
Neo-Adjuvant Treatment in Primary Resectable Pancreatic Cancer: A Systematic Review and PRISMA-Compliant Updated Metanalysis of Oncological Outcomes
 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Data Extraction
- Study characteristics: first author, year, country, observation period, and study design.
- Sample size: total, NAT, and US sample size, respectively.
- Patients’ demographic characteristics: gender and age.
- Primary outcome: survival data (OS and DFS).
- Secondary outcome: R0 resection rate and positive lymph node rate (N+).
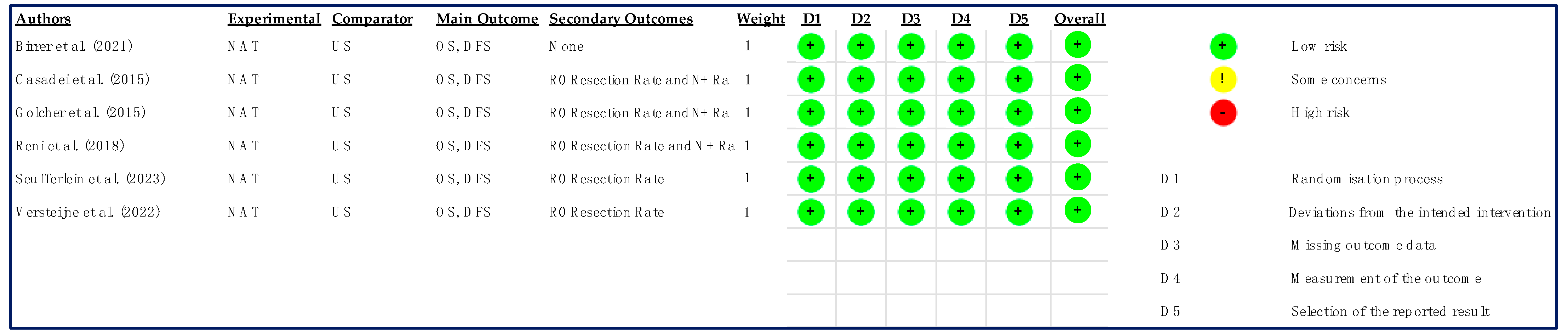
2.4. Risk of Bias—Quality Assessment
2.5. Statistical Analysis
3. Results
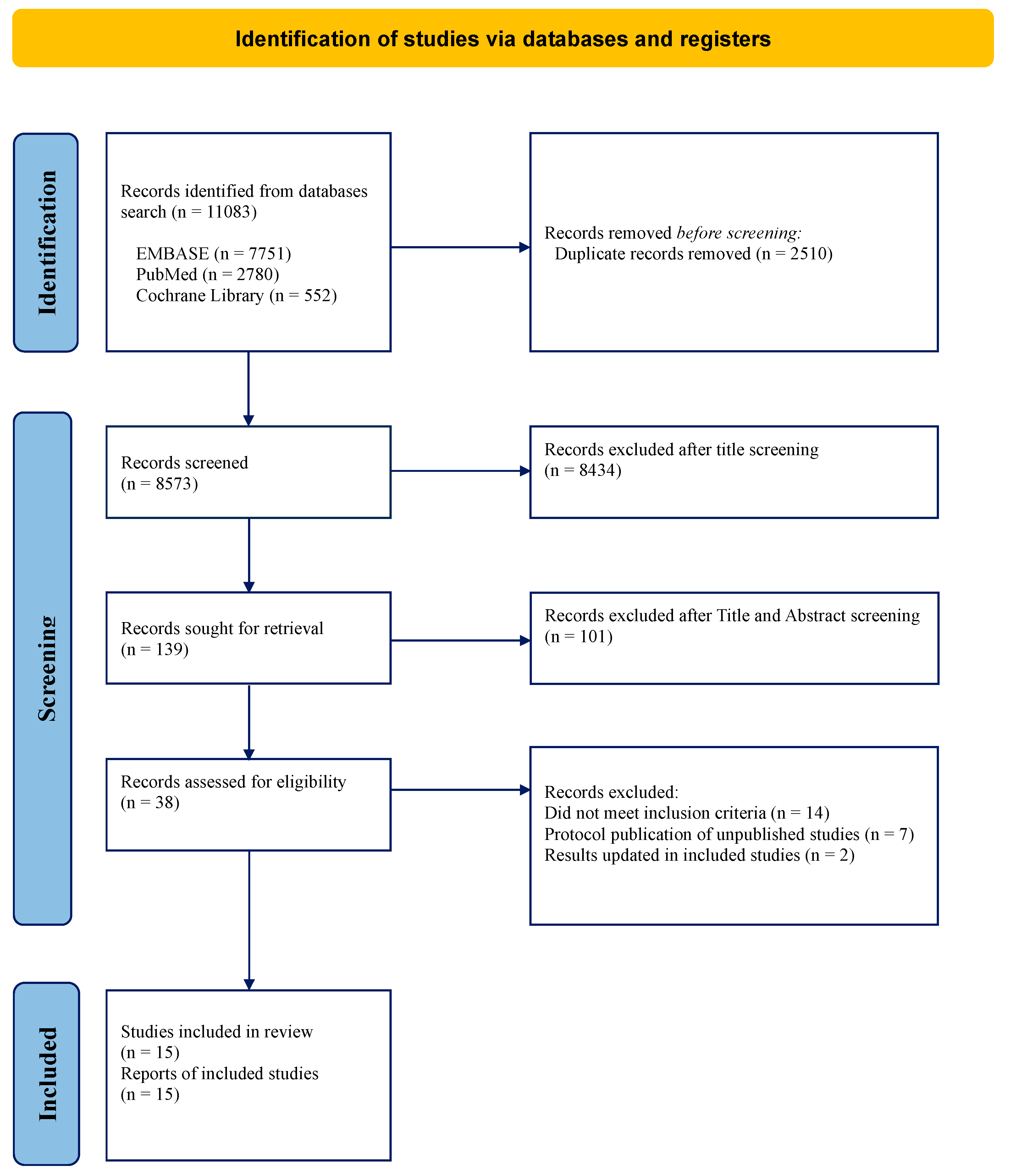
3.1. Search Results and Studies Characteristics
3.2. Studies Characteristics
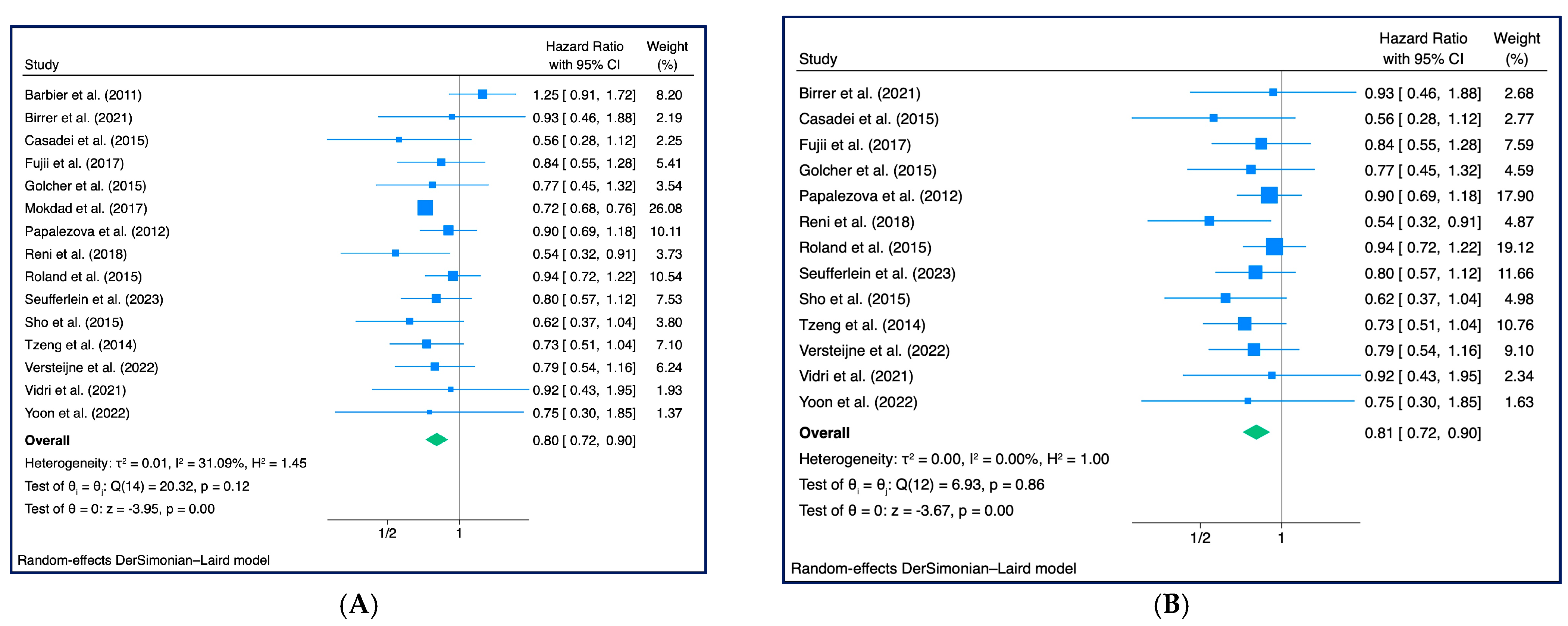
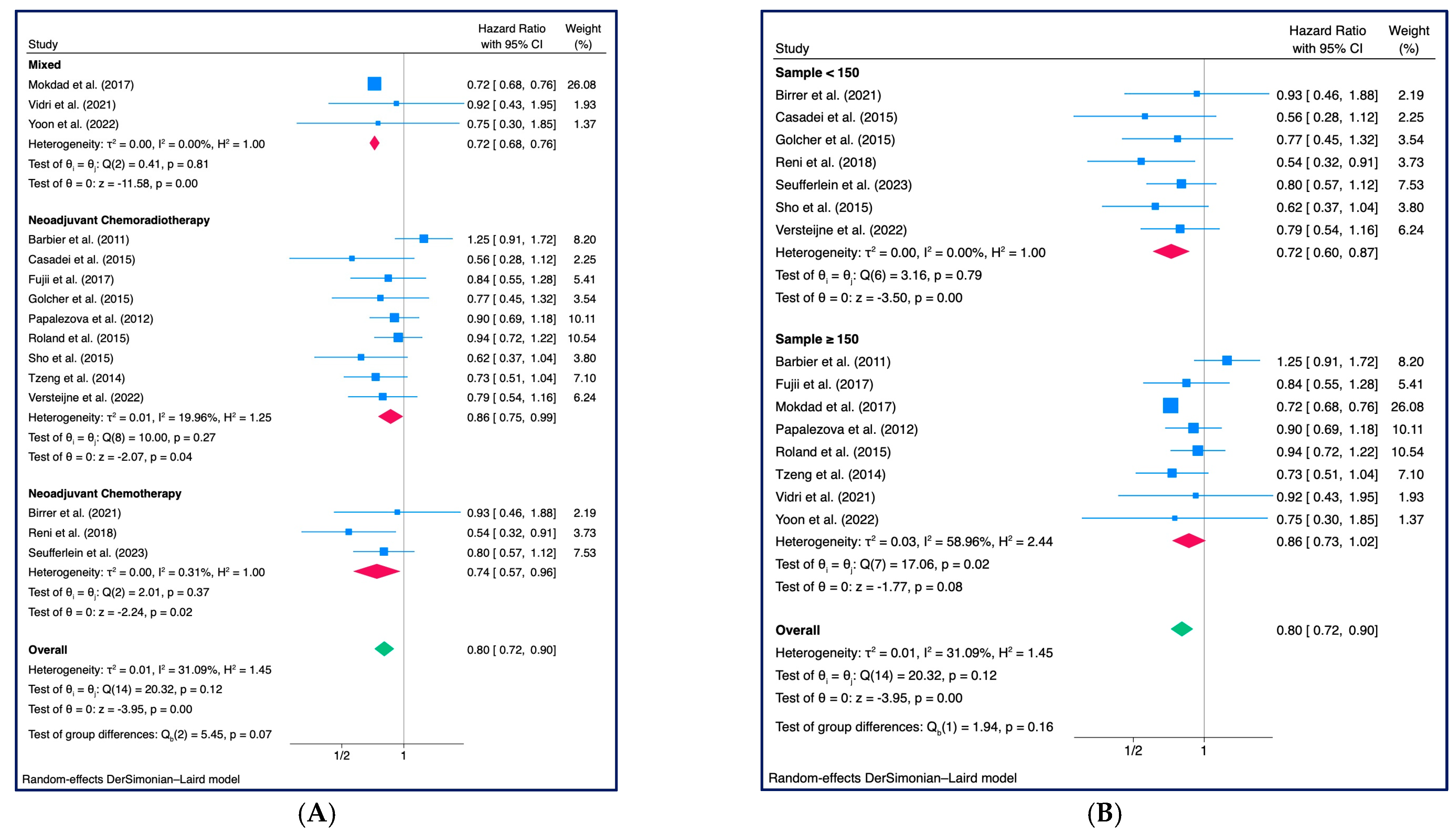
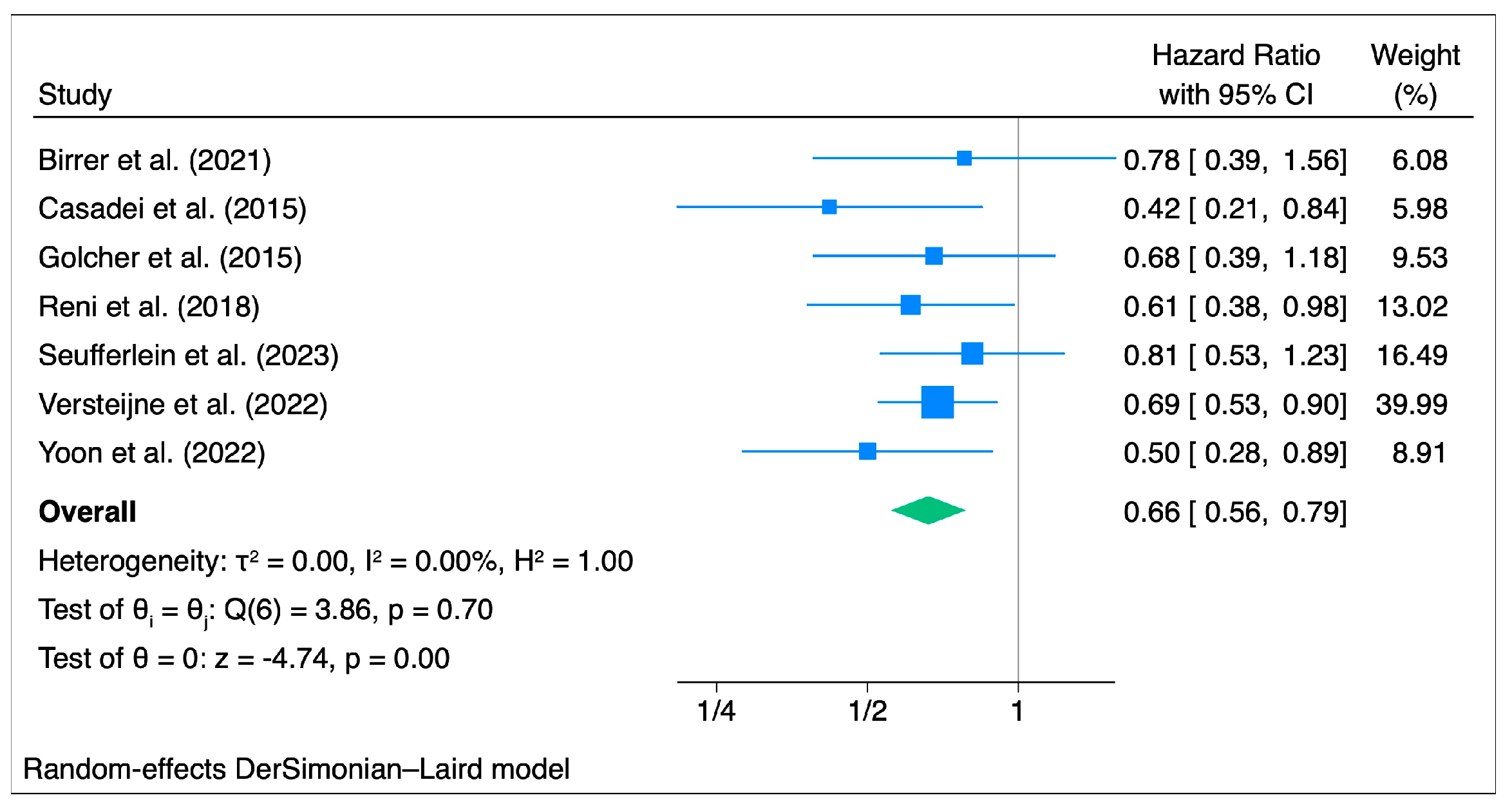
3.3. Overall Survival
3.4. Disease-Free Survival
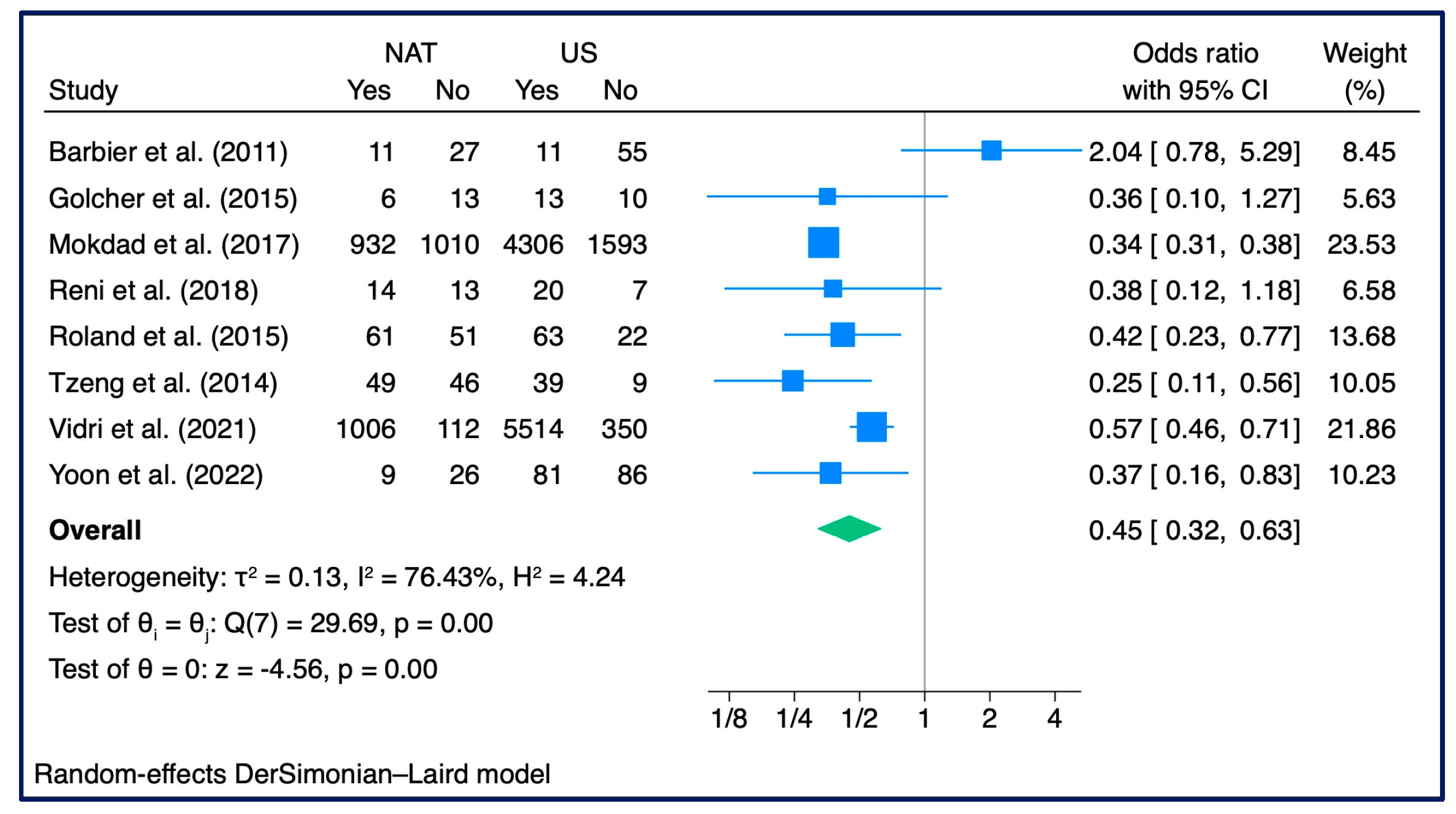
3.5. R0 Resection Rate
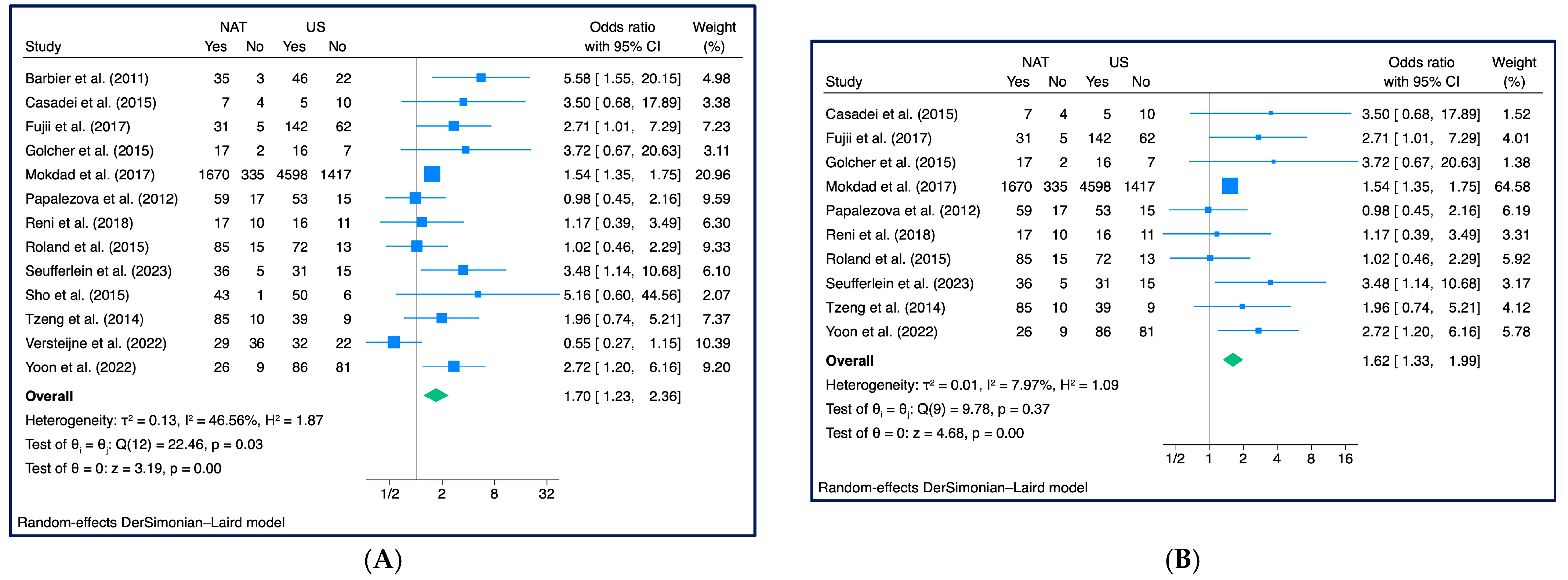
3.6. N+ Rate
4. Discussion
5. Conclusions and Future Directions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.J.; Wong, M.C.S. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Rahib, L.; Smith, B.D.; Aizenberg, R.; Rosenzweig, A.B.; Fleshman, J.M.; Matrisian, L.M. Projecting cancer incidence and deaths to 2030: The unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014, 74, 2913–2921. [Google Scholar] [CrossRef]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Behrman, S.W.; Benson, A.B.; Cardin, D.B.; Chiorean, E.G.; Chung, V.; Czito, B.; Del Chiaro, M.; et al. Pancreatic Adenocarcinoma, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc Netw. 2021, 19, 439–457. [Google Scholar] [CrossRef] [PubMed]
- Al-Hawary, M.M.; Francis, I.R.; Chari, S.T.; Fishman, E.K.; Hough, D.M.; Lu, D.S.; Macari, M.; Megibow, A.J.; Miller, F.H.; Mortele, K.J.; et al. Pancreatic ductal adenocarcinoma radiology reporting template: Consensus statement of the society of abdominal radiology and the american pancreatic association. Gastroenterology 2014, 146, 291–304.e291. [Google Scholar] [CrossRef] [PubMed]
