
Effects of Hyperthermia and Hyperthermic Intraperitoneal Chemoperfusion on the Peritoneal and Tumor Immune Contexture
 , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
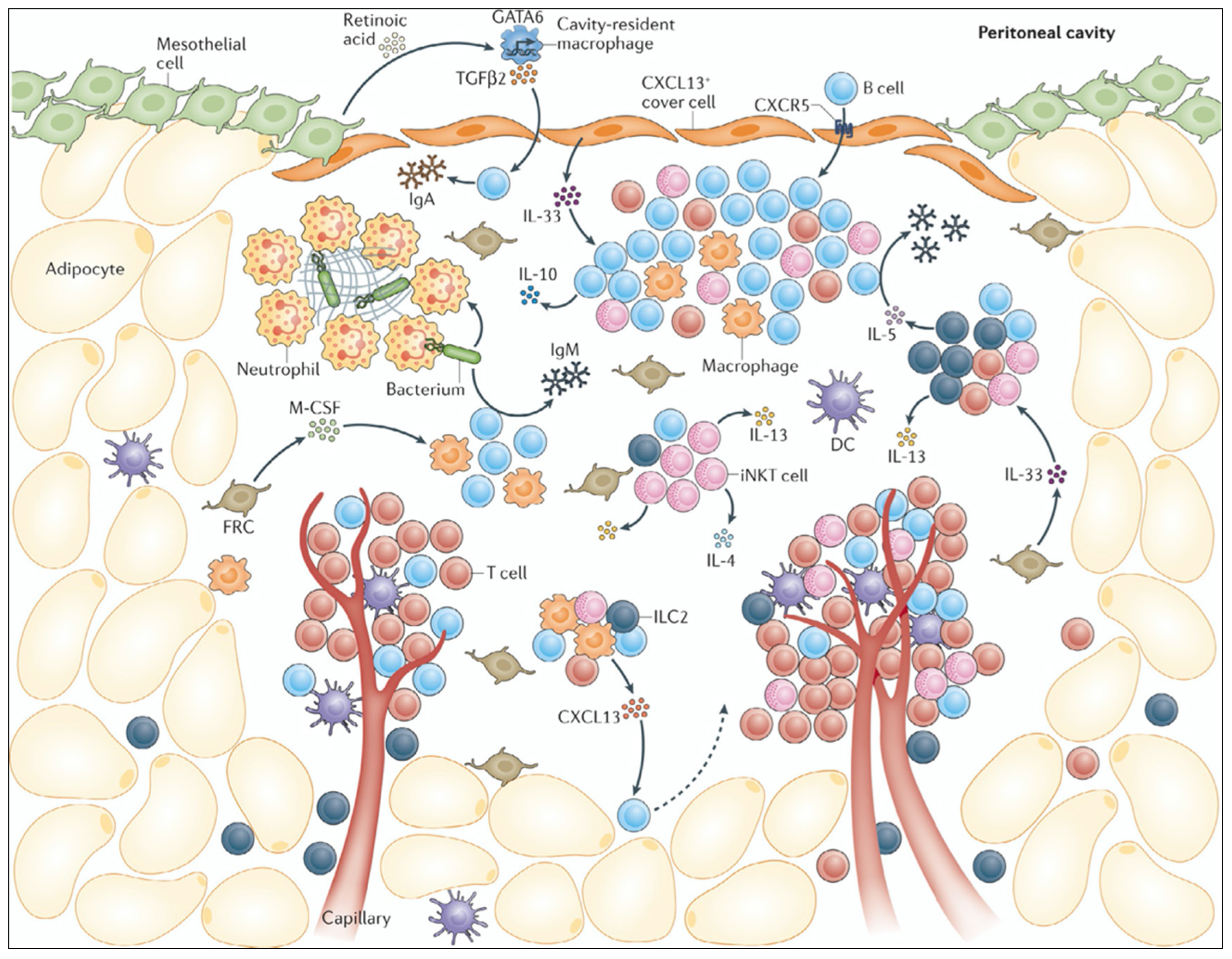
2. Immune Contexture of the Healthy Peritoneal Cavity
3. Immune Contexture of Peritoneal Metastases
4. Non-Immune Related Effects of HIPEC
4.1. Effects on Peritoneal Blood Flow and Pharmacokinetics
4.2. Effect on Chemotherapy Cytotoxicity
4.3. Effects on Peritoneal and Gut Integrity
5. Immune Effects of HIPEC
Clinical and Translational Studies
6. Biomechanical Effects of Hyperthermia
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jacquet, P.; Sugarbaker, P.H. Peritoneal-plasma barrier. Cancer Treat. Res. 1996, 82, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, P.H.; Gianola, F.J.; Speyer, J.C.; Wesley, R.; Barofsky, I.; Meyers, C.E. Prospective, randomized trial of intravenous versus intraperitoneal 5-fluorouracil in patients with advanced primary colon or rectal cancer. Surgery 1985, 98, 414–422. [Google Scholar] [PubMed]
- Spratt, J.S.; Adcock, R.A.; Sherrill, W.; Travathen, S. Hyperthermic peritoneal perfusion system in canines. Cancer Res. 1980, 40, 253–255. [Google Scholar] [PubMed]
- Koga, S.; Hamazoe, R.; Maeta, M.; Shimizu, N.; Kanayama, H.; Osaki, Y. Treatment of implanted peritoneal cancer in rats by continuous hyperthermic peritoneal perfusion in combination with an anticancer drug. Cancer Res. 1984, 44, 1840–1842. [Google Scholar] [PubMed]
- Fujimoto, S.; Shrestha, R.D.; Kokubun, M.; Ohta, M.; Takahashi, M.; Kobayashi, K.; Kiuchi, S.; Okui, K.; Miyoshi, T.; Arimizu, N.; et al. Intraperitoneal hyperthermic perfusion combined with surgery effective for gastric cancer patients with peritoneal seeding. Ann. Surg. 1988, 208, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Witkamp, A.J.; de Bree, E.; Van Goethem, R.; Zoetmulder, F.A. Rationale and techniques of intra-operative hyperthermic intraperitoneal chemotherapy. Cancer Treat. Rev. 2001, 27, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Gremonprez, F.; Gossye, H.; Ceelen, W. Use of hyperthermia versus normothermia during intraperitoneal chemoperfusion with oxaliplatin for colorectal peritoneal carcinomatosis: A propensity score matched analysis. Eur. J. Surg. Oncol. 2019, 45, 366–370. [Google Scholar] [CrossRef]
- Casado-Adam, A.; Rodriguez-Ortiz, L.; Rufian-Peña, S.; Muñoz-Casares, C.; Caro-Cuenca, T.; Ortega-Salas, R.; Fernandez-Peralbo, M.A.; Luque-de-Castro, M.D.; Sanchez-Hidalgo, J.M.; Hervas-Martinez, C.; et al. The Role of Intraperitoneal Intraoperative Chemotherapy with Paclitaxel in the Surgical Treatment of Peritoneal Carcinomatosis from Ovarian Cancer-Hyperthermia versus Normothermia: A Randomized Controlled Trial. J. Clin. Med. 2022, 11, 5785. [Google Scholar] [CrossRef]
- Rau, B.; Lang, H.; Königsrainer, A.; Gockel, I.; Rau, H.G.; Seeliger, H.; Lerchenmüller, C.; Reim, D.; Wahba, R.; Angele, M.; et al. 1376O The effect of hyperthermic intraperitoneal chemotherapy (HIPEC) upon cytoreductive surgery (CRS) in gastric cancer (GC) with synchronous peritoneal metastasis (PM): A randomized multicentre phase III trial (GASTRIPEC-I-trial). Ann. Oncol. 2021, 32, S1040. [Google Scholar] [CrossRef]
- Quénet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 256–266. [Google Scholar] [CrossRef]
- van Driel, W.J.; Koole, S.N.; Sikorska, K.; Schagen van Leeuwen, J.H.; Schreuder, H.W.R.; Hermans, R.H.M.; de Hingh, I.; van der Velden, J.; Arts, H.J.; Massuger, L.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N. Engl. J. Med. 2018, 378, 230–240. [Google Scholar] [CrossRef]
