
Clinical Features of Gastric Signet Ring Cell Cancer: Results from a Systematic Review and Meta-Analysis

 , , , ,
, , , ,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
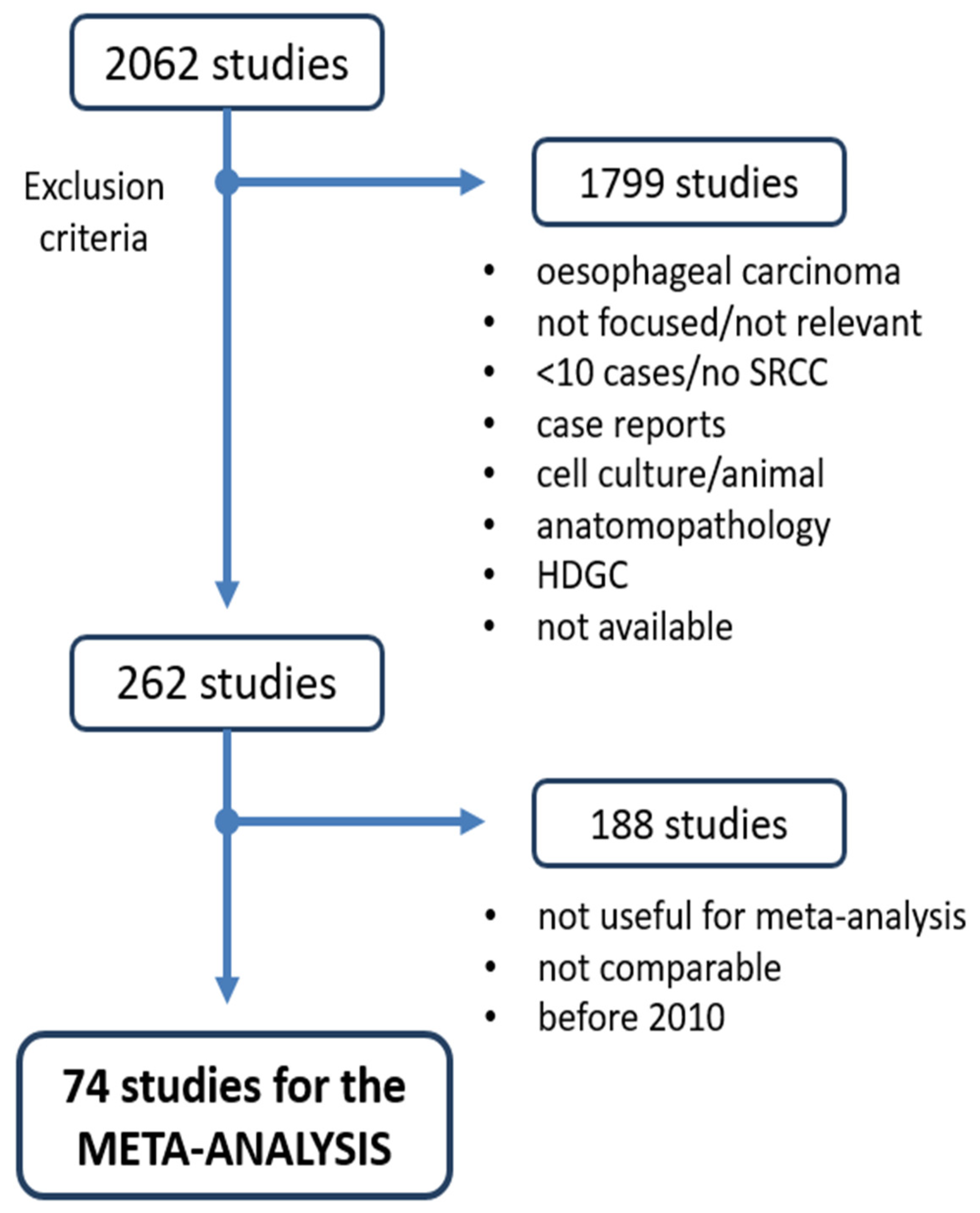
2.1. Search Strategy and Study Selection
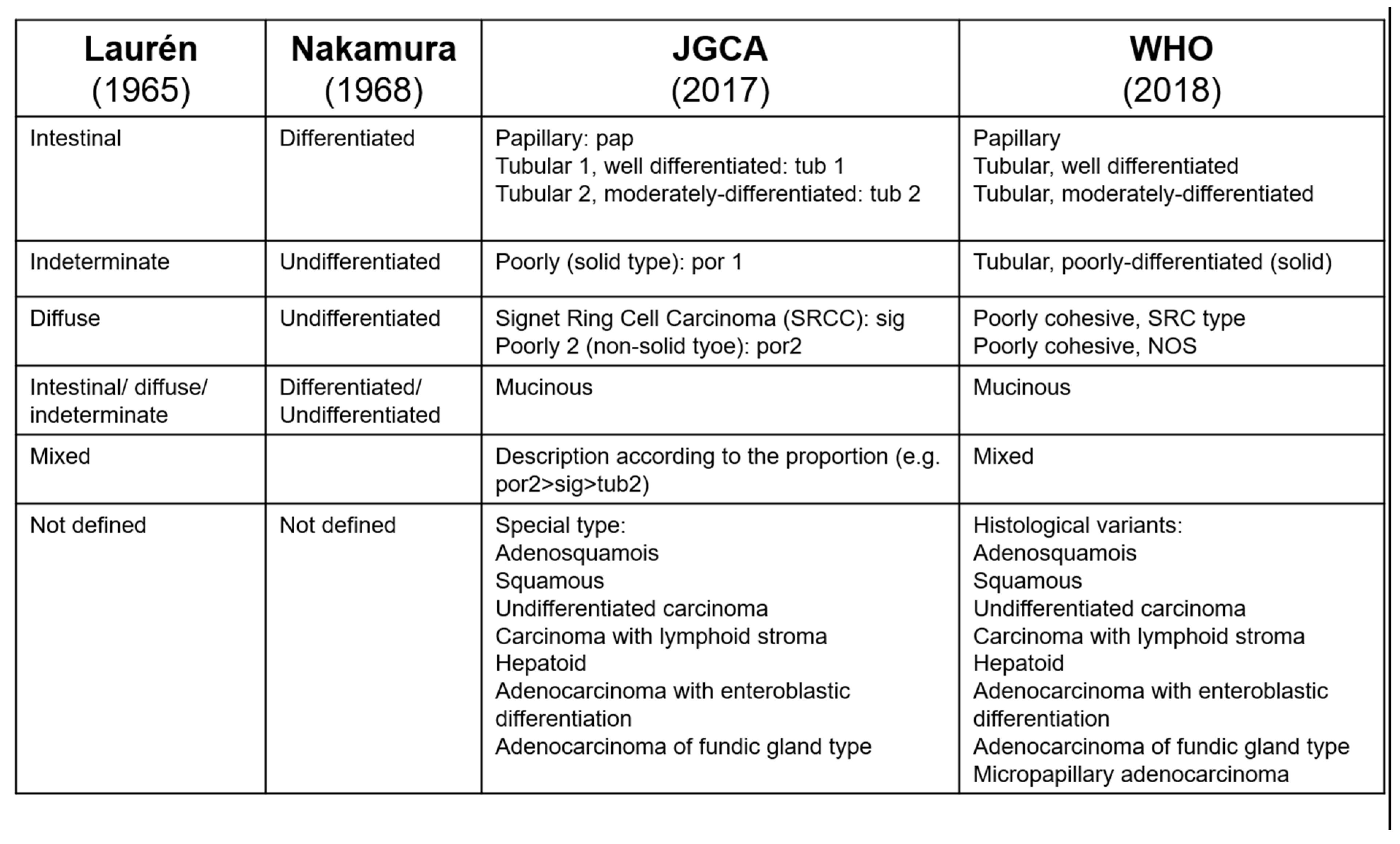
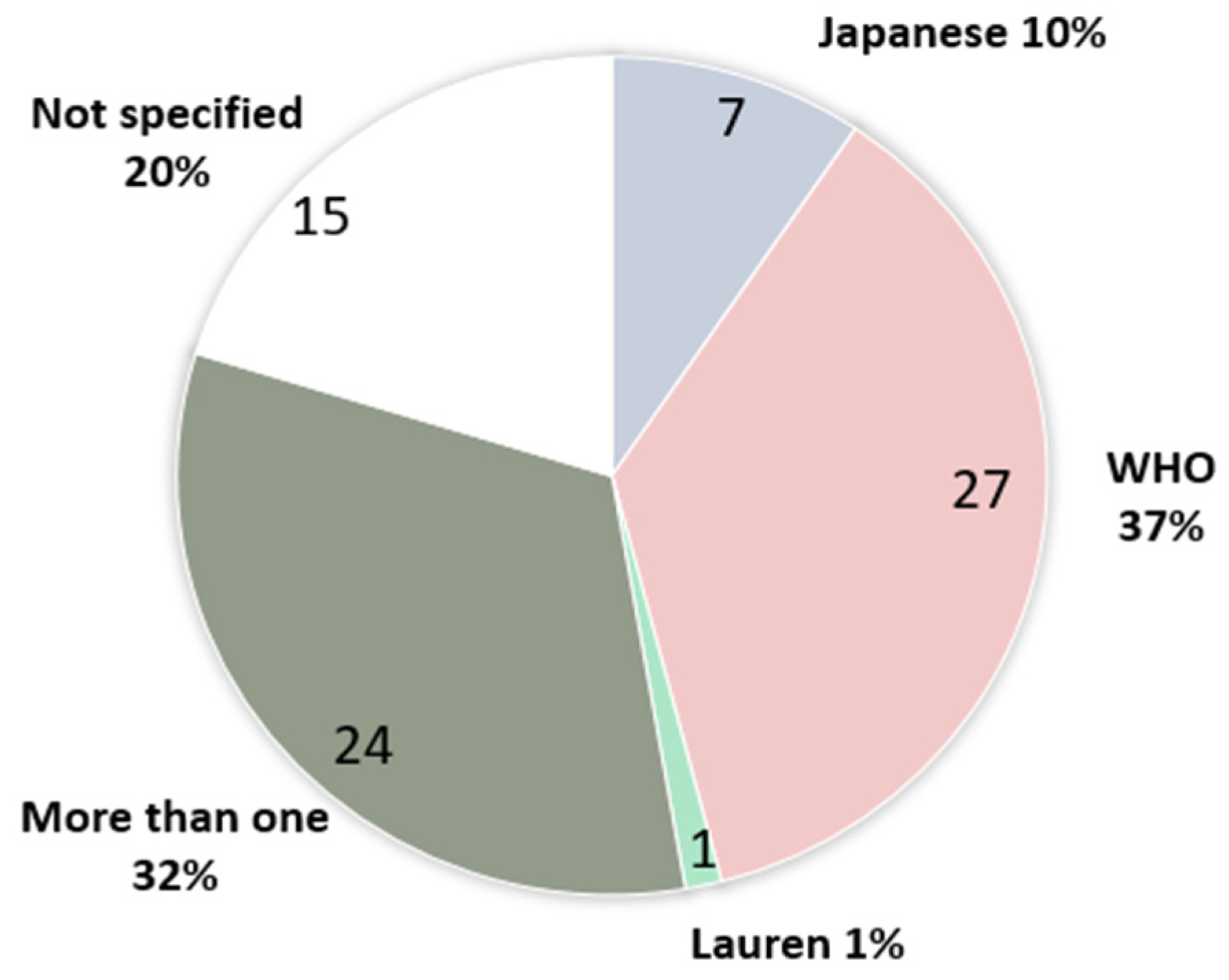
2.2. Analysis of Histopathologic Classification Systems and Definitions of SRCC
2.3. Statistical Analysis—Meta-Analysis
3. Results
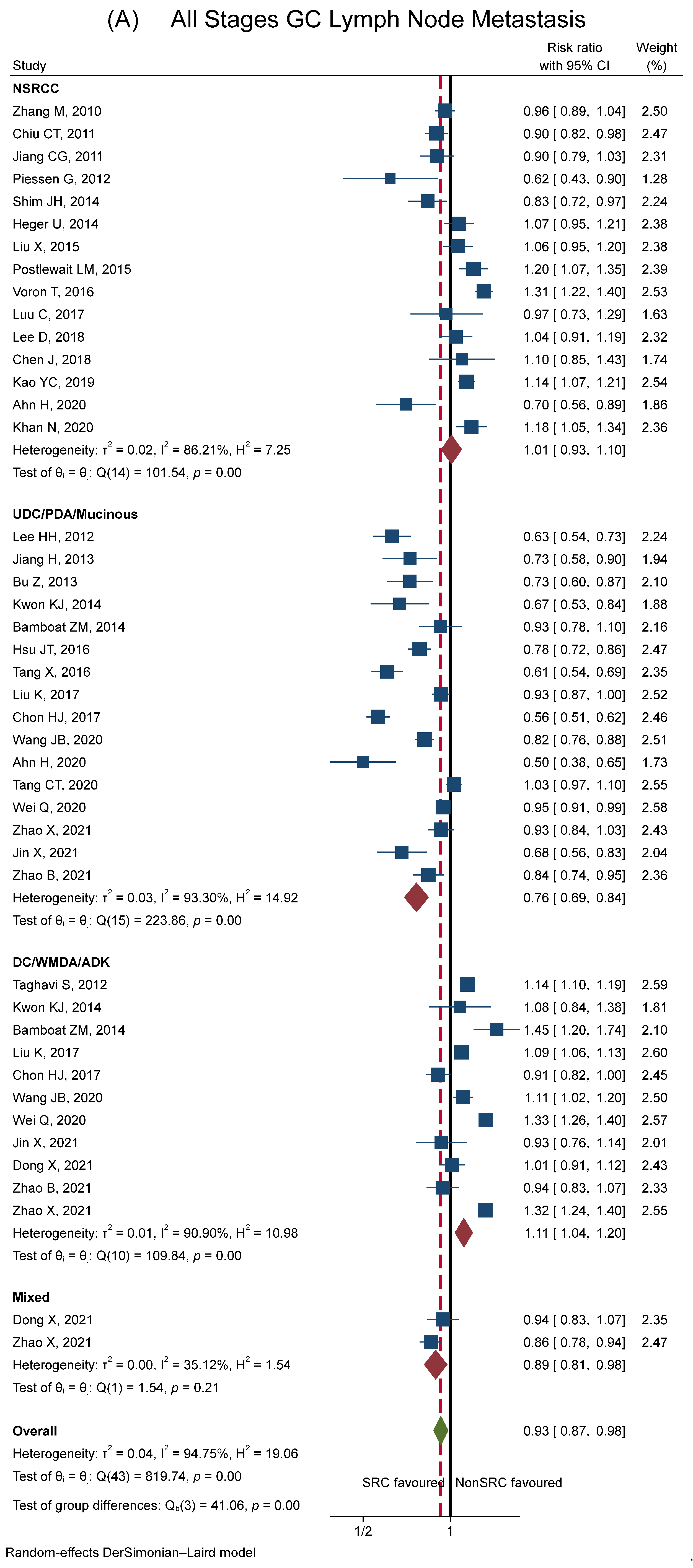
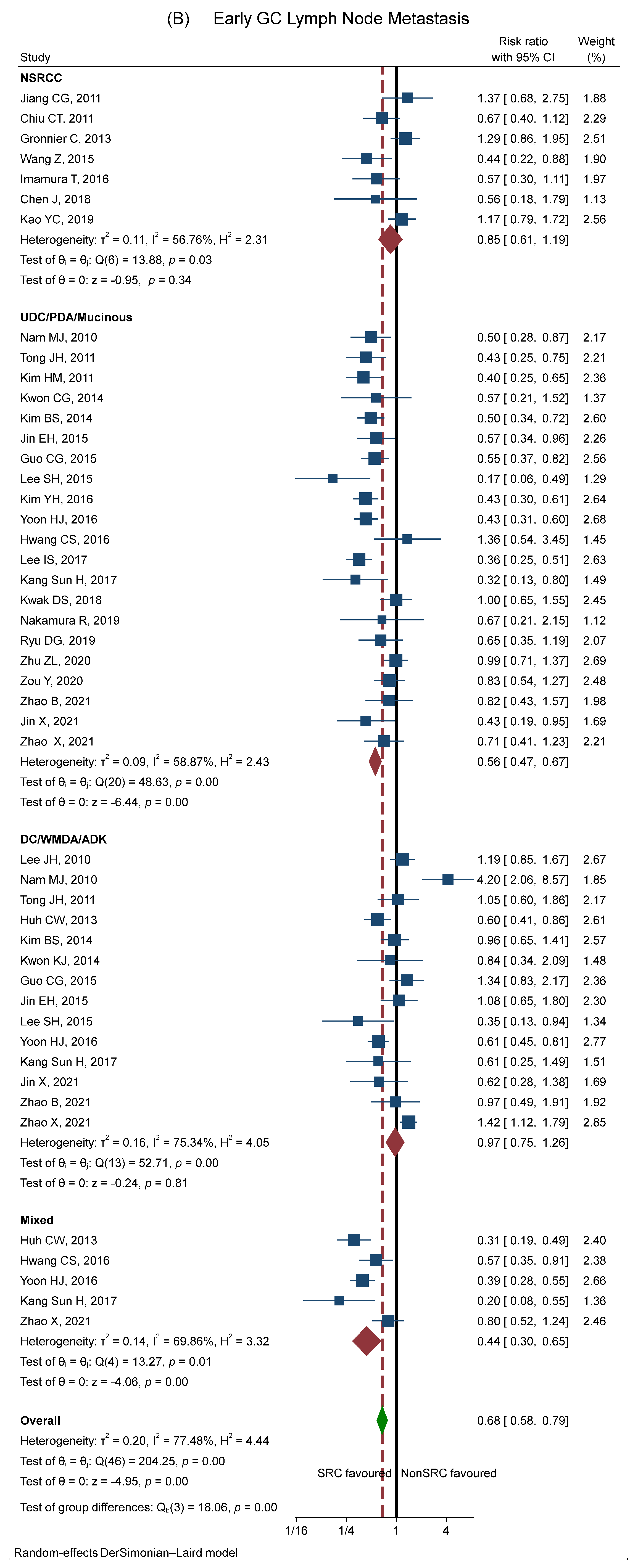
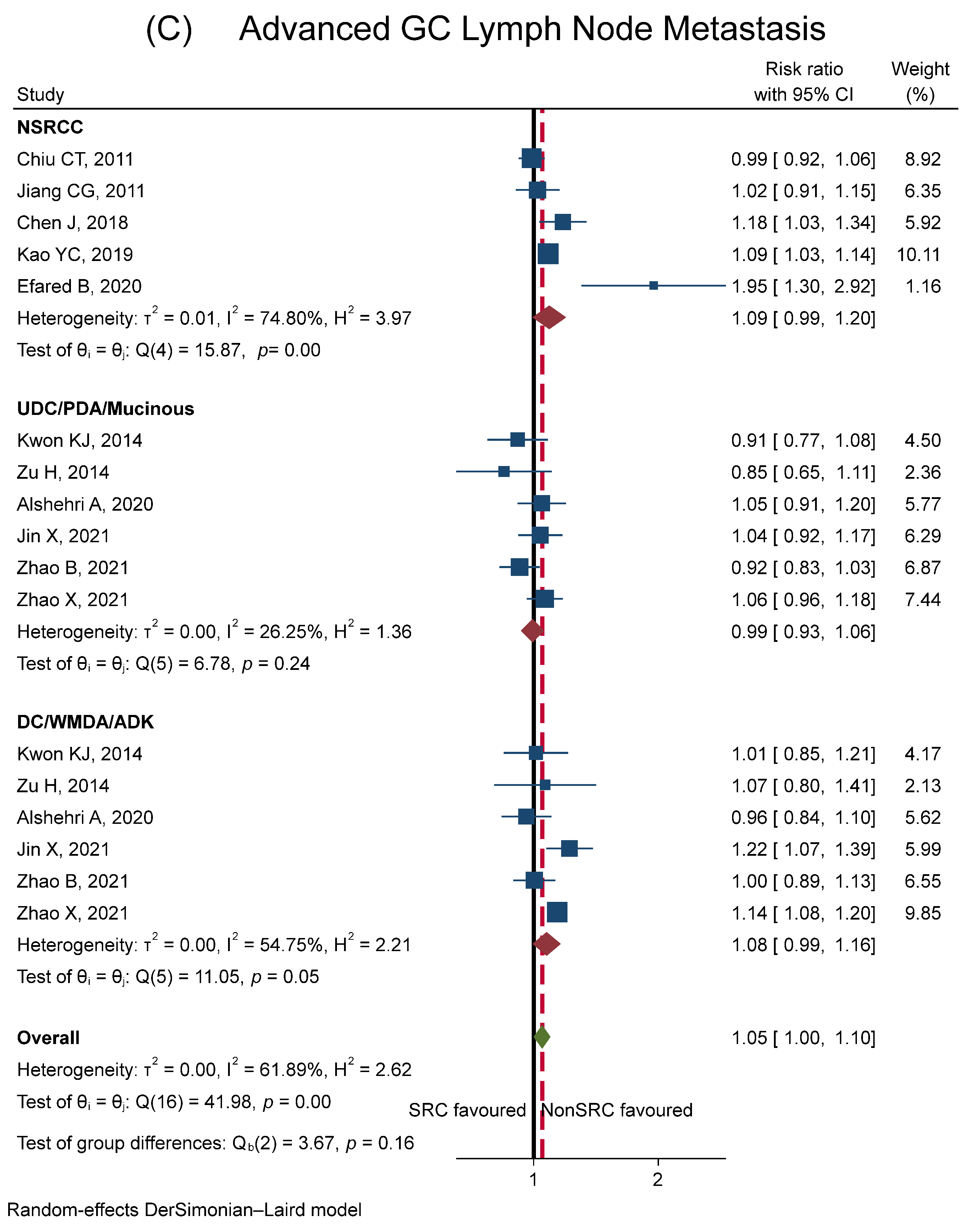
3.1. Lymph Node Metastasis
3.2. Lymphovascular Invasion
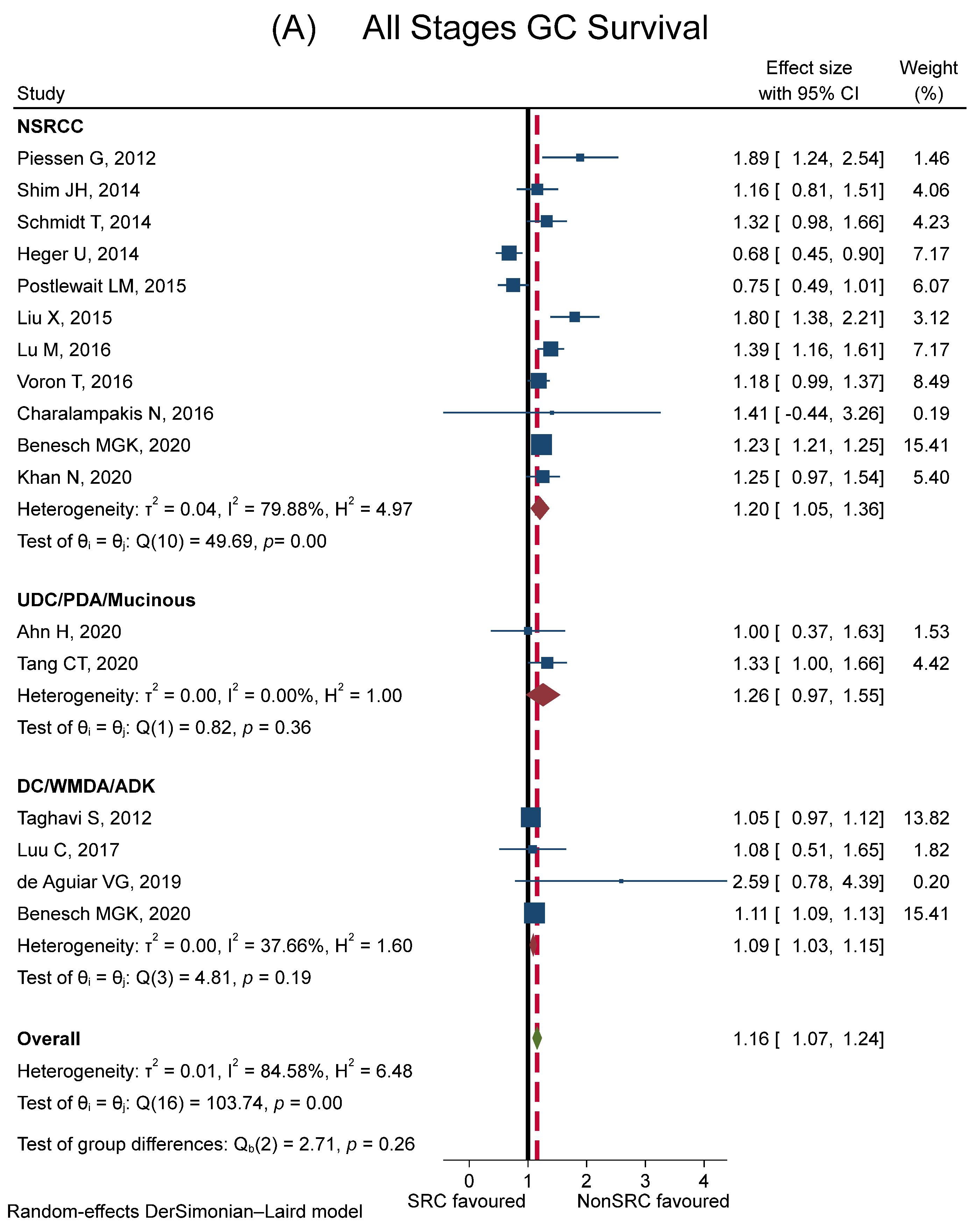
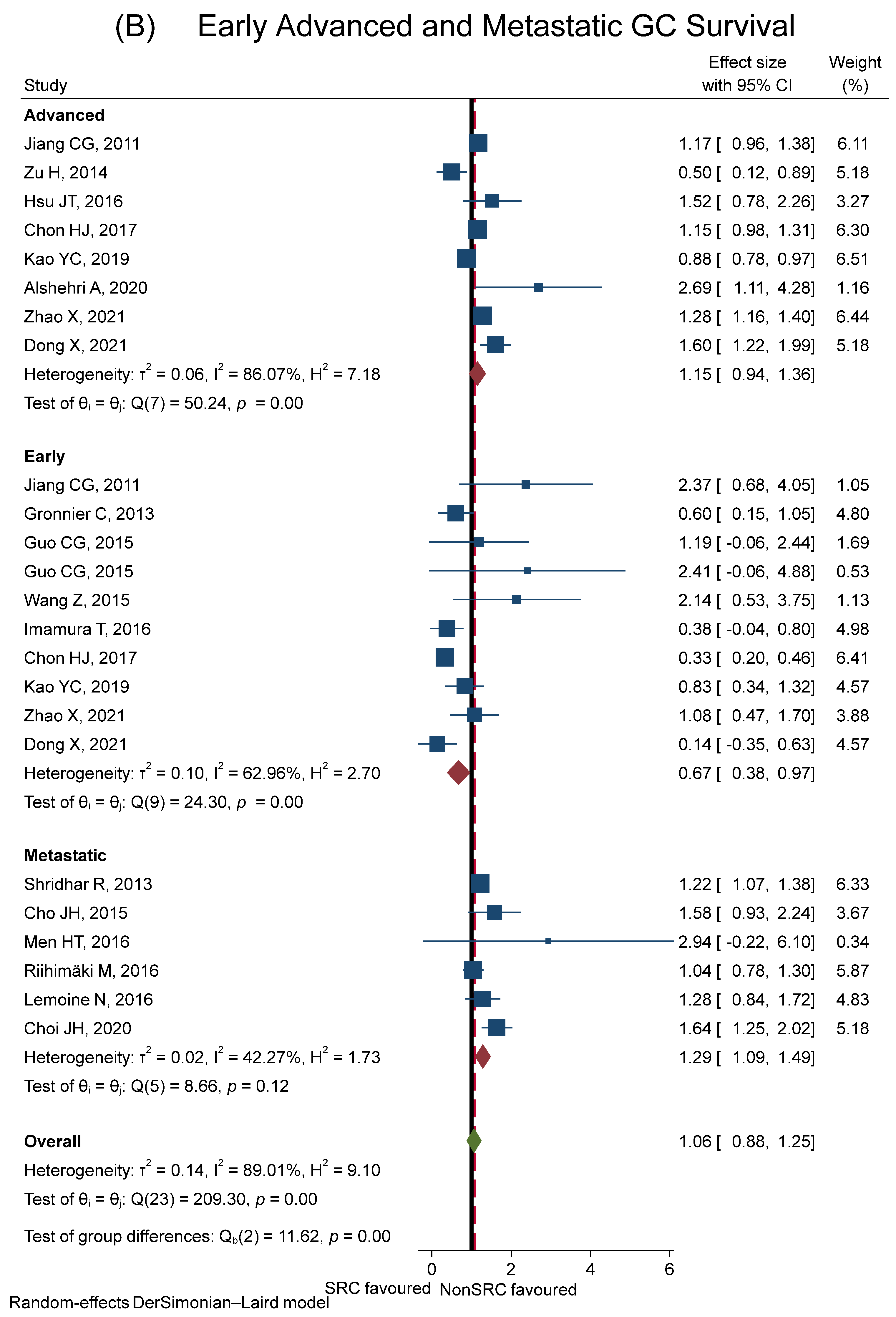
3.3. Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Thrift, A.P.; Wenker, T.N.; El-Serag, H.B. Global burden of gastric cancer: Epidemiological trends, risk factors, screening and prevention. Nat. Rev. Clin. Oncol. 2023, 20, 338–349. [Google Scholar] [CrossRef] [PubMed]
