Squamous Cell Carcinoma of the Oral Cavity, Oropharynx, and Larynx: A Scoping Review of Treatment Guidelines Worldwide

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methodology
2.1. Information Sources and Search
2.2. Selection of Sources of Evidence
2.3. Eligibility Criteria
2.4. Data Synthesis and Descriptive Analysis
3. Results
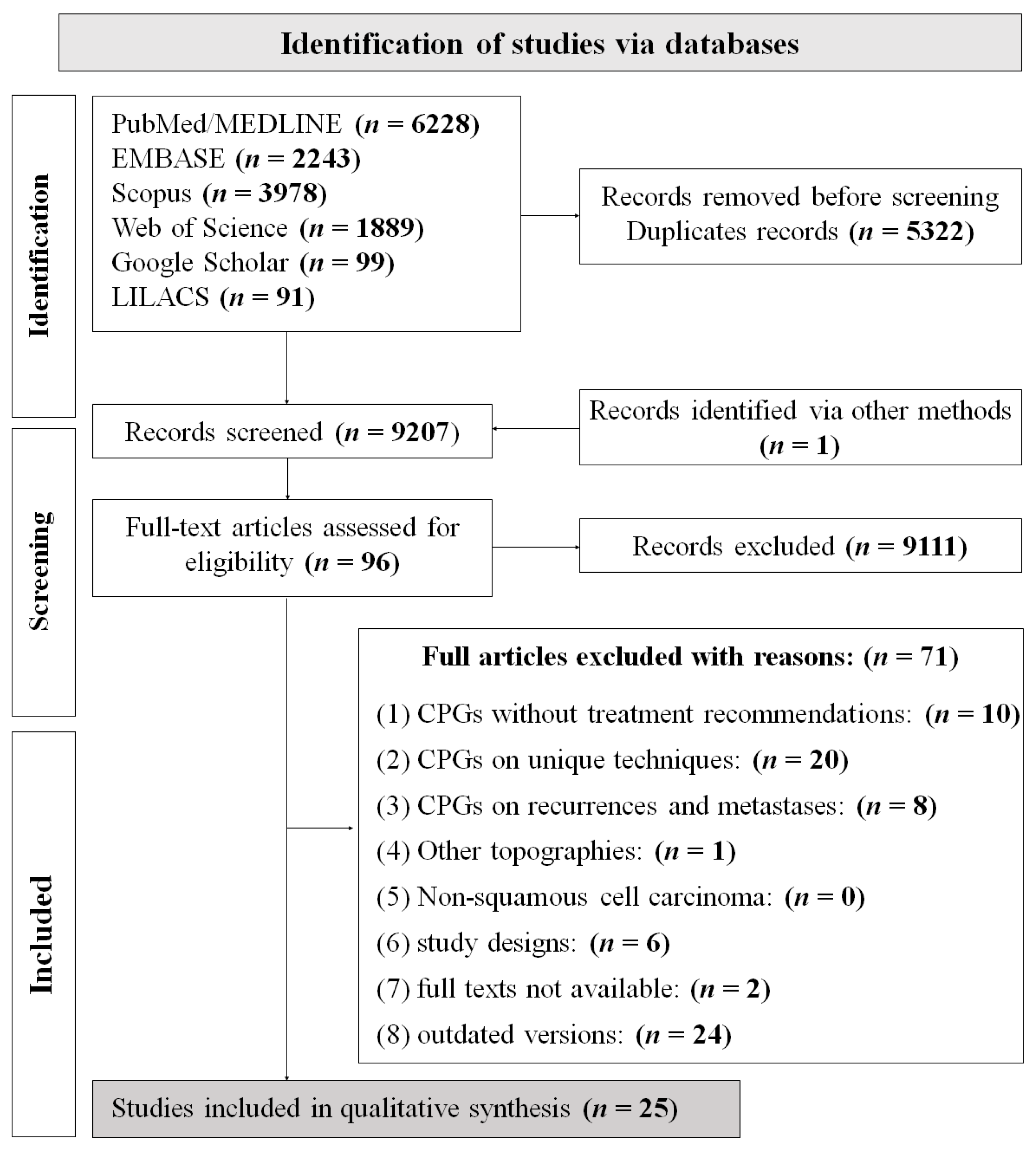
3.1. Selection of Sources of Evidence
3.2. Guideline Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Correction Statement
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Goyal, N.; Hennessy, M.; Lehman, E.; Lin, W.; Agudo, A.; Ahrens, W.; Boccia, S.; Brennan, P.; Brenner, H.; Cadoni, G.; et al. Risk factors for head and neck cancer in more and less developed countries: Analysis from the INHANCE consortium. Oral. Dis. 2023, 29, 1565–1578. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Anzai, Y.; Brizel, D.M.; Bruce, J.Y.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. Head and Neck Cancers, Version 2.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 873–898. [Google Scholar] [CrossRef]
- Hajmohammadi, E.; Molaei, T.; Mowlaei, S.H.; Alam, M.; Abbasi, K.; Khayatan, D.; Rahbar, M.; Tebyanian, H. Sonodynamic therapy and common head and neck cancers: In vitro and in vivo studies. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 5113–5121. [Google Scholar] [CrossRef] [PubMed]
- Mosaddad, S.A.; Mahootchi, P.; Rastegar, Z.; Abbasi, B.; Alam, M.; Abbasi, K.; Fani-Hanifeh, S.; Amookhteh, S.; Sadeghi, S.; Soufdoost, R.S.; et al. Photodynamic Therapy in Oral Cancer: A Narrative Review. Photobiomodul Photomed. Laser Surg. 2023, 41, 248–264. [Google Scholar] [CrossRef]
- De Felice, F.; Tombolini, V.; Valentini, V.; de Vincentiis, M.; Mezi, S.; Brugnoletti, O.; Polimeni, A. Advances in the Management of HPV-Related Oropharyngeal Cancer. J. Oncol. 2019, 2019, 9173729. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R.; Carrasco-Labra, A.; Guyatt, G.H. How to Interpret and Use a Clinical Practice Guideline or Recommendation: Users’ Guides to the Medical Literature. JAMA 2021, 326, 1516–1523. [Google Scholar] [CrossRef]
- Dykewicz, C.A.; Centers for Disease Control and Prevention (U.S.); Infectious Diseases Society of America; American Society of Blood and Marrow Transplantation. Summary of the Guidelines for Preventing Opportunistic Infections among Hematopoietic Stem Cell Transplant Recipients. Clin. Infect. Dis. 2001, 33, 139–144. [Google Scholar] [CrossRef]
- Lang, K.; Menzin, J.; Earle, C.C.; Jacobson, J.; Hsu, M.A. The economic cost of squamous cell cancer of the head and neck: Findings from linked SEER-Medicare data. Arch. Otolaryngol. Head. Neck Surg. 2004, 130, 1269–1275. [Google Scholar] [CrossRef]
- Fagan, J.J. Africa: A window on challenges and opportunities for head and neck cancer. Laryngoscope Investig. Otolaryngol. 2021, 6, 414–419. [Google Scholar] [CrossRef]
- Paleri, V.; Roland, N. Introduction to the United Kingdom National Multidisciplinary Guidelines for Head and Neck Cancer. J. Laryngol. Otol. 2016, 130, S3–S4. [Google Scholar] [CrossRef]
