
The CAPRA&PDE4D5/7/9 Prognostic Model Is Significantly Associated with Adverse Post-Surgical Pathology Outcomes

Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Cohort and Samples
2.2. Clinical Risk Metrics
2.3. Laboratory Methods
2.4. Data Analysis and Statistics
3. Results
3.1. Patient Demographics
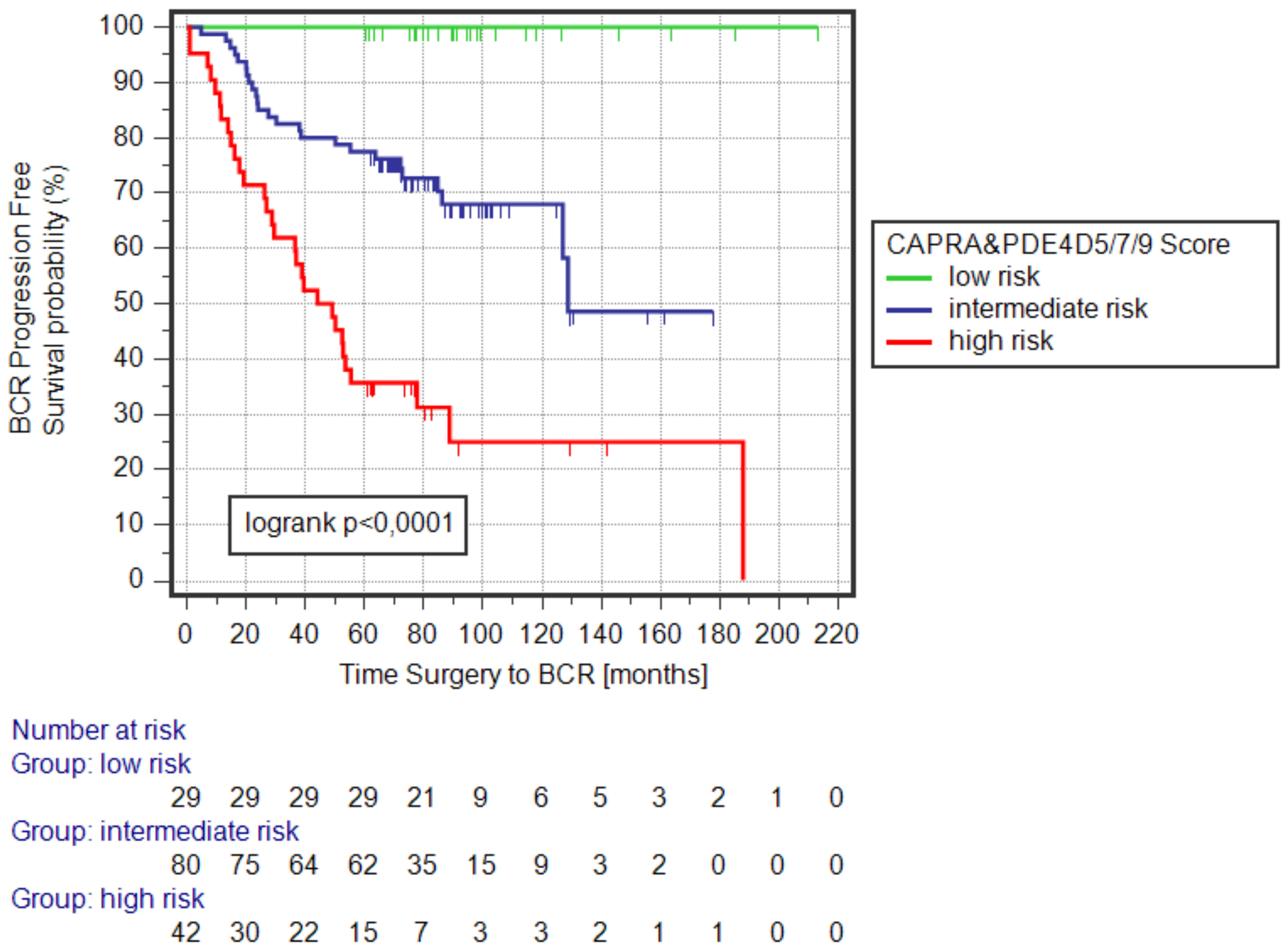
3.2. Kaplan–Meier Survival Analysis of the CAPRA&PDE4D5/7/9_BCR Logistic Regression Model
3.3. Analysis of CAPRA&PDE4D5/7/9_BCR Risk Model
3.4. Univariable Logistic Regression (UVLR) Analysis
3.5. Multivariable Logistic Regression (MVLR) Modeling
3.6. Negative Predictive Values
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AS | active surveillance; |
| RP | radical prostatectomy; |
| BCR | biochemical recurrence; |
| PCSS | prostate cancer specific survival; |
| OS | overall survival; |
| SRT | salvage radiation therapy; |
| SADT | salvage androgen deprivation therapy; |
| OR | odds ratio; |
| CI | confidence interval; |
| NPV | negative predictive value; |
| PPV | positive predictive value; |
| ROC | Receiver Operating Characteristics; |
| AUROC | area under the ROC curve; |
| CAPRA | Cancer of the Prostate Risk Assessment; |
| PRIAS | Prostate Cancer Research International: Active Surveillance |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gleason, D.F. Classification of prostatic carcinomas. Cancer Chemother. Rep. 1966, 50, 125–128. [Google Scholar] [PubMed]
- Epstein, J.I.; Allsbrook, W.C.; Amin, M.B.; Egevad, L.L.; Committee, I.G. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Shappley, W.V.; Kenfield, S.A.; Kasperzyk, J.L.; Qiu, W.; Stampfer, M.J.; Sanda, M.G.; Chan, J.M. Prospective study of determinants and outcomes of deferred treatment or watchful waiting among men with prostate cancer in a nationwide cohort. J. Clin. Oncol. 2009, 27, 4980–4985. [Google Scholar] [CrossRef] [Green Version]
- Stattin, P.; Holmberg, E.; Johansson, J.E.; Holmberg, L.; Adolfsson, J.; Hugosson, J.; National Prostate Cancer Register (NPCR) of Sweden. Outcomes in localized prostate cancer: National Prostate Cancer Register of Sweden follow-up study. J. Natl. Cancer Inst. 2010, 102, 950–958. [Google Scholar] [CrossRef] [Green Version]
- Parker, C.; Muston, D.; Melia, J.; Moss, S.; Dearnaley, D. A model of the natural history of screen-detected prostate cancer, and the effect of radical treatment on overall survival. Br. J. Cancer 2006, 94, 1361–1368. [Google Scholar] [CrossRef]
