

Comparing Prognosis for BRCA1, BRCA2, and Non-BRCA Breast Cancer
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
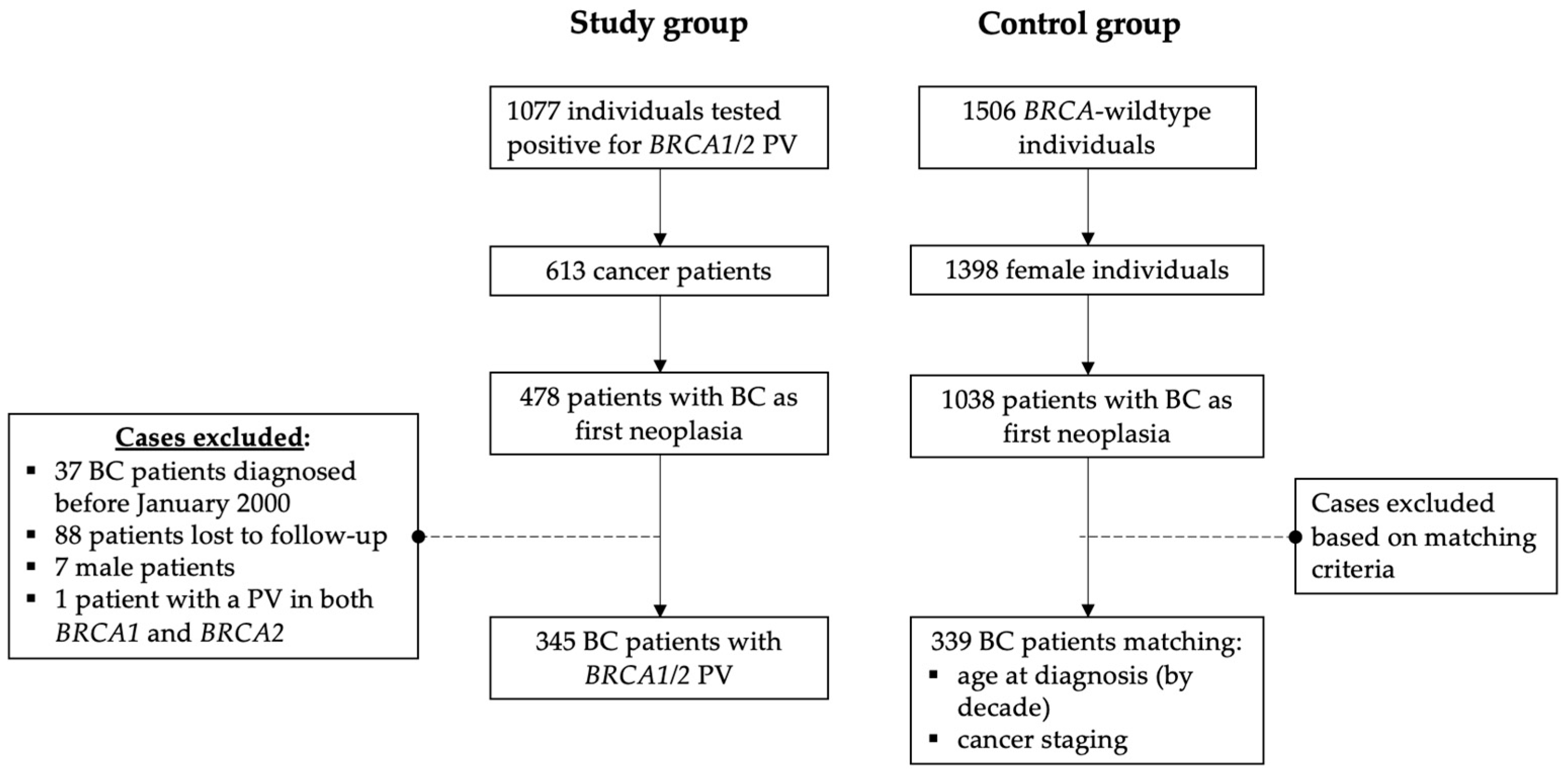
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Uptake of Risk-Reducing Surgeries
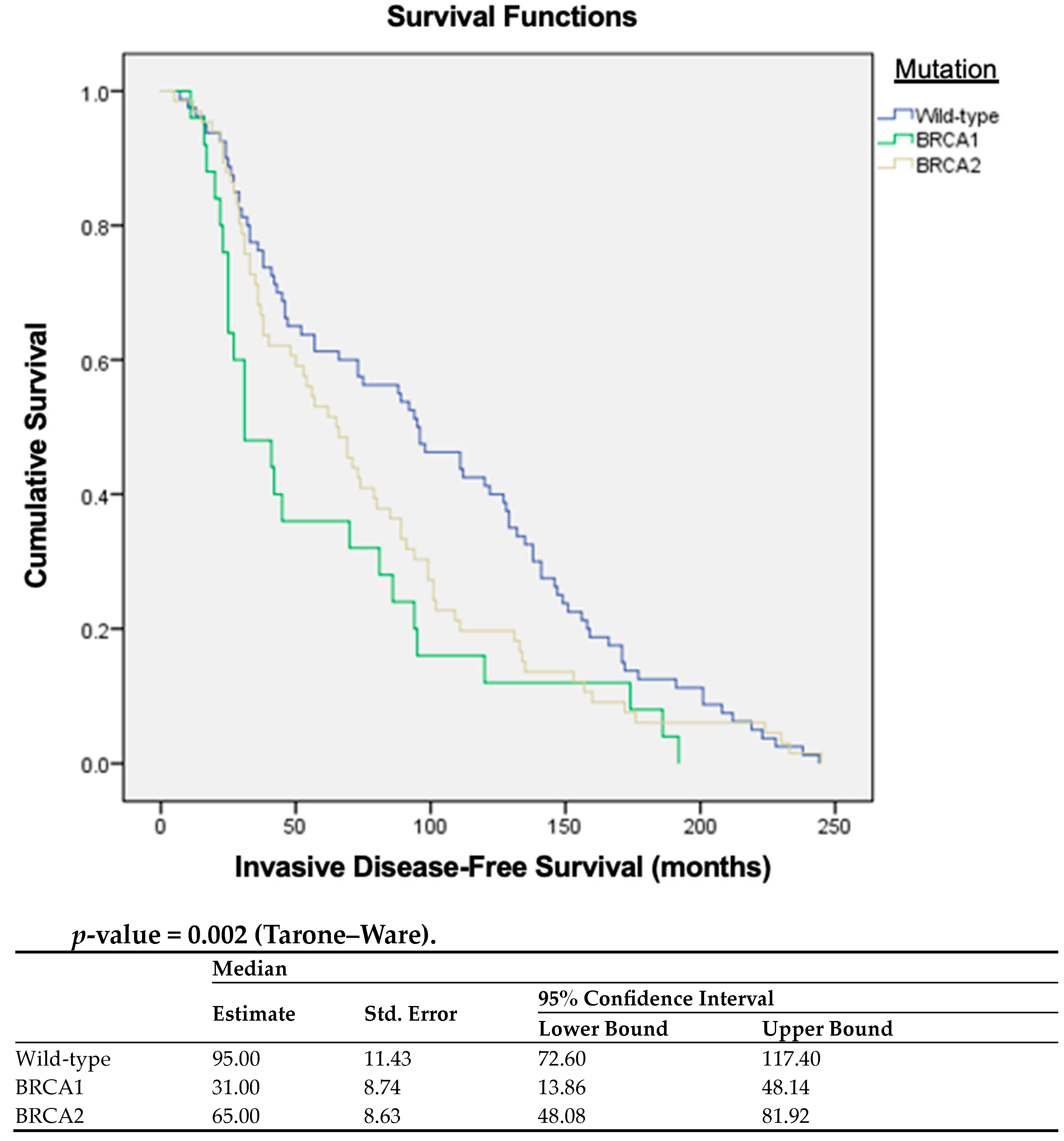
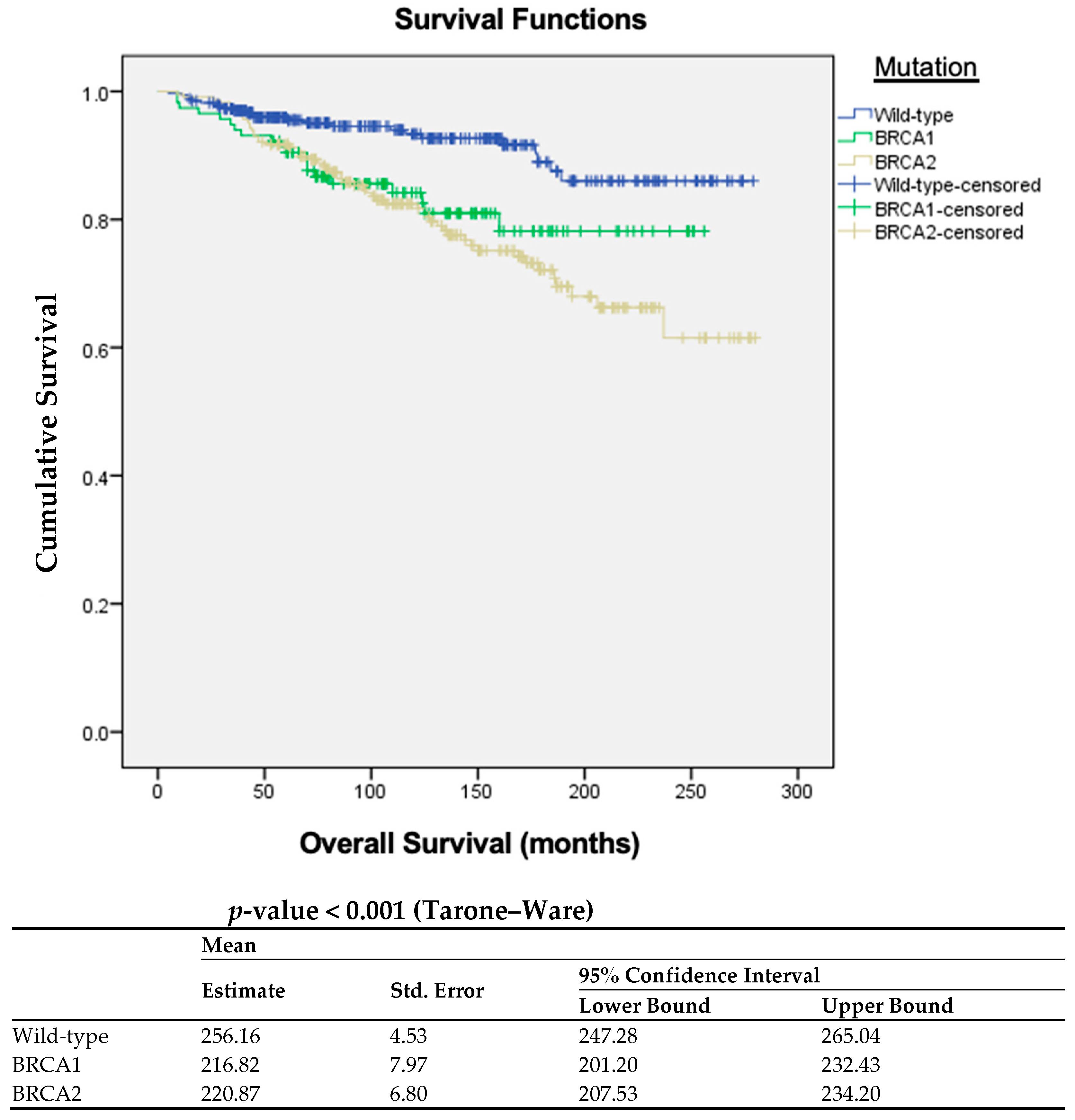
3.3. Invasive Disease-Free Survival and Overall Survival Analysis
3.4. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Wooster, R.; Weber, B.L. Breast and Ovarian Cancer. N. Engl. J. Med. 2003, 348, 2339–2347. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, A.; Pharoah, P.D.; Narod, S.; Risch, H.A.; Eyfjord, J.E.; Hopper, J.L.; Loman, N.; Olsson, H.; Johannsson, O.; Borg, A.; et al. Average Risks of Breast and Ovarian Cancer Associated with BRCA1 or BRCA2 Mutations Detected in Case Series Unselected for Family History: A Combined Analysis of 22 Studies. Am. J. Hum. Genet. 2003, 72, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Parmigiani, G. Meta-Analysis of BRCA1 and BRCA2 Penetrance. J. Clin. Oncol. 2007, 25, 1329–1333. [Google Scholar] [CrossRef] [PubMed]
- King, M.-C.; Marks, J.H.; Mandell, J.B. Breast and Ovarian Cancer Risks Due to Inherited Mutations in BRCA1 and BRCA2. Science 2003, 302, 643–646. [Google Scholar] [CrossRef] [PubMed]
- Domchek, S.M.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Association of Risk-Reducing Surgery in BRCA1 or BRCA2 Mutation Carriers with Cancer Risk and Mortality. JAMA 2010, 304, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Rebbeck, T.R.; Lynch, H.T.; Neuhausen, S.L.; Narod, S.A.; Veer, L.V.; Garber, J.E.; Evans, G.; Isaacs, C.; Daly, M.B.; Matloff, E.; et al. Prophylactic Oophorectomy in Carriers of BRCA1 or BRCA2 Mutations. N. Engl. J. Med. 2002, 346, 1616–1622. [Google Scholar] [CrossRef]