- Raut, C.P.; Tseng, J.F.; Sun, C.C.; Wang, H.; Wolff, R.A.; Crane, C.H.; Hwang, R.; Vauthey, J.N.; Abdalla, E.K.; Lee, J.E.; et al. Impact of resection status on pattern of failure and survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann. Surg. 2007, 246, 52–60. [Google Scholar] [CrossRef]
- Weyhe, D.; Obonyo, D.; Uslar, V.N.; Stricker, I.; Tannapfel, A. Predictive factors for long-term survival after surgery for pancreatic ductal adenocarcinoma: Making a case for standardized reporting of the resection margin using certified cancer center data. PLoS ONE 2021, 16, e0248633. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouché, O.; Guimbaud, R.; Bécouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardière, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef]
- Neoptolemos, J.; Palmer, D.; Ghaneh, P.; Valle, J.W.; Cunningham, D.; Wadsley, J.; Meyer, T.; Anthoney, A.; Glimelius, B.; Falk, S.; et al. ESPAC-4: A multicenter, international, open label randomized controlled phase III trial of adjuvant combination chemotherapy of gemcitabine (GEM) and capecitabine (CAP), versus monotherapy gemcitabine in patients with resected pancreatic ductal adenocarcinoma. Pancreatology 2016, 16, S63. [Google Scholar]
- Neoptolemos, J.P.; Palmer, D.H.; Ghaneh, P.; Psarelli, E.E.; Valle, J.W.; Halloran, C.M.; Faluyi, O.; O’Reilly, D.A.; Cunningham, D.; Wadsley, J.; et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet 2017, 389, 1011–1024. [Google Scholar] [CrossRef]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zülke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef] [PubMed]
- Altman, A.M.; Wirth, K.; Marmor, S.; Lou, E.; Chang, K.; Hui, J.Y.C.; Tuttle, T.M.; Jensen, E.H.; Denbo, J.W. Completion of Adjuvant Chemotherapy After Upfront Surgical Resection for Pancreatic Cancer Is Uncommon Yet Associated With Improved Survival. Ann. Surg. Oncol. 2019, 26, 4108–4116. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Bentrem, D.J.; Ko, C.Y.; Tomlinson, J.S.; Stewart, A.K.; Winchester, D.P.; Talamonti, M.S. Multimodality therapy for pancreatic cancer in the U.S.: Utilization, outcomes, and the effect of hospital volume. Cancer 2007, 110, 1227–1234. [Google Scholar] [CrossRef]
