
Surgical Treatment of Carcinomas of the Oral Minor Salivary Glands—Oncological Outcome in Dependence of Tumor Entity and Therapeutic Strategies
 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Collective and Obtained Data
2.2. Statistics
3. Results
3.1. Patient Cohort
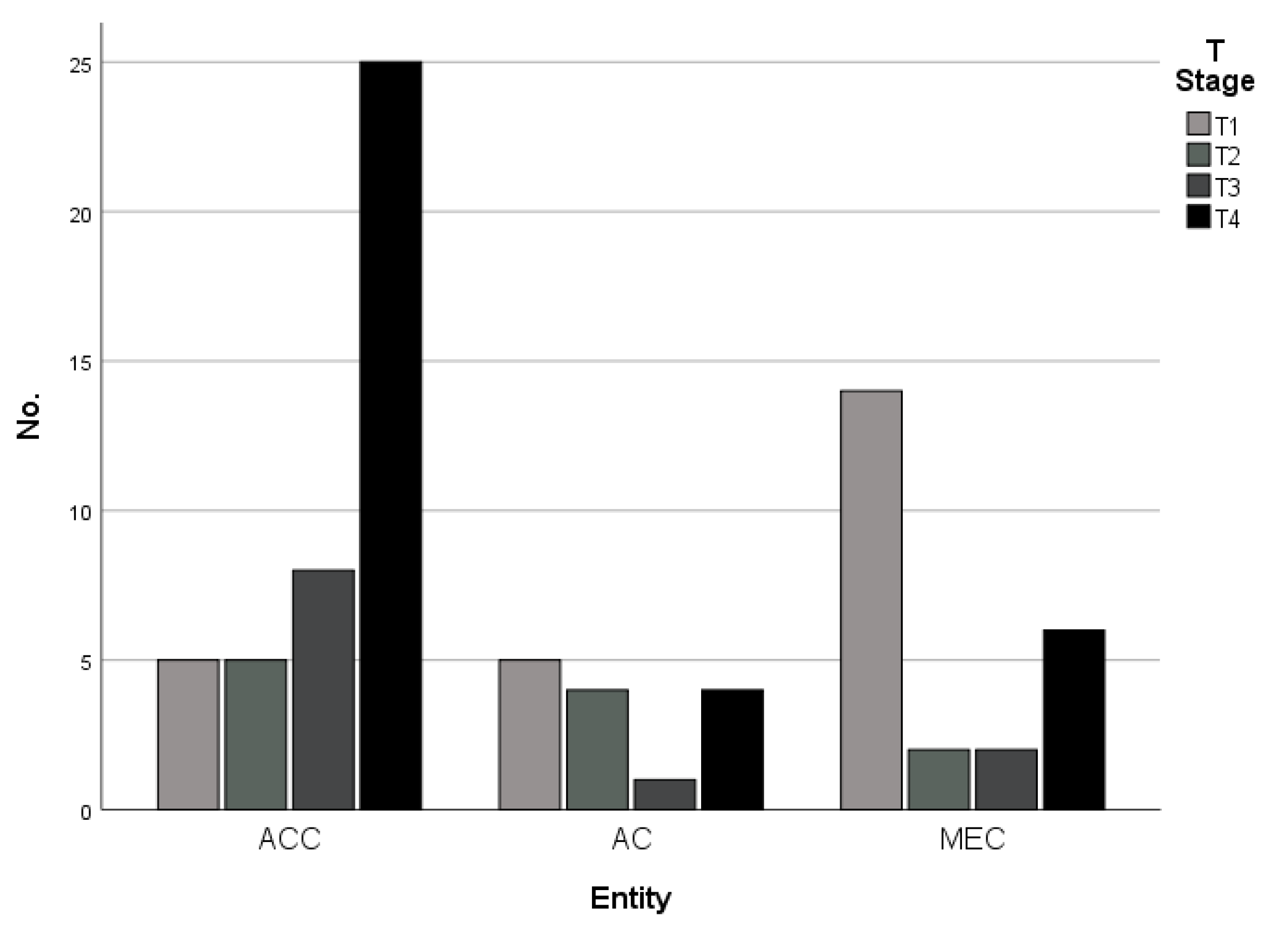
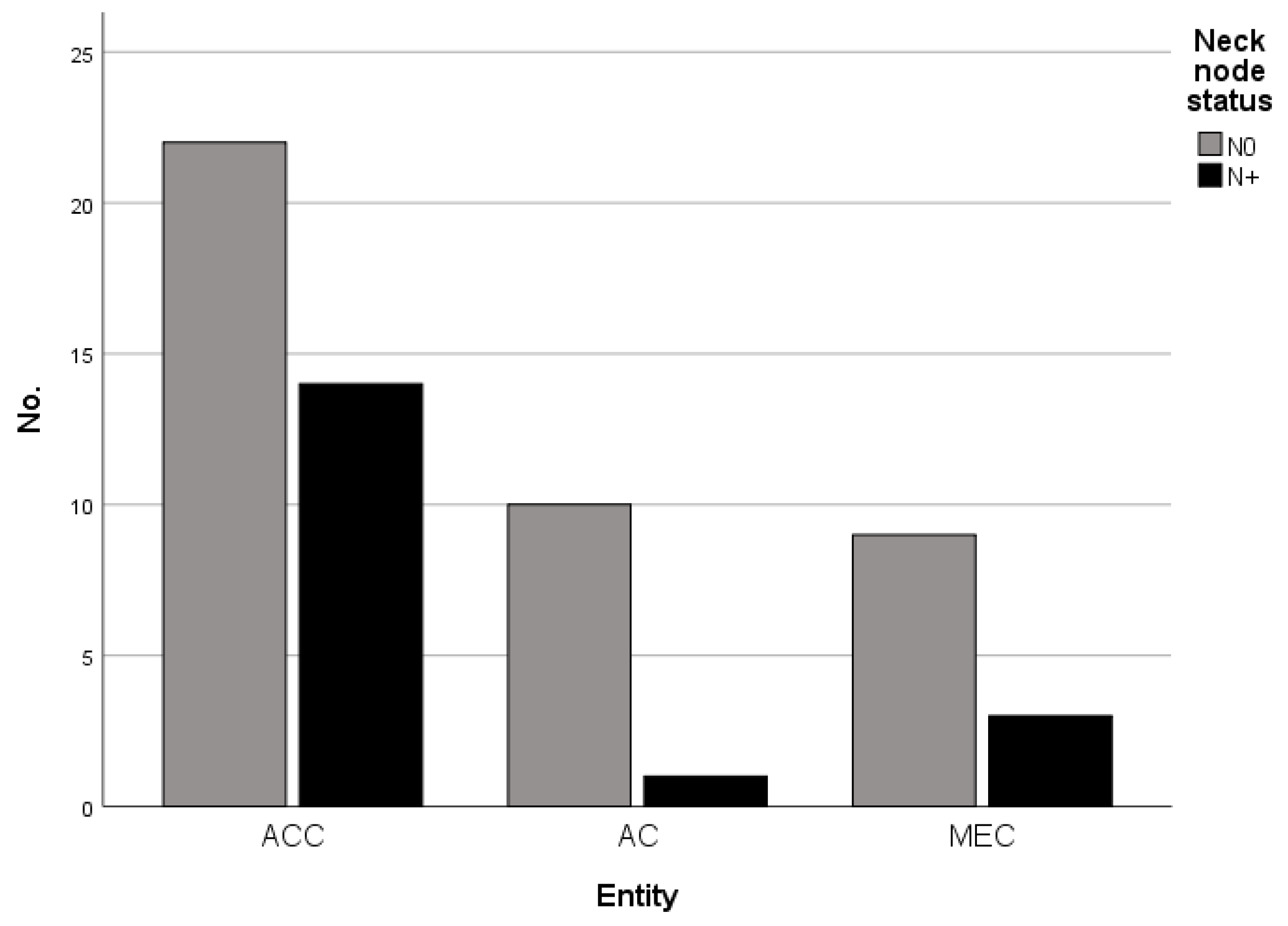
3.2. Tumor Stage and Cervical Metastases
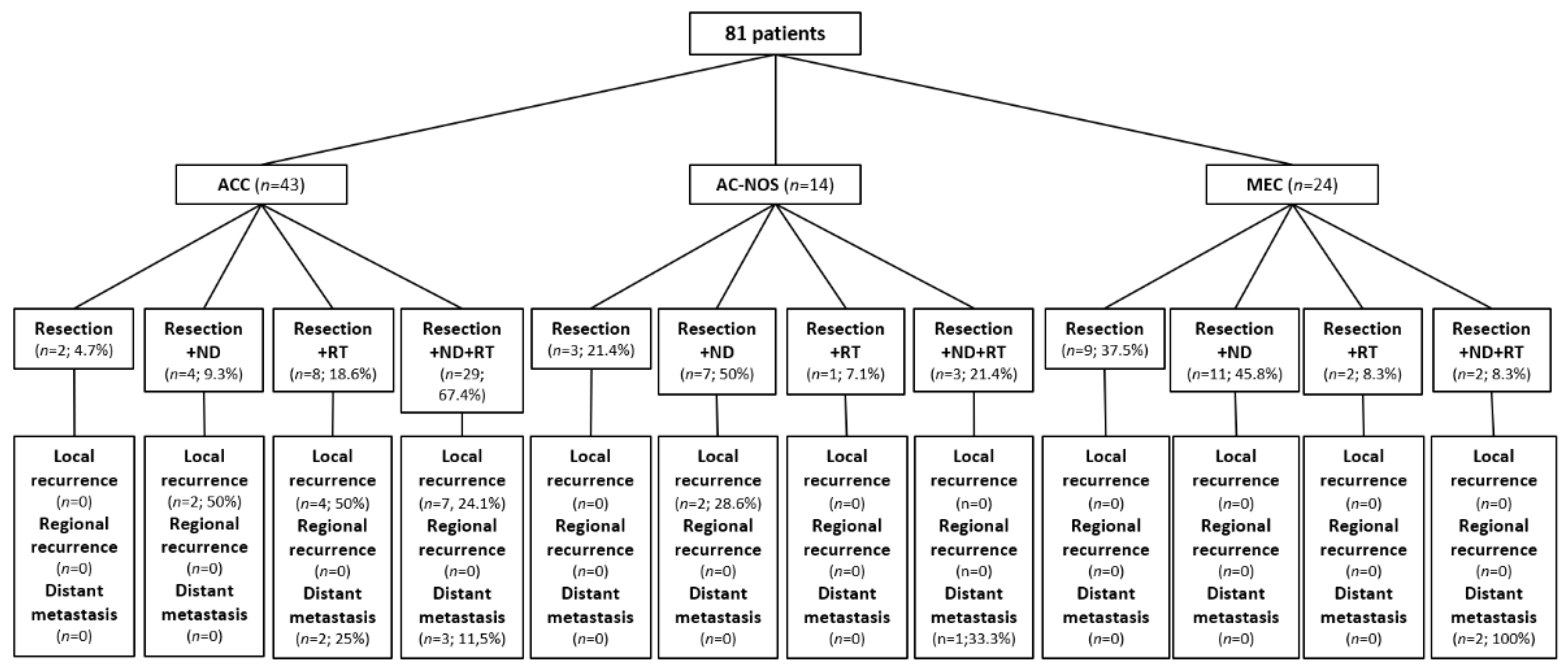
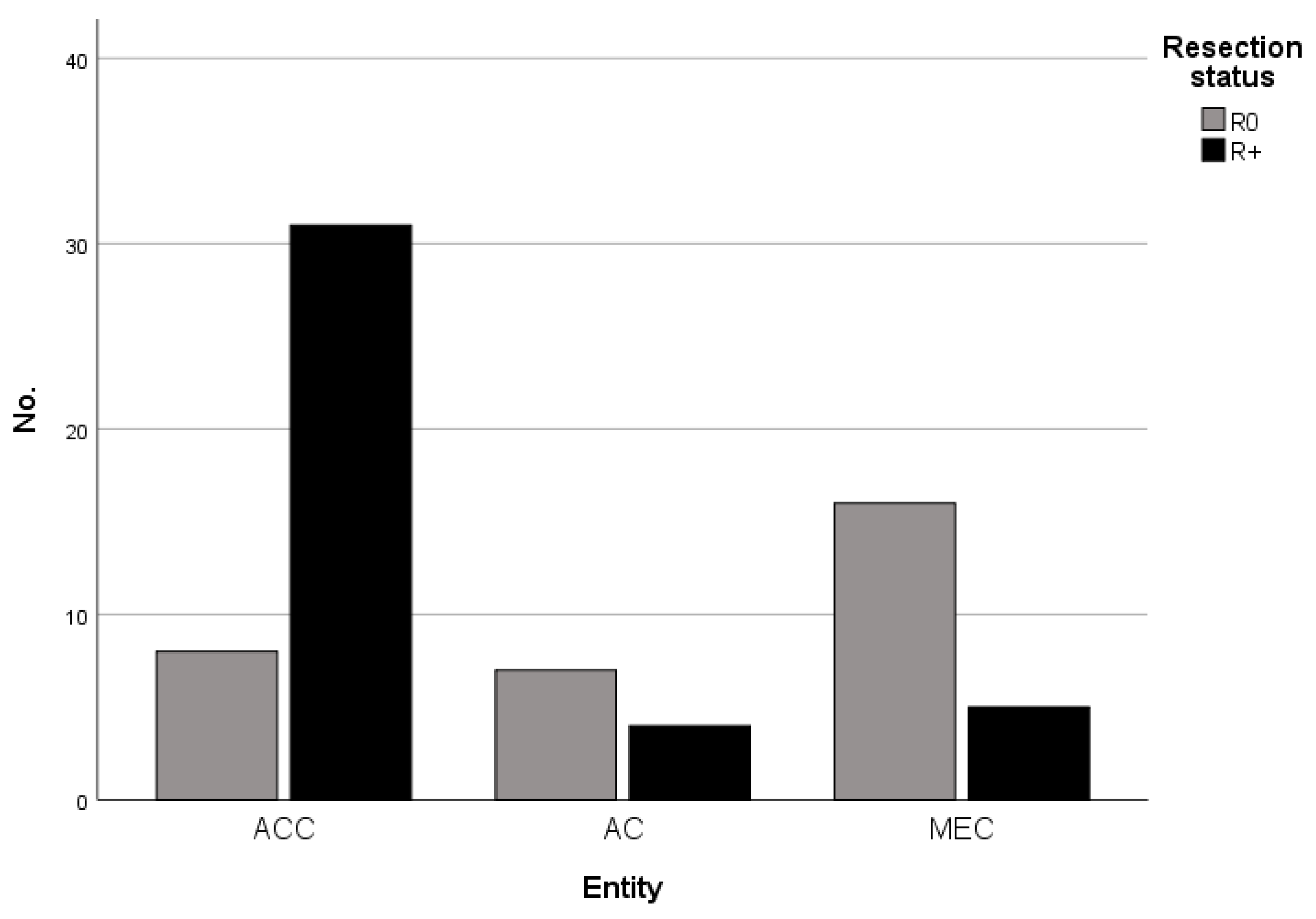
3.3. Therapeutic Procedures
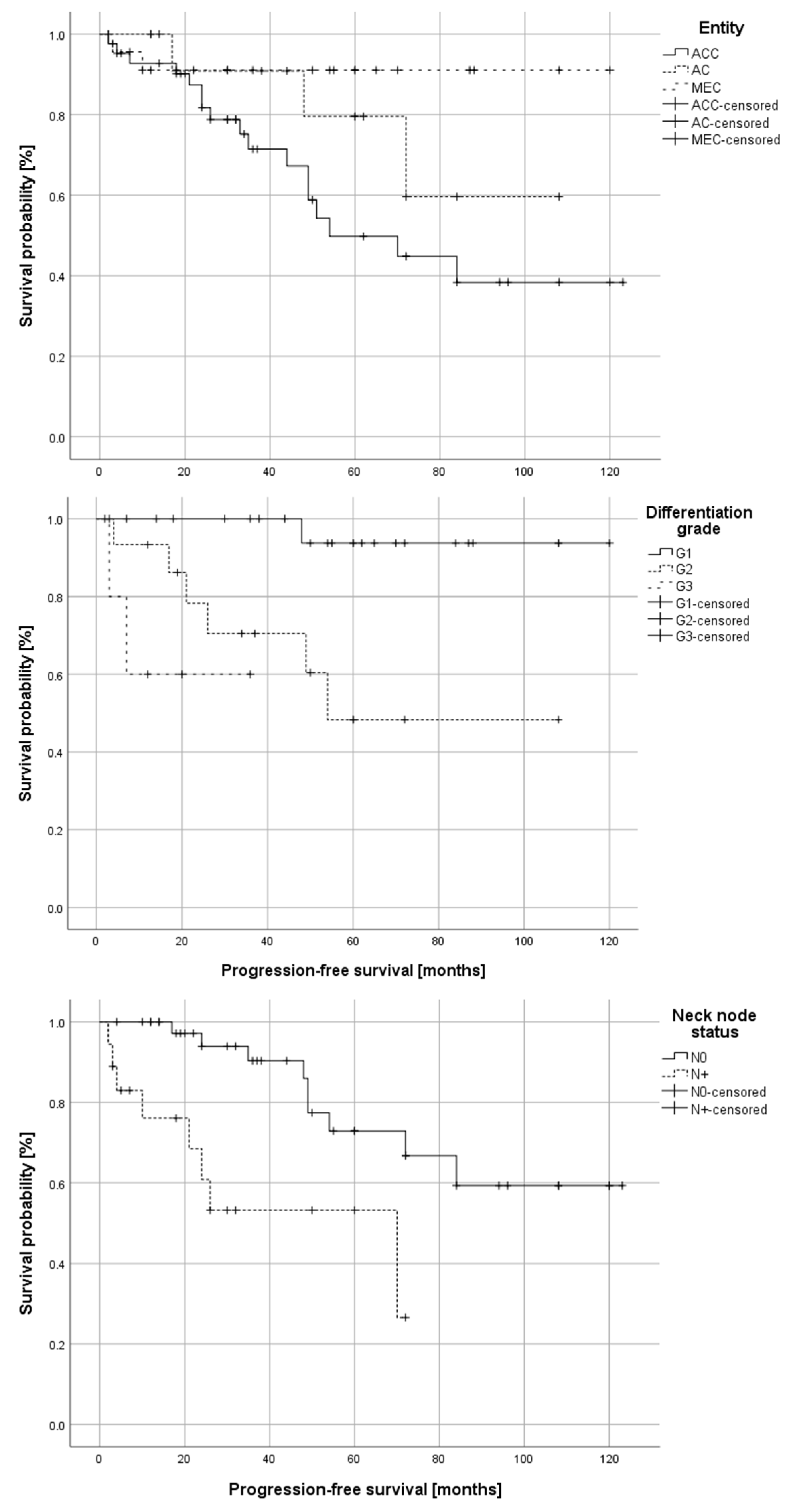
3.4. Disease Recurrence and Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Speight, P.M.; Palmer, S.; Moles, D.R.; Downer, M.C.; Smith, D.H.; Henriksson, M.; Augustovski, F. The cost-effectiveness of screening for oral cancer in primary care. Health Technol. Assess. 2006, 10, 1–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carvalho, A.L.; Nishimoto, I.N.; Califano, J.A.; Kowalski, L.P. Trends in incidence and prognosis for head and neck cancer in the United States: A site-specific analysis of the SEER database. Int. J. Cancer 2005, 114, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; Guzzo, M.; Locati, L.D.; McGurk, M.; Prott, F.J. Major and minor salivary gland tumours. Crit. Rev. Oncol. Hematol. 2020, 152, 102959. [Google Scholar] [CrossRef] [PubMed]
- Namboodiripad, P.C. A review: Immunological markers for malignant salivary gland tumors. J. Oral. Biol. Craniofac. Res. 2014, 4, 127–134. [Google Scholar] [CrossRef] [Green Version]
- Ettl, T.; Schwarz-Furlan, S.; Gosau, M.; Reichert, T.E. Salivary gland carcinomas. Oral. Maxillofac. Surg. 2012, 16, 267–283. [Google Scholar] [CrossRef]
- Buchner, A.; Merrell, P.W.; Carpenter, W.M. Relative frequency of intra-oral minor salivary gland tumors: A study of 380 cases from northern California and comparison to reports from other parts of the world. J. Oral. Pathol. Med. 2007, 36, 207–214. [Google Scholar] [CrossRef]
- Pires, F.R.; Pringle, G.A.; de Almeida, O.P.; Chen, S.Y. Intra-oral minor salivary gland tumors: A clinicopathological study of 546 cases. Oral. Oncol. 2007, 43, 463–470. [Google Scholar] [CrossRef]
