
Involvement of HHV-4 (Epstein–Barr Virus) and HHV-5 (Cytomegalovirus) in Inflammatory Bowel Disease and Colorectal Cancer: A Meta-Analysis

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
- Adenoviridae: Adenovirus (ADV).
- Anelloviridae: Transfusion Transmitted Virus (or Torque Teno virus, TTV).
- Astroviridae: Astrovirus (AstV).
- Bunyaviridae: members of the Orthobunyavirus genus (BV).
- Caliciviridae: Norovirus (NV), Sapovirus (SaV).
- Herpesviridae: Human Herpesvirus 1 (HHV-1 or Herpes Simplex virus), Human Herpesvirus 3 (HHV-3, or Varicella Zoster virus), Human Herpesvirus 4 (HHV-4, or Epstein–Barr virus), Human Herpesvirus 5 (HHV-5, or Cytomegalovirus), Human Herpesvirus 6 (HHV-6), Human Herpesvirus 8 (HHV-8, or Kaposi’s sarcoma-associated herpesvirus), Inoue–Melnick virus (IMV).
- Hepadnaviridae: Human Hepatitis B virus (HBV).
- Flaviviridae: Human Hepatitis C virus (HCV).
- Matonaviridae: Rubella virus (RuV).
- Retroviridae: Human Immunodeficiency virus (HIV), Human T-cell lymphotropic virus type 1 (HTLV-I).
- Papillomaviridae: Human Papilloma virus (HPV).
- Parvoviridae: Parvovirus B19 (B19), Bocaparvovirus (HuBV).
- Polyomaviridae: BK virus (BKV), John Cunningham virus (JCV), Merkel cell polyomavirus (MCPV), Polyovirus 5 (PyV6), Simian virus 40 (SV40).
- Paramyxoviridae: Measles virus (MeV), Mumps virus (MuV).
- Reoviridae: Reovirus (RV), Rotavirus (RoV).
- Syphoviridae: phages of the order Caudovirales.
- Myoviridae: phages of the order Caudovirales.
- Inoviridae: member of the Inovirus genus.
- Herpesviruses (Herpesviridae).
- Respiratory viruses (Adenoviridae, Bocaviridae).
- Papillomaviruses (Papillomaviridae).
- Epithelial viruses (Anelloviridae, Bunyaviridae, Matonaviridae, Paramyxoviridae, Parvoviridae).
- Intestinal viruses (Astroviridae, Caliciviridae, Noroviridae, Reoviridae).
- Polyomaviruses (Polyomaviridae).
- Hepadnaviruses (Hepadnaviridae).
- Flaviruses (Flaviviridae).
- Retroviruses (Retroviridae).
- Phages (Syphoviridae, Myoviridae, Inoviridae).
2.2. Eligibility Criteria
2.3. Information Sources
2.4. Search
- Pathology: “intestinal neoplasm”, “colorectal cancer”, “rectal neoplasia”, “Crohn’s disease”, “inflammatory bowel disease”, “ulcerative colitis”, “regional enteritis”, “granulomatous colitis”, “terminal ileitis”.
- Pathogen: “virus”, “giant virus”, “bacteriophage”, “Siphoviridae”, “Podoviridae”, “T7-like virus”, “φ-like virus”, “Herellevirus”, “Myoviridae”, “Tristromavirus”, “Bicaudavirus”, “Pycodnaviridae”, “Caudovirales”, “Ackermannvirus”, “Ampullavirus”, “Clavavirus”, “Corticoviridae”, “Cystoviridae”, “Fuselloviridae”, “Globulovirus”, “Guttaviridae”, “Inoviridae”, “Leviviridae”, “Lipothrixviridae”, “Microviridae”, “Plasmavirus”, “Pleolipovirus”, “Rudiviridae”, “Sphaerolipovirus”, “Tectivirus”, “Turrivirus”, “Polyomaviridae”, “Poxviridae”, “Simian virus 40”, “Papillomaviridae”, “Herpesviridae”.
2.5. Study Selection
2.6. Data Collection Process
2.7. Data Items
2.8. Risk of Bias in the Individual Studies
2.9. Summary Measures
2.10. Synthesis of the Results
2.11. Risk of Bias across the Studies
- Representativeness: if the selected article included more than 50 participants, a cut-off accepted to provide the statistically solid results, a positive value was assigned.
- Control group: if the selected article included a control group, a positive value was assigned.
- Documentation: if the selected article was not a letter, a positive value was assigned.
- Outcome: if the selected article was not a virome study, a positive value was assigned.
- Co-infections: if the selected article did not report samples with co-infections, a positive value was assigned.
- 5 points: High
- 3–4 points: Moderate
- 1–2 points: Low
2.12. Additional Analyses
2.13. Statistical Analysis
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Disease
- CRC (n = 123, 48.2%).
- GC (n = 28, 11.0%).
- IBD (n = 104, 40.8%).
3.2.2. Detection Method
- Hybridization (n = 49, 18.8%). Fluorescent immuno-assay (IFA), in situ hybridization (ISH) or immuno-histochemistry (IHC).
- PCR (n = 118, 46.5%). Polymerase chain reaction (PCR), both end-point or quantitative.
- Archival (n = 25, 9.8%). Medical records obtained from the retrospective studies, and without direct detection of the virus within the specimens.
- Serology (n = 55, 21.6%). Enzyme-linked immunoassay (ELISA) and plaque assay.
- Virome (n = 9, 3.5%). Whole-genome sequencing (WGS) by massively parallel sequencing (MPS).
3.2.3. Type of Tissue
- Colon and rectum tissue (n = 114, 44.7%).
- Gastrointestinal (stomach) tissue (n = 43, 16.9%).
- Stools (n = 18, 7.1%).
- Sera (n = 56, 22.0%).
- Medical records (n = 24, 9.4%).
3.2.4. Viral Groups
- Respiratory viruses (n = 8, 3.1%).
- Intestinal viruses (n = 11, 4.3%).
- Epithelial viruses (n = 20, 7.8%).
- Herpesviruses (n = 107, 42.0%).
- Retroviruses (n = 5, 2.0%).
- Polyomaviruses (n = 44, 17.3%).
- Papillomaviruses (n = 28, 11.0%).
- Hepadnaviruses (n = 16, 6.3%).
- Flaviviruses (n = 9, 3.5%).
- Phage group (n = 7, 2.7%).
3.3. Quantitative Analysis: CRC
3.4. Quantitative Analysis: GC
3.5. Quantitative Analysis: IBD
3.6. Qualitative Analysis of the Virome Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Plummer, M.; de Martel, C.; Vignat, J.; Ferlay, J.; Bray, F.; Franceschi, S. Global Burden of Cancers Attributable to Infections in 2012: A Synthetic Analysis. Lancet Glob. Health 2016, 4, e609–e616. [Google Scholar] [CrossRef] [Green Version]
- De Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, G.M. Global Burden of Cancer Attributable to Infections in 2018: A Worldwide Incidence Analysis. Lancet Glob. Health 2020, 8, e180–e190. [Google Scholar] [CrossRef] [Green Version]
- Oyervides-Muoz, M.A.; Prez-Maya, A.A.; Rodrguez-Gutirrez, H.F.; Gmez-Macias, G.S.; Fajardo-Ramrez, O.R.; Trevio, V.; Barrera-Saldaa, H.A.; Garza-Rodrguez, M.L. Understanding the HPV Integration and Its Progression to Cervical Cancer. Infect. Genet. Evol. 2018, 61, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Bucchi, D.; Stracci, F.; Buonora, N.; Masanotti, G. Human Papillomavirus and Gastrointestinal Cancer: A Review. World J. Gastroenterol. 2016, 22, 7415–7430. [Google Scholar] [CrossRef] [PubMed]
- Forman, D.; de Martel, C.; Lacey, C.J.; Soerjomatarama, I.; Lortet-Tieulent, J.; Bruni, L.; Vignat, J.; Ferlay, J.; Bray, F.; Plummer, M.; et al. Global Burden of Human Papillomavirus and Related Diseases. Vaccine 2012, 30, F12–F23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries and 25 Major Cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Ma, H.; Brosens, L.A.A.; Offerhaus, G.J.A.; Giardiello, F.M.; de Leng, W.W.J.; Montgomery, E.A. Pathology and Genetics of Hereditary Colorectal Cancer. Pathology 2018, 50, 49–59. [Google Scholar] [CrossRef]
- Müller, M.F.; Ibrahim, A.E.; Arends, M.J. Molecular Pathological Classification of Colorectal Cancer. Virchows Arch. 2016, 469, 125–134. [Google Scholar] [CrossRef] [Green Version]
- Rawla, P.; Barsouk, A. Epidemiology of Gastric Cancer: Global Trends, Risk Factors and Prevention. Przeglad Gastroenterol. 2019, 14, 26–38. [Google Scholar] [CrossRef]
- Simon, K. Colorectal Cancer Development and Advances in Screening. Clin. Interv. Aging 2016, 11, 967–976. [Google Scholar] [CrossRef]
- Hruby, A.; Hu, F.B. The Epidemiology of Obesity: A Big Picture. PharmacoEconomics 2015, 33, 673–689. [Google Scholar] [CrossRef]
- Machlowska, J.; Baj, J.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies. Int. J. Mol. Sci. 2020, 21, 4012. [Google Scholar] [CrossRef]
- Axelrad, J.E.; Lichtiger, S.; Yajnik, V. Inflammatory Bowel Disease and Cancer: The Role of Inflammation, Immunosuppression, and Cancer Treatment. World J. Gastroenterol. 2016, 22, 4794. [Google Scholar] [CrossRef]
- Murata, M. Inflammation and Cancer. Environ. Health Prev. Med. 2018, 23, 50. [Google Scholar] [CrossRef] [Green Version]
- Weedon, D.D.; Shorter, R.G.; Ilstrup, D.M.; Huizenga, K.A.; Taylor, W.F. Crohn’s Disease and Cancer. N. Engl. J. Med. 1973, 289, 1099–1103. [Google Scholar] [CrossRef]