- Aloia, T.A.; Lee, J.E.; Vauthey, J.N.; Abdalla, E.K.; Wolff, R.A.; Varadhachary, G.R.; Abbruzzese, J.L.; Crane, C.H.; Evans, D.B.; Pisters, P.W. Delayed recovery after pancreaticoduodenectomy: A major factor impairing the delivery of adjuvant therapy? J. Am. Coll. Surg. 2007, 204, 347–355. [Google Scholar] [CrossRef]
- Exarchakou, A.; Papacleovoulou, G.; Rous, B.; Magadi, W.; Rachet, B.; Neoptolemos, J.P.; Coleman, M.P. Pancreatic cancer incidence and survival and the role of specialist centres in resection rates in England, 2000 to 2014: A population-based study. Pancreatology 2020, 20, 454–461. [Google Scholar] [CrossRef]
- Li, Q.; Feng, Z.; Miao, R.; Liu, X.; Liu, C.; Liu, Z. Prognosis and survival analysis of patients with pancreatic cancer: Retrospective experience of a single institution. World J. Surg. Oncol. 2022, 20, 11. [Google Scholar] [CrossRef]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef]
- Versteijne, E.; van Dam, J.L.; Suker, M.; Janssen, Q.P.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; et al. Neoadjuvant Chemoradiotherapy Versus Upfront Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Long-Term Results of the Dutch Randomized PREOPANC Trial. J. Clin. Oncol. 2022, 40, 1220–1230. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Ghanem, I.; Lora, D.; Herradón, N.; de Velasco, G.; Carretero-González, A.; Jiménez-Varas, M.; Vázquez de Parga, P.; Feliu, J. Neoadjuvant chemotherapy with or without radiotherapy versus upfront surgery for resectable pancreatic adenocarcinoma: A meta-analysis of randomized clinical trials. ESMO Open 2022, 7, 100485. [Google Scholar] [CrossRef]
- Ye, M.; Zhang, Q.; Chen, Y.; Fu, Q.; Li, X.; Bai, X.; Liang, T. Neoadjuvant chemotherapy for primary resectable pancreatic cancer: A systematic review and meta-analysis. HPB 2020, 22, 821–832. [Google Scholar] [CrossRef]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Updated guidance for trusted systematic reviews: A new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst. Rev. 2019, 10, Ed000142. [Google Scholar] [CrossRef]
- Sanderson, S.; Tatt, I.D.; Higgins, J.P. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: A systematic review and annotated bibliography. Int. J. Epidemiol. 2007, 36, 666–676. [Google Scholar] [CrossRef] [PubMed]
- Deeks, J.J.; Higgins, J.P.T.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane, 2022; Available online: www.training.cochrane.org/handbook (accessed on 29 August 2023).