- Machiels, J.P.; René Leemans, C.; Golusinski, W.; Grau, C.; Licitra, L.; Gregoire, V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1462–1475. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Caudell, J.J.; Gillison, M.L.; Maghami, E.; Spencer, S.; Pfister, D.G.; Adkins, D.; Birkeland, A.C.; Brizel, D.M.; Busse, P.M.; Cmelak, A.J.; et al. NCCN Guidelines® Insights: Head and Neck Cancers, Version 1.2022. J. Natl. Compr. Cancer Netw. 2022, 20, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Chinese Society of Clinical Oncology (CSCO) Diagnosis and Treatment Guidelines for Head and Neck Cancer Working Group. Chinese Society of Clinical Oncology (CSCO) diagnosis and treatment guidelines for head and neck cancer 2018 (English version). Chin. J. Cancer Res. 2019, 31, 84–98. [Google Scholar] [CrossRef] [PubMed]
- Beitler, J.J.; Quon, H.; Jones, C.U.; Salama, J.K.; Busse, P.M.; Cooper, J.S.; Koyfman, S.A.; Ridge, J.A.; Saba, N.F.; Siddiqui, F.; et al. ACR Appropriateness Criteria(®) Locoregional therapy for resectable oropharyngeal squamous cell carcinomas. Head. Neck 2016, 38, 1299–1309. [Google Scholar] [CrossRef]
- Bilde, A.; von Buchwald, C.; Johansen, J.; Bastholt, L.; Sørensen, J.A.; Marker, P.; Krogdahl, A.; Hansen, H.S.; Specht, L.; Kirkegaard, J.; et al. The Danish national guidelines for treatment of oral squamous cell carcinoma. Acta Oncol. 2006, 45, 294–299. [Google Scholar] [CrossRef]
- Bootz, F. Guideline on diagnosis, treatment, and follow-up of laryngeal cancer. Best. Pract. Onkol. 2020, 15, 430–438. [Google Scholar] [CrossRef]
- Cervenka, B.; Pipkorn, P.; Fagan, J.; Zafereo, M.; Aswani, J.; Macharia, C.; Kundiona, I.; Mashamba, V.; Zender, C.; Moore, M. Oral cavity cancer management guidelines for low-resource regions. Head. Neck 2019, 41, 799–812. [Google Scholar] [CrossRef]
- Chaturvedi, P.; Prabhash, K.; Babu, G.; Kuriakose, M.; Birur, P.; Anand, A.; Kaushal, A.; Mahajan, A.; Syiemlieh, J.; Singhal, M.; et al. Indian clinical practice consensus guidelines for the management of oral cavity cancer. Indian. J. Cancer 2020, 57, S6–S8. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, A.; Lin, T.; Anand, A.K.; Atmakusuma, D.; Calaguas, M.J.; Chitapanarux, I.; Cho, B.C.; Goh, B.C.; Guo, Y.; Hsieh, W.S.; et al. Consensus recommendations for management of head and neck cancer in Asian countries: A review of international guidelines. Oral. Oncol. 2013, 49, 872–877. [Google Scholar] [CrossRef]
- D’Cruz, A.K.; Sharma, S.; Agarwal, J.P.; Thakar, A.; Teli, A.; Arya, S.; Desai, C.; Chaturvedi, P.; Sebastian, P.; Verghese, B.T.; et al. Indian Council of Medical Research consensus document for the management of tongue cancer. Indian. J. Med. Paediatr. Oncol. 2015, 36, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Ismaila, N.; Lewin, J.S.; Nathan, C.A.; Adelstein, D.J.; Eisbruch, A.; Fass, G.; Fisher, S.G.; Laurie, S.A.; Le, Q.T.; et al. Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1143–1169. [Google Scholar] [CrossRef]
- Jones, T.M.; De, M.; Foran, B.; Harrington, K.; Mortimore, S. Laryngeal cancer: United Kingdom National Multidisciplinary guidelines. J. Laryngol. Otol. 2016, 130, S75–S82. [Google Scholar] [CrossRef] [PubMed]
