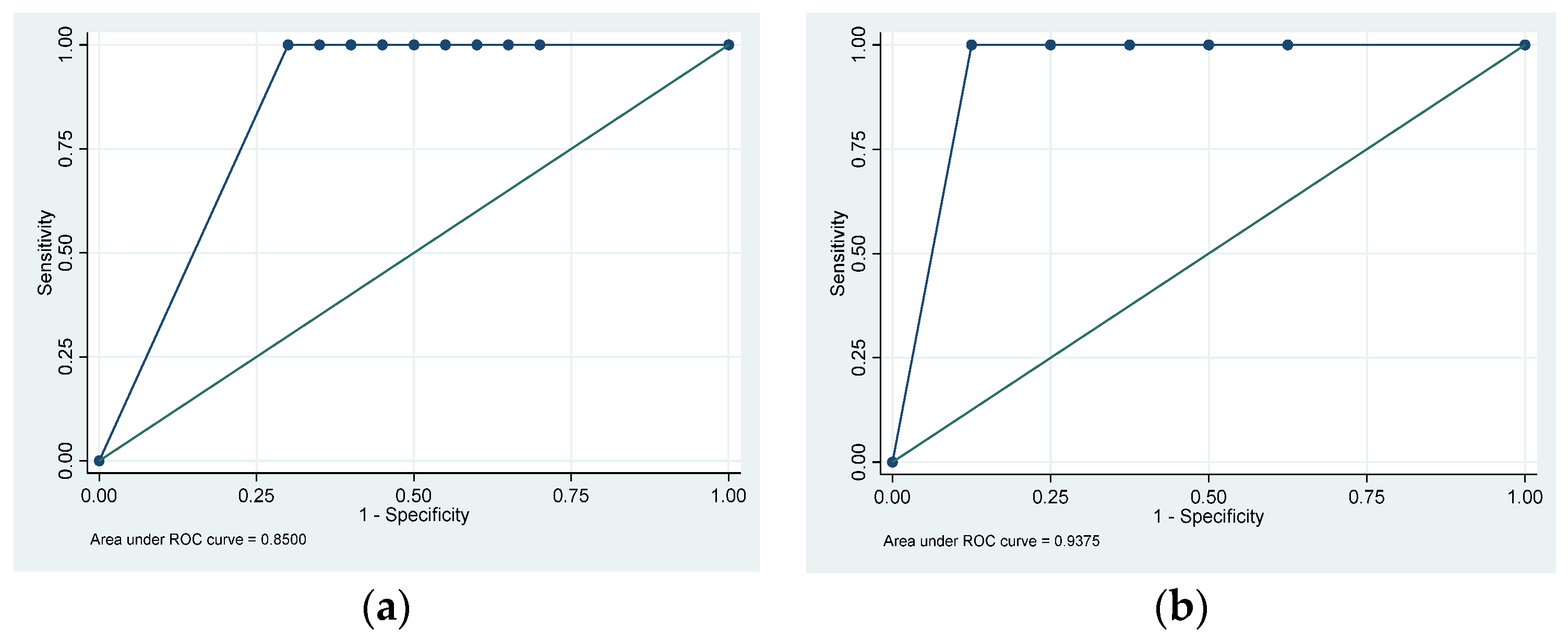
3.2. Pancreatic Exocrine Insufficiency Results
3.3. The Impact of New-Onset Diabetes Mellitus
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xiao, A.Y.; Tan, M.L.; Wu, L.M.; Asrani, V.M.; Windsor, J.A.; Yadav, D.; Petrov, M.S. Global incidence and mortality of pancreatic diseases: A systematic review, meta-analysis, and meta-regression of population-based cohort studies. Lancet Gastroenterol. Hepatol. 2016, 1, 45–55. [Google Scholar] [CrossRef]
- Park, W.; Chawla, A.; O’Reilly, E.M. Pancreatic Cancer: A Review. JAMA 2021, 326, 851–862. [Google Scholar] [CrossRef] [PubMed]
- Cabasag, C.J.; Arnold, M.; Rutherford, M.; Bardot, A.; Ferlay, J.; Morgan, E.; Little, A.; De, P.; Dixon, E.; Woods, R.R.; et al. Pancreatic cancer survival by stage and age in seven high-income countries (ICBP SURVMARK-2): A population-based study. Br. J. Cancer 2022, 126, 1774–1782. [Google Scholar] [CrossRef]
- Lohr, J.M.; Oliver, M.R.; Frulloni, L. Synopsis of recent guidelines on pancreatic exocrine insufficiency. United Eur. Gastroenterol. J. 2013, 1, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Vujasinovic, M.; Valente, R.; Del Chiaro, M.; Permert, J.; Lohr, J.M. Pancreatic Exocrine Insufficiency in Pancreatic Cancer. Nutrients 2017, 9, 183. [Google Scholar] [CrossRef]
- Sikkens, E.C.; Cahen, D.L.; de Wit, J.; Looman, C.W.; van Eijck, C.; Bruno, M.J. A prospective assessment of the natural course of the exocrine pancreatic function in patients with a pancreatic head tumor. J. Clin. Gastroenterol. 2014, 48, e43–e46. [Google Scholar] [CrossRef] [PubMed]
- Roeyen, G.; Berrevoet, F.; Borbath, I.; Geboes, K.; Peeters, M.; Topal, B.; Van Cutsem, E.; Van Laethem, J.L. Expert opinion on management of pancreatic exocrine insufficiency in pancreatic cancer. ESMO Open 2022, 7, 100386. [Google Scholar] [CrossRef]
- Lohr, J.M.; Dominguez-Munoz, E.; Rosendahl, J.; Besselink, M.; Mayerle, J.; Lerch, M.M.; Haas, S.; Akisik, F.; Kartalis, N.; Iglesias-Garcia, J.; et al. United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU). United Eur. Gastroenterol. J. 2017, 5, 153–199. [Google Scholar] [CrossRef]
- Gonzalez-Sanchez, V.; Amrani, R.; Gonzalez, V.; Trigo, C.; Pico, A.; de-Madaria, E. Diagnosis of exocrine pancreatic insufficiency in chronic pancreatitis: (13)C-Mixed Triglyceride Breath Test versus Fecal Elastase. Pancreatology 2017, 17, 580–585. [Google Scholar] [CrossRef]
- Powell-Brett, S.; Hall, L.; Edwards, M.; Roberts, K. A systematic review and meta-analysis of the accuracy and methodology of the (13)C mixed triglyceride breath test for the evaluation of pancreatic function. Pancreatology 2023, 23, 283–293. [Google Scholar] [CrossRef]