- Barbier, L.; Turrini, O.; Grégoire, E.; Viret, F.; Le Treut, Y.P.; Delpero, J.R. Pancreatic head resectable adenocarcinoma: Preoperative chemoradiation improves local control but does not affect survival. HPB 2011, 13, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Birrer, D.L.; Golcher, H.; Casadei, R.; Haile, S.R.; Fritsch, R.; Hussung, S.; Brunner, T.B.; Fietkau, R.; Meyer, T.; Grutzmann, R.; et al. Neoadjuvant Therapy for Resectable Pancreatic Cancer: A New Standard of Care. Pooled Data From 3 Randomized Controlled Trials. Ann. Surg. 2021, 274, 713–720. [Google Scholar] [CrossRef]
- Casadei, R.; Di Marco, M.; Ricci, C.; Santini, D.; Serra, C.; Calculli, L.; D’Ambra, M.; Guido, A.; Morselli-Labate, A.M.; Minni, F. Neoadjuvant Chemoradiotherapy and Surgery Versus Surgery Alone in Resectable Pancreatic Cancer: A Single-Center Prospective, Randomized, Controlled Trial Which Failed to Achieve Accrual Targets. J. Gastrointest. Surg. 2015, 19, 1802–1812. [Google Scholar] [CrossRef]
- Fujii, T.; Satoi, S.; Yamada, S.; Murotani, K.; Yanagimoto, H.; Takami, H.; Yamamoto, T.; Kanda, M.; Yamaki, S.; Hirooka, S.; et al. Clinical benefits of neoadjuvant chemoradiotherapy for adenocarcinoma of the pancreatic head: An observational study using inverse probability of treatment weighting. J. Gastroenterol. 2017, 52, 81–93. [Google Scholar] [CrossRef] [PubMed]
- Golcher, H.; Brunner, T.B.; Witzigmann, H.; Marti, L.; Bechstein, W.O.; Bruns, C.; Jungnickel, H.; Schreiber, S.; Grabenbauer, G.G.; Meyer, T.; et al. Neoadjuvant chemoradiation therapy with gemcitabine/cisplatin and surgery versus immediate surgery in resectable pancreatic cancer: Results of the first prospective randomized phase II trial. Strahlenther. Onkol. 2015, 191, 7–16. [Google Scholar] [CrossRef]
- Mokdad, A.A.; Minter, R.M.; Zhu, H.; Augustine, M.M.; Porembka, M.R.; Wang, S.C.; Yopp, A.C.; Mansour, J.C.; Choti, M.A.; Polanco, P.M. Neoadjuvant Therapy Followed by Resection Versus Upfront Resection for Resectable Pancreatic Cancer: A Propensity Score Matched Analysis. J. Clin. Oncol. 2017, 35, 515–522. [Google Scholar] [CrossRef]
