Predictive Factors for Chemoradiation-Induced Oral Mucositis and Dysphagia in Head and Neck Cancer: A Scoping Review

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
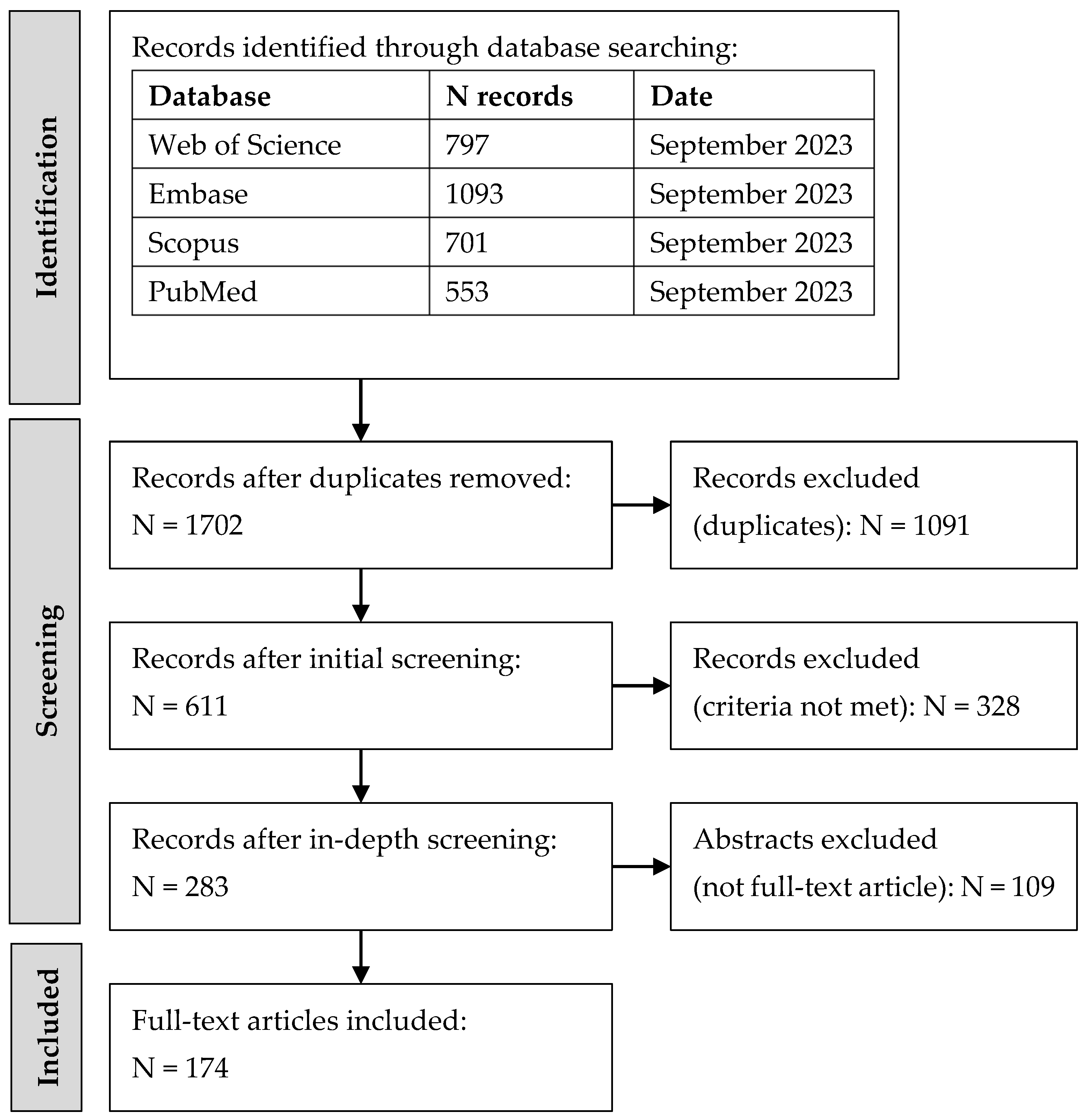
3.1. Identification and Selection of Studies
3.2. Overview of Included Studies
3.3. Predictors of Oral Mucositis
3.4. Predictors of Dysphagia
3.5. Predictive Models for Oral Mucositis and Dysphagia
4. Discussion
4.1. Predictors of OM and Dysphagia
4.2. Performance of Predictive Models
4.3. Limitations of Predictive Models
4.4. Recommendations for Future Model Development
4.5. Limitations of this Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Database | Search String | N Results | Date |
|---|---|---|---|
| Embase | TITLE = (toxicit* OR morbidit* OR “side effect*” OR mucositis OR dysphagia OR deglutition OR swallow* OR “tube feed*” OR ryle* OR enteral OR nasogastric OR intubation OR aspiration OR stricture* OR gastronom* OR “oral intake”) AND (predict* OR model* OR correlat* OR corresp* OR depend* OR assoc* OR relation* OR interact* OR link* OR “risk factors”) TI/AB/KW = (mucositis OR dysphagia OR deglutition OR swallow* OR “tube feed*” OR ryle* OR enteral OR nasogastric OR intubation OR gastronom* OR “oral intake”) AND (radiation OR chemotherap* OR radiotherap* OR chemoradiation OR chemoradiotherap* OR radiochemotherap* OR pharmacotherap* OR “IMRT” OR “VMAT” OR “3DCRT” OR “CRT”) FILTERS Publication Year >= 2000 Abstract OR Article | 1093 | 9/2023 |
| PubMed | (((“Stomatitis”[Mesh] OR “Deglutition Disorders”[Mesh]) AND (“Radiotherapy”[Mesh] OR “Drug Therapy”[Mesh]))) AND ((predict*[Title] OR model*[Title] OR correlat*[Title] OR corresp*[Title] OR depend*[Title] OR assoc*[Title] OR relat*[Title] OR interact*[Title] OR link*[Title] OR “risk*”[Title])) FILTERS Publication Year >= 2000 | 553 | 9/2023 |
| Scopus | TITLE = (toxicit* OR morbidit* OR “side effect*” OR mucositis OR dysphagia OR deglutition OR swallow* OR “tube feed*” OR ryle* OR enteral OR nasogastric OR intubation OR aspiration OR stricture* OR gastronom* OR “oral intake”) AND (predict* OR model* OR correlat* OR corresp* OR depend* OR assoc* OR relation* OR interact* OR link* OR “risk factors”) TI/AB/KW = (mucositis OR dysphagia OR deglutition OR swallow* OR “tube feed*” OR ryle* OR enteral OR nasogastric OR intubation OR gastronom* OR “oral intake”) AND (radiation OR chemotherap* OR radiotherap* OR chemoradiation OR chemoradiotherap* OR radiochemotherap* OR pharmacotherap* OR “IMRT” OR “VMAT” OR “3DCRT” OR “CRT”) FILTERS Publication Year >= 2000 Abstract OR Article | 701 | 9/2023 |
| Web of Science | TITLE = (toxicit* OR morbidit* OR “side effect*” OR mucositis OR dysphagia OR deglutition OR swallow* OR “tube feed*” OR ryle* OR enteral OR nasogastric OR intubation OR aspiration OR stricture* OR gastronom* OR “oral intake”) AND (predict* OR model* OR correlat* OR corresp* OR depend* OR assoc* OR relation* OR interact* OR link* OR “risk factors”) TOPIC = (mucositis OR dysphagia OR deglutition OR swallow* OR “tube feed*” OR ryle* OR enteral OR nasogastric OR intubation OR gastronom* OR “oral intake”) AND (radiation OR chemotherap* OR radiotherap* OR chemoradiation OR chemoradiotherap* OR radiochemotherap* OR pharmacotherap* OR “IMRT” OR “VMAT” OR “3DCRT” OR “CRT”) FILTERS Publication Year >= 2000 Abstract OR Article | 797 | 9/2023 |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gormley, M.; Creaney, G.; Schache, A.; Ingarfield, K.; Conway, D.I. Reviewing the Epidemiology of Head and Neck Cancer: Definitions, Trends and Risk Factors. Br. Dent. J. 2022, 233, 780–786. [Google Scholar] [CrossRef] [PubMed]
- Gianfaldoni, S.; Gianfaldoni, R.; Wollina, U.; Lotti, J.; Tchernev, G.; Lotti, T. An Overview on Radiotherapy: From Its History to Its Current Applications in Dermatology. Open Access Maced J. Med. Sci. 2017, 5, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Tepper, J.E. Radiation Therapy-Associated Toxicity: Etiology, Management, and Prevention. CA Cancer J. Clin. 2021, 71, 437–454. [Google Scholar] [CrossRef] [PubMed]
- Bowen, J.; Al-Dasooqi, N.; Bossi, P.; Wardill, H.; Van Sebille, Y.; Al-Azri, A.; Bateman, E.; Correa, M.E.; Raber-Durlacher, J.; Kandwal, A.; et al. The Pathogenesis of Mucositis: Updated Perspectives and Emerging Targets. Support. Care Cancer 2019, 27, 4023–4033. [Google Scholar] [CrossRef] [PubMed]
- Cox, J.D.; Stetz, J.; Pajak, T.F. Toxicity Criteria of the Radiation Therapy Oncology Group (Rtog) and the European Organization for Research and Treatment of Cancer (EORTC). Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1341–1346. [Google Scholar] [CrossRef]
- Brook, I. Late Side Effects of Radiation Treatment for Head and Neck Cancer. Radiat. Oncol. J. 2020, 38, 84–92. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE); Version 5.0; US Department of Health and Human Services: Washington, DC, USA, 2017.
- World Health Organization. Who Handbook for Reporting Results of Cancer Treatment; World Health Organization: Geneva, Switzerland, 1979. [Google Scholar]
- Fesinmeyer, M.D.; Mehta, V.; Blough, D.; Tock, L.; Ramsey, S.D. Effect of Radiotherapy Interruptions on Survival in Medicare Enrollees with Local and Regional Head-and-Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 675–681. [Google Scholar] [CrossRef]
- Brown, T.J.; Gupta, A. Management of Cancer Therapy–Associated Oral Mucositis. JCO Oncol. Pract. 2020, 16, 103–109. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events; Version 4.0; US Department of Health and Human Services: Washington, DC, USA, 2010.