- Epstein, J.I.; Feng, Z.; Trock, B.J.; Pierorazio, P.M. Upgrading and downgrading of prostate cancer from biopsy to radical prostatectomy: Incidence and predictive factors using the modified Gleason grading system and factoring in tertiary grades. Eur. Urol. 2012, 61, 1019–1024. [Google Scholar] [CrossRef] [Green Version]
- Iremashvili, V.; Pelaez, L.; Manoharan, M.; Jorda, M.; Rosenberg, D.L.; Soloway, M.S. Pathologic prostate cancer characteristics in patients eligible for active surveillance: A head-to-head comparison of contemporary protocols. Eur. Urol. 2012, 62, 462–468. [Google Scholar] [CrossRef]
- Fang, Y.; Fliss, A.E.; Robins, D.M.; Caplan, A.J. Hsp90 regulates androgen receptor hormone binding affinity in vivo. J. Biol. Chem. 1996, 271, 28697–28702. [Google Scholar] [CrossRef]
- Merkle, D.; Hoffmann, R. Roles of cAMP and cAMP-dependent protein kinase in the progression of prostate cancer: Cross-talk with the androgen receptor. Cell Signal. 2011, 23, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Sarwar, M.; Sandberg, S.; Abrahamsson, P.A.; Persson, J.L. Protein kinase A (PKA) pathway is functionally linked to androgen receptor (AR) in the progression of Prostate Cancer. Urol. Oncol. 2014, 32, 25.e1–25.e12. [Google Scholar]
- Moen, L.V.; Ramberg, H.; Zhao, S.; Grytli, H.H.; Sveen, A.; Berge, V.; Skotheim, R.I.; Taskén, K.A.; Skålhegg, B.S. Observed correlation between the expression levels of catalytic subunit, Cβ2, of cyclic adenosine monophosphate-dependent protein kinase and prostate cancer aggressiveness. Urol. Oncol. 2017, 35, 111.e1–111.e8. [Google Scholar] [CrossRef] [PubMed]
- Khor, L.Y.; Bae, K.; Al-Saleem, T.; Hammond, E.H.; Grignon, D.J.; Sause, W.T.; Pilepich, M.V.; Okunieff, P.P.; Sandler, H.M.; Pollack, A. Protein kinase A RI-alpha predicts for prostate cancer outcome: Analysis of radiation therapy oncology group trial 86-10. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1309–1315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazareth, L.V.; Weigel, N.L. Activation of the human androgen receptor through a protein kinase A signaling pathway. J. Biol. Chem. 1996, 271, 19900–19907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagar, M.; Singh, J.P.; Dagar, G.; Tyagi, R.K.; Bagchi, G. Phosphorylation of HSP90 by protein kinase A is essential for the nuclear translocation of androgen receptor. J. Biol. Chem. 2019, 294, 8699–8710. [Google Scholar] [CrossRef] [Green Version]
- Azevedo, M.F.; Faucz, F.R.; Bimpaki, E.; Horvath, A.; Levy, I.; de Alexandre, R.B.; Ahmad, F.; Manganiello, V.; Stratakis, C.A. Clinical and molecular genetics of the phosphodiesterases (PDEs). Endocr. Rev. 2014, 35, 195–233. [Google Scholar] [CrossRef]