- Dominguez-Munoz, J.E.; Nieto, L.; Vilarino, M.; Lourido, M.V.; Iglesias-Garcia, J. Development and Diagnostic Accuracy of a Breath Test for Pancreatic Exocrine Insufficiency in Chronic Pancreatitis. Pancreas 2016, 45, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Carnie, L.E.; Shah, D.; Vaughan, K.; Kapacee, Z.A.; McCallum, L.; Abraham, M.; Backen, A.; McNamara, M.G.; Hubner, R.A.; Barriuso, J.; et al. Prospective Observational Study of Prevalence, Assessment and Treatment of Pancreatic Exocrine Insufficiency in Patients with Inoperable Pancreatic Malignancy (PANcreatic Cancer Dietary Assessment-PanDA). Cancers 2023, 15, 2277. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Munoz, J.E.; de la Iglesia-Garcia, D.; Nieto-Garcia, L.; Alvarez-Castro, A.; San Bruno-Ruz, A.; Monteserin-Ron, L.; Lopez-Diaz, J.; Iglesias-Garcia, J. Endoscopic Pancreatic Drainage Improves Exocrine Pancreatic Function in Patients With Unresectable Pancreatic Cancer: A Double-Blind, Prospective, Randomized, Single-Center, Interventional Study. Pancreas 2021, 50, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Kato, H.; Nakao, A.; Kishimoto, W.; Nonami, T.; Harada, A.; Hayakawa, T.; Takagi, H. 13C-labeled trioctanoin breath test for exocrine pancreatic function test in patients after pancreatoduodenectomy. Am. J. Gastroenterol. 1993, 88, 64–69. [Google Scholar]
- Weaver, L.T.; Amarri, S.; Swart, G.R. 13C mixed triglyceride breath test. Gut 1998, 43 (Suppl. S3), S13–S19. [Google Scholar] [CrossRef]
- Loser, C.; Mollgaard, A.; Folsch, U.R. Faecal elastase 1: A novel, highly sensitive, and specific tubeless pancreatic function test. Gut 1996, 39, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, J.; Traverso, L.W. Exocrine function following the whipple operation as assessed by stool elastase. J. Gastrointest. Surg. 2006, 10, 1225–1229. [Google Scholar] [CrossRef]
- Capurso, G.; Traini, M.; Piciucchi, M.; Signoretti, M.; Arcidiacono, P.G. Exocrine pancreatic insufficiency: Prevalence, diagnosis, and management. Clin. Exp. Gastroenterol. 2019, 12, 129–139. [Google Scholar] [CrossRef]
- Chari, S.T.; Maitra, A.; Matrisian, L.M.; Shrader, E.E.; Wu, B.U.; Kambadakone, A.; Zhao, Y.Q.; Kenner, B.; Rinaudo, J.A.S.; Srivastava, S.; et al. Early Detection Initiative: A randomized controlled trial of algorithm-based screening in patients with new onset hyperglycemia and diabetes for early detection of pancreatic ductal adenocarcinoma. Contemp. Clin. Trials 2022, 113, 106659. [Google Scholar] [CrossRef]