- Moroney, L.B.; Helios, J.; Ward, E.C.; Crombie, J.; Wockner, L.F.; Burns, C.L.; Spurgin, A.-L.; Blake, C.; Kenny, L.; Hughes, B.G.M. Patterns of Dysphagia and Acute Toxicities in Patients with Head and Neck Cancer Undergoing Helical Imrt±Concurrent Chemotherapy. Oral Oncol. 2017, 64, 1–8. [Google Scholar] [CrossRef]
- O’Neill, C.B.; Baxi, S.S.; Atoria, C.L.; O’Neill, J.P.; Henman, M.C.; Sherman, E.J.; Lee, N.Y.; Pfister, D.G.; Elkin, E.B. Treatment-Related Toxicities in Older Adults with Head and Neck Cancer: A Population-Based Analysis. Cancer 2015, 121, 2083–2089. [Google Scholar] [CrossRef] [PubMed]
- Prisma Extension for Scoping Reviews (Prisma-Scr): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [CrossRef] [PubMed]
- Zhu, X.X.; Yang, X.J.; Chao, Y.L.; Zheng, H.M.; Sheng, H.F.; Liu, H.Y.; He, Y.; Zhou, H.W. The Potential Effect of Oral Microbiota in the Prediction of Mucositis During Radiotherapy for Nasopharyngeal Carcinoma. eBioMedicine 2017, 18, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, E.; Iacovelli, N.A.; Rancati, T.; Cicchetti, A.; Bossi, P.; Pignoli, E.; Bergamini, C.; Licitra, L.; Fallai, C.; Valdagni, R.; et al. Multivariable Model for Predicting Acute Oral Mucositis During Combined Imrt and Chemotherapy for Locally Advanced Nasopharyngeal Cancer Patients. Oral Oncol. 2018, 86, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Sharabiani, M.; Clementel, E.; Andratschke, N.; Collette, L.; Fortpied, C.; Gregoire, V.; Overgaard, J.; Willmann, J.; Hurkmans, C. Independent External Validation Using the Eortc Hncg-Rog 1219 Dahanca Trial Data of Ntcp Models for Acute Oral Mucositis. Radiother. Oncol. 2021, 161, 35–39. [Google Scholar] [CrossRef] [PubMed]
- Dean, J.A.; Wong, K.H.; Welsh, L.C.; Jones, A.B.; Schick, U.; Newbold, K.L.; Bhide, S.A.; Harrington, K.J.; Nutting, C.M.; Gulliford, S.L. Normal Tissue Complication Probability (NTCP) Modelling Using Spatial Dose Metrics and Machine Learning Methods for Severe Acute Oral Mucositis Resulting from Head and Neck Radiotherapy. Radiother. Oncol. 2016, 120, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Huang, L.; Wang, H.; Shi, Z.; Huang, Y.; Liang, L.; Wang, R.; Hu, K. Predicting Nomogram for Severe Oral Mucositis in Patients with Nasopharyngeal Carcinoma During Intensity-Modulated Radiation Therapy: A Retrospective Cohort Study. Curr. Oncol. 2023, 30, 219–232. [Google Scholar] [CrossRef]
- Li, P.J.; Li, K.X.; Jin, T.; Lin, H.M.; Fang, J.B.; Yang, S.Y.; Shen, W.; Chen, J.; Zhang, J.; Chen, X.Z.; et al. Predictive Model and Precaution for Oral Mucositis During Chemo-Radiotherapy in Nasopharyngeal Carcinoma Patients. Front. Oncol. 2020, 10, 596822. [Google Scholar] [CrossRef]
- Hansen, C.R.; Bertelsen, A.; Zukauskaite, R.; Johnsen, L.; Bernchou, U.; Thwaites, D.I.; Eriksen, J.G.; Johansen, J.; Brink, C. Prediction of Radiation-Induced Mucositis of H&N Cancer Patients Based on a Large Patient Cohort. Radiother. Oncol. 2020, 147, 15–21. [Google Scholar] [CrossRef]
- Dong, Y.; Zhang, J.; Lam, S.; Zhang, X.; Liu, A.; Teng, X.; Han, X.; Cao, J.; Li, H.; Lee, F.K.; et al. Multimodal Data Integration to Predict Severe Acute Oral Mucositis of Nasopharyngeal Carcinoma Patients Following Radiation Therapy. Cancers 2023, 15, 2032. [Google Scholar] [CrossRef]
- Al-Qadami, G.; Bowen, J.; Van Sebille, Y.; Secombe, K.; Dorraki, M.; Verjans, J.; Wardill, H.; Le, H. Baseline Gut Microbiota Composition Is Associated with Oral Mucositis and Tumour Recurrence in Patients with Head and Neck Cancer: A Pilot Study. Support. Care Cancer 2023, 31, 98. [Google Scholar] [CrossRef] [PubMed]
- Bansal, A.; Bedi, N.; Kaur, R.; Singh, G.; Benipal, R.P.S.; Dangwal, V. Correlation of Oral Mucosa Dose and Volume Parameters with Grade 3 Mucositis, in Patients Treated with Volumetric Modulated Arc Radiotherapy for Oropharyngeal Cancer? Jpn. J. Clin. Oncol. 2022, 53, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Chung, A.; Chung, Y.-T.; Liang, Y.-W.; Chung, Y.-L. Waldeyer Ring Microbiome in Relation to Chemoradiation-Induced Oral Mucositis in Patients with Nasopharyngeal Carcinoma. Head Neck 2023, 45, 2047–2057. [Google Scholar] [CrossRef] [PubMed]
- Lv, J.; Liao, S.; Li, B.; Pan, L.; Wang, R. Scheduling Radiotherapy for Patients with Nasopharyngeal Carcinoma in the Corresponding Time Window Can Reduce Radiation-Induced Oral Mucositis: A Randomized, Prospective Study. Cancer Med. 2023, 12, 16032–16040. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Yang, G.; An, W.; Wang, W.; Li, F.; Meng, Y.; Wang, X. Correlations between the Severity of Radiation-Induced Oral Mucositis and Salivary Epidermal Growth Factor as Well as Inflammatory Cytokines in Patients with Head and Neck Cancer. Head Neck 2023, 45, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Alterovitz, G.; Tuthill, C.; Rios, I.; Modelska, K.; Sonis, S. Personalized Medicine for Mucositis: Bayesian Networks Identify Unique Gene Clusters Which Predict the Response to Gamma-D-Glutamyl-L-Tryptophan (Scv-07) for the Attenuation of Chemoradiation-Induced Oral Mucositis. Oral Oncol. 2011, 47, 951–955. [Google Scholar] [CrossRef] [PubMed]
- Bentzen, S.M.; Saunders, M.I.; Dische, S.; Bond, S.J. Radiotherapy-Related Early Morbidity in Head and Neck Cancer: Quantitative Clinical Radiobiology as Deduced from the Chart Trial. Radiother. Oncol. 2001, 60, 123–135. [Google Scholar] [CrossRef]
- Bjarnason, G.A.; Mackenzie, R.G.; Nabid, A.; Hodson, I.D.; El-Sayed, S.; Grimard, L.; Brundage, M.; Wright, J.; Hay, J.; Ganguly, P.; et al. Comparison of Toxicity Associated with Early Morning Versus Late Afternoon Radiotherapy in Patients with Head-and-Neck Cancer: A Prospective Randomized Trial of the National Cancer Institute of Canada Clinical Trials Group (Hn3). Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 166–172. [Google Scholar] [CrossRef]
- Brzozowska, A.; Mlak, R.; Homa-Mlak, I.; Golebiowski, P.; Mazurek, M.; Ciesielka, M.; and Malecka-Massalska, T. Polymorphism of Regulatory Region of Apeh Gene (C. −521g > C, Rs4855883) as a Relevant Predictive Factor for Radiotherapy Induced Oral Mucositis and Overall Survival in Head Neck Cancer Patients. Oncotarget 2018, 9, 29644–29653. [Google Scholar] [CrossRef]
- Brzozowska, A.; Powrozek, T.; Homa-Mlak, I.; Mlak, R.; Ciesielka, M.; Golebiowski, P.; Malecka-Massalska, T. Polymorphism of Promoter Region of Tnfrsf1a Gene (−610 T > G) as a Novel Predictive Factor for Radiotherapy Induced Oral Mucositis in Hnc Patients. Pathol. Oncol. Res. 2018, 24, 135–143. [Google Scholar] [CrossRef]
- Brzozowska, A.; Mlak, R.; Golebiowski, P.; Malecka-Massalska, T. Status of Hydration Assessed by Bioelectrical Impedance Analysis: A Valuable Predictive Factor for Radiation-Induced Oral Mucositis in Head and Neck Cancer Patients. Clin. Transl. Oncol. 2019, 21, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.C.; Lai, Y.H.; Huang, B.S.; Lin, C.Y.; Fan, K.H.; Chang, J.T. Changes and Predictors of Radiation-Induced Oral Mucositis in Patients with Oral Cavity Cancer During Active Treatment. Eur. J. Oncol. Nurs. 2015, 19, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Wu, M.; Li, G.; Hua, L.; Chen, S.; Huang, H. Association between Xrcc1 Single-Nucleotide Polymorphism and Acute Radiation Reaction in Patients with Nasopharyngeal Carcinoma: A Cohort Study. Med. Baltim. 2017, 96, e8202. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Jiang, H.; Jiang, D.; Wu, Q.; Li, Z.; Hua, X.; Hu, X.; Zhao, H.; Wang, X.; Yu, H.; et al. Pretreatment Serum Vitamin Level Predicts Severity of Radiation-Induced Oral Mucositis in Patients with Nasopharyngeal Carcinoma. Head Neck 2021, 43, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Correia, A.V.; Coelho, M.R.; de Oliveira Mendes Cahu, G.G.; de Almeida Silva, J.L.; da Mota Vasconcelos Brasil, C.; de Castro, J.F. Seroprevalence of Hsv-1/2 and Correlation with Aggravation of Oral Mucositis in Patients with Squamous Cell Carcinoma of the Head and Neck Region Submitted to Antineoplastic Treatment. Support. Care Cancer 2015, 23, 2105–2111. [Google Scholar] [CrossRef] [PubMed]
- Desilets, A.; McCarvill, W.; Aubin, F.; Bahig, H.; Ballivy, O.; Charpentier, D.; Filion, E.; Jamal, R.; Lambert, L.; Nguyen-Tan, P.F.; et al. Upfront Dpyd Genotyping and Toxicity Associated with Fluoropyrimidine-Based Concurrent Chemoradiotherapy for Oropharyngeal Carcinomas: A Work in Progress. Curr. Oncol. 2022, 29, 497–509. [Google Scholar] [CrossRef] [PubMed]
- Devaraju, C.J.; Lokanatha, D.; Bapsy, P.P.; Suresh, A.V.; Viswanath, G.; Sandhya, B. Risk Scoring for Predicting Mucositis in Indian Patients with Esophageal Carcinoma Receiving Concurrent Chemoradiotherapy. Gastrointest. Cancer Res. 2009, 3, 4–6. [Google Scholar]
- Epstein, J.B.; Gorsky, M.; Guglietta, A.; Le, N.; Sonis, S.T. The Correlation between Epidermal Growth Factor Levels in Saliva and the Severity of Oral Mucositis During Oropharyngeal Radiation Therapy. Cancer 2000, 89, 2258–2265. [Google Scholar] [CrossRef]
- Fanetti, G.; Polesel, J.; Fratta, E.; Muraro, E.; Lupato, V.; Alfieri, S.; Gobitti, C.; Minatel, E.; Matrone, F.; Caroli, A.; et al. Prognostic Nutritional Index Predicts Toxicity in Head and Neck Cancer Patients Treated with Definitive Radiotherapy in Association with Chemotherapy. Nutrients 2021, 13, 12. [Google Scholar] [CrossRef]
- Gu, F.; Farrugia, M.K.; Duncan, W.D.; Feng, Y.; Hutson, A.D.; Schlecht, N.F.; Repasky, E.A.; Antoch, M.P.; Miller, A.; Platek, A.; et al. Daily Time of Radiation Treatment Is Associated with Subsequent Oral Mucositis Severity During Radiotherapy in Head and Neck Cancer Patients. Cancer Epidemiol. Biomark. Prev. 2020, 29, 949–955. [Google Scholar] [CrossRef]