- Kaanders, J.H.; Hordijk, G.J. Dutch Cooperative Head and Neck Oncology Group. Carcinoma of the larynx: The Dutch national guideline for diagnostics, treatment, supportive care and rehabilitation. Radiother. Oncol. 2002, 63, 299–307. [Google Scholar] [CrossRef]
- Keam, B.; Machiels, J.P.; Kim, H.R.; Licitra, L.; Golusinski, W.; Gregoire, V.; Lee, Y.G.; Belka, C.; Guo, Y.; Rajappa, S.J.; et al. Pan-Asian adaptation of the EHNS-ESMO-ESTRO Clinical Practice Guidelines for the diagnosis, treatment and follow-up of patients with squamous cell carcinoma of the head and neck. ESMO Open 2021, 6, 100309. [Google Scholar] [CrossRef]
- Kerawala, C.; Roques, T.; Jeannon, J.P.; Bisase, B. Oral cavity and lip cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S83–S89. [Google Scholar] [CrossRef]
- Manos, M.; Giralt, J.; Rueda, A.; Cabrera, J.; Martinez-Trufero, J.; Marruecos, J.; Lopez-Pousa, A.; Rodrigo, J.P.; Castelo, B.; Martinez-Galan, J.; et al. Multidisciplinary management of head and neck cancer: First expert consensus using Delphi methodology from the Spanish Society for Head and Neck Cancer (part 1). Oral. Oncol. 2017, 70, 58–64. [Google Scholar] [CrossRef]
- Mehanna, H.; Evans, M.; Beasley, M.; Chatterjee, S.; Dilkes, M.; Homer, J.; O’Hara, J.; Robinson, M.; Shaw, R.; Sloan, P. Oropharyngeal cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S90–S96. [Google Scholar] [CrossRef]
- Mesia, R.; Iglesias, L.; Lambea, J.; Martinez-Trufero, J.; Soria, A.; Taberna, M.; Trigo, J.; Chaves, M.; Garcia-Castano, A.; Cruz, J. SEOM clinical guidelines for the treatment of head and neck cancer (2020). Clin. Transl. Oncol. 2021, 23, 913–921. [Google Scholar] [CrossRef]
- National Collaborating Centre for Cancer (UK). Cancer of the upper Aerodigestive Tract: Assessment and Management in People Aged 16 and Over; National Institute for Health and Care Excellence (NICE): London, UK, 2018; Volume NICE Guideline, No. 36. [Google Scholar]
- Nibu, K.; Hayashi, R.; Asakage, T.; Ojiri, H.; Kimata, Y.; Kodaira, T.; Nagao, T.; Nakashima, T.; Fujii, T.; Fujii, H.; et al. Japanese Clinical Practice Guideline for Head and Neck Cancer. Auris Nasus Larynx 2017, 44, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Paleri, V.; Kerawala, C.; Winter, S.; Robinson, M.; Jarrom, D.; Prettyjohns, M. Upper aerodigestive tract cancer: Summary of the National Institute for Health and Care Excellence guidelines for England and Wales. Clin. Otolaryngol. 2017, 42, 3–10. [Google Scholar] [CrossRef]
- Prabhash, K.; Babu, G.; Chaturvedi, P.; Kuriakose, M.; Birur, P.; Anand, A.; Kaushal, A.; Mahajan, A.; Syiemlieh, J.; Singhal, M.; et al. Indian clinical practice consensus guidelines for the management of oropharyngeal cancer. Indian. J. Cancer 2020, 57, S12–S15. [Google Scholar] [CrossRef] [PubMed]
- Ridge, J.A.; Lawson, J.; Yom, S.S.; Garg, M.K.; McDonald, M.W.; Quon, H.; Saba, N.; Salama, J.K.; Smith, R.V.; Worden, F.; et al. American College of Radiology Appropriateness Criteria(®) treatment of stage I T1 glottic cancer. Head. Neck 2014, 36, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Ridley, M.B. Clinical Practice Guidelines for Malignancies of the Head and Neck Larynx, Oropharynx, and Oral Cavity. Cancer Control 1996, 3, 442–444. [Google Scholar] [CrossRef]
