
Thyroid Cancer Persistence in Patients with Unreliable Thyroglobulin Measurement: Circulating microRNA as Candidate Alternative Biomarkers
 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Response Assessment and Follow-Up
2.3. Imaging Studies
2.4. Laboratory Analysis
2.5. Biochemical Markers
2.6. Serum miRNAs Measurement
2.6.1. RNA Isolation, Reverse Transcription, and miRNAs Expression by Real Time PCR
2.6.2. RT-Quantitative Polymerase Chain Reaction (qPCR) of miRNAs
3. Results
Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aschebrook-Kilfoy, B.; Ward, M.H.; Sabra, M.M.; Devesa, S.S. Thyroid cancer incidence patterns in the United States by histologic type, 1992–2006. Thyroid 2011, 21, 125–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pacini, F.; Molinaro, E.; Lippi, F.; Castagna, M.G.; Agate, L.; Ceccarelli, C.; Taddei, D.; Elisei, R.; Capezzone, M.; Pinchera, A. Prediction of disease status by recombinant human TSH-stimulated serum Tg in the postsurgical follow-up of differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 2001, 86, 5686–5690. [Google Scholar] [CrossRef]
- Torlontano, M.; Crocetti, U.; D’Aloiso, L.; Bonfitto, N.; Di Giorgio, A.; Modoni, S.; Valle, G.; Frusciante, V.; Bisceglia, M.; Filetti, S.; et al. Serum thyroglobulin and 131I whole body scan after recombinant human TSH stimulation in the follow-up of low-risk patients with differentiated thyroid cancer. Eur. J. Endocrinol. 2003, 148, 19–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamartina, L.; Grani, G.; Durante, C.; Borget, I.; Filetti, S.; Schlumberger, M. Follow-up of differentiated thyroid cancer—What should (and what should not) be done. Nat. Rev. Endocrinol. 2018, 14, 538–551. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.; Tennant, S.; Perros, P. Serum thyroglobulin in the monitoring of differentiated thyroid cancer. Scand. J. Clin. Lab. Investig. Suppl. 2016, 245, S119–S123. [Google Scholar] [CrossRef]