- Saslow, D.; Boetes, C.; Burke, W.; Harms, S.; Leach, M.O.; Lehman, C.D.; Morris, E.; Pisano, E.; Schnall, M.; Sener, S.; et al. American Cancer Society Guidelines for Breast Screening with MRI as an Adjunct to Mammography. CA Cancer J. Clin. 2007, 57, 75–89. [Google Scholar] [CrossRef]
- Thompson, D.; Easton, D.F. Cancer Incidence in BRCA1 Mutation Carriers. J. Natl. Cancer Inst. 2002, 94, 1358–1365. [Google Scholar] [CrossRef]
- Breast Cancer Linkage Consortium. Cancer Risks in BRCA2 Mutation Carriers. J. Natl. Cancer Inst. 1999, 91, 1310–1316. [Google Scholar] [CrossRef]
- Segev, Y.; Iqbal, J.; Lubinski, J.; Ping, S.; Rosen, B.; Narod, S. The incidence of endometrial cancer in women with BRCA1 and BRCA2 mutations. Gynecol. Oncol. 2013, 130, 127–131. [Google Scholar] [CrossRef]
- Machado, P.M.; Brandao, R.D.; Cavaco, B.M.; Eugénio, J.; Bento, S.; Nave, M.; Rodrigues, P.; Fernandes, A.; Vaz, F. Screening for a BRCA2 rearrangement in high-risk breast/ovarian cancer families: Evidence for a founder effect and analysis of the associated phenotypes. J. Clin. Oncol. 2007, 25, 2027–2034. [Google Scholar] [CrossRef]
- de Oliveira, I.C.; Fragoso, S.; Santos, S.; Duarte, T.; Bexiga, C.; Mira, B.; Isália, M.; Luís, A.; Vaz, F. Geographical patterns of pathogenic genetic variants associated with hereditary breast, ovarian and prostate cancer (HBOPC) in Portugal. In Proceedings of the San Antonio Breast Cancer Symposium 2021, San Antonio, TX, USA, 5–7 December 2021. [Google Scholar] [CrossRef]
- Zhu, Y.; Wu, J.; Zhang, C.; Sun, S.; Zhang, J.; Liu, W.; Huang, J.; Zhang, Z. BRCA mutations and survival in breast cancer: An updated systematic review and meta-analysis. Oncotarget 2016, 7, 70113–70127. [Google Scholar] [CrossRef] [PubMed]
- van den Broek, A.J.; Schmidt, M.K.; Van t Veer, L.J.; Tollenaar, R.A.; van Leeuwen, F.E. Worse Breast Cancer Prognosis of BRCA1/BRCA2 Mutation Carriers: What’s the Evidence? A Systematic Review with Meta-Analysis. PLoS ONE 2015, 10, e0120189. [Google Scholar] [CrossRef] [PubMed]
