
The Clinical Significance of Circulating Lymphocytes Morphology in Diffuse Large B-Cell Lymphoma As Determined by a Novel, Highly Sensitive Microscopy

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
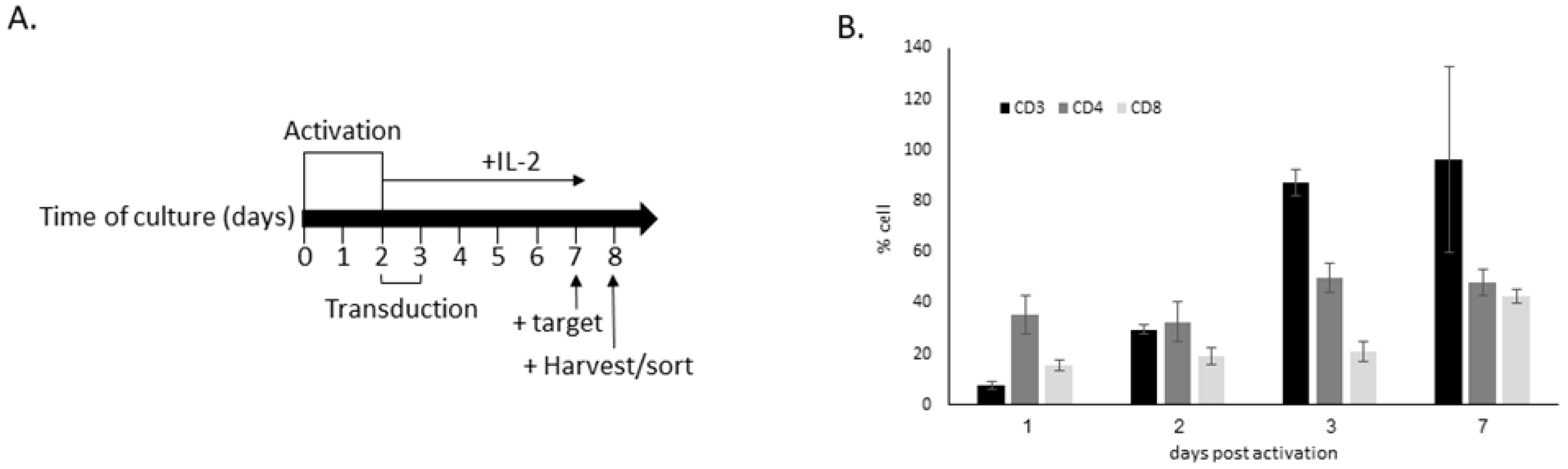
2.1. In Vitro Generation and Activation of CAR T
2.2. Flow Cytometry Analysis and Sorting
2.3. Preparation of Slides from CAR T Products
2.4. Patient Cohort and Clinical Analysis
2.5. Peripheral Blood Smears’ Preparation and Staining
