
Robot-Assisted Magnetic Resonance Imaging-Targeted versus Systematic Prostate Biopsy; Systematic Review and Meta-Analysis
 , , , , , and
, , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials & Methods
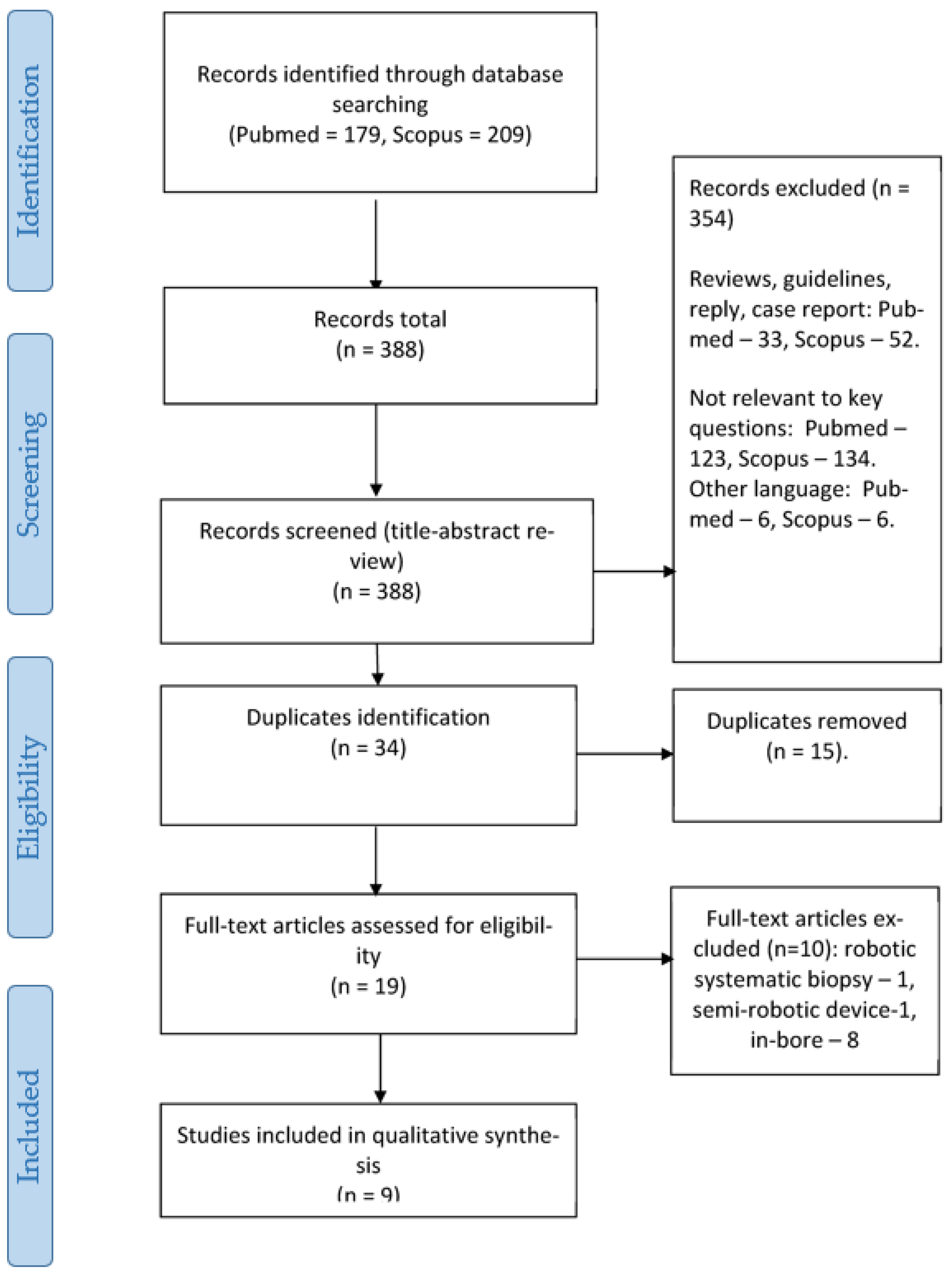
2.1. Search Strategy and Inclusion Criteria
- P—Patients with suspected PCa or on active surveillance;
- I—Robot-assisted MRI-targeted prostate biopsy;
- C—Systematic or MRI-targeted biopsy (with and without robot assistance);
- O—Detection rate of csPCa, overall detection rate of PCa, cancer detection rate per core, and complication rate;
- S—Both prospective and retrospective studies.
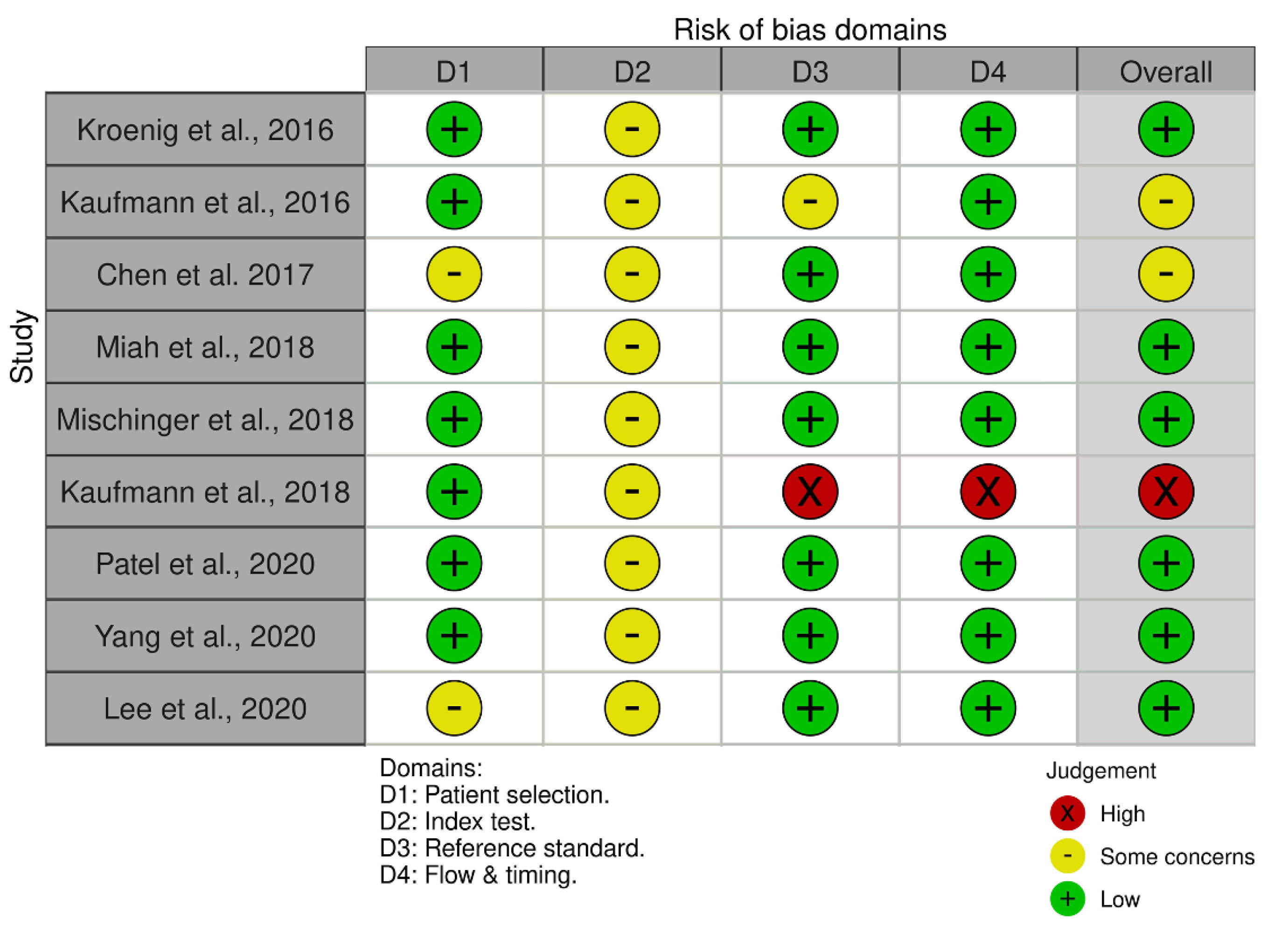
2.2. Studies’ Quality Assessment
2.3. Data Extraction
2.4. Methods of Meta-Analysis
3. Results
3.1. Demographics
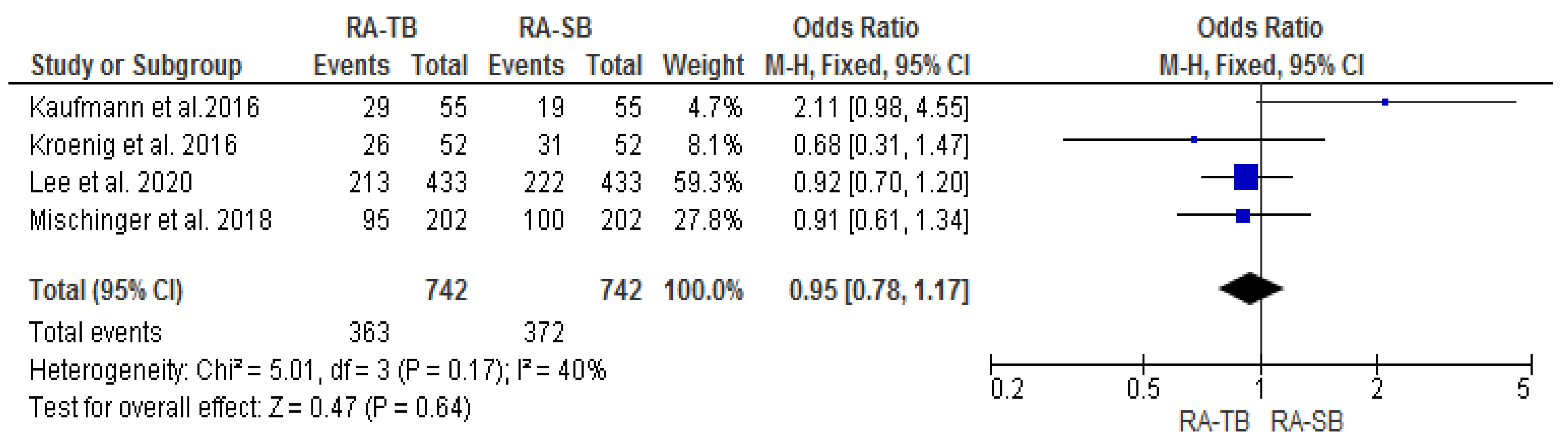
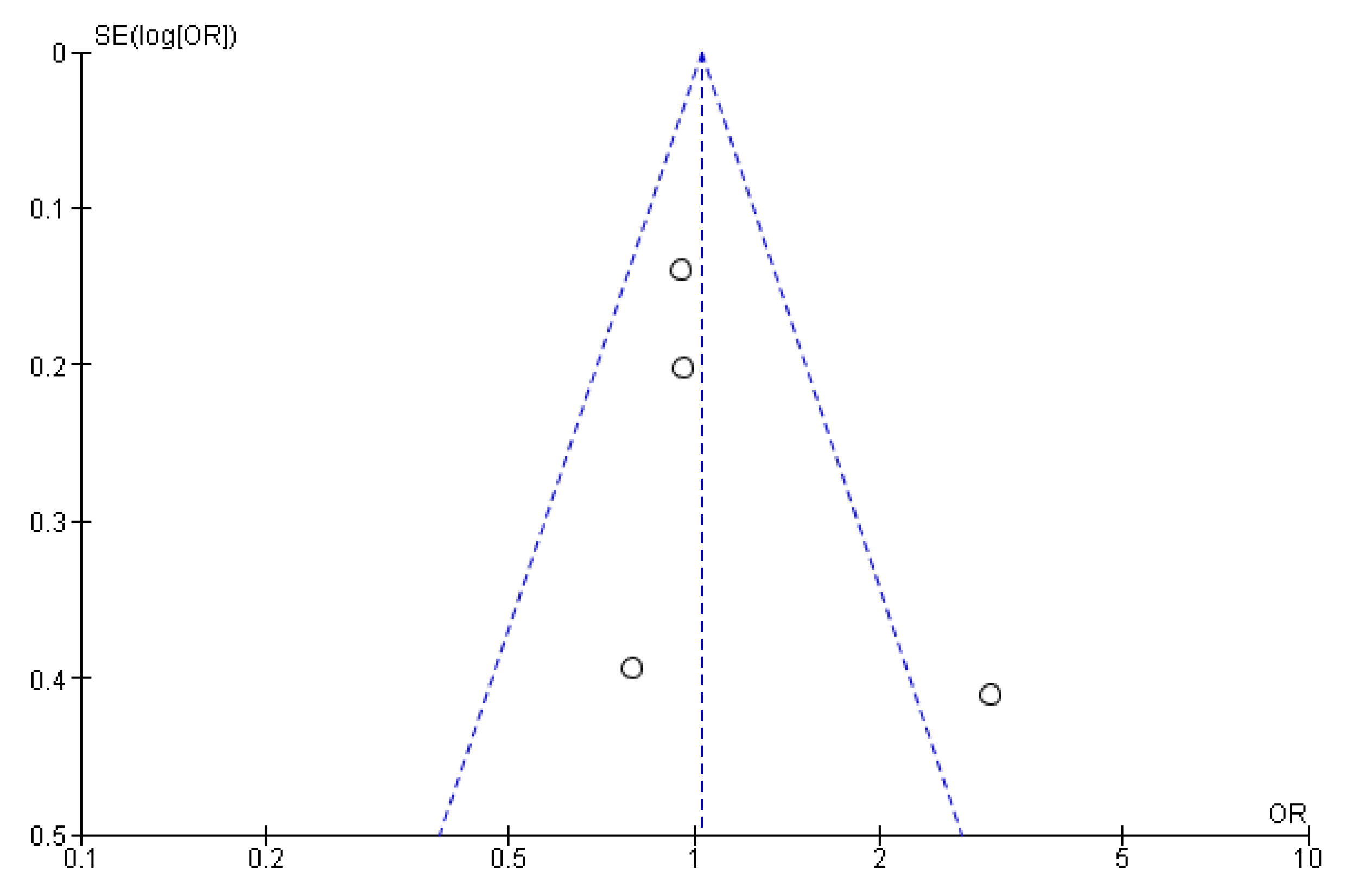
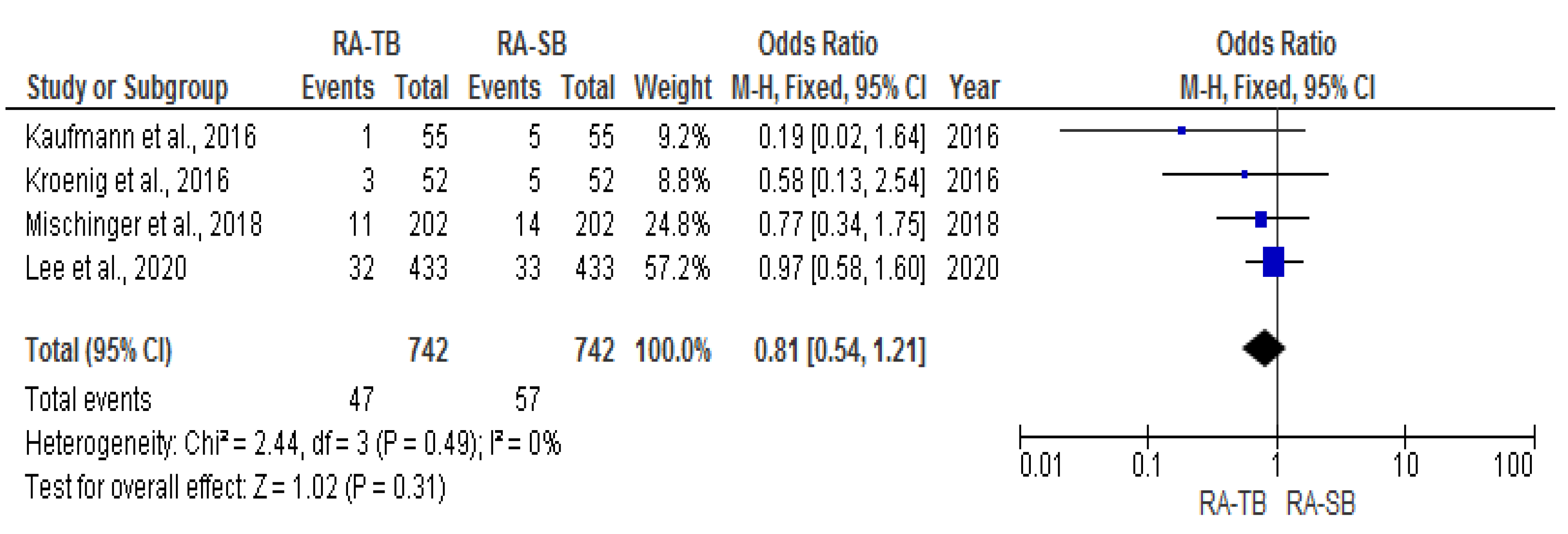
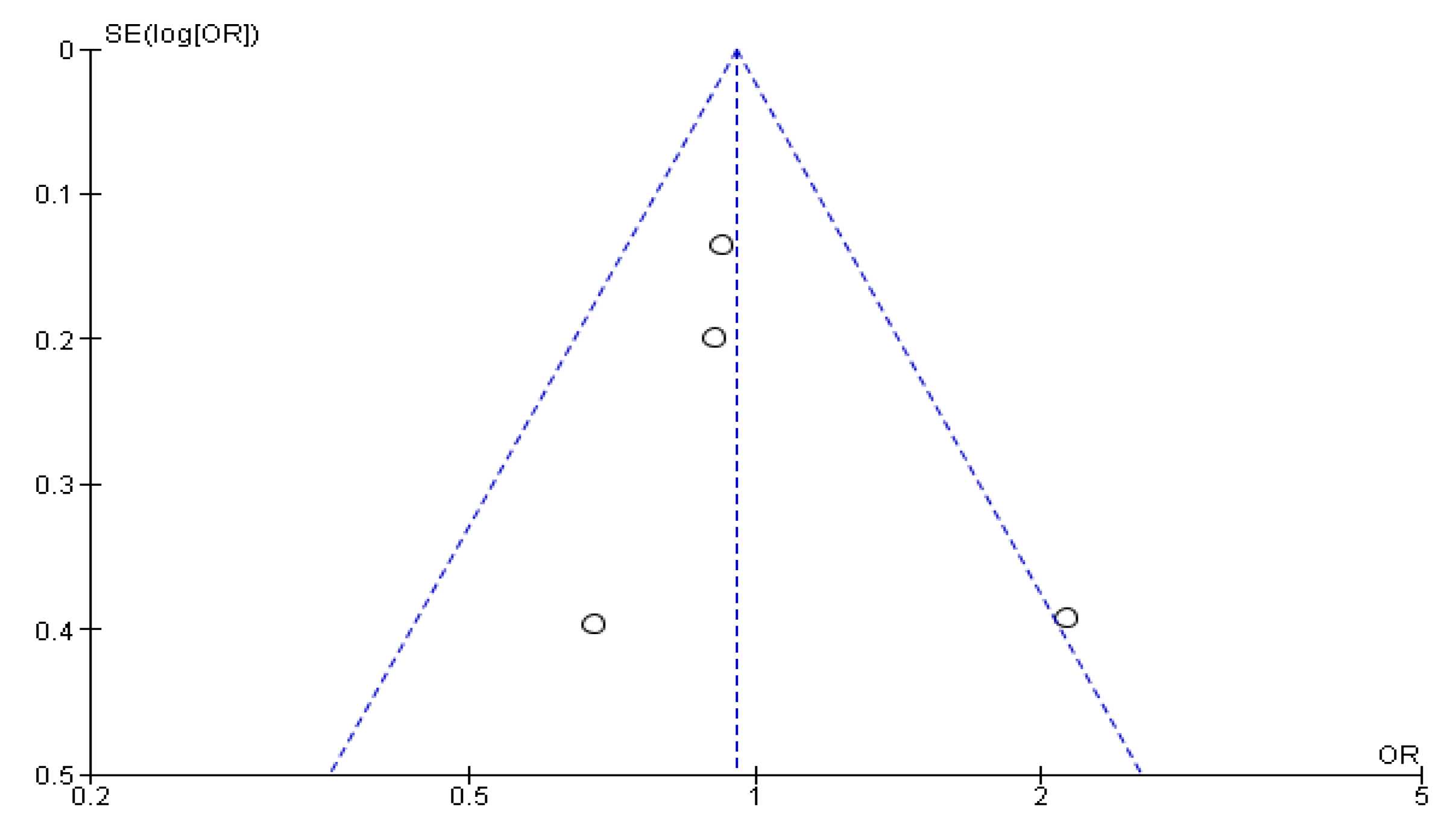
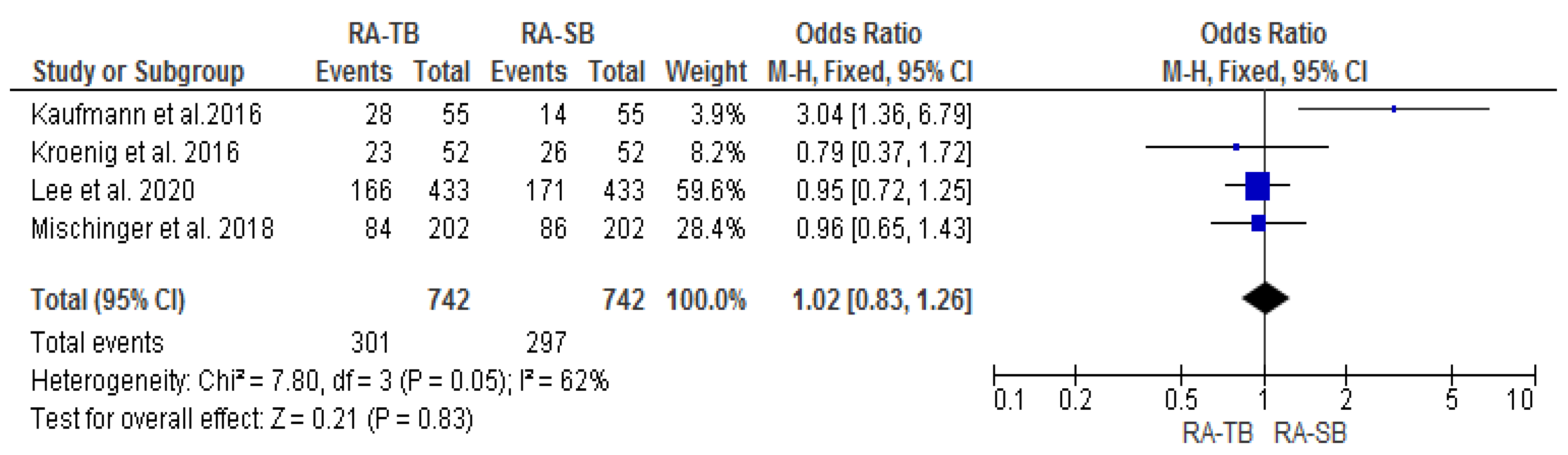
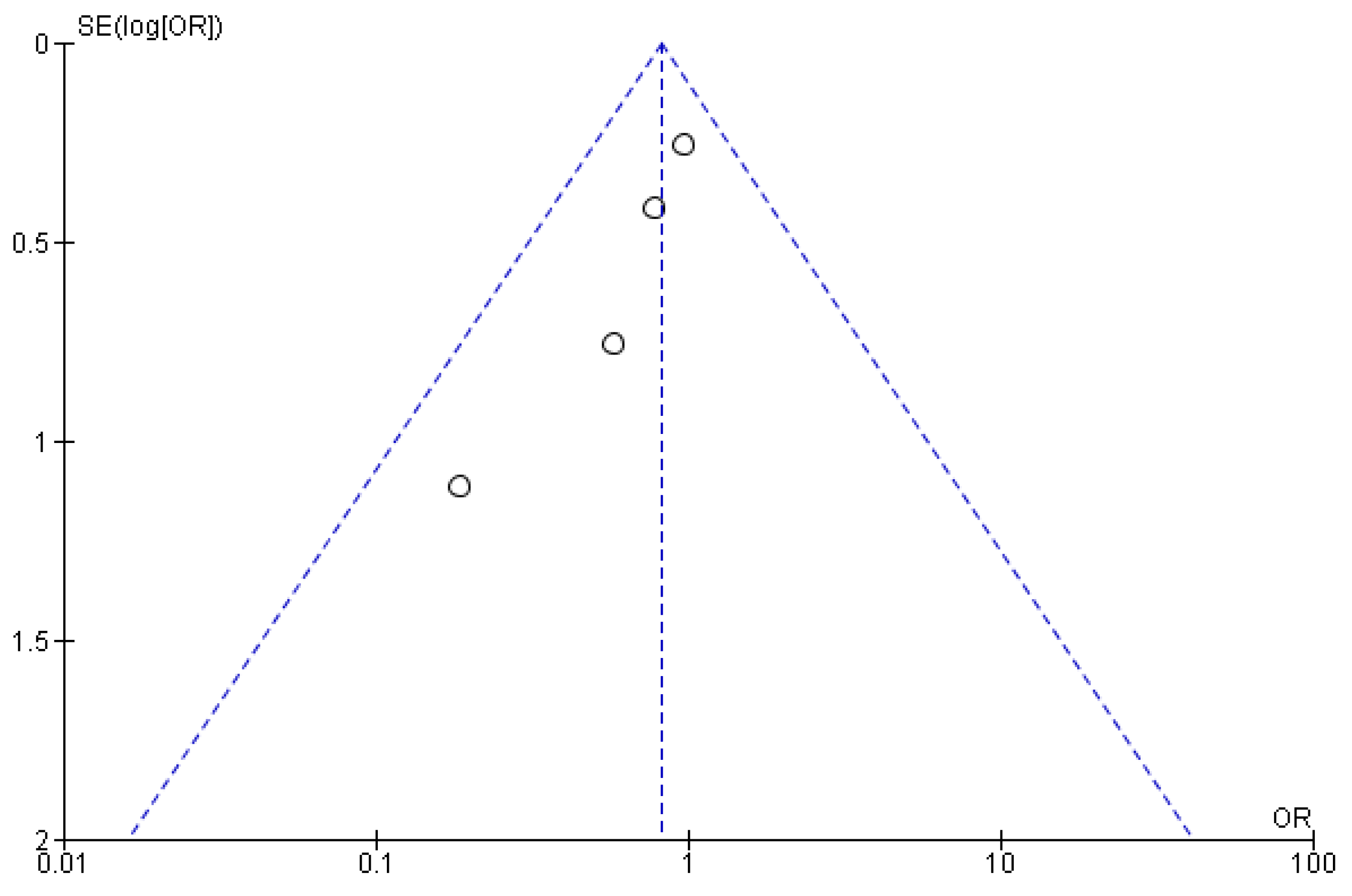
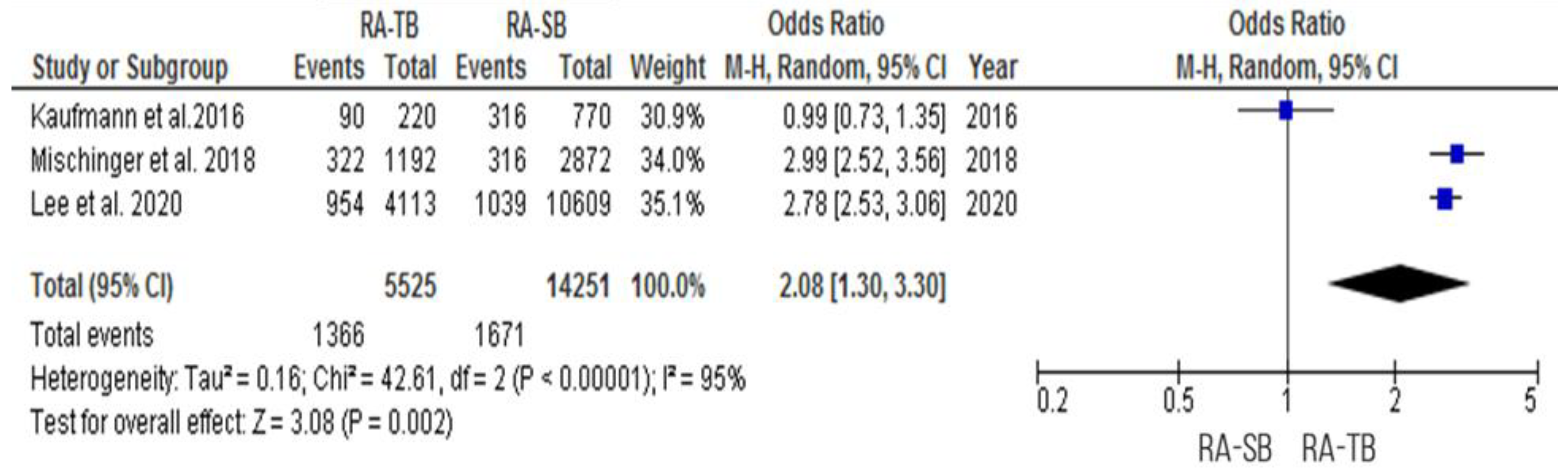
3.2. Cancer Detection Rate (CDR) “per Patient”
3.3. Additional Utility
3.4. Cancer Detection Rate “per Core”
3.5. Cancer Detection Rate “per Prior Negative Patient”
3.6. Anesthesia
3.7. Procedure Time
3.8. Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| PCa | prostate cancer |
| MRI | magnetic resonance imaging |
| CDR | cancer detection rate |
| cisCDR | clinically insignificant cancer detection rate |
| csCDR | clinically significant cancer detection rate |
| cisPCa | clinically insignificant prostate cancer |
| csPCa | clinically significant prostate cancer |
| MCCL | maximum cancer core length |
| RA-TB | robot-assisted targeted biopsy |
| RA-SB | robot-assisted systematic biopsy |
| MRI-TB | in-bore MR-targeted biopsy |
| FUS-TB | MRI-TRUS fusion targeted biopsy |
| COG-TB | cognitive registration TRUS-targeted biopsy. |
References
- Mottet, N.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef] [PubMed]
- Welch, H.G.; Fisher, E.S.; Gottlieb, D.J.; Barry, M.J. Detection of prostate cancer via biopsy in the medicare-SEER population during the PSA era. J. Natl. Cancer Inst. 2007, 99, 1395–1400. [Google Scholar] [CrossRef] [PubMed]