- Baretta, Z.; Mocellin, S.; Goldin, E.; Olopade, O.I.; Huo, D. Effect of BRCA germline mutations on breast cancer prognosis: A sys-tematic review and meta-analysis. Medicine 2016, 95, e4975. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.H.; Park, S.K.; Park, B.; Kim, S.W.; Lee, M.H.; Ahn, S.H.; Son, B.H.; Yoo, K.-Y.; Kang, D.; KOHBRA Research Group; et al. Effect of BRCA1/2 mutation on short-term and long-term breast cancer survival: A systematic review and meta-analysis. Breast Cancer Res. Treat. 2010, 122, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Templeton, A.J.; Gonzalez, L.D.; Vera-Badillo, F.E.; Tibau, A.; Goldstein, R.; Šeruga, B.; Srikanthan, A.; Pandiella, A.; Amir, E.; Ocana, A. Interaction between Hormonal Receptor Status, Age and Survival in Patients with BRCA1/2 Germline Mutations: A Systematic Review and Meta-Regression. PLoS ONE 2016, 11, e0154789. [Google Scholar] [CrossRef] [PubMed]
- Narod, S.A. Which Genes for Hereditary Breast Cancer? N. Engl. J. Med. 2021, 384, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Breast Cancer Association Consortium. Breast Cancer Risk Genes—Association Analysis in More than 113,000 Women. N. Engl. J. Med. 2021, 384, 428–439. [Google Scholar] [CrossRef]
- Hu, C.; Hart, S.N.; Gnanaolivu, R.; Huang, H.; Lee, K.Y.; Na, J.; Gao, C.; Lilyquist, J.; Yadav, S.; Boddicker, N.J.; et al. A Population-Based Study of Genes Previously Implicated in Breast Cancer. N. Engl. J. Med. 2021, 384, 440–451. [Google Scholar] [CrossRef]
- Kwong, A.; Shin, V.Y.; Ho, J.C.W.; Kang, E.; Nakamura, S.; Teo, S.-H.; Lee, A.S.G.; Sng, J.-H.; Ginsburg, O.M.; Kurian, A.W.; et al. Comprehensive spectrum of BRCA1 and BRCA2 deleterious mutations in breast cancer in Asian countries. J. Med. Genet. 2016, 53, 15–23. [Google Scholar] [CrossRef]
