
Pelvic Exenteration for Recurrent Endometrial Cancer: A 15-Year Monocentric Retrospective Study
 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
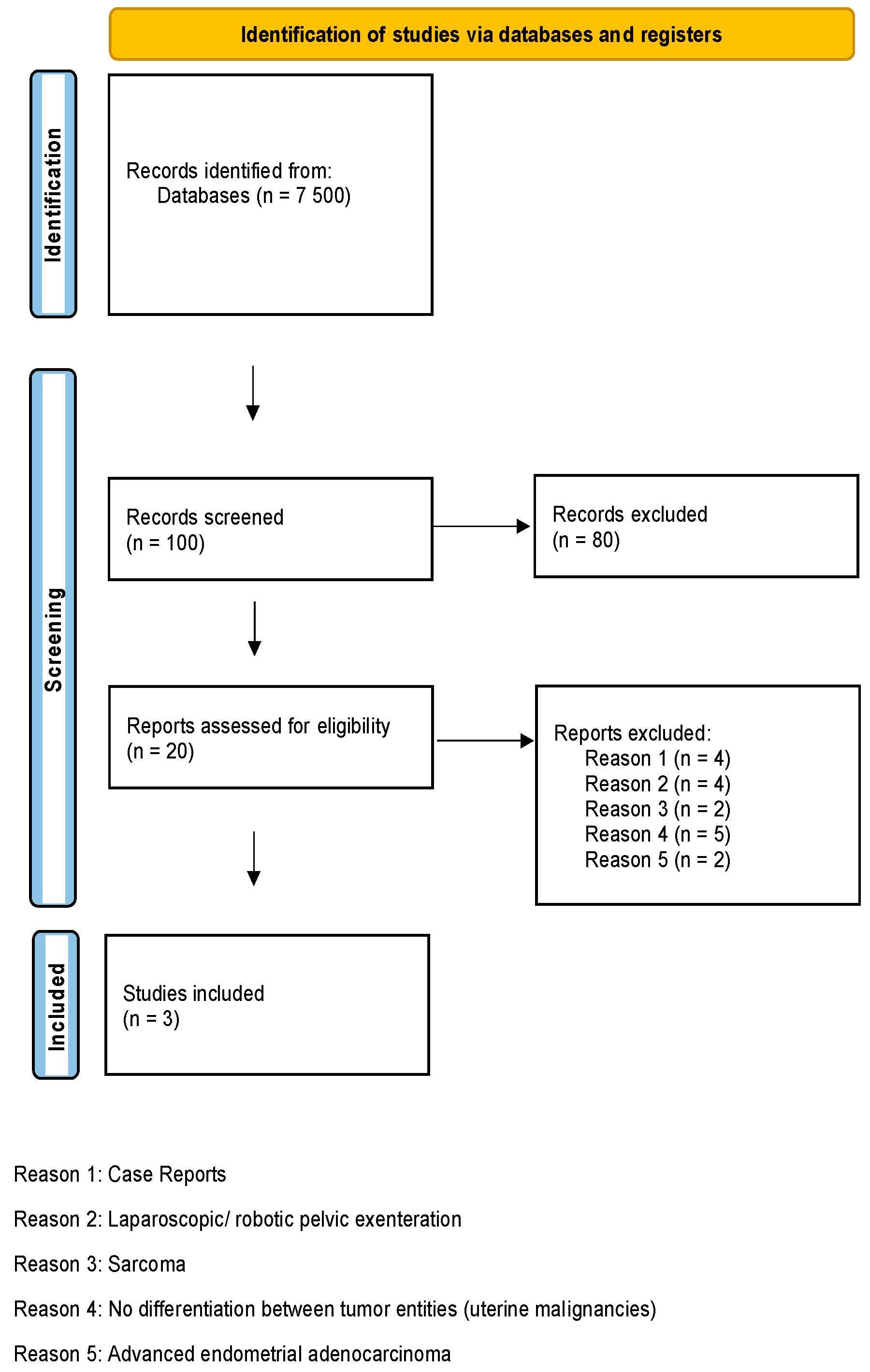
2.2. Literature Review
3. Results
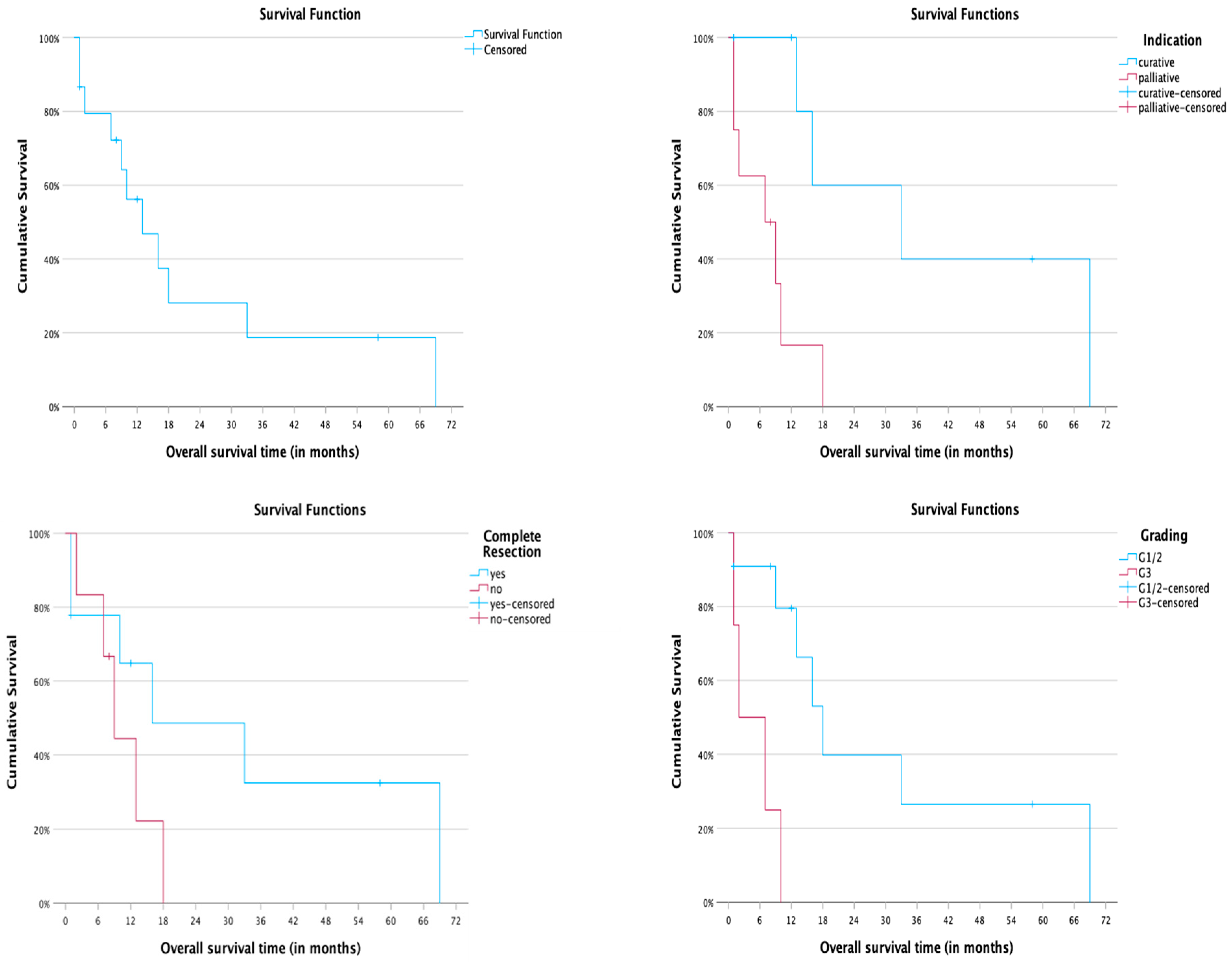
3.1. Data Analysis
3.2. Literature Review
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Independent Variable | Hazard Ratio |
|---|---|
| Age at Surgery | HR = 0.98 [95% CI 0.86–1.12] |
| Indication for Surgery | HR = 7.47 [95% CI 1.47–37.96] |
| Complete Cytoreduction | HR = 0.41 [95% CI 0.11–1.57] |
| Tumor Grading | HR = 8.72 [95% CI 1.54–49.42] |
| Lymphatic Vessel Invasion | HR = 0.04 [95% CI non-applicable] |
| Blood Vessel Invasion | HR = 0.04 [95% CI non-applicable] |
| p53-status | HR = 1.59 [95% CI 0.33–7.55] |
| L1CAM-status | HR = 1.75 [95% CI 0.34–9.13] |
| Age at Surgery | HR = 0.98 [95% CI 0.86–1.12] |
| Indication for Surgery | HR = 7.47 [95% CI 1.47–37.96] |
| Complete Cytoreduction | HR = 0.41 [95% CI 0.11–1.57] |
| Tumor Grading | HR = 8.72 [95% CI 1.54–49.42] |
| Lymphatic Vessel Invasion | HR = 0.04 [95% CI non-applicable] |
| Blood Vessel Invasion | HR = 0.04 [95% CI non-applicable] |
References
- Vermij, L.; Jobsen, J.J.; León-Castillo, A.; Brinkhuis, M.; Roothaan, S.; Powell, M.E.; De Boer, S.M.; Khaw, P.; Mileshkin, L.R.; Fyles, A.; et al. Prognostic refinement of NSMP high-risk endometrial cancers using oestrogen receptor immunohistochemistry. Br. J. Cancer 2023, 128, 1360–1368. [Google Scholar] [CrossRef]
- Gordhandas, S.; Zammarrelli, W.A.; Rios-Doria, E.V.; Green, A.K.; Makker, V. Current evidence-based systemic therapy for advanced and recurrent endometrial cancer. J. Natl. Compr. Cancer Netw. 2023, 21, 217–226. [Google Scholar] [CrossRef]
- Westin, S.N.; Rallapalli, V.; Fellman, B.; Urbauer, D.L.; Pal, N.; Frumovitz, M.M.; Ramondetta, L.M.; Bodurka, D.C.; Ramirez, P.T.; Soliman, P.T. Overall survival after pelvic exenteration for gynecologic malignancy. Gynecol. Oncol. 2014, 134, 546–551. [Google Scholar] [CrossRef]
- Barakat, R.R.; Goldman, N.A.; Patel, D.A.; Venkatraman, E.S.; Curtin, J.P. Pelvic exenteration for recurrent endometrial cancer. Gynecol. Oncol. 1999, 75, 99–102. [Google Scholar] [CrossRef]
- Brunschwig, A. Complete excision of pelvic viscera for advanced carcinoma. A one-stage abdominoperineal operation with end colostomy and bilateral ureteral implantation into the colon above the colostomy. Cancer 1948, 1, 177–183. [Google Scholar] [CrossRef]