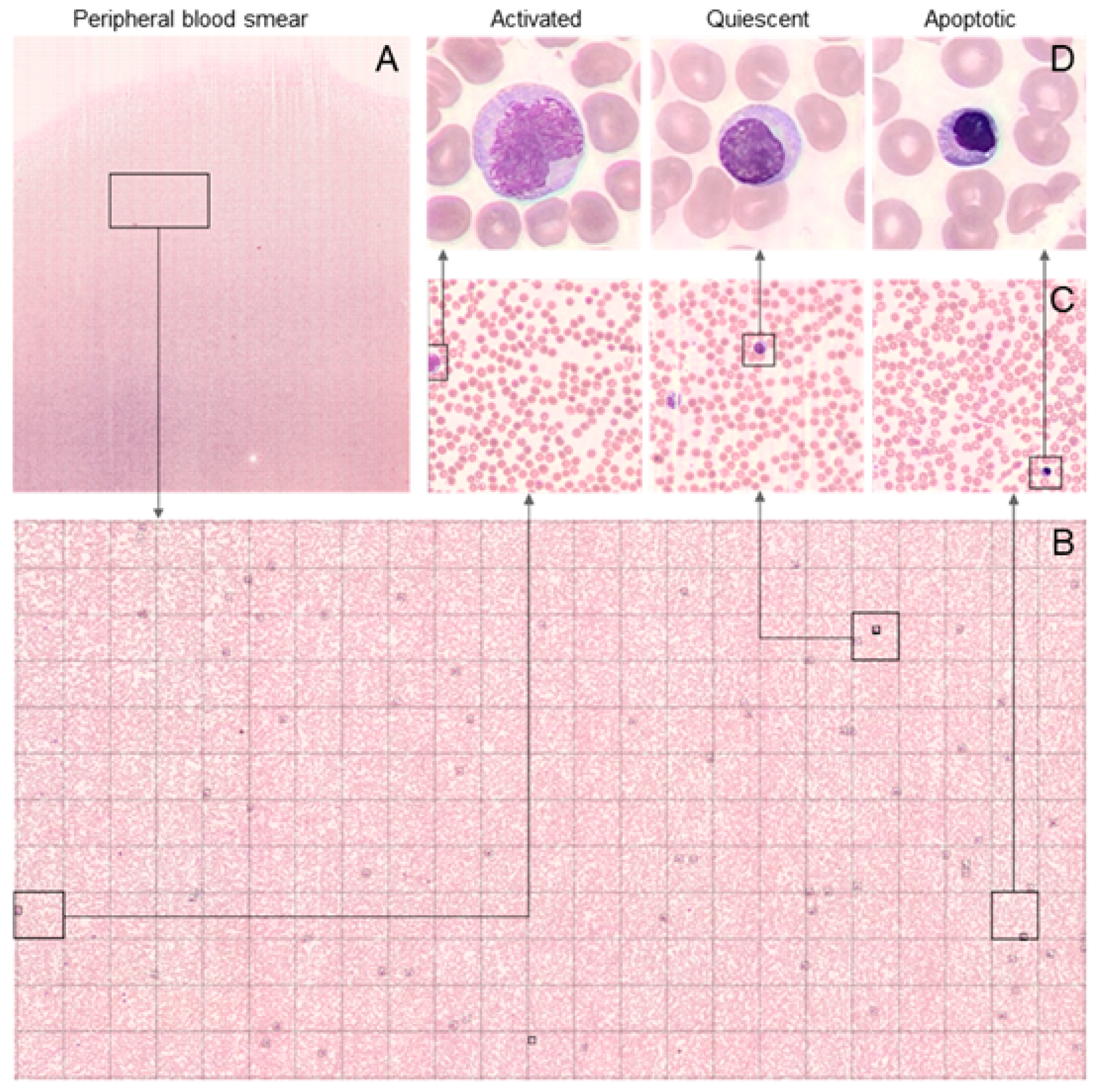
2.6. Morphological Analysis of PBS
2.7. Flow Cytometry
2.8. Laboratory Data
2.9. Statistics
3. Results
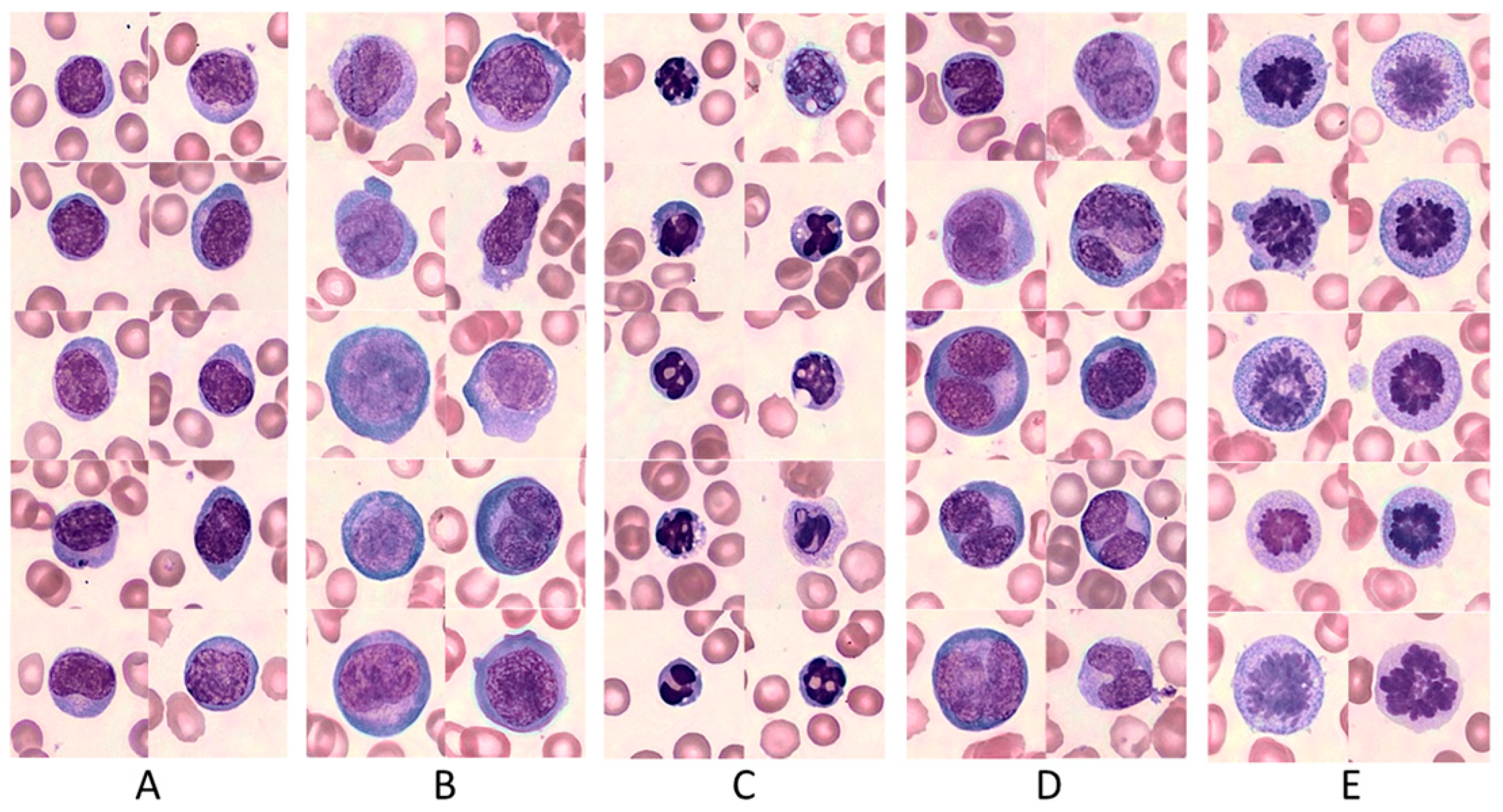
3.1. The Diverse CAR T-Cell Morphology
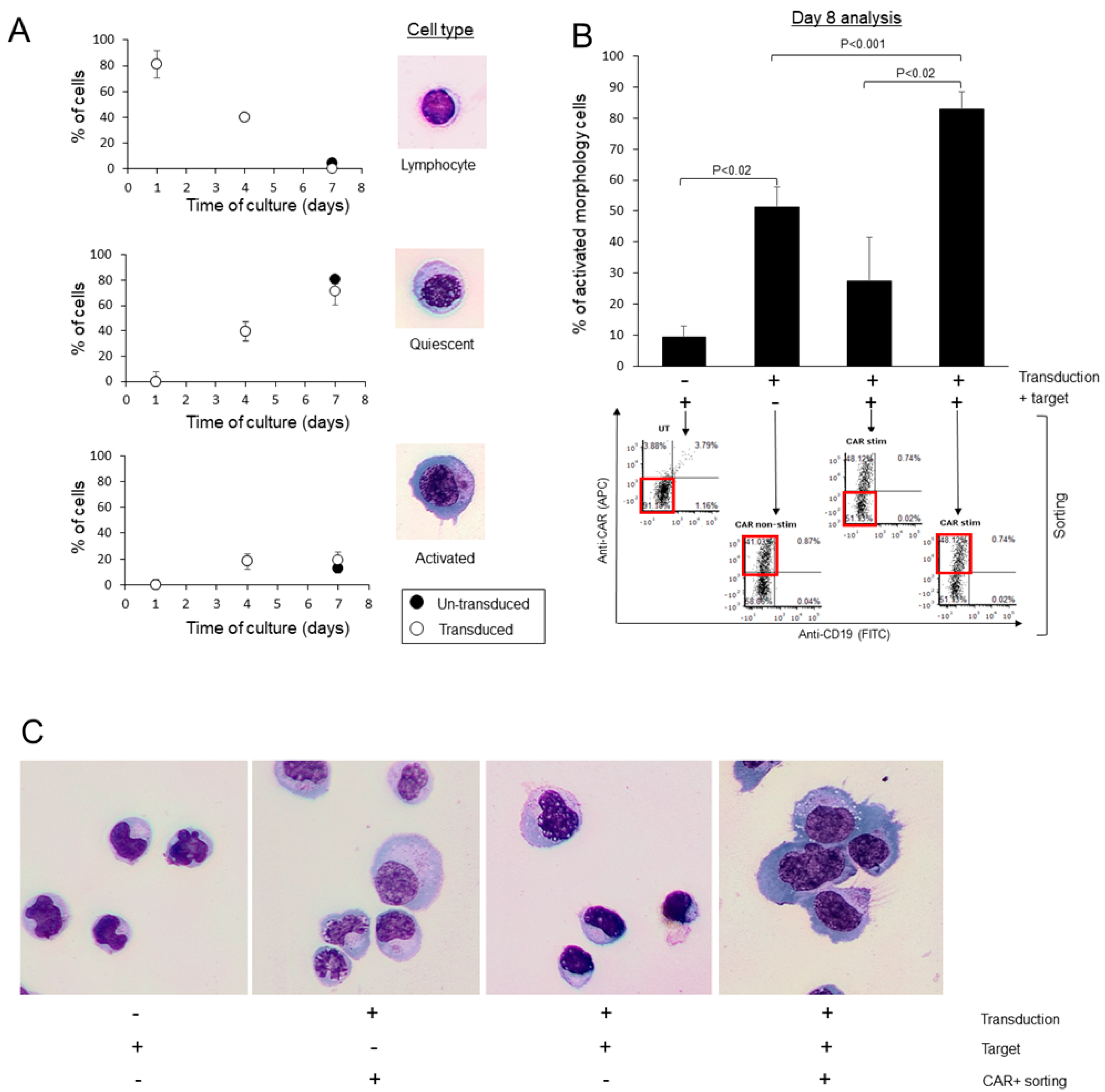
3.2. Characterization of CAR T-Cells’ Morphology during Their Production Process
3.3. Assessment of CAR T Morphological Significance
3.4. Patients’ Characteristics
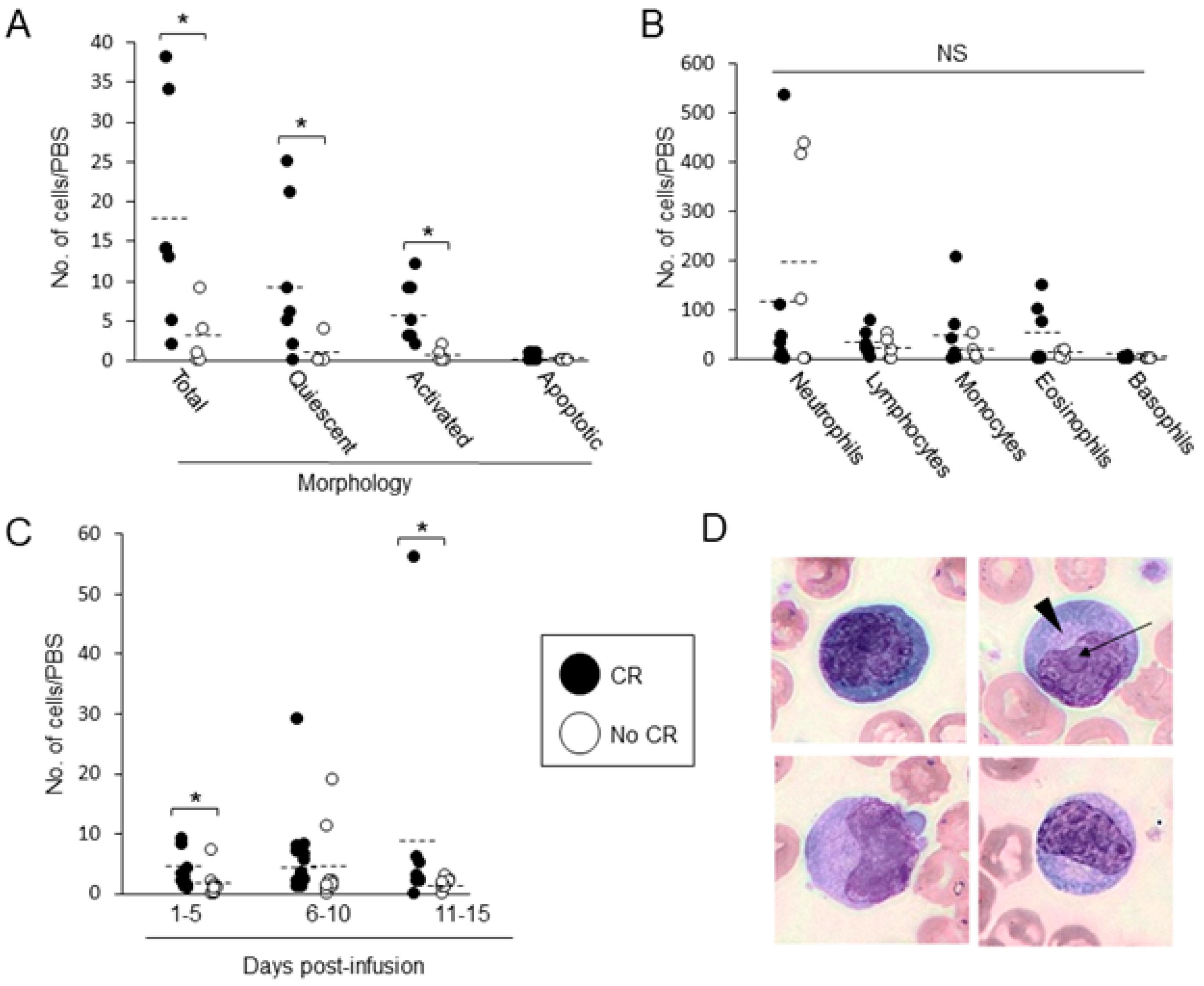