- Ossa, C.A.; Torres, D. Founder and Recurrent Mutations in BRCA1 and BRCA2 Genes in Latin American Countries: State of the Art and Literature Review. Oncologist 2016, 21, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Rebbeck, T.R.; Friebel, T.M.; Friedman, E.; Hamann, U.; Huo, D.; Kwong, A.; Olah, E.; Olopade, O.I.; Solano, A.R.; Teo, S.-H.; et al. Mutational spectrum in a worldwide study of 29,700 families with BRCA1 or BRCA2 mutations. Hum. Mutat. 2018, 39, 593–620. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Zayed, H. Breast cancer in the GCC countries: A focus on BRCA1/2 and non-BRCA1/2 genes. Gene 2017, 633, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Heramb, C.; Wangensteen, T.; Grindedal, E.M.; Ariansen, S.L.; Lothe, S.; Heimdal, K.R.; Mæhle, L. BRCA1 and BRCA2 mutation spectrum—An update on mutation distribution in a large cancer genetics clinic in Norway. Hered. Cancer Clin. Pract. 2018, 10, 3. [Google Scholar] [CrossRef] [PubMed]
- Janavičius, R. Founder BRCA1/2 mutations in the Europe: Implications for hereditary breast-ovarian cancer prevention and control. EPMA J. 2010, 1, 397–412. [Google Scholar] [CrossRef] [PubMed]
- Loi, M.; Desideri, I.; Olmetto, E.; Francolini, G.; Greto, D.; Bonomo, P.; Simontacchi, G.; Di Brina, L.; Meattini, I.; Livi, L. BRCA mutation in breast cancer patients: Prognostic impact and implications on clinical management. Breast J. 2018, 24, 1019–1023. [Google Scholar] [CrossRef]
- Mavaddat, N.; Barrowdale, D.; Andrulis, I.L.; Domchek, S.M.; Eccles, D.; Nevanlinna, H.; Ramus, S.J.; Spurdle, A.; Robson, M.; Sherman, M.; et al. Pathology of Breast and Ovarian Cancers among BRCA1 and BRCA2 Mutation Carriers: Results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol. Biomark. Prev. 2012, 21, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Krammer, J.; Pinker-Domenig, K.; Robson, M.E.; Gönen, M.; Bernard-Davila, B.; Morris, E.A.; Mangino, D.A.; Jochelson, M.S. Breast cancer detection and tumor characteristics in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. Treat. 2017, 163, 565–571. [Google Scholar] [CrossRef]