- Hanin, S.M.A.; Dharman, S.; Girija, A.S.S. Association of Salivary Microbes with Oral Mucositis among Patients Undergoing Chemoradiotherapy in Head and Neck Cancer: A Hospital-Based Prospective Study. J. Int. Oral Health 2022, 14, 53–60. [Google Scholar] [CrossRef]
- Homa-Mlak, I.; Brzozowska, A.; Mlak, R.; Szudy-Szczyrek, A.; Malecka-Massalska, T. Neutrophil-to-Lymphocyte Ratio as a Factor Predicting Radiotherapy Induced Oral Mucositis in Head Neck Cancer Patients Treated with Radiotherapy. J. Clin. Med. 2021, 10, 15. [Google Scholar] [CrossRef] [PubMed]
- Jehmlich, N.; Stegmaier, P.; Golatowski, C.; Salazar, M.G.; Rischke, C.; Henke, M.; Volker, U. Differences in the Whole Saliva Baseline Proteome Profile Associated with Development of Oral Mucositis in Head and Neck Cancer Patients Undergoing Radiotherapy. J. Proteom. 2015, 125, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Kawashita, Y.; Kitamura, M.; Soutome, S.; Ukai, T.; Umeda, M.; Saito, T. Association of Neutrophil-to-Lymphocyte Ratio with Severe Radiation-Induced Mucositis in Pharyngeal or Laryngeal Cancer Patients: A Retrospective Study. BMC Cancer 2021, 21, 1064. [Google Scholar] [CrossRef] [PubMed]
- Kawashita, Y.; Soutome, S.; Umeda, M.; Saito, T. Predictive Risk Factors Associated with Severe Radiation-Induced Mucositis in Nasopharyngeal or Oropharyngeal Cancer Patients: A Retrospective Study. Biomedicines 2022, 10, 8. [Google Scholar] [CrossRef]
- Kazmierska, J.; Barczak, W.; Winiecki, T.; Luczewski, L.; Marciniak, M.; Suchorska, W. The Kinetics of Gamma-H2ax During Radiotherapy of Head and Neck Cancer Potentially Allow for Prediction of Severe Mucositis. Radiol. Oncol. 2020, 54, 96–102. [Google Scholar] [CrossRef]
- Le, Z.; Niu, X.; Chen, Y.; Ou, X.; Zhao, G.; Liu, Q.; Tu, W.; Hu, C.; Kong, L.; Liu, Y. Predictive Single Nucleotide Polymorphism Markers for Acute Oral Mucositis in Patients with Nasopharyngeal Carcinoma Treated with Radiotherapy. Oncotarget 2017, 8, 63026–63037. [Google Scholar] [CrossRef]
- Li, H.; You, Y.; Lin, C.; Zheng, M.; Hong, C.; Chen, J.; Li, D.; Au, W.W.; Chen, Z. Xrcc1 Codon 399gln Polymorphism Is Associated with Radiotherapy-Induced Acute Dermatitis and Mucositis in Nasopharyngeal Carcinoma Patients. Radiat. Oncol. 2013, 8, 31. [Google Scholar] [CrossRef]
- Li, P.; Du, C.R.; Xu, W.C.; Shi, Z.L.; Zhang, Q.; Li, Z.B.; Fu, S. Correlation of Dynamic Changes in Gamma-H2ax Expression in Peripheral Blood Lymphocytes from Head and Neck Cancer Patients with Radiation-Induced Oral Mucositis. Radiat. Oncol. 2013, 8, 155. [Google Scholar] [CrossRef]
- Li, K.; Yang, L.; Hu, Q.Y.; Chen, X.Z.; Chen, M.; Chen, Y. Oral Mucosa Dose Parameters Predicting Grade >/=3 Acute Toxicity in Locally Advanced Nasopharyngeal Carcinoma Patients Treated with Concurrent Intensity-Modulated Radiation Therapy and Chemotherapy: An Independent Validation Study Comparing Oral Cavity Versus Mucosal Surface Contouring Techniques. Transl. Oncol. 2017, 10, 752–759. [Google Scholar] [CrossRef]
- Li, Q.; Liang, Y.; Liu, Z.; Yu, C. Associations of Gwas-Identified Risk Loci with Progression, Efficacy and Toxicity of Radiotherapy of Head and Neck Squamous Cell Carcinoma Treated with Radiotherapy. Pharmgenom. Pers. Med. 2021, 14, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Manur, J.G.; Vidyasagar, N. Correlation of Planning Target Volume with Mucositis for Head-and-Neck Cancer Patients Undergoing Chemoradiation. J. Cancer Res. Ther. 2020, 16, 565–568. [Google Scholar] [CrossRef] [PubMed]
- Mazzola, R.; Ricchetti, F.; Fersino, S.; Fiorentino, A.; Giaj Levra, N.; Di Paola, G.; Ruggieri, R.; Alongi, F. Predictors of Mucositis in Oropharyngeal and Oral Cavity Cancer in Patients Treated with Volumetric Modulated Radiation Treatment: A Dose-Volume Analysis. Head Neck 2016, 38 (Suppl. S1), E815–E819. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, H.; Miyai, H.; Yokoi, A.; Kobayashi, T.; Inabu, C.; Maruyama, T.; Ekuni, D.; Mizukawa, N.; Kariya, S.; Nishizaki, K.; et al. Relationship between Renal Dysfunction and Oral Mucositis in Patients Undergoing Concurrent Chemoradiotherapy for Pharyngeal Cancer: A Retrospective Cohort Study. In Vivo 2019, 33, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Mlak, R.; Powrozek, T.; Brzozowska, A.; Homa-Mlak, I.; Mazurek, M.; Golebiowski, P.; Sobieszek, G.; Malecka-Massalska, T. The Relationship between Tnf-Alpha Gene Promoter Polymorphism (−1211 T > C), the Plasma Concentration of Tnf-Alpha, and Risk of Oral Mucositis and Shortening of Overall Survival in Patients Subjected to Intensity-Modulated Radiation Therapy Due to Head and Neck Cancer. Support. Care Cancer 2020, 28, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Morais-Faria, K.; Palmier, N.R.; de Lima Correia, J.; de Castro Junior, G.; Dias, R.B.; da Graca Pinto, H.; Lopes, M.A.; Ribeiro, A.C.P.; Brandao, T.B.; Santos-Silva, A.R. Young Head and Neck Cancer Patients Are at Increased Risk of Developing Oral Mucositis and Trismus. Support. Care Cancer 2020, 28, 4345–4352. [Google Scholar] [CrossRef] [PubMed]
- Musha, A.; Shimada, H.; Shirai, K.; Saitoh, J.; Yokoo, S.; Chikamatsu, K.; Ohno, T.; Nakano, T. Prediction of Acute Radiation Mucositis Using an Oral Mucosal Dose Surface Model in Carbon Ion Radiotherapy for Head and Neck Tumors. PLoS ONE 2015, 10, e0141734. [Google Scholar] [CrossRef]
- Musha, A.; Fukata, K.; Saitoh, J.I.; Shirai, K.; Abe, T.; Mizukami, T.; Kawashima, M.; Yokoo, S.; Chikamatsu, K.; Ohno, T.; et al. Tongue Surface Model Can Predict Radiation Tongue Mucositis Due to Intensity-Modulated Radiation Therapy for Head and Neck Cancer. Int. J. Oral Maxillofac. Surg. 2020, 49, 44–50. [Google Scholar] [CrossRef]
- Nejatinamini, S.; Debenham, B.J.; Clugston, R.D.; Mawani, A.; Parliament, M.; Wismer, W.V.; Mazurak, V.C. Poor Vitamin Status Is Associated with Skeletal Muscle Loss and Mucositis in Head and Neck Cancer Patients. Nutrients 2018, 10, 11. [Google Scholar] [CrossRef]
- Nguyen, H.G.; Avanesov, A.; Gvozdikova, E.; Kandakova, E.; Kruchinina, L.; Alymov, Y.; Khaydar, D.; Golub, S. Microcirculatory Alterations in Patients with Oropharyngeal Cancer after Radiation Therapy: A Possible Correlation with Mucositis? Archiv. Euromed. 2020, 10, 128–133. [Google Scholar] [CrossRef]
- Nishii, M.; Soutome, S.; Kawakita, A.; Yutori, H.; Iwata, E.; Akashi, M.; Hasegawa, T.; Kojima, Y.; Funahara, M.; Umeda, M.; et al. Factors Associated with Severe Oral Mucositis and Candidiasis in Patients Undergoing Radiotherapy for Oral and Oropharyngeal Carcinomas: A Retrospective Multicenter Study of 326 Patients. Support. Care Cancer 2020, 28, 1069–1075. [Google Scholar] [CrossRef]
- Porock, D.; Nikoletti, S.; Cameron, F. The Relationship between Factors That Impair Wound Healing and the Severity of Acute Radiation Skin and Mucosal Toxicities in Head and Neck Cancer. Cancer Nurs. 2004, 27, 71–78. [Google Scholar] [CrossRef]
- Rupe, C.; Gioco, G.; Almadori, G.; Galli, J.; Micciche, F.; Olivieri, M.; Cordaro, M.; Lajolo, C. Oral Candida spp. Colonisation Is a Risk Factor for Severe Oral Mucositis in Patients Undergoing Radiotherapy for Head & Neck Cancer: Results from a Multidisciplinary Mono-Institutional Prospective Observational Study. Cancers 2022, 14, 4746. [Google Scholar] [CrossRef]
- Saedi, H.S.; Gerami, H.; Soltanipour, S.; Habibi, A.F.; Mirhosseyni, M.; Montazeri, S.; Nemati, S. Frequency of Chemoradiotherapy-Induced Mucositis and Related Risk Factors in Patients with the Head-and-Neck Cancers: A Survey in the North of Iran. Dent. Res. J. Isfahan 2019, 16, 354–359. [Google Scholar] [CrossRef]
- Saito, N.; Imai, Y.; Muto, T.; Sairenchi, T. Low Body Mass Index as a Risk Factor of Moderate to Severe Oral Mucositis in Oral Cancer Patients with Radiotherapy. Support. Care Cancer 2012, 20, 3373–3377. [Google Scholar] [CrossRef]
- Saito, N.; Truong, M.T.; Qureshi, M.M.; Lee, R.J.; Wang, J.W.; Ozonoff, A.; Sakai, O. Correlation of Mucositis During Head and Neck Radiotherapy with Computed Tomography Perfusion Imaging of the Oropharyngeal Mucosa. J. Comput. Assist. Tomogr. 2013, 37, 499–504. [Google Scholar] [CrossRef]
- Sakamoto, K.; Takeda, S.; Kanekiyo, S.; Nishiyama, M.; Kitahara, M.; Ueno, T.; Yamamoto, S.; Yoshino, S.; Hazama, S.; Okayama, N.; et al. Association of Tumor Necrosis Factor-Alpha Polymorphism with Chemotherapy-Induced Oral Mucositis in Patients with Esophageal Cancer. Mol. Clin. Oncol. 2017, 6, 125–129. [Google Scholar] [CrossRef]
- Sakashita, T.; Homma, A.; Hatakeyama, H.; Furusawa, J.; Kano, S.; Mizumachi, T.; Iizuka, S.; Onimaru, R.; Tsuchiya, K.; Yasuda, K.; et al. Comparison of Acute Toxicities Associated with Cetuximab-Based Bioradiotherapy and Platinum-Based Chemoradiotherapy for Head and Neck Squamous Cell Carcinomas: A Single-Institution Retrospective Study in Japan. Acta Otolaryngol. 2015, 135, 853–858. [Google Scholar] [CrossRef]
- Sanches, G.L.G.; da Silva Menezes, A.S.; Santos, L.I.; Duraes, C.P.; Fonseca, L.L.; Baldo, M.P.; de Oliveira Faria, T.; de Araujo Andrade, L.A.; Ekel, P.I.; Santos, S.H.S.; et al. Local Tissue Electrical Parameters Predict Oral Mucositis in Hnscc Patients: A Diagnostic Accuracy Double-Blind, Randomized Controlled Trial. Sci. Rep. 2020, 10, 9530. [Google Scholar] [CrossRef]
- Sanguineti, G.; Sormani, M.P.; Marur, S.; Gunn, G.B.; Rao, N.; Cianchetti, M.; Ricchetti, F.; McNutt, T.; Wu, B.; Forastiere, A. Effect of Radiotherapy and Chemotherapy on the Risk of Mucositis During Intensity-Modulated Radiation Therapy for Oropharyngeal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 235–242. [Google Scholar] [CrossRef]