- Giovanella, L. Circulating biomarkers for the detection of tumor recurrence in the postsurgical follow-up of differentiated thyroid carcinoma. Curr. Opin. Oncol. 2020, 32, 7–12. [Google Scholar] [CrossRef]
- Giovanella, L.; Feldt-Rasmussen, U.; Verburg, F.A.; Grebe, S.K.; Plebani, M.; Clark, P.M. Thyroglobulin measurement by highly sensitive assays: Focus on laboratory challenges. Clin. Chem. Lab. Med. 2015, 53, 1301–1314. [Google Scholar] [CrossRef]
- Verburg, F.A.; Luster, M.; Cupini, C.; Chiovato, L.; Duntas, L.; Elisei, R.; Feldt-Rasmussen, U.; Rimmele, H.; Seregni, E.; Smit, J.W.; et al. Implications of thyroglobulin antibody positivity in patients with differentiated thyroid cancer: A clinical position statement. Thyroid 2013, 23, 1211–1225. [Google Scholar] [CrossRef]
- Chiovato, L.; Latrofa, F.; Braverman, L.E.; Pacini, F.; Capezzone, M.; Masserini, L.; Grasso, L.; Pinchera, A. Disappearance of humoral thyroid autoimmunity after complete removal of thyroid antigens. Ann. Intern. Med. 2003, 139, 346–351. [Google Scholar] [CrossRef]
- Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; Pacini, F.; Schlumberger, M.; et al. Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartel, D.P. MicroRNAs: Target recognition and regulatory functions. Cell 2009, 136, 215–233. [Google Scholar] [CrossRef] [Green Version]
- Lim, L.P.; Lau, N.C.; Garrett-Engele, P.; Grimson, A.; Schelter, J.M.; Castle, J.; Bartel, D.P.; Linsley, P.S.; Johnson, J.M. Microarray analysis shows that some microRNAs downregulate large numbers of target mRNAs. Nature 2005, 433, 769–773. [Google Scholar] [CrossRef] [PubMed]
- Calin, G.A.; Croce, C.M. MicroRNA signatures in human cancers. Nat. Rev. Cancer 2006, 6, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Calin, G.A.; Croce, C.M. MicroRNA-cancer connection: The beginning of a new tale. Cancer Res. 2006, 66, 7390–7394. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Pan, X.; Cobb, G.P.; Anderson, T.A. microRNAs as oncogenes and tumor suppressors. Dev. Biol. 2007, 302, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hydbring, P. Badalian-Very G: Clinical applications of microRNAs. Version 3. F1000Res 2013, 2, 136. [Google Scholar] [CrossRef]