- Ford, D.; Easton, D.F.; Bishop, D.T.; Narod, S.A.; Goldgar, D.E. Risks of cancer in BRCA1-mutation carriers. Lancet 1994, 343, 692–695. [Google Scholar] [CrossRef]
- Brose, M.S.; Rebbeck, T.R.; Calzone, K.A.; Stopfer, J.E.; Nathanson, K.L.; Weber, B.L. Cancer risk estimates for BRCA1 mutation carriers identified in a risk evaluation program. J. Natl. Cancer Inst. 2002, 94, 1365–1372. [Google Scholar] [CrossRef]
- Mersch, J.; Jackson, M.A.; Park, M.; Nebgen, D.; Peterson, S.K.; Singletary, C.; Arun, B.K.; Litton, J.K. Cancers associated with BRCA1 and BRCA2 mutations other than breast and ovarian. Cancer 2015, 121, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Van Asperen, C.J.; Brohet, R.M.; Meijers-Heijboer, E.J.; Hoogerbrugge, N.; Verhoef, S.; Vasen, H.F.A.; Ausems, M.G.E.M.; Menko, F.H.; Garcia, E.B.G.; Klijn, J.G.M.; et al. Cancer risks in BRCA2 families: Estimates for sites other than breast and ovary. J. Med. Genet. 2005, 42, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; O’Hara, C.; Khan, S.; Shack, L.; Woodward, E.; Maher, E.R.; Lalloo, F.; Evans, D.G. Risk of cancer other than breast or ovarian in individuals with BRCA1 and BRCA2 mutations. Fam. Cancer 2012, 11, 235–242. [Google Scholar] [CrossRef]
- Easton, D.F.; Steele, L.; Fields, P.; Ormiston, W.; Averill, D.; Daly, P.A.; McManus, R.; Neuhausen, S.L.; Ford, D.; Wooster, R.; et al. Cancer risks in two large breast cancer families linked to BRCA2 on chromosome 13q12-13. Am. J. Hum. Genet. 1997, 61, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, K.A.; Lubinski, J.; Ghadirian, P.; Lynch, H.; Kim-Sing, C.; Friedman, E.; Foulkes, W.D.; Domchek, S.; Ainsworth, P.; Isaacs, C.; et al. Predictors of contralateral prophylactic mastectomy in women with a BRCA1 or BRCA2 mutation: The hereditary breast cancer clinical study group. J. Clin. Oncol. 2008, 26, 1093–1097. [Google Scholar] [CrossRef]