- Antonio, C.C.P.; Alida, G.G.; Elena, G.G.; Rocío, G.S.; Jerónimo, M.G.; Luis, A.R.J.; Aníbal, N.D.; Francisco, B.V.; Jesús, G.; Pablo, R.R.; et al. Cytoreductive Surgery with or without HIPEC after Neoadjuvant Chemotherapy in Ovarian Cancer: A Phase 3 Clinical Trial. Ann. Surg. Oncol. 2022, 29, 2617–2625. [Google Scholar] [CrossRef] [PubMed]
- Lim, M.C.; Chang, S.J.; Park, B.; Yoo, H.J.; Yoo, C.W.; Nam, B.H.; Park, S.Y. Survival after Hyperthermic Intraperitoneal Chemotherapy and Primary or Interval Cytoreductive Surgery in Ovarian Cancer: A Randomized Clinical Trial. JAMA Surg. 2022, 157, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.W.; Meneses, J.J. Effects of hyperthermia on the production and activity of primary and secondary cytolytic T-lymphocytes in vitro. Cancer Res. 1978, 38, 1120–1126. [Google Scholar] [PubMed]
- Agarwal, S.S.; Katz, E.J.; Loeb, L.A. Effect of hyperthermia on the survival of normal human peripheral blood mononuclear cells. Cancer Res. 1983, 43, 3124–3126. [Google Scholar] [PubMed]
- Jung, D.H.; Son, S.Y.; Oo, A.M.; Park, Y.S.; Shin, D.J.; Ahn, S.H.; Park, D.J.; Kim, H.H. Feasibility of hyperthermic pressurized intraperitoneal aerosol chemotherapy in a porcine model. Surg. Endosc. 2016, 30, 4258–4264. [Google Scholar] [CrossRef]
- Bachmann, C.; Sautkin, I.; Nadiradze, G.; Archid, R.; Weinreich, F.J.; Königsrainer, A.; Reymond, M.A. Technology development of hyperthermic pressurized intraperitoneal aerosol chemotherapy (hPIPAC). Surg. Endosc. 2021, 35, 6358–6365. [Google Scholar] [CrossRef]
- Nowacki, M.; Peterson, M.; Kloskowski, T.; McCabe, E.; Guiral, D.C.; Polom, K.; Pietkun, K.; Zegarska, B.; Pokrywczynska, M.; Drewa, T.; et al. Nanoparticle as a novel tool in hyperthermic intraperitoneal and pressurized intraperitoneal aerosol chemotheprapy to treat patients with peritoneal carcinomatosis. Oncotarget 2017, 8, 78208–78224. [Google Scholar] [CrossRef]
- van Baal, J.O.; Van de Vijver, K.K.; Nieuwland, R.; van Noorden, C.J.; van Driel, W.J.; Sturk, A.; Kenter, G.G.; Rikkert, L.G.; Lok, C.A. The histophysiology and pathophysiology of the peritoneum. Tissue Cell 2017, 49, 95–105. [Google Scholar] [CrossRef]
- Mutsaers, S.E.; Prêle, C.M.; Pengelly, S.; Herrick, S.E. Mesothelial cells and peritoneal homeostasis. Fertil. Steril. 2016, 106, 1018–1024. [Google Scholar] [CrossRef]
- Yung, S.; Li, F.K.; Chan, T.M. Peritoneal mesothelial cell culture and biology. Perit. Dial. Int. 2006, 26, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.B.; Li, M.; Li, J.C. Recent advances in the research of lymphatic stomata. Anat. Rec. 2010, 293, 754–761. [Google Scholar] [CrossRef] [PubMed]
- Meza-Perez, S.; Randall, T.D. Immunological Functions of the Omentum. Trends Immunol. 2017, 38, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Silva-Sanchez, A.; Randall, T.D.; Meza-Perez, S. Specialized immune responses in the peritoneal cavity and omentum. J. Leukoc. Biol. 2021, 109, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Jackson-Jones, L.H.; Smith, P.; Portman, J.R.; Magalhaes, M.S.; Mylonas, K.J.; Vermeren, M.M.; Nixon, M.; Henderson, B.E.P.; Dobie, R.; Vermeren, S.; et al. Stromal Cells Covering Omental Fat-Associated Lymphoid Clusters Trigger Formation of Neutrophil Aggregates to Capture Peritoneal Contaminants. Immunity 2020, 52, 700–715.e706. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, P.; Laganson, A.; Deng, M. GATA6(+) Peritoneal Resident Macrophage: The Immune Custodian in the Peritoneal Cavity. Front. Pharmacol. 2022, 13, 866993. [Google Scholar] [CrossRef] [PubMed]
- Rosas, M.; Davies, L.C.; Giles, P.J.; Liao, C.T.; Kharfan, B.; Stone, T.C.; O’Donnell, V.B.; Fraser, D.J.; Jones, S.A.; Taylor, P.R. The transcription factor Gata6 links tissue macrophage phenotype and proliferative renewal. Science 2014, 344, 645–648. [Google Scholar] [CrossRef]