- Afolabi, P.R.; McDonnell, D.; Byrne, C.D.; Wilding, S.; Goss, V.; Walters, J.; Hamady, Z.Z. DEPEND study protocol: Early detection of patients with pancreatic cancer—A pilot study to evaluate the utility of faecal elastase-1 and (13)C-mixed triglyceride breath test as screening tools in high-risk individuals. BMJ Open 2022, 12, e057271. [Google Scholar] [CrossRef]
- Iglesia, D.; Avci, B.; Kiriukova, M.; Panic, N.; Bozhychko, M.; Sandru, V.; de-Madaria, E.; Capurso, G. Pancreatic exocrine insufficiency and pancreatic enzyme replacement therapy in patients with advanced pancreatic cancer: A systematic review and meta-analysis. United Eur. Gastroenterol. J. 2020, 8, 1115–1125. [Google Scholar] [CrossRef]
- Perez, M.M.; Newcomer, A.D.; Moertel, C.G.; Go, V.L.; Dimagno, E.P. Assessment of weight loss, food intake, fat metabolism, malabsorption, and treatment of pancreatic insufficiency in pancreatic cancer. Cancer 1983, 52, 346–352. [Google Scholar] [CrossRef]
- Keller, J.; Bruckel, S.; Jahr, C.; Layer, P. A modified (1)(3)C-mixed triglyceride breath test detects moderate pancreatic exocrine insufficiency. Pancreas 2011, 40, 1201–1205. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Morifuji, M.; Murakami, Y.; Uemura, K.; Ohge, H.; Hayashidani, Y.; Sudo, T.; Sueda, T. Usefulness of a 13C-labeled mixed triglyceride breath test for assessing pancreatic exocrine function after pancreatic surgery. Surgery 2009, 145, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Vantrappen, G.R.; Rutgeerts, P.J.; Ghoos, Y.F.; Hiele, M.I. Mixed triglyceride breath test: A noninvasive test of pancreatic lipase activity in the duodenum. Gastroenterology 1989, 96, 1126–1134. [Google Scholar] [CrossRef] [PubMed]
- Loser, C.; Brauer, C.; Aygen, S.; Hennemann, O.; Folsch, U.R. Comparative clinical evaluation of the 13C-mixed triglyceride breath test as an indirect pancreatic function test. Scand. J. Gastroenterol. 1998, 33, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Keller, J.; Meier, V.; Wolfram, K.U.; Rosien, U.; Layer, P. Sensitivity and specificity of an abbreviated (13)C-mixed triglyceride breath test for measurement of pancreatic exocrine function. United Eur. Gastroenterol. J. 2014, 2, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Dahlerup, S.; Andersen, R.C.; Nielsen, B.S.; Schjodt, I.; Christensen, L.A.; Gerdes, L.U.; Dahlerup, J.F. First-time urea breath tests performed at home by 36,629 patients: A study of Helicobacter pylori prevalence in primary care. Helicobacter 2011, 16, 468–474. [Google Scholar] [CrossRef]
- Keller, J.; Hammer, H.F.; Hauser, B. (13) C-gastric emptying breath tests: Clinical use in adults and children. Neurogastroenterol. Motil. 2021, 33, e14172. [Google Scholar] [CrossRef]
- Bozek, M.; Jonderko, K.; Pilka, M. On a refinement of the (1)(3)C-mixed TAG breath test. Br. J. Nutr. 2012, 107, 211–217. [Google Scholar] [CrossRef]
