
Risk of Intraepithelial Neoplasia Grade 3 or Worse (CIN3+) among Women Examined by a 5-Type HPV mRNA Test during 2003 and 2004, Followed through 2015
 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source and Study Sample
2.2. Screening Guidelines
2.3. Human Papillomavirus mRNA Testing
2.4. Outcome
2.5. Statistical Analyses
3. Results
3.1. Human Papillomavirus Status at Baseline
3.2. Cumulative Incidence of Cervical Intraepithelial Neoplasia Grade 3 or Worse
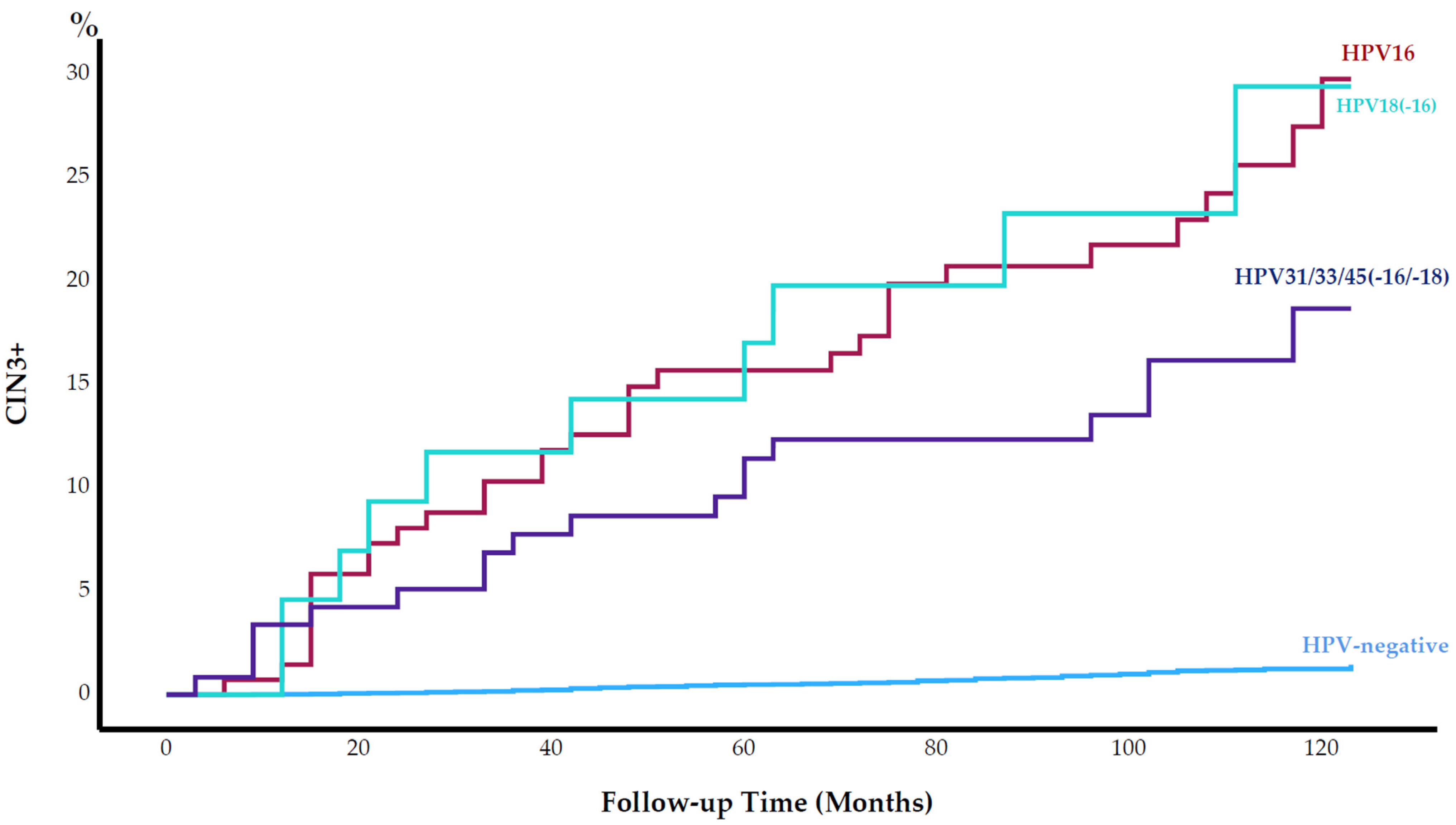
3.3. Cervical Intraepithelial Neoplasia Grade 3 or Worse by Human Papillomavirus Type
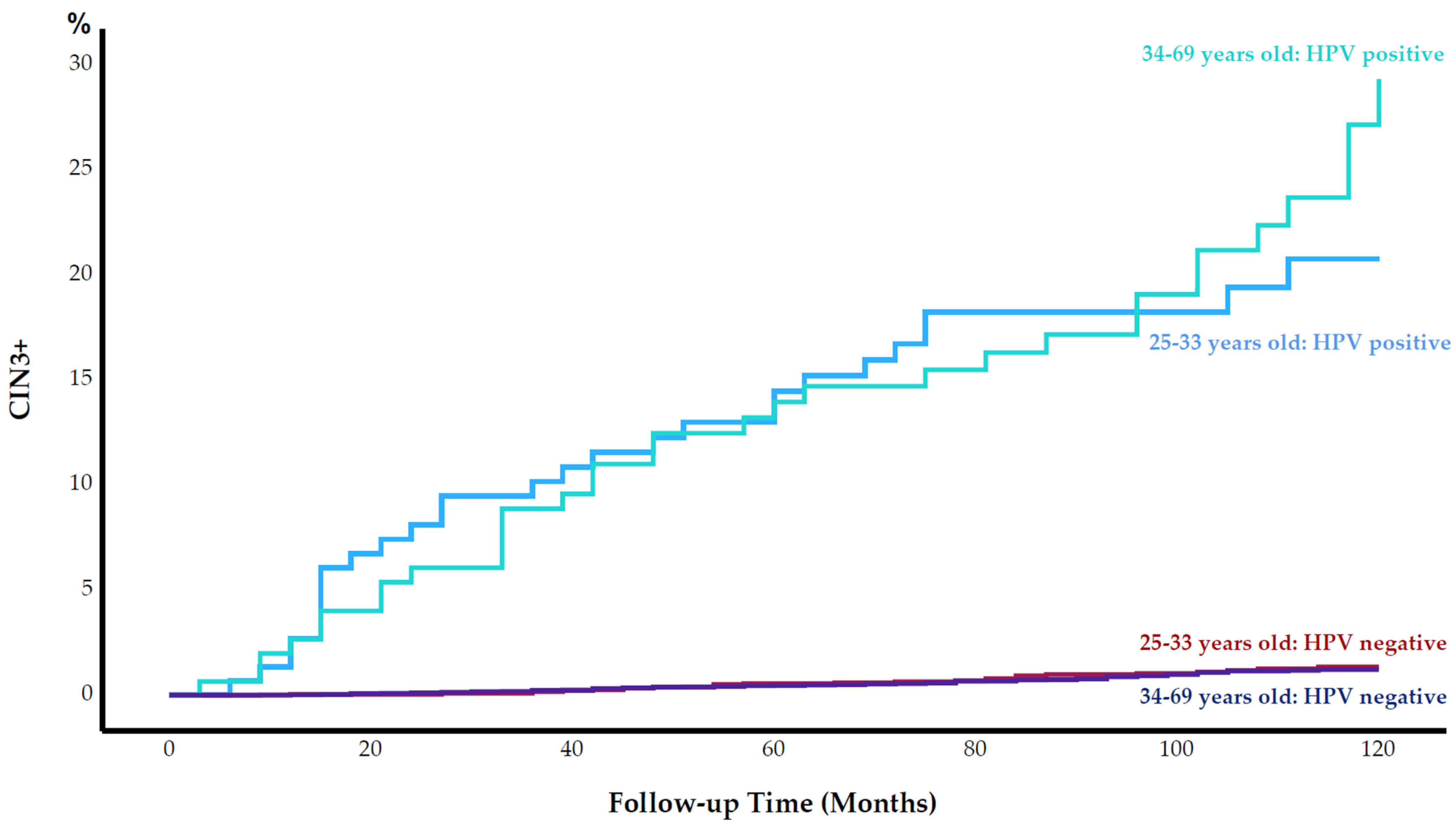
3.4. Cervical Intraepithelial Neoplasia Grade 3 or Worse by Age
3.5. Cancer Cases
4. Discussion
4.1. Cervical Intraepithelial Neoplasia Grade 3 or Worse among Human Papillomavirus-Positive Women
4.2. Cervical Intraepithelial Neoplasia Grade 3 or Worse among Human Papillomavirus-Negative Women
4.3. Age-Independent Ability to Predict Cervical Intraepithelial Neoplasia Grade 3 or Worse
4.4. Human Papillomavirus Positivity Rate
4.5. Human Papillomavirus Types Included in the mRNA Test
4.6. Cancer Cases
4.7. Strengths
4.8. Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Global Cancer Observatory. World-Source: Globocan 2020. 2021. Available online: http://gco.iarc.fr/today/data/factsheets/populations/900-world-fact-sheets.pdf (accessed on 1 April 2023).
- Cuschieri, K.S.; Cubie, H.A.; Whitley, M.W.; Gilkison, G.; Arends, M.J.; Graham, C.; McGoogan, E. Persistent high risk HPV infection associated with development of cervical neoplasia in a prospective population study. J. Clin. Pathol. 2005, 58, 946–950. [Google Scholar] [CrossRef] [Green Version]