3.5. Evaluation of CAR T Morphology in PBS, Following Infusion
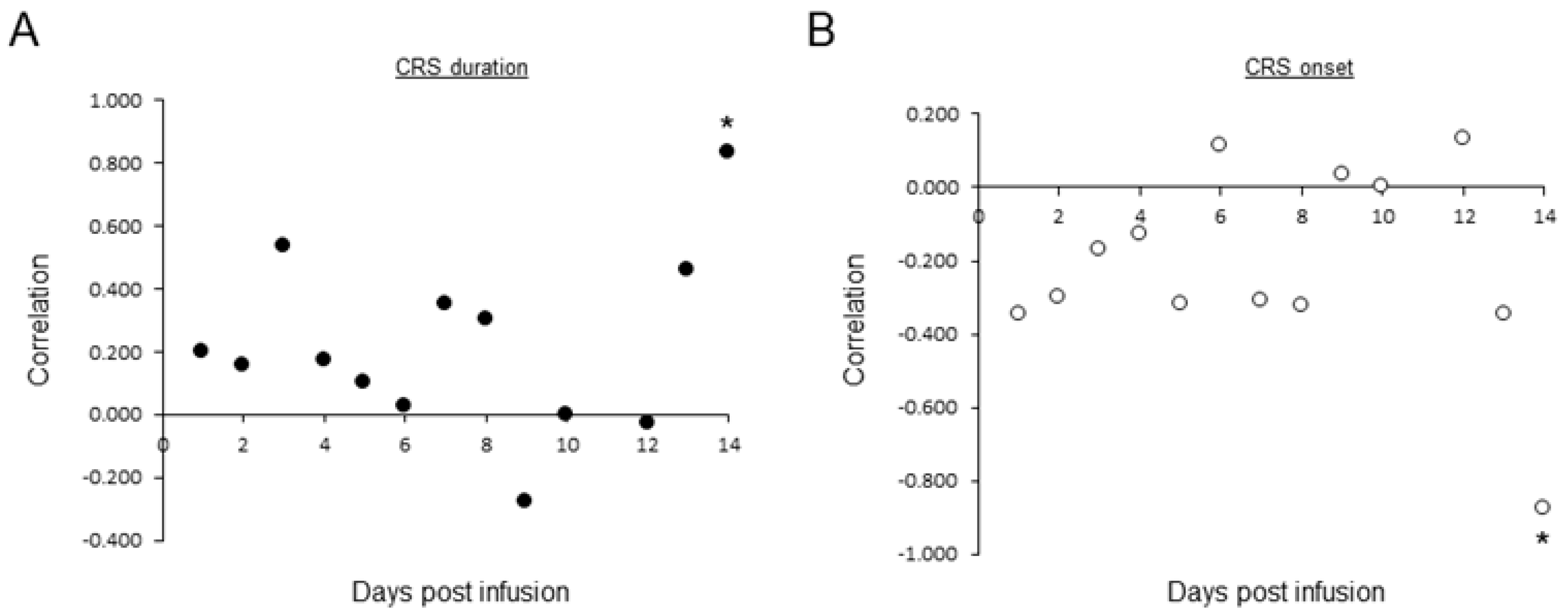
3.6. Association between CAR T in PBS and Patients’ Outcomes
3.7. Association between CAR T in PBS and Adverse Events
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sehn, L.H.; Salles, G. Diffuse Large B-Cell Lymphoma. N. Eng. J. Med. 2021, 384, 842–858. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.J.; Svoboda, J.; Chong, E.A.; Nasta, S.D.; Mato, A.R.; Anak, Ö.; Brogdon, J.L.; Pruteanu-Malinici, I.; Bhoj, V.; Landsburg, D.; et al. Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas. N. Eng. J. Med. 2017, 377, 2545–2554. [Google Scholar] [CrossRef] [PubMed]
- Westin, J.R.; Kersten, M.J.; Salles, G.; Abramson, J.S.; Schuster, S.J.; Locke, F.L.; Andreadis, C. Efficacy and safety of CD19-directed CAR-T cell therapies in patients with relapsed/refractory aggressive B-cell lymphomas: Observations from the JULIET, ZUMA-1, and TRANSCEND trials. Am. J. Hematol. 2021, 96, 1295–1312. [Google Scholar] [CrossRef] [PubMed]
- FDA. KYMRIAH (Tisagenlecleucel). Available online: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/kymriah-tisagenlecleucel (accessed on 5 June 2022).
- FDA. YESCARTA (Axicabtagene Ciloleucel). Available online: https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-products/yescarta-axicabtagene-ciloleucel (accessed on 5 June 2022).