- Bacalbasa, N.; Balescu, I.; Vilcu, M.; Neacsu, A.; Dima, S.; Croitoru, A.; Brezean, I. Pelvic exenteration for locally advanced and relapsed pelvic malignancies—An analysis of 100 cases. Vivo 2019, 33, 2205–2210. [Google Scholar] [CrossRef]
- Vigneswaran, H.T.; Schwarzman, L.S.; Madueke, I.C.; David, S.M.; Nordenstam, J.; Moreira, D.; Abern, M.R. Morbidity and mortality of total pelvic exenteration for malignancy in the US. Ann. Surg. Oncol. 2020, 28, 2790–2800. [Google Scholar] [CrossRef]
- Chiantera, V.; Rossi, M.; De Iaco, P.; Koehler, C.; Marnitz, S.; Gallotta, V.; Margariti, A.P.; Parazzini, F.; Scambia, G.; Schneider, A.; et al. Pelvic exenteration for recurrent endometrial adenocarcinoma: A retrospective multi-institutional study about 21 patients. Int. J. Gynecol. Cancer 2014, 24, 880–884. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Research. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Kommoss, S.; McConechy, M.K.; Kommoss, F.; Leung, S.; Bunz, A.; Magrill, J.; Britton, H.; Kommoss, F.; Grevenkamp, F.; Karnezis, A.; et al. Final validation of the ProMisE molecular classifier for endometrial carcinoma in a large population-based case series. Ann. Oncol. 2018, 29, 1180–1188. [Google Scholar] [CrossRef]
- Edmondson, R.J.; Crosbie, E.J.; Nickkho-Amiry, M.; Kaufmann, A.; Stelloo, E.; Nijman, H.W.; Leary, A.; Auguste, A.; Mileshkin, L.; Pollock, P.; et al. Markers of the p53 pathway further refine molecular profiling in high-risk endometrial cancer: A TransPORTEC initiative. Gynecol. Oncol. 2017, 146, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Alexa, M.; Hasenburg, A.; Battista, M.J. The TCGA molecular classification of endometrial cancer and its possible impact on adjuvant treatment decisions. Cancers 2021, 13, 1478. [Google Scholar] [CrossRef] [PubMed]
- Van Gool, I.C.; Stelloo, E.; Nout, R.A.; Nijman, H.W.; Edmondson, R.J.; Church, D.N.; Mackay, H.J.; Leary, A.; Powell, M.E.; Mileshkin, L.; et al. Prognostic significance of L1CAM expression and its association with mutant p53 expression in high-risk endometrial cancer. Mod. Pathol. 2016, 29, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, S.I.; Kim, N.R.; Kim, H.; Kim, H.S.; Chung, H.H.; Kim, J.; Lee, C.; Lee, M. Prognostic significance of L1CAM expression in addition to promise in endometrial cancer. Gynecol. Oncol. 2023, 174, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef]