- Ronco, G.; Giorgi-Rossi, P.; Carozzi, F.; Confortini, M.; Dalla Palma, P.; Del Mistro, A.; Ghiringhello, B.; Girlando, S.; Gillio-Tos, A.; De Marco, L.; et al. Efficacy of human papillomavirus testing for the detection of invasive cervical cancers and cervical intraepithelial neoplasia: A randomised controlled trial. Lancet Oncol. 2010, 11, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Snijders, P.J.F.; Meijer, C.J.L.M.; Berkhof, J.; Cuschieri, K.; Kocjan, B.J.; Poljak, M. Which high-risk HPV assays fulfil criteria for use in primary cervical cancer screening? Clin. Microbiol. Infect. 2015, 21, 817–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woodman, C.B.; Collins, S.I.; Young, L.S. The natural history of cervical HPV infection: Unresolved issues. Nat. Rev. Cancer 2007, 7, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Kraus, I.; Molden, T.; Holm, R.; Lie, A.K.; Karlsen, F.; Kristensen, G.B.; Skomedal, H. Presence of E6 and E7 mRNA from human papillomavirus types 16, 18, 31, 33, and 45 in the majority of cervical carcinomas. J. Clin. Microbiol. 2006, 44, 1310–1317. [Google Scholar] [CrossRef] [Green Version]
- Rad, A.; Sorbye, S.W.; Dreyer, G.; Hovland, S.; Falang, B.M.; Louw, M.; Skjeldestad, F.E. HPV types in cervical cancer tissue in South Africa: A head-to-head comparison by mRNA and DNA tests. Medicine 2017, 96, e8752. [Google Scholar] [CrossRef]
- Westre, B.; Giske, A.; Guttormsen, H.; Sorbye, S.W.; Skjeldestad, F.E. 5-type HPV mRNA versus 14-type HPV DNA test: Test performance, over-diagnosis and overtreatment in triage of women with minor cervical lesions. BMC Clin. Pathol. 2016, 16, 9. [Google Scholar] [CrossRef] [Green Version]
- Sorbye, S.W.; Fismen, S.; Gutteberg, T.J.; Mortensen, E.S.; Skjeldestad, F.E. HPV mRNA is more specific than HPV DNA in triage of women with minor cervical lesions. PLoS ONE 2014, 9, e112934. [Google Scholar] [CrossRef] [Green Version]