- Gontarz, M.; Bargiel, J.; Gąsiorowski, K.; Marecik, T.; Szczurowski, P.; Zapała, J.; Wyszyńska-Pawelec, G. Epidemiology of Primary Epithelial Salivary Gland Tumors in Southern Poland-A 26-Year, Clinicopathologic, Retrospective Analysis. J. Clin. Med. 2021, 10, 1663. [Google Scholar] [CrossRef]
- Wahlberg, P.; Anderson, H.; Biorklund, A.; Moller, T.; Perfekt, R. Carcinoma of the parotid and submandibular glands--a study of survival in 2465 patients. Oral Oncol. 2002, 38, 706–713. [Google Scholar] [CrossRef]
- Spiro, R.H.; Koss, L.G.; Hajdu, S.I.; Strong, E.W. Tumors of minor salivary origin. A clinicopathologic study of 492 cases. Cancer 1973, 31, 117–129. [Google Scholar] [CrossRef]
- Trenkic Bozinovic, M.; Krasic, D.; Katic, V.; Krstic, M. A retrospective review of 139 major and minor salivary gland tumors. Med. Glas. 2015, 12, 73–78. [Google Scholar]
- Guzzo, M.; Locati, L.D.; Prott, F.J.; Gatta, G.; McGurk, M.; Licitra, L. Major and minor salivary gland tumors. Crit. Rev. Oncol. Hematol. 2010, 74, 134–148. [Google Scholar] [CrossRef]
- Moratin, J.; Ledermann, A.; Schulz, A.D.; Metzger, K.; Ristow, O.; Hofele, C.; Engel, M.; Hoffmann, J.; Freier, K.; Lang, K.; et al. Neck involvement and disease recurrence in adenoid cystic carcinoma of the minor salivary glands: The role of surgery in primary and progressive disease. Int. J. Oral. Maxillofac. Surg. 2020, 10, 1663. [Google Scholar] [CrossRef]
- Vander Poorten, V.; Hunt, J.; Bradley, P.J.; Haigentz, M., Jr.; Rinaldo, A.; Mendenhall, W.M.; Suarez, C.; Silver, C.; Takes, R.P.; Ferlito, A. Recent trends in the management of minor salivary gland carcinoma. Head. Neck 2014, 36, 444–455. [Google Scholar] [CrossRef]
- Moratin, J.; Metzger, K.; Kansy, K.; Ristow, O.; Engel, M.; Hoffmann, J.; Flechtenmacher, C.; Freier, K.; Freudlsperger, C.; Horn, D. The prognostic significance of the lymph node ratio in oral cancer differs for anatomical subsites. Int. J. Oral. Maxillofac. Surg. 2020, 49, 558–563. [Google Scholar] [CrossRef]