- Gyde, S.N.; Prior, P.; Macartney, J.C.; Thompson, H.; Waterhouse, J.A.; Allan, R.N. Malignancy in Crohn’s Disease. Gut 1980, 21, 1024–1029. [Google Scholar] [CrossRef] [Green Version]
- Kalla, R.; Ventham, N.T.; Satsangi, J.; Arnott, I.D.R. Crohn’s Disease. BMJ Online 2014, 349, g6670. [Google Scholar] [CrossRef] [Green Version]
- Bounthavong, M.; Li, M.; Watanabe, J.H. An Evaluation of Health Care Expenditures in Crohn’s Disease Using the United States Medical Expenditure Panel Survey from 2003 to 2013. Res. Soc. Adm. Pharm. 2017, 13, 530–538. [Google Scholar] [CrossRef] [Green Version]
- Kappelman, M.D.; Moore, K.R.; Allen, J.K.; Cook, S.F. Recent Trends in the Prevalence of Crohn’s Disease and Ulcerative Colitis in a Commercially Insured US Population. Dig. Dis. Sci. 2013, 58, 519–525. [Google Scholar] [CrossRef] [Green Version]
- Lucas, C.; Barnich, N.; Nguyen, H.T.T. Microbiota, Inflammation and Colorectal Cancer. Int. J. Mol. Sci. 2017, 18, 1310–1337. [Google Scholar] [CrossRef]
- Hendler, S.A.; Barber, G.E.; Okafor, P.N.; Chang, M.S.; Limsui, D.; Limketkai, B.N. Cytomegalovirus Infection Is Associated with Worse Outcomes in Inflammatory Bowel Disease Hospitalizations Nationwide. Int. J. Colorectal Dis. 2020, 35, 897–903. [Google Scholar] [CrossRef]
- Waldum, H.; Fossmark, R. Gastritis, Gastric Polyps and Gastric Cancer. Int. J. Mol. Sci. 2021, 22, 6548. [Google Scholar] [CrossRef]
- Peng, C.; Ouyang, Y.; Lu, N.; Li, N. The NF-ΚB Signaling Pathway, the Microbiota, and Gastrointestinal Tumorigenesis: Recent Advances. Front. Immunol. 2020, 11, 1387. [Google Scholar] [CrossRef]
- Ng, C.; Li, H.; Wu, W.K.K.; Wong, S.H.; Yu, J. Genomics and Metagenomics of Colorectal Cancer. J. Gastrointest. Oncol. 2019, 10, 1164–1170. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.; Pfeiffer, R.; Camargo, M.C.; Rabkin, C.S. Meta-Analysis Shows That Prevalence of Epstein-Barr Virus-Positive Gastric Cancer Differs Based on Sex and Anatomic Location. Gastroenterology 2009, 137, 824–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, D.; Hogan, A.M.; Winter, D.C. Microbial and Viral Pathogens in Colorectal Cancer. Lancet Oncol. 2011, 12, 504–512. [Google Scholar] [CrossRef]
- Tamboli, C.P.; Neut, C.; Desreumaux, P.; Colombel, J.F. Dysbiosis in Inflammatory Bowel Disease. Gut 2004, 53, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cougnoux, A.; Dalmasso, G.; Martinez, R.; Buc, E.; Delmas, J.; Gibold, L.; Sauvanet, P.; Darcha, C.; Déchelotte, P.; Bonnet, M.; et al. Bacterial Genotoxin Colibactin Promotes Colon Tumour Growth by Inducing a Senescence-Associated Secretory Phenotype. Gut 2014, 63, 1932–1942. [Google Scholar] [CrossRef] [PubMed]
- Tjalsma, H.; Boleij, A.; Marchesi, J.R.; Dutilh, B.E. A Bacterial Driver-Passenger Model for Colorectal Cancer: Beyond the Usual Suspects. Nat. Rev. Microbiol. 2012, 10, 575–582. [Google Scholar] [CrossRef]
- De Paoli, P.; Carbone, A. Carcinogenic Viruses and Solid Cancers without Sufficient Evidence of Causal Association. Int. J. Cancer 2013, 133, 1517–1529. [Google Scholar] [CrossRef]
- Baandrup, L.; Thomsen, L.T.; Olesen, T.B.; Andersen, K.K.; Norrild, B.; Kjaer, S.K. The Prevalence of Human Papillomavirus in Colorectal Adenomas and Adenocarcinomas: A Systematic Review and Meta-Analysis. Eur. J. Cancer 2014, 50, 1446–1461. [Google Scholar] [CrossRef]
- Burnett-Hartman, A.N.; Newcomb, P.A.; Potter, J.D. Infectious Agents and Colorectal Cancer: A Review of Helicobacter pylori, Streptococcus Bovis, JC Virus, and Human Papillomavirus. Cancer Epidemiol. Biomarkers Prev. 2008, 17, 2970–2979. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.; Chen, X.-Z.; Waterboer, T.; Castro, F.A.; Brenner, H. Viral Infections and Colorectal Cancer: A Systematic Review of Epidemiological Studies. Int. J. Cancer 2015, 137, 12–24. [Google Scholar] [CrossRef]
- Coelho, T.R.; Almeida, L.; Lazo, P.A. JC Virus in the Pathogenesis of Colorectal Cancer, an Etiological Agent or Another Component in a Multistep Process? Virol. J. 2010, 7, 1–8. [Google Scholar] [CrossRef] [Green Version]
- De Villiers, E.-M.; Gunst, K.; Chakraborty, D.; Ernst, C.; Bund, T.; zur Hausen, H. A Specific Class of Infectious Agents Isolated from Bovine Serum and Dairy Products and Peritumoral Colon Cancer Tissue. Emerg. Microbes Infect. 2019, 8, 1205–1218. [Google Scholar] [CrossRef] [Green Version]
- Lepage, P.; Colombet, J.; Marteau, P.; Sime-Ngando, T. Dor Dysbiosis in Inflammatory Bowel Disease: A Role for Bacteriophages? Gut 2008, 57, 424–425. [Google Scholar] [CrossRef] [Green Version]
- Zuo, T.; Lu, X.J.; Zhang, Y.; Cheung, C.P.; Lam, S.; Zhang, F.; Tang, W.; Ching, J.Y.L.; Zhao, R.; Chan, P.K.S.; et al. Gut Mucosal Virome Alterations in Ulcerative Colitis. Gut 2019, 68, 1169–1179. [Google Scholar] [CrossRef] [Green Version]
- Norman, J.M.; Handley, S.A.; Baldridge, M.T.; Droit, L.; Liu, C.Y.; Keller, B.C.; Kambal, A.; Monaco, C.L.; Zhao, G.; Fleshner, P.; et al. Disease-Specific Alterations in the Enteric Virome in Inflammatory Bowel Disease. Cell 2015, 160, 447–460. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Nguyen, N.H.; Singh, S. A Primer on Systematic Reviews and Meta-Analyses. Semin. Liver Dis. 2018, 38, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sedgwick, P. Meta-Analyses: What Is Heterogeneity? BMJ 2015, 350, h1435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantel, N.; Haenszel, W. Statistical Aspects of the Analysis of Data from Retrospective Studies of Disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Lin, L.; Chu, H. Quantifying Publication Bias in Meta-Analysis. Biometrics 2018, 74, 785–794. [Google Scholar] [CrossRef]
- Van der Willik, E.M.; van Zwet, E.W.; Hoekstra, T.; van Ittersum, F.J.; Hemmelder, M.H.; Zoccali, C.; Jager, K.J.; Dekker, F.W.; Meuleman, Y. Funnel Plots of Patient-Reported Outcomes to Evaluate Health-Care Quality: Basic Principles, Pitfalls and Considerations. Nephrol. Carlton Vic. 2021, 26, 95–104. [Google Scholar] [CrossRef]
- Lo, C.K.L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing Reviewers’ to Authors’ Assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [Green Version]
- Perez-Brocal, V.; Garcia-Lopez, R.; Vazquez-Castellanos, J.F.; Nos, P.; Beltran, B.; Latorre, A.; Moya, A. Study of the Viral and Microbial Communities Associated with Crohn’s Disease: A Metagenomic Approach. Clin. Transl. Gastroenterol. 2013, 4, e36. [Google Scholar] [CrossRef]
- Perez-Brocal, V.; Garcia-Lopez, R.; Nos, P.; Beltran, B.; Moret, I.; Moya, A. Metagenomic Analysis of Crohn’s Disease Patients Identifies Changes in the Virome and Microbiome Related to Disease Status and Therapy, and Detects Potential Interactions and Biomarkers. Inflamm. Bowel Dis. 2015, 21, 2515–2532. [Google Scholar] [CrossRef]
- Fernandes, M.A.; Verstraete, S.G.; Phan, T.G.; Deng, X.; Stekol, E.; LaMere, B.; Lynch, S.V.; Heyman, M.B.; Delwart, E. Enteric Virome and Bacterial Microbiota in Children with Ulcerative Colitis and Crohn Disease. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 30–36. [Google Scholar] [CrossRef]
- Nakatsu, G.; Zhou, H.; Wu, W.K.K.; Wong, S.H.; Coker, O.O.; Dai, Z.; Li, X.; Szeto, C.H.; Sugimura, N.; Lam, T.Y.T.; et al. Alterations in Enteric Virome Are Associated with Colorectal Cancer and Survival Outcomes. Gastroenterology 2018, 155, 529–541.e5. [Google Scholar] [CrossRef]
- Hannigan, G.D.; Duhaime, M.B.; Ruffin, M.T.; Koumpouras, C.C.; Schloss, P.D. Diagnostic Potential and Interactive Dynamics of the Colorectal Cancer Virome. mBio 2018, 9, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Wagner, J.; Maksimovic, J.; Farries, G.; Sim, W.H.; Bishop, R.F.; Cameron, D.J.; Catto-Smith, A.G.; Kirkwood, C.D. Bacteriophages in Gut Samples from Pediatric Crohn’s Disease Patients. Inflamm. Bowel Dis. 2013, 19, 1598–1608. [Google Scholar] [CrossRef]
