
Immune-Related Adverse Events, Biomarkers of Systemic Inflammation, and Survival Outcomes in Patients Receiving Pembrolizumab for Non-Small-Cell Lung Cancer

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. Procedure and Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez–Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-Small-Cell Lung Cancer with PD-L1 Tumor Proportion Score of 50% or Greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Haanen, J.; Obeid, M.; Spain, L.; Carbonnel, F.; Wang, Y.; Robert, C.; Lyon, A.; Wick, W.; Kostine, M.; Peters, S.; et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 1217–1238. [Google Scholar] [CrossRef]
- Vaddepally, R.; Doddamani, R.; Sodavarapu, S.; Madam, N.R.; Katkar, R.; Kutadi, A.P.; Mathew, N.; Garje, R.; Chandra, A.B. Review of Immune-Related Adverse Events (irAEs) in Non-Small-Cell Lung Cancer (NSCLC)-Their Incidence, Management, Multiorgan irAEs, and Rechallenge. Biomedicines 2022, 10, 790. [Google Scholar] [CrossRef]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef]
- Morimoto, K.; Yamada, T.; Takumi, C.; Ogura, Y.; Takeda, T.; Onoi, K.; Chihara, Y.; Taniguchi, R.; Yamada, T.; Hiranuma, O.; et al. Immune-Related Adverse Events Are Associated with Clinical Benefit in Patients with Non-Small-Cell Lung Cancer Treated with Immunotherapy Plus Chemotherapy: A Retrospective Study. Front. Oncol. 2021, 11, 630136. [Google Scholar] [CrossRef]
- Daniello, L.; Elshiaty, M.; Bozorgmehr, F.; Kuon, J.; Kazdal, D.; Schindler, H.; Shah, R.; Volckmar, A.-L.; Lusky, F.; Diekmann, L.; et al. Therapeutic and Prognostic Implications of Immune-Related Adverse Events in Advanced Non-Small-Cell Lung Cancer. Front. Oncol. 2021, 11, 703893. [Google Scholar] [CrossRef]
- Toi, Y.; Sugawara, S.; Kawashima, Y.; Aiba, T.; Kawana, S.; Saito, R.; Tsurumi, K.; Suzuki, K.; Shimizu, H.; Sugisaka, J.; et al. Association of Immune-Related Adverse Events with Clinical Benefit in Patients with Advanced Non-Small-Cell Lung Cancer Treated with Nivolumab. Oncologist 2018, 23, 1358–1365. [Google Scholar] [CrossRef]
- Fukuoka, T.; Yamamoto, Y.; Utsunomiya, J.; Usami, E.; Kimura, M.; Yoshimura, T.; Nakamura, M.; Toda, Y. Association between immune-related dermatologic adverse events and efficacy of pembrolizumab in non-small cell lung cancer patients. Pharmazie 2021, 76, 239–242. [Google Scholar] [PubMed]
- Haratani, K.; Hayashi, H.; Chiba, Y.; Kudo, K.; Yonesaka, K.; Kato, R.; Kaneda, H.; Hasegawa, Y.; Tanaka, K.; Takeda, M.; et al. Association of Immune-Related Adverse Events with Nivolumab Efficacy in Non-Small-Cell Lung Cancer. JAMA Oncol. 2018, 4, 374–378. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Wang, X.; Qu, J.; Zuo, W.; Tang, Y.; Zhu, H.; Chen, X. Immune-Related Adverse Events Associated with Outcomes in Patients with NSCLC Treated with Anti-PD-1 Inhibitors: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 708195. [Google Scholar] [CrossRef] [PubMed]