- Kim, K.W.; Williams, J.W.; Wang, Y.T.; Ivanov, S.; Gilfillan, S.; Colonna, M.; Virgin, H.W.; Gautier, E.L.; Randolph, G.J. MHC II+ resident peritoneal and pleural macrophages rely on IRF4 for development from circulating monocytes. J. Exp. Med. 2016, 213, 1951–1959. [Google Scholar] [CrossRef]
- Haas, K.M. B-1 lymphocytes in mice and nonhuman primates. Ann. N. Y Acad. Sci. 2015, 1362, 98–109. [Google Scholar] [CrossRef]
- Trim, W.V.; Lynch, L. Immune and non-immune functions of adipose tissue leukocytes. Nat. Rev. Immunol. 2022, 22, 371–386. [Google Scholar] [CrossRef]
- Demuytere, J.; Ernst, S.; van Ovost, J.; Cosyns, S.; Ceelen, W. The tumor immune microenvironment in peritoneal carcinomatosis. Int. Rev. Cell Mol. Biol. 2022, 371, 63–95. [Google Scholar] [CrossRef] [PubMed]
- Lemoine, L.; Sugarbaker, P.; Van der Speeten, K. Pathophysiology of colorectal peritoneal carcinomatosis: Role of the peritoneum. World J. Gastroenterol. 2016, 22, 7692–7707. [Google Scholar] [CrossRef] [PubMed]
- Mikuła-Pietrasik, J.; Uruski, P.; Tykarski, A.; Książek, K. The peritoneal “soil” for a cancerous “seed”: A comprehensive review of the pathogenesis of intraperitoneal cancer metastases. Cell. Mol. Life Sci. 2018, 75, 509–525. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Guiral, D.; Hübner, M.; Alyami, M.; Bhatt, A.; Ceelen, W.; Glehen, O.; Lordick, F.; Ramsay, R.; Sgarbura, O.; Van Der Speeten, K.; et al. Primary and metastatic peritoneal surface malignancies. Nat. Rev. Dis. Primers 2021, 7, 91. [Google Scholar] [CrossRef]
- Liu, Y.; Cao, X. Characteristics and Significance of the Pre-metastatic Niche. Cancer Cell 2016, 30, 668–681. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, H.; Huang, Y.; Chen, Y.; Chen, C.; Zhuo, W.; Teng, L. Comprehensive Roles and Future Perspectives of Exosomes in Peritoneal Metastasis of Gastric Cancer. Front. Oncol. 2021, 11, 684871. [Google Scholar] [CrossRef] [PubMed]
- Deng, G.; Qu, J.; Zhang, Y.; Che, X.; Cheng, Y.; Fan, Y.; Zhang, S.; Na, D.; Liu, Y.; Qu, X. Gastric cancer-derived exosomes promote peritoneal metastasis by destroying the mesothelial barrier. FEBS Lett. 2017, 591, 2167–2179. [Google Scholar] [CrossRef]
- Demuytere, J.; Ceelen, W.; Van Dorpe, J.; Hoorens, A. The role of the peritoneal microenvironment in the pathogenesis of colorectal peritoneal carcinomatosis. Exp. Mol. Pathol. 2020, 115, 104442. [Google Scholar] [CrossRef]
- Wei, M.; Yang, T.; Chen, X.; Wu, Y.; Deng, X.; He, W.; Yang, J.; Wang, Z. Malignant ascites-derived exosomes promote proliferation and induce carcinoma-associated fibroblasts transition in peritoneal mesothelial cells. Oncotarget 2017, 8, 42262–42271. [Google Scholar] [CrossRef]
- Song, H.; Wang, T.; Tian, L.; Bai, S.; Chen, L.; Zuo, Y.; Xue, Y. Macrophages on the Peritoneum are involved in Gastric Cancer Peritoneal Metastasis. J. Cancer 2019, 10, 5377–5387. [Google Scholar] [CrossRef]
- Gwee, Y.X.; Chia, D.K.A.; So, J.; Ceelen, W.; Yong, W.P.; Tan, P.; Ong, C.J.; Sundar, R. Integration of Genomic Biology into Therapeutic Strategies of Gastric Cancer Peritoneal Metastasis. J. Clin. Oncol. 2022, 40, 2830. [Google Scholar] [CrossRef] [PubMed]
- Solass, W.; Horvath, P.; Struller, F.; Königsrainer, I.; Beckert, S.; Königsrainer, A.; Weinreich, F.J.; Schenk, M. Functional vascular anatomy of the peritoneum in health and disease. Pleura Peritoneum 2016, 1, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Bezu, L.; Raineau, M.; Deloménie, M.; Cholley, B.; Pirracchio, R. Haemodynamic management during hyperthermic intraperitoneal chemotherapy: A systematic review. Anaesth. Crit. Care Pain. Med. 2020, 39, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Vos, L.M.C.; Aronson, S.L.; van Driel, W.J.; Huitema, A.D.R.; Schagen van Leeuwen, J.H.; Lok, C.A.R.; Sonke, G.S. Translational and pharmacological principles of hyperthermic intraperitoneal chemotherapy for ovarian cancer. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 78, 86–102. [Google Scholar] [CrossRef] [PubMed]