- Morris, M.; Alvarez, R.D.; Kinney, W.K.; Wilson, T.O. Treatment of recurrent adenocarcinoma of the endometrium with pelvic exenteration. Gynecol. Oncol. 1996, 60, 288–291. [Google Scholar] [CrossRef]
- Schmidt, A.; Imesch, P.; Fink, D.; Egger, H. Pelvic exenterations for advanced and recurrent endometrial cancer: Clinical outcomes of 40 patients. Int. J. Gynecol. Cancer 2016, 26, 716–721. [Google Scholar] [CrossRef]
- Kaur, M.; Joniau, S.; D’Hoore, A.; Van Calster, B.; Van Limbergen, E.; Leunen, K.; Penninckx, F.; Van Poppel, H.; Amant, F.; Vergote, I. Pelvic exenterations for Gynecological malignancies. Int. J. Gynecol. Cancer 2012, 22, 889–896. [Google Scholar] [CrossRef]
- Fotopoulou, C.; Neumann, U.; Kraetschell, R.; Schefold, J.C.; Weidemann, H.; Lichtenegger, W.; Sehouli, J. Long-term clinical outcome of pelvic exenteration in patients with advanced gynecological malignancies. J. Surg. Oncol. 2010, 101, 507–512. [Google Scholar] [CrossRef]
- Benn, T.; Brooks, R.; Zhang, Q.; Powell, M.; Thaker, P.; Mutch, D.; Zighelboim, I. Pelvic exenteration in gynecologic oncology: A single institution study over 20 years. Gynecol. Oncol. 2011, 122, 14–18. [Google Scholar] [CrossRef]
- de Wilt, J.H.; van Leeuwen, D.H.; Logmans, A.; Verhoef, C.; Kirkels, W.J.; Vermaas, M.; Ansink, A.C. Pelvic exenteration for primary and recurrent gynaecological malignancies. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 134, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Margolis, B.; Kim, S.W.; Chi, D.S. Long-term survival after anterior pelvic exenteration and total vaginectomy for recurrent endometrial carcinoma with metastatic inguinal nodes at the time of surgery. Gynecol. Oncol. Rep. 2017, 19, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Kojima, M.; Soeda, S.; Okabe, C.; Sato, T.; Kamo, N.; Ueda, M.; Endo, Y.; Nomura, S.; Tokuda, E.; Furukawa, S.; et al. Successful management of pelvic recurrence of MSI-high endometrial cancer by total pelvic exenteration followed by administration of pembrolizumab: A case report. Fukushima J. Med. Sci. 2022, 68, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Mäenpää, J.U.; Kangasniemi, K.; Luukkaala, T. Pelvic exenteration for gynecological malignancies: An analysis of 15 cases operated on at a single institution. Acta Obstet. Gynecol. Scand. 2010, 89, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Ang, C.; Bryant, A.; Barton, D.P.; Pomel, C.; Naik, R. Exenterative surgery for recurrent gynaecological malignancies. Cochrane Database Syst. Rev. 2014, 2014, CD010449. [Google Scholar] [CrossRef]