- Lombardi, D.; McGurk, M.; Vander Poorten, V.; Guzzo, M.; Accorona, R.; Rampinelli, V.; Nicolai, P. Surgical treatment of salivary malignant tumors. Oral. Oncol. 2017, 65, 102–113. [Google Scholar] [CrossRef]
- Klussmann, J.P.; Ponert, T.; Mueller, R.P.; Dienes, H.P.; Guntinas-Lichius, O. Patterns of lymph node spread and its influence on outcome in resectable parotid cancer. Eur. J. Surg. Oncol. 2008, 34, 932–937. [Google Scholar] [CrossRef]
- Carrillo, J.F.; Maldonado, F.; Carrillo, L.C.; Ramirez-Ortega, M.C.; Pizano, J.G.; Melo, C.; Chanona, J.G.; Luna-Ortiz, K.; Ocana, L.F. Prognostic factors in patients with minor salivary gland carcinoma of the oral cavity and oropharynx. Head. Neck 2011, 33, 1406–1412. [Google Scholar] [CrossRef]
- Jang, S.; Patel, P.N.; Kimple, R.J.; McCulloch, T.M. Clinical Outcomes and Prognostic Factors of Adenoid Cystic Carcinoma of the Head and Neck. Anticancer. Res. 2017, 37, 3045–3052. [Google Scholar] [CrossRef]
- Ferrarotto, R.; Mitani, Y.; McGrail, D.J.; Li, K.; Karpinets, T.V.; Bell, D.; Frank, S.J.; Song, X.; Kupferman, M.E.; Liu, B.; et al. Proteogenomic Analysis of Salivary Adenoid Cystic Carcinomas Defines Molecular Subtypes and Identifies Therapeutic Targets. Clin. Cancer Res. 2021, 27, 852–864. [Google Scholar] [CrossRef]
- Feeney, L.; Hapuarachi, B.; Adderley, H.; Rack, S.; Morgan, D.; Walker, R.; Rauch, R.; Herz, E.; Kaye, J.; Harrington, K.; et al. Clinical disease course and survival outcomes following disease recurrence in adenoid cystic carcinoma with and without NOTCH signaling pathway activation. Oral. Oncol. 2022, 133, 106028. [Google Scholar] [CrossRef]
- Yan, K.; Yesensky, J.; Hasina, R.; Agrawal, N. Genomics of mucoepidermoid and adenoid cystic carcinomas. Laryngoscope Investig. Otolaryngol. 2018, 3, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freitag, V.; Lettmaier, S.; Semrau, S.; Hecht, M.; Mantsopoulos, K.; Muller, S.K.; Traxdorf, M.; Iro, H.; Agaimy, A.; Fietkau, R.; et al. High-grade salivary gland cancer: Is surgery followed by radiotherapy an adequate treatment to reach tumor control? Results from a tertiary referral centre focussing on incidence and management of distant metastases. Eur. Arch. Otorhinolaryngol. 2022, 279, 2553–2563. [Google Scholar] [CrossRef]