- Ratnam, S.; Coutlee, F.; Fontaine, D.; Bentley, J.; Escott, N.; Ghatage, P.; Gadag, V.; Holloway, G.; Bartellas, E.; Kum, N.; et al. Aptima HPV E6/E7 mRNA test is as sensitive as Hybrid Capture 2 Assay but more specific at detecting cervical precancer and cancer. J. Clin. Microbiol. 2011, 49, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reinholdt, K.; Juul, K.E.; Dehlendorff, C.; Munk, C.; Kjær, S.K.; Thomsen, L.T. Triage of low-grade squamous intraepithelial lesions using human papillomavirus messenger ribonucleic acid tests—A prospective population-based register study. Acta Obstet. Gynecol. Scand. 2020, 99, 204–212. [Google Scholar] [CrossRef]
- Khan, M.J.; Castle, P.E.; Lorincz, A.T.; Wacholder, S.; Sherman, M.; Scott, D.R.; Rush, B.B.; Glass, A.G.; Shiffman, M. The elevated 10-year risk of cervical precancer and cancer in women with human papillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPV testing in clinical practice. J. Natl. Cancer Inst. 2005, 97, 1072–1079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kjaer, S.K.; Frederiksen, K.; Munk, C.; Iftner, T. Long-term Absolute Risk of Cervical Intraepithelial Neoplasia Grade 3 or Worse Following Human Papillomavirus Infection: Role of Persistence. J. Natl. Cancer Inst. 2010, 102, 1478–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Registry of Norway. HPV in Primary Screening. 2018. Available online: https://www.kreftregisteret.no/screening/livmorhalsprogrammet/Helsepersonell/screeningstrategi-og-nasjonale-retningslinjer/HPV-i-primarscreening/ (accessed on 1 April 2023).
- Cancer Registry of Norway. Primary HPV Test—Now Also for Women under 34. 2023. Available online: https://www.kreftregisteret.no/screening/livmorhalsprogrammet/hpv/ (accessed on 1 April 2023).