- Dolan, R.D.; Laird, B.J.A.; Horgan, P.G.; McMillan, D.C. The prognostic value of the systemic inflammatory response in randomised clinical trials in cancer: A systematic review. Crit. Rev. Oncol. Hematol. 2018, 132, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Laird, B.J.; Fallon, M.; Hjermstad, M.J.; Tuck, S.; Kaasa, S.; Klepstad, P.; McMillan, D.C. Quality of Life in Patients with Advanced Cancer: Differential Association with Performance Status and Systemic Inflammatory Response. J. Clin. Oncol. 2016, 34, 2769–2775. [Google Scholar] [CrossRef]
- Simmons, C.P.; Koinis, F.; Fallon, M.T.; Fearon, K.C.; Bowden, J.; Solheim, T.S.; Gronberg, B.H.; McMillan, D.C.; Gioulbasanis, I.; Laird, B.J. Prognosis in advanced lung cancer—A prospective study examining key clinicopathological factors. Lung Cancer 2015, 88, 304–309. [Google Scholar] [CrossRef]
- Stares, M.; Ding, T.; Stratton, C.; Thomson, F.; Baxter, M.; Cagney, H.; Cumming, K.; Swan, A.; Ross, F.; Barrie, C.; et al. Biomarkers of systemic inflammation predict survival with first-line immune checkpoint inhibitors in non-small-cell lung cancer. ESMO Open 2022, 7, 100445. [Google Scholar] [CrossRef]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef]
- Simmons, C.; McMillan, D.C.; Tuck, S.; Graham, C.; McKeown, A.; Bennett, M.; O’Neill, C.; Wilcock, A.; Usborne, C.; Fearon, K.C.; et al. ‘How Long Have I Got?’—A Prospective Cohort Study Comparing Validated Prognostic Factors for Use in Patients with Advanced Cancer. Oncologist 2019, 24, e960–e967. [Google Scholar] [CrossRef]
- Leitch, E.F.; Chakrabarti, M.; Crozier, J.E.M.; McKee, R.F.; Anderson, J.H.; Horgan, P.G.; McMillan, D.C. Comparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancer. Br. J. Cancer 2007, 97, 1266–1270. [Google Scholar] [CrossRef]
- Jin, J.; Yang, L.; Liu, D.; Li, W. Association of the neutrophil to lymphocyte ratio and clinical outcomes in patients with lung cancer receiving immunotherapy: A meta-analysis. BMJ Open 2020, 10, e035031. [Google Scholar] [CrossRef] [PubMed]
- Petrova, M.P.; Eneva, M.I.; Arabadjiev, J.I.; Conev, N.V.; Dimitrova, E.G.; Koynov, K.D.; Karanikolova, T.S.; Valev, S.S.; Gencheva, R.B.; Zhbantov, G.A.; et al. Neutrophil to lymphocyte ratio as a potential predictive marker for treatment with pembrolizumab as a second line treatment in patients with non-small cell lung cancer. Biosci. Trends. 2020, 14, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Sun, S.; Gao, X.-S.; Xiong, W.; Qin, S.; Qi, X.; Ma, M.; Li, X.; Zhou, D.; Wang, W.; et al. Prognostic value of platelet to lymphocyte ratio in non-small cell lung cancer: Evidence from 3,430 patients. Sci. Rep. 2016, 6, 23893. [Google Scholar] [CrossRef] [PubMed]
- Ksienski, D.; Wai, E.S.; Alex, D.; Croteau, N.S.; Freeman, A.T.; Chan, A.; Patterson, T.; Clarkson, M.; Fiorino, L.; Poonja, Z.; et al. Prognostic significance of the neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio for advanced non-small cell lung cancer patients with high PD-L1 tumor expression receiving pembrolizumab. Transl. Lung Cancer Res. 2021, 10, 355–367. [Google Scholar] [CrossRef]