- Schack, L.M.H.; Naderi, E.; Fachal, L.; Dorling, L.; Luccarini, C.; Dunning, A.M.; The Head and Neck Group of the Radiogenomics Consortium; The Danish Head and Neck Cancer Group (DAHANCA); Ong, E.H.W.; Chua, M.L.K.; et al. A Genome-Wide Association Study of Radiotherapy Induced Toxicity in Head and Neck Cancer Patients Identifies a Susceptibility Locus Associated with Mucositis. Br. J. Cancer 2022, 126, 1082–1090. [Google Scholar] [CrossRef]
- Schauer, M.C.; Holzmann, B.; Peiper, M.; Friess, H.; Knoefel, W.T.; Theisen, J. Interleukin-10 and -12 Predict Chemotherapy-Associated Toxicity in Esophageal Adenocarcinoma. J. Thorac. Oncol. 2010, 5, 1849–1854. [Google Scholar] [CrossRef]
- Soutome, S.; Yanamoto, S.; Nishii, M.; Kojima, Y.; Hasegawa, T.; Funahara, M.; Akashi, M.; Saito, T.; Umeda, M. Risk Factors for Severe Radiation-Induced Oral Mucositis in Patients with Oral Cancer. J. Dent. Sci. 2021, 16, 1241–1246. [Google Scholar] [CrossRef]
- Sunaga, T.; Nagatani, A.; Fujii, N.; Hashimoto, T.; Watanabe, T.; Sasaki, T. The Association between Cumulative Radiation Dose and the Incidence of Severe Oral Mucositis in Head and Neck Cancers During Radiotherapy. Cancer Rep. Hoboken 2021, 4, e1317. [Google Scholar] [CrossRef]
- Suresh, A.V.; Varma, P.P.; Sinha, S.; Deepika, S.; Raman, R.; Srinivasan, M.; Mandapal, T.; Reddy, C.O.; Anand, B.B. Risk-Scoring System for Predicting Mucositis in Patients of Head and Neck Cancer Receiving Concurrent Chemoradiotherapy [Rssm-Hn]. J. Cancer Res. Ther. 2010, 6, 448–451. [Google Scholar] [CrossRef]
- Tao, Z.; Gao, J.; Qian, L.; Huang, Y.; Zhou, Y.; Yang, L.; He, J.; Yang, J.; Wang, R.; Zhang, Y. Factors Associated with Acute Oral Mucosal Reaction Induced by Radiotherapy in Head and Neck Squamous Cell Carcinoma: A Retrospective Single-Center Experience. Med. Baltim. 2017, 96, e8446. [Google Scholar] [CrossRef]
- van den Broek, G.B.; Balm, A.J.; van den Brekel, M.W.; Hauptmann, M.; Schornagel, J.H.; Rasch, C.R. Relationship between Clinical Factors and the Incidence of Toxicity after Intra-Arterial Chemoradiation for Head and Neck Cancer. Radiother. Oncol. 2006, 81, 143–150. [Google Scholar] [CrossRef]
- Venkatesh, G.H.; Manjunath, V.B.; Mumbrekar, K.D.; Negi, H.; Fernandes, D.J.; Sharan, K.; Banerjee, S.; Bola Sadashiva, S.R. Polymorphisms in Radio-Responsive Genes and Its Association with Acute Toxicity among Head and Neck Cancer Patients. PLoS ONE 2014, 9, e89079. [Google Scholar] [CrossRef]
- Vera-Llonch, M.; Oster, G.; Hagiwara, M.; Sonis, S. Oral Mucositis in Patients Undergoing Radiation Treatment for Head and Neck Carcinoma. Cancer 2006, 106, 329–336. [Google Scholar] [CrossRef]
- Wu, C.; Liu, Y.; Shi, F.; Chen, F.; Zhao, Y.; Zhao, H. The Relationship of Serum Gastrin-17 and Oral Mucositis in Head and Neck Carcinoma Patients Receiving Radiotherapy. Discov. Oncol. 2022, 13, 110. [Google Scholar] [CrossRef]
- Yahya, S.; Benghiat, H.; Nightingale, P.; Tiffany, M.; Sanghera, P.; Hartley, A. Does Dose to an Oral Mucosa Organ at Risk Predict the Duration of Grade 3 Mucositis after Intensity-Modulated Radiotherapy for Oropharyngeal Cancer? Clin. Oncol. R. Coll. Radiol. 2016, 28, e216–e219. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Liu, Z. Potentially Functional Variants of Autophagy-Related Genes Are Associated with the Efficacy and Toxicity of Radiotherapy in Patients with Nasopharyngeal Carcinoma. Mol. Genet. Genom. Med. 2019, 7, e1030. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.W.; Wang, T.M.; Zhang, J.B.; Li, X.Z.; He, Y.Q.; Xiao, R.; Xue, W.Q.; Zheng, X.H.; Zhang, P.F.; Zhang, S.D.; et al. Genome-Wide Association Study Identifies Genetic Susceptibility Loci and Pathways of Radiation-Induced Acute Oral Mucositis. J. Transl. Med. 2020, 18, 224. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Huang, Y.; Liu, L.; Wang, J.; Yin, J.; Huang, L.; Chen, S.; Li, J.; Yuan, H.; Yang, G.; et al. Genetic Polymorphisms of Wnt/Beta-Catenin Pathway Genes Are Associated with the Efficacy and Toxicities of Radiotherapy in Patients with Nasopharyngeal Carcinoma. Oncotarget 2016, 7, 82528–82537. [Google Scholar] [CrossRef] [PubMed]
- Zahn, K.L.; Wong, G.; Bedrick, E.J.; Poston, D.G.; Schroeder, T.M.; Bauman, J.E. Relationship of Protein and Calorie Intake to the Severity of Oral Mucositis in Patients with Head and Neck Cancer Receiving Radiation Therapy. Head Neck 2012, 34, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Deneuve, S.; Bastogne, T.; Duclos, M.; Mirjolet, C.; Bois, P.; Bachmann, P.; Nokovitch, L.; Roux, P.E.; Girodet, D.; Poupart, M.; et al. Predicting Acute Severe Toxicity for Head and Neck Squamous Cell Carcinomas by Combining Dosimetry with a Radiosensitivity Biomarker: A Pilot Study. Tumori 2022, 3008916221078061. [Google Scholar] [CrossRef]
- Otter, S.; Schick, U.; Gulliford, S.; Lal, P.; Franceschini, D.; Newbold, K.; Nutting, C.; Harrington, K.; Bhide, S. Evaluation of the Risk of Grade 3 Oral and Pharyngeal Dysphagia Using Atlas-Based Method and Multivariate Analyses of Individual Patient Dose Distributions. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 507–515. [Google Scholar] [CrossRef]
- Srivastava, S.; Rastogi, M.; Gandhi, A.K.; Khurana, R.; Hadi, R.; Sapru, S.; Srivastava, A.; Bharati, A.; Husain, N.; Mishra, S.P.; et al. Correlation of Pd-L1 Expression with Toxicities and Response in Oropharyngeal Cancers Treated with Definitive Chemoradiotherapy. Contemp. Oncol. Pozn. 2022, 26, 180–186. [Google Scholar] [CrossRef]
- Werbrouck, J.; De Ruyck, K.; Duprez, F.; Veldeman, L.; Claes, K.; Van Eijkeren, M.; Boterberg, T.; Willems, P.; Vral, A.; De Neve, W.; et al. Acute Normal Tissue Reactions in Head-and-Neck Cancer Patients Treated with Imrt: Influence of Dose and Association with Genetic Polymorphisms in DNA Dsb Repair Genes. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 1187–1195. [Google Scholar] [CrossRef]
- De Ruyck, K.; Duprez, F.; Werbrouck, J.; Sabbe, N.; de Sofie, L.; Boterberg, T.; Madani, I.; Thas, O.; de Wilfried, N.; Thierens, H. A Predictive Model for Dysphagia Following Imrt for Head and Neck Cancer: Introduction of the Emlasso Technique. Radiother. Oncol. 2013, 107, 295–299. [Google Scholar] [CrossRef]
- Willemsen, A.C.H.; Kok, A.; Baijens, L.W.J.; de Boer, J.P.; de Bree, R.; Devriese, L.A.; Driessen, C.M.L.; van Herpen, C.M.L.; Hoebers, F.J.P.; Kaanders, J.; et al. Development and External Validation of a Prediction Model for Tube Feeding Dependency for at Least Four Weeks During Chemoradiotherapy for Head and Neck Cancer. Clin. Nutr. 2022, 41, 177–185. [Google Scholar] [CrossRef]
- Gaito, S.; France, A.; Foden, P.; Abravan, A.; Burnet, N.; Garcez, K.; Kota, V.R.; Lee, L.W.; Price, J.; Sykes, A.; et al. A Predictive Model for Reactive Tube Feeding in Head and Neck Cancer Patients Undergoing Definitive (Chemo) Radiotherapy. Clin. Oncol. R. Coll. Radiol. 2021, 33, e433–e441. [Google Scholar] [CrossRef]
- Willemsen, A.C.H.; Kok, A.; van Kuijk, S.M.J.; Baijens, L.W.J.; de Bree, R.; Devriese, L.A.; Hoebers, F.J.P.; Lalisang, R.I.; Schols, A.; Terhaard, C.H.J.; et al. Prediction Model for Tube Feeding Dependency During Chemoradiotherapy for at Least Four Weeks in Head and Neck Cancer Patients: A Tool for Prophylactic Gastrostomy Decision Making. Clin. Nutr. 2020, 39, 2600–2608. [Google Scholar] [CrossRef]
- Dean, J.; Wong, K.; Gay, H.; Welsh, L.; Jones, A.B.; Schick, U.; Oh, J.H.; Apte, A.; Newbold, K.; Bhide, S.; et al. Incorporating Spatial Dose Metrics in Machine Learning-Based Normal Tissue Complication Probability (NTCP) Models of Severe Acute Dysphagia Resulting from Head and Neck Radiotherapy. Clin. Transl. Radiat. Oncol. 2018, 8, 27–39. [Google Scholar] [CrossRef]
- Yahya, N.; Linge, A.; Leger, K.; Maile, T.; Kemper, M.; Haim, D.; Johrens, K.; Troost, E.G.C.; Krause, M.; Lock, S. Assessment of Gene Expressions from Squamous Cell Carcinoma of the Head and Neck to Predict Radiochemotherapy-Related Xerostomia and Dysphagia. Acta Oncol. 2022, 61, 856–863. [Google Scholar] [CrossRef]
- Soderstrom, K.; Nilsson, P.; Laurell, G.; Zackrisson, B.; Jaghagen, E.L. Dysphagia - Results from Multivariable Predictive Modelling on Aspiration from a Subset of the Artscan Trial. Radiother. Oncol. 2017, 122, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Christianen, M.E.; van der Schaaf, A.; van der Laan, H.P.; Verdonck-de Leeuw, I.M.; Doornaert, P.; Chouvalova, O.; Steenbakkers, R.J.; Leemans, C.R.; Oosting, S.F.; van der Laan, B.F.; et al. Swallowing Sparing Intensity Modulated Radiotherapy (Sw-Imrt) in Head and Neck Cancer: Clinical Validation According to the Model-Based Approach. Radiother. Oncol. 2016, 118, 298–303. [Google Scholar] [CrossRef]
- Kalendralis, P.; Sloep, M.; Moni George, N.; Snel, J.; Veugen, J.; Hoebers, F.; Wesseling, F.; Unipan, M.; Veening, M.; Langendijk, J.A.; et al. Independent Validation of a Dysphagia Dose Response Model for the Selection of Head and Neck Cancer Patients to Proton Therapy. Phys. Imaging Radiat. Oncol. 2022, 24, 47–52. [Google Scholar] [CrossRef]
- Christianen, M.E.; Schilstra, C.; Beetz, I.; Muijs, C.T.; Chouvalova, O.; Burlage, F.R.; Doornaert, P.; Koken, P.W.; Leemans, C.R.; Rinkel, R.N.; et al. Predictive Modelling for Swallowing Dysfunction after Primary (Chemo)Radiation: Results of a Prospective Observational Study. Radiother. Oncol. 2012, 105, 107–114. [Google Scholar] [CrossRef]
- Wopken, K.; Bijl, H.P.; van der Schaaf, A.; Christianen, M.E.; Chouvalova, O.; Oosting, S.F.; van der Laan, B.F.; Roodenburg, J.L.; Leemans, C.R.; Slotman, B.J.; et al. Development and Validation of a Prediction Model for Tube Feeding Dependence after Curative (Chemo-) Radiation in Head and Neck Cancer. PLoS ONE 2014, 9, e94879. [Google Scholar] [CrossRef]