- Moe, A.; Hayne, D. Transrectal ultrasound biopsy of the prostate: Does it still have a role in prostate cancer diagnosis? Transl. Androl. Urol. 2021, 9, 3018–3024. [Google Scholar] [CrossRef] [PubMed]
- Gordon, L.A.N.; Kam, J.; Gilbourd, D.; Haxhimolla, H. Australian ultrasound-guided biopsy trends: A 17-year analysis of national data. Prostate Int. 2019, 7, 150–155. [Google Scholar] [CrossRef]
- Mottet, N.; Cornford, P.; van der Bergh, R.; Briers, E.; De Santis, M.; Gillesen, S.; Grummet, J.; Henry, A.M.; van der Kwast, T.H.; Lam, T.B.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer; European Association of Urology: Arnhem, The Netherlands, 2022; pp. 1–229. [Google Scholar]
- Jacewicz, M.; Günzel, K.; Rud, E.; Sandbæk, G.; Magheli, A.; Busch, J.; Hinz, S.; Baco, E. Antibiotic prophylaxis versus no antibiotic prophylaxis in transperineal prostate biopsies (NORAPP): A randomised, open-label, non-inferiority trial. Lancet Infect. Dis. 2022, 22, 1465–1471. [Google Scholar] [CrossRef]
- Loeb, S.; Bjurlin, M.A.; Nicholson, J.; Tammela, T.L.; Penson, D.F.; Carter, H.B.; Carroll, P.; Etzioni, R. Overdiagnosis and overtreatment of prostate cancer. Eur. Urol. 2014, 65, 1046–1055. [Google Scholar] [CrossRef]
- Kim, S.P.; Karnes, R.J.; Mwangi, R.; Van Houten, H.; Gross, C.P.; Gershman, B.; Leapman, M.S.; Shah, N.D. Contemporary Trends in Magnetic Resonance Imaging at the Time of Prostate Biopsy: Results from a Large Private Insurance Database. Eur. Urol. Focus 2021, 7, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Wegelin, O.; van Melick, H.H.E.; Hooft, L.; Bosch, J.L.H.R.; Reitsma, H.B.; Barentsz, J.O.; Somford, D.M. Comparing Three Different Techniques for Magnetic Resonance Imaging-targeted Prostate Biopsies: A Systematic Review of In-bore versus Magnetic Resonance Imaging-transrectal Ultrasound fusion versus Cognitive Registration. Is There a Preferred Technique? Eur. Urol. 2017, 71, 517–531. [Google Scholar] [CrossRef]