- Locke, F.L.; Ghobadi, A.; Jacobson, C.A.; Miklos, D.B.; Lekakis, L.J.; Oluwole, O.O.; Lin, Y.; Braunschweig, I.; Hill, B.T.; Timmerman, J.M.; et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): A single-arm, multicentre, phase 1–2 trial. Lancet Oncol. 2019, 20, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Schuster, S.J.; Bishop, M.R.; Tam, C.S.; Waller, E.K.; Borchmann, P.; McGuirk, J.P.; Jäger, U.; Jaglowski, S.; Andreadis, C.; Westin, J.R.; et al. Tisagenlecleucel in Adult Relapsed or Refractory Diffuse Large B-Cell Lymphoma. N. Eng. J. Med. 2019, 380, 45–56. [Google Scholar] [CrossRef]
- Bachy, E.; le Gouill, S.; di Blasi, R.; Sesques, P.; Cartron, G.; Beauvais, D.; Roulin, L.; Gros, F.X.; Sylvain, C.; Bories, P.; et al. A Propensity Score-Matched Comparison of Axi-Cel and Tisa-Cel for Relapsed/Refractory Diffuse Large B-Cell Lymphoma in Real-Life: A Lysa Study from the Descar-T Registry. Blood 2021, 138 (Suppl. S1), 92. [Google Scholar] [CrossRef]
- Schuster, S.; Bishop, M.; Tam, C.; Borchmann, P.; Jaeger, U.; Waller, E.K.; Holte, H.; McGuirk, J.P.; Jaglowski, S.; Tobinai, K.; et al. Sustained Disease Control for Adult Patients with Relapsed or Refractory Diffuse Large B-Cell Lymphoma: An Updated Analysis of Juliet, a Global Pivotal Phase 2 Trial of Tisagenlecleucel. Blood 2018, 132 (Suppl. S1), 1684. [Google Scholar] [CrossRef]
- Weber, E.W.; Maus, M.V.; Mackall, C.L. The Emerging Landscape of Immune Cell Therapies. Cell 2020, 181, 46–62. [Google Scholar] [CrossRef]
- Rafiq, S.; Hackett, C.S.; Brentjens, R.J. Engineering strategies to overcome the current roadblocks in CAR T cell therapy. Nat. Rev. Clin. Oncol. 2019, 17, 147–167. [Google Scholar] [CrossRef]
- Vercellino, L.; di Blasi, R.; Kanoun, S.; Tessoulin, B.; Rossi, C.; D’Aveni-Piney, M.; Oberic, L.; Bodet-Milin, C.; Bories, P.; Olivier, P.; et al. Predictive factors of early progression after CAR T-cell therapy in relapsed/refractory diffuse large B-cell lymphoma. Blood Adv. 2020, 4, 5607–5615. [Google Scholar] [CrossRef]
- Locke, F.L.; Rossi, J.M.; Neelapu, S.S.; Jacobson, C.A.; Miklos, D.B.; Ghobadi, A.; Oluwole, O.O.; Reagan, P.M.; Lekakis, L.J.; Lin, Y.; et al. Tumor burden, inflammation, and product attributes determine outcomes of axicabtagene ciloleucel in large B-cell lymphoma. Blood Adv. 2020, 4, 4898–4911. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.; Riccitelli, N.; Valencia, N.; Chen, I.L.; Tangri, S.; Brogdon, J.L.; Kalfoglou, C.; Mueller, K.T.; Pollner, R. Monitoring of tisagenlecleucel transgene DNA using a quantitative polymerase chain reaction assay. Mol. Ther. 2021, 20, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Awasthi, R.; Pacaud, L.; Waldron, E.; Tam, C.S.; Jäger, U.; Borchmann, P.; Jaglowski, S.; Foley, S.R.; van Besien, K.; Wagner-Johnston, N.D.; et al. Tisagenlecleucel cellular kinetics, dose, and immunogenicity in relation to clinical factors in relapsed/refractory DLBCL. Blood Adv. 2020, 4, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Shimono, J.; Takahashi, S.; Takemura, R.; Kakinoki, Y. Useful prognostic tools based on complete blood cell counts in diffuse large B-cell lymphoma. Int. J. Lab. Hematol. 2019, 41, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Faude, S.; Wei, J.; Muralidharan, K.; Xu, X.; Wertheim, G.; Paessler, M.; Bhoj, V.G.; Grupp, S.A.; Maude, S.L.; Rheingold, S.R.; et al. Absolute lymphocyte count proliferation kinetics after CAR T-cell infusion impact response and relapse. Blood Adv. 2021, 5, 2128–2136. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.; Frey, N.; Porter, D.; June, C.; Lacey, S.; Bagg, A. The cytological features of CAR (T) cells. Br. J. Haematol. 2016, 175, 366. [Google Scholar] [CrossRef] [PubMed]