- Ortiz-Quintero, B. Extracellular MicroRNAs as Intercellular Mediators and Noninvasive Biomarkers of Cancer. Cancers 2020, 12, 3455. [Google Scholar] [CrossRef] [PubMed]
- Hitu, L.; Gabora, K.; Bonci, E.A.; Piciu, A.; Hitu, A.C.; Stefan, P.A.; Piciu, D. MicroRNA in Papillary Thyroid Carcinoma: A Systematic Review from 2018 to June 2020. Cancers 2020, 12, 3118. [Google Scholar] [CrossRef]
- Hu, Y.; Wang, H.; Chen, E.; Xu, Z.; Chen, B.; Lu, G. Candidate microRNAs as Biomarkers of Thyroid Carcinoma: A Systematic Review, Meta-Analysis, and Experimental Validation. Cancer Med. 2016, 5, 2602–2614. [Google Scholar] [CrossRef]
- Dettmer, M.; Perren, A.; Moch, H.; Komminoth, P.; Nikiforov, Y.E.; Nikiforova, M.N. Comprehensive MicroRNA expression profiling identifies novel markers in follicular variant of papillary thyroid carcinoma. Thyroid 2013, 23, 1383–1389. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Z.; Hang, Y.K.; Liu, J.B.; Hou, Y.Q.; Wang, N.; Wang, M.J. Over-expression of microRNA-375 inhibits papillary thyroid carcinoma cell proliferation and induces cell apoptosis by targeting ERBB2. J. Pharmacol. Sci. 2016, 130, 78–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, S.; Liu, Y.; Wang, J.; Guo, Z.; Zhang, Q.; Yu, F.; Zhang, Y.; Huang, K.; Li, Y.; Song, E.; et al. Circulating microRNA profiles as potential biomarkers for diagnosis of papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2012, 97, 2084–2092. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.S.; Lim, Y.S.; Lee, J.C.; Wang, S.G.; Park, H.Y.; Kim, S.Y.; Lee, B.J. Differential expression levels of plasma-derived miR-146b and miR-155 in papillary thyroid cancer. Oral Oncol. 2015, 51, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Rosignolo, F.; Sponziello, M.; Giacomelli, L.; Russo, D.; Pecce, V.; Biffoni, M.; Bellantone, R.; Lombardi, C.P.; Lamartina, L.; Grani, G.; et al. Identification of Thyroid-Associated Serum microRNA Profiles and Their Potential Use in Thyroid Cancer Follow-Up. J. Endocr. Soc. 2017, 1, 3–13. [Google Scholar]