- Francis, S.H.; Blount, M.A.; Corbin, J.D. Mammalian cyclic nucleotide phosphodiesterases: Molecular mechanisms and physiological functions. Physiol. Rev. 2011, 91, 651–690. [Google Scholar] [CrossRef] [Green Version]
- Henderson, D.J.; Byrne, A.; Dulla, K.; Jenster, G.; Hoffmann, R.; Baillie, G.S.; Houslay, M.D. The cAMP phosphodiesterase-4D7 (PDE4D7) is downregulated in androgen-independent prostate cancer cells and mediates proliferation by compartmentalising cAMP at the plasma membrane of VCaP prostate cancer cells. Br. J. Cancer 2014, 110, 1278–1287. [Google Scholar] [CrossRef] [Green Version]
- Böttcher, R.; Dulla, K.; van Strijp, D.; Dits, N.; Verhoef, E.I.; Baillie, G.S.; van Leenders, G.J.L.H.; Houslay, M.D.; Jenster, G.; Hoffmann, R. Human PDE4D isoform composition is deregulated in primary prostate cancer and indicative for disease progression and development of distant metastases. Oncotarget 2016, 7, 70669–70684. [Google Scholar] [CrossRef] [Green Version]
- Böttcher, R.; Henderson, D.J.; Dulla, K.; van Strijp, D.; Waanders, L.F.; Tevz, G.; Hoffmann, R. Human phosphodiesterase 4D7 (PDE4D7) expression is increased in TMPRSS2-ERG-positive primary prostate cancer and independently adds to a reduced risk of post-surgical disease progression. Br. J. Cancer 2015, 113, 1502–1511. [Google Scholar] [CrossRef] [PubMed]
- Van Strijp, D.; de Witz, C.; Vos, P.C.; den Biezen-Timmermans, E.; van Brussel, A.; Wrobel, J.; Baillie, G.S.; Tennstedt, P.; Schlomm, T.; Heitkötter, B.; et al. The Prognostic PDE4D7 Score in a Diagnostic Biopsy Prostate Cancer Patient Cohort with Longitudinal Biological Outcomes. Prostate Cancer 2018, 2018, 5821616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves de Inda, M.; van Strijp, D.; den Biezen-Timmermans, E.; van Brussel, A.; Wrobel, J.; van Zon, H.; Vos, P.; Baillie, G.S.; Tennstedt, P.; Schlomm, T.; et al. Validation of Cyclic Adenosine Monophosphate Phosphodiesterase-4D7 for its Independent Contribution to Risk Stratification in a Prostate Cancer Patient Cohort with Longitudinal Biological Outcomes. Eur. Urol. Focus. 2018, 4, 376–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Strijp, D.; de Witz, C.; Heitkötter, B.; Huss, S.; Bögemann, M.; Baillie, G.S.; Houslay, M.D.; Bangma, C.; Semjonow, A.; Hoffmann, R. The Association of the Long Prostate Cancer Expressed PDE4D Transcripts to Poor Patient Outcome Depends on the Tumour’s TMPRSS2-ERG Fusion Status. Prostate Cancer 2019, 2019, 8107807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henderson, D.J.P.; Houslay, M.D.; Bangma, C.H.; Hoffmann, R. Creating a potential diagnostic for prostate cancer risk stratification (InformMDx™) by translating novel scientific discoveries concerning cAMP degrading phosphodiesterase-4D7 (PDE4D7). Clin. Sci. 2019, 133, 269–286. [Google Scholar] [CrossRef] [Green Version]