- Golembeski, C.P.; Genta, R.M. Signet-ring cell carcinoma in gastric biopsies: Expecting the unexpected. J. Clin. Pathol. 2013, 66, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Thiels, C.A.; Ikoma, N.; Fournier, K.; Das, P.; Blum, M.; Estrella, J.S.; Minsky, B.D.; Ajani, J.; Mansfield, P.; Badgwell, B.D. Repeat staging laparoscopy for gastric cancer after preoperative therapy. J. Surg. Oncol. 2018, 118, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Simon, M.; Mal, F.; Perniceni, T.; Ferraz, J.M.; Strauss, C.; Levard, H.; Louvet, C.; Fuks, D.; Gayet, B. Accuracy of staging laparoscopy in detecting peritoneal dissemination in patients with gastroesophageal adenocarcinoma. Dis. Esophagus 2016, 29, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Nassour, I.; Fullington, H.; Hynan, L.S.; Yopp, A.C.; Augustine, M.M.; Polanco, P.M.; Choti, M.A.; Mansour, J.C.; Wang, S.C.; Porembka, M.R. The Yield of Staging Laparoscopy in Gastric Cancer is Affected by Racial and Ethnic Differences in Disease Presentation. Ann. Surg. Oncol. 2017, 24, 1787–1794. [Google Scholar] [CrossRef]
- Bamboat, Z.M.; Tang, L.H.; Vinuela, E.; Kuk, D.; Gonen, M.; Shah, M.A.; Brennan, M.F.; Coit, D.G.; Strong, V.E. Stage-stratified prognosis of signet ring cell histology in patients undergoing curative resection for gastric adenocarcinoma. Ann. Surg. Oncol. 2014, 21, 1678–1685. [Google Scholar] [CrossRef]