- Graham, M.E.; Hart, R.D.; Douglas, S.; Makki, F.M.; Pinto, D.; Butler, A.L.; Bullock, M.; Rigby, M.H.; Trites, J.R.; Taylor, S.M.; et al. Serum microRNA profiling to distinguish papillary thyroid cancer from benign thyroid masses. J. Otolaryngol. Head Neck Surg. 2015, 44, 33. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.C.; Zhao, J.T.; Clifton-Bligh, R.J.; Gill, A.; Gundara, J.S.; Ip, J.C.; Glover, A.; Sywak, M.S.; Delbridge, L.W.; Robinson, B.G.; et al. MicroRNA-222 and microRNA-146b are tissue and circulating biomarkers of recurrent papillary thyroid cancer. Cancer 2013, 119, 4358–4365. [Google Scholar] [CrossRef]
- Campennì, A.; Giovanella, L.; Pignata, S.A.; Vento, A.; Alibrandi, A.; Sturiale, L.; Laudicella, R.; Comis, A.D.; Filice, R.; Giuffrida, G.; et al. Undetectable or low (<1 ng/ml) postsurgical thyroglobulin values do not rule out metastases in early stage differentiated thyroid cancer patients. Oncotarget 2018, 9, 17491–17500. [Google Scholar]
- Campennì, A.; Giovanella, L.; Siracusa, M.; Stipo, M.E.; Alibrandi, A.; Cucinotta, M.; Ruggeri, R.M.; Baldari, S. Is malignant nodule topography an additional risk factor for metastatic disease in low-risk differentiated thyroid cancer? Thyroid 2014, 24, 1607–1611. [Google Scholar] [CrossRef]
- Campennì, A.; Giovanella, L.; Pignata, S.A.; Violi, M.A.; Siracusa, M.; Alibrandi, A.; Moleti, M.; Amato, E.; Ruggeri, R.M.; Vermiglio, F.; et al. Thyroid remnant ablation in differentiated thyroid cancer: Searching for the most effective radioiodine activity and stimulation strategy in a real-life scenario. Nucl. Med. Commun. 2015, 36, 1100–1106. [Google Scholar] [CrossRef]