- Brajtbord, J.S.; Leapman, M.S.; Cooperberg, M.R. The CAPRA Score at 10 Years: Contemporary Perspectives and Analysis of Supporting Studies. Eur. Urol. 2017, 71, 705–709. [Google Scholar] [CrossRef] [Green Version]
- Stark, J.R.; Perner, S.; Stampfer, M.J.; Sinnott, J.A.; Finn, S.; Eisenstein, A.S.; Ma, J.; Fiorentino, M.; Kurth, T.; Loda, L.; et al. Gleason score and lethal prostate cancer: Does 3 + 4 = 4 + 3? J. Clin. Oncol. 2009, 27, 3459–3464. [Google Scholar] [CrossRef]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; et al. Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2019, 17, 479–505. [Google Scholar] [CrossRef] [Green Version]
- El Hajj, A.; Ploussard, G.; de la Taille, A.; Allory, Y.; Vordos, D.; Hoznek, A.; Abbou, C.C.; Salomon, L. Analysis of outcomes after radical prostatectomy in patients eligible for active surveillance (PRIAS). BJU Int. 2013, 111, 53–59. [Google Scholar] [CrossRef]
- Song, S.H.; Pak, S.; Park, S.; Song, C.; Jeong, I.G.; Choi, H.J.; Kim, J.K.; Cho, K.-S.; Kim, C.-S.; Ahn, H. Predictors of unfavorable disease after radical prostatectomy in patients at low risk by D’Amico Criteria: Role of multiparametric magnetic resonance imaging. J. Urol. 2014, 192, 402–408. [Google Scholar] [CrossRef]
- Klein, E.A.; Cooperberg, M.R.; Magi-Galluzzi, C.; Simko, J.P.; Falzarano, S.M.; Maddala, T.; Chan, J.M.; Li, J.; Cowan, J.E.; Tsiatis, A.C.; et al. A 17-gene assay to predict prostate cancer aggressiveness in the context of Gleason grade heterogeneity, tumormultifocality, and biopsy under sampling. Eur. Urol. 2014, 66, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Cullen, J.; Rosner, I.L.; Brand, T.C.; Zhang, N.; Tsiatis, A.C.; Moncur, J.; Ali, A.; Chen, Y.; Knezevic, D.; Maddala, T.; et al. A Biopsy-based 17-gene genomic prostate score predicts recurrence after radical prostatectomy and adverse surgical pathology in a racially diverse population of men with clinically low- and intermediate-risk Prostate Cancer. Eur. Urol. 2015, 68, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Den, R.B.; Yousefi, K.; Trabulsi, E.J.; Abdollah, F.; Choeurng, V.; Feng, F.Y.; Dicker, A.P.; Lallas, C.D.; Gomella, L.G.; Davicioni, E.; et al. Genomic classifier identifies men with adverse pathology after radical prostatectomy who benefit from adjuvant radiation therapy. J. Clin. Oncol. 