- Terkelsen, T.; Rønning, H.; Skytte, A.-B. Impact of genetic counseling on the uptake of contralateral prophylactic mastectomy among younger women with breast cancer. Acta Oncol. 2019, 59, 60–65. [Google Scholar] [CrossRef]
- Hanley, G.E.; McAlpine, J.N.; Cheifetz, R.; Schrader, K.A.; McCullum, M.; Huntsman, D. Selected Medical Interventions in Women with a Deleterious Brca Mutation: A Population-Based Study in British Columbia. Curr. Oncol. 2019, 26, e17–e23. [Google Scholar] [CrossRef]
- Anderson, W.F.; Chen, B.E.; Jatoi, I.; Rosenberg, P.S. Effects of Estrogen Receptor Expression and Histopathology on Annual Hazard Rates of Death from Breast Cancer. Breast Cancer Res. Treat. 2006, 100, 121–126. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| BRCA-wt N = 339 | BRCA1 N = 116 | BRCA2 N = 229 | p-Value | |
|---|---|---|---|---|
| Age at diagnosis—median (IQR) | 44.0 (21–88) | 40.5 (28–64) | 42.0 (25–80) | 0.020 |
| Molecular subtype—n (%) | <0.001 | |||
| Luminal A | 221 (65.2) | 30 (26.1) | 170 (75.6) | |
| Luminal B | 40 (11.8) | 6 (5.2) | 17 (7.6) | |
| HER2 enriched | 21 (6.2) | 3 (2.6) | 4 (1.8) | |
| Triple-negative | 57 (16.8) | 76 (66.1) | 34 (15.1) | |
| Clinical stage IV at diagnosis—n (%) | 6 (1.8) | 4 (3.5) | 6 (2.7) | 0.357 |
| Relapse (yes)—n (%) | 79 (23.7) | 25 (21.9) | 66 (29.3) | 0.203 |
| Vital status—n (%) | <0.001 | |||
| Alive | 315 (92.9) | 96 (82.8) | 174 (76.0) | |
| Dead | 24 (7.1) | 20 (17.2) | 55 (24.0) |
| Patients Undergoing Mastectomy | No | Yes | p-Value |
|---|---|---|---|
| Invasive disease (yes)—n (%) | 28 (33.7) | 17 (10.2) | <0.001 |
| iDFS—median (IQR) | 40.0 (83) | 70.0 (60) | 0.543 |