- MD Anderson Head and Neck Cancer Symptom Working Group. Beyond Mean Pharyngeal Constrictor Dose for Beam Path Toxicity in Non-Target Swallowing Muscles: Dose-Volume Correlates of Chronic Radiation-Associated Dysphagia (Rad) after Oropharyngeal Intensity Modulated Radiotherapy. Radiother. Oncol. 2016, 118, 304–314. [Google Scholar] [CrossRef] [PubMed]
- Wentzel, A.; Hanula, P.; van Dijk, L.V.; Elgohari, B.; Mohamed, A.S.R.; Cardenas, C.E.; Fuller, C.D.; Vock, D.M.; Canahuate, G.; Marai, G.E. Precision Toxicity Correlates of Tumor Spatial Proximity to Organs at Risk in Cancer Patients Receiving Intensity-Modulated Radiotherapy. Radiother. Oncol. 2020, 148, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Wopken, K.; Bijl, H.P.; van der Schaaf, A.; van der Laan, H.P.; Chouvalova, O.; Steenbakkers, R.J.; Doornaert, P.; Slotman, B.J.; Oosting, S.F.; Christianen, M.E.; et al. Development of a Multivariable Normal Tissue Complication Probability (Ntcp) Model for Tube Feeding Dependence after Curative Radiotherapy/Chemo-Radiotherapy in Head and Neck Cancer. Radiother. Oncol. 2014, 113, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Alexidis, P.; Bangeas, P.; Efthymiadis, K.; Drevelegkas, K.; Kolias, P. Investigating Factors Associated to Dysphagia and Need for Percutaneous Endoscopic Gastrostomy in Patients with Head and Neck Cancer Receiving Radiation Therapy. J. Cancer 2022, 13, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Al-Othman, M.O.; Amdur, R.J.; Morris, C.G.; Hinerman, R.W.; Mendenhall, W.M. Does Feeding Tube Placement Predict for Long-Term Swallowing Disability after Radiotherapy for Head and Neck Cancer? Head Neck 2003, 25, 741–747. [Google Scholar] [CrossRef]
- Anderson, N.J.; Jackson, J.E.; Smith, J.G.; Wada, M.; Schneider, M.; Poulsen, M.; Rolfo, M.; Fahandej, M.; Gan, H.; Joon, D.L.; et al. Pretreatment Risk Stratification of Feeding Tube Use in Patients Treated with Intensity-Modulated Radiotherapy for Head and Neck Cancer. Head Neck 2018, 40, 2181–2192. [Google Scholar] [CrossRef] [PubMed]
- Awan, M.J.; Mohamed, A.S.; Lewin, J.S.; Baron, C.A.; Gunn, G.B.; Rosenthal, D.I.; Holsinger, F.C.; Schwartz, D.L.; Fuller, C.D.; Hutcheson, K.A. Late Radiation-Associated Dysphagia (Late-Rad) with Lower Cranial Neuropathy after Oropharyngeal Radiotherapy: A Preliminary Dosimetric Comparison. Oral Oncol. 2014, 50, 746–752. [Google Scholar] [CrossRef]
- Barnhart, M.K.; Ward, E.C.; Cartmill, B.; Robinson, R.A.; Simms, V.A.; Chandler, S.J.; Wurth, E.T.; Smee, R.I. Pretreatment Factors Associated with Functional Oral Intake and Feeding Tube Use at 1 and 6 Months Post-Radiotherapy (+/− Chemotherapy) for Head and Neck Cancer. Eur. Arch. Otorhinolaryngol. 2017, 274, 507–516. [Google Scholar] [CrossRef]
- Best, S.R.; Ha, P.K.; Blanco, R.G.; Saunders, J.R., Jr.; Zinreich, E.S.; Levine, M.A.; Pai, S.I.; Walker, M.; Trachta, J.; Ulmer, K.; et al. Factors Associated with Pharyngoesophageal Stricture in Patients Treated with Concurrent Chemotherapy and Radiation Therapy for Oropharyngeal Squamous Cell Carcinoma. Head Neck 2011, 33, 1727–1734. [Google Scholar] [CrossRef]
- Bhayani, M.K.; Hutcheson, K.A.; Barringer, D.A.; Lisec, A.; Alvarez, C.P.; Roberts, D.B.; Lai, S.Y.; Lewin, J.S. Gastrostomy Tube Placement in Patients with Oropharyngeal Carcinoma Treated with Radiotherapy or Chemoradiotherapy: Factors Affecting Placement and Dependence. Head Neck 2013, 35, 1634–1640. [Google Scholar] [CrossRef]
- Bhide, S.A.; Gulliford, S.; Kazi, R.; El-Hariry, I.; Newbold, K.; Harrington, K.J.; Nutting, C.M. Correlation between Dose to the Pharyngeal Constrictors and Patient Quality of Life and Late Dysphagia Following Chemo-Imrt for Head and Neck Cancer. Radiother. Oncol. 2009, 93, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Caglar, H.B.; Tishler, R.B.; Othus, M.; Burke, E.; Li, Y.; Goguen, L.; Wirth, L.J.; Haddad, R.I.; Norris, C.M.; Court, L.E.; et al. Dose to Larynx Predicts for Swallowing Complications after Intensity-Modulated Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Caudell, J.J.; Schaner, P.E.; Meredith, R.F.; Locher, J.L.; Nabell, L.M.; Carroll, W.R.; Magnuson, J.S.; Spencer, S.A.; Bonner, J.A. Factors Associated with Long-Term Dysphagia after Definitive Radiotherapy for Locally Advanced Head-and-Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 73, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Caudell, J.J.; Schaner, P.E.; Desmond, R.A.; Meredith, R.F.; Spencer, S.A.; Bonner, J.A. Dosimetric Factors Associated with Long-Term Dysphagia after Definitive Radiotherapy for Squamous Cell Carcinoma of the Head and Neck. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Charters, E.; Bogaardt, H.; Clark, J.; Milross, C.; Freeman-Sanderson, A.; Ballard, K.; Britton, R.; McCabe, N.; Davis, H.; Sullivan, T.; et al. Functional Swallowing Outcomes Related to Radiation Exposure to Dysphagia and Aspiration-Related Structures in Patients with Head and Neck Cancer Undergoing Definitive and Postoperative Intensity-Modulated Radiotherapy. Head Neck 2022, 44, 399–411. [Google Scholar] [CrossRef] [PubMed]
- Chera, B.S.; Fried, D.; Price, A.; Amdur, R.J.; Mendenhall, W.; Lu, C.; Das, S.; Sheets, N.; Marks, L.; Mavroidis, P. Dosimetric Predictors of Patient-Reported Xerostomia and Dysphagia with Deintensified Chemoradiation Therapy for Hpv-Associated Oropharyngeal Squamous Cell Carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Deantonio, L.; Masini, L.; Brambilla, M.; Pia, F.; Krengli, M. Dysphagia after Definitive Radiotherapy for Head and Neck Cancer. Correlation of Dose-Volume Parameters of the Pharyngeal Constrictor Muscles. Strahlenther. Onkol. 2013, 189, 230–236. [Google Scholar] [CrossRef]
- Dirix, P.; Abbeel, S.; Vanstraelen, B.; Hermans, R.; Nuyts, S. Dysphagia after Chemoradiotherapy for Head-and-Neck Squamous Cell Carcinoma: Dose-Effect Relationships for the Swallowing Structures. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 385–392. [Google Scholar] [CrossRef]
- Eisbruch, A.; Levendag, P.C.; Feng, F.Y.; Teguh, D.; Lyden, T.; Schmitz, P.I.; Haxer, M.; Noever, I.; Chepeha, D.B.; Heijmen, B.J. Can Imrt or Brachytherapy Reduce Dysphagia Associated with Chemoradiotherapy of Head and Neck Cancer? The Michigan and Rotterdam Experiences. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69 (Suppl. S2), S40–S42. [Google Scholar] [CrossRef]
- Eisbruch, A.; Kim, H.M.; Feng, F.Y.; Lyden, T.H.; Haxer, M.J.; Feng, M.; Worden, F.P.; Bradford, C.R.; Prince, M.E.; Moyer, J.S.; et al. Chemo-Imrt of Oropharyngeal Cancer Aiming to Reduce Dysphagia: Swallowing Organs Late Complication Probabilities and Dosimetric Correlates. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e93–e99. [Google Scholar] [CrossRef]
- Feng, F.Y.; Kim, H.M.; Lyden, T.H.; Haxer, M.J.; Feng, M.; Worden, F.P.; Chepeha, D.B.; Eisbruch, A. Intensity-Modulated Radiotherapy of Head and Neck Cancer Aiming to Reduce Dysphagia: Early Dose-Effect Relationships for the Swallowing Structures. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1289–1298. [Google Scholar] [CrossRef] [PubMed]
- Frowen, J.; Hornby, C.; Collins, M.; Senthi, S.; Cassumbhoy, R.; Corry, J. Reducing Posttreatment Dysphagia: Support for the Relationship between Radiation Dose to the Pharyngeal Constrictors and Swallowing Outcomes. Pract. Radiat. Oncol. 2013, 3, e187–e194. [Google Scholar] [CrossRef] [PubMed]
- Fua, T.F.; Corry, J.; Milner, A.D.; Cramb, J.; Walsham, S.F.; Peters, L.J. Intensity-Modulated Radiotherapy for Nasopharyngeal Carcinoma: Clinical Correlation of Dose to the Pharyngo-Esophageal Axis and Dysphagia. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 976–981. [Google Scholar] [CrossRef] [PubMed]
- Ghadjar, P.; Simcock, M.; Zimmermann, F.; Betz, M.; Bodis, S.; Bernier, J.; Studer, G.; Aebersold, D.M.; Swiss Group for Clinical Cancer, R. Predictors of Severe Late Radiotherapy-Related Toxicity after Hyperfractionated Radiotherapy with or without Concomitant Cisplatin in Locally Advanced Head and Neck Cancer. Secondary Retrospective Analysis of a Randomized Phase Iii Trial (Sakk 10/94). Radiother. Oncol. 2012, 104, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Goepfert, R.P.; Lewin, J.S.; Barrow, M.P.; Fuller, C.D.; Lai, S.Y.; Song, J.; Hobbs, B.P.; Gunn, G.B.; Beadle, B.M.; Rosenthal, D.I.; et al. Predicting Two-Year Longitudinal Md Anderson Dysphagia Inventory Outcomes after Intensity Modulated Radiotherapy for Locoregionally Advanced Oropharyngeal Carcinoma. Laryngoscope 2017, 127, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Guo, G.Z.; Sutherland, K.R.; Myers, C.; Lambert, P.; Loewen, S.K.; Quon, H.C. Prospective Swallowing Outcomes after Imrt for Oropharyngeal Cancer: Dosimetric Correlations in a Population-Based Cohort. Oral Oncol. 2016, 61, 135–141. [Google Scholar] [CrossRef]
- Haderlein, M.; Semrau, S.; Ott, O.; Speer, S.; Bohr, C.; Fietkau, R. Dose-Dependent Deterioration of Swallowing Function after Induction Chemotherapy and Definitive Chemoradiotherapy for Laryngopharyngeal Cancer. Strahlenther. Onkol. 2014, 190, 192–198. [Google Scholar] [CrossRef]
- Harms, A.; Kansara, S.; Stach, C.; Richardson, P.A.; Chen, G.; Lai, S.; Sikora, A.G.; Parke, R.; Donovan, D.; Chiao, E.; et al. Swallowing Function in Survivors of Oropharyngeal Cancer Is Associated with Advanced T Classification. Ann. Otol. Rhinol. Laryngol. 2019, 128, 696–703. [Google Scholar] [CrossRef]
- Jensen, K.; Lambertsen, K.; Grau, C. Late Swallowing Dysfunction and Dysphagia after Radiotherapy for Pharynx Cancer: Frequency, Intensity and Correlation with Dose and Volume Parameters. Radiother. Oncol. 2007, 85, 74–82. [Google Scholar] [CrossRef]