- Szarewski, A.; Mesher, D.; Cadman, L.; Austin, J.; Ashdown-Barr, L.; Ho, L.; Terry, G.; Liddle, S.; Young, M.; Stoler, M.; et al. Comparison of seven tests for high-grade cervical intraepithelial neoplasia in women with abnormal smears: The Predictors 2 study. J. Clin. Microbiol. 2012, 50, 1867–1873. [Google Scholar] [CrossRef] [Green Version]
- Arbyn, M.; Roelens, J.; Cuschieri, K.; Cuzick, J.; Szarewski, A.; Ratnam, S.; Reuschenbach, M.; Belinson, S.; Belinson, J.L.; Monsonego, J. The APTIMA HPV assay versus the Hybrid Capture 2 test in triage of women with ASC-US or LSIL cervical cytology: A meta-analysis of the diagnostic accuracy. Int. J. Cancer 2013, 132, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Sorbye, S.W.; Fismen, S.; Gutteberg, T.J.; Mortensen, E.S.; Skjeldestad, F.E. Primary cervical cancer screening with an HPV mRNA test: A prospective cohort study. BMJ Open 2016, 6, e011981. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC). Cytopathology of the Uterine Cervix—Digital Atlas (The Bethesda System). 2021. Available online: https://screening.iarc.fr/atlasclassifbethesda.php (accessed on 1 April 2023).
- World Health Organization (WHO). Comprehensive Cervical Cancer Control: A guide to essential practice. In Comprehensive Cervical Cancer Control: A Guide to Essential Practice; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Cancer Registry of Norway. Masseundersøkelsen mot Livmorhalskreft. 2008. Available online: www.kreftregisteret.no/globalassets/publikasjoner-og-rapporter/livmorhalskreft/rapport_screeningintervall.pdf (accessed on 1 April 2023).
- World Health Organization (WHO). WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, 2nd ed.; WHO: Geneva, Switzerland, 2021.