- Barlin, J.N.; Puri, I.; Bristow, R.E. Cytoreductive surgery for advanced or recurrent endometrial cancer: A meta-analysis. Gynecol. Oncol. 2010, 118, 14–18. [Google Scholar] [CrossRef]
- Moukarzel, L.A.; Braxton, K.F.; Zhou, Q.C.; Nobre, S.P.; Iasonos, A.; Alektiar, K.M.; Tew, W.P.; Abu-Rustum, N.R.; Leitao Jr, M.M.; Chi, D.S.; et al. Non-exenterative surgical management of recurrent endometrial carcinoma. Gynecol. Oncol. 2021, 162, 268–276. [Google Scholar] [CrossRef]
- PelvEx Collaborative. Simultaneous pelvic exenteration and liver resection for primary rectal cancer with synchronous liver metastases: Results from the PelvEx collaborative. Color. Dis. 2020, 22, 1216. [Google Scholar] [CrossRef]
- Shine, R.J.; Glyn, T.; Frizelle, F. Pelvic exenteration: A review of current issues/controversies. ANZ J. Surg. 2022, 92, 2822–2828. [Google Scholar] [CrossRef]
- Lee, P.; Francis, K.E.; Solomon, M.J.; Ramsey-Stewart, G.; Austin, K.K.; Koh, C. Triangle of Marcille: The anatomical gateway to lateral pelvic exenteration. ANZ J. Surg. 2016, 87, 582–586. [Google Scholar] [CrossRef]
- Daix, M.; Martinez Gomez, C.; Angeles, M.A.; Tock, S.; Gladieff, L.; Gabiache, E.; Mery, E.; Martinez, A.; Cibula, D.; Ferron, G. Extended pelvic resection for gynecological malignancies: A review of out-of-the-box surgery. Gynecol. Oncol. 2022, 165, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Vizzielli, G.; Naik, R.; Dostalek, L.; Bizzarri, N.; Kucukmetin, A.; Tinelli, G.; Scambia, G.; Cibula, D. Laterally extended pelvic resection for gynaecological malignancies: A multicentric experience with out-of-the-Box surgery. Ann. Surg. Oncol. 2018, 26, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M. Ultra-radical compartmentalized surgery in gynaecological oncology. Eur. J. Surg. Oncol. 2006, 32, 859–865. [Google Scholar] [CrossRef]
- Khoury-Collado, F.; Einstein, M.H.; Bochner, B.H.; Alektiar, K.M.; Sonoda, Y.; Abu-Rustum, N.R.; Brown, C.L.; Gardner, G.J.; Barakat, R.R.; Chi, D.S. Pelvic exenteration with curative intent for recurrent uterine malignancies. Gynecol. Oncol. 2012, 124, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Di Donato, V.; D’Oria, O.; Giannini, A.; Bogani, G.; Fischetti, M.; Santangelo, G.; Tomao, F.; Palaia, I.; Perniola, G.; Muzii, L.; et al. Age-adjusted charlson comorbidity index predicts survival in endometrial cancer patients. Gynecol. Obstet. Investig. 2022, 87, 191–199. [Google Scholar] [CrossRef]