- Geiger, J.L.; Ismaila, N.; Beadle, B.; Caudell, J.J.; Chau, N.; Deschler, D.; Glastonbury, C.; Kaufman, M.; Lamarre, E.; Lau, H.Y.; et al. Management of Salivary Gland Malignancy: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1909–1941. [Google Scholar] [CrossRef] [PubMed]
- Terhaard, C.H.; Lubsen, H.; Van der Tweel, I.; Hilgers, F.J.; Eijkenboom, W.M.; Marres, H.A.; Tjho-Heslinga, R.E.; de Jong, J.M.; Roodenburg, J.L.; Dutch, H.; et al. Salivary gland carcinoma: Independent prognostic factors for locoregional control, distant metastases, and overall survival: Results of the Dutch head and neck oncology cooperative group. Head. Neck 2004, 26, 681–692. [Google Scholar] [CrossRef] [PubMed]
- Zeidan, Y.H.; Pekelis, L.; An, Y.; Holsinger, F.C.; Kong, C.S.; Chang, D.T.; Le, Q.T. Survival benefit for adjuvant radiation therapy in minor salivary gland cancers. Oral. Oncol. 2015, 51, 438–445. [Google Scholar] [CrossRef]
- Wang, X.; Luo, Y.; Li, M.; Yan, H.; Sun, M.; Fan, T. Management of salivary gland carcinomas—A review. Oncotarget 2017, 8, 3946–3956. [Google Scholar] [CrossRef] [Green Version]
- Lopes, M.A.; Santos, G.C.; Kowalski, L.P. Multivariate survival analysis of 128 cases of oral cavity minor salivary gland carcinomas. Head. Neck 1998, 20, 699–706. [Google Scholar] [CrossRef]
- Shi, X.; Huang, N.S.; Shi, R.L.; Wei, W.J.; Wang, Y.L.; Ji, Q.H. Prognostic value of primary tumor surgery in minor salivary-gland carcinoma patients with distant metastases at diagnosis: First evidence from a SEER-based study. Cancer Manag. Res. 2018, 10, 2163–2172. [Google Scholar] [CrossRef] [Green Version]
- Beckhardt, R.N.; Weber, R.S.; Zane, R.; Garden, A.S.; Wolf, P.; Carrillo, R.; Luna, M.A. Minor salivary gland tumors of the palate: Clinical and pathologic correlates of outcome. Laryngoscope 1995, 105, 1155–1160. [Google Scholar] [CrossRef]