- Facy, O.; Al Samman, S.; Magnin, G.; Ghiringhelli, F.; Ladoire, S.; Chauffert, B.; Rat, P.; Ortega-Deballon, P. High pressure enhances the effect of hyperthermia in intraperitoneal chemotherapy with oxaliplatin: An experimental study. Ann. Surg. 2012, 256, 1084–1088. [Google Scholar] [CrossRef]
- Pestieau, S.R.; Belliveau, J.F.; Griffin, H.; Stuart, O.A.; Sugarbaker, P.H. Pharmacokinetics of intraperitoneal oxaliplatin: Experimental studies. J. Surg. Oncol. 2001, 76, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Zeamari, S.; Floot, B.; Van der Vange, N.; Stewart, F.A. Pharmacokinetics and pharmacodynamics of cisplatin after Intraoperative Hyperthermic Intraperitoneal Chemoperfusion (HIPEC). Anticancer Res. 2003, 23, 1643–1648. [Google Scholar] [PubMed]
- Mas-Fuster, M.I.; Ramon-Lopez, A.; Lacueva, F.J.; Arroyo, A.; Más-Serrano, P.; Nalda-Molina, R. Population pharmacokinetics of oxaliplatin after intraperitoneal administration with hyperthermia in Wistar rats. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2018, 119, 22–30. [Google Scholar] [CrossRef]
- Los, G.; Sminia, P.; Wondergem, J.; Mutsaers, P.H.; Havemen, J.; ten Bokkel Huinink, D.; Smals, O.; Gonzalez-Gonzalez, D.; McVie, J.G. Optimisation of intraperitoneal cisplatin therapy with regional hyperthermia in rats. Eur. J. Cancer 1991, 27, 472–477. [Google Scholar] [CrossRef]
- Piché, N.; Leblond, F.A.; Sidéris, L.; Pichette, V.; Drolet, P.; Fortier, L.-P.; Mitchell, A.; Dubé, P. Rationale for heating oxaliplatin for the intraperitoneal treatment of peritoneal carcinomatosis: A study of the effect of heat on intraperitoneal oxaliplatin using a murine model. Ann. Surg. 2011, 254, 138–144. [Google Scholar] [CrossRef]
- Sørensen, O.; Andersen, A.M.; Kristian, A.; Giercksky, K.-E.; Flatmark, K. Impact of hyperthermia on pharmacokinetics of intraperitoneal mitomycin C in rats investigated by microdialysis. J. Surg. Oncol. 2014, 109, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Klaver, Y.L.B.; Hendriks, T.; Lomme, R.M.L.M.; Rutten, H.J.T.; Bleichrodt, R.P.; de Hingh, I.H.J.T. Hyperthermia and Intraperitoneal Chemotherapy for the Treatment of Peritoneal Carcinomatosis: An Experimental Study. Ann. Surg. 2011, 254, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Xie, F.; Van Bocxlaer, J.; Colin, P.; Carlier, C.; Van Kerschaver, O.; Weerts, J.; Denys, H.; Tummers, P.; Willaert, W.; Ceelen, W.; et al. PKPD Modeling and Dosing Considerations in Advanced Ovarian Cancer Patients Treated with Cisplatin-Based Intraoperative Intraperitoneal Chemotherapy. AAPS J. 2020, 22, 96. [Google Scholar] [CrossRef]
- Benoit, L.; Duvillard, C.; Rat, P.; Chauffert, B. The effect of intra-abdominal temperature on the tissue and tumor diffusion of intraperitoneal cisplatin in a model of peritoneal carcinomatosis in rats. Chirurgie 1999, 124, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Jacquet, P.; Averbach, A.; Stuart, O.A.; Chang, D.; Sugarbaker, P.H. Hyperthermic intraperitoneal doxorubicin: Pharmacokinetics, metabolism, and tissue distribution in a rat model. Cancer Chemother. Pharmacol. 1998, 41, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Sticca, R.P.; Dach, B.W. Rationale for hyperthermia with intraoperative intraperitoneal chemotherapy agents. Surg. Oncol. Clin. N. Am. 2003, 12, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Panteix, G.; Guillaumont, M.; Cherpin, L.; Cuichard, J.; Gilly, F.N.; Carry, P.Y.; Sayag, A.; Salle, B.; Brachet, A.; Bienvenu, J.; et al. Study of the pharmacokinetics of mitomycin C in humans during intraperitoneal chemohyperthermia with special mention of the concentration in local tissues. Oncology 1993, 50, 366–370. [Google Scholar] [CrossRef]