- Johannet, P.; Sawyers, A.; Qian, Y.; Kozloff, S.; Gulati, N.; Donnelly, D.; Zhong, J.; Osman, I. Baseline prognostic nutritional index and changes in pretreatment body mass index associate with immunotherapy response in patients with advanced cancer. J. Immunother. Cancer 2020, 8, e001674. [Google Scholar] [CrossRef]
- Li, D.; Yuan, X.; Liu, J.; Li, C.; Li, W. Prognostic value of prognostic nutritional index in lung cancer: A meta-analysis. J. Thorac. Dis. 2018, 10, 5298–5307. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Common Terminology Criteria for Adverse Events CTCAE) Version 5.0. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf (accessed on 11 October 2023).
- Jones, M.; Fowler, R. Immortal time bias in observational studies of time-to-event outcomes. J. Crit. Care 2016, 36, 195–199. [Google Scholar] [CrossRef]
- Lin, L.; Liu, Y.; Chen, C.; Wei, A.; Li, W. Association between immune-related adverse events and immunotherapy efficacy in non-small-cell lung cancer: A meta-analysis. Front. Pharmacol. 2023, 14, 1190001. [Google Scholar] [CrossRef]
- Zhang, Q.; Tang, L.; Zhou, Y.; He, W.; Li, W. Immune Checkpoint Inhibitor-Associated Pneumonitis in Non-Small Cell Lung Cancer: Current Understanding in Characteristics, Diagnosis, and Management. Front. Immunol. 2021, 12, 663986. [Google Scholar] [CrossRef]
- Kawai, T.; Taguchi, S.; Nakagawa, T.; Kamei, J.; Nakamura, Y.; Obinata, D.; Yamaguchi, K.; Kaneko, T.; Kakutani, S.; Tokunaga, M.; et al. Impact of immune-related adverse events on the therapeutic efficacy of pembrolizumab in urothelial carcinoma: A multicenter retrospective study using time-dependent analysis. J. Immunother. Cancer 2022, 10, e003965. [Google Scholar] [CrossRef]
- Newman, N.B.; Brett, C.L.; Kluwe, C.A.; Patel, C.G.; Attia, A.; Osmundson, E.C.; Kachnic, L.A. Immortal Time Bias in National Cancer Database Studies. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Dall’Olio, F.G.; Di Nunno, V.; Massari, F. Immortal Time Bias Question in the Association between Toxicity and Outcome of Immune Checkpoint Inhibitors. J. Clin. Oncol. 2020, 38, 105–106. [Google Scholar] [CrossRef] [PubMed]
- Socinski, M.A.; Jotte, R.M.; Cappuzzo, F.; Nishio, M.; Mok, T.S.K.; Reck, M.; Finley, G.G.; Kaul, M.D.; Yu, W.; Paranthaman, N.; et al. Association of Immune-Related Adverse Events with Efficacy of Atezolizumab in Patients with Non-Small Cell Lung Cancer: Pooled Analyses of the Phase 3 IMpower130, IMpower132, and IMpower150 Randomized Clinical Trials. JAMA Oncol. 2023, 9, 527–535. [Google Scholar] [CrossRef]
- Kfoury, M.; Najean, M.; Lappara, A.; Voisin, A.L.; Champiat, S.; Michot, J.M.; Laghouati, S.; Robert, C.; Besse, B.; Soria, J.C.; et al. Analysis of the association between prospectively collected immune-related adverse events and survival in patients with solid tumor treated with immune-checkpoint blockers, taking into account immortal-time bias. Cancer Treat. Rev. 2022, 110, 102452. [Google Scholar] [CrossRef] [PubMed]
- Owen, D.H.; Wei, L.; Bertino, E.M.; Edd, T.; Villalona-Calero, M.A.; He, K.; Shields, P.G.; Carbone, D.P.; Otterson, G.A. Incidence, Risk Factors, and Effect on Survival of Immune-related Adverse Events in Patients with Non-Small-cell Lung Cancer. Clin. Lung Cancer 2018, 19, e893–e900. [Google Scholar] [CrossRef]