- Charalampakis, N.; Xiao, L.; Elimova, E.; Wadhwa, R.; Shiozaki, H.; Shimodaira, Y.; Blum, M.A.; Planjery, V.; Rogers, J.E.; Matamoros, A.; et al. Initial standardized uptake value of positron emission tomography influences the prognosis of patients with localized gastric adenocarcinoma treated preoperatively. Oncology 2015, 89, 305–310. [Google Scholar] [CrossRef]
- Heger, U.; Blank, S.; Wiecha, C.; Langer, R.; Weichert, W.; Lordick, F.; Bruckner, T.; Dobritz, M.; Burian, M.; Springfeld, C.; et al. Is preoperative chemotherapy followed by surgery the appropriate treatment for signet ring cell containing adenocarcinomas of the esophagogastric junction and stomach? Ann. Surg. Oncol. 2014, 21, 1739–1748. [Google Scholar] [CrossRef] [PubMed]
- Arai, T. Where does signet-ring cell carcinoma come from and where does it go? Gastric Cancer 2019, 22, 651–652. [Google Scholar] [CrossRef]
- Watanabe, H.; Jass, J.; Sobin, J. WHO International Histological Classification of Tumours; Springer: Berlin, Germany, 1990. [Google Scholar]
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the Digestive System, 4th ed.; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- International Agency for Research on Cancer. WHO Classification of Tumours Editorial Board: Digestive System Tumours; International Agency for Research on Cancer: Lyon, France, 2019. [Google Scholar]
- Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2014 (ver. 4). Gastric Cancer 2017, 20, 1–19. [Google Scholar] [CrossRef]
- Lauren, p. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Nakamura, K.; Sugano, H.; Takagi, K. Carcinoma of the stomach in incipient phase: Its histogenesis and histological appearances. GANN Jpn. J. Cancer Res. 1968, 59, 251–258. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kerckhoffs, K.G.P.; Liu, D.H.W.; Saragoni, L.; van der Post, R.S.; Langer, R.; Bencivenga, M.; Iglesias, M.; Gallo, G.; Hewitt, L.C.; Fazzi, G.E.; et al. Mucin expression in gastric- and gastro-oesophageal signet-ring cell cancer: Results from a comprehensive literature review and a large cohort study of Caucasian and Asian gastric cancer. Gastric Cancer 2020, 23, 765–779. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 15 September 2023).