- Cai, S.; Ma, J.; Wang, Y.; Cai, Y.; Xie, L.; Chen, X.; Yang, Y.; Peng, Q. Biomarker Value of miR-221 and miR-222 as Potential Substrates in the Differential Diagnosis of Papillary Thyroid Cancer Based on Data Synthesis and Bioinformatics Approach. Front. Endocrinol. 2022, 12, 794490. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Zheng, X.; Hu, M.; Cui, Y.; Zhong, Q.; Wang, S.; Huang, F. MiRNA-221/222 in Thyroid Cancer: A Meta-Analysis. Clin. Chim. Acta 2018, 484, 284–292. [Google Scholar] [CrossRef]
- Ye, T.; Zhong, L.; Ye, X.; Liu, J.; Li, L.; Yi, H. miR-221-3p and miR-222-3p Regulate the SOCS3/STAT3 Signaling Pathway to Downregulate the Expression of NIS and Reduce Radiosensitivity in Thyroid Cancer. Exp. Ther. Med. 2021, 21, 652. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Chen, Y.; Lin, W.; Zheng, J.; Liu, Y.; Zou, J.; Cai, J.; Chen, Y.; Li, Z.; Chen, Y. Prognostic and ImmuneInfiltrate Significance of miR-222-3p and Its Target Genes in Thyroid Cancer. Front. Genet. 2021, 12, 710412. [Google Scholar] [CrossRef] [PubMed]
- Diao, Y.; Fu, H.; Wang, Q. MiR-221 Exacerbate Cell Proliferation and Invasion by Targeting TIMP3 in Papillary Thyroid Carcinoma. Am. J. Ther. 2017, 24, e317–e328. [Google Scholar] [CrossRef] [Green Version]
- Mahmoudian-Sani, M.R.; Mehri-Ghahfarrokhi, A.; Asadi-Samani, M.; Mobini, G.R. RNAs as Biomarkers for the Diagnosis and Prognosis of Thyroid Cancer. Eur. Thyroid J. 2017, 6, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Pfaffl, M.W. A new mathematical model for relative quantification in real-time RT-PCR. Nucleic Acids Res. 2001, 29, e45. [Google Scholar] [CrossRef]
- Lu, J.; Getz, G.; Miska, E.A.; Alvarez-Saavedra, E.; Lamb, J.; Peck, D.; Sweet-Cordero, A.; Ebert, B.L.; Mak, R.H.; Ferrando, A.A.; et al. MicroRNA expression profiles classify human cancers. Nature 2005, 435, 834–838. [Google Scholar] [CrossRef]
- Orellana, E.A.; Kasinski, A.L. MicroRNAs in cancer: A historical perspective on the path from discovery to therapy. Cancers 2015, 7, 1388–1405. [Google Scholar] [CrossRef]