- Weberpals, J.; Jansen, L.; Silversmit, G.; Verbeeck, J.; van der Geest, L.; Vissers, P.A.; Zadnik, V.; Brenner, H. Comparative performance of a modified landmark approach when no time of treatment data are available within oncological databases: Exemplary cohort study among resected pancreatic cancer patients. Clin. Epidemiol. 2018, 10, 1109–1125. [Google Scholar] [CrossRef]
- Petrelli, F.; Signorelli, D.; Ghidini, M.; Ghidini, A.; Pizzutilo, E.G.; Ruggieri, L.; Cabiddu, M.; Borgonovo, K.; Dognini, G.; Brighenti, M.; et al. Association of Steroids use with Survival in Patients Treated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-Analysis. Cancers 2020, 12, 546. [Google Scholar] [CrossRef]
- Wang, Y.; Yang, M.; Tao, M.; Liu, P.; Kong, C.; Li, H.; Chen, Y.; Yin, X.; Yan, X. Corticosteroid administration for cancer-related indications is an unfavorable prognostic factor in solid cancer patients receiving immune checkpoint inhibitor treatment. Int. Immunopharmacol. 2021, 99, 108031. [Google Scholar] [CrossRef]
- Bai, X.; Hu, J.; Warner, A.B.; Quach, H.T.; Cann, C.G.; Zhang, M.Z.; Si, L.; Tang, B.; Cui, C.; Yang, X.; et al. Early Use of High-Dose Glucocorticoid for the Management of irAE Is Associated with Poorer Survival in Patients with Advanced Melanoma Treated with Anti-PD-1 Monotherapy. Clin. Cancer Res. 2021, 27, 5993–6000. [Google Scholar] [CrossRef]
- Suazo-Zepeda, E.; Bokern, M.; Vinke, P.C.; Hiltermann, T.J.N.; de Bock, G.H.; Sidorenkov, G. Risk factors for adverse events induced by immune checkpoint inhibitors in patients with non-small-cell lung cancer: A systematic review and meta-analysis. Cancer Immunol. Immunother. 2021, 70, 3069–3080. [Google Scholar] [CrossRef]
- Chennamadhavuni, A.; Abushahin, L.; Jin, N.; Presley, C.J.; Manne, A. Risk Factors and Biomarkers for Immune-Related Adverse Events: A Practical Guide to Identifying High-Risk Patients and Rechallenging Immune Checkpoint Inhibitors. Front. Immunol. 2022, 13, 779691. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Shimizu, J.; Oya, Y.; Watanabe, N.; Hasegawa, T.; Horio, Y.; Inaba, Y.; Fujiwara, Y. Risk factors for pneumonitis in patients with non-small cell lung cancer treated with immune checkpoint inhibitors plus chemotherapy: A retrospective analysis. Thorac. Cancer 2022, 13, 724–731. [Google Scholar] [CrossRef]
- Fujimoto, A.; Toyokawa, G.; Koutake, Y.; Kimura, S.; Kawamata, Y.; Fukuishi, K.; Yamazaki, K.; Takeo, S. Association between pretreatment neutrophil-to-lymphocyte ratio and immune-related adverse events due to immune checkpoint inhibitors in patients with non-small cell lung cancer. Thorac. Cancer 2021, 12, 2198–2204. [Google Scholar] [CrossRef] [PubMed]