- Spiro, R.H.; Thaler, H.T.; Hicks, W.F.; Kher, U.A.; Huvos, A.H.; Strong, E.W. The importance of clinical staging of minor salivary gland carcinoma. Am. J. Surg. 1991, 162, 330–336. [Google Scholar] [CrossRef]
- Al-Qurayshi, Z.; Sullivan, C.B.; Allison, D.B.; Buchakjian, M.R. Presentation and outcomes of patients with clinically T1-2, N0 parotid mucoepidermoid carcinoma: The roles of elective neck dissection and adjuvant radiotherapy. Head. Neck 2022, 44, 2151–2161. [Google Scholar] [CrossRef]
- D'Cruz, A.K.; Vaish, R.; Kapre, N.; Dandekar, M.; Gupta, S.; Hawaldar, R.; Agarwal, J.P.; Pantvaidya, G.; Chaukar, D.; Deshmukh, A.; et al. Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer. N. Engl. J. Med. 2015, 373, 521–529. [Google Scholar] [CrossRef]
- Ning, C.; Zhao, T.; Wang, Z.; Li, D.; Kou, Y.; Huang, S. Cervical lymph node metastases in salivary gland adenoid cystic carcinoma: A systematic review and meta-analysis. Cancer Manag. Res. 2018, 10, 1677–1685. [Google Scholar] [CrossRef] [Green Version]
- Amit, M.; Binenbaum, Y.; Sharma, K.; Ramer, N.; Ramer, I.; Agbetoba, A.; Glick, J.; Yang, X.; Lei, D.; Bjørndal, K.; et al. Incidence of cervical lymph node metastasis and its association with outcomes in patients with adenoid cystic carcinoma. An international collaborative study. Head Neck 2015, 37, 1032–1037. [Google Scholar] [CrossRef] [Green Version]
- Song, X.M.; Yang, G.; Tu, Z.W.; Wang, L. Is prophylactic neck irradiation indicated for patients with cN0 adenoid cystic carcinoma of the paranasal sinuses? Radiother. Oncol. 2022, 173, 292–298. [Google Scholar] [CrossRef]
- Moratin, J.; Horn, D.; Metzger, K.; Ristow, O.; Flechtenmacher, C.; Engel, M.; Hoffmann, J.; Freier, K.; Freudlsperger, C. Squamous cell carcinoma of the mandible—Patterns of metastasis and disease recurrence in dependence of localization and therapy. J. Craniomaxillofac Surg. 2020, 48, 1158–1163. [Google Scholar] [CrossRef]
- Atallah, S.; Moya-Plana, A.; Malard, O.; Poissonnet, G.; Fakhry, N.; Bettoni, J.; Gallet, P.; Ransy, P.; Vergez, S.; De Gabory, L.; et al. Should a neck dissection be performed on patients with cN0 adenoid cystic carcinoma? A REFCOR propensity score matching study. Eur. J. Cancer 2020, 130, 250–258. [Google Scholar] [CrossRef]