- Ungaro, F.; Massimino, L.; Furfaro, F.; Rimoldi, V.; Peyrin-Biroulet, L.; D’Alessio, S.; Danese, S. Metagenomic Analysis of Intestinal Mucosa Revealed a Specific Eukaryotic Gut Virome Signature in Early-Diagnosed Inflammatory Bowel Disease. Gut Microbes 2019, 10, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Zapatka, M.; Borozan, I.; Brewer, D.S.; Iskar, M.; Grundhoff, A.; Alawi, M.; Desai, N.; Sültmann, H.; Moch, H.; Cooper, C.S.; et al. The Landscape of Viral Associations in Human Cancers. Nat. Genet. 2020, 52, 320–330. [Google Scholar] [CrossRef] [Green Version]
- Dickersin, K.; Min, Y.-I. Publication Bias: The Problem That Won’t Go Away. Ann. N. Y. Acad. Sci. 1993, 703, 135–148. [Google Scholar] [CrossRef]
- DeVito, N.J.; Goldacre, B. Catalogue of Bias: Publication Bias. BMJ Evid.-Based Med. 2019, 24, 53–54. [Google Scholar] [CrossRef] [Green Version]
- Spineli, L.M.; Pandis, N. Publication Bias: Graphical and Statistical Methods. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Its Const. Soc. Am. Board Orthod. 2021, 159, 248–251. [Google Scholar] [CrossRef]
- Fletcher, J. What Is Heterogeneity and Is It Important? BMJ 2007, 334, 94–96. [Google Scholar] [CrossRef]
- Ibragimova, M.K.; Tsyganov, M.M.; Litviakov, N.V. Human Papillomavirus and Colorectal Cancer. Med. Oncol. Northwood Lond. Engl. 2018, 35, 140. [Google Scholar] [CrossRef]
- Akram, N.; Imran, M.; Noreen, M.; Ahmed, F.; Atif, M.; Fatima, Z.; Bilal Waqar, A. Oncogenic Role of Tumor Viruses in Humans. Viral Immunol. 2017, 30, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Sezgin, E.; An, P.; Winkler, C.A. Host Genetics of Cytomegalovirus Pathogenesis. Front. Genet. 2019, 10, 616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malki, M.I.; Gupta, I.; Fernandes, Q.; Aboulkassim, T.; Yasmeen, A.; Vranic, S.; Al Moustafa, A.-E.; Al-Thawadi, H.A. Co-Presence of Epstein-Barr Virus and High-Risk Human Papillomaviruses in Syrian Colorectal Cancer Samples. Hum. Vaccines Immunother. 2020, 16, 2403–2407. [Google Scholar] [CrossRef] [PubMed]
- Marongiu, L.; Allgayer, H. Viruses in Colorectal Cancer. Mol. Oncol. 2022, 16, 1423–1450. [Google Scholar] [CrossRef]
- Tsai, C.-L.; Li, H.-P.; Lu, Y.-J.; Hsueh, C.; Liang, Y.; Chen, C.-L.; Tsao, S.W.; Tse, K.-P.; Yu, J.-S.; Chang, Y.-S. Activation of DNA Methyltransferase 1 by EBV LMP1 Involves C-Jun NH(2)-Terminal Kinase Signaling. Cancer Res. 2006, 66, 11668–11676. [Google Scholar] [CrossRef] [Green Version]
- Jeon, Y.K.; Lee, B.Y.; Kim, J.E.; Lee, S.S.; Kim, C.W. Molecular Characterization of Epstein-Barr Virus and Oncoprotein Expression in Nasopharyngeal Carcinoma in Korea. Head Neck 2004, 26, 573–583. [Google Scholar] [CrossRef]
- Hsu, C.-Y.; Yi, Y.-H.; Chang, K.-P.; Chang, Y.-S.; Chen, S.-J.; Chen, H.-C. The Epstein-Barr Virus-Encoded MicroRNA MiR-BART9 Promotes Tumor Metastasis by Targeting E-Cadherin in Nasopharyngeal Carcinoma. PLoS Pathog. 2014, 10, e1003974. [Google Scholar] [CrossRef]
- Lin, Z.; Wan, X.; Jiang, R.; Deng, L.; Gao, Y.; Tang, J.; Yang, Y.; Zhao, W.; Yan, X.; Yao, K.; et al. Epstein-Barr Virus-Encoded Latent Membrane Protein 2A Promotes the Epithelial-Mesenchymal Transition in Nasopharyngeal Carcinoma via Metastatic Tumor Antigen 1 and Mechanistic Target of Rapamycin Signaling Induction. J. Virol. 2014, 88, 11872–11885. [Google Scholar] [CrossRef] [Green Version]
- Cyprian, F.S.; Al-Antary, N.; Al Moustafa, A.-E. HER-2/Epstein-Barr Virus Crosstalk in Human Gastric Carcinogenesis: A Novel Concept of Oncogene/Oncovirus Interaction. Cell Adhes. Migr. 2018, 12, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Gaur, N.; Gandhi, J.; Robertson, E.S.; Verma, S.C.; Kaul, R. Epstein-Barr Virus Latent Antigens EBNA3C and EBNA1 Modulate Epithelial to Mesenchymal Transition of Cancer Cells Associated with Tumor Metastasis. Tumour Biol. J. Int. Soc. Oncodevelopmen. Biol. Med. 2015, 36, 3051–3060. [Google Scholar] [CrossRef]
- Cyprian, F.S.; Al-Farsi, H.F.; Vranic, S.; Akhtar, S.; Al Moustafa, A.-E. Epstein-Barr Virus and Human Papillomaviruses Interactions and Their Roles in the Initiation of Epithelial-Mesenchymal Transition and Cancer Progression. Front. Oncol. 2018, 8, 111. [Google Scholar] [CrossRef]
- Teo, W.H.; Chen, H.-P.; Huang, J.C.; Chan, Y.-J. Human Cytomegalovirus Infection Enhances Cell Proliferation, Migration and Upregulation of EMT Markers in Colorectal Cancer-Derived Stem Cell-like Cells. Int. J. Oncol. 2017, 51, 1415–1426. [Google Scholar] [CrossRef] [Green Version]
- Ryan, J.L.; Shen, Y.J.; Morgan, D.R.; Thorne, L.B.; Kenney, S.C.; Dominguez, R.L.; Gulley, M.L. Epstein-Barr Virus Infection Is Common in Inflamed Gastrointestinal Mucosa. Dig. Sci. 2012, 57, 1887–1898. [Google Scholar] [CrossRef] [Green Version]
- Magro, F.; Santos-Antunes, J.; Albuquerque, A.; Vilas-Boas, F.; Macedo, G.N.; Nazareth, N.; Lopes, S.; Sobrinho-Simões, J.; Teixeira, S.; Dias, C.C.; et al. Epstein-Barr Virus in Inflammatory Bowel Disease-Correlation with Different Therapeutic Regimens. Inflamm. Bowel Dis. 2013, 19, 1710–1716. [Google Scholar] [CrossRef]
- Li, X.; Chen, N.; You, P.; Peng, T.; Chen, G.; Wang, J.; Li, J.; Liu, Y. The Status of Epstein-Barr Virus Infection in Intestinal Mucosa of Chinese Patients with Inflammatory Bowel Disease. Digestion 2019, 99, 126–132. [Google Scholar] [CrossRef]
- Núñez Ortiz, A.; Rojas Feria, M.; de la Cruz Ramírez, M.D.; Gómez Izquierdo, L.; Trigo Salado, C.; Herrera Justiniano, J.M.; Leo Carnerero, E. Impact of Epstein-Barr Virus Infection on Inflammatory Bowel Disease (IBD) Clinical Outcomes. Rev. Espanola Enfermedades Dig. Organo Of. Soc. Espanola Patol. Dig. 2022, 114, 259–265. [Google Scholar] [CrossRef]
- Ciccocioppo, R.; Racca, F.; Paolucci, S.; Campanini, G.; Pozzi, L.; Betti, E.; Riboni, R.; Vanoli, A.; Baldanti, F.; Corazza, G.R. Human Cytomegalovirus and Epstein-Barr Virus Infection in Inflammatory Bowel Disease: Need for Mucosal Viral Load Measurement. World J. Gastroenterol. 2015, 21, 1915–1926. [Google Scholar] [CrossRef]
- Lapsia, S.; Koganti, S.; Spadaro, S.; Rajapakse, R.; Chawla, A.; Bhaduri-McIntosh, S. Anti-TNFα Therapy for Inflammatory Bowel Diseases Is Associated with Epstein-Barr Virus Lytic Activation. J. Med. Virol. 2016, 88, 312–318. [Google Scholar] [CrossRef] [Green Version]
- Nissen, L.H.C.; Nagtegaal, I.D.; de Jong, D.J.; Kievit, W.; Derikx, L.A.A.P.; Groenen, P.J.T.A.; van Krieken, J.H.J.M.; Hoentjen, F. Epstein-Barr Virus in Inflammatory Bowel Disease: The Spectrum of Intestinal Lymphoproliferative Disorders. J. Crohns Colitis 2015, 9, 398–403. [Google Scholar] [CrossRef] [Green Version]
- Ambelil, M.; Saulino, D.M.; Ertan, A.; DuPont, A.W.; Younes, M. The Significance of So-Called Equivocal Immunohistochemical Staining for Cytomegalovirus in Colorectal Biopsies. Arch. Pathol. Lab. Med. 2019, 143, 985–989. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.C.; Itzkowitz, S.H. Colorectal Cancer in Inflammatory Bowel Disease: Mechanisms and Management. Gastroenterology 2022, 162, 715–730.e3. [Google Scholar] [CrossRef]
- Wu, S.; He, C.; Tang, T.-Y.; Li, Y.-Q. A Review on Co-Existent Epstein-Barr Virus-Induced Complications in Inflammatory Bowel Disease. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1085–1091. [Google Scholar] [CrossRef]
- Afzal, M.; Nigam, G.B. EBV Colitis with Ulcerative Colitis: A Double Whammy. BMJ Case Rep. 2018, 2018, bcr-2018-224963. [Google Scholar] [CrossRef]
- Losco, A.; Gianelli, U.; Cassani, B.; Baldini, L.; Conte, D.; Basilisco, G. Epstein-Barr Virus-Associated Lymphoma in Crohn’s Disease. Inflamm. Bowel Dis. 2004, 10, 425–429. [Google Scholar] [CrossRef] [Green Version]
- Sankaran-Walters, S.; Ransibrahmanakul, K.; Grishina, I.; Hung, J.; Martinez, E.; Prindiville, T.; Dandekar, S. Epstein-Barr Virus Replication Linked to B Cell Proliferation in Inflamed Areas of Colonic Mucosa of Patients with Inflammatory Bowel Disease. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2011, 50, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Subramaniam, K.; D’Rozario, J.; Pavli, P. Lymphoma and Other Lymphoproliferative Disorders in Inflammatory Bowel Disease: A Review. J. Gastroenterol. Hepatol. 2013, 28, 24–30. [Google Scholar] [CrossRef]