- Ceelen, W.; Demuytere, J.; de Hingh, I. Hyperthermic Intraperitoneal Chemotherapy: A Critical Review. Cancers 2021, 13, 3114. [Google Scholar] [CrossRef]
- Sakaguchi, Y.; Kohnoe, S.; Emi, Y.; Maehara, Y.; Kusumoto, T.; Sugimachi, K. Cytotoxicity of mitomycin C and carboquone combined with hyperthermia against hypoxic tumor cells in vitro. Oncology 1992, 49, 227–232. [Google Scholar] [CrossRef]
- Teicher, B.A.; Kowal, C.D.; Kennedy, K.A.; Sartorelli, A.C. Enhancement by hyperthermia of the in vitro cytotoxicity of mitomycin C toward hypoxic tumor cells. Cancer Res. 1981, 41, 1096–1099. [Google Scholar]
- Helderman, R.; Loke, D.R.; Verhoeff, J.; Rodermond, H.M.; van Bochove, G.G.W.; Boon, M.; van Kesteren, S.; Garcia Vallejo, J.J.; Kok, H.P.; Tanis, P.J.; et al. The Temperature-Dependent Effectiveness of Platinum-Based Drugs Mitomycin-C and 5-FU during Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Colorectal Cancer Cell Lines. Cells 2020, 9, 1775. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.; Canet-Jourdan, C.; Annereau, M.; Zajac, O.; Gelli, M.; Broutin, S.; Mercier, L.; Paci, A.; Lemare, F.; Ducreux, M.; et al. Organoids as preclinical models to improve intraperitoneal chemotherapy effectiveness for colorectal cancer patients with peritoneal metastases: Preclinical models to improve HIPEC. Int. J. Pharm. 2017, 531, 143–152. [Google Scholar] [CrossRef] [PubMed]
- de Jong, L.A.W.; Elekonawo, F.M.K.; de Reuver, P.R.; Bremers, A.J.A.; de Wilt, J.H.W.; Jansman, F.G.A.; ter Heine, R.; van Erp, N.P. Hyperthermic intraperitoneal chemotherapy with oxaliplatin for peritoneal carcinomatosis: A clinical pharmacological perspective on a surgical procedure. Br. J. Clin. Pharmacol. 2019, 85, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, S.; Takahashi, M.; Kobayashi, K.; Mutou, T.; Toyosawa, T.; Izawa, E.; Numai, T.; Kondoh, F.; Ohkubo, H. Histologic evaluation of preventive measures for scald injury on the peritoneo-serosal surface due to intraoperative hyperthermic chemoperfusion for patients with gastric cancer and peritoneal metastasis. Int. J. Hyperth. 1998, 14, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Dewhirst, M.W.; Viglianti, B.L.; Lora-Michiels, M.; Hanson, M.; Hoopes, P.J. Basic principles of thermal dosimetry and thermal thresholds for tissue damage from hyperthermia. Int. J. Hyperth. 2003, 19, 267–294. [Google Scholar] [CrossRef] [PubMed]
- Yarmolenko, P.S.; Moon, E.J.; Landon, C.; Manzoor, A.; Hochman, D.W.; Viglianti, B.L.; Dewhirst, M.W. Thresholds for thermal damage to normal tissues: An update. Int. J. Hyperth. 2011, 27, 320–343. [Google Scholar] [CrossRef] [PubMed]
- Lambert, G.P.; Gisolfi, C.V.; Berg, D.J.; Moseley, P.L.; Oberley, L.W.; Kregel, K.C. Selected contribution: Hyperthermia-induced intestinal permeability and the role of oxidative and nitrosative stress. J. Appl. Physiol. 2002, 92, 1750–1761; discussion 1749. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Li, H.; Lu, A.; Zhong, Y.; Hou, X.; Wang, N.; Jia, D.; Zan, J.; Zhao, H.; Xu, J.; et al. Reduction of intestinal mucosal immune function in heat-stressed rats and bacterial translocation. Int. J. Hyperth. 2012, 28, 756–765. [Google Scholar] [CrossRef]
- Bozer, M.; Türkçapar, N.; Bayar, S.; Kocaoglu, H. Intraperitoneal hyperthermic perfusion may induce bacterial translocation. Hepatogastroenterology. 2005, 52, 111–114. [Google Scholar]
- Ghulam Mohyuddin, S.; Khan, I.; Zada, A.; Qamar, A.; Arbab, A.A.I.; Ma, X.B.; Yu, Z.C.; Liu, X.X.; Yong, Y.H.; Ju, X.H.; et al. Influence of Heat Stress on Intestinal Epithelial Barrier Function, Tight Junction Protein, and Immune and Reproductive Physiology. Biomed. Res. Int. 2022, 2022, 8547379. [Google Scholar] [CrossRef]