- Wegelin, O.; Exterkate, L.; van der Leest, M.; Kummer, J.A.; Vreuls, W.; de Bruin, P.C.; Bosch, J.L.H.R.; Barentsz, J.O.; Somford, D.M.; van Melick, H.H.E. The FUTURE Trial: A Multicenter Randomised Controlled Trial on Target Biopsy Techniques Based on Magnetic Resonance Imaging in the Diagnosis of Prostate Cancer in Patients with Prior Negative Biopsies. Eur. Urol. 2019, 75, 582–590. [Google Scholar] [CrossRef]
- Zangos, S.; Herzog, C.; Eichler, K.; Hammerstingl, R.; Lukoschek, A.; Guthmann, S.; Gutmann, B.; Schoepf, U.J.; Costello, P.; Vogl, T.J. MR-compatible assistance system for punction in a high-field system: Device and feasibility of transgluteal biopsies of the prostate gland. Eur. Radiol. 2007, 17, 1118–1124. [Google Scholar] [CrossRef]
- Patriciu, A.; Petrisor, D.; Muntener, M.; Mazilu, D.; Schär, M.; Stoianovici, D. Automatic brachytherapy seed placement under MRI guidance. IEEE Trans. Biomed. Eng. 2007, 54, 1499–1506. [Google Scholar] [CrossRef] [PubMed]
- Halstuch, D.; Baniel, J.; Lifshitz, D.; Sela, S.; Ber, Y.; Margel, D. Characterizing the learning curve of MRI-US fusion prostate biopsies. Prostate Cancer Prostatic Dis. 2019, 22, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Tu, X.; Liu, Z.; Chang, T.; Qiu, S.; Xu, H.; Bao, Y.; Yang, L.; Wei, Q. Transperineal Magnetic Resonance Imaging–Targeted Biopsy May Perform Better Than Transrectal Route in the Detection of Clinically Significant Prostate Cancer: Systematic Review and Meta-analysis. Clin. Genitourin. Cancer 2019, 17, e860–e870. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.S.S.; Mohan, P.; Lim, E.D.; Li, D.L.; Yuen, J.S.; Ng, W.S.; Lau, W.K.; Cheng, C.W. Robotic ultrasound-guided prostate intervention device: System description and results from phantom studies. Int. J. Med. Robot. Comput. Assist. Surg. 2009, 5, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Kroenig, M.; Schaal, K.; Benndorf, M.; Soschynski, M.; Lenz, P.; Krauss, T.; Drendel, V.; Kayser, G.; Kurz, P.; Werner, M.; et al. Diagnostic Accuracy of Robot-Guided, Software Based Transperineal MRI/TRUS Fusion Biopsy of the Prostate in a High Risk Population of Previously Biopsy Negative Men. Biomed. Res. Int. 2016, 2016, 2384894. [Google Scholar] [CrossRef]