- Morisco, F.; Castiglione, F.; Rispo, A.; Stroffolini, T.; Sansone, S.; Vitale, R.; Guarino, M.; Biancone, L.; Caruso, A.; D’Inca, R.; et al. Effect of Immunosuppressive Therapy on Patients with Inflammatory Bowel Diseases and Hepatitis B or C Virus Infection. J. Viral Hepat. 2013, 20, 200–208. [Google Scholar] [CrossRef]
- Seeger, C.; Mason, W.S. Molecular Biology of Hepatitis B Virus Infection. Virology 2015, 479–480, 672–686. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.-Y.; Wang, S.-Y.; Deng, M.; Li, Y.-C.; Ling, Z.-X.; Shao, L.; Ruan, B. Immune Response to Hepatitis B Vaccination among People with Inflammatory Bowel Diseases: A Systematic Review and Meta-Analysis. Vaccine 2017, 35, 2633–2641. [Google Scholar] [CrossRef]
- Liu, S.; Koh, S.S.Y.; Lee, C.G.L. Hepatitis B Virus X Protein and Hepatocarcinogenesis. Int. J. Mol. Sci. 2016, 17, 940. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Li, S.; Tao, H.; Zhan, Y.; Ni, K.; Gong, J.; Li, G. Higher Titer Hepatitis B Core Antibody Predicts a Higher Risk of Liver Metastases and Worse Survival in Patients with Colorectal Cancer. World J. Surg. Oncol. 2021, 19, 251. [Google Scholar] [CrossRef] [PubMed]
- López-Serrano, P.; Pérez-Calle, J.L.; Sánchez-Tembleque, M.D. Hepatitis B and Inflammatory Bowel Disease: Role of Antiviral Prophylaxis. World J. Gastroenterol. 2013, 19, 1342–1348. [Google Scholar] [CrossRef]
- Boltin, D.; Vilkin, A.; Levi, Z.; Elkayam, O.; Niv, Y. JC Virus T-Antigen DNA in Gastrointestinal Mucosa of Immunosuppressed Patients: A Prospective, Controlled Study. Dig. Sci. 2010, 55, 1975–1981. [Google Scholar] [CrossRef]
- Bellaguarda, E.; Keyashian, K.; Pekow, J.; Rubin, D.T.; Cohen, R.D.; Sakuraba, A. Prevalence of Antibodies Against JC Virus in Patients with Refractory Crohn’s Disease and Effects of Natalizumab Therapy. Clin. Gastroenterol. Hepatol. Off. Clin. Pract. J. Am. Gastroenterol. Assoc. 2015, 13, 1919–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verbeeck, J.; van Assche, G.; Ryding, J.; Wollants, E.; Rans, K.; Vermeire, S.; Pourkarim, M.R.; Noman, M.; Dillner, J.; van Ranst, M.; et al. JC Viral Loads in Patients with Crohn’s Disease Treated with Immunosuppression: Can We Screen for Elevated Risk of Progressive Multifocal Leukoencephalopathy? Gut 2008, 57, 1393–1397. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, A.; Barucca, V.; Di Nardo, G.; Fioriti, F.; Iebba, V.; Schippa, S.; Conte, M.P.; Proietti Checchi, M.; Colosimo, M.T.; Cucchiara, S.; et al. JC Viral Reactivation in a Pediatric Patient with Crohn’s Disease. Int. J. Immunopathol. Pharmacol. 2010, 23, 955–959. [Google Scholar] [CrossRef] [PubMed]
- Altschuler, E.L. Is JC Polyoma Virus the Cause of Ulcerative Colitis and Multiple Sclerosis? Med. Hypotheses 2000, 55, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Razzaghi, H.; Saraiya, M.; Thompson, T.D.; Henley, S.J.; Viens, L.; Wilson, R. Five-Year Relative Survival for Human Papillomavirus-Associated Cancer Sites. Cancer 2018, 124, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Kirgan, D.; Manalo, P.; McGregor, B. Immunohistochemical Demonstration of Human Papilloma Virus Antigen in Human Colon Neoplasms. J. Surg. Res. 1990, 48, 397–402. [Google Scholar] [CrossRef]
- Damin, D.C.; Caetano, M.B.; Rosito, M.A.; Schwartsmann, G.; Damin, A.S.; Frazzon, A.P.; Ruppenthal, R.D.; Alexandre, C.O.P. Evidence for an Association of Human Papillomavirus Infection and Colorectal Cancer. Eur. J. Surg. Oncol. 2007, 33, 569–574. [Google Scholar] [CrossRef]
- Pelizzer, T.; Dias, C.P.; Poeta, J.; Torriani, T.; Roncada, C. Colorectal Cancer Prevalence Linked to Human Papillomavirus: A Systematic Review with Meta-Analysis. Rev. Bras. Epidemiol. Braz. J. Epidemiol. 2016, 19, 791–802. [Google Scholar] [CrossRef]
- Lorenzon, L.; Ferri, M.; Pilozzi, E.; Torrisi, M.R.; Ziparo, V.; French, D. Human Papillomavirus and Colorectal Cancer: Evidences and Pitfalls of Published Literature. Int. J. Colorectal Dis. 2011, 26, 135–142. [Google Scholar] [CrossRef]
- Roesch-Dietlen, F.; Cano-Contreras, A.D.; Sánchez-Maza, Y.J.; Espinosa-González, J.M.; Vázquez-Prieto, M.Á.; Valdés-de la, O.E.J.; Díaz-Roesch, F.; Carrasco-Arroniz, M.Á.; Cruz-Palacios, A.; Grube-Pagola, P.; et al. Frequency of human papillomavirus infection in patients with gastrointestinal cancer. Rev. Gastroenterol. Mex. Engl. 2018, 83, 253–258. [Google Scholar] [CrossRef]
- Zhang, X.-H.; Wang, W.; Wang, Y.-Q.; Jia, D.-F.; Zhu, L. Human Papillomavirus Infection and Colorectal Cancer in the Chinese Population: A Meta-Analysis. Colorectal Dis. Off. J. Assoc. Coloproctol. G. B. Irel. 2018, 20, 961–969. [Google Scholar] [CrossRef]
- Chao, G.; Hong, X.; Chen, X.; Zhang, S. The Prevalence of Human Papillomavirus in Colorectal Cancer and Adenoma: A Meta-Analysis. J. Cancer Res. Ther. 2020, 16, 1656–1663. [Google Scholar] [CrossRef]
- Dojcinov, S.D.; Venkataraman, G.; Raffeld, M.; Pittaluga, S.; Jaffe, E.S. EBV Positive Mucocutaneous Ulcer--a Study of 26 Cases Associated with Various Sources of Immunosuppression. Am. J. Surg. Pathol. 2010, 34, 405–417. [Google Scholar] [CrossRef]
- Moran, N.R.; Webster, B.; Lee, K.M.; Trotman, J.; Kwan, Y.-L.; Napoli, J.; Leong, R.W. Epstein Barr Virus-Positive Mucocutaneous Ulcer of the Colon Associated Hodgkin Lymphoma in Crohn’s Disease. World J. Gastroenterol. 2015, 21, 6072–6076. [Google Scholar] [CrossRef]
- Juan, A.; Lobatón, T.; Tapia, G.; Mañosa, M.; Cabré, E.; Domènech, E. Epstein-Barr Virus-Positive Mucocutaneous Ulcer in Crohn’s Disease. A Condition to Consider in Immunosuppressed IBD Patients. Dig. Liver Dis. Off. J. Ital. Soc. Gastroenterol. Ital. Assoc. Study Liver 2017, 49, 934–937. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Y.; Meng, X.; Duan, X.; Wang, M.; Chen, W.; Tang, T.; Li, Y. Epstein-Barr Virus-Associated T-Cell Lymphoproliferative Disorder Presenting as Chronic Diarrhea and Intestinal Bleeding: A Case Report. Front. Immunol. 2018, 9, 2583. [Google Scholar] [CrossRef]
- Liu, Y.; Li, Y.; Li, Y.; Wu, S.; Tian, X.; Tang, T.; Sun, H.; He, C. Clinical Features of Intestinal Ulcers Complicated by Epstein-Barr Virus Infection: Importance of Active Infection. Dis. Markers 2021, 2021, 6627620. [Google Scholar] [CrossRef]
- Wang, Z.; Zhang, W.; Luo, C.; Zhu, M.; Zhen, Y.; Mu, J.; Zhang, Y.; Hu, R.; Wang, Y.; Wen, Z.; et al. Primary Intestinal Epstein-Barr Virus-Associated Natural Killer/T-Cell Lymphoproliferative Disorder: A Disease Mimicking Inflammatory Bowel Disease. J. Crohns Colitis 2018, 12, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Xu, W.; Jiang, X.; Chen, J.; Mao, Q.; Zhao, X.; Sun, X.; Zhong, L.; Rong, L. Chronic Active Epstein-Barr Virus Infection Involving Gastrointestinal Tract Mimicking Inflammatory Bowel Disease. BMC Gastroenterol. 2020, 20, 257. [Google Scholar] [CrossRef] [PubMed]
- Ambinder, R.F. Gammaherpesviruses and “Hit-and-Run” Oncogenesis. Am. J. Pathol. 2000, 156, 1–3. [Google Scholar] [CrossRef]
- Skinner, G.R. Transformation of Primary Hamster Embryo Fibroblasts by Type 2 Simplex Virus: Evidence for a “Hit and Run” Mechanism. Br. J. Exp. Pathol. 1976, 57, 361–376. [Google Scholar] [PubMed]
- Gao, Y.; Lu, Y.-J.; Xue, S.-A.; Chen, H.; Wedderburn, N.; Griffin, B.E. Hypothesis: A Novel Route for Immortalization of Epithelial Cells by Epstein-Barr Virus. Oncogene 2002, 21, 825–835. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, P.G.; Simas, J.P.; Efstathiou, S. Immune Control of Mammalian Gamma-Herpesviruses: Lessons from Murid Herpesvirus-4. J. Gen. Virol. 2009, 90, 2317–2330. [Google Scholar] [CrossRef]
- Marongiu, L.; Landry, J.J.M.; Rausch, T.; Abba, M.L.; Delecluse, S.; Delecluse, H.-J.; Allgayer, H. Metagenomic Analysis of Primary Colorectal Carcinomas and Their Metastases Identifies Potential Microbial Risk Factors. Mol. Oncol. 2021, 15, 3363–3384. [Google Scholar] [CrossRef]
- Tatiya-Aphiradee, N.; Chatuphonprasert, W.; Jarukamjorn, K. Immune Response and Inflammatory Pathway of Ulcerative Colitis. J. Basic Clin. Physiol. Pharmacol. 2018, 30, 1–10. [Google Scholar] [CrossRef]
- Glauser, M.P.; Meylan, P.; Bille, J. The Inflammatory Response and Tissue Damage. The Example of Renal Scars Following Acute Renal Infection. Pediatr. Nephrol. Berl. Ger. 1987, 1, 615–622. [Google Scholar] [CrossRef]