- Riibe, M.O.; Sorbye, S.W.; Simonsen, G.S.; Sundsfjord, A.; Ekgren, J.; Maltau, J.M. Risk of cervical intraepithelial neoplasia grade 3 or higher (CIN3+) among women with HPV-test in 1990–1992, a 30-year follow-up study. Infect. Agents Cancer 2021, 16, 46. [Google Scholar] [CrossRef]
- Rad, A.; Sørbye, S.W.; Brenn, T.; Tiwari, S.; Løchen, M.-L.; Skjeldestad, F.E. 13-Type HPV DNA Test versus 5-Type HPV mRNA Test in Triage of Women Aged 25–33 Years with Minor Cytological Abnormalities–6 Years of Follow-Up. Int. J. Environ. Res. Public Health 2023, 20, 4119. [Google Scholar] [CrossRef]
- Cuzick, J.; Cadman, L.; Mesher, D.; Austin, J.; Ashdown-Barr, L.; Ho, L.; Terry, G.; Liddle, S.; Wright, C.; Lyons, D.; et al. Comparing the performance of six human papillomavirus tests in a screening population. Br. J. Cancer 2013, 108, 908–913. [Google Scholar] [CrossRef]
- Katki, H.A.; Kinney, W.K.; Fetterman, B.; Lorey, T.; Poitras, N.E.; Cheung, L.; Demuth, F.; Schiffman, M.; Wacholder, S.; Castle, P.E. Cervical cancer risk for women undergoing concurrent testing for human papillomavirus and cervical cytology: A population-based study in routine clinical practice. Lancet Oncol. 2011, 12, 663–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, G.; Dillner, J.; Elfstrom, K.M.; Tunesi, S.; Snijders, P.J.; Arbyn, M.; Kitchener, H.; Segnan, N.; Gilham, C.; Giorgi-Rossi, P.; et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: Follow-Up of four European randomised controlled trials. Lancet 2014, 383, 524–532. [Google Scholar] [CrossRef]
- Ramakrishnan, S.; Partricia, S.; Mathan, G. Overview of high-risk HPV’s 16 and 18 infected cervical cancer: Pathogenesis to prevention. Biomed. Pharmacother. 2015, 70, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Powell, N.G.; Hibbitts, S.J.; Boyde, A.M.; Newcombe, R.G.; Tristram, A.J.; Fiander, A.N. The risk of cervical cancer associated with specific types of human papillomavirus: A case-control study in a UK population. Int. J. Cancer 2011, 128, 1676–1682. [Google Scholar] [CrossRef] [PubMed]
- Moberg, M.; Gustavsson, I.; Wilander, E.; Gyllensten, U. High viral loads of human papillomavirus predict risk of invasive cervical carcinoma. Br. J. Cancer 2005, 92, 891–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans: Human Papillomaviruses; International Agency for Research on Cancer: Lyon, France, 2007; pp. 1–636.
- Castle, P.E.; Rodriguez, A.C.; Burk, R.D.; Herrero, R.; Wacholder, S.; Alfaro, M.; Morales, J.; Guillen, D.; Sherman, M.E.; Solomon, D.; et al. Short term persistence of human papillomavirus and risk of cervical precancer and cancer: Population based cohort study. Br. Med. J. 2009, 339, b2569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castle, P.E.; Glass, A.G.; Rush, B.B.; Scott, D.R.; Wentzensen, N.; Gage, J.C.; Buckland, J.; Rydzak, G.; Lorincz, A.T.; Wacholder, S. Clinical human papillomavirus detection forecasts cervical cancer risk in women over 18 years of follow-up. J. Clin. Oncol. 2012, 30, 3044–3050. [Google Scholar] [CrossRef] [PubMed]
- Naucler, P.; Ryd, W.; Tornberg, S.; Strand, A.; Wadell, G.; Hansson, B.G.; Rylander, E.; Dillner, J. HPV type-specific risks of high-grade CIN during 4 years of follow-up: A population-based prospective study. Br. J. Cancer 2007, 97, 129–132. [Google Scholar] [CrossRef] [Green Version]
- Arbyn, M.; Tommasino, M.; Depuydt, C.; Dillner, J. Are 20 human papillomavirus types causing cervical cancer? J. Pathol. 2014, 234, 431–435. [Google Scholar] [CrossRef]
- Sundstrom, K.; Dillner, J. How many Human Papillomavirus types do we need to screen for? J. Infect. Dis. 2021, 223, 1510–1511. [Google Scholar] [CrossRef]
- Nygard, M.; Hansen, B.T.; Kjaer, S.K.; Hortlund, M.; Tryggvadottir, L.; Munk, C.; Lagheden, C.; Sigurdardottir, L.G.; Campbell, S.; Liaw, K.L.; et al. Human papillomavirus genotype-specific risks for cervical intraepithelial lesions. Hum. Vaccin. Immunother. 2021, 17, 972–981. [Google Scholar] [CrossRef]
- World Health Organization. Cervical Cancer Elimination Initiative. 2021. Available online: https://www.who.int/initiatives/cervical-cancer-elimination-initiative (accessed on 1 April 2023).