- Cordesmeyer, R.; Kauffmann, P.; Laskawi, R.; Rau, A.; Bremmer, F. The incidence of occult metastasis and the status of elective neck dissection in salivary adenoid cystic carcinoma: A single center study. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2018, 125, 516–519. [Google Scholar] [CrossRef] [Green Version]
- Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Werning, J.W.; Hinerman, R.W.; Villaret, D.B. Radiotherapy alone or combined with surgery for adenoid cystic carcinoma of the head and neck. Head Neck 2004, 26, 154–162. [Google Scholar] [CrossRef]
- Chen, A.M.; Garcia, J.; Granchi, P.J.; Johnson, J.; Eisele, D.W. Late recurrence from salivary gland cancer: When does "cure" mean cure? Cancer 2008, 112, 340–344. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, B.; Copelli, C.; Cocchi, R.; Ferrari, S.; Pederneschi, N.; Sesenna, E. Adenoid cystic carcinoma of intraoral minor salivary glands. Oral. Oncol. 2008, 44, 1026–1031. [Google Scholar] [CrossRef] [PubMed]
- DeAngelis, A.F.; Tsui, A.; Wiesenfeld, D.; Chandu, A. Outcomes of patients with adenoid cystic carcinoma of the minor salivary glands. Int. J. Oral. Maxillofac. Surg. 2011, 40, 710–714. [Google Scholar] [CrossRef]
- Ishida, E.; Ogawa, T.; Rokugo, M.; Ishikawa, T.; Wakamori, S.; Ohkoshi, A.; Usubuchi, H.; Higashi, K.; Ishii, R.; Nakanome, A.; et al. Management of adenoid cystic carcinoma of the head and neck: A single-institute study with over 25-year follow-up. Head. Face Med. 2020, 16, 14. [Google Scholar] [CrossRef] [PubMed]
- Horn, D.; Zittel, S.; Moratin, J.; Metzger, K.; Ristow, O.; Krisam, J.; Bodem, J.; Engel, M.; Freudlsperger, C.; Hoffmann, J.; et al. Prospective feasibility analysis of salvage surgery in recurrent oral cancer in terms of quality of life. Oral. Oncol. 2020, 102, 104580. [Google Scholar] [CrossRef]
- Horn, D.; Bodem, J.; Freudlsperger, C.; Zittel, S.; Weichert, W.; Hoffmann, J.; Freier, K. Outcome of heavily pretreated recurrent oral squamous cell carcinoma after salvage resection: A monocentric retrospective analysis. J. Craniomaxillofac Surg. 2016, 44, 1061–1066. [Google Scholar] [CrossRef]