- Hylander, B.L.; Repasky, E.A. Temperature as a modulator of the gut microbiome: What are the implications and opportunities for thermal medicine? Int. J. Hyperth. 2019, 36, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.S.; Repasky, E.A.; Fisher, D.T. Fever and the thermal regulation of immunity: The immune system feels the heat. Nat. Rev. Immunol. 2015, 15, 335–349. [Google Scholar] [CrossRef] [PubMed]
- Scutigliani, E.M.; Lobo-Cerna, F.; Mingo Barba, S.; Scheidegger, S.; Krawczyk, P.M. The Effects of Heat Stress on the Transcriptome of Human Cancer Cells: A Meta-Analysis. Cancers 2022, 15, 113. [Google Scholar] [CrossRef] [PubMed]
- Chin, Y.; Gumilar, K.E.; Li, X.G.; Tjokroprawiro, B.A.; Lu, C.H.; Lu, J.; Zhou, M.; Sobol, R.W.; Tan, M. Targeting HSF1 for cancer treatment: Mechanisms and inhibitor development. Theranostics 2023, 13, 2281–2300. [Google Scholar] [CrossRef] [PubMed]
- Minnaar, C.A.; Szasz, A. Forcing the Antitumor Effects of HSPs Using a Modulated Electric Field. Cells 2022, 11, 1838. [Google Scholar] [CrossRef] [PubMed]
- Cyran, A.M.; Zhitkovich, A. Heat Shock Proteins and HSF1 in Cancer. Front. Oncol. 2022, 12, 860320. [Google Scholar] [CrossRef] [PubMed]
- Seclì, L.; Fusella, F.; Avalle, L.; Brancaccio, M. The dark-side of the outside: How extracellular heat shock proteins promote cancer. Cell. Mol. Life Sci. 2021, 78, 4069–4083. [Google Scholar] [CrossRef] [PubMed]
- Calderwood, S.K.; Gong, J. Heat Shock Proteins Promote Cancer: It’s a Protection Racket. Trends Biochem. Sci. 2016, 41, 311–323. [Google Scholar] [CrossRef]
- Chakafana, G.; Shonhai, A. The Role of Non-Canonical Hsp70s (Hsp110/Grp170) in Cancer. Cells 2021, 10, 254. [Google Scholar] [CrossRef]
- Bohonowych, J.E.; Hance, M.W.; Nolan, K.D.; Defee, M.; Parsons, C.H.; Isaacs, J.S. Extracellular Hsp90 mediates an NF-κB dependent inflammatory stromal program: Implications for the prostate tumor microenvironment. Prostate 2014, 74, 395–407. [Google Scholar] [CrossRef]
- Li, D.Y.; Liang, S.; Wen, J.H.; Tang, J.X.; Deng, S.L.; Liu, Y.X. Extracellular HSPs: The Potential Target for Human Disease Therapy. Molecules 2022, 27, 2361. [Google Scholar] [CrossRef] [PubMed]
- Javid, H.; Hashemian, P.; Yazdani, S.; Sharbaf Mashhad, A.; Karimi-Shahri, M. The role of heat shock proteins in metastatic colorectal cancer: A review. J. Cell. Biochem. 2022, 123, 1704–1735. [Google Scholar] [CrossRef] [PubMed]
- Adnan, A.; Muñoz, N.M.; Prakash, P.; Habibollahi, P.; Cressman, E.N.K.; Sheth, R.A. Hyperthermia and Tumor Immunity. Cancers 2021, 13, 2507. [Google Scholar] [CrossRef] [PubMed]
- Scutigliani, E.M.; Liang, Y.; Crezee, H.; Kanaar, R.; Krawczyk, P.M. Modulating the Heat Stress Response to Improve Hyperthermia-Based Anticancer Treatments. Cancers 2021, 13, 1243. [Google Scholar] [CrossRef] [PubMed]
- Toraya-Brown, S.; Sheen, M.R.; Zhang, P.; Chen, L.; Baird, J.R.; Demidenko, E.; Turk, M.J.; Hoopes, P.J.; Conejo-Garcia, J.R.; Fiering, S. Local hyperthermia treatment of tumors induces CD8(+) T cell-mediated resistance against distal and secondary tumors. Nanomedicine 2014, 10, 1273–1285. [Google Scholar] [CrossRef] [PubMed]
- Nevo, N.; Lee Goldstein, A.; Bar-David, S.; Abu-Abeid, A.; Dayan, D.; Lahat, G.; Nizri, E. Immunological effects of heated intraperitoneal chemotherapy can be augmented by thymosin α1. Int. Immunopharmacol. 2023, 116, 109829. [Google Scholar] [CrossRef] [PubMed]
- Geva, R.; Alon, G.; Nathanson, M.; Bar-David, S.; Nevo, N.; Aizic, A.; Peles-Avraham, S.; Lahat, G.; Nizri, E. PD-1 Blockade Combined with Heated Intraperitoneal Chemotherapy Improves Outcome in Experimental Peritoneal Metastases from Colonic Origin in a Murine Model. Ann. Surg. Oncol. 2023, 30, 2657–2663. [Google Scholar] [CrossRef] [PubMed]
- Zunino, B.; Ricci, J.E. Hyperthermic intra-peritoneal chemotherapy and anticancer immune response. Oncoimmunology 2016, 5, e1060392. [Google Scholar] [CrossRef]