- Kanayama, N.; Kierkels, R.G.J.; van der Schaaf, A.; Steenbakkers, R.; Yoshioka, Y.; Nishiyama, K.; Fujii, T.; Ogawa, K.; Langendijk, J.A.; Teshima, T. External Validation of a Multifactorial Normal Tissue Complication Probability Model for Tube Feeding Dependence at 6 Months after Definitive Radiotherapy for Head and Neck Cancer. Radiother. Oncol. 2018, 129, 403–408. [Google Scholar] [CrossRef]
- Karsten, R.T.; Stuiver, M.M.; van der Molen, L.; Navran, A.; de Boer, J.P.; Hilgers, F.J.M.; Klop, W.M.C.; Smeele, L.E. From Reactive to Proactive Tube Feeding During Chemoradiotherapy for Head and Neck Cancer: A Clinical Prediction Model-Based Approach. Oral Oncol. 2019, 88, 172–179. [Google Scholar] [CrossRef]
- Kierkels, R.G.J.; Wopken, K.; Visser, R.; Korevaar, E.W.; van der Schaaf, A.; Bijl, H.P.; Langendijk, J.A. Multivariable Normal Tissue Complication Probability Model-Based Treatment Plan Optimization for Grade 2-4 Dysphagia and Tube Feeding Dependence in Head and Neck Radiotherapy. Radiother. Oncol. 2016, 121, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Hamauchi, S.; Kawai, S.; Onozawa, Y.; Yasui, H.; Yamashita, A.; Ogawa, H.; Onoe, T.; Kamijo, T.; Iida, Y.; et al. Pretreatment Predictive Factors for Feasibility of Oral Intake in Adjuvant Concurrent Chemoradiotherapy for Patients with Locally Advanced Squamous Cell Carcinoma of the Head and Neck. Int. J. Clin. Oncol. 2020, 25, 258–266. [Google Scholar] [CrossRef] [PubMed]
- Koiwai, K.; Shikama, N.; Sasaki, S.; Shinoda, A.; Kadoya, M. Risk Factors for Severe Dysphagia after Concurrent Chemoradiotherapy for Head and Neck Cancers. Jpn. J. Clin. Oncol. 2009, 39, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Langendijk, J.A.; Doornaert, P.; Rietveld, D.H.; Verdonck-de Leeuw, I.M.; Leemans, C.R.; Slotman, B.J. A Predictive Model for Swallowing Dysfunction after Curative Radiotherapy in Head and Neck Cancer. Radiother. Oncol. 2009, 90, 189–195. [Google Scholar] [CrossRef] [PubMed]
- Lango, M.N.; Egleston, B.; Ende, K.; Feigenberg, S.; D’Ambrosio, D.J.; Cohen, R.B.; Ahmad, S.; Nicolaou, N.; Ridge, J.A. Impact of Neck Dissection on Long-Term Feeding Tube Dependence in Patients with Head and Neck Cancer Treated with Primary Radiation or Chemoradiation. Head Neck 2010, 32, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.T.; Akst, L.M.; Adelstein, D.J.; Saxton, J.P.; Wood, B.G.; Strome, M.; Butler, R.S.; Esclamado, R.M. Risk Factors for Hypopharyngeal/Upper Esophageal Stricture Formation after Concurrent Chemoradiation. Head Neck 2006, 28, 808–812. [Google Scholar] [CrossRef]
- Levendag, P.C.; Teguh, D.N.; Voet, P.; van der Est, H.; Noever, I.; de Kruijf, W.J.; Kolkman-Deurloo, I.K.; Prevost, J.B.; Poll, J.; Schmitz, P.I.; et al. Dysphagia Disorders in Patients with Cancer of the Oropharynx Are Significantly Affected by the Radiation Therapy Dose to the Superior and Middle Constrictor Muscle: A Dose-Effect Relationship. Radiother. Oncol. 2007, 85, 64–73. [Google Scholar] [CrossRef]
- Li, B.; Li, D.; Lau, D.H.; Farwell, D.G.; Luu, Q.; Rocke, D.M.; Newman, K.; Courquin, J.; Purdy, J.A.; Chen, A.M. Clinical-Dosimetric Analysis of Measures of Dysphagia Including Gastrostomy-Tube Dependence among Head and Neck Cancer Patients Treated Definitively by Intensity-Modulated Radiotherapy with Concurrent Chemotherapy. Radiat. Oncol. 2009, 4, 52. [Google Scholar] [CrossRef]
- Lim, S.B.; Lee, N.; Zakeri, K.; Greer, P.; Fuangrod, T.; Coffman, F.; Cervino, L.; Lovelock, D.M. Can the Risk of Dysphagia in Head and Neck Radiation Therapy Be Predicted by an Automated Transit Fluence Monitoring Process During Treatment? A First Comparative Study of Patient Reported Quality of Life and the Fluence-Based Decision Support Metric. Technol. Cancer Res. Treat. 2021, 20, 15330338211027906. [Google Scholar] [CrossRef]
- Liu, H.C.; Williamson, C.W.; Zou, J.; Todd, J.R.; Nelson, T.J.; Hill, L.M.; Linnemeyer, K.E.; Henderson, G.; Madgula, P.; Faung, B.; et al. Quantitative Prediction of Aspiration Risk in Head and Neck Cancer Patients Treated with Radiation Therapy. Oral Oncol. 2022, 136, 106247. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A.; Rademaker, A.W.; Pauloski, B.R.; Lazarus, C.L.; Mittal, B.B.; Brockstein, B.; MacCracken, E.; Haraf, D.J.; Vokes, E.E.; Newman, L.A.; et al. Site of Disease and Treatment Protocol as Correlates of Swallowing Function in Patients with Head and Neck Cancer Treated with Chemoradiation. Head Neck 2006, 28, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Loser, A.; Grohmann, M.; Finger, A.; Greinert, F.; Krause, L.; Molwitz, I.; Krull, A.; Petersen, C. Impact of Dosimetric Factors on Long-Term Percutaneous Enteral Gastrostomy (Peg) Tube Dependence in Head and Neck Cancer Patients after (Chemo)Radiotherapy-Results from a Prospective Randomized Trial. Strahlenther. Onkol. 2022, 198, 1016–1024. [Google Scholar] [CrossRef] [PubMed]
- Machtay, M.; Moughan, J.; Trotti, A.; Garden, A.S.; Weber, R.S.; Cooper, J.S.; Forastiere, A.; Ang, K.K. Factors Associated with Severe Late Toxicity after Concurrent Chemoradiation for Locally Advanced Head and Neck Cancer: An Rtog Analysis. J. Clin. Oncol. 2008, 26, 3582–3589. [Google Scholar] [CrossRef]
- Mangar, S.; Slevin, N.; Mais, K.; Sykes, A. Evaluating Predictive Factors for Determining Enteral Nutrition in Patients Receiving Radical Radiotherapy for Head and Neck Cancer: A Retrospective Review. Radiother. Oncol. 2006, 78, 152–158. [Google Scholar] [CrossRef]
- Mattei, P.; Thamphya, B.; Chamorey, E.; Scheller, B.; Chateau, Y.; Dassonville, O.; Poissonnet, G.; Culie, D.; Koulmann, P.H.; Hechema, R.; et al. Therapeutic Strategies, Oncologic and Swallowing Outcomes and Their Predictive Factors in Patients with Locally Advanced Hypopharyngeal Cancer. Eur. Arch. Otorhinolaryngol. 2022, 279, 3629–3637. [Google Scholar] [CrossRef]
- Mazzola, R.; Ricchetti, F.; Fiorentino, A.; Fersino, S.; Giaj Levra, N.; Naccarato, S.; Sicignano, G.; Albanese, S.; Di Paola, G.; Alterio, D.; et al. Dose-Volume-Related Dysphagia after Constrictor Muscles Definition in Head and Neck Cancer Intensity-Modulated Radiation Treatment. Br. J. Radiol. 2014, 87, 20140543. [Google Scholar] [CrossRef]
- Mierzwa, M.L.; Gharzai, L.A.; Li, P.; Wilkie, J.R.; Hawkins, P.G.; Aryal, M.P.; Lee, C.; Rosen, B.; Lyden, T.; Blakely, A.; et al. Early Mri Blood Volume Changes in Constrictor Muscles Correlate with Postradiation Dysphagia. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 566–573. [Google Scholar] [CrossRef]
- Monti, S.; Palma, G.; D’Avino, V.; Gerardi, M.; Marvaso, G.; Ciardo, D.; Pacelli, R.; Jereczek-Fossa, B.A.; Alterio, D.; Cella, L. Voxel-Based Analysis Unveils Regional Dose Differences Associated with Radiation-Induced Morbidity in Head and Neck Cancer Patients. Sci. Rep. 2017, 7, 7220. [Google Scholar] [CrossRef]
- Mortensen, H.R.; Overgaard, J.; Jensen, K.; Specht, L.; Overgaard, M.; Johansen, J.; Evensen, J.F.; Andersen, E.; Andersen, L.J.; Hansen, H.S.; et al. Factors Associated with Acute and Late Dysphagia in the Dahanca 6 & 7 Randomized Trial with Accelerated Radiotherapy for Head and Neck Cancer. Acta Oncol. 2013, 52, 1535–1542. [Google Scholar] [CrossRef]
- Mortensen, H.R.; Jensen, K.; Aksglaede, K.; Behrens, M.; Grau, C. Late Dysphagia after Imrt for Head and Neck Cancer and Correlation with Dose-Volume Parameters. Radiother. Oncol. 2013, 107, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Mouw, K.W.; Haraf, D.J.; Stenson, K.M.; Cohen, E.E.; Xi, X.; Witt, M.E.; List, M.; Blair, E.A.; Vokes, E.E.; Salama, J.K. Factors Associated with Long-Term Speech and Swallowing Outcomes after Chemoradiotherapy for Locoregionally Advanced Head and Neck Cancer. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Murono, S.; Tsuji, A.; Endo, K.; Kondo, S.; Wakisaka, N.; Yoshizaki, T. Factors Associated with Gastrostomy Tube Dependence after Concurrent Chemoradiotherapy for Hypopharyngeal Cancer. Support. Care Cancer 2015, 23, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Nevens, D.; Goeleven, A.; Duprez, F.; Braeken, R.; Decabooter, E.; De Smet, M.; Lutters, L.; Dejaeger, E.; De Neve, W.; Nuyts, S. Does the Total Dysphagia Risk Score Correlate with Swallowing Function Examined by Videofluoroscopy? Br. J. Radiol. 2018, 91, 20170714. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.P.; Frank, C.; Moltz, C.C.; Vos, P.; Smith, H.J.; Nguyen, P.D.; Martinez, T.; Karlsson, U.; Dutta, S.; Lemanski, C.; et al. Analysis of Factors Influencing Aspiration Risk Following Chemoradiation for Oropharyngeal Cancer. Br. J. Radiol. 2009, 82, 675–680. [Google Scholar] [CrossRef] [PubMed]
- Orlandi, E.; Miceli, R.; Infante, G.; Mirabile, A.; Alterio, D.; Cossu Rocca, M.; Denaro, N.; Vigna-Taglianti, R.; Merlotti, A.; Schindler, A.; et al. Predictors of Patient-Reported Dysphagia Following Imrt Plus Chemotherapy in Oropharyngeal Cancer. Dysphagia 2019, 34, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Ortigara, G.B.; Schulz, R.E.; Soldera, E.B.; Bonzanini, L.I.L.; Danesi, C.C.; Antoniazzi, R.P.; Ferrazzo, K.L. Association between Trismus and Dysphagia-Related Quality of Life in Survivors of Head and Neck Cancer in Brazil. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 235–242. [Google Scholar] [CrossRef]
- Ottosson, S.; Lindblom, U.; Wahlberg, P.; Nilsson, P.; Kjellen, E.; Zackrisson, B.; Levring Jaghagen, E.; Laurell, G. Weight Loss and Body Mass Index in Relation to Aspiration in Patients Treated for Head and Neck Cancer: A Long-Term Follow-Up. Support. Care Cancer 2014, 22, 2361–2369. [Google Scholar] [CrossRef]
- Petersson, K.; Finizia, C.; Tuomi, L. Predictors of Severe Dysphagia Following Radiotherapy for Head and Neck Cancer. Laryngoscope Investig. Otolaryngol. 2021, 6, 1395–1405. [Google Scholar] [CrossRef]