- Goodwin, B.C.; Myers, L.; Ireland, M.J.; March, S.; Ralph, N.; Dunn, J.; Chambers, S.; Aitken, J. Barriers to home bowel cancer screening. Psychooncology 2021, 30, 1756–1764. [Google Scholar] [CrossRef] [PubMed]
- Kotzur, M.; Macdonald, S.; O’Carroll, R.E.; O’Connor, R.C.; Irvine, A.; Steele, R.J.C.; Robb, K.A. What are common barriers and helpful solutions to colorectal cancer screening? A cross-sectional survey to develop intervention content for a planning support tool. BMJ Open 2022, 12, e062738. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.J.; Bannister, C.A.; Schrem, H. Enzyme replacement improves survival among patients with pancreatic cancer: Results of a population based study. Pancreatology 2019, 19, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Landers, A.; Muircroft, W.; Brown, H. Pancreatic enzyme replacement therapy (PERT) for malabsorption in patients with metastatic pancreatic cancer. BMJ Support. Palliat. Care 2016, 6, 75–79. [Google Scholar] [CrossRef] [PubMed]
- La Torre, M.; Ziparo, V.; Nigri, G.; Cavallini, M.; Balducci, G.; Ramacciato, G. Malnutrition and pancreatic surgery: Prevalence and outcomes. J. Surg. Oncol. 2013, 107, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.P.; Oldfield, L.; Ney, A.; Hart, P.A.; Keane, M.G.; Pandol, S.J.; Li, D.; Greenhalf, W.; Jeon, C.Y.; Koay, E.J.; et al. Early detection of pancreatic cancer. Lancet Gastroenterol. Hepatol. 2020, 5, 698–710. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, D.; Cheang, A.W.E.; Wilding, S.; Wild, S.H.; Frampton, A.E.; Byrne, C.D.; Hamady, Z.Z. Elevated Glycated Haemoglobin (HbA1c) Is Associated with an Increased Risk of Pancreatic Ductal Adenocarcinoma: A UK Biobank Cohort Study. Cancers 2023, 15, 4078. [Google Scholar] [CrossRef]
- Tiwari, A.K.; Kumar, V.; Yadav, D.P.; Shukla, S.K.; Das, D.; Singh, G.; Chaturvedi, D.; Dixit, V.K.; Chaturvedi, V.K. Hypercalcemia—An enigmatic cause of acute pancreatitis. J. Clin. Transl. Res. 2022, 8, 176–180. [Google Scholar]
- Herzog, D.C.; Delvin, E.E.; Albert, C.; Marcotte, J.E.; Pelletier, V.A.; Seidman, E.G. 13C-labeled mixed triglyceride breath test (13C MTG-BT) in healthy children and children with cystic fibrosis (CF) under pancreatic enzyme replacement therapy (PERT): A pilot study. Clin. Biochem. 2008, 41, 1489–1492. [Google Scholar] [CrossRef]
- Jonderko, K.; Dus, Z.; Szymszal, M.; Kasicka-Jonderko, A.; Blonska-Fajfrowska, B. Normative values for the 13C-mixed triglyceride breath test in two age groups. Med. Sci. Monit. 2009, 15, CR255–CR259. [Google Scholar]