| OS—median (IQR) | 127.0 (111) | 119.0 (92) | 0.898 |
| Patients Undergoing Salpingo-Oophorectomy | No | Yes | p-Value |
|---|---|---|---|
| Invasive disease (yes)—n (%) | 23 (34.3) | 44 (65.7) | 0.012 |
| iDFS—median (IQR) | 33.0 (39) | 73.5 (90) | 0.001 |
| OS—median (IQR) | 105.5 (110) | 135.0 (91) | 0.015 |
| BRCA-wt | BRCA1 | BRCA2 | |
|---|---|---|---|
| N (%) | 20 (5.9) | 22 (19.0) | 48 (21.0) |
| Bladder | 0 | 1 | 0 |
| Breast | 2 | 9 | 27 |
| CNS | 0 | 0 | 1 |
| Colorectal | 3 | 1 | 0 |
| Endometrial | 5 | 1 | 0 |
| Gastric | 0 | 0 | 3 |
| Head and neck | 0 | 1 | 1 |
| Kidney | 0 | 0 | 1 |
| Lung | 1 | 0 | 2 |
| Lymphoma/leukemia | 2 | 1 | 2 |
| Ovary | 2 | 6 | 7 |
| Pancreatic | 2 | 1 | 2 |
| Sarcoma | 2 | 0 | 0 |
| Thyroid | 1 | 1 | 2 |
| Subgroup/Predictor(s) | ||||
|---|---|---|---|---|
| B | Exp (B) | 95% CI for Exp (B) | p | |
| OS | ||||
| Mastectomy | −1.624 | 0.197 | 0.082–0.475 | 0.000 |
| iDFS | ||||
| Oophorectomy | −0.899 | 0.407 | 0.215–0.773 | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antunes Meireles, P.; Fragoso, S.; Duarte, T.; Santos, S.; Bexiga, C.; Nejo, P.; Luís, A.; Mira, B.; Miguel, I.; Rodrigues, P.; et al. Comparing Prognosis for BRCA1, BRCA2, and Non-BRCA Breast Cancer. Cancers 2023, 15, 5699. https://doi.org/10.3390/cancers15235699
Antunes Meireles P, Fragoso S, Duarte T, Santos S, Bexiga C, Nejo P, Luís A, Mira B, Miguel I, Rodrigues P, et al. Comparing Prognosis for BRCA1, BRCA2, and Non-BRCA Breast Cancer. Cancers. 2023; 15(23):5699. https://doi.org/10.3390/cancers15235699
Chicago/Turabian StyleAntunes Meireles, Pedro, Sofia Fragoso, Teresa Duarte, Sidónia Santos, Catarina Bexiga, Priscila Nejo, Ana Luís, Beatriz Mira, Isália Miguel, Paula Rodrigues, and et al. 2023. "Comparing Prognosis for BRCA1, BRCA2, and Non-BRCA Breast Cancer" Cancers 15, no. 23: 5699. https://doi.org/10.3390/cancers15235699