- Papalezova, K.T.; Tyler, D.S.; Blazer, D.G., 3rd; Clary, B.M.; Czito, B.G.; Hurwitz, H.I.; Uronis, H.E.; Pappas, T.N.; Willett, C.G.; White, R.R. Does preoperative therapy optimize outcomes in patients with resectable pancreatic cancer? J. Surg. Oncol. 2012, 106, 111–118. [Google Scholar] [CrossRef]
- Reni, M.; Balzano, G.; Zanon, S.; Zerbi, A.; Rimassa, L.; Castoldi, R.; Pinelli, D.; Mosconi, S.; Doglioni, C.; Chiaravalli, M.; et al. Safety and efficacy of preoperative or postoperative chemotherapy for resectable pancreatic adenocarcinoma (PACT-15): A randomised, open-label, phase 2-3 trial. Lancet Gastroenterol. Hepatol. 2018, 3, 413–423. [Google Scholar] [CrossRef] [PubMed]
- Roland, C.L.; Yang, A.D.; Katz, M.H.; Chatterjee, D.; Wang, H.; Lin, H.; Vauthey, J.N.; Pisters, P.W.; Varadhachary, G.R.; Wolff, R.A.; et al. Neoadjuvant therapy is associated with a reduced lymph node ratio in patients with potentially resectable pancreatic cancer. Ann. Surg. Oncol. 2015, 22, 1168–1175. [Google Scholar] [CrossRef] [PubMed]
- Seufferlein, T.; Uhl, W.; Kornmann, M.; Algül, H.; Friess, H.; König, A.; Ghadimi, M.; Gallmeier, E.; Bartsch, D.K.; Lutz, M.P.; et al. Perioperative or only adjuvant gemcitabine plus nab-paclitaxel for resectable pancreatic cancer (NEONAX)-a randomized phase II trial of the AIO pancreatic cancer group. Ann. Oncol. 2023, 34, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Sho, M.; Akahori, T.; Tanaka, T.; Kinoshita, S.; Nagai, M.; Tamamoto, T.; Ohbayashi, C.; Hasegawa, M.; Kichikawa, K.; Nakajima, Y. Importance of resectability status in neoadjuvant treatment for pancreatic cancer. J. Hepatobiliary Pancreat. Sci. 2015, 22, 563–570. [Google Scholar] [CrossRef]
- Tzeng, C.W.; Tran Cao, H.S.; Lee, J.E.; Pisters, P.W.; Varadhachary, G.R.; Wolff, R.A.; Abbruzzese, J.L.; Crane, C.H.; Evans, D.B.; Wang, H.; et al. Treatment sequencing for resectable pancreatic cancer: Influence of early metastases and surgical complications on multimodality therapy completion and survival. J. Gastrointest. Surg. 2014, 18, 16–24, discussion 24-15. [Google Scholar] [CrossRef] [PubMed]
- Vidri, R.J.; Olsen, W.T.; Clark, D.E.; Fitzgerald, T.L. Upfront resection versus neoadjuvant therapy for T1/T2 pancreatic cancer. HPB 2021, 23, 279–289. [Google Scholar] [CrossRef]