- Haycock, G.B.; Schwartz, G.J.; Wisotsky, D.H. Geometric method for measuring body surface area: A height-weight formula validated in infants, children, and adults. J. Pediatr. 1978, 93, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.N.; Altman, D.G.; Campbell, M.J.; Royston, P. Analysis of serial measurements in medical research. BMJ 1990, 300, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Kalivianakis, M.; Verkade, H.J.; Stellaard, F.; Van Der Werf, M.; Elzinga, H.; Vonk, R.J. The 13C-mixed triglyceride breath test in healthy adults: Determinants of the 13CO2 response. Eur. J. Clin. Investig. 1997, 27, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Erickson, J.A.; Aldeen, W.E.; Grenache, D.G.; Ashwood, E.R. Evaluation of a fecal pancreatic elastase-1 enzyme-linked immunosorbent assay: Assessment versus an established assay and implication in classifying pancreatic function. Clin. Chim. Acta 2008, 397, 87–91. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Participant Characteristics | Healthy Volunteers (n = 24) | Pancreatic Ductal Adenocarcinoma (n = 23) | Chronic Pancreatitis (n = 12) | p Value |
|---|---|---|---|---|
| Age, Years *, | 63 (58–71) | 68 (56–75) | 64 (52–70) | 0.63 |
| Sex †, Men (%) | 13 (54.2%) | 16 (69.9%) | 10 (83.3%) | 0.17 |
| Weight, kg # | 81.3 ± 19.9 | 77.1 ± 9.6 | 79.9 ± 20.3 | 0.70 |
| Body Mass Index, kg/m2 # | 28.3 ± 6.5 | 26.0 ± 3.7 | 26.7 ± 6.0 | 0.36 |
| Diabetes Mellitus †, Yes | 2 (8.3%) a,b | 8 (34.8%) | 4 (33.3%) | 0.09 |
| New-Onset Diabetes Mellitus †, Yes (<36 months since diagnosis of diabetes mellitus) | 0 | 7 (30.4%) | 1 (8.3%) | 0.004 |
| Cumulative Percentage Dose Recovered of 13CO2 at 240 min, % * | 31.5 (28.1–37.4) a,b | 14.2 (7.3–28.8) | 15.9 (2.2–27.0) | <0.001 |
| Faecal Elastase-1, µg/g * | 500 (n/a) a,b | 87.5 (15–500) | 21 (15–386) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McDonnell, D.; Afolabi, P.R.; Wilding, S.; Griffiths, G.O.; Swann, J.R.; Byrne, C.D.; Hamady, Z.Z. Utilising Pancreatic Exocrine Insufficiency in the Detection of Resectable Pancreatic Ductal Adenocarcinoma. Cancers 2023, 15, 5756. https://doi.org/10.3390/cancers15245756
McDonnell D, Afolabi PR, Wilding S, Griffiths GO, Swann JR, Byrne CD, Hamady ZZ. Utilising Pancreatic Exocrine Insufficiency in the Detection of Resectable Pancreatic Ductal Adenocarcinoma. Cancers. 2023; 15(24):5756. https://doi.org/10.3390/cancers15245756
Chicago/Turabian StyleMcDonnell, Declan, Paul R. Afolabi, Sam Wilding, Gareth O. Griffiths, Jonathan R. Swann, Christopher D. Byrne, and Zaed Z. Hamady. 2023. "Utilising Pancreatic Exocrine Insufficiency in the Detection of Resectable Pancreatic Ductal Adenocarcinoma" Cancers 15, no. 24: 5756. https://doi.org/10.3390/cancers15245756