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Efared, B.; Kadi, M.; Tahiri, L.; Lahmidani, N.; Hassani, K.M.; Bouhaddouti, H.E.; Benbrahim, Z.; Adil, I.S.; Chbani, L. Gastric Signet Ring Cell Carcinoma: A Comparative Analysis of Clinicopathologic Features. Cancer Control 2020, 27, 1073274820976596. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Choi, I.J.; Kook, M.C.; Nam, B.H.; Kim, Y.W.; Ryu, K.W. Risk factors for lymph node metastasis in patients with early gastric cancer and signet ring cell histology. Br. J. Surg. 2010, 97, 732–736. [Google Scholar] [CrossRef]
- Nam, M.J.; Oh, S.J.; Oh, C.A.; Kim, D.H.; Bae, Y.S.; Choi, M.G.; Noh, J.H.; Sohn, T.S.; Bae, J.M.; Kim, S. Frequency and predictive factors of lymph node metastasis in mucosal cancer. J. Gastric Cancer 2010, 10, 162–167. [Google Scholar] [CrossRef]
- Kim, H.M.; Pak, K.H.; Chung, M.J.; Cho, J.H.; Hyung, W.J.; Noh, S.H.; Kim, C.B.; Lee, Y.C.; Song, S.Y.; Lee, S.K. Early gastric cancer of signet ring cell carcinoma is more amenable to endoscopic treatment than is early gastric cancer of poorly differentiated tubular adenocarcinoma in select tumor conditions. Surg. Endosc. 2011, 25, 3087–3093. [Google Scholar] [CrossRef]
- Tong, J.H.; Sun, Z.; Wang, Z.N.; Zhao, Y.H.; Huang, B.J.; Li, K.; Xu, Y.; Xu, H.M. Early gastric cancer with signet-ring cell histologic type: Risk factors of lymph node metastasis and indications of endoscopic surgery. Surgery 2011, 149, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Huh, C.W.; Jung, D.H.; Kim, J.H.; Lee, Y.C.; Kim, H.; Kim, H.; Yoon, S.O.; Youn, Y.H.; Park, H.; Lee, S.I.; et al. Signet ring cell mixed histology may show more aggressive behavior than other histologies in early gastric cancer. J. Surg. Oncol. 2013, 107, 124–129. [Google Scholar] [CrossRef]
- Kim, B.S.; Oh, S.T.; Yook, J.H. Signet ring cell type and other histologic types: Differing clinical course and prognosis in T1 gastric cancer. Surgery 2014, 155, 1030–1035. [Google Scholar] [CrossRef]
- Guo, C.G.; Zhao, D.B.; Liu, Q.; Zhou, Z.X.; Zhao, P.; Wang, G.Q.; Cai, J.Q. Risk Factors for Lymph Node Metastasis in Early Gastric Cancer with Signet Ring Cell Carcinoma. J. Gastrointest. Surg. 2015, 19, 1958–1965. [Google Scholar] [CrossRef] [PubMed]
- Jin, E.H.; Lee, D.H.; Jung, S.A.; Shim, K.N.; Seo, J.Y.; Kim, N.; Shin, C.M.; Yoon, H.; Jung, H.C. Clinicopathologic factors and molecular markers related to lymph node metastasis in early gastric cancer. World J. Gastroenterol. 2015, 21, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Jee, S.R.; Kim, J.H.; Seol, S.Y. Intramucosal gastric cancer: The rate of lymph node metastasis in signet ring cell carcinoma is as low as that in well-differentiated adenocarcinoma. Eur. J. Gastroenterol. Hepatol. 2015, 27, 170–174. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, X.; Hu, J.; Zeng, W.; Zhou, Z. Clinicopathological features and outcomes in patients undergoing radical resection for early gastric cancer with signet ring cell histology. J. Visc. Surg. 2015, 152, 357–361. [Google Scholar] [CrossRef]
- Hwang, C.S.; Ahn, S.; Lee, B.E.; Lee, S.J.; Kim, A.; Choi, C.I.; Kim, D.H.; Jeon, T.Y.; Kim, G.H.; Song, G.A.; et al. Risk of lymph node metastasis in mixed-type early gastric cancer determined by the extent of the poorly differentiated component. World J. Gastroenterol. 2016, 22, 4020–4026. [Google Scholar] [CrossRef]
- Imamura, T.; Komatsu, S.; Ichikawa, D.; Kawaguchi, T.; Kosuga, T.; Okamoto, K.; Konishi, H.; Shiozaki, A.; Fujiwara, H.; Otsuji, E. Early signet ring cell carcinoma of the stomach is related to favorable prognosis and low incidence of lymph node metastasis. J. Surg. Oncol. 2016, 114, 607–612. [Google Scholar] [CrossRef]
- Kim, Y.H.; Kim, J.H.; Kim, H.K.; Kim, H.; Lee, Y.C.; Lee, S.K.; Shin, S.K.; Park, J.C.; Chung, H.S.; Park, J.J.; et al. Is the recent WHO histological classification for gastric cancer helpful for application to endoscopic resection? Gastric Cancer 2016, 19, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.J.; Kim, Y.H.; Kim, J.H.; Kim, H.K.; Kim, H.; Park, J.J.; Youn, Y.H.; Park, H.; Kim, J.W.; Hyung, W.J.; et al. Are new criteria for mixed histology necessary for endoscopic resection in early gastric cancer? Pathol. Res. Pract. 2016, 212, 410–414. [Google Scholar] [CrossRef]
- Bang, C.S.; Park, J.M.; Baik, G.H.; Park, J.J.; Joo, M.K.; Jang, J.Y.; Jeon, S.W.; Choi, S.C.; Sung, J.K.; Cho, K.B. The therapeutic outcomes of endoscopic resection of early gastric cancer with undifferentiated-type histology: A korean ESD registry database analysis. Clin. Endosc. 2017, 50, 569–577. [Google Scholar] [CrossRef]
- Kang Sun, H.; Moon Hee, S.; Sung Jae, K.; Jeong Hyun, Y. Signet ring cell carcinoma of early gastric cancer, is endoscopic treatment really risky? Ann. Oncol. 2017, 96, e7532. [Google Scholar] [CrossRef]
- Lee, I.S.; Lee, S.; Park, Y.S.; Gong, C.S.; Yook, J.H.; Kim, B.S. Applicability of endoscopic submucosal dissection for undifferentiated early gastric cancer: Mixed histology of poorly differentiated adenocarcinoma and signet ring cell carcinoma is a worse predictive factor of nodal metastasis. Surg. Oncol. 2017, 26, 8–12. [Google Scholar] [CrossRef]
- Horiuchi, Y.; Fujisaki, J.; Yamamoto, N.; Ishizuka, N.; Omae, M.; Ishiyama, A.; Yoshio, T.; Hirasawa, T.; Yamamoto, Y.; Nagahama, M.; et al. Mixed poorly differentiated adenocarcinoma in undifferentiated-type early gastric cancer predicts endoscopic noncurative resection. Gastric Cancer 2018, 21, 689–695. [Google Scholar] [CrossRef]
- Kwak, D.S.; Min, Y.W.; Lee, J.H.; Kang, S.H.; Jang, S.H.; Lee, H.; Min, B.H.; Kim, J.J.; Kim, K.M.; Sohn, T.S.; et al. Outcomes of endoscopic submucosal dissection for early gastric cancer with undifferentiated-type histology: A clinical simulation using a non- selected surgical cohort. Gut Liver 2018, 12, 263–270. [Google Scholar] [CrossRef]
- Nakamura, R.; Omori, T.; Mayanagi, S.; Irino, T.; Wada, N.; Kawakubo, H.; Kameyama, K.; Kitagawa, Y. Risk of lymph node metastasis in undifferentiated-type mucosal gastric carcinoma. World J. Surg. Oncol. 2019, 17, 32. [Google Scholar] [CrossRef]
- Ryu, D.G.; Choi, C.W.; Kim, S.J.; Kang, D.H.; Kim, H.W.; Park, S.B.; Nam, H.S. Possible indication of endoscopic resection in undifferentiated early gastric cancer. Sci. Rep. 2019, 9, 16869. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.L.; Shi, H.P.; Beeharry, M.K.; Feng, T.N.; Yan, M.; Yuan, F.; Zhu, Z.-G.; Zhang, B.Y.; Wu, W. Expanding the indication of endoscopic submucosal dissection for undifferentiated early gastric cancer is safe or not? Asian J. Surg. 2020, 43, 526–531. [Google Scholar] [CrossRef]
- Zou, Y.; Wu, L.; Yang, Y.; Shen, X.; Zhu, C. Risk factors of tumor invasion and node metastasis in early gastric cancer with undifferentiated component: A multicenter retrospective study on biopsy specimens and clinical data. Ann. Transl. Med. 2020, 8, 360. [Google Scholar] [CrossRef] [PubMed]
- Zu, H.; Wang, H.; Li, C.; Xue, Y. Clinicopathologic characteristics and prognostic value of various histological types in advanced gastric cancer. Int. J. Clin. Exp. Pathol. 2014, 7, 5692–5700. [Google Scholar] [PubMed]
- Alshehri, A.; Alanezi, H.; Kim, B.S. Prognosis factors of advanced gastric cancer according to sex and age. World J. Clin. Cases 2020, 8, 1608–1619. [Google Scholar] [CrossRef]
- Cho, J.H.; Lim, J.Y.; Choi, A.R.; Choi, S.M.; Kim, J.W.; Choi, S.H.; Cho, J.Y. Comparison of Surgery Plus Chemotherapy and Palliative Chemotherapy Alone for Advanced Gastric Cancer with Krukenberg Tumor. Cancer Res. Treat. 2015, 47, 697–705. [Google Scholar] [CrossRef]