- Ho, H.; Yuen, J.S.P.; Cheng, C.W.S. Robotic prostate biopsy and its relevance to focal therapy of prostate cancer. Nat. Rev. Urol. 2011, 8, 579–585. [Google Scholar] [CrossRef]
- Perlis, N.; Lawendy, B.; Barkin, J. How I Do It-MRI-ultrasound fusion prostate biopsy using the Fusion MR and Fusion Bx systems. Can. J. Urol. 2020, 27, 10185–10191. [Google Scholar]
- Linder, N.; Schaudinn, A.; Petersen, T.O.; Bailis, N.; Stumpp, P.; Horn, L.C.; Stolzenburg, J.U.; Kahn, T.; Moche, M.; Busse, H. In-bore biopsies of the prostate assisted by a remote-controlled manipulator at 1.5 T. Magn. Reson. Mater. Phys. Biol. Med. 2019, 32, 599–605. [Google Scholar] [CrossRef]
- Tilak, G.; Tuncali, K.; Song, S.E.; Tokuda, J.; Olubiyi, O.; Fennessy, F.; Fedorov, A.; Penzkofer, T.; Tempany, C.; Hata, N. 3T MR-guided in-bore transperineal prostate biopsy: A comparison of robotic and manual needle-guidance templates. J. Magn. Reson. Imaging 2015, 42, 63–71. [Google Scholar] [CrossRef]
- Vilanova, J.C.; Pérez de Tudela, A.; Puig, J.; Hoogenboom, M.; Barceló, J.; Planas, M.; Sala, S.; Thió-Henestrosa, S. Robotic-assisted transrectal MRI-guided biopsy. Technical feasibility and role in the current diagnosis of prostate cancer: An initial single-center experience. Abdom. Radiol. 2020, 45, 4150–4159. [Google Scholar] [CrossRef]
- Ball, M.W.; Ross, A.E.; Ghabili, K.; Kim, C.; Jun, C.; Petrisor, D.; Pan, L.; Epstein, J.I.; Macura, K.J.; Stoianovici, D.S.; et al. Safety and Feasibility of Direct Magnetic Resonance Imaging-guided Transperineal Prostate Biopsy Using a Novel Magnetic Resonance Imaging-safe Robotic Device. Urology 2017, 109, 216–221. [Google Scholar] [CrossRef]
- Barral, M.; Lefevre, A.; Camparo, P.; Hoogenboom, M.; Pierre, T.; Soyer, P.; Cornud, F. Biopsy With Robotic Assistance in An Analysis of 57 Patients. AJR Am. J. Roentgenol. 2019, 213, W171–W179. [Google Scholar] [CrossRef] [PubMed]