- Singhal, M.; Prabhash, K.; Babu, G.; Chaturvedi, P.; Kuriakose, M.; Birur, P.; Anand, A.; Kaushal, A.; Mahajan, A.; Syiemlieh, J.; et al. Indian clinical practice consensus guidelines for the management of laryngeal cancer. Indian. J. Cancer 2020, 57, S19–S21. [Google Scholar] [CrossRef]
- Yoo, J.; Lacchetti, C.; Hammond, J.A.; Gilbert, R.W. Role of endolaryngeal surgery (with or without laser) compared with radiotherapy in the management of early (T1) glottic cancer: A clinical practice guideline. Curr. Oncol. 2013, 20, 132–135. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Prabhash, K.; Babu, G.; Chaturvedi, P.; Kuriakose, M.; Birur, P.; Anand, A.; Kaushal, A.; Mahajan, A.; Syiemlieh, J.; Singhal, M.; et al. Indian clinical practice consensus guidelines for the management of squamous cell carcinoma of head and neck. Indian. J. Cancer 2020, 57, S1–S5. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C. AJCC Cancer Staging Manual; Springer International Publishing: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Liu, Y.; Zhong, L.; Puram, S.V.; Mazul, A.L. Neighborhood Socioeconomic Status and Racial and Ethnic Survival Disparities in Oral Cavity and Laryngeal Cancer. Cancer Epidemiol. Biomark. Prev. 2023, 32, 642–652. [Google Scholar] [CrossRef] [PubMed]
- Chu, K.P.; Shema, S.; Wu, S.; Gomez, S.L.; Chang, E.T.; Le, Q.T. Head and neck cancer-specific survival based on socioeconomic status in Asians and Pacific Islanders. Cancer 2011, 117, 1935–1945. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Country/Continent | Guideline | Society/Organization | Anatomical Site Covered | Year of Publication |
|---|---|---|---|---|
| Africa | Guidelines for low-resource regions | African Head and Neck Society | Oral Cavity | 2019 |
| Asia | Consensus recommendations for management of HNC in Asian countries | The Asia Pacific HNC Expert Panel | Head and Neck | 2013 |
| Pan-Asian Adaptation of the European Society for Medical Oncology | European Society for Medical Oncology and Korean Society of Medical Oncology | Head and Neck | 2021 | |
| Canada | Clinical practice guideline | Cancer Care Ontario’s HNC disease site group | Larynx | 2013 |
| China | Diagnosis and treatment guidelines for HNC working group | Chinese Society of Clinical Oncology | Head and Neck | 2019 |
| Denmark | The Danish National Guidelines | Danish Society for Head and Neck Oncology | Oral Cavity | 2006 |
| Europe | EHNS-ESMO-ESTRO Clinical Practice Guidelines | The EHNS Executive Board, ESMO Guidelines Committee, and ESTRO Executive Board | Head and Neck | 2020 |
| Germany | The German S3 Guideline | German Cancer Society and German Cancer Aid | Larynx | 2020 |
| India | Indian Clinical Practice Consensus | Oral Cancer Task Force with a Multidisciplinary Expert Panel | Oropharynx | 2020 |
| Oral Cavity | 2020 | |||
| Larynx | 2020 | |||
| Indian Council of Medical Research Consensus | Indian Council of Medical Research | Oral cavity | 2015 | |
| Japan | Japanese Clinical Practice Guideline for HNC | Japan Society for Head and Neck Cancer | Head and Neck | 2017 |