- Mills, S.; Shanahan, F.; Stanton, C.; Hill, C.; Coffey, A.; Ross, R.P. Movers and Shakers: Influence of Bacteriophages in Shaping the Mammalian Gut Microbiota. Gut Microbes 2013, 4, 4–16. [Google Scholar] [CrossRef]
- Aarnio, M.T.; Bohm, J.P.; Nuorva, K.P.; Pitkanen, R.I.; Kuopio, T.H.; Voutilainen, M.E. Absence of Cytomegalovirus from the Gastrointestinal Tract of Patients with Active Crohn’s Disease. In Vivo 2012, 26, 151–155. [Google Scholar]
- Abdel-Moneim, A.S.; El-Fol, H.A.; Kamel, M.M.; Soliman, A.S.; Mahdi, E.A.; El-Gammal, A.S.; Mahran, T.Z. Screening of Human Bocavirus in Surgically Excised Cancer Specimens. Arch. Virol 2016, 161, 2095–2102. [Google Scholar] [CrossRef]
- Abdirad, A.; Ghaderi-Sohi, S.; Shuyama, K.; Koriyama, C.; Nadimi-Barforoosh, H.; Emami, S.; Mosavi-Jarrahi, A.; Nahvijou, A.; Akiba, S. Epstein-Barr Virus Associated Gastric Carcinoma: A Report from Iran in the Last Four Decades. Diagn. Pathol. 2007, 2, 25. [Google Scholar] [CrossRef] [Green Version]
- Adams, D.J.; Nylund, C.M. Hospitalization for Varicella and Zoster in Children with Inflammatory Bowel Disease. J. Pediatr 2016, 171, 140–145. [Google Scholar] [CrossRef]
- Afzal, M.A.; Armitage, E.; Ghosh, S.; Williams, L.C.; Minor, P.D. Further Evidence of the Absence of Measles Virus Genome Sequence in Full Thickness Intestinal Specimens from Patients with Crohn’s Disease. J. Med. Virol. 2000, 62, 377–382. [Google Scholar] [CrossRef]
- Afzal, M.A.; Armitage, E.; Begley, J.; Bentley, M.L.; Minor, P.D.; Ghosh, S.; Ferguson, A. Absence of Detectable Measles Virus Genome Sequence in Inflammatory Bowel Disease Tissues and Peripheral Blood Lymphocytes. J. Med. Virol. 1998, 55, 243–249. [Google Scholar] [CrossRef]
- Aghakhani, A.; Hamkar, R.; Ramezani, A.; Bidari-Zerehpoosh, F.; Sabeti, S.; Ghavami, N.; Banifazl, M.; Rashidi, N.; Eslamifar, A. Lack of Human Papillomavirus DNA in Colon Adenocarcinama and Adenoma. J. Cancer Res. Ther. 2014, 10, 531–534. [Google Scholar] [CrossRef]
- Ahmad, W.; Nguyen, N.H.; Boland, B.S.; Dulai, P.S.; Pride, D.T.; Bouland, D.; Sandborn, W.J.; Singh, S. Comparison of Multiplex Gastrointestinal Pathogen Panel and Conventional Stool Testing for Evaluation of Diarrhea in Patients with Inflammatory Bowel Diseases. Dig. Sci. 2019, 64, 382–390. [Google Scholar] [CrossRef] [Green Version]
- Akintola-Ogunremi, O.; Luo, Q.; He, T.C.; Wang, H.L. Is Cytomegalovirus Associated with Human Colorectal Tumorigenesis? Am. J. Clin. Pathol 2005, 123, 244–249. [Google Scholar] [CrossRef]
- Alacam, S.; Karabulut, N.; Bakir, A.; Onel, M.; Buyuk, M.; Gulluoglu, M.; Agacfidan, A. Diagnostic Significance of Cytomegalovirus DNA Quantitation in Gastrointestinal Biopsies: Comparison with Histopathological Data and Blood Cytomegalovirus DNA. Eur. J. Gastroenterol. Hepatol. 2021, 33, 40–45. [Google Scholar] [CrossRef]
- Alain, S.; Ducancelle, A.; Le Pors, M.J.S.; Mazeron, M.C.; de Saussure, P.; Bouhnik, Y.; Lavergne, A. Cytomegalovirus Infection in Patients with Active Inflammatory Bowel Disease. J. Clin. Virol. 2005, 33, 180–182. [Google Scholar] [CrossRef]
- Alipov, G.; Nakayama, T.; Nakashima, M.; Wen, C.Y.; Niino, D.; Kondo, H.; Pruglo, Y.; Sekine, I. Epstein-Barr Virus-Associated Gastric Carcinoma in Kazakhstan. World J. Gastroenterol. 2005, 11, 27–30. [Google Scholar] [CrossRef]
- Audeau, A.; Han, H.W.; Johnston, M.J.; Whitehead, M.W.; Frizelle, F.A. Does Human Papilloma Virus Have a Role in Squamous Cell Carcinoma of the Colon and Upper Rectum? Eur. J. Surg. Oncol. 2002, 28, 657–660. [Google Scholar] [CrossRef]
- Axelrad, J.E.; Joelson, A.; Green, P.H.R.; Lawlor, G.; Lichtiger, S.; Cadwell, K.; Lebwohl, B. Enteric Infections Are Common in Patients with Flares of Inflammatory Bowel Disease. Am. J. Gastroenterol. 2018, 113, 1530–1539. [Google Scholar] [CrossRef]
- Axelrad, J.E.; Olen, O.; Askling, J.; Lebwohl, B.; Khalili, H.; Sachs, M.C.; Ludvigsson, J.F. Gastrointestinal Infection Increases Odds of Inflammatory Bowel Disease in a Nationwide Case-Control Study. Clin. Gastroenterol. Hepatol. 2019, 17, 1311. [Google Scholar] [CrossRef]
- Balzola, F.A.; Khan, K.; Pera, A.; Bonino, F.; Pounder, R.E.; Wakefield, A.J. Measles IgM Immunoreactivity in Patients with Inflammatory Bowel Disease. Ital. J. Gastroenterol. Hepatol. 1998, 30, 378–382. [Google Scholar]
- Baran, M.; Aksoy, B.; Vardı, K.; Appak, Y.Ç.; Öncel, E.K.; Çiftdoğan, D.Y. The Frequency and Importance of Cytomegalovirus and Epstein-Barr Virus Infections in Children with Inflammatory Bowel Disease: Single Center Experience. J. Pediatr. Infect. Cocuk Enfeksiyon Derg. 2018, 12, e140–e146. [Google Scholar] [CrossRef]
- Bellaguarda, E.; Pekow, J.; Cohen, R.D.; Rubin, D.T.; Sakuraba, A. Prevalence of Serum JC Virus Antibody in Refractory Crohn’s Disease Patients. Gastroenterology 2014, 146, S580. [Google Scholar] [CrossRef]
- Bender, C.; Zipeto, D.; Bidoia, C.; Costantini, S.; Zamo, A.; Menestrina, F.; Bertazzoni, U. Analysis of Colorectal Cancers for Human Cytomegalovirus Presence. Infect. Agent Cancer 2009, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Bernabe-Dones, R.D.; Gonzalez-Pons, M.; Villar-Prados, A.; Lacourt-Ventura, M.; Rodriguez-Arroyo, H.; Fonseca-Williams, S.; Velazquez, F.E.; Diaz-Algorri, Y.; Lopez-Diaz, S.M.; Rodriguez, N.; et al. High Prevalence of Human Papillomavirus in Colorectal Cancer in Hispanics: A Case-Control Study. Gastroenterol Res. Pract. 2016, 2016, 7896716. [Google Scholar] [CrossRef] [Green Version]
- Bernstein, C.N.; Rawsthorne, P.; Blanchard, J.F. Population-Based Case-Control Study of Measles, Mumps, and Rubella and Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2007, 13, 759–762. [Google Scholar] [CrossRef] [PubMed]
- Bertalot, G.; Villanacci, V.; Gramegna, M.; Orvieto, E.; Negrini, R.; Saleri, A.; Terraroli, C.; Ravelli, P.; Cestari, R.; Viale, G. Evidence of Epstein-Barr Virus Infection in Ulcerative Colitis. Dig. Liver Dis. 2001, 33, 551–558. [Google Scholar] [CrossRef]
- Biancone, L.; DelleMonache, M.; Ricci, G.L.; Pallone, F. Hepatitis B and C Virus Infection in Crohn’s Disease. Gastroenterology 2001, 7, 287–294. [Google Scholar] [CrossRef]
- Bodaghi, S.; Yamanegi, K.; Xiao, S.Y.; Da Costa, M.; Palefsky, J.M.; Zheng, Z.M. Colorectal Papillomavirus Infection in Patients with Colorectal Cancer. Clin. Cancer Res. 2005, 11, 2862–2867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brichacek, B.; Hirsch, I.; Zavadova, H.; Prochazka, M.; Faltyn, J.; Vonka, V. Absence of Cytomegalovirus DNA from Adenocarcinoma of the Colon. Intervirology 1980, 14, 223–227. [Google Scholar] [CrossRef]
- Burnett-Hartman, A.N.; Newcomb, P.A.; Mandelson, M.T.; Galloway, D.A.; Madeleine, M.M.; Wurscher, M.A.; Carter, J.J.; Makar, K.W.; Potter, J.D.; Schwartz, S.M. No Evidence for Human Papillomavirus in the Etiology of Colorectal Polyps. Cancer Epidemiol Biomark. Prev. 2011, 20, 2288–2297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burnett-Hartman, A.N.; Newcomb, P.A.; Schwartz, S.M.; Bostick, R.M.; Pawlita, M.; Waterboer, T.; Potter, J.D. No Association between Antibodies to Sexually Transmitted Infections and Colorectal Hyperplastic Polyps in Men: Minnesota Cancer Prevention Research Unit Polyp Study. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1599–1601. [Google Scholar] [CrossRef] [Green Version]
- Burnett-Hartman, A.N.; Feng, Q.; Popov, V.; Kalidindi, A.; Newcomb, P.A. Human Papillomavirus DNA Is Rarely Detected in Colorectal Carcinomas and Not Associated with Microsatellite Instability: The Seattle Colon Cancer Family Registry. Cancer Epidemiol. Biomark. Prev. 2013, 22, 317–319. [Google Scholar] [CrossRef] [Green Version]
- Butt, J.; Romero-Hernandez, B.; Perez-Gomez, B.; Willhauck-Fleckenstein, M.; Holzinger, D.; Martin, V.; Moreno, V.; Linares, C.; Dierssen-Sotos, T.; Barricarte, A.; et al. Association of Streptococcus Gallolyticus Subspecies Gallolyticus with Colorectal Cancer: Serological Evidence. Int. J. Cancer 2016, 138, 1670–1679. [Google Scholar] [CrossRef] [Green Version]