- Yonemura, Y.; de Aretxabala, X.; Fujimura, T.; Fushida, S.; Katayama, K.; Bandou, E.; Sugiyama, K.; Kawamura, T.; Kinoshita, K.; Endou, Y.; et al. Intraoperative chemohyperthermic peritoneal perfusion as an adjuvant to gastric cancer: Final results of a randomized controlled study. Hepatogastroenterology 2001, 48, 1776–1782. [Google Scholar]
- Huang, J.Y.; Xu, Y.Y.; Sun, Z.; Zhu, Z.; Song, Y.X.; Guo, P.T.; You, Y.; Xu, H.M. Comparison different methods of intraoperative and intraperitoneal chemotherapy for patients with gastric cancer: A meta-analysis. Asian Pac. J. Cancer Prev. 2012, 13, 4379–4385. [Google Scholar] [CrossRef]
- Bonnot, P.E.; Piessen, G.; Kepenekian, V.; Decullier, E.; Pocard, M.; Meunier, B.; Bereder, J.M.; Abboud, K.; Marchal, F.; Quenet, F.; et al. Cytoreductive Surgery with or without Hyperthermic Intraperitoneal Chemotherapy for Gastric Cancer with Peritoneal Metastases (CYTO-CHIP study): A Propensity Score Analysis. J. Clin. Oncol. 2019, 37, 2028–2040. [Google Scholar] [CrossRef] [PubMed]
- Farrell, R.; Burling, M.; Lee, Y.C.; Pather, S.; Robledo, K.; Mercieca-Bebber, R.; Stockler, M. Clinical Trial Protocol for HyNOVA: Hyperthermic and Normothermic intraperitoneal chemotherapy following interval cytoreductive surgery for stage III epithelial OVArian, fallopian tube and primary peritoneal cancer (ANZGOG1901/2020). J. Gynecol. Oncol. 2022, 33, e1. [Google Scholar] [CrossRef] [PubMed]
- Dellinger, T.H.; Han, E.S.; Raoof, M.; Lee, B.; Wu, X.; Cho, H.; He, T.F.; Lee, P.; Razavi, M.; Liang, W.S.; et al. Hyperthermic Intraperitoneal Chemotherapy-Induced Molecular Changes in Humans Validate Preclinical Data in Ovarian Cancer. JCO Precis. Oncol. 2022, 6, e2100239. [Google Scholar] [CrossRef] [PubMed]
- Moukarzel, L.A.; Ferrando, L.; Dopeso, H.; Stylianou, A.; Basili, T.; Pareja, F.; Da Cruz Paula, A.; Zoppoli, G.; Abu-Rustum, N.R.; Reis-Filho, J.S.; et al. Hyperthermic intraperitoneal chemotherapy (HIPEC) with carboplatin induces distinct transcriptomic changes in ovarian tumor and normal tissues. Gynecol. Oncol. 2022, 165, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cui, S.; Zhang, X.; Wu, Y.; Tang, H. High expression of heat shock protein 90 is associated with tumor aggressiveness and poor prognosis in patients with advanced gastric cancer. PLoS ONE 2013, 8, e62876. [Google Scholar] [CrossRef] [PubMed]
- Abi Zamer, B.; El-Huneidi, W.; Eladl, M.A.; Muhammad, J.S. Ins and Outs of Heat Shock Proteins in Colorectal Carcinoma: Its Role in Carcinogenesis and Therapeutic Perspectives. Cells 2021, 10, 2862. [Google Scholar] [CrossRef] [PubMed]
- Ge, H.; Yan, Y.; Guo, L.; Tian, F.; Wu, D. Prognostic role of HSPs in human gastrointestinal cancer: A systematic review and meta-analysis. Onco Targets Ther. 2018, 11, 351–359. [Google Scholar] [CrossRef]
- Salavati, H.; Debbaut, C.; Pullens, P.; Ceelen, W. Interstitial fluid pressure as an emerging biomarker in solid tumors. Biochim. Biophys. Acta Rev. Cancer 2022, 1877, 188792. [Google Scholar] [CrossRef]
- Salavati, H.; Pullens, P.; Ceelen, W.; Debbaut, C. Drug transport modeling in solid tumors: A computational exploration of spatial heterogeneity of biophysical properties. Comput. Biol. Med. 2023, 163, 107190. [Google Scholar] [CrossRef]
- Löke, D.R.; Helderman, R.F.C.P.A.; Franken, N.A.P.; Oei, A.L.; Tanis, P.J.; Crezee, J.; Kok, H.P. Simulating drug penetration during hyperthermic intraperitoneal chemotherapy. Drug Deliv. 2021, 28, 145–161. [Google Scholar] [CrossRef]
- Kerch, G. Tissue Integrity and COVID-19. Encyclopedia 2021, 1, 206–219. [Google Scholar] [CrossRef]
- Costa, A. Permeability-porosity relationship: A reexamination of the Kozeny-Carman equation based on a fractal pore-space geometry assumption. Geophys. Res. Lett. 2006, 33. [Google Scholar] [CrossRef]