- Yoon, M.S.; Lee, H.S.; Kang, C.M.; Lee, W.J.; Keum, J.; Sung, M.J.; Kim, S.S.; Park, M.S.; Jo, J.H.; Chung, M.J.; et al. Response to Neoadjuvant Therapy and Prognosis in Patients with Resectable Pancreatic Cancer: A Propensity Score Matching Analysis. Gut Liver 2022, 16, 118–128. [Google Scholar] [CrossRef]
- Sohal, D.P.S.; Duong, M.; Ahmad, S.A.; Gandhi, N.S.; Beg, M.S.; Wang-Gillam, A.; Wade, J.L., 3rd; Chiorean, E.G.; Guthrie, K.A.; Lowy, A.M.; et al. Efficacy of Perioperative Chemotherapy for Resectable Pancreatic Adenocarcinoma: A Phase 2 Randomized Clinical Trial. JAMA Oncol. 2021, 7, 421–427. [Google Scholar] [CrossRef]
- Uson Junior, P.L.S.; Dias, E.S.D.; de Castro, N.M.; da Silva Victor, E.; Rother, E.T.; Araújo, S.E.A.; Borad, M.J.; Moura, F. Does neoadjuvant treatment in resectable pancreatic cancer improve overall survival? A systematic review and meta-analysis of randomized controlled trials. ESMO Open 2023, 8, 100771. [Google Scholar] [CrossRef]
- Casadei, R.; Di Marco, M.; Ricci, C.; Santini, D.; Serra, C.; Calculli, L.; D’Ambra, M.; Guido, A.; Morselli-Labate, A.M.; Minni, F. Neoadjuvant chemoradiotherapy and surgery versus surgery alone in resectable pancreatic cancer: Long term follow-up results from a single-center prospective, randomized, controlled trial. Tumori 2015, 106, 1802–1812. [Google Scholar]
- Satoi, S.; Unno, M.; Motoi, F.; Matsuyama, Y.; Matsumoto, I.; Aosasa, S.; Shirakawa, H.; Wada, K.; Fujii, T.; Yoshitomi, H.; et al. The effect of neoadjuvant chemotherapy with gemcitabine and S-1 for resectable pancreatic cancer (randomized phase II/III trial; Prep-02/JSAP-05). J. Clin. Oncol. 2019, 37, 4126. [Google Scholar] [CrossRef]
- Janssen, Q.P.; van Dam, J.L.; Bonsing, B.A.; Bos, H.; Bosscha, K.P.; Coene, P.; van Eijck, C.H.J.; de Hingh, I.; Karsten, T.M.; van der Kolk, M.B.; et al. Total neoadjuvant FOLFIRINOX versus neoadjuvant gemcitabine-based chemoradiotherapy and adjuvant gemcitabine for resectable and borderline resectable pancreatic cancer (PREOPANC-2 trial): Study protocol for a nationwide multicenter randomized controlled trial. BMC Cancer 2021, 21, 300. [Google Scholar] [CrossRef]