- Moratin, J.; Mrosek, J.; Horn, D.; Metzger, K.; Ristow, O.; Zittel, S.; Engel, M.; Freier, K.; Hoffmann, J.; Freudlsperger, C. Full-Thickness Tumor Resection of Oral Cancer Involving the Facial Skin-Microsurgical Reconstruction of Extensive Defects after Radical Treatment of Advanced Squamous Cell Carcinoma. Cancers 2021, 13, 2122. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Number of Cases (%) |
|---|---|
| Gender | |
| Female | 41 (50.6) |
| Male | 40 (49.4) |
| Age | |
| <20 years | 2 (2.5) |
| 21–40 years | 13 (16) |
| 41–60 years | 31 (42) |
| 61–80 years | 29 (35.8) |
| >81 years | 3 (3.7) |
| Tumor Localizations | |
| Hard palate | 48 (59.3) |
| Soft palate | 6 (7.4) |
| Mandible | 11 (13.6) |
| Planum buccale | 11 (13.6) |
| Tongue | 2 (2.5) |
| Lip | 3 (3.6) |
| Tumor Entities | |
| Adenoid cystic carcinoma (ACC) | 43 (53.1%) |
| Adenocarcinoma not otherwise specified (AC-NOS) | 14 (17.3%) |
| Mucoepidermoid Carcinoma (MEC) | 24 (29.6%) |
| ACC | AC-NOS | MEC | p-Value | |
|---|---|---|---|---|
| Mean patient age (years) | 54.7 ± 14.8 | 64.4 ± 12.8 | 49.8 ± 17.3 | 0.02 |
| Gender | ||||
| Male | 21 (52.5%) | 8 (20%) | 11 (27.5%) | 0.79 |
| Female | 22 (53.7%) | 6 (14.6%) | 13 (31.7%) | |
| Pathological tumor stage (T) | ||||
| T1 | 5 (11.6%) | 5 (35.7%) | 14 (58.4%) | 0.002 |
| T2 | 5 (11.6%) | 4 (28.6%) | 2 (8.3%) | |
| T3 | 8 (18.6%) | 1 (7.1%) | 2 (8.3%) | |
| T4 | 25 (58.2%) | 4 (28.6%) | 6 (25%) | |
| Grading (G) | ||||
| G1 | 0 | 8 (72.7%) | 16 (84.2%) | <0.001 |
| G2 | 12 (80%) | 2 (18.2%) | 2 (10.5%) | |
| G3 | 3 (20%) | 1 (9.1%) | 1 (5.3%) | |
| Neck node metastases (N) | ||||
| N0 | 22 (61.1%) | 10 (90.9%) | 9 (75%) | 0.154 |
| N+ | 14 (38.9%) | 1 (9.1%) | 3 (25%) | |
| Resection status (R) | ||||
| R0 | 10 (23.3%) | 9 (64.3%) | 21 (87.5%) | <0.001 |
| R + (R1/2/X) | 33 (76.7%) | 5 (35.7%) | 3 (12.5%) | |
| Perineural invasion (PN) | ||||
| PN0 | 13 (31.7%) | 9 (64.3%) | 19 (86.4%) | <0.001 |