- Yakar, D.; Schouten, M.G.; Bosboom, D.G.H.; Barentsz, J.O.; Scheenen, T.W.J.; Fütterer, J.J. Feasibility of a pneumatically actuated MR-compatible robot for transrectal prostate biopsy guidance. Radiology 2011, 260, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Bomers, J.G.R.; Bosboom, D.G.H.; Tigelaar, G.H.; Sabisch, J.; Fütterer, J.J.; Yakar, D. Feasibility of a 2nd generation MR-compatible manipulator for transrectal prostate biopsy guidance. Eur. Radiol. 2017, 27, 1776–1782. [Google Scholar] [CrossRef] [PubMed]
- Schouten, M.G.; Bomers, J.G.R.; Yakar, D.; Huisman, H.; Rothgang, E.; Bosboom, D.; Scheenen, T.W.; Misra, S.; Fütterer, J.J. Evaluation of a robotic technique for transrectal MRI-guided prostate biopsies. Eur. Radiol. 2012, 22, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Tay, K.J.; Law, Y.M.; Aydin, H.; Ho, H.; Cheng, C.; Yuen, J.S.P. Outcomes of combination MRI-targeted and transperineal template biopsy in restaging low-risk prostate cancer for active surveillance. Asian J. Urol. 2018, 5, 184–193. [Google Scholar] [CrossRef]
- Kaufmann, S.; Mischinger, J.; Amend, B.; Rausch, S.; Adam, M.; Scharpf, M.; Fend, F.; Kramer, U.; Notohamiprodjo, M.; Nikolaou, K.; et al. First report of robot-assisted transperineal fusion versus off-target biopsy in patients undergoing repeat prostate biopsy. World J. Urol. 2017, 35, 1023–1029. [Google Scholar] [CrossRef]
- Kaufmann, S.; Russo, G.I.; Bamberg, F.; Löwe, L.; Morgia, G.; Nikolaou, K.; Stenzl, A.; Kruck, S.; Bedke, J. Prostate cancer detection in patients with prior negative biopsy undergoing cognitive-, robotic- or in-bore MRI target biopsy. World J. Urol. 2018, 36, 761–768. [Google Scholar] [CrossRef]
- Lee, A.Y.M.; Yang, X.Y.; Lee, H.J.; Law, Y.M.; Huang, H.H.; Lau, W.K.O.; Lee, L.S.; Ho, H.S.S.; Tay, K.J.; Cheng, C.W.S.; et al. Multiparametric MRI-ultrasonography software fusion prostate biopsy: Initial results using a stereotactic robotic-assisted transperineal prostate biopsy platform comparing systematic vs targeted biopsy. BJU Int. 2020, 126, 568–576. [Google Scholar] [CrossRef]
- Miah, S.; Servian, P.; Patel, A.; Lovegrove, C.; Skelton, L.; Shah, T.T.; Eldred-Evans, D.; Arya, M.; Tam, H.; Ahmed, H.U.; et al. A prospective analysis of robotic targeted MRI-US fusion prostate biopsy using the centroid targeting approach. J. Robot. Surg. 2020, 14, 69–74. [Google Scholar] [CrossRef]