- Groot, V.P.; Mosier, S.; Javed, A.A.; Teinor, J.A.; Gemenetzis, G.; Ding, D.; Haley, L.M.; Yu, J.; Burkhart, R.A.; Hasanain, A.; et al. Circulating Tumor DNA as a Clinical Test in Resected Pancreatic Cancer. Clin. Cancer Res. 2019, 25, 4973–4984. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Is the Case Definition Adequate? | Representativeness of the Cases | Selection of Controls | Definition of Controls | Comparability of Cases and Controls on the Basis of the Design or Analysis | Ascertainment of Exposure | Same Method of Ascertainment for Cases and Controls | Non-Response Rate | Total Score |
|---|---|---|---|---|---|---|---|---|---|
| Barbier et al. (2011) [25] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Fujii et al. (2017) [28] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 7 |
| Mokdad et al. (2017) [30] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 7 |
| Papalezova et al. (2012) [31] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 1 | 8 |
| Roland et al. (2015) [33] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 6 |
| Sho et al. (2015) [35] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 0 | 7 |
| Tzeng et al. (2014) [36] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 1 | 8 |
| Vidri et al. (2021) [37] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 1 | 8 |
| Yoon et al. (2022) [38] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 1 | 8 |
| Author | Country | Period | Multicenter Study | Study Design | Sample | Median OS | ||
|---|---|---|---|---|---|---|---|---|
| Total | NAT | US | ||||||
| Barbier et al. (2011) [25] | France | 1997–2006 | No | Retrospective Study | 173 | 88 | 85 | NAT: 15 mo (3–72) |
| US: 17 mo (1–109) | ||||||||
| Birrer et al. (2021) [26] | Switzerland | 2009–2018 | No | RCT | 34 | 16 | 18 | NR |
| Casadei et al. (2015) [27] | Italy | 2007–2014 | No | RCT | 38 | 18 | 20 | NAT: 22.4 mo (10.2–34.6) |
| US: 19.5 mo (7.5–31.5) | ||||||||
| Fujii et al. (2017) [28] | Japan | 2001–2013 | Yes | NR | 273 | 40 | 233 | NAT: 24.9 mo |
| US: 23.5 mo | ||||||||
| Golcher et al. (2015) [29] | Germany | 2003–2009 | Yes | RCT | 66 | 33 | 33 | NAT: 17.4 mo |
| US: 17.4 mo | ||||||||
| Mokdad et al. (2017) [30] | USA | 2006–2012 | No | NR | 8020 | 2005 | 6015 | NAT: 26 mo |
| US: 21 mo | ||||||||
| Papalezova et al. (2012) [31] | USA | 1999–2007 | No | Retrospective Study | 236 | 144 | 92 | NAT: 15 mo |
| US: 13 mo | ||||||||