- Faam, B.; Ghaffari, M.A.; Ghadiri, A.; Azizi, F. Epigenetic modifications in human thyroid cancer. Biomed. Rep. 2015, 3, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Zhang, D.; Niu, Q.; Nan, Y.; Shi, C.; Zhao, H.; Liang, X. Value of distinguishing differentiated thyroid carcinoma by miRNA. Oncol. Lett. 2016, 12, 79–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cong, D.; He, M.; Chen, S.; Liu, X.; Liu, X.; Sun, H. Expression profiles of pivotal microRNAs and targets in thyroid papillary carcinoma: An analysis of The Cancer Genome Atlas. Onco Targets Ther. 2015, 8, 2271–2277. [Google Scholar] [PubMed]
- Yang, Z.; Yuan, Z.; Fan, Y.; Deng, X.; Zheng, Q. Integrated analyses of microRNA and mRNA expression profiles in aggressive papillary thyroid carcinoma. Mol. Med. Rep. 2013, 8, 1353–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Zhang, H.; He, L.; Dong, W.; Li, J.; Shan, Z.; Teng, W. Association between the expression of four upregulated miRNAs and extrathyroidal invasion in papillary thyroid carcinoma. Onco Targets Ther. 2013, 6, 281–287. [Google Scholar] [CrossRef] [Green Version]
- Zembska, A.; Jawiarczyk-Przybyłowska, A.; Wojtczak, B.; Bolanowski, M. MicroRNA Expression in the Progression and Aggressiveness of Papillary Thyroid Carcinoma. Anticancer Res. 2019, 39, 33–40. [Google Scholar] [CrossRef]
- Zhang, Y.; Xu, D.; Pan, J.; Yang, Z.; Chen, M.; Han, J.; Zhang, S.; Sun, L.; Qiao, H. Dynamic monitoring of circulating microRNAs as a predictive biomarker for the diagnosis and recurrence of papillary thyroid carcinoma. Oncol. Lett. 2017, 13, 4252–4266. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
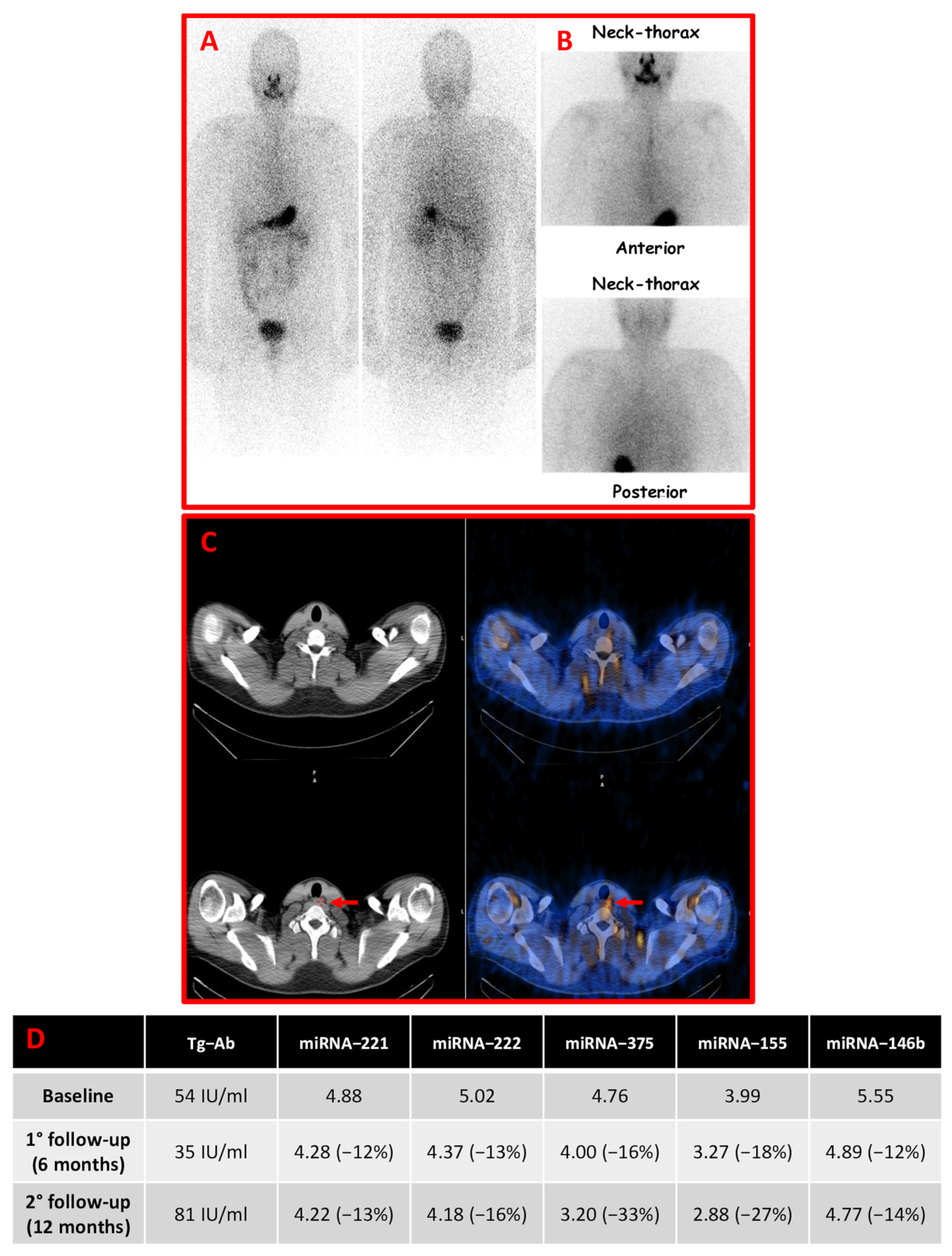
| miRNA-221 | miRNA-222 | miRNA-375 | miRNA-155 | miRNA-146b | |
|---|---|---|---|---|---|
| PTC patients (n = 49) | |||||
| Mean ± SD | 3.64 ± 0.89 | 3.56 ± 0.91 | 3.18 ± 0.63 | 3.11 ± 0.66 | 3.49 ± 0.78 |
| Median | 3.47 | 3.15 | 3.22 | 3.05 | 3.26 |
| Range | 2.45–5.86 | 2.75–6.50 | 2.11–4.76 | 2.24–4.89 | 2.98–5.55 |