- Hannon, G.; Tansi, F.L.; Hilger, I.; Prina-Mello, A. The Effects of Localized Heat on the Hallmarks of Cancer. Adv. Ther. 2021, 4, 2000267. [Google Scholar] [CrossRef]
- Liu, Y.; Liu, L.; Chen, M.; Zhang, Q. Double thermal transitions of type I collagen in acidic solution. J. Biomol. Struct. Dyn. 2013, 31, 862–873. [Google Scholar] [CrossRef] [PubMed]
- Kolosnjaj-Tabi, J.; Marangon, I.; Nicolas-Boluda, A.; Silva, A.K.A.; Gazeau, F. Nanoparticle-based hyperthermia, a local treatment modulating the tumor extracellular matrix. Pharmacol. Res. 2017, 126, 123–137. [Google Scholar] [CrossRef] [PubMed]
- Sadjadi, Z.; Zhao, R.; Hoth, M.; Qu, B.; Rieger, H. Migration of Cytotoxic T Lymphocytes in 3D Collagen Matrices. Biophys. J. 2020, 119, 2141–2152. [Google Scholar] [CrossRef] [PubMed]
- Tabdanov, E.; Rodríguez-Merced, N.; Cartagena-Rivera, A.; Puram, V.; Callaway, M.; Ensminger, E.; Pomeroy, E.; Yamamoto, K.; Lahr, W.; Webber, B. Engineering T cells to enhance 3D migration through structurally and mechanically complex tumor microenvironments. Nat. Commun. 2021, 12, 2815. [Google Scholar] [CrossRef]
- Bougherara, H.; Mansuet-Lupo, A.; Alifano, M.; Ngô, C.; Damotte, D.; Le Frère-Belda, M.A.; Donnadieu, E.; Peranzoni, E. Real-Time Imaging of Resident T Cells in Human Lung and Ovarian Carcinomas Reveals How Different Tumor Microenvironments Control T Lymphocyte Migration. Front. Immunol. 2015, 6, 500. [Google Scholar] [CrossRef]
- Larsen, A.M.H.; Kuczek, D.E.; Kalvisa, A.; Siersbæk, M.S.; Thorseth, M.L.; Johansen, A.Z.; Carretta, M.; Grøntved, L.; Vang, O.; Madsen, D.H. Collagen Density Modulates the Immunosuppressive Functions of Macrophages. J. Immunol. 2020, 205, 1461–1472. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Completed and Ongoing Clinical Trials of Hyperthermia for the Treatment of PM | ||||
|---|---|---|---|---|
| Study | Cancer Type | Treatment | Status | Results |
| OVIP1 (NCT02567253) | Ovarian Cancer | Normothermic (37 °C) vs. Hyperthermic (41 °C) Cisplatin (H)IPEC | Completed | Hyperthermia increased the absorption rate of cisplatin by 16.3% [53]; clinical results not yet published. |
| NCT02739698 | Ovarian Cancer | Normothermic (37 °C) vs. Hyperthermic (42–43 °C) Paclitaxel (H)IPEC | Completed | No difference observed in tissue penetration, pathological response, or apoptosis [8] |
| HyNOVA (ACTRN12621000269831) | Ovarian Cancer | Normothermic (37 °C) vs. Hyperthermic (42 °C) Cisplatin (H)IPEC | Ongoing | |
| Potential Benefits and Adverse Effects of Hyperthermia | |
|---|---|
| Benefits | Adverse Effects |
| Direct cytotoxic effects | Increased systemic uptake of chemotherapy |
| Synergism with some chemotherapeutic compounds | Heat shock response |
| Increased tissue penetration | Immunosuppressive effects |
| Immune-enhancing effects | Scald injury to the peritoneal surface |
| Increased blood flow and decreased interstitial fluid pressure → improved drug delivery | Increased bacterial translocation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chia, D.K.A.; Demuytere, J.; Ernst, S.; Salavati, H.; Ceelen, W. Effects of Hyperthermia and Hyperthermic Intraperitoneal Chemoperfusion on the Peritoneal and Tumor Immune Contexture. Cancers 2023, 15, 4314. https://doi.org/10.3390/cancers15174314
Chia DKA, Demuytere J, Ernst S, Salavati H, Ceelen W. Effects of Hyperthermia and Hyperthermic Intraperitoneal Chemoperfusion on the Peritoneal and Tumor Immune Contexture. Cancers. 2023; 15(17):4314. https://doi.org/10.3390/cancers15174314
Chicago/Turabian StyleChia, Daryl K. A., Jesse Demuytere, Sam Ernst, Hooman Salavati, and Wim Ceelen. 2023. "Effects of Hyperthermia and Hyperthermic Intraperitoneal Chemoperfusion on the Peritoneal and Tumor Immune Contexture" Cancers 15, no. 17: 4314. https://doi.org/10.3390/cancers15174314