| Reni et al. (2018) [32] | Italy | 2010–2015 | No | RCT | 62 | 32 | 30 | NAT: 38.2 mo (27.3–49.1) |
| US: 26.4 mo (15.8–26.7) | ||||||||
| Roland et al. (2015) [33] | USA | 1990–2008 | No | Retrospective Study | 307 | 222 | 85 | NR |
| NR | ||||||||
| Seufferlein et al. (2023) [34] | Germany | 2015–2019 | Yes | RCT | 118 | 59 | 59 | NAT: 25.5 mo (19.7–29.7) |
| US: 16.7 mo (11.6–22.2) | ||||||||
| Sho et al. (2015) [35] | Japan | 2006–2013 | No | Retrospective Study | 100 | 44 | 56 | NAT: 50.2 mo |
| US: 32.7 mo | ||||||||
| Tzeng et al. (2014) [36] | USA | 2002–2007 | No | Retrospective Study | 167 | 115 | 52 | NAT: 28 mo (21.7–34.3) |
| US: 25.3 mo (19.9–30.7) | ||||||||
| Versteijne et al. (2022) [18] | Netherlands | 2013–2017 | Yes | RCT | 133 | 65 | 68 | NAT: 15.7 mo (12.9–20.6) |
| US: 14.3 mo (12.7–17.9) | ||||||||
| Vidri et al. (2021) [37] | USA | 1989–2021 | Yes | Retrospective Study | 6802 | 1118 | 5684 | NAT: 27.6 mo (IQR: 38.8) |
| US: 25.6 mo (IQR: 40.9) | ||||||||
| Yoon et al. (2022) [38] | Korea | 2012–2019 | No | Retrospective Study | 202 | 167 | 35 | NR |
| NR | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roesel, R.; Deantonio, L.; Bernardi, L.; Garo, M.L.; Majno-Hurst, P.; Vannelli, A.; Cefalì, M.; Palmarocchi, M.C.; Valli, M.C.; Pesola, G.; et al. Neo-Adjuvant Treatment in Primary Resectable Pancreatic Cancer: A Systematic Review and PRISMA-Compliant Updated Metanalysis of Oncological Outcomes. Cancers 2023, 15, 4627. https://doi.org/10.3390/cancers15184627
Roesel R, Deantonio L, Bernardi L, Garo ML, Majno-Hurst P, Vannelli A, Cefalì M, Palmarocchi MC, Valli MC, Pesola G, et al. Neo-Adjuvant Treatment in Primary Resectable Pancreatic Cancer: A Systematic Review and PRISMA-Compliant Updated Metanalysis of Oncological Outcomes. Cancers. 2023; 15(18):4627. https://doi.org/10.3390/cancers15184627
Chicago/Turabian StyleRoesel, Raffaello, Letizia Deantonio, Lorenzo Bernardi, Maria Luisa Garo, Pietro Majno-Hurst, Alberto Vannelli, Marco Cefalì, Maria Celeste Palmarocchi, Maria Carla Valli, Guido Pesola, and et al. 2023. "Neo-Adjuvant Treatment in Primary Resectable Pancreatic Cancer: A Systematic Review and PRISMA-Compliant Updated Metanalysis of Oncological Outcomes" Cancers 15, no. 18: 4627. https://doi.org/10.3390/cancers15184627