- Mischinger, J.; Kaufmann, S.; Russo, G.I.; Harland, N.; Rausch, S.; Amend, B.; Scharpf, M.; Loewe, L.; Todenhoefer, T.; Notohamiprodjo, M.; et al. Targeted vs systematic robot-assisted transperineal magnetic resonance imaging-transrectal ultrasonography fusion prostate biopsy. BJU Int. 2018, 121, 791–798. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.I.; Muter, S.; Vladica, P.; Gillatt, D. Robotic-assisted magnetic resonance imaging ultrasound fusion results in higher significant cancer detection compared to cognitive prostate targeting in biopsy naive men. Transl. Androl. Urol. 2020, 9, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.Y.; Lee, A.Y.; Law, Y.M.; Sim, A.S.P.; Tay, K.J.; Lau, W.K.O.; Ho, H.S.S.; Yuen, J.S.P.; Chen, K. Stereotactic robot-assisted transperineal prostate biopsy under local anaesthesia and sedation: Moving robotic biopsy from operating theatre to clinic. J. Robot. Surg. 2020, 14, 767–772. [Google Scholar] [CrossRef]
- Rouvière, O.; Puech, P.; Renard-Penna, R.; Claudon, M.; Roy, C.; Mège-Lechevallier, F.; Decaussin-Petrucci, M.; Dubreuil-Chambardel, M.; Magaud, L.; Remontet, L.; et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): A prospective, multicentre, paired diagnostic study. Lancet Oncol. 2019, 20, 100–109. [Google Scholar] [CrossRef]
- Van der Leest, M.; Cornel, E.; Israël, B.; Hendriks, R.; Padhani, A.R.; Hoogenboom, M.; Zamecnik, P.; Bakker, D.; Setiasti, A.Y.; Veltman, J.; et al. Head-to-head Comparison of Transrectal Ultrasound-guided Prostate Biopsy Versus Multiparametric Prostate Resonance Imaging with Subsequent Magnetic Resonance-guided Biopsy in Biopsy-naïve Men with Elevated Prostate-specific Antigen: A Large Prospective Mu. Eur. Urol. 2019, 75, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.-J.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. [Google Scholar] [CrossRef] [PubMed]
- National Library of Medicine (US). Transrectal Ultrasound Robot-Assisted Prostate Biopsy; Identifier: NCT02871726; National Library of Medicine (US): Bethesda, MD, USA, 2016.