- Petras, K.G.; Rademaker, A.W.; Refaat, T.; Choi, M.; Thomas, T.O.; Pauloski, B.R.; Mittal, B.B. Dose-Volume Relationship for Laryngeal Substructures and Aspiration in Patients with Locally Advanced Head-and-Neck Cancer. Radiat. Oncol. 2019, 14, 49. [Google Scholar] [CrossRef]
- Poulsen, M.G.; Riddle, B.; Keller, J.; Porceddu, S.V.; Tripcony, L. Predictors of Acute Grade 4 Swallowing Toxicity in Patients with Stages Iii and Iv Squamous Carcinoma of the Head and Neck Treated with Radiotherapy Alone. Radiother. Oncol. 2008, 87, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Prameela, C.G.; Ravind, R.; Renil Mon, P.S.; Sheejamol, V.S.; Dinesh, M. Radiation Dose to Dysphagia Aspiration-Related Structures and Its Effect on Swallowing: Comparison of Three-Dimensional Conformal Radiotherapy and Intensity-Modulated Radiation Therapy Plans. J. Cancer Res. Ther. 2016, 12, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Pu, D.; Lee, V.H.F.; Chan, K.M.K.; Yuen, M.T.Y.; Quon, H.; Tsang, R.K.Y. The Relationships between Radiation Dosage and Long-Term Swallowing Kinematics and Timing in Nasopharyngeal Carcinoma Survivors. Dysphagia 2022, 37, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Ray, X.; Sumner, W.; Sutton, L.; Sanghvi, P.; Deichaite, I.; Moiseenko, V. Evaluating Predictive Factors for Toxicities Experienced by Head & Neck Cancer Patients Undergoing Radiotherapy. J. Transl. Med. 2021, 19, 380. [Google Scholar] [CrossRef] [PubMed]
- Rwigema, J.M.; Langendijk, J.A.; Paul van der Laan, H.; Lukens, J.N.; Swisher-McClure, S.D.; Lin, A. A Model-Based Approach to Predict Short-Term Toxicity Benefits with Proton Therapy for Oropharyngeal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, S.; Refaat, T.; Bacchus, I.D.; Sathiaseelan, V.; Mittal, B.B. Age Most Significant Predictor of Requiring Enteral Feeding in Head-and-Neck Cancer Patients. Radiat. Oncol. 2015, 10, 93. [Google Scholar] [CrossRef]
- Saito, H.; Shodo, R.; Yamazaki, K.; Katsura, K.; Ueki, Y.; Nakano, T.; Oshikane, T.; Yamana, N.; Tanabe, S.; Utsunomiya, S.; et al. The Association between Oral Candidiasis and Severity of Chemoradiotherapy-Induced Dysphagia in Head and Neck Cancer Patients: A Retrospective Cohort Study. Clin. Transl. Radiat. Oncol. 2020, 20, 13–18. [Google Scholar] [CrossRef]
- Salama, J.K.; Stenson, K.M.; List, M.A.; Mell, L.K.; Maccracken, E.; Cohen, E.E.; Blair, E.; Vokes, E.E.; Haraf, D.J. Characteristics Associated with Swallowing Changes after Concurrent Chemotherapy and Radiotherapy in Patients with Head and Neck Cancer. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 1060–1065. [Google Scholar] [CrossRef]
- Sanguineti, G.; Gunn, G.B.; Parker, B.C.; Endres, E.J.; Zeng, J.; Fiorino, C. Weekly Dose-Volume Parameters of Mucosa and Constrictor Muscles Predict the Use of Percutaneous Endoscopic Gastrostomy During Exclusive Intensity-Modulated Radiotherapy for Oropharyngeal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 52–59. [Google Scholar] [CrossRef]
- Schwartz, D.L.; Hutcheson, K.; Barringer, D.; Tucker, S.L.; Kies, M.; Holsinger, F.C.; Ang, K.K.; Morrison, W.H.; Rosenthal, D.I.; Garden, A.S.; et al. Candidate Dosimetric Predictors of Long-Term Swallowing Dysfunction after Oropharyngeal Intensity-Modulated Radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1356–1365. [Google Scholar] [CrossRef]
- Setton, J.; Lee, N.Y.; Riaz, N.; Huang, S.H.; Waldron, J.; O’Sullivan, B.; Zhang, Z.; Shi, W.; Rosenthal, D.I.; Hutcheson, K.A.; et al. A Multi-Institution Pooled Analysis of Gastrostomy Tube Dependence in Patients with Oropharyngeal Cancer Treated with Definitive Intensity-Modulated Radiotherapy. Cancer 2015, 121, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Strom, T.; Trotti, A.M.; Kish, J.; Rao, N.G.; McCaffrey, J.; Padhya, T.A.; Lin, H.Y.; Fulp, W.; Caudell, J.J. Risk Factors for Percutaneous Endoscopic Gastrostomy Tube Placement During Chemoradiotherapy for Oropharyngeal Cancer. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 1242–1246. [Google Scholar] [CrossRef]
- Teguh, D.N.; Levendag, P.C.; Ghidey, W.; van Montfort, K.; Kwa, S.L. Risk Model and Nomogram for Dysphagia and Xerostomia Prediction in Head and Neck Cancer Patients Treated by Radiotherapy and/or Chemotherapy. Dysphagia 2013, 28, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.T.; Lee, R.; Saito, N.; Qureshi, M.M.; Ozonoff, A.; Romesser, P.B.; Wang, J.; Sakai, O. Correlating Computed Tomography Perfusion Changes in the Pharyngeal Constrictor Muscles During Head-and-Neck Radiotherapy to Dysphagia Outcome. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e119–e127. [Google Scholar] [CrossRef]
- Tsai, C.J.; Jackson, A.; Setton, J.; Riaz, N.; McBride, S.; Leeman, J.; Kowalski, A.; Happersett, L.; Lee, N.Y. Modeling Dose Response for Late Dysphagia in Patients with Head and Neck Cancer in the Modern Era of Definitive Chemoradiation. JCO Clin. Cancer Inform. 2017, 1, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Ursino, S.; Giuliano, A.; Martino, F.D.; Cocuzza, P.; Molinari, A.; Stefanelli, A.; Giusti, P.; Aringhieri, G.; Morganti, R.; Neri, E.; et al. Incorporating Dose-Volume Histogram Parameters of Swallowing Organs at Risk in a Videofluoroscopy-Based Predictive Model of Radiation-Induced Dysphagia after Head and Neck Cancer Intensity-Modulated Radiation Therapy. Strahlenther. Onkol. 2021, 197, 209–218. [Google Scholar] [CrossRef]
- Van der Laan, H.P.; Bijl, H.P.; Steenbakkers, R.J.; van der Schaaf, A.; Chouvalova, O.; Vemer-van den Hoek, J.G.; Gawryszuk, A.; van der Laan, B.F.; Oosting, S.F.; Roodenburg, J.L.; et al. Acute Symptoms During the Course of Head and Neck Radiotherapy or Chemoradiation Are Strong Predictors of Late Dysphagia. Radiother. Oncol. 2015, 115, 56–62. [Google Scholar] [CrossRef]
- Van der Molen, L.; Heemsbergen, W.D.; de Jong, R.; van Rossum, M.A.; Smeele, L.E.; Rasch, C.R.; Hilgers, F.J. Dysphagia and Trismus after Concomitant Chemo-Intensity-Modulated Radiation Therapy (Chemo-Imrt) in Advanced Head and Neck Cancer; Dose-Effect Relationships for Swallowing and Mastication Structures. Radiother. Oncol. 2013, 106, 364–369. [Google Scholar] [CrossRef]
- Vangelov, B.; Smee, R.I. Clinical Predictors for Reactive Tube Feeding in Patients with Advanced Oropharynx Cancer Receiving Radiotherapy +/- Chemotherapy. Eur. Arch. Otorhinolaryngol. 2017, 274, 3741–3749. [Google Scholar] [CrossRef]
- Vidyasagar, N.; Manur Gururajachar, J. Predicting Toxicity for Head and Neck Cancer Patients Undergoing Radiation Therapy: An Independent and External Validation of Mdasi-Hn Based Nomogram. Rep. Pract. Oncol. Radiother. 2020, 25, 355–359. [Google Scholar] [CrossRef]
- Wang, Y.; Xiao, F.; Zhao, Y.; Mao, C.X.; Yu, L.L.; Wang, L.Y.; Xiao, Q.; Liu, R.; Li, X.; McLeod, H.L.; et al. A Two-Stage Genome-Wide Association Study to Identify Novel Genetic Loci Associated with Acute Radiotherapy Toxicity in Nasopharyngeal Carcinoma. Mol. Cancer 2022, 21, 169. [Google Scholar] [CrossRef] [PubMed]
- Wentzel, A.; Luciani, T.; van Dijk, L.V.; Taku, N.; Elgohari, B.; Mohamed, A.S.R.; Canahuate, G.; Fuller, C.D.; Vock, D.M.; Elisabeta Marai, G.; et al. Precision Association of Lymphatic Disease Spread with Radiation-Associated Toxicity in Oropharyngeal Squamous Carcinomas. Radiother. Oncol. 2021, 161, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; McNutt, T.R.; Dudley, S.A.; Kumar, R.; Starmer, H.M.; Gourin, C.G.; Moore, J.A.; Evans, K.; Allen, M.; Agrawal, N.; et al. Predictive Factors for Prophylactic Percutaneous Endoscopic Gastrostomy (Peg) Tube Placement and Use in Head and Neck Patients Following Intensity-Modulated Radiation Therapy (Imrt) Treatment: Concordance, Discrepancies, and the Role of Gabapentin. Dysphagia 2016, 31, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Alexidis, P.; Kolias, P.; Mentesidou, V.; Topalidou, M.; Kamperis, E.; Giannouzakos, V.; Efthymiadis, K.; Bangeas, P.; Timotheadou, E. Investigating Predictive Factors of Dysphagia and Treatment Prolongation in Patients with Oral Cavity or Oropharyngeal Cancer Receiving Radiation Therapy Concurrently with Chemotherapy. Curr. Oncol. 2023, 30, 5168–5178. [Google Scholar] [CrossRef]
- Beddok, A.; Maynadier, X.; Krhili, S.; Ala Eddine, C.; Champion, L.; Chilles, A.; Goudjil, F.; Zefkili, S.; Amessis, M.; Choussy, O.; et al. Predictors of Toxicity after Curative Reirradiation with Intensity Modulated Radiotherapy or Proton Therapy for Recurrent Head and Neck Carcinoma: New Dose Constraints for Pharyngeal Constrictors Muscles and Oral Cavity. Strahlenther. Onkol. 2023. [Google Scholar] [CrossRef]
- Vasquez Osorio, E.; Abravan, A.; Green, A.; van Herk, M.; Lee, L.W.; Ganderton, D.; McPartlin, A. Dysphagia at 1 Year Is Associated with Mean Dose to the Inferior Section of the Brain Stem. Int. J. Radiat. Oncol. Biol. Phys. 2023. [CrossRef]
- Alexandra, G.; Alexandru, M.; Stefan, C.F.; Petruta-Maria, D.; Gabriel, B.M.; Dragos-Eugen, G.; Teodor, G.M. Blood Group Type Association with Head and Neck Cancer. Hematol. Rep. 2022, 14, 24–30. [Google Scholar] [CrossRef]

| Summary Statistic | OM | Dysphagia |
|---|---|---|
| Full-text articles (N) | 77 | 101 |
| Patient cohort size (median) | 91 | 100 |
| Patient cohort with radiotherapy history (%) | 100 | 100 |
| Patient cohort with chemotherapy history (%) | 80 | 88 |
| Patient cohort with surgical history (%) | 54 | 24 |
| Clinician-rated outcome (%) | 85 | 84 |
| Patient-reported outcome * (%) | 4 | 21 |
| Investigated acute toxicity (%) | 80 | 40 |
| Investigated late toxicity (%) | 1 | 62 |
| Studies with univariate analysis only (%) | 59 | 37 |