- Pavan, A.; Calvetti, L.; Maso, A.D.; Attili, I.; Del Bianco, P.; Pasello, G.; Guarneri, V.; Aprile, G.; Conte, P.; Bonanno, L. Peripheral Blood Markers Identify Risk of Immune-Related Toxicity in Advanced Non-Small Cell Lung Cancer Treated with Immune-Checkpoint Inhibitors. Oncologist 2019, 24, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Matsukane, R.; Watanabe, H.; Minami, H.; Hata, K.; Suetsugu, K.; Tsuji, T.; Masuda, S.; Okamoto, I.; Nakagawa, T.; Ito, T.; et al. Continuous monitoring of neutrophils to lymphocytes ratio for estimating the onset, severity, and subsequent prognosis of immune related adverse events. Sci. Rep. 2021, 11, 1324. [Google Scholar] [CrossRef]
- Stares, M.; Swan, A.; Cumming, K.; Ding, T.-E.; Leach, J.; Stratton, C.; Thomson, F.; Barrie, C.; MacLennan, K.; Campbell, S.; et al. Hypoalbuminaemia as a prognostic biomarker of first-line treatment resistance in metastatic non-small cell lung cancer. Front. Nutr. 2021, 8, 734735. [Google Scholar] [CrossRef]
- Shah, M.; Marmarelis, M.E.; Mamtani, R.; Hennessy, S. Association between Survival and Very High Versus High PD-L1 Expression in Patients Receiving Pembrolizumab as First-line Treatment for Advanced Non-Small Cell Lung Cancer. Clin. Lung Cancer 2022, 23, 731–736. [Google Scholar] [CrossRef]
- Aguilar, E.J.; Ricciuti, B.; Gainor, J.F.; Kehl, K.L.; Kravets, S.; Dahlberg, S.; Nishino, M.; Sholl, L.M.; Adeni, A.; Subegdjo, S.; et al. Outcomes to first-line pembrolizumab in patients with non-small-cell lung cancer and very high PD-L1 expression. Ann. Oncol. 2019, 30, 1653–1659. [Google Scholar] [CrossRef]
- Lebbé, C.; Meyer, N.; Mortier, L.; Marquez-Rodas, I.; Robert, C.; Rutkowski, P.; Menzies, A.M.; Eigentler, T.; Ascierto, P.A.; Smylie, M.; et al. Evaluation of Two Dosing Regimens for Nivolumab in Combination with Ipilimumab in Patients with Advanced Melanoma: Results from the Phase IIIb/IV CheckMate 511 Trial. J. Clin. Oncol. 2019, 37, 867–875. [Google Scholar] [CrossRef]
- Ghorani, E.; Quartagno, M.; Blackhall, F.; Gilbert, D.C.; O’Brien, M.; Ottensmeier, C.; Pizzo, E.; Spicer, J.; Williams, A.; Badman, P.; et al. REFINE-Lung implements a novel multi-arm randomised trial design to address possible immunotherapy overtreatment. Lancet Oncol. 2023, 24, e219–e227. [Google Scholar] [CrossRef]
- Merrick, S.; Nankivell, M.; Quartagno, M.; Clarke, C.S.; Joharatnam-Hogan, N.; Waddell, T.; O’Carrigan, B.; Seckl, M.; Ghorani, E.; Banks, E.; et al. REFINE (REduced Frequency ImmuNE checkpoint inhibition in cancers): A multi-arm phase II basket trial testing reduced intensity immunotherapy across different cancers. Contemp. Clin. Trials 2023, 124, 107030. [Google Scholar] [CrossRef] [PubMed]
- Buckley, H.L.; Collinson, F.J.; Ainsworth, G.; Poad, H.; Flanagan, L.; Katona, E.; Howard, H.C.; Murden, G.; Banks, R.E.; Brown, J.; et al. PRISM protocol: A randomised phase II trial of nivolumab in combination with alternatively scheduled ipilimumab in first-line treatment of patients with advanced or metastatic renal cell carcinoma. BMC Cancer 2019, 19, 1102. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Total | Without irAE | With irAE | p | |
|---|---|---|---|---|---|
| n = 262 | n = 179 | n = 83 | |||
| n (%) | n (%) | n (%) | |||
| Age (years) | <75 | 220 (84) | 155 (87) | 65 (78) | 0.089 |