- Campello, C.; Comar, M.; Zanotta, N.; Minicozzi, A.; Rodella, L.; Poli, A. Detection of SV40 in Colon Cancer: A Molecular Case-Control Study from Northeast Italy. J. Med. Virol. 2010, 82, 1197–1200. [Google Scholar] [CrossRef] [Green Version]
- Campello, C.; Comar, M.; D’Agaro, P.; Minicozzi, A.; Rodella, L.; Poli, A. A Molecular Case-Control Study of the Merkel Cell Polyomavirus in Colon Cancer. J. Med. Virol. 2011, 83, 721–724. [Google Scholar] [CrossRef] [Green Version]
- Cardenas-Mondragon, M.G.; Torres, J.; Flores-Luna, L.; Camorlinga-Ponce, M.; Carreon-Talavera, R.; Gomez-Delgado, A.; Kasamatsu, E.; Fuentes-Panana, E.M. Case-Control Study of Epstein-Barr Virus and Helicobacter pylori Serology in Latin American Patients with Gastric Disease. Br. J. Cancer 2015, 112, 1866–1873. [Google Scholar] [CrossRef] [Green Version]
- Carrascal, E.; Koriyama, C.; Akiba, S.; Tamayo, O.; Itoh, T.; Eizuru, Y.; Garcia, F.; Sera, M.; Carrasquilla, G.; Piazuelo, M.B.; et al. Epstein-Barr Virus-Associated Gastric Carcinoma in Cali, Colombia. Oncol Rep. 2003, 10, 1059–1062. [Google Scholar] [CrossRef]
- Casini, B.; Borgese, L.; Del Nonno, F.; Galati, G.; Izzo, L.; Caputo, M.; Donnorso, R.P.; Castelli, M.; Risuleo, G.; Visca, P. Presence and Incidence of DNA Sequences of Human Polyomaviruses BKV and JCV in Colorectal Tumor Tissues. Anticancer Res. 2005, 25, 1079–1085. [Google Scholar]
- Chan, H.C.; Wong, V.W.; Wong, G.L.; Tang, W.; Wu, J.C.; Ng, S.C. Prevalence of Hepatitis B and Clinical Outcomes in Inflammatory Bowel Disease Patients in a Viral-Endemic Region. BMC Gastroenterol. 2016, 16, 100. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.P.; Jiang, J.K.; Chen, C.Y.; Yang, C.Y.; Chen, Y.C.; Lin, C.H.; Chou, T.Y.; Cho, W.L.; Chan, Y.J. Identification of Human Cytomegalovirus in Tumour Tissues of Colorectal Cancer and Its Association with the Outcome of Non-Elderly Patients. J. Gen. Virol. 2016, 97, 2411–2420. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.P.; Jiang, J.K.; Lai, P.Y.; Teo, W.H.; Yang, C.Y.; Chou, T.Y.; Lin, C.H.; Chan, Y.J. Serological and Viraemic Status of Human Cytomegalovirus Infection in Patients with Colorectal Cancer Is Not Correlated with Viral Replication and Transcription in Tumours. J. Gen. Virol. 2016, 97, 152–159. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Luo, S.; Ben, Q.; Lu, L.; Wan, X.; Wu, J. Prevalence of Hepatitis B and C and Factors for Infection and Nonimmune in Inflammatory Bowel Disease Patients in China. Eur. J. Gastroenterol. Hepatol. 2017, 29, 509–515. [Google Scholar] [CrossRef]
- Chevaux, J.B.; Nani, A.; Oussalah, A.; Venard, V.; Bensenane, M.; Belle, A.; Gueant, J.L.; Bigard, M.A.; Bronowicki, J.P.; Peyrin-Biroulet, L. Prevalence of Hepatitis B and C and Risk Factors for Nonvaccination in Inflammatory Bowel Disease Patients in Northeast France. Inflamm. Bowel Dis. 2010, 16, 916–924. [Google Scholar] [CrossRef] [Green Version]
- Cho, Y.J.; Chang, M.S.; Park, S.H.; Kim, H.S.; Kim, W.H. In Situ Hybridization of Epstein-Barr Virus in Tumor Cells and Tumor-Infiltrating Lymphocytes of the Gastrointestinal Tract. Hum. Pathol. 2001, 32, 297–301. [Google Scholar] [CrossRef]
- Coelho, T.R.; Gaspar, R.; Figueiredo, P.; Mendonca, C.; Lazo, P.A.; Almeida, L. Human JC Polyomavirus in Normal Colorectal Mucosa, Hyperplastic Polyps, Sporadic Adenomas, and Adenocarcinomas in Portugal. J. Med. Virol. 2013, 85, 2119–2127. [Google Scholar] [CrossRef]
- Cohen, S.; Martinez-Vinson, C.; Aloi, M.; Turner, D.; Assa, A.; de Ridder, L.; Wolters, V.M.; de Meij, T.; Alvisi, P.; Bronsky, J.; et al. Cytomegalovirus Infection in Pediatric Severe Ulcerative Colitis-A Multicenter Study from the Pediatric Inflammatory Bowel Disease Porto Group of the European Society of Pediatric Gastroenterology, Hepatology and Nutrition. Pediatr. Infect. J. 2018, 37, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Dalla Libera, L.S.; de Siqueira, T.; Santos, I.L.; Porto Ramos, J.E.; Milhomen, A.X.; Alencar, R. de C.G. de; Rabelo Santos, S.H.; Dos Santos Carneiro, M.A.; Figueiredo Alves, R.R.; Saddi, V.A. Detection of Human Papillomavirus and the Role of P16INK4a in Colorectal Carcinomas. PLoS ONE 2020, 15, e0235065. [Google Scholar] [CrossRef] [PubMed]
- De Francisco, R.; Castaño-García, A.; Martínez-González, S.; Pérez-Martínez, I.; González-Huerta, A.J.; Morais, L.R.; Fernández-García, M.S.; Jiménez, S.; Díaz-Coto, S.; Flórez-Díez, P.; et al. Impact of Epstein-Barr Virus Serological Status on Clinical Outcomes in Adult Patients with Inflammatory Bowel Disease. Aliment. Pharmacol. Ther. 2018, 48, 723–730. [Google Scholar] [CrossRef] [PubMed]
- De Lima, M.A.; Ferreira, M.V.; Barros, M.A.; Pardini, M.I.; Ferrasi, A.C.; Rabenhorst, S.H. Epstein-Barr Virus-Associated Gastric Carcinoma in Brazil: Comparison between in Situ Hybridization and Polymerase Chain Reaction Detection. Braz. J. Microbiol. 2012, 43, 393–404. [Google Scholar] [CrossRef]
- De Saussure, P.; Lavergne-Slove, A.; Mazeron, M.C.; Alain, S.; Matuchansky, C.; Bouhnik, Y. A Prospective Assessment of Cytomegalovirus Infection in Active Inflammatory Bowel Disease. Aliment Pharmacol. Ther. 2004, 20, 1323–1327. [Google Scholar] [CrossRef]
- De Souza, C.R.T.; Almeida, M.C.A.; Khayat, A.S.; da Silva, E.L.; Soares, P.C.; Chaves, L.C.; Burbano, R.M.R. Association between Helicobacter pylori, Epstein-Barr Virus, Human Papillomavirus and Gastric Adenocarcinomas. World J. Gastroenterol. 2018, 24, 4928–4938. [Google Scholar] [CrossRef]
- De Villiers, E.M.; Schmidt, R.; Delius, H.; zur Hausen, H. Heterogeneity of TT Virus Related Sequences Isolated from Human Tumour Biopsy Specimens. J. Mol. Med. Berl. 2002, 80, 44–50. [Google Scholar] [CrossRef]
- De Villiers, E.M. TTV Infection in Colorectal Cancer Tissues and Normal Mucosa 1. Int. J. Cancer 2007, 121, 2109–2112. [Google Scholar] [CrossRef]
- Del Moral-Hernández, O.; Castañón-Sánchez, C.A.; Reyes-Navarrete, S.; Martínez-Carrillo, D.N.; Betancourt-Linares, R.; Jiménez-Wences, H.; de la Peña, S.; Román-Román, A.; Hernández-Sotelo, D.; Fernández-Tilapa, G. Multiple Infections by EBV, HCMV and Helicobacter pylori Are Highly Frequent in Patients with Chronic Gastritis and Gastric Cancer from Southwest Mexico: An Observational Study. Med. Baltim. 2019, 98, e14124. [Google Scholar] [CrossRef]
- Deschoolmeester, V.; Van Marck, V.; Baay, M.; Weyn, C.; Vermeulen, P.; Van Marck, E.; Lardon, F.; Fontaine, V.; Vermorken, J.B. Detection of HPV and the Role of P16INK4A Overexpression as a Surrogate Marker for the Presence of Functional HPV Oncoprotein E7 in Colorectal Cancer. BMC Cancer 2010, 10, 117. [Google Scholar] [CrossRef]
- Dimitroulia, E.; Spanakis, N.; Konstantinidou, A.E.; Legakis, N.J.; Tsakris, A. Frequent Detection of Cytomegalovirus in the Intestine of Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2006, 12, 879–884. [Google Scholar] [CrossRef]
- Dimitroulia, E.; Pitiriga, V.C.; Piperaki, E.T.; Spanakis, N.E.; Tsakris, A. Inflammatory Bowel Disease Exacerbation Associated with Epstein-Barr Virus Infection. Colon Rectum. 2013, 56, 322–327. [Google Scholar] [CrossRef]
- Dimberg, J.; Hong, T.T.; Skarstedt, M.; Lofgren, S.; Zar, N.; Matussek, A. Detection of Cytomegalovirus DNA in Colorectal Tissue from Swedish and Vietnamese Patients with Colorectal Cancer. Anticancer Res. 2013, 33, 4947–4950. [Google Scholar]
- Do Carmo, A.M.; Santos, F.M.; Ortiz-Agostinho, C.L.; Nishitokukado, I.; Frota, C.S.; Gomes, F.U.; Leite, A.Z.; Pannuti, C.S.; Boas, L.S.; Teixeira, M.G.; et al. Cytomegalovirus Infection in Inflammatory Bowel Disease Is Not Associated with Worsening of Intestinal Inflammatory Activity. PLoS ONE 2014, 9, e111574. [Google Scholar] [CrossRef]
- El-Matary, W.; Stefanovici, C.; Van Caeseele, P.; Deora, V.; McCurdy, J. Detection of Cytomegalovirus in Colonic Mucosa of Children with Inflammatory Bowel Disease: Inflammatory Bowel Disease. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 221–224. [Google Scholar] [CrossRef]