| PN1 | 28 (68.3%) | 5 (35.7%) | 3 (13.6%) | |
| Lymphatic invasion (L) | ||||
| L0 | 32 (76.2%) | 13 (92.9%) | 22 (95.7%) | 0.073 |
| L1 | 10 (23.8%) | 1 (7.1%) | 1 (4.3%) | |
| Vascular invasion (V) | ||||
| V0 | 38 (90.5%) | 13 (92.9%) | 22 (95.7%) | 0.751 |
| V1 | 4 (9.5%) | 1 (7.1%) | 1 (4.3%) | |
| Adjuvant radiotherapy (RT) | ||||
| No adjuvant RT | 8 (18.6%) | 10 (71.4%) | 20 (83.3%) | <0.001 |
| Adjuvant RT | 35 (81.4%) | 4 (28.6%) | 4 (16.7%) |
| ACC | AC-NOS | MEC | p-Value | |
|---|---|---|---|---|
| Disease recurrence | 17 (77.3%) | 3 (13.6%) | 2 (9.1%) | 0.02 |
| Type of disease recurrence | ||||
| Local recurrence | 8 (80%) | 2 (20%) | 0 | |
| Distant metastases | 4 (57.1%) | 1 (14.3%) | 2 (28.6%) |
| Hazard Ratio (95-CI) | p-Value | |
|---|---|---|
| T Stage | 3.1 (0.9–10.1) | 0.067 |
| N0/N+ | 14 (1.7–114.1) | 0.014 |
| Tumor entity | 1.3 (0.5–3.5) | 0.564 |
| Differentiation grade | 1.6 (0.3–8.0) | 0.558 |
| Patient age | 1.1 (1.0–1.1) | 0.098 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moratin, J.; Horn, D.; Semmelmayer, K.; Ristow, O.; Engel, M.; Hoffmann, J.; Bleymehl, M.; Held, T.; Zittel, S.; Freudlsperger, C. Surgical Treatment of Carcinomas of the Oral Minor Salivary Glands—Oncological Outcome in Dependence of Tumor Entity and Therapeutic Strategies. Cancers 2023, 15, 3895. https://doi.org/10.3390/cancers15153895
Moratin J, Horn D, Semmelmayer K, Ristow O, Engel M, Hoffmann J, Bleymehl M, Held T, Zittel S, Freudlsperger C. Surgical Treatment of Carcinomas of the Oral Minor Salivary Glands—Oncological Outcome in Dependence of Tumor Entity and Therapeutic Strategies. Cancers. 2023; 15(15):3895. https://doi.org/10.3390/cancers15153895
Chicago/Turabian StyleMoratin, Julius, Dominik Horn, Karl Semmelmayer, Oliver Ristow, Michael Engel, Jürgen Hoffmann, Moritz Bleymehl, Thomas Held, Sven Zittel, and Christian Freudlsperger. 2023. "Surgical Treatment of Carcinomas of the Oral Minor Salivary Glands—Oncological Outcome in Dependence of Tumor Entity and Therapeutic Strategies" Cancers 15, no. 15: 3895. https://doi.org/10.3390/cancers15153895