- Men, H.T.; Gou, H.F.; Liu, J.Y.; Li, Q.; Luo, D.Y.; Bi, F.; Qiu, M. Prognostic factors of intraperitoneal chemotherapy for peritoneal carcinomatosis of gastric cancer: A retrospective study from a single center. Oncol. Lett. 2016, 11, 3501–3507. [Google Scholar] [CrossRef]
- Choi, J.H.; Choi, Y.W.; Kang, S.Y.; Jeong, G.S.; Lee, H.W.; Jeong, S.H.; Park, J.S.; Ahn, M.S.; Sheen, S.S. Combination versus single-agent as palliative chemotherapy for gastric cancer. BMC Cancer 2020, 20, 167. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhu, G.; Zhang, H.; Gao, H.; Xue, Y. Clinicopathologic features of gastric carcinoma with signet ring cell histology. J. Gastrointest. Surg. 2010, 14, 601–606. [Google Scholar] [CrossRef]
- Chiu, C.T.; Kuo, C.J.; Yeh, T.S.; Hsu, J.T.; Liu, K.H.; Yeh, C.N.; Hwang, T.L.; Jan, Y.Y.; Lin, C.J. Early signet ring cell gastric cancer. Dig. Dis. Sci. 2011, 56, 1749–1756. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.G.; Wang, Z.N.; Sun, Z.; Liu, F.N.; Yu, M.; Xu, H.M. Clinicopathologic characteristics and prognosis of signet ring cell carcinoma of the stomach: Results from a chinese mono-institutional study. J. Surg. Oncol. 2011, 103, 700–703. [Google Scholar] [CrossRef]
- Lee, H.H.; Song, K.Y.; Park, C.H.; Jeon, H.M. Undifferentiated-type gastric adenocarcinoma: Prognostic impact of three histological types. World J. Surg. Oncol. 2012, 10, 1–8. [Google Scholar] [CrossRef]
- Bu, Z.; Zheng, Z.; Li, Z.; Wu, X.; Zhang, L.; Wu, A.; Zong, X.; Ji, J. Clinicopathological and prognostic differences between mucinous gastric carcinoma and signet-ring cell carcinoma. Chin. J. Cancer Res. 2013, 25, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Zhang, H.; Tian, L.; Zhang, X.; Xue, Y. The difference in clinic-pathological features between signet ring cell carcinoma and gastric mucinous adenocarcinoma. Tumor Biol. 2013, 34, 2625–2631. [Google Scholar] [CrossRef] [PubMed]
- Kwon, K.J.; Shim, K.N.; Song, E.M.; Choi, J.Y.; Kim, S.E.; Jung, H.K.; Jung, S.A. Clinicopathological characteristics and prognosis of signet ring cell carcinoma of the stomach. Gastric Cancer 2014, 17, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Shim, J.H.; Song, K.Y.; Kim, H.H.; Han, S.U.; Kim, M.C.; Hyung, W.J.; Kim, W.; Lee, H.J.; Ryu, S.W.; Cho, G.S.; et al. Signet ring cell histology is not an independent predictor of poor prognosis after curative resection for gastric cancer. Medicine 2014, 93, 1–9. [Google Scholar] [CrossRef]
- Liu, X.; Cai, H.; Sheng, W.; Yu, L.; Long, Z.; Shi, Y.; Wang, Y. Clinicopathological characteristics and survival outcomes of primary signet ring cell carcinoma in the stomach: Retrospective analysis of single center database. PLoS ONE 2015, 10, 1–13. [Google Scholar] [CrossRef]
- Hsu, J.T.; Wang, C.W.; Le, P.H.; Wu, R.C.; Chen, T.H.; Chiang, K.C.; Lin, C.J.; Yeh, T.S. Clinicopathological characteristics and outcomes in stage I-III mucinous gastric adenocarcinoma: A retrospective study at a single medical center. World J. Surg. Oncol. 2016, 14, 1–9. [Google Scholar] [CrossRef]
- Kong, P.; Wu, R.; Yang, C.; Geng, Q.; Liu, J.; Chen, S.; Liu, X.; Ye, M.; He, W.; Yang, Q.; et al. Prognostic impact of the signet ring cell type in node-negative gastric cancer. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef]
- Lu, M.; Yang, Z.; Feng, Q.; Yu, M.; Zhang, Y.; Mao, C.; Shen, L.; Tang, J. The characteristics and prognostic value of signet ring cell histology in gastric cancer: A retrospective cohort study of 2199 consecutive patients. Medicine 2016, 95, e4052. [Google Scholar] [CrossRef]
- Tang, X.; Zhang, J.; Che, X.; Lan, Z.; Chen, Y.; Wang, C. The Clinicopathological Features and Long-Term Survival Outcomes of Mucinous Gastric Carcinoma: A Consecutive Series of 244 Cases from a Single Institute. J. Gastrointest. Surg. 2016, 20, 693–699. [Google Scholar] [CrossRef]
- Wang, Z.; Xu, J.; Shi, Z.; Shen, X.; Luo, T.; Bi, J.; Nie, M. Clinicopathologic characteristics and prognostic of gastric cancer in young patients. Scand. J. Gastroenterol. 2016, 51, 1043–1049. [Google Scholar] [CrossRef]
- Chon, H.J.; Hyung, W.J.; Kim, C.; Park, S.; Kim, J.H.; Park, C.H.; Ahn, J.B.; Kim, H.; Chung, H.C.; Rha, S.Y.; et al. Differential Prognostic Implications of Gastric Signet Ring Cell Carcinoma: Stage Adjusted Analysis From a Single High-volume Center in Asia. Ann. Surg. 2017, 265, 946–953. [Google Scholar] [CrossRef]
- Chen, J.; Cai, R.; Ren, G.; Zhao, J.; Li, H.; Guo, C.; He, W.; Wu, X.; Zhang, W. Differences in clinicopathological characteristics and computed tomography findings between signet ring cell carcinoma and nonsignet ring cell carcinoma in early and advanced gastric cancer. Cancer Med. 2018, 7, 1160–1169. [Google Scholar] [CrossRef]
- Lee, D.; Son, S.Y.; Kim, Y.B.; Han, S.U.; Hur, H. Neural Invasion is a Significant Contributor to Peritoneal Recurrence in Signet Ring Cell Gastric Carcinoma. Ann. Surg. Oncol. 2018, 25, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Kao, Y.C.; Fang, W.L.; Wang, R.F.; Li, A.F.Y.; Yang, M.H.; Wu, C.W.; Shyr, Y.M.; Huang, K.H. Clinicopathological differences in signet ring cell adenocarcinoma between early and advanced gastric cancer. Gastric Cancer 2019, 22, 255–263. [Google Scholar] [CrossRef]
- Ahn, H.; Chung, W.C.; Kim, Y.J.; Ryu, S.; Lim, E. Clinical Outcomes of Mucinous Gastric Carcinomas Compared with Non-mucinous and Signet Ring Cell Carcinomas. Korean J. Gastroenterol. 2020, 76, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.H.; Chen, M.H.; Fang, W.L.; Lin, C.H.; Chao, Y.; Lo, S.S.; Li, A.F.; Wu, C.W.; Shyr, Y.M. The Clinicopathological Characteristics And Genetic Alterations of Signet-ring Cell Carcinoma in Gastric Cancer. Cancers 2020, 12, 2318. [Google Scholar] [CrossRef]
- Wang, J.B.; Lin, M.Q.; Xie, J.W.; Lin, J.X.; Lu, J.; Chen, Q.Y.; Cao, L.L.; Lin, M.; Tu, R.H.; Li, P.; et al. BMI-adjusted prognosis of signet ring cell carcinoma in patients undergoing radical gastrectomy for gastric adenocarcinoma. Asian J. Surg. 2021, 44, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.; Sun, G.; Qu, H.; He, Q.; Hao, Z. Prognostic Significance of Signet-Ring Cell Components in Patients with Gastric Carcinoma of Different Stages. Front. Surg. 2021, 8, 642468. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Wu, W.; Zhao, J.; Song, S.; Zhang, C.; Sun, W.; Lv, B. Clinical Features and Risk Factors for Lymph Node Metastasis in Early Signet Ring Cell Gastric Cancer. Front. Oncol. 2021, 11, 630675. [Google Scholar] [CrossRef]
- Zhao, B.; Lu, H.; Luo, R.; Bao, S.; Mei, D.; Xu, H.; Huang, B. Different clinicopathologic features and prognostic significance of signet ring cell histology in early and locally advanced gastric cancer patients. Clin. Res. Hepatol. Gastroenterol. 2021, 45, 101454. [Google Scholar] [CrossRef]
- Bozkaya, Y.; Erdem, G.U.; Ozdemir, N.Y.; Demirci, N.S.; Hocazade, C.; Yazıcı, O.; Zengin, N. Comparison of clinicopathological and prognostic characteristics in patients with mucinous carcinoma and signet ring cell carcinoma of the stomach. Curr. Med. Res. Opin. 2017, 33, 109–116. [Google Scholar] [CrossRef]
- Gronnier, C.; Messager, M.; Robb, W.B.; Thiebot, T.; Louis, D.; Luc, G.; Piessen, G.; Mariette, C.; Dhari, A.; Regimbeau, J.M.; et al. Is the negative prognostic impact of signet ring cell histology maintained in early gastric adenocarcinoma? Surgery 2013, 154, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, N.; Adenis, A.; Bouche, O.; Duhamel, A.; Heurgue, A.; Leteurtre, E.; Amela, E.; Salleron, J.; Hebbar, M. Signet ring cells and efficacy of first-line chemotherapy in advanced gastric or oesogastric junction adenocarcinoma. Anticancer Res. 2016, 36, 5543–5549. [Google Scholar] [CrossRef] [PubMed]