| ≥75 | 42 (16) | 24 (13) | 18 (22) | ||
| Sex | Male | 114 (44) | 81 (45) | 33 (40) | 0.404 |
| Female | 148 (56) | 98 (55) | 50 (60) | ||
| ECOG-performance status | 0/1 | 218 (83) | 146 (82) | 72 (87) | 0.296 |
| 2 | 44 (17) | 33 (18) | 11 (13) | ||
| Histologic subtype | Squamous | 54 (21) | 32 (18) | 22 (17) | 0.108 |
| Non-squamous | 208 (79) | 147 (82) | 61 (73) | ||
| PD-L1 expression | <90 | 127 (48) | 94 (53) | 33 (40) | 0.055 |
| ≥90 | 135 (52) | 85 (47) | 50(60) | ||
| KRAS status * | Wildtype | 95 (47) | 65 (45) | 30 (51) | 0.485 |
| Mutant | 107 (53) | 78 (55) | 29 (49) | ||
| Total | Mild irAE (Grade 1–2) | Severe irAE (Grade 3–5) | Time to iRAE (months) | Treated with Steroids | Pembrolizumab Discontinued Secondary to irAE | Progression-Free Survival | Overall Survival | |
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | Median (IQR) | n (%) | n (%) | HR (95% CI) p | HR (95% CI) p | |
| Patients | ||||||||
| Without irAE | 179 (68) | n/a | n/a | n/a | n/a | n/a | ref | ref |
| With irAE | 83 (32) | 52 (63) | 31 (37) | 3.4 (1.4–7.4) | 53 (65) | 42 (51) | 0.41 (0.30–0.56) <0.001 | 0.36 (0.26–0.50) <0.001 |
| irAE Events | ||||||||
| All | 102 | 70 (69) | 32 (31) | 3.5 (2.0–7.5) | 58 (57) | 44 (43) | n/a | n/a |
| Dermatological | 19 (19) | 13 (68) | 6 (19) | 3.0 (1.4–7.9) | 9 (47) | 7 (37) | 0.37 (0.20–0.69) 0.002 | 0.35 (0.19–0.67) 0.001 |
| Endocrine | 33 (32) | ≥28 (≥85) | ≤5 (≤15) | 3.4 (2.0–12.3) | ≤5 (≤15) | ≤5 (≤15) | 0.36 (0.23–0.57) <0.001 | 0.30 (0.18–0.49) <0.001 |
| Gastrointestinal | 13 (13) | ≤5 (≤38) | ≥8 (≥62) | 7.3 (5.7–12.3) | 13 (100) | 11 (85) | 0.23 (0.10–0.52) <0.001 | 0.21 (0.09–0.52) 0.001 |
| Hepatic | 11 (11) | ≤5 (≤45) | ≥6 (≥55) | 3.4 (1.2–6.7) | 8 (73) | 8 (73) | 0.34 (0.15–0.78) 0.011 | 0.27 (0.11–0.67) 0.005 |
| Musculoskeletal | 8 (8) | 8 (100) | 0 (0) | 2.3 (1.9–5.0) | 8 (100) | ≤5 (≤63) | 0.42 (0.19–0.96) 0.039 | 0.49 (0.22–1.11) 0.088 |
| Pulmonary | 10 (10) | ≤5 (≤50 | ≥5 (≥50) | 2.3 (0.3–5.0) | 10 (100) | 9 (90) | 1.12 (0.57–2.18) 0.752 | 1.33 (0.68–2.61) 0.408 |
| Other (Cardiac, Neurological, Renal) | 8 (8) | 8 (100) | 0 (0) | 4.1 (1.7–6.6) | 6 (75) | 6 (75) | n/a | n/a |
| PFS | HR | p | OS | HR | p | |
|---|---|---|---|---|---|---|
| All | ||||||
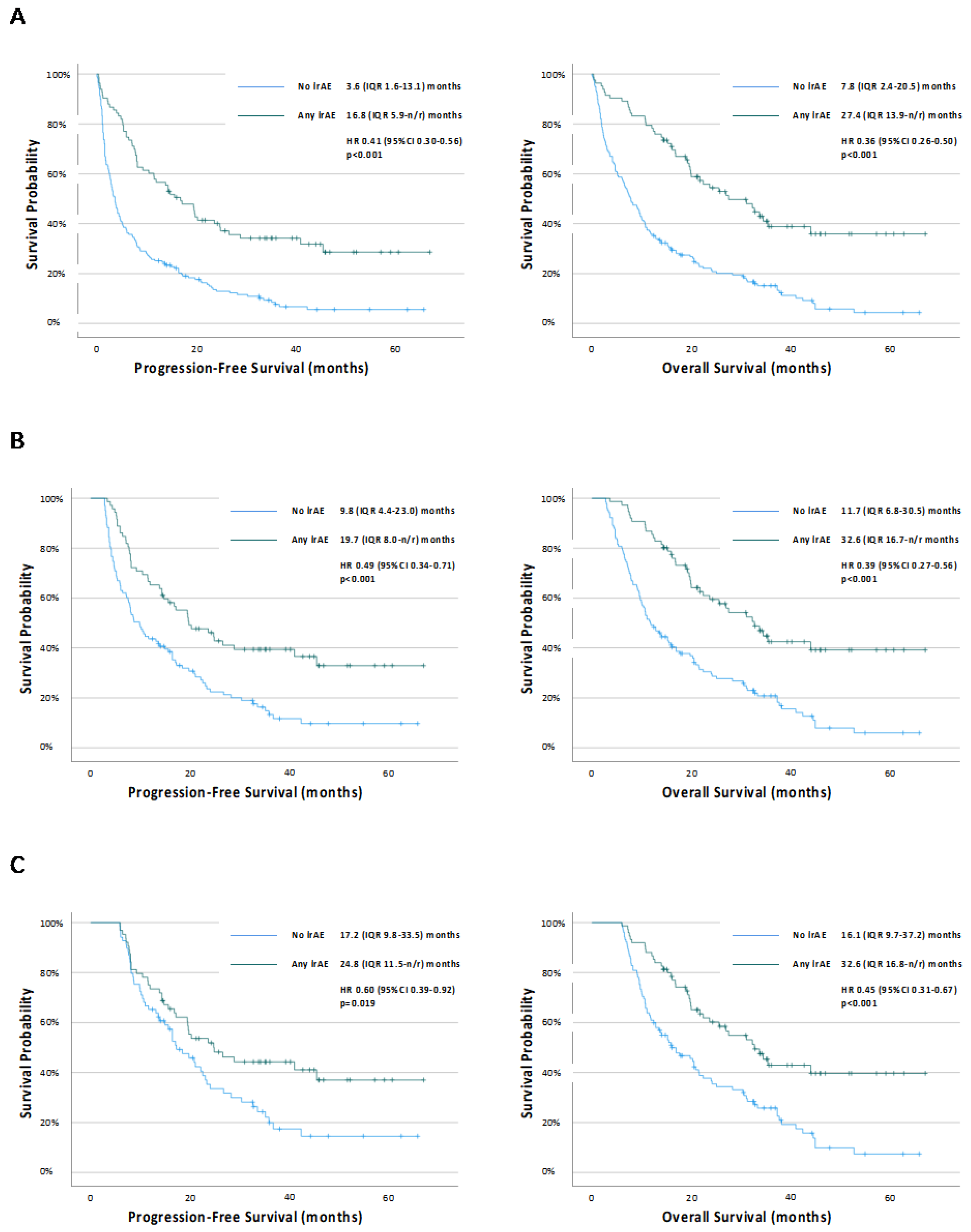
| No irAE | 3.6 (1.3–13.1) | ref | ref | 7.8 (2.4–20.5) | ref | ref |
| Severe irAE | 7.8 (2.2–20.2) | 0.61 (0.40–0.94) | 0.024 | 16.1 (7.3–34.3) | 0.55 (0.35–0.86) | 0.008 |
| Mild irAE | 24.7 (8.1-n/r) | 0.32 (0.22–0.48) | <0.001 | 35.3 (19.7-n/r) | 0.27 (0.18–0.42) | <0.001 |
| 12-week Landmark | ||||||
| No irAE | 9.8 (4.4–23.0) | ref | ref | 11.7 (6.8–30.5) | ref | ref |
| Severe irAE | 14.3 (7.0-n/r) | 0.64 (0.38–1.08) | 0.094 | 22.3 (13.9-n/r) | 0.51 (0.31–0.86) | 0.011 |
| Mild irAE | 24.8 (10.4-n/r) | 0.43 (0.28–0.66) | <0.001 | 35.3 (19.8-n/r) | 0.33 (0.21–0.52) | <0.001 |
| 24-week Landmark | ||||||
| No irAE | 17.2 (9.8–33.5) | ref | ref | 16.1 (9.7–37.2) | ref | ref |
| Severe irAE | 14.7 (7.8-n/r) | 0.81 (0.44–1.47) | 0.481 | 22.3 (13.9-n/r) | 0.62 (0.37–1.05) | 0.074 |