- Katz, B.Z.; Feldman, M.D.; Tessema, M.; Benisty, D.; Toles, G.S.; Andre, A.; Shtreker, B.; Paz, F.M.; Edwards, J.; Jengehino, D.; et al. Evaluation of Scopio Labs X100 Full Field PBS: The first high-resolution full field viewing of peripheral blood specimens combined with artificial intelligence-based morphological analysis. Int. J. Lab. Hematol. 2021, 43, 1408–1416. [Google Scholar] [CrossRef]
- Globerson Levin, A.; Rawet Slobodkin, M.; Waks, T.; Horn, G.; Ninio-Many, L.; Deshet Unger, N.; Ohayon, Y.; Suliman, S.; Cohen, Y.; Tartakovsky, B.; et al. Treatment of Multiple Myeloma Using Chimeric Antigen Receptor T Cells with Dual SpecificityMM Treatment with dCAR138-38–Redirected T Cells. Cancer Immunol. Res. 2020, 8, 1485–1495. [Google Scholar] [CrossRef]
- Eshhar, Z.; Waks, T.; Bendavid, A.; Schindler, D.G. Functional expression of chimeric receptor genes in human T cells. J. Immunol. Meth. 2001, 248, 67–76. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Lee, D.W.; Santomasso, B.D.; Locke, F.L.; Ghobadi, A.; Turtle, C.J.; Brudno, J.N.; Maus, M.V.; Park, J.H.; Mead, E.; Pavletic, S.; et al. ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biol. Blood Marrow Transplant. 2019, 25, 625–638. [Google Scholar] [CrossRef]
- Park, J.H.; Geyer, M.B.; Brentjens, R.J. CD19-targeted CAR T-cell therapeutics for hematologic malignancies: Interpreting clinical outcomes to date. Blood 2016, 127, 3312–3320. [Google Scholar] [CrossRef]
- Maryamchik, E.; Gallagher, K.M.E.; Preffer, F.I.; Kadauke, S.; Maus, M.V. New directions in chimeric antigen receptor T cell [CAR-T] therapy and related flow cytometry. Cytom. Part B Clin. Cytom. 2020, 98, 299–327. [Google Scholar] [CrossRef]
- Mueller, K.T.; Maude, S.L.; Porter, D.L.; Frey, N.; Wood, P.; Han, X.; Waldron, E.; Chakraborty, A.; Awasthi, R.; Levine, B.L.; et al. Cellular kinetics of CTL019 in relapsed/refractory B-cell acute lymphoblastic leukemia and chronic lymphocytic leukemia. Blood 2017, 130, 2317–2325. [Google Scholar] [CrossRef]
- Turicek, D.P.; Giordani, V.M.; Moraly, J.; Taylor, N.; Shah, N.N. CAR T-cell detection scoping review: An essential biomarker in critical need of standardization. J. Immunother. Cancer 2023, 11, e006596. [Google Scholar] [CrossRef]
- Barnes, P.W.; McFadden, S.L.; Machin, S.J.; Simson, E. The international consensus group for hematology review: Suggested criteria for action following automated CBC and WBC differential analysis. Lab. Hematol. 2005, 11, 83–90. [Google Scholar] [CrossRef]
- Benmebarek, M.R.; Karches, C.H.; Cadilha, B.L.; Lesch, S.; Endres, S.; Kobold, S. Killing mechanisms of chimeric antigen receptor (CAR) T cells. Int. J. Mol. Sci. 2019, 20, 1283. [Google Scholar] [CrossRef]
- Poorebrahim, M.; Melief, J.; Pico de Coaña, Y.; Wickström, S.L.; Cid-Arregui, A.; Kiessling, R. Counteracting CAR T cell dysfunction. Oncogene 2020, 40, 421–435. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, D.; Wong, R.A.; Yang, X.; Wang, D.; Pecoraro, J.R.; Kuo, C.F.; Aguilar, B.; Qi, Y.; Ann, D.K.; Starr, R.; et al. IL15 Enhances CAR-T Cell Antitumor Activity by Reducing mTORC1 Activity and Preserving Their Stem Cell Memory PhenotypeSuperior Antitumor Activity of CAR-T Cells Cultured in IL15. Cancer Immunol. Res. 2019, 7, 759–772. [Google Scholar] [CrossRef] [PubMed]
- Lynn, R.C.; Weber, E.W.; Sotillo, E.; Gennert, D.; Xu, P.; Good, Z.; Anbunathan, H.; Lattin, J.; Jones, R.; Tieu, V.; et al. c-Jun overexpression in CAR T cells induces exhaustion resistance. Nature 2019, 576, 293–300. [Google Scholar] [CrossRef]