2015, 33, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Moussa, A.S.; Kattan, M.W.; Berglund, R.; Yu, C.; Fareed, K.; Jones, J.S. A nomogram for predicting upgrading in patients with low- and intermediate-grade prostate cancer in the era of extended prostate sampling. BJU Int. 2010, 105, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.; Slezak, J.A.; Lin, C.P.; Iremashvili, V.; Sado, M.; Razmaria, A.A.; Leverson, G.; Soloway, M.S.; Eggener, S.E.; Abel, E.J.; et al. Development and multi-institutional validation of an upgrading risk tool for Gleason 6 Prostate Cancer. Cancer 2013, 119, 3992–4002. [Google Scholar] [CrossRef] [Green Version]
- Nasri, J.; Barthe, F.; Parekh, S.; Ratnani, P.; Pedraza, A.M.; Wagaskar, V.G.; Olivier, J.; Villers, A.; Tewari, A. Nomogram Predicting Adverse Pathology Outcome on Radical Prostatectomy in Low-Risk Prostate Cancer Men. Urology 2022, 166, 189–195. [Google Scholar] [CrossRef]
- Baillie, G.S.; Tejeda, G.S.; Kelly, M.P. Therapeutic targeting of 3′,5′-cyclic nucleotide phosphodiesterases: Inhibition and beyond. Nat. Rev. Drug Discov. 2019, 18, 770–796. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Entire Cohort (n = 151) | Low–Intermediate Risk Cohort (n = 84) | CAPRA&PDE4D579_low_risk (n = 22) | |
|---|---|---|---|---|
| Demographic and Clinical Range (median; IQR) | Age range (at RP) | 47.4–77.4 (64.9; 8.5) | 52.3–76.9 (64.4; 8.3) | 54.6–74.0 (64.6; 7.3) |
| Preoperative PSA range | 2.0–49.1 (8.1; 5.7) | 2.0–49.1 (7.5; 4.9) | 2.6–17.2 (5.7; 2.8) | |
| Prostate Volume range | 13.6–148.0 (38.5; 19.2) | 13.6–148.0 (39.5; 19.0) | 15.4–105.7 (37.6; 18.5) | |
| PSA density range | 0.03–1.6 (0.2; 0.17) | 0.03–0.92 (0.2; 0.16) | 0.03–0.48 (0.16; 0.12) | |
| CAPRA Risk Category Number of Patients (%) | Low Risk (CARPA 0–2) | 38 (25.2%) | 32 (38.1%) | 15 (68.2%) |
| Intermediate Risk (CAPRA 3–5) | 82(54.3%) | 52 (61.9%) | 7 (31.8%) | |
| High Risk (CAPRA > 5) | 31 (20.5%) | 0 | 0 | |
| Pre-Surgery Pathology Number of Patients (%) | Biopsy Gleason 3+3 (ISUP grade 1) | 77 (51.0%) | 53 (63.1%) | 18 |
| Biopsy Gleason 3+4 (ISUP grade 2) | 38 (25.2%) | 23 (27.4%) | 4 | |
| Biopsy Gleason 4+3 (ISUP grade 3) | 20 (13.2%) | 4 (4.8%) | 0 | |
| Biopsy Gleason 8 (ISUP grade 4) | 16 (10.6%) | 4 (4.8%) | 0 | |
| Clinical Stage cT1 | 97 (64.2%) | 84 (100%) | 22 (100%) | |
| Clinical Stage cT2 | ||||
| Clinical Stage cT3 | 54 (35.8%) | 0 | 0 | |