- Riihimäki, M.; Hemminki, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. Metastatic spread in patients with gastric cancer. Oncotarget 2016, 7, 52307–52316. [Google Scholar] [CrossRef]
- Piessen, G.; Amielh, D.; Messager, M.; Vinatier, E.; Leteurtre, E.; Triboulet, J.P.; Mariette, C. Is pretreatment endoscopic biopsy a good predictor of signet ring cell histology in gastric carcinoma? World J. Surg. 2012, 36, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, T.; Sicic, L.; Blank, S.; Becker, K.; Weichert, W.; Bruckner, T.; Parakonthun, T.; Langer, R.; Büchler, M.W.; Siewert, J.R.; et al. Prognostic value of histopathological regression in 850 neoadjuvantly treated oesophagogastric adenocarcinomas. Br. J. Cancer 2014, 110, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Voron, T.; Messager, M.; Duhamel, A.; Lefevre, J.; Mabrut, J.Y.; Goere, D.; Meunier, B.; Brigand, C.; Hamy, A.; Glehen, O.; et al. Is signet-ring cell carcinoma a specific entity among gastric cancers? Gastric Cancer 2016, 19, 1027–1040. [Google Scholar] [CrossRef]
- Khan, N.; Donohoe, C.L.; Phillips, A.W.; Griffin, S.M.; Reynolds, J.V. Signet ring gastric and esophageal adenocarcinomas: Characteristics and prognostic implications. Dis. Esophagus 2020, 33, doaa016. [Google Scholar] [CrossRef] [PubMed]
- Shridhar, R.; Almhanna, K.; Hoffe, S.E.; Fulp, W.; Weber, J.; Chuong, M.D.; Meredith, K.L. Increased survival associated with surgery and radiation therapy in metastatic gastric cancer: A Surveillance, Epidemiology, and End Results database analysis. Cancer 2013, 119, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Taghavi, S.; Jayarajan, S.N.; Davey, A.; Willis, A.I. Prognostic significance of signet ring gastric cancer. J. Clin. Oncol. 2012, 30, 3493–3498. [Google Scholar] [CrossRef] [PubMed]
- Postlewait, L.M.; Squires, M.H.; Kooby, D.A.; Poultsides, G.A.; Weber, S.M.; Bloomston, M.; Fields, R.C.; Pawlik, T.M.; Votanopoulos, K.I.; Schmidt, C.R.; et al. The Prognostic Value of Signet-Ring Cell Histology in Resected Gastric Adenocarcinoma. Ann. Surg. Oncol. 2015, 22, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Charalampakis, N.; Nogueras González, G.M.; Elimova, E.; Wadhwa, R.; Shiozaki, H.; Shimodaira, Y.; Blum, M.A.; Rogers, J.E.; Harada, K.; Matamoros, A., Jr.; et al. The Proportion of Signet Ring Cell Component in Patients with Localized Gastric Adenocarcinoma Correlates with the Degree of Response to Pre-Operative Chemoradiation. Oncology 2016, 90, 239–247. [Google Scholar] [CrossRef]
- Liu, K.; Wan, J.; Bei, Y.; Chen, X.; Lu, M. Prognostic Impact of Different Histological Types on Gastric Adenocarcinoma: A Surveillance, Epidemiology, and End Results Database Analysis. Pathol. Oncol. Res. 2017, 23, 881–887. [Google Scholar] [CrossRef]
- Luu, C.; Thapa, R.; Woo, K.; Coppola, D.; Almhanna, K.; Pimiento, J.M.; Chen, D.T.; Marquez, D.D.; Hodul, P.J. Does histology really influence gastric cancer prognosis? J. Gastrointest. Oncol. 2017, 8, 1026–1036. [Google Scholar] [CrossRef] [PubMed]
- Benesch, M.G.K.; Mathieson, A. Epidemiology of Signet Ring Cell Adenocarcinomas. Cancers 2020, 12, 1544. [Google Scholar] [CrossRef]
- Tang, C.T.; Chen, Y.; Zeng, C. Prognostic analysis of gastric signet ring cell carcinoma and mucinous carcinoma: A propensity score-matched study and competing risk analysis. Aging 2020, 12, 22059–22077. [Google Scholar] [CrossRef]
- Wei, Q.; Gao, Y.; Qi, C.; Yuan, X.; Li, J.; Xu, Q.; Luo, C.; Chen, L.; Zhuo, W.; Xu, Z.; et al. Clinicopathological Characteristics and Prognosis of Signet Ring Gastric Cancer: A Population-Based Study. Front. Oncol. 2021, 11, 580545. [Google Scholar] [CrossRef]
- Zhao, X.; Li, Y.; Yang, Z.; Zhang, H.; Wang, H.; Lin, J.; Liu, J.; Zhao, Q. Adenocarcinoma with Mixed Subtypes in the Early and Advanced Gastric Cancer. Can. J. Gastroenterol. Hepatol. 2021, 2021, 8497305. [Google Scholar] [CrossRef] [PubMed]
- de Aguiar, V.G.; Segatelli, V.; Macedo, A.L.V.; Goldenberg, A.; Gansl, R.C.; Maluf, F.C.; Usón Junior, P.L.S. Signet ring cell component, not the Lauren subtype, predicts poor survival: An analysis of 198 cases of gastric cancer. Future Oncol. 2019, 15, 401–408. [Google Scholar] [CrossRef]
- Zhang, C.; Liu, R.; Zhang, W.H.; Chen, X.Z.; Liu, K.; Yang, K.; Chen, X.L.; Zhao, L.Y.; Chen, Z.X.; Zhou, Z.G.; et al. Difference Between Signet Ring Cell Gastric Cancers and Non-Signet Ring Cell Gastric Cancers: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 618477. [Google Scholar] [CrossRef]
- Zhao, S.; Lv, L.; Zheng, K.; Tian, Y.; Zheng, J.C.; Jiang, C.G. Prognosis and Biological Behavior of Gastric Signet-Ring Cell Carcinoma Better or Worse: A Meta-Analysis. Front. Oncol. 2021, 11, 603070. [Google Scholar] [CrossRef]
- Zhao, B.; Lv, W.; Zhang, J.; Huang, B.; Lin, J. Different prognostic significance of signet ring cell histology for early and advanced gastric cancer patients: A systematic review and meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2020, 14, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, M.F.; De Paiva, T.F.; Silva, M.J.B.; Benevides, C.F.L.; Guimarães, A.P.G.; Gimenes, D.L.; Pinheiro, E.D.; Rinck, J.A.; Nicolau, U.R.; Sanches, S.M.; et al. Predictors of peritoneal carcinomatosis in patients with gastric cancer treated at a single institution in Brazil. J. Surg. Oncol. 2009, 100, 452–455. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, M.F.; Silva, M.J.B.; De Paiva, T.F.; Chinen, L.T.D.; Guimarães, A.P.G.; Gimenes, D.L.; Pinheiro, E.D.; Rinck, J.A.; Nicolau, U.R.; Sanches, S.M.; et al. Factors correlated with peritoneal carcinomatosis and survival in patients with gastric cancer treated at a single institution in Brazil. Int. J. Clin. Oncol. 2009, 14, 326–331. [Google Scholar] [CrossRef]
- Thomassen, I.; Van Gestel, Y.R.; Van Ramshorst, B.; Luyer, M.D.; Bosscha, K.; Nienhuijs, S.W.; Lemmens, V.E.; De Hingh, I.H. Peritoneal carcinomatosis of gastric origin: A population-based study on incidence, survival and risk factors. Int. J. Cancer 2014, 134, 622–628. [Google Scholar] [CrossRef]
- Rhomberg, W.; Gruber, U. Liver metastasis in cancer of the stomach and its dependence on the histology of the primary tumor: An autopsy study on 102 cases. Clin. Exp. Metastasis 1989, 7, 585–590. [Google Scholar] [CrossRef]
- Honoré, C.; Goéré, D.; Messager, M.; Souadka, A.; Dumont, F.; Piessen, G.; Elias, D.; Mariette, C.; FRENCH, F.W.G. Risk factors of peritoneal recurrence in eso-gastric signet ring cell adenocarcinoma: Results of a multicentre retrospective study. Eur. J. Surg. Oncol. 2013, 39, 235–241. [Google Scholar] [CrossRef]
- Königsrainer, I.; Horvath, P.; Struller, F.; Königsrainer, A.; Beckert, S. Initial clinical experience with cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in signet-ring cell gastric cancer with peritoneal metastases. J. Gastric Cancer 2014, 14, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Nadiradze, G.; Giger-Pabst, U.; Zieren, J.; Strumberg, D.; Solass, W.; Reymond, M.A. Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) with Low-Dose Cisplatin and Doxorubicin in Gastric Peritoneal Metastasis. J. Gastrointest. Surg. 2016, 20, 367–373. [Google Scholar] [CrossRef]
- Mariette, C.; Carneiro, F.; Grabsch, H.I.; van der Post, R.S.; Allum, W.; de Manzoni, G. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer 2019, 22, 1–9. [Google Scholar] [CrossRef]
- Bencivenga, M.; Treppiedi, E.; Dal Cero, M.; Torroni, L.; Verlato, G.; Iglesias, M.; Renaud, F.; Tomezzoli, A.; Castelli, C.; Piessen, G.; et al. The amount of signet ring cells is significantly associated with tumour stage and survival in gastric poorly cohesive tumours. J. Surg. Oncol. 2020, 121, 1084–1089. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Eto, K.; Iwagami, S.; Ogawa, K.; Sawayama, H.; Ishimoto, T.; Iwatsuki, M.; Baba, Y.; Miyamoto, Y.; Yoshida, N.; et al. Clinicopathological characteristics and prognosis of poorly cohesive cell subtype of gastric cancer. Int. J. Clin. Oncol. 2022, 27, e0144420. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Continent | Patients’ Source | Stage | n. SRCC | n. NSRCC | % SRCC | |