| Spain | Spanish multidisciplinary consensus | Spanish Society for Head and Neck Cancer | Head and Neck | 2017 |
| Spanish Society of Medical Oncology | Spanish Group for the Treatment of Head and Neck Tumors and SEOM | Head and Neck | 2021 | |
| Netherlands | The Dutch National Guideline | Dutch Cooperative Head and Neck Oncology Group | Larynx | 2002 |
| UK | United Kingdom National Multidisciplinary Guidelines | Specialty associations involved in the care of HNC in the UK | Oropharynx | 2016 |
| Oral cavity | 2016 | |||
| Larynx | 2016 | |||
| National Institute for Health and Care Excellence Guidelines for England and Wales | NICE Guideline Committee | Head and Neck | 2016 | |
| USA | American Society of Clinical Oncology Clinical Practice Guideline | American Society of Clinical Oncology | Larynx | 2018 |
| American College of Radiology Appropriateness Criteria | The ACR Expert Panel on Radiation Oncology—HNC | Oropharynx | 2016 | |
| Larynx | 2014 | |||
| Clinical Practice Guidelines for HNC | H. Lee Moffitt Cancer Center and Research Institute-Clinical Practice Guidelines Committee for the Head and Neck Program | Head and Neck | 1996 | |
| National Comprehensive Cancer Network Guidelines | NCCN Head and Neck Cancers Panel Members | Head and Neck | 2023 |
| Cancer Type | Oral Cancer | Oropharyngeal Cancer | Laryngeal Cancer | |||
|---|---|---|---|---|---|---|
| Clinical Stage | Early | Advance | Early | Advance | Early | Advance |
| Standard therapy recommendations * | Surgery (preferred) or RT Elective neck dissection (ipsilateral or bilateral) | Surgery (preferred),RT, or CCRT | Transoral/open resection or RT Ipsilateral/bilateral neck dissection | CCRT or surgery followed by postoperative RT/CRT or ICT | Surgery (endoscopic resection, partial laryngectomy, or open resection) or RT Elective neck dissection (except in the early-stage glottic cancer) | Surgery, RT, CCRT, and ICT Neck dissection |
| Recommendations according to limitations/resources of each country |
|
| ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arboleda, L.P.A.; de Carvalho, G.B.; Santos-Silva, A.R.; Fernandes, G.A.; Vartanian, J.G.; Conway, D.I.; Virani, S.; Brennan, P.; Kowalski, L.P.; Curado, M.P. Squamous Cell Carcinoma of the Oral Cavity, Oropharynx, and Larynx: A Scoping Review of Treatment Guidelines Worldwide. Cancers 2023, 15, 4405. https://doi.org/10.3390/cancers15174405
Arboleda LPA, de Carvalho GB, Santos-Silva AR, Fernandes GA, Vartanian JG, Conway DI, Virani S, Brennan P, Kowalski LP, Curado MP. Squamous Cell Carcinoma of the Oral Cavity, Oropharynx, and Larynx: A Scoping Review of Treatment Guidelines Worldwide. Cancers. 2023; 15(17):4405. https://doi.org/10.3390/cancers15174405
Chicago/Turabian StyleArboleda, Lady Paola Aristizabal, Genival Barbosa de Carvalho, Alan Roger Santos-Silva, Gisele Aparecida Fernandes, Jose Guilherme Vartanian, David I. Conway, Shama Virani, Paul Brennan, Luiz Paulo Kowalski, and Maria Paula Curado. 2023. "Squamous Cell Carcinoma of the Oral Cavity, Oropharynx, and Larynx: A Scoping Review of Treatment Guidelines Worldwide" Cancers 15, no. 17: 4405. https://doi.org/10.3390/cancers15174405