| Post-Surgery Pathology Number of Patients (%) | Pathology Gleason 3+3 (ISUP grade 1) | 46 (30.5%) | 34 (40.5%) | 13 (59.1%) |
| Pathology Gleason 3+4 (ISUP grade 2) | 52 (34.4%) | 32 (38.1%) | 9 (40.9%) | |
| Pathology Gleason 4+3 (ISUP grade 3) | 31 (20.5%) | 11 (13.1%) | 0 | |
| Pathology Gleason 8 (ISUP grade 4) | 22 (14.6%) | 7 (8.3%) | 0 | |
| Pathology Stage pT2 | 88 (58.3%) | 61 (72.6%) | 17 (77.3%) | |
| Pathology Stage pT3 | 63 (41.7%) | 22 (26.2%) | 5 (22.7%) | |
| Pathology Stage pT4 | 0 (0%) | 1 (1.2%) | 0 | |
| Positive Surgical Margins | 33 (21.9%) | 17 (20.2%) | 4 (18.2%) | |
| Capsular Status penetrated with tumor cells | 75/145 (51.7%) | 23/82 (28.0%) | 4/21 (19.0%) | |
| Positive Lymph Node Invasion | 10 (6.6%) | 2 (2.4%) | 0 | |
| Follow-up (months) | Mean | 73.7 | 87.0 | 102.8 |
| Median | 73.6 | 82.1 | 92.8 | |
| BCR events (%) | BCR within 5 years | 45 (29.8%) | 16 (19.0%) | 0 |
| Salvage Treatment Events (%) | SRT within 5 years | 12 (7.9%) | 4 (4.8%) | 0 |
| SADT within 5 years | 16 (10.6%) | 6 (7.1%) | 0 | |
| Survival Events (%) | PCSS within 5 years | 0 (0.7%) | 0 | 0 |
| OS within 5 years | 1 (0.7%) | 0 | 0 |
| Model | n | Outcome | n (Sample_1; Mean Probability p) | n (Sample_2; Mean Probability p) | p-Value |
|---|---|---|---|---|---|
| CAPRA&PDE4D5/7/9_BCR | 84 | Adverse Pathology (no vs. yes) | No (n = 52; 0.3) | Yes (n = 32; 0.5) | 0.006 |
| CAPRA&PDE4D5/7/9_BCR | 84 | RP ISUP Gleason (≤2 vs. ≥3) | ≤2 (n = 66; 0.5) | ≥3 (n = 18; 0.65) | <0.0001 |
| CAPRA&PDE4D5/7/9_BCR | 84 | Pathology pT (≤pT3a vs. > pT3a) | ≤pT3a (n = 76; 0.34) | >pT3a (n = 8; 0.71) | 0.002 |
| Model | n | Outcome | OR | OR (95% CI) | p-Value | AUROC |
|---|---|---|---|---|---|---|
| CAPRA Score | 84 | Adverse Pathology | 1.4 | 0.95–2.1 | 0.09 | 0.6 |
| PDE4D5/7/9_BCR | 1.6 | 1.1–2.3 | 0.02 | 0.67 | ||
| CAPRA&PDE4D579_BCR | 1.4 | 1.1–1.7 | 0.01 | 0.68 | ||
| CAPRA Score | 84 | RP ISUP Gleason >2 | 2.4 | 1.4–4.1 | 0.002 | 0.74 |
| PDE4D5/7/9_BCR | 2.5 | 1.5–4.1 | 0.0004 | 0.8 | ||
| CAPRA&PDE4D579_BCR | 1.9 | 1.4–2.7 | 0.0002 | 0.82 | ||
| CAPRA Score | 84 | RP ISUP Gleason >1 | 1.6 | 1.1–2.4 | 0.02 | 0.65 |
| PDE4D5/7/9_BCR | 1.4 | 1.0–2.2 | 0.04 | 0.65 | ||
| CAPRA&PDE4D579_BCR | 1.4 | 1.1–1.7 | 0.01 | 0.68 |
| Model | n | Outcome | OR | OR (95% CI) | p-Value | AUROC |
|---|---|---|---|---|---|---|
| CAPRA Score | 84 | Adverse Pathology | 1.3 | 0.8–1.9 | 0.3 | 0.67 |
| PDE4D5/7/9_BCR | 1.5 | 1.0–2.2 | 0.04 | |||
| CAPRA Score | 84 | RP ISUP Gleason >2 | 2 | 1.1–3.8 | 0.02 | 0.82 |
| PDE4D5/7/9_BCR | 2.2 | 1.3–3.7 | 0.004 | |||