- Checcucci, E.; Piramide, F.; Amparore, D.; De Cillis, S.; Granato, S.; Sica, M.; Verri, P.; Volpi, G.; Piana, A.; Garrou, D.; et al. Beyond the Learning Curve of Prostate MRI/TRUS Target Fusion Biopsy after More than 1000 Procedures. Urology 2021, 155, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.; Jun, C.; Chang, D.; Petrisor, D.; Han, M.; Stoianovici, D. Robotic Transrectal Ultrasound-Guided Prostate Biopsy. IEEE Trans. Biomed. Eng. 2019, 66, 2527. [Google Scholar] [CrossRef] [PubMed]
- Muntener, M.; Patriciu, A.; Petrisor, D.; Schär, M.; Ursu, D.; Song, D.Y.; Stoianovici, D. Transperineal prostate intervention: Robot for fully automated MR imaging-System description and proof of principle in a canine model. Radiology 2008, 247, 543–549. [Google Scholar] [CrossRef]
- Marra, G.; Marquis, A.; Tappero, S.; D’Agate, D.; Oderda, M.; Calleris, G.; Falcone, M.; Faletti, R.; Molinaro, L.; Zitella, A.; et al. Transperineal Free-hand mpMRI Fusion-targeted Biopsies Under Local Anesthesia: Technique and Feasibility From a Single-center Prospective Study. Urology 2020, 140, 122–131. [Google Scholar] [CrossRef]
- Ho, H.; Yuen, J.S.P.; Mohan, P.; Lim, E.W.; Cheng, C.W.S. Robotic Transperineal Prostate Biopsy: Pilot Clinical Study. Urology 2011, 78, 1203–1208. [Google Scholar] [CrossRef]
- Stoianovici, D.; Kim, C.; Petrisor, D.; Jun, C.; Lim, S.; Ball, M.W.; Ross, A.; Macura, K.J.; Allaf, M. MR Safe Robot, FDA Clearance, Safety and Feasibility of Prostate Biopsy Clinical Trial. IEEE/ASME Trans. Mechatron. 2017, 22, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Wetterauer, C.; Shahin, O.; Federer-Gsponer, J.R.; Keller, N.; Wyler, S.; Seifert, H.H.; Kwiatkowski, M. Feasibility of freehand MRI/US cognitive fusion transperineal biopsy of the prostate in local anaesthesia as in-office procedure—Experience with 400 patients. Prostate Cancer Prostatic Dis. 2020, 23, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Pradere, B.; Veeratterapillay, R.; Dimitropoulos, K.; Yuan, Y.; Omar, M.I.; MacLennan, S.; Cai, T.; Bruyère, F.; Bartoletti, R.; Köves, B.; et al. Nonantibiotic Strategies for the Prevention of Infectious Complications following Prostate Biopsy: A Systematic Review and Meta-Analysis. J. Urol. 2021, 205, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Johansen, T.E.B.; Zahl, P.H.; Baco, E.; Bartoletti, R.; Bonkat, G.; Bruyere, F.; Cai, T.; Cek, M.; Kulchavenya, E.; Köves, B.; et al. Antibiotic resistance, hospitalizations, and mortality related to prostate biopsy: First report from the Norwegian Patient Registry. World J. Urol. 2020, 38, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Borghesi, M.; Ahmed, H.; Nam, R.; Schaeffer, E.; Schiavina, R.; Taneja, S.; Weidner, W.; Loeb, S. Complications After Systematic, Random, and Image-guided Prostate Biopsy. Eur. Urol. 2017, 71, 353–365. [Google Scholar] [CrossRef]
- Schouten, M.G.; Ansems, J.; Renema, W.K.J.; Bosboom, D.; Scheenen, T.W.J.; Fütterer, J.J. The accuracy and safety aspects of a novel robotic needle guide manipulator to perform transrectal prostate biopsies. Med. Phys. 2010, 37, 4744–4750. [Google Scholar] [CrossRef]
- Checcucci, E.; De Cillis, S.; Piramide, F.; Amparore, D.; Kasivisvanathan, V.; Giganti, F.; Fiori, C.; Moore, C.M.; Porpiglia, F. The role of additional standard biopsy in the MRI-targeted biopsy era. Minerva Urol. Nefrol. 2020, 72, 637–639. [Google Scholar] [CrossRef]
- Delongchamps, N.B.; Portalez, D.; Bruguière, E.; Rouvière, O.; Malavaud, B.; Mozer, P.; Fiard, G.; Cornud, F.; MURIELLE Study Group. Are Magnetic Resonance Imaging-Transrectal Ultrasound Guided Targeted Biopsies Noninferior to Transrectal Ultrasound Guided Systematic Biopsies for the Detection of Prostate Cancer? J. Urol. 2016, 196, 1069–1075. [Google Scholar] [CrossRef]
- Wegelin, O.; Exterkate, L.; van der Leest, M.; Kelder, J.C.; Bosch, J.L.H.R.; Barentsz, J.O.; Somford, D.M.; van Melick, H.H.E. Complications and Adverse Events of Three Magnetic Resonance Imaging-based Target Biopsy Techniques in the Diagnosis of Prostate Cancer Among Men with Prior Negative Biopsies: Results from the FUTURE Trial, a Multicentre Randomised Controlled Trial. Eur. Urol. Oncol. 2019, 2, 617–624. [Google Scholar] [CrossRef]
- Huang, H.; Wang, W.; Lin, T.; Zhang, Q.; Zhao, X.; Lian, H.; Guo, H. Comparison of the complications of traditional 12 cores transrectal prostate biopsy with image fusion guided transperineal prostate biopsy. BMC Urol. 2016, 16, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, C.M.; Kasivisvanathan, V.; Eggener, S.; Emberton, M.; Fütterer, J.J.; Gill, I.S.; Grubb Iii, R.L.; Hadaschik, B.; Klotz, L.; Margolis, D.J.; et al. Standards of reporting for MRI-targeted biopsy studies (START) of the prostate: Recommendations from an International Working Group. Eur. Urol. 2013, 64, 544–552. [Google Scholar] [CrossRef] [PubMed]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Type of Study, Level of Evidence | Number, Type of Patients | Age, Years | PSA, ng/mL | Prostate Volume, cm3 | MRI Flux Density, T | MRI Lesions Targeted | Number of MRI Lesions | Definition of csPCa |
|---|---|---|---|---|---|---|---|---|---|
| Kroenig et al., 2016 [16] | Retrospective, 2b | 52—prior negative | Mean 65.8 (±7.3) Median 66.0 (IQR 60.0–71.8) | Mean 9.9 (± 5.9) Median 8.8 (IQR 5.7–13.04) | Mean 57.6 (± 26.6) Median 49.3 (IQR 37.8–73.3) | NA | 2–5 | PI-RADS unclassified—12 PI-RADS 2—16 PI-RADS 3—55 PI-RADS 4—40 PI-RADS 5—12 | Gleason grade ≥ 4 |
| Kaufmann et al., 2016 [28] | Prospective, nonrandomized, 2b | 55—prior negative | Mean 65.0 (± 7.9; range 50–78) | Mean10.2 (±5.2; range 3.2–25.1) | Mean 43.9 (± 22.6; range 13.4–108) | 1.5 3.0 | NA | ≥4—24 ≥3—33 | GS ≥ 3 + 4 |
| Chen et al., 2017 [27] | Prospective, nonrandomized, 2b | 18—active surveillance | Mean 65.4 (±4.9) | Mean 7.0 (± 1.8) | Mean 32.1 (± 13.4) | 3.0 | ≥3 | PI-RADS 3—5 PI-RADS 4—7 PI-RADS 5—6 | Gleason grade ≥ 4 |
| Miah et al., 2018 [31] | Prospective, nonrandomized, 2b | 86—biopsy-naive, prior negative | Mean 64.24 (±6.97) | Mean 10.00 (±8.53) | Mean 51.03 (±25.24) | 1.5 3.0 | ≥3 | PI-RADS unclassified—9 PI-RADS 3—22 PI-RADS 4—55 PI-RADS 5—30 | GS > 3 + 3 |
| Mischinger et al., 2018 [32] | Retrospective, 2b | 130—biopsy-naive 72—prior negative | Median 66 (±7.6; IQR 60–73) | Median 8 (±5.8; IQR 6–11.9) | Median 36 (±21.8; IQR 26.9–47.8) | 1.5 3,0 | 1–5 | PI-RADS 1—1 PI-RADS 2—38 PI-RADS 3—39 PI-RADS 4—107 PI-RADS 5—17 | GS ≥ 3 + 4 |