{kind=link}
{kind=link}
| Eligible for Study Participation | 19,153 | |
|---|---|---|
| Exclusion Criteria | n | |
| Age < 25 years | 2020 | |
| Age > 69 years | 223 | |
| Previous diagnosis of CIN1+ | 883 | |
| Previous ASC-US+ cytology | 4756 | |
| Unsatisfactory cytology | 501 | |
| No cytology sample collected | 627 | |
| No follow-up information | 561 | |
| Total exclusions | 9571 | |
| Final study sample | 9582 |
| HPV Status * | 25–33 Years n = 2610 (%) | 34–69 Years n = 6972 (%) | Total n = 9582 (%) |
|---|---|---|---|
| HPV Negative | 94.3 | 97.8 | 96.8 |
| HPV Positive | 5.7 * | 2.2 * | 3.2 |
| HPV16 | 2.8 * | 1.0 * | 1.5 |
| HPV18 | 0.8 * | 0.3 * | 0.5 |
| HPV31/33/45 | 2.1 * | 0.9 * | 1.2 |
| Case No. | At Study Start | At Diagnosis | ||||||
|---|---|---|---|---|---|---|---|---|
| Age (yrs.) | HPV Type | Screening History Prior to Study Start | Time to Last Smear Prior to Study Start (Months) | Diagnosed in | Time from Study Start (Months) | Histological Type | Stage | |
| 1 | 38 | 45 | 1 normal smear | 32 | Regular screening | 93 | SCC | 1 |
| 2 | 39 | 16 | 8 normal smears | 23 | Regular screening | 38 | SCC | 1 |
| 3 | 41 | 18 | 3 normal smears | 34 | Delayed screening | 58 | ADC | 2B |
| 4 | 48 | Neg. | 4 normal smears | 33 | Regular screening | 28 | SCC | 1A |
| 5 | 51 | Neg. | 6 normal smears | 27 | Delayed screening | 65 | SCC | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rad, A.; Sørbye, S.W.; Tiwari, S.; Løchen, M.-L.; Skjeldestad, F.E. Risk of Intraepithelial Neoplasia Grade 3 or Worse (CIN3+) among Women Examined by a 5-Type HPV mRNA Test during 2003 and 2004, Followed through 2015. Cancers 2023, 15, 3106. https://doi.org/10.3390/cancers15123106
Rad A, Sørbye SW, Tiwari S, Løchen M-L, Skjeldestad FE. Risk of Intraepithelial Neoplasia Grade 3 or Worse (CIN3+) among Women Examined by a 5-Type HPV mRNA Test during 2003 and 2004, Followed through 2015. Cancers. 2023; 15(12):3106. https://doi.org/10.3390/cancers15123106
Chicago/Turabian StyleRad, Amir, Sveinung Wergeland Sørbye, Sweta Tiwari, Maja-Lisa Løchen, and Finn Egil Skjeldestad. 2023. "Risk of Intraepithelial Neoplasia Grade 3 or Worse (CIN3+) among Women Examined by a 5-Type HPV mRNA Test during 2003 and 2004, Followed through 2015" Cancers 15, no. 12: 3106. https://doi.org/10.3390/cancers15123106