- Enam, S.; Del Valle, L.; Lara, C.; Gan, D.D.; Ortiz-Hidalgo, C.; Palazzo, J.P.; Khalili, K. Association of Human Polyomavirus JCV with Colon Cancer: Evidence for Interaction of Viral T-Antigen and Beta-Catenin. Cancer Res. 2002, 62, 7093–7101. [Google Scholar]
- Esmailzadeh, N.; Ranaee, M.; Alizadeh, A.; Khademian, A.; Saber Amoli, S.; Sadeghi, F. Presence of JC Polyomavirus in Nonneoplastic Inflamed Colon Mucosa and Primary and Metastatic Colorectal Cancer. Gastrointest. Tumors 2020, 7, 30–40. [Google Scholar] [CrossRef]
- Eyre-Brook, I.A.; Dundas, S. Incidence and Clinical Significance of Colonic Cytomegalovirus Infection in Idiopathic Inflammatory Bowel Disease Requiring Colectomy. Gut 1986, 27, 1419–1425. [Google Scholar] [CrossRef] [Green Version]
- Fahal, A.H.; el Razig, S.A.; Suliman, S.H.; Ibrahim, S.Z.; Tigani, A.E. Gastrointestinal Tract Cancer in Association with Hepatitis and HIV Infection. East. Afr. Med. J. 1995, 72, 424–426. [Google Scholar]
- Farmer, G.W.; Vincent, M.M.; Fuccillo, D.A.; Horta-Barbosa, L.; Ritman, S.; Sever, J.L.; Gitnick, G.L. Viral Investigations in Ulcerative Colitis and Regional Enteritis. Gastroenterology 1973, 65, 8–18. [Google Scholar] [CrossRef]
- Fiorina, L.; Ricotti, M.; Vanoli, A.; Luinetti, O.; Dallera, E.; Riboni, R.; Paolucci, S.; Brugnatelli, S.; Paulli, M.; Pedrazzoli, P.; et al. Systematic Analysis of Human Oncogenic Viruses in Colon Cancer Revealed EBV Latency in Lymphoid Infiltrates. Infect. Agent Cancer 2014, 9, 18. [Google Scholar] [CrossRef] [Green Version]
- Flores, V.; Rodriguez-sanchez, B.; Marin-Jimenez, I.; Bouza, E.; Menchen, L.; Munoz, P. Prospective Study of Bk Virus Infection in Inflammatory Bowel Disease Patients. Gastroenterology 2014, 136, A190. [Google Scholar] [CrossRef] [Green Version]
- Gauss, A.; Rosenstiel, S.; Schnitzler, P.; Hinz, U.; Rehlen, T.; Kadmon, M.; Ehehalt, R.; Stremmel, W.; Zawierucha, A. Intestinal Cytomegalovirus Infection in Patients Hospitalized for Exacerbation of Inflammatory Bowel Disease: A 10-Year Tertiary Referral Center Experience. Eur. J. Gastroenterol. Hepatol. 2015, 27, 712–720. [Google Scholar] [CrossRef]
- Gazzaz, F.; Mosli, M.H.; Jawa, H.; Sibiany, A. Detection of Human Papillomavirus Infection by Molecular Tests and Its Relation to Colonic Polyps and Colorectal Cancer. Saudi Med. J. 2016, 37, 256–261. [Google Scholar] [CrossRef]
- Genitsch, V.; Novotny, A.; Seiler, C.A.; Kroll, D.; Walch, A.; Langer, R. Epstein-Barr Virus in Gastro-Esophageal Adenocarcinomas—Single Center Experiences in the Context of Current Literature. Front. Oncol. 2015, 5, 73. [Google Scholar] [CrossRef] [Green Version]
- Giuliani, L.; Ronci, C.; Bonifacio, D.; Di Bonito, L.; Favalli, C.; Perno, C.F.; Syrjänen, K.; Ciotti, M. Detection of Oncogenic DNA Viruses in Colorectal Cancer. Anticancer Res. 2008, 28, 1405–1410. [Google Scholar]
- Goel, A.; Li, M.S.; Nagasaka, T.; Shin, S.K.; Fuerst, F.; Ricciardiello, L.; Wasserman, L.; Boland, C.R. Association of JC Virus T-Antigen Expression with the Methylator Phenotype in Sporadic Colorectal Cancers. Gastroenterology 2006, 130, 1950–1961. [Google Scholar] [CrossRef]
- Gong, S.S.; Fan, Y.H.; Han, Q.Q.; Lv, B.; Xu, Y. Nested Case-Control Study on Risk Factors for Opportunistic Infections in Patients with Inflammatory Bowel Disease. World J. Gastroenterol. 2019, 25, 2240–2250. [Google Scholar] [CrossRef]
- Gonzalez, H.C.; Lamerato, L.; Rogers, C.G.; Gordon, S.C. Chronic Hepatitis C Infection as a Risk Factor for Renal Cell Carcinoma. Dig. Sci. 2015, 60, 1820–1824. [Google Scholar] [CrossRef]
- Gordon, J.; Ramaswami, A.; Beuttler, M.; Jossen, J.; Pittman, N.; Lai, J.; Dunkin, D.; Benkov, K.; Dubinsky, M. EBV Status and Thiopurine Use in Pediatric IBD. J. Pediatr. Gastroenterol. Nutr. 2016, 62, 711–714. [Google Scholar] [CrossRef] [PubMed]
- Gornick, M.C.; Castellsague, X.; Sanchez, G.; Giordano, T.J.; Vinco, M.; Greenson, J.K.; Capella, G.; Raskin, L.; Rennert, G.; Gruber, S.B.; et al. Human Papillomavirus Is Not Associated with Colorectal Cancer in a Large International Study. Cancer Causes Control 2010, 21, 737–743. [Google Scholar] [CrossRef] [PubMed]
- Green, M.; Orth, G.; Wold, W.S.; Sanders, P.R.; Mackey, J.K.; Favre, M.; Croissant, O. Analysis of Human Cancers, Normal Tissues, and Verruce Plantares for DNA Sequences of Human Papillomavirus Types 1 and 2. Virology 1981, 110, 176–184. [Google Scholar] [CrossRef]
- Greenberg, H.B.; Gebhard, R.L.; McClain, C.J.; Soltis, R.D.; Kapikian, A.Z. Antibodies to Viral Gastroenteritis Viruses in Crohn’s Disease. Gastroenterology 1979, 76, 349–350. [Google Scholar] [CrossRef]
- Grinstein, S.; Preciado, M.V.; Gattuso, P.; Chabay, P.A.; Warren, W.H.; De Matteo, E.; Gould, V.E. Demonstration of Epstein-Barr Virus in Carcinomas of Various Sites. Cancer Res. 2002, 62, 4876–4878. [Google Scholar]
- Gupta, I.; Al Farsi, H.; Jabeen, A.; Skenderi, F.; Al-Thawadi, H.; AlAhmad, Y.M.; Al Moustafa, A.-E.; Vranic, S. High-Risk Human Papillomaviruses and Epstein-Barr Virus in Colorectal Cancer and Their Association with Clinicopathological Status. Pathogens 2020, 9, 452. [Google Scholar] [CrossRef]
- Haga, Y.; Funakoshi, O.; Kuroe, K.; Kanazawa, K.; Nakajima, H.; Saito, H.; Murata, Y.; Munakata, A.; Yoshida, Y. Absence of Measles Viral Genomic Sequence in Intestinal Tissues from Crohn’s Disease by Nested Polymerase Chain Reaction. Gut 1996, 38, 211–215. [Google Scholar] [CrossRef]
- Haghi-Navand, A.; Teimoori, A.; Makvandi, M.; Nisi, N.; Pourjabari, K. Study on JV Virus in Patients with Colon Cancer Type Adenocarcinoma. Asian Pac. J. Cancer Prev. 2019, 20, 1147–1151. [Google Scholar] [CrossRef] [Green Version]
- Hamada, Y.; Nagata, N.; Nishijima, T.; Shimbo, T.; Asayama, N.; Kishida, Y.; Sekine, K.; Tanaka, S.; Aoki, T.; Watanabe, K.; et al. Impact of HIV Infection on Colorectal Tumors: A Prospective Colonoscopic Study of Asian Patients. J. Acquir. Immune Defic. Syndr. 2014, 65, 312–317. [Google Scholar] [CrossRef]
- Hampras, S.S.; Viscidi, R.P.; Helzlsouer, K.J.; Lee, J.H.; Fulp, W.J.; Giuliano, A.R.; Platz, E.A.; Rollison, D.E. Prospective Study of Seroreactivity to JC Virus T-Antigen and Risk of Colorectal Cancers and Adenomas. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2591–2596. [Google Scholar] [CrossRef] [Green Version]
- Harkins, L.; Volk, A.L.; Samanta, M.; Mikolaenko, I.; Britt, W.J.; Bland, K.I.; Cobbs, C.S. Specific Localisation of Human Cytomegalovirus Nucleic Acids and Proteins in Human Colorectal Cancer. Lancet 2002, 360, 1557–1563. [Google Scholar] [CrossRef]
- Harsh, P.; Gupta, V.; Kedia, S.; Bopanna, S.; Pilli, S.; Surendernath; Makharia, G.K.; Ahuja, V. Prevalence of Hepatitis B, Hepatitis C and Human Immunodeficiency Viral Infections in Patients with Inflammatory Bowel Disease in North India. Intest. Res. 2017, 15, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Hart, H.; Neill, W.A.; Norval, M. Lack of Association of Cytomegalovirus with Adenocarcinoma of the Colon. Gut 1982, 23, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, K.; Teramoto, N.; Akagi, T.; Sasaki, Y.; Suzuki, T. In Situ Detection of Epstein-Barr Virus in the Gastric Glands with Intestinal Metaplasia. Am. J. Gastroenterol. 1996, 91, 1481. [Google Scholar]
- He, Y.; Xu, P.; Chen, Y.; Yang, R.; Chen, B.; Zeng, Z.; Chen, M. Prevalence and Influences of Hepatitis B Virus Infection on Inflammatory Bowel Disease: A Retrospective Study in Southern China. Int. J. Clin. Exp. Med. 2015, 8, 8078–8085. [Google Scholar]
- Hernandez-Losa, J.; Fernandez-Soria, V.; Parada, C.; Sanchez-Prieto, R.; Ramon y Cajal, S. JC Virus and Human Colon Carcinoma: An Intriguing and Inconclusive Association. Gastroenterology 2003, 124, 268–270. [Google Scholar] [CrossRef]
- Herrera-Goepfert, R.; Akiba, S.; Koriyama, C.; Ding, S.; Reyes, E.; Itoh, T.; Minakami, Y.; Eizuru, Y. Epstein-Barr Virus-Associated Gastric Carcinoma: Evidence of Age-Dependence among a Mexican Population. World J. Gastroenterol. 2005, 11, 6096–6103. [Google Scholar] [CrossRef]
- Hirata, T.; Nakamoto, M.; Nakamura, M.; Kinjo, N.; Hokama, A.; Kinjo, F.; Fujita, J. Low Prevalence of Human T Cell Lymphotropic Virus Type 1 Infection in Patients with Gastric Cancer. J. Gastroenterol. Hepatol. 2007, 22, 2238–2241. [Google Scholar] [CrossRef]