| Kaufmann et al., 2018 [29] | Prospective, nonrandomized, 3b | 156—prior negative | Median 67.0 (IQR 61.0–72.0) | Median 9.0 (IQR 6.0–13.0) | NA | 3.0 | NA | NA | GS ≥ 3 + 4 GS 3 + 3 MCCL ≥ 5 mm |
| Patel et al., 2020 [33] | Retrospective, 2b | 92—biopsy-naive | Median 63 (IQR 58–68) | NA | Median 53.0 (IQR 41.5–75.5) | 3.0 | 3–5 | PI-RADS 3—28 PI-RADS 4—41 PI-RADS 5—22 | ISUP ≥ 2 |
| Yang et al., 2020 [34] | Prospective, nonrandomized, 2b | 5—biopsy-naive 25—prior negative | Median 66 (range 53–80) | Median 8.1 (range 4.2–20.6) | Median 40.0 (range 18.6–70.0) | NA | 3–5 | NA | Epstein criteria |
| Lee et al., 2020 [30] | Retrospective, 2b | 67—active surveillance 288—biopsy naive 145—prior negative | Mean 66.1 (±7.8) | Mean 10.4 (±8.3) | Mean 43.2 (±18.4) | 3.0 | 3–5 | PI-RADS 3—92 PI-RADS 4—288 PI-RADS 5—120 | ISUP ≥ 2 |
| Author, Year | Type of RA-TB | Software | Hardware | Approach | Number of Cores | Comparator, Number of Cores | csCDR | oCDR | CDR per Core | CDR per Lesion | Additional Utility | Procedure Duration, min | Complication |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kroenig et al., 2016 [16] | FUS-TB NA NA | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Mean 10.2 (±4.8), median 9.0 (IQR 6.0–14.0) | RA-SB (Ginsburg study scheme), mean 30.0 (±5.6), median 32.0 (IQR 24.0–32.0) | 23/52 (44.2%) RA-TB 26/52 (50.0%) RA-SB 27/52 (51.9%) Combined RA | 26/52 (50.0%) RA-TB 31/52 (59.6%) RA-SB 31/52 (59.6%) Combined RA | NA | NA | 2 (3.9%) PCa RA-SB | NA | 1/52 (1.9%)—rectal perforation 1/52 (1.9%)— rectal bleeding |
| Kaufmann et al., 2016 [28] | FUS-TB First Unblinded | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | 4 | RA-SB, 14 | 28/55 (50.9%) RA-TB 14/55 (25.4%) RA-SB 29/55 (52.7%) Combined RA | 29/55 (52.7%) RA-TB 19/55 (34.5%) RA-SB 34/55 (61.8%) Combined RA | 90/220 (41%) RA-TB 37/770 (5%) RA-SB | NA | 5 (9.1%) PCa RA-SB 1 (1.8%) csPCa RA-SB | Mean 43 (±6) | CD 1—9/55 (16.3%) 3/55 (5.4%)—bladder catheterization 1/55 (1.8%)—prolonged bleeding 5/55 (9.1%)—mild hematuria |
| Chen et al., 2017 [27] | COG-TB Second Blinded | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Mean 13.3 (±5.8) | RA-SB, mean 26.9 (± 8.2) | 4/18 (22.2%) RA-TB 3/18 (16.6%) RA-SB 5/18 (27.8%) Combined RA | 10/18 (55.6%) RA-TB 14/18 (77.7%) RA-SB 14/18 (77.7%) Combined RA | 28/239 (11.7%) RA-TB 33/511 (6.4%) RA-SB | NA | 1 (5.5%) PCa RA-SB | Median 15 (range 13–21) | No severe complications |
| Miah et al., 2018 [31] | FUS-TB First NA | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Mean 8.15 (±3.82) | RA-SB (Barzell scheme), mean 20.20 (±6.18) | 35/86 (40.1%) RA-TB 44/86 (51.2%) Combined RA | NA | NA | 48/116 (41.8%) Combined RA | 9 (10.5%) csPCa RA-SB | NA | 1/86 (1.1%)—urosepsis |
| Mischinger et al., 2018 [32] | FUS-TB First Unblinded | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Mean 5.8 (±2.8) | RA-SB, mean 14.2 | 84/202 (41.6%) RA-TB 86/202 (42.6%) RA-SB 105/202 (52.0%) Combined RA | 95/202 (47.0%) RA-TB 100/202 (49.5%) RA-SB 123/202 (60.9%) Combined RA | 322/1192 (27.0%) RA-TB 316/2872 (11.0%) RA-SB | NA | 28 (13.8%) PCa RA-SB 21 (10.4%) csCPa RA-SB | Mean 43 (±6) | CD ≤ II—6/202 (3.0%) 3/202 (1.5%)—AUR 3/202 (1.5%)—hematoma CD ≥ III —1/202 (0.5%) 1/202 (0.5%)—rectal injury, peritonitis |
| Kaufmann et al., 2018 [29] | FUS-TB NA NA | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Median 3.0 (IQR 2.0–5.0) | MRI-TB manually, median 3.0 (IQR 2.0–5.0) TRUS COG-TB, median 3.0 (IQR 2.0–5.0) | 26/73 (35.6%) RA-TB 18/45 (40%) %) In-bore manually 9/38 (23.6%) Cognitive TB | 39/73 (53.4%) RA-TB 23/45 (51.1%) In-bore manually 11/38 (28.9%) Cognitive TB | NA | NA | NA | NA | No severe complications |
| Patel et al., 2020 [33] | FUS-TB First NA | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Median 4 (IQR 3–5) | RA-SB (Ginsburg protocol), 24 Cognitive registration TB, median 3 (IQR 2–3) + SB (Ginsburg protocol), 24 | 17/53 (32.1%) RA-TB 21/53 (39.6%) Combined RA 4/39 (10.3%) Cognitive TB 14/39 (35.9%) Combined Cognitive TB + SB | 25/53 (47.2%) RA-TB 32/53 (60.2%) Combined RA 5/39 (12.8%) Cognitive TB 17/39 (43.6%) Combined cognitive TB + SB | NA | NA | 4 (7.5%) csPCa SB-RA | Median 24 (IQR 21–28) Combined RA Median 32 (IQR 31–36) Combined cognitive TB + SB | Combined RA 1/53 (1.9%)—AUR 4/53 (7.5%) hematuria Combined cognitive TB + SB 5/39 (12.8%)—AUR 15/39 (38.5%) hematuria |
| Yang et al., 2020 [34] | FUS-TB NA NA | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Median 8 (range 5–16) | RA-SB, median 21 (range 9–48) | 16/30 (53.3%) Combined RA | 19/30 (63.3%) Combined RA | NA | NA | NA | Median 33 (range 19–49) | CD II—2/30 (6.7%) 1/30 (3.3%)—UTI 1/30 (3.3%)—AUR |
| Lee et al., 2020 [30] | FUS-TB First Unblinded | Urofusion Urobiopsy | iSR’obot Mona Lisa (Biobot Surgical) | TP | Mean 9.5 (±3.9) | RA-SB, mean 24.5 (±7.7) | 166/433 (38.3%) RA-TB 171/433 (39.5%) RA-SB 199/433 (44.9%) Combined RA Active surveillance 20/67 (29.8%) RA-TB 21/67 (31.3%) RA-SB 23/67 (34.3%) Combined RA | 213/433 (49.2%) RA-TB 222/433 (50.8%) RA-SB 248/433 (57.3%) Combined RA Active surveillance 40/67 (59.7%) RA-TB 41/67 (61.2%) RA-SB 48/67 (71.6%) Combined RA | NA | NA | NA | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petov, V.; Azilgareeva, C.; Shpikina, A.; Morozov, A.; Krupinov, G.; Kozlov, V.; Singla, N.; Gómez Rivas, J.; Jesús, M.-S.; Puliatti, S.; et al. Robot-Assisted Magnetic Resonance Imaging-Targeted versus Systematic Prostate Biopsy; Systematic Review and Meta-Analysis. Cancers 2023, 15, 1181. https://doi.org/10.3390/cancers15041181
Petov V, Azilgareeva C, Shpikina A, Morozov A, Krupinov G, Kozlov V, Singla N, Gómez Rivas J, Jesús M-S, Puliatti S, et al. Robot-Assisted Magnetic Resonance Imaging-Targeted versus Systematic Prostate Biopsy; Systematic Review and Meta-Analysis. Cancers. 2023; 15(4):1181. https://doi.org/10.3390/cancers15041181
Chicago/Turabian StylePetov, Vladislav, Camilla Azilgareeva, Anastasia Shpikina, Andrey Morozov, German Krupinov, Vasiliy Kozlov, Nirmish Singla, Juan Gómez Rivas, Moreno-Sierra Jesús, Stefano Puliatti, and et al. 2023. "Robot-Assisted Magnetic Resonance Imaging-Targeted versus Systematic Prostate Biopsy; Systematic Review and Meta-Analysis" Cancers 15, no. 4: 1181. https://doi.org/10.3390/cancers15041181