| Mild irAE | 28.8 (14.3-n/r) | 0.51 (0.31–0.84) | 0.008 | 43.9 (19.8-n/r) | 0.38 (0.23–0.61) | <0.001 |
| Characteristics | All | 12-Week Landmark | 24-Week Landmark | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Without irAE | With irAE | OR (95% CI) p | Without irAE | With irAE | OR (95% CI) p | Without irAE | With irAE | OR (95% CI) p | ||
| n = 179 | n = 83 | n = 130 | n = 76 | n = 105 | n = 75 | |||||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||||
| White Cell Count | ≤11.0 × 109/L | 109 (61) | 64 (77) | 2.16 (1.20–3.91) 0.011 | 89 (68) | 59 (78) | 1.60 (0.83–3.08) 0.158 | 80 (76) | 59 (79) | 1.15 (0.57–2.35) 0.696 |
| >11.0 × 109/L | 70 (39) | 19 (23) | 41 (32) | 17 (22) | 25 (24) | 16 (21) | ||||
| Median (IQR) | 10.1 (7.8–13.2) | 8.5 (6.8–10.8) | 0.008 | 9.5 (7.3–11.6) | 8.4 (6.8–10.6) | 0.191 | 9.3 (7.1–11.5) | 8.4 (6.8–10.6) | 0.198 | |
| Neutrophil Count | ≤7.5 × 109/L | 101 (56) | 63 (76) | 2.43 (1.35–4.36) 0.003 | 84 (65) | 58 (76) | 1.76 (0.93–3.34) 0.082 | 70 (67) | 58 (77) | 1.71 (0.87–3.35) 0.120 |
| >7.5 × 109/L | 78 (44) | 20 (24) | 46 (35) | 18 (24) | 35 (33) | 17 (23) | ||||
| Median (IQR) | 6.8 (5.1–10.0) | 5.9 (4.5–7.4) | 0.010 | 5.8 (4.5–7.4) | 6.1 (4.8–8.4) | 0.245 | 5.7 (4.6–7.9) | 6.0 (4.6–8.3) | 0.624 | |
| NLR | <5 | 104 (58) | 51 (61) | 1.15 (0.67–1.96) 0.608 | 89 (68) | 49 (64) | 0.84 (0.46–1.52) 0.557 | 75 (71) | 49 (65) | 0.76 (0.40–1.43) 0.384 |
| ≥5 | 75 (42) | 32 (39) | 41 (32) | 27 (36) | 30 (29) | 26 (35) | ||||
| Median (IQR) | 4.3 (2.8–7.4) | 4.3 (2.8–6.5) | 0.122 | 3.8 (2.6–2.0) | 3.9 (2.8–5.7) | 0.524 | 3.6 (2.6–5.1) | 4.4 (2.9–6.6) | 0.737 | |
| PLR | ≤180 | 51 (28) | 28 (34) | 1.28 (0.73–2.23) 0.390 | 41 (32) | 28 (37) | 1.27 (0.70–2.30) 0.437 | 39 (37) | 28 (62) | 1.01 (0.55–1.86) 0.979 |
| >180 | 128 (72) | 55 (66) | 89 (68) | 48 (66) | 66 (63) | 47 (38) | ||||
| Median (IQR) | 225 (169–321) | 238 (155–238) | 0.548 | 219 (165–306) | 226 (145–336) | 0.477 | 202 (150–276) | 260 (163–352) | 0.216 | |
| Albumin | ≥35 g/L | 86 (48) | 55 (66) | 2.12 (1.24–3.65) 0.006 | 71 (55) | 53 (70) | 1.91 (1.05–3.49) 0.034 | 62 (59) | 52 (69) | 1.57 (0.84–2.93) 0.159 |
| <35 g/L | 93 (52) | 28 (34) | 59 (45) | 23 (30) | 43 (41) | 23 (31) | ||||
| Median (IQR) | 34 (29–38) | 36 (32–41) | 0.005 | 35 (31–39) | 37 (33–41) | 0.07 | 35 (31–38) | 36 (33–41) | 0.285 | |
| PNI | ≥45 | 66 (37) | 39 (47) | 1.52 (0.90–2.57) 0.121 | 55 (42) | 38 (50) | 1.36 (0.77–2.41) 0.285 | 49 (47) | 37 (49) | 1.11 (0.61–2.01) 0.724 |
| <45 | 113 (63) | 44 (53) | 75 (68) | 38 (50) | 56 (53) | 38 (51) | ||||
| Median (IQR) | 42.0 (36.5–47.5) | 44.8 (40.3–49.0) | 0.411 | 43.0 (38.7–48.0) | 45.0 (41.4–49.5) | 0.679 | 43.2 (37.9–46.3) | 45.6 (40.8–49.3) | 0.743 | |
| SIPS | 0 | 65 (36) | 44 (53) | 1.98 (1.67–3.35) 0.011 | 56 (43) | 42 (55) | 1.63 (0.92–2.88) 0.09 | 48 (46) | 42 (56) | 1.51 (0.84–2.74) 0.174 |
| 1/2 | 114 (64) | 39 (47) | 74 (57) | 34 (45) | 57 (54) | 33 (44) | ||||
| Progression-Free Survival | Overall Survival | ||||||
|---|---|---|---|---|---|---|---|