- Roos, E.J.; de Graeff, A.; van Eijkeren, M.A.; Boon, T.A.; Heintz, A.P. Quality of life after pelvic exenteration. Gynecol. Oncol. 2004, 93, 610–614. [Google Scholar] [CrossRef]
- Fernandes, A.; Bryan, S.; Kolomainen, D.; Phipps, R.; Power, K.; Thompson, A.; Barton, D. What is life like after pelvic exenteration? The longitudinal assessment of quality of life after pelvic exenteration for recurrent/persistent gynaecological cancer. Gynaecol. Cancer 2019, 29, A34. [Google Scholar] [CrossRef]
- Ter Glane, L.; Hegele, A.; Wagner, U.; Boekhoff, J. Pelvic exenteration for recurrent or advanced gynecologic malignancies—Analysis of outcome and complications. Gynecol. Oncol. Rep. 2021, 36, 100757. [Google Scholar] [CrossRef]
- Makker, V.; Colombo, N.; Herráez, A.C.; Monk, B.J.; Mackay, H.; Santin, A.D.; Miller, D.S.; Moore, R.G.; Baron-Hay, S.; Ray-Coquard, I.; et al. Lenvatinib plus Pembrolizumab in previously treated advanced endometrial cancer: Updated efficacy and safety from the randomized phase III study 309/KEYNOTE-775. J. Clin. Oncol. 2023, 41, 2904–2910. [Google Scholar] [CrossRef]
- El-ghazzi, N.; Durando, X.; Giro, A.; Herrmann, T. Targeted treatment of advanced endometrial cancer: Focus on Pembrolizumab. OncoTargets Ther. 2023, 16, 359–369. [Google Scholar] [CrossRef]
- PelvEx Collaborative. Palliative pelvic exenteration: A systematic review of patient-centered outcomes. Eur. J. Surg. Oncol. 2019, 45, 1787–1795. [Google Scholar] [CrossRef] [PubMed]




| Patient | Age at Surgery (Years) | PE | Initial Treatment | Initial FIGO-Stage | Risk Group * | Recurrence | Indication | Grading | Complete Cytoreduction | LVI | BVI | p53 | L1CAM | Complications (Clavien–Dindo) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | 72 | Total | S 1 + RT 2 | II | High-intermediate | Second | Curative | G2 | R0 | L1 | V1 | M | − | 1 |
| 2. | 63 | Total | S 1 + RCT 4 | IB | Intermediate | First | Curative | G2 | R1 | LX | VX | M | + | 1 |
| 3. | 67 | Posterior | S 1 + RT 2 | II | High-intermediate | Second | Curative | G2 | R0 | LX | VX | WT | − | 1 |
| 4. | 66 | Total | S 1 + RCT 4 | Unk. | Unk. | Fourth | Palliative | G2 | R0 | L0 | V0 | WT | − | 5 |