|---|---|---|---|---|---|---|---|---|
| 1 | Efared B [22] | 2020 | Africa | Single institution | AGC | 56 | 127 | 31% |
| 2 | Lee JH [23] | 2010 | Asia | Single institution | EGC | 448 | 914 | 33% |
| 3 | Nam MJ [24] | 2010 | Asia | Single institution | EGC | 720 | 1804 | 29% |
| 4 | Kim HM [25] | 2011 | Asia | Single institution | EGC | 419 | 288 | 59% |
| 5 | Tong JH [26] | 2011 | Asia | Single institution | EGC | 102 | 320 | 24% |
| 6 | Huh CW [27] | 2013 | Asia | Single institution | EGC | 696 | 1512 | 32% |
| 7 | Kim BS [28] | 2014 | Asia | Single institution | EGC | 345 | 1705 | 17% |
| 8 | Guo CG [29] | 2015 | Asia | Single institution | EGC | 198 | 869 | 19% |
| 9 | Jin EH [30] | 2015 | Asia | Single institution | EGC | 227 | 877 | 21% |
| 10 | Lee SH [31] | 2015 | Asia | Single institution | EGC | 114 | 582 | 16% |
| 11 | Wang Z [32] | 2015 | Asia | Single institution | EGC | 115 | 219 | 34% |
| 12 | Hwang CS [33] | 2016 | Asia | Single institution | EGC | 233 | 317 | 42% |
| 13 | Imamura T [34] | 2016 | Asia | Single institution | EGC | 190 | 556 | 25% |
| 14 | Kim YH [35] | 2016 | Asia | Single institution | EGC | 927 | 368 | 72% |
| 15 | Yoon HJ [36] | 2016 | Asia | Single institution | EGC | 930 | 2489 | 27% |
| 16 | Bang CS [37] | 2017 | Asia | Single institution | EGC | 89 | 186 | 32% |
| 17 | Kang Sun H [38] | 2017 | Asia | Single institution | EGC | 91 | 731 | 11% |
| 18 | Lee IS [39] | 2017 | Asia | Single institution | EGC | 652 | 1185 | 35% |
| 19 | Horiuchi Y [40] | 2018 | Asia | Single institution | EGC | 129 | 139 | 48% |
| 20 | Kwak DS [41] | 2018 | Asia | Single institution | EGC | 331 | 206 | 62% |
| 21 | Nakamura R [42] | 2019 | Asia | Single institution | EGC | 209 | 117 | 64% |
| 22 | Ryu DG [43] | 2019 | Asia | Single institution | EGC | 233 | 143 | 62% |
| 23 | Zhu ZL [44] | 2020 | Asia | Single institution | EGC | 287 | 230 | 56% |
| 24 | Zou Y [45] | 2020 | Asia | Single institution | EGC | 146 | 177 | 45% |
| 25 | Zu H [46] | 2014 | Asia | Single institution | AGC | 44 | 697 | 6% |
| 26 | Alshehri A [47] | 2020 | Asia | Single institution | AGC | 219 | 1786 | 11% |
| 27 | Cho JH [48] | 2015 | Asia | Single institution | MGC | 111 | 125 | 47% |
| 28 | Men HT [49] | 2016 | Asia | Single institution | MGC | 40 | 17 | 70% |
| 29 | Choi JH [50] | 2020 | Asia | Single institution | MGC | 171 | 516 | 25% |
| 30 | Zhang M [51] | 2010 | Asia | Single institution | All Stages | 218 | 1221 | 15% |
| 31 | Chiu CT [52] | 2011 | Asia | Single institution | All Stages | 505 | 1934 | 21% |
| 32 | Jiang CG [53] | 2011 | Asia | Single institution | All Stages | 211 | 2104 | 9% |
| 33 | Lee HH [54] | 2012 | Asia | Single institution | All Stages | 320 | 1056 | 23% |
| 34 | Bu Z [55] | 2013 | Asia | Single institution | All Stages | 107 | 74 | 59% |
| 35 | Jiang H [56] | 2013 | Asia | Single institution | All Stages | 288 | 80 | 78% |
| 36 | Kwon KJ [57] | 2014 | Asia | Single institution | All Stages | 108 | 661 | 14% |
| 37 | Shim JH [58] | 2014 | Asia | Multicentric | All Stages | 377 | 2266 | 14% |
| 38 | Liu X [59] | 2015 | Asia | Single institution | All Stages | 138 | 1326 | 9% |
| 39 | Hsu JT [60] | 2016 | Asia | Single institution | All Stages | 545 | 925 | 37% |
| 40 | Kong P [61] | 2016 | Asia | Single institution | All Stages | 90 | 390 | 19% |
| 41 | Lu M [62] | 2016 | Asia | Single institution | All Stages | 354 | 1845 | 16% |
| 42 | Tang X [63] | 2016 | Asia | Single institution | All Stages | 260 | 244 | 52% |
| 43 | Wang Z [64] | 2016 | Asia | Single institution | All Stages | 620 | 3310 | 16% |
| 44 | Chon HJ [65] | 2017 | Asia | Single institution | All Stages | 1646 | 6021 | 21% |
| 45 | Chen J [66] | 2018 | Asia | Single institution | All Stages | 62 | 179 | 26% |
| 46 | Lee D [67] | 2018 | Asia | Single institution | All Stages | 176 | 588 | 23% |
| 47 | Kao YC [68] | 2019 | Asia | Single institution | All Stages | 755 | 2216 | 25% |
| 48 | Ahn H [69] | 2020 | Asia | Single institution | All Stages | 200 | 260 | 43% |
| 49 | Huang KH [70] | 2020 | Asia | Single institution | All Stages | 181 | 260 | 41% |
| 50 | Wang JB [71] | 2020 | Asia | Single institution | All Stages | 449 | 2893 | 13% |
| 51 | Dong X [72] | 2021 | Asia | Single institution | All Stages | 254 | 3885 | 6% |
| 52 | Jin X [73] | 2021 | Asia | Single institution | All Stages | 121 | 2045 | 6% |
| 53 | Zhao B [74] | 2021 | Asia | Single institution | All Stages | 235 | 1656 | 12% |
| 54 | Bozkaya Y [75] | 2016 | Asia–Europe | Single institution | All Stages | 142 | 51 | 74% |
| 55 | Gronnier C [76] | 2013 | Europe | Multicentric | EGC | 104 | 317 | 25% |
| 56 | Lemoine N [77] | 2016 | Europe | Multicentric | MGC | 57 | 146 | 28% |
| 57 | Riihimäki M [78] | 2016 | Europe | Swedish registry | MGC | 82 | 736 | 10% |
| 58 | Piessen G [79] | 2012 | Europe | Single institution | All Stages | 96 | 158 | 38% |
| 59 | Heger U [8] | 2014 | Europe | Single institution | All Stages | 235 | 488 | 33% |
| 60 | Schmidt T [80] | 2014 | Europe | Multicentric | All Stages | 221 | 516 | 30% |
| 61 | Voron T [81] | 2016 | Europe | FREGAT | All Stages | 899 | 900 | 50% |
| 62 | Khan N [82] | 2020 | Europe | Multicentric | All stages | 198 | 2302 | 8% |
| 63 | Shridhar R [83] | 2013 | North America | SEER | MGC | 372 | 4200 | 8% |
| 64 | Taghavi S [84] | 2012 | North America | SEER | All Stages | 2666 | 7580 | 26% |
| 65 | Bamboat ZM [6] | 2014 | North America | Single institution | All Stages | 210 | 359 | 37% |
| 66 | Postlewait LM [85] | 2015 | North America | Multicentric | All Stages | 312 | 456 | 41% |
| 67 | Charalampakis N [86] | 2016 | North America | Single institution | All Stages | 62 | 45 | 58% |
| 68 | Liu K [87] | 2017 | North America | SEER | All Stages | 4418 | 14877 | 23% |
| 69 | Luu C [88] | 2017 | North America | Single institution | All Stages | 57 | 153 | 27% |
| 70 | Benesch MGK [89] | 2020 | North America | SEER | All Stages | 17942 | 65218 | 22% |
| 71 | Tang CT [90] | 2020 | North America | SEER | All Stages | 5265 | 752 | 88% |
| 72 | Wei Q [91] | 2020 | North America | SEER | All Stages | 1751 | 7493 | 19% |
| 73 | Zhao X [92] | 2021 | North America | SEER | All Stages | 3006 | 3673 | 45% |
| 74 | de Aguiar VG [93] | 2019 | South America | Single institution | All Stages | 72 | 144 | 33% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dal Cero, M.; Bencivenga, M.; Liu, D.H.W.; Sacco, M.; Alloggio, M.; Kerckhoffs, K.G.P.; Filippini, F.; Saragoni, L.; Iglesias, M.; Tomezzoli, A.; et al. Clinical Features of Gastric Signet Ring Cell Cancer: Results from a Systematic Review and Meta-Analysis. Cancers 2023, 15, 5191. https://doi.org/10.3390/cancers15215191
Dal Cero M, Bencivenga M, Liu DHW, Sacco M, Alloggio M, Kerckhoffs KGP, Filippini F, Saragoni L, Iglesias M, Tomezzoli A, et al. Clinical Features of Gastric Signet Ring Cell Cancer: Results from a Systematic Review and Meta-Analysis. Cancers. 2023; 15(21):5191. https://doi.org/10.3390/cancers15215191
Chicago/Turabian StyleDal Cero, Mariagiulia, Maria Bencivenga, Drolaiz H. W. Liu, Michele Sacco, Mariella Alloggio, Kelly G. P. Kerckhoffs, Federica Filippini, Luca Saragoni, Mar Iglesias, Anna Tomezzoli, and et al. 2023. "Clinical Features of Gastric Signet Ring Cell Cancer: Results from a Systematic Review and Meta-Analysis" Cancers 15, no. 21: 5191. https://doi.org/10.3390/cancers15215191