| Without irAE | With irAE | HR (95% CI) p | Without irAE | With irAE | HR (95% CI) p | ||
| Median (IQR) | Median (IQR) | Median (IQR) | Median (IQR) | ||||
| SIPS | 0 | 7.6 (2.7–23.3) | 14.7 (5.3-n/r) | 0.57 (0.36–0.91) 0.015 | 14.0 (2.8–5.3) | 34.3 (18.9-n/r) | 0.40 (0.24–0.67) 0.001 |
| 1 | 3.6 (1.8–13.6) | 19.5 (7.1–45.4) | 0.38 (0.22–0.64) <0.001 | 8.2 (3.0–21.5) | 23.6 (12.3-n/r) | 0.40 (0.24–0.69) 0.001 | |
| 2 | 1.6 (0.8–4.0) | 8.1 (7.5–28.8) | 0.26 (0.11–0.64) 0.003 | 2.9 (1.5–9.2) | 16.7 (7.5–33.2) | 0.35 (0.16–0.81) 0.013 | |
| HR (95% CI) p | 1.75 (1.43–2.14) <0.001 | 1.15 (0.78–1.69) 0.479 | 1.67 (1.37–2.04) <0.001 | 1.53 (1.03–2.28) 0.037 | |||
| White Cell Count | ≤11.0 × 109/L | 4.6 (1.8–16.4) | 15.6 (5.9–45.4) | 0.50 (0.35–0.72) <0.001 | 10.1 (4.1–28.2) | 32.2 (14.3-n/r) | 0.43 (0.29–0.63) <0.001 |
| >11.0 × 109/L | 1.6 (0.9–6.0) | 19.6 (7.5-n/r) | 0.27 (0.14–0.51) <0.001 | 4.1 (1.7–11.8) | 25.5 (7.5-n/r) | 0.28 (0.14–0.53) <0.001 | |
| HR (95% CI) p | 1.74 (1.26–3.40) 0.001 | 0.85 (0.45–1.62) 0.621 | 1.80 (1.30–2.49) <0.001 | 1.05 (0.53–2.07) 0.896 | |||
| Neutrophil Count | ≤7.5 × 109/L | 11.0 (6.0–14.9) | 20.4 (15.6–27.1) | 0.54 (0.38–0.78) 0.001 | 10.7 (4.5–31.0) | 32.2 (14.3-n/r) | 0.46 (0.31–0.68) <0.001 |
| >7.5 × 109/L | 3.3 (1.6–5.2) | 17.9 (19.6–28.8) | 0.25 (0.13–0.47) <0.001 | 4.1 (1.6–10.4) | 25.5 (7.5-n/r) | 0.26 (0.13–0.49) <0.001 | |
| HR (95% CI) p | 2.11 (1.54–2.91) <0.001 | 0.83 (0.44–1.57) 0.560 | 2.02 (1.46–2.78) <0.001 | 1.06 (0.54–2.09) 0.868 | |||
| Albumin | ≥35 g/L | 6.0 (1.7–23.0) | 17.1 (5.9-n/r) | 0.48 (0.32–0.73) 0.001 | 11.0 (4.6–32.6) | 43.9 (19.2-n/r) | 0.35 (0.22–0.56) <0.001 |
| <35 g/L | 2.5 (1.2–5.9) | 14.3 (5.9–26.5) | 0.35 (0.22–0.57) <0.001 | 4.7 (1.7–11.7) | 16.7 (8.0–32.6) | 0.42 (0.26–0.67) <0.001 | |
| HR (95% CI) p | 1.97 (1.43–2.72) <0.001 | 1.53 (0.89–2.61) 0.123 | 1.88 (1.37–2.59) <0.001 | 2.30 (1.29–4.10) 0.005 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raynes, G.; Stares, M.; Low, S.; Haron, D.; Sarwar, H.; Abhi, D.; Barrie, C.; Laird, B.; Caledonian Cachexia Collaborative; Phillips, I.; et al. Immune-Related Adverse Events, Biomarkers of Systemic Inflammation, and Survival Outcomes in Patients Receiving Pembrolizumab for Non-Small-Cell Lung Cancer. Cancers 2023, 15, 5502. https://doi.org/10.3390/cancers15235502
Raynes G, Stares M, Low S, Haron D, Sarwar H, Abhi D, Barrie C, Laird B, Caledonian Cachexia Collaborative, Phillips I, et al. Immune-Related Adverse Events, Biomarkers of Systemic Inflammation, and Survival Outcomes in Patients Receiving Pembrolizumab for Non-Small-Cell Lung Cancer. Cancers. 2023; 15(23):5502. https://doi.org/10.3390/cancers15235502
Chicago/Turabian StyleRaynes, George, Mark Stares, Samantha Low, Dhania Haron, Hussain Sarwar, Dhruv Abhi, Colin Barrie, Barry Laird, Caledonian Cachexia Collaborative, Iain Phillips, and et al. 2023. "Immune-Related Adverse Events, Biomarkers of Systemic Inflammation, and Survival Outcomes in Patients Receiving Pembrolizumab for Non-Small-Cell Lung Cancer" Cancers 15, no. 23: 5502. https://doi.org/10.3390/cancers15235502