- Neelapu, S.S.; Locke, F.L.; Bartlett, N.L.; Lekakis, L.J.; Miklos, D.B.; Jacobson, C.A.; Braunschweig, I.; Oluwole, O.O.; Siddiqi, T.; Lin, Y.; et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma. N. Eng. J. Med. 2017, 377, 2531–2544. [Google Scholar] [CrossRef] [PubMed]
- Locke, F.L.; Miklos, D.B.; Jacobson, C.A.; Perales, M.-A.; Kersten, M.-J.; Oluwole, O.O.; Ghobadi, A.; Rapoport, A.P.; McGuirk, J.; Pagel, J.M.; et al. Axicabtagene Ciloleucel as Second-Line Therapy for Large B-Cell Lymphoma. N. Eng. J. Med. 2022, 386, 640–654. [Google Scholar] [CrossRef] [PubMed]
- Bishop, M.R.; Dickinson, M.; Purtill, D.; Barba, P.; Santoro, A.; Hamad, N.; Kato, K.; Sureda, A.; Greil, R.; Thieblemont, C.; et al. Second-Line Tisagenlecleucel or Standard Care in Aggressive B-Cell Lymphoma. N. Eng. J. Med. 2022, 386, 629–639. [Google Scholar] [CrossRef] [PubMed]
- EBMT 2022—Program. Available online: https://ebmt2022.abstractserver.com/program/#/details/presentations/1153 (accessed on 28 April 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics at CAR T Transfusion | |||
|---|---|---|---|
| Variable | All Patients | Patients’ Characteristics by Product | |
| Tisagenlecleucel | Axicabtagene Ciloleucel | ||
| No. of patients | 26 | 21 | 5 |
| Disease type—no. (%) | |||
| DLBCL | 23 (88.5) | 19 (90) | 4 (80) |
| PMBCL | 3 (11.5) | 2 (7.7) | 1 (20) |
| Age–Median (range) yr. | 71 (20–84) | 71 (20–84) | 72 (27–74) |
| Gender (Male)—no. (%) | 12 (46.1) | 11 (52.3) | 1 (20) |
| IPI Score—no. (%) | |||
| 0–2 | 5 (19.2) | 5 (23.8) | 0 (0) |
| 3–4 | 21 (80.7) | 16 (76.1) | 5 (100) |
| Prior therapies—no. (%) | |||
| 1–2 | 17 (65.3) | 15 (71.4) | 2 (40) |
| ≥3 | 9 (34.6) | 6 (28.5) | 3 (60) |
| ECOG status score of 1—no. (%) | 11 (42.3) | 10 (47.6) | 1 (20) |
| LDH (U/L) before infusion, Median (range) | 402.5 (215–3636) | 401 (215–3636) | 421 (372–553) |
| Response and adverse events following CAR T treatment | |||
| Response at one month—no. (%) | |||
| CR/PR | 13 (50)/5 (19.2) | 10 (47.6)/4 (19) | 3 (60)/1 (20) |
| SD/PD | 0 (0)/8 (30.7) | 0 (0)/7 (33.3) | 0 (0)/1 (20) |
| CRS—no. (%) | |||
| Any grade | 18 (69.2) | 15 (71.4) | 3 (60) |
| Grade 1–2 | 15 (57.6) | 12 (57.1) | 3 (100) |
| Grade ≥ 3 | 3 (11.5) | 3 (14.2) | 0 (0) |
| ICANS—no. (%) | |||
| Any grade | 7 (26.9) | 5 (23.8) | 2 (40) |
| Grade 1–2 | 5 (19.2) | 2 (15.3) | 2 (40) |
| Grade ≥ 3 | 2 (7.69) | 3 (14.2) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fridberg, G.; Horn, G.; Globerson Levin, A.; Benisty, D.; Kay, S.; Glait-Santar, C.; Perry, C.; Ram, R.; Avivi, I.; Katz, B.-Z. The Clinical Significance of Circulating Lymphocytes Morphology in Diffuse Large B-Cell Lymphoma As Determined by a Novel, Highly Sensitive Microscopy. Cancers 2023, 15, 5611. https://doi.org/10.3390/cancers15235611
Fridberg G, Horn G, Globerson Levin A, Benisty D, Kay S, Glait-Santar C, Perry C, Ram R, Avivi I, Katz B-Z. The Clinical Significance of Circulating Lymphocytes Morphology in Diffuse Large B-Cell Lymphoma As Determined by a Novel, Highly Sensitive Microscopy. Cancers. 2023; 15(23):5611. https://doi.org/10.3390/cancers15235611
Chicago/Turabian StyleFridberg, Gil, Galit Horn, Anat Globerson Levin, Dan Benisty, Sigi Kay, Chen Glait-Santar, Chava Perry, Ron Ram, Irit Avivi, and Ben-Zion Katz. 2023. "The Clinical Significance of Circulating Lymphocytes Morphology in Diffuse Large B-Cell Lymphoma As Determined by a Novel, Highly Sensitive Microscopy" Cancers 15, no. 23: 5611. https://doi.org/10.3390/cancers15235611