| Toxicity | Timeframe | OM Outcome | Incidence | Reported by N Studies |
|---|---|---|---|---|
| OM | Acute | RTOG/CTCAE/WHO grade 3+ | 42% | 47 |
| RTOG/CTCAE/WHO grade 2+ | 56% | 8 | ||
| Dysphagia | Acute | Tube feeding(use/indication/dependence) | 37% | 13 |
| RTOG/CTCAE grade 3+ | 37% | 11 | ||
| RTOG/CTCAE grade 2+ | 49% | 2 | ||
| Late | Tube feeding(use/indication/dependence) | 17% | 14 | |
| RTOG/CTCAE grade 3+ | 23% | 7 | ||
| RTOG/CTCAE grade 2+ | 28% | 4 |
| Factor Type | Factor | Multivariate or Model | All Analyses |
|---|---|---|---|
| Clinical laboratory tests | Blood, saliva, or stool properties | 13 | 25 |
| Dose | RT dose to oral cavity (entire volume) | 9 | 10 |
| RT dose to oral mucosa (surface only) | 6 | 7 | |
| RT dose to parotid glands | 3 | 3 | |
| RT dose to pharyngeal space | 1 | 1 | |
| RT dose to constrictor muscle | 0 | 1 | |
| RT dose to tongue | 0 | 1 | |
| Treatment | Concurrent chemotherapy | 8 | 13 |
| Chemotherapy drug | 2 | 2 | |
| RT fractionation | 2 | 3 | |
| Neoadjuvant chemotherapy | 2 | 2 | |
| Retropharyngeal lymph node irradiation | 1 | 1 | |
| RT delivery time | 1 | 3 | |
| RT field size | 1 | 1 | |
| RT modality | 1 | 1 | |
| Surgery-related factors | 1 | 2 | |
| Number of chemotherapy cycles | 0 | 1 | |
| Use of tongue immobilizer | 0 | 1 | |
| Patient | Smoking | 7 | 10 |
| Sex | 4 | 6 | |
| Body mass index | 3 | 6 | |
| Age | 3 | 9 | |
| Baseline weight loss | 2 | 3 | |
| Performance status score | 1 | 3 | |
| Number of teeth | 1 | 1 | |
| Alcohol-related | 0 | 2 | |
| Tumor | Tumor site | 5 | 7 |
| T-stage | 3 | 5 | |
| N-stage | 3 | 3 | |
| Primary tumor volume | 0 | 1 | |
| Genetic | Genetic factors | 4 | 14 |
| Other | Radiomics/dosiomics features | 1 | 1 |
| Bioelectrical impedance measurement | 0 | 2 | |
| Perfusion/blood flow measurement | 0 | 1 |
| Factor Type | Factor | Multivariate or Model | All Analyses |
|---|---|---|---|
| Tumor | T-stage | 9 | 11 |
| Tumor site | 8 | 14 | |
| N-stage | 6 | 8 | |
| Treatment | Concurrent chemotherapy | 9 | 11 |
| RT fractionation | 4 | 7 | |
| Chemotherapy drug type | 3 | 4 | |
| Neck irradiation regimen | 3 | 6 | |
| RT field size | 2 | 3 | |
| Surgery-related factors | 2 | 2 | |
| Adjuvant chemotherapy | 1 | 1 | |
| Brachytherapy | 1 | 1 | |
| Neoadjuvant chemotherapy | 1 | 1 | |
| RT modality | 1 | 2 | |
| Dose | RT dose to constrictor muscles | 7 | 12 |
| RT dose to inferior pharyngeal constrictor (IPC) | 5 | 6 | |
| RT dose to superior pharyngeal constrictor (SPC) | 5 | 8 | |
| RT dose to middle pharyngeal constrictor (MPC) | 3 | 5 | |
| RT dose to oral cavity volume/oral mucosa surface | 3 | 4 | |
| RT dose to parotids | 3 | 3 | |
| RT dose to larynx | 2 | 5 | |
| RT dose to esophageal inlet/cricopharnygeus | 2 | 3 | |
| RT dose to esophagus | 1 | 2 | |
| RT dose to pharyngeal mucosa | 1 | 1 | |
| RT dose to pharynx | 1 | 1 | |
| RT dose to submandibular glands | 1 | 1 | |
| RT dose to primary tumor | 1 | 1 | |
| Patient | Age | 6 | 8 |
| Body mass index | 4 | 4 | |
| Performance status score | 4 | 5 | |
| Baseline weight loss | 3 | 5 | |
| Sex | 3 | 5 | |
| Smoking history | 3 | 5 | |
| Pretreatment dysphagia | 2 | 4 | |
| Constrictor muscle geometry | 1 | 1 | |
| Clinical laboratory tests | Blood or saliva properties | 2 | 2 |
| Genetic | Genetic factors | 3 | 3 |
| Factor Type | Factor | Multivariate or Model | All Analyses |
|---|---|---|---|
| Dose | RT dose to constrictor muscles | 16 | 26 |
| RT dose to superior pharyngeal constrictor (SPC) | 16 | 18 | |
| RT dose to larynx | 10 | 16 | |
| RT dose to middle pharyngeal constrictor (MPC) | 10 | 12 | |
| RT dose to inferior pharyngeal constrictor (IPC) | 9 | 12 | |
| RT dose to esophageal inlet/cricopharnygeus | 5 | 8 | |
| RT dose to oral cavity volume/oral mucosa surface | 4 | 5 | |
| RT dose to parotids | 3 | 7 | |
| RT dose to tongue or base of tongue | 3 | 6 | |
| RT dose to esophagus | 2 | 4 | |
| RT dose to inferior brain stem | 1 | 1 | |
| RT dose to submandibular glands | 0 | 2 | |
| Tumor | T-stage | 12 | 20 |
| Tumor site | 10 | 17 | |
| N-stage | 7 | 11 | |
| Patient | Age | 12 | 13 |
| Smoking history | 6 | 6 | |
| Baseline/acute weight loss | 5 | 8 | |
| Pretreatment or acute dysphagia | 3 | 7 | |
| Body mass index | 1 | 2 | |
| Performance status score | 1 | 4 | |
| Sex | 1 | 3 | |
| Constrictor muscle geometry | 1 | 1 | |
| Alcohol use | 0 | 1 | |
| Treatment | Concurrent chemotherapy | 9 | 9 |
| Surgery-related factors | 4 | 6 | |
| RT fractionation | 3 | 11 | |
| Neck irradiation regimen | 2 | 8 | |
| Chemotherapy drug type | 1 | 3 | |
| Neoadjuvant chemotherapy | 1 | 3 | |
| Adjuvant chemotherapy | 1 | 2 | |
| RT modality | 1 | 2 | |
| Brachytherapy | 1 | 1 | |
| RT field size | 0 | 2 | |
| Clinical laboratory tests | Blood or saliva properties | 1 | 1 |
| Ref. | Time Frame | Endpoint | Model Features * | Sample Size | Validation Type | Test AUC |
|---|---|---|---|---|---|---|
| [16] | Acute | Increase from RTOG G1-G2 | Oral bacteria genetic information | 41 | Internal | 0.646 |
| [17] | Acute | CTCAE G3+ OM | BMI, Combined parotid glands EUD, Oral cavity EUD | 132 | Internal | 0.67 |
| [18] | Acute | CTCAE G3+ OM | Oral cavity Dmean, Mean RT dose at which 50% of patients experience toxicity (51 Gy), Slope of dose response curve | 169 | External | 0.67 |
| [19] | Acute | CTCAE G3+ OM | Definitive RT, Male, Age, Chemotherapy modality, Chemotherapy drug, Tumor site, Volumes of oral cavity receiving 20-260cGy per fraction in 20cGy/fraction increments | 351 | Internal | 0.71 |
| [20] | Acute | WHO G3+ OM | Age, N-stage, # of cycles of neoadjuvant chemotherapy, V40 (oral cavity) | 190 | Internal | 0.759 |
| [21] | Acute | RTOG G3+ OM | BMI, RLN irradiation, Mucosa surface contour V55 | 270 | Internal | 0.782 |
| [22] | Acute | DAHANCA G3+ OM | Extended oral cavity DVH parameters converted into 2 Principal Components, Treatment acceleration | 802 | Internal | 0.808 |
| [23] | Acute | CTCAE G3+ OM | 4 cT1-w MR and 1 CECT radiomics texture features extracted from gross tumor volume (primary and nodal tumor) | 242 | Internal | 0.81 |
| Ref. | Time Frame | Endpoint | Model Features * | Sample Size | Validation Type | Test AUC |
|---|---|---|---|---|---|---|
| [93] | Acute | CTCAE G3+ dysphagia | CCT, D2 SPCM, Rs321345_TC(XRCC1) polymorphism | 189 | Internal | 0.6 |
| [94] | Acute | Tube feeding use ≥ 4 weeks | Pre-treatment weight change %, Texture modified diet., ECOG > 0, Tumor site, N-stage ≥ 2, Dmean contralateral parotid, Dmean oral cavity | 334 | External | 0.624 |
| [95] | Acute | Tube feeding use ≥ 4 weeks | Tumor site, T-stage ≥ 3, Chemotherapy (vs. RT alone), Dmean contralateral parotid | 225 | Internal | 0.708 |
| [96] | Acute | Tube feeding use ≥ 4 weeks | BMI, Texture-modified diet, WHO performance scale > 0, Tumor site, T-stage ≥ 2, N-stage ≥ 2, CCT (vs. RT alone), Dmean contralateral submandibular gland, Dmean contralateral parotid | 450 | Internal | 0.723 |
| [97] | Acute | CTCAE G3+ dysphagia | Definitive RT, Male, Age, IC, No CCT, Chemotherapy drug, Tumor site, Volumes of Pharyngeal mucosa receiving 20-260cGy per fraction in 20cGy/fraction increments | 90 | External | 0.82 |
| [98] | Late | Dysphagia improvement (reduction of at least one grade from CTCAE grade ≥ 3) | Dmin larynx | 90 | Internal | 0.697 |
| [99] | Late | Aspiration (>25 months) | Age, Neck dissection, Dmean MPCM | 107 | Internal | 0.73 |
| [100] | Late | RTOG G2+ dysphagia (6 months) | Dmean SPCM, Dmean supraglottic larynx | 186 | External | 0.75 |
| [101] | Late | CTCAE G2+ dysphagia (6 months) | Dmean oral cavity, Dmean SPCM, Dmean MPCM, Dmean IPCM, Tumor site, Baseline dysphagia score | 277 | External | 0.8 |
| [102] | Late | RTOG G2+ dysphagia (6 months) | Dmean SPCM, Dmean supraglottic larynx | 354 | Internal | 0.8 |
| [103] | Late | Tube feeding dependence (6 months) | T-stage ≥ 3, N-stage > 0, Baseline weight loss, Accelerated RT, CRT, Neck irradiation | 183 | External | 0.82 |
| [104] | Late | Aspiration or stricture or tube feeding or aspiration pneumonia (>12 months) | Age, V69 Mylo/geniohyoid complex | 300 | Internal | 0.835 |
| [105] | Late | Feeding tube insertion or aspiration (6 months) | Tumor–organ distances for superior, inferior, and medial pharyngeal constrictors, plus mylogeniohyoid, cricopharyngeal muscle, and supraglottic larynx, Clinical feature clusters comprising smoking status, T-stage, N-stage, HPV status, Pathological grade, tumor site, CRT combination, tumor laterality, age, total dose to tumor | 200 | Internal | 0.84 |
| [106] | Late | Tube feeding dependence (6 months) | T-stage ≥ 3, Baseline weight loss > 10%, RT + cetuximab, Accelerated RT, CCT, Dmean SPCM, Dmean ICPM, Dmean contralateral parotid, Dmean cricopharyngeal muscle | 355 | Internal | 0.85 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicol, A.J.; Ching, J.C.F.; Tam, V.C.W.; Liu, K.C.K.; Leung, V.W.S.; Cai, J.; Lee, S.W.Y. Predictive Factors for Chemoradiation-Induced Oral Mucositis and Dysphagia in Head and Neck Cancer: A Scoping Review. Cancers 2023, 15, 5705. https://doi.org/10.3390/cancers15235705
Nicol AJ, Ching JCF, Tam VCW, Liu KCK, Leung VWS, Cai J, Lee SWY. Predictive Factors for Chemoradiation-Induced Oral Mucositis and Dysphagia in Head and Neck Cancer: A Scoping Review. Cancers. 2023; 15(23):5705. https://doi.org/10.3390/cancers15235705
Chicago/Turabian StyleNicol, Alexander J., Jerry C. F. Ching, Victor C. W. Tam, Kelvin C. K. Liu, Vincent W. S. Leung, Jing Cai, and Shara W. Y. Lee. 2023. "Predictive Factors for Chemoradiation-Induced Oral Mucositis and Dysphagia in Head and Neck Cancer: A Scoping Review" Cancers 15, no. 23: 5705. https://doi.org/10.3390/cancers15235705