| Healthy Controls (n = 20) | |||||
| Mean ± SD | 0.85 ± 0.21 | 0.76 ± 0.27 | 0.74 ± 0.32 | 0.78 ± 0.28 | 0.75 ± 0.25 |
| Median | 0.89 | 0.83 | 0.82 | 0.86 | 0.84 |
| Range | 0.24–1.11 | 0.11–1.11 | 0.11–1.15 | 0.11–1.14 | 0.32–1.12 |
| p-value * | 0.0001 | 0.0001 | 0.0001 | 0.0001 | 0.0001 |
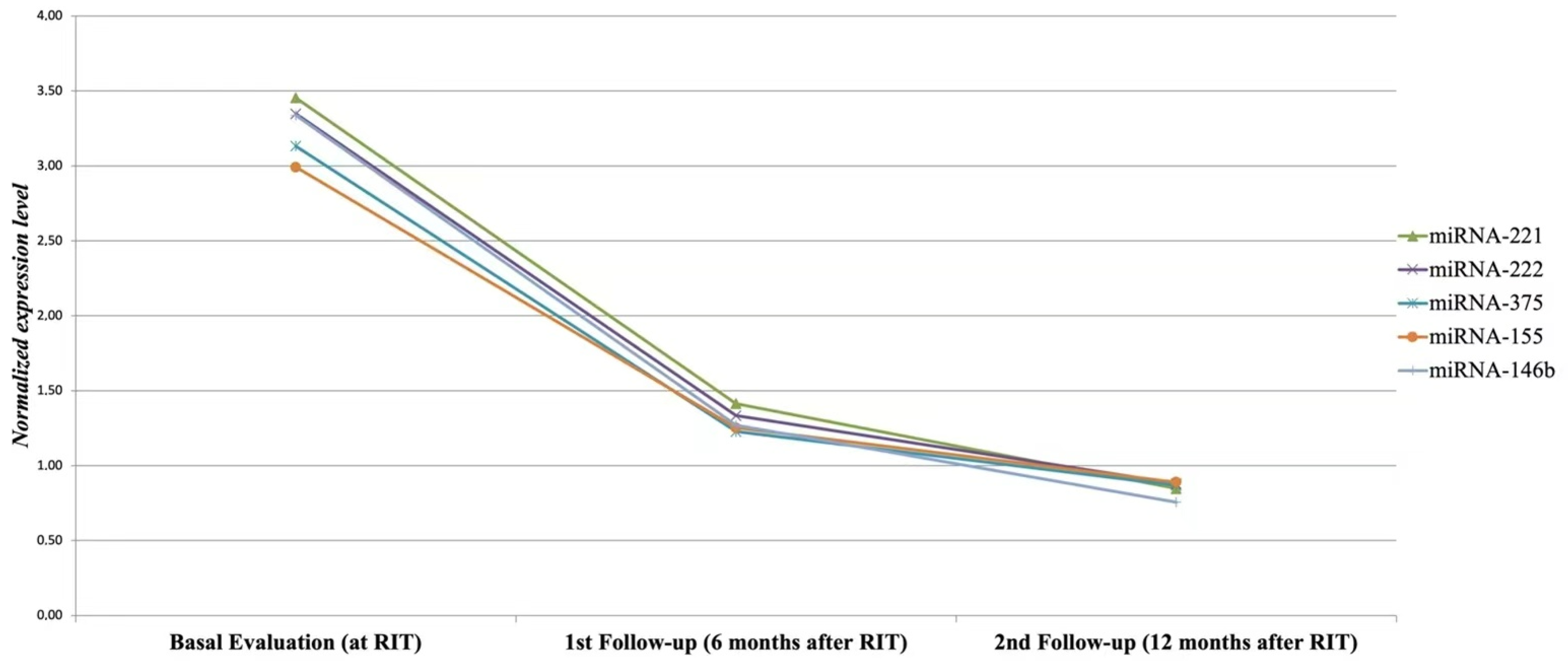
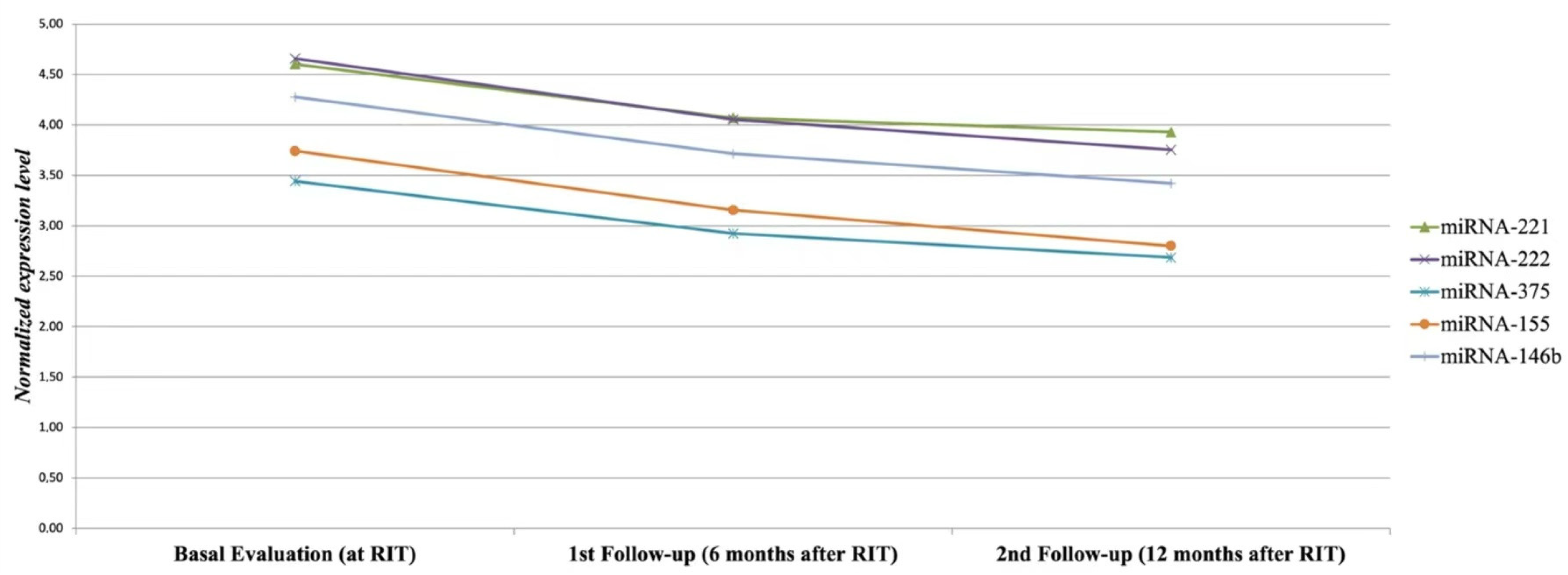
| miRNAs * | Basal Evaluation | 1st Follow-up | 2nd Follow-up |
|---|---|---|---|
| 221 mean ± SD median value | 3.64 ± 0.89 3.47 | 1.84 ± 1.1 1.46 | 1.35 ± 1.20 0.97 |
| 222 mean ± SD median value | 3.56 ± 0.91 3.15 | 1.77 ± 1.11 1.34 | 1.34 ± 1.12 0.99 |
| 375 mean ± SD median value | 3.18 ± 0.63 3.22 | 1.50 ± 0.72 1.22 | 1.16 ± 0.72 0.97 |
| 155 mean ± SD median value | 3.11 ± 0.66 3.05 | 1.56 ± 0.82 1.22 | 1.20 ± 0.77 0.99 |
| 146b mean ± SD median value | 3.49 ± 0.78 3.26 | 1.66 ± 0.99 1.22 | 1.19 ± 1.03 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campennì, A.; Aguennouz, M.; Siracusa, M.; Alibrandi, A.; Polito, F.; Oteri, R.; Baldari, S.; Ruggeri, R.M.; Giovanella, L. Thyroid Cancer Persistence in Patients with Unreliable Thyroglobulin Measurement: Circulating microRNA as Candidate Alternative Biomarkers. Cancers 2022, 14, 5620. https://doi.org/10.3390/cancers14225620
Campennì A, Aguennouz M, Siracusa M, Alibrandi A, Polito F, Oteri R, Baldari S, Ruggeri RM, Giovanella L. Thyroid Cancer Persistence in Patients with Unreliable Thyroglobulin Measurement: Circulating microRNA as Candidate Alternative Biomarkers. Cancers. 2022; 14(22):5620. https://doi.org/10.3390/cancers14225620
Chicago/Turabian StyleCampennì, Alfredo, M’hammed Aguennouz, Massimiliano Siracusa, Angela Alibrandi, Francesca Polito, Rosaria Oteri, Sergio Baldari, Rosaria Maddalena Ruggeri, and Luca Giovanella. 2022. "Thyroid Cancer Persistence in Patients with Unreliable Thyroglobulin Measurement: Circulating microRNA as Candidate Alternative Biomarkers" Cancers 14, no. 22: 5620. https://doi.org/10.3390/cancers14225620