| CAPRA Score | 84 | RP ISUP Gleason >1 | 1.5 | 0.99–2.3 | 0.06 | 0.68 |
| PDE4D5/7/9_BCR | 1.4 | 0.92–2.1 | 0.1 |
| Adverse Pathology Outcome | NPV [%] | |
|---|---|---|
| Model | CAPRA&PDE4D5/7/9_BCR | PRIAS (Active Surveillance Inclusion) |
| Model cut-off | risk score < 0.1 (n = 22; 26.2%) | PSA < 10 ng/mL; PSAD < 0.2; ISUP Gleason grade 1; cT ≤ cT2; ≤2 tumor positive biopsy cores (n = 18; 21.4%) |
| Freedom of Adverse Pathology (AP) | 82.0 | 72.1 |
| ISUP pathology Gleason ≤2 | 100 | 94.4 |
| ISUP pathology Gleason = 1 | 59.1 | 55.6 |
| Pathological pT ≤3a | 100 | 94.4 |
| Pathological pT ≤2 | 77.3 | 77.8 |
| Capsular Status (not penetrated) | 81.8 | 76.5 |
| Negative Surgical Margins | 81.8 | 94.1 |
| Freedom of Lymph Node Invasion | 100 | 100 |
| Freedom of BCR | 100 | 94.4 |
| Freedom of Secondary Therapy | 100 | 100 |
| Adverse Pathology Outcome | NPV [%] |
|---|---|
| Model | CAPRA&PDE4D5/7/9_BCR |
| Model cut-off | risk score <0.1 (n = 29; 19.2%) |
| Freedom of Adverse Pathology (AP) | 72.4 |
| ISUP pathology Gleason ≤2 | 93.1 |
| ISUP pathology Gleason = 1 | 53.3 |
| Pathological pT ≤3a | 96.6 |
| Pathological pT ≤2 | 75.9 |
| Capsular Status (not penetrated) | 75.9 |
| Negative Surgical Margins | 75.9 |
| Freedom of Lymph Node Invasion | 100 |
| Freedom of BCR | 100 |
| Freedom of Secondary Therapy | 100 |
| Adverse Pathology Outcome | PPV [%] |
|---|---|
| Model | CAPRA&PDE4D5/7/9_BCR |
| Model cut-off | risk score >0.835 (n = 42; 27.8%) |
| Adverse Pathology (AP) | 81.0 |
| ISUP pGleason >2 | 64.2 |
| ISUP pGleason >1 | 92.9 |
| Pathological pT >3a | 38.1 |
| Pathological pT >2 | 69,0 |
| Capsular Status (penetrated) | 58.5 |
| Positive Surgical Margins | 24.1 |
| Lymph Node Invasion | 14.3 |
| BCR | 71.4 |
| Secondary Therapy | 40.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gulliver, C.; Huss, S.; Semjonow, A.; Baillie, G.S.; Hoffmann, R. The CAPRA&PDE4D5/7/9 Prognostic Model Is Significantly Associated with Adverse Post-Surgical Pathology Outcomes. Cancers 2023, 15, 262. https://doi.org/10.3390/cancers15010262
Gulliver C, Huss S, Semjonow A, Baillie GS, Hoffmann R. The CAPRA&PDE4D5/7/9 Prognostic Model Is Significantly Associated with Adverse Post-Surgical Pathology Outcomes. Cancers. 2023; 15(1):262. https://doi.org/10.3390/cancers15010262
Chicago/Turabian StyleGulliver, Chloe, Sebastian Huss, Axel Semjonow, George S. Baillie, and Ralf Hoffmann. 2023. "The CAPRA&PDE4D5/7/9 Prognostic Model Is Significantly Associated with Adverse Post-Surgical Pathology Outcomes" Cancers 15, no. 1: 262. https://doi.org/10.3390/cancers15010262