- Hori, R.; Murai, Y.; Tsuneyama, K.; Abdel-Aziz, H.O.; Nomoto, K.; Takahashi, H.; Cheng, C.M.; Kuchina, T.; Harman, B.V.; Takano, Y. Detection of JC Virus DNA Sequences in Colorectal Cancers in Japan. Virchows Arch. 2005, 447, 723–730. [Google Scholar] [CrossRef]
- Hradsky, O.; Copova, I.; Zarubova, K.; Durilova, M.; Nevoral, J.; Maminak, M.; Hubacek, P.; Bronsky, J. Seroprevalence of Epstein-Barr Virus, Cytomegalovirus, and Polyomaviruses in Children with Inflammatory Bowel Disease. Dig. Sci. 2015, 60, 3399–3407. [Google Scholar] [CrossRef]
- Hsieh, L.L.; Lin, P.J.; Chen, T.C.; Ou, J.T. Frequency of Epstein-Barr Virus-Associated Gastric Adenocarcinoma in Taiwan. Cancer Lett. 1998, 129, 125–129. [Google Scholar] [CrossRef]
- Huang, E.S.; Roche, J.K. Cytomegalovirus D.N.A. and Adenocarcinoma of the Colon: Evidence for Latent Viral Infection. Lancet 1978, 1, 957–960. [Google Scholar] [CrossRef]
- Iizuka, M.; Saito, H.; Yukawa, M.; Itou, H.; Shirasaka, T.; Chiba, M.; Fukushima, T.; Watanabe, S. No Evidence of Persistent Mumps Virus Infection in Inflammatory Bowel Disease. Gut 2001, 48, 637–641. [Google Scholar] [CrossRef] [Green Version]
- Ito, M.; Rodriguez-Bigas, M.A.; Creaven, P.J.; Petrelli, N.J. High Prevalence of Inoue-Melnick Virus Antibodies in Patients with Colorectal Carcinoma. Cancer Lett. 1992, 65, 233–237. [Google Scholar] [CrossRef]
- Jarzynski, A.; Zajac, P.; Zebrowski, R.; Boguszewska, A.; Polz-Dacewicz, M. Occurrence of BK Virus and Human Papilloma Virus in Colorectal Cancer. Ann. Agric. Env. Med. 2017, 24, 440–445. [Google Scholar] [CrossRef] [Green Version]
- Jung, W.T.; Li, M.S.; Goel, A.; Boland, C.R. JC Virus T-Antigen Expression in Sporadic Adenomatous Polyps of the Colon. Cancer 2008, 112, 1028–1036. [Google Scholar] [CrossRef] [Green Version]
- Jung, Y.S.; Kim, N.H.; Park, J.H.; Park, D.I.; Sohn, C.I. Correlation between Hepatitis B Virus Infection and Colorectal Neoplasia. J. Clin. Med. 2019, 8, 2085. [Google Scholar] [CrossRef] [Green Version]
- Kambham, N.; Vij, R.; Cartwright, C.A.; Longacre, T. Cytomegalovirus Infection in Steroid-Refractory Ulcerative Colitis: A Case-Control Study. Am. J. Surg. Pathol. 2004, 28, 365–373. [Google Scholar] [CrossRef]
- Kamiza, A.B.; Su, F.H.; Wang, W.C.; Sung, F.C.; Chang, S.N.; Yeh, C.C. Chronic Hepatitis Infection Is Associated with Extrahepatic Cancer Development: A Nationwide Population-Based Study in Taiwan. BMC Cancer 2016, 16, 861. [Google Scholar] [CrossRef] [Green Version]
- Kane, S.P.; Nye, F.J.E.B. Virus Antibody in Crohn’s Disease. Lancet 1971, 1, 233. [Google Scholar] [CrossRef]
- Karbalaie Niya, M.; Tameshkel, F.; Alemrajabi, M.; Taherizadeh, M.; Keshavarz, M.; Rezaee, M.; Kevyani, H. Molecular Survey on Merkel Cell Polyomavlrus in Patients with Colorectal Cancer. Med. J. Indones. 2018, 27, 229–236. [Google Scholar] [CrossRef]
- Karim, N.; Pallesen, G. Epstein-Barr Virus (EBV) and Gastric Carcinoma in Malaysian Patients. Malays J. Pathol. 2003, 25, 45–47. [Google Scholar] [PubMed]
- Karpinski, P.; Myszka, A.; Ramsey, D.; Kielan, W.; Sasiadek, M.M. Detection of Viral DNA Sequences in Sporadic Colorectal Cancers in Relation to CpG Island Methylation and Methylator Phenotype. Tumour Biol. 2011, 32, 653–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kattoor, J.; Koriyama, C.; Akiba, S.; Itoh, T.; Ding, S.; Eizuru, Y.; Abraham, E.K.; Chandralekha, B.; Amma, N.S.; Nair, M.K. Epstein-Barr Virus-Associated Gastric Carcinoma in Southern India: A Comparison with a Large-Scale Japanese Series. J. Med. Virol. 2002, 68, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, H.; Mori, T.; Kashiwagi, Y.; Takekuma, K.; Hoshika, A.; Wakefield, A. Detection and Sequencing of Measles Virus from Peripheral Mononuclear Cells from Patients with Inflammatory Bowel Disease and Autism. Dig. Sci. 2000, 45, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Kayamba, V.; Monze, M.; Asombang, A.W.; Zyambo, K.; Kelly, P. Serological Response to Epstein-Barr Virus Early Antigen Is Associated with Gastric Cancer and Human Immunodeficiency Virus Infection in Zambian Adults: A Case-Control Study. Pan. Afr. Med. J. 2016, 23, 45. [Google Scholar] [CrossRef]
- Keller, S.C.; Momplaisir, F.; Lo Re, V.; Newcomb, C.; Liu, Q.; Ratcliffe, S.J.; Long, J.A. Colorectal Cancer Incidence and Screening in US Medicaid Patients with and without HIV Infection. Aids Care-Psychol. Socio-Med. Asp. AidsHiv 2014, 26, 716–722. [Google Scholar] [CrossRef]
- Khabaz, M.N.; Nedjadi, T.; Gari, M.A.; Atta, H.M.; Basuni, A.A.; Elderzi, D.A.; Bakarman, M. Simian Virus 40 Is Not Involved in the Development of Colorectal Adenocarcinoma. Future Virol. 2016, 11, 175–180. [Google Scholar] [CrossRef]
- Kiewe, P.; Wojtke, S.; Thiel, E.; Nagorsen, D. Antiviral Cellular Immunity in Colorectal Cancer Patients. Hum. Immunol. 2009, 70, 85–88. [Google Scholar] [CrossRef]
- Kim, J.J.; Simpson, N.; Klipfel, N.; Debose, R.; Barr, N.; Laine, L. Cytomegalovirus Infection in Patients with Active Inflammatory Bowel Disease. Dig. Sci. 2010, 55, 1059–1065. [Google Scholar] [CrossRef]
- Kim, E.S.; Cho, K.B.; Park, K.S.; Jang, B.I.; Kim, K.O.; Jeon, S.W.; Kim, E.Y.; Yang, C.H.; Kim, W.J. Prevalence of Hepatitis-B Viral Markers in Patients with Inflammatory Bowel Disease in a Hepatitis-B-Endemic Area: Inadequate Protective Antibody Levels in Young Patients. J. Clin. Gastroenterol. 2014, 48, 553–558. [Google Scholar] [CrossRef]
- Kishore, J.; Ghoshal, U.; Ghoshal, U.C.; Krishnani, N.; Kumar, S.; Singh, M.; Ayyagari, A. Infection with Cytomegalovirus in Patients with Inflammatory Bowel Disease: Prevalence, Clinical Significance and Outcome. J. Med. Microbiol. 2004, 53, 1155–1160. [Google Scholar] [CrossRef]
- Knoell, K.A.; Hendrix, J.D.; Stoler, M.H.; Patterson, J.W.; Montes, C.M. Absence of Human Herpesvirus 8 in Sarcoidosis and Crohn Disease Granulomas. Arch. Dermatol. 2005, 141, 909–910. [Google Scholar] [CrossRef]
- Knosel, T.; Schewe, C.; Dietel, M.; Petersen, I. Cytomegalovirus Is Not Associated with Progression and Metastasis of Colorectal Cancer. Cancer Lett. 2004, 211, 243–247. [Google Scholar] [CrossRef]
- Knosel, T.; Schewe, C.; Petersen, N.; Dietel, M.; Petersen, I. Prevalence of Infectious Pathogens in Crohn’s Disease. Pathol. Res. Pr. 2009, 205, 223–230. [Google Scholar] [CrossRef]
- Kocoglu, H.; Karaca, M.; Tural, D.; Hocaoglu, E.; Okuturlar, Y.; Fetullahoglu, Z.; Gunaldi, M.; Ciftci, R.; Tuna, S.; Yucil, O.K.; et al. Hepatitis B and C Rates Are Significantly Increased in Certain Solid Tumors: A Large Retrospective Study. J. Cancer Res. Ther. 2018, 14, S774–S778. [Google Scholar] [CrossRef]
- Kojima, T.; Watanabe, T.; Hata, K.; Shinozaki, M.; Yokoyama, T.; Nagawa, H. Cytomegalovirus Infection in Ulcerative Colitis. Scand J. Gastroenterol. 2006, 41, 706–711. [Google Scholar] [CrossRef]
- Kolho, K.L.; Klemola, P.; Simonen-Tikka, M.L.; Ollonen, M.L.; Roivainen, M. Enteric Viral Pathogens in Children with Inflammatory Bowel Disease. J. Med. Virol. 2012, 84, 345–347. [Google Scholar] [CrossRef]
- Kong, C.S.; Welton, M.L.; Longacre, T.A. Role of Human Papillomavirus in Squamous Cell Metaplasia-Dysplasia-Carcinoma of the Rectum. Am. J. Surg. Pathol. 2007, 31, 919–925. [Google Scholar] [CrossRef]
- Ksiaa, F.; Ziadi, S.; Mokni, M.; Korbi, S.; Trimeche, M. The Presence of JC Virus in Gastric Carcinomas Correlates with Patient’s Age, Intestinal Histological Type and Aberrant Methylation of Tumor Suppressor Genes. Mod. Pathol. 2010, 23, 522–530. [Google Scholar] [CrossRef] [Green Version]
- Ksiaa, F.; Allous, A.; Ziadi, S.; Mokni, M.; Trimeche, M. Assessment and Biological Significance of JC Polyomavirus in Colorectal Cancer in Tunisia. J. Buon 2015, 20, 762–769. [Google Scholar]
- Laghi, L.; Randolph, A.E.; Chauhan, D.P.; Marra, G.; Major, E.O.; Neel, J.V.; Boland, C.R. JC Virus DNA Is Present in the Mucosa of the Human Colon and in Colorectal Cancers. Proc. Natl. Acad. Sci. USA 1999, 96, 7484–7489. [Google Scholar] [CrossRef]
- Lavy, A.; Broide, E.; Reif, S.; Keter, D.