| 5. | 66 | Total | S 1 + RT 2 | Unk. | Unk. | Second | Curative | G2 | R0 | L0 | V0 | WT | − | 3b |
| 6. | 60 | Anterior | S 1 + RT 2 | II | High-intermediate | First | Curative | G2 | R0 | L0 | V0 | WT | − | 2 |
| 7. | 61 | Anterior | S 1 + RCT 4 | II | High-intermediate | First | Curative | G2 | R0 | L0 | V0 | WT | − | 1 |
| 8. | 65 | Posterior | S 1 | IA | Low | First | Palliative | G2 | R1 | LX | VX | WT | − | 1 |
| 9. | 64 | Total | S 1 + RCT 4 | II | High-intermediate | First | Curative | G2 | R0 | L0 | V0 | WT | − | 1 |
| 10. | 70 | Total | S 1 + CT 3 | IVA | High | First | Palliative | G3 | R1 | L0 | V0 | WT | − | 5 |
| 11. | 74 | Total | S 1 + RCT 4 | IA | Intermediate | Third | Palliative | G3 | R0 | LX | VX | WT | − | 5 |
| 12. | 54 | Posterior | S 1 + CT 3 | IA | Intermediate | First | Palliative | G3 | R1 | L0 | V0 | WT | − | 2 |
| 13. | 67 | Total | S 1 | IA | Low | First | Palliative | G1 | R1 | L0 | V0 | WT | − | 3b |
| 14. | 63 | Total | S 1 | III | High | First | Palliative | G3 | R0 | L0 | V0 | M | + | 2 |
| 15. | 76 | Anterior | S 1 + CT 3 | III | High | First | Palliative | G2 | R1 | L0 | V0 | Unk. | Unk. | 2 |
| Number | Author | Year | Study Design | N | Mean Age (Years) | Complication Rate | Overall Survival Rates at 5 Years |
|---|---|---|---|---|---|---|---|
| 1 | Chiantera et al. [8] | 2014 | retrospective | 21 | 66 | 43% | 40% |
| 2 | Barakat et al. [4] | 1999 | retrospective | 44 | 60 | 80% | 20% |
| 3 | Morris et al. [16] | 1996 | retrospective | 20 | 65 | 60% | 56% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fix, N.; Classen-von Spee, S.; Baransi, S.; Luengas-Würzinger, V.; Rawert, F.; Lippert, R.; Mallmann, P.; Lampe, B. Pelvic Exenteration for Recurrent Endometrial Cancer: A 15-Year Monocentric Retrospective Study. Cancers 2023, 15, 4725. https://doi.org/10.3390/cancers15194725
Fix N, Classen-von Spee S, Baransi S, Luengas-Würzinger V, Rawert F, Lippert R, Mallmann P, Lampe B. Pelvic Exenteration for Recurrent Endometrial Cancer: A 15-Year Monocentric Retrospective Study. Cancers. 2023; 15(19):4725. https://doi.org/10.3390/cancers15194725
Chicago/Turabian StyleFix, Nando, Sabrina Classen-von Spee, Saher Baransi, Verónica Luengas-Würzinger, Friederike Rawert, Ruth Lippert, Peter Mallmann, and Björn Lampe. 2023. "Pelvic Exenteration for Recurrent Endometrial Cancer: A 15-Year Monocentric Retrospective Study" Cancers 15, no. 19: 4725. https://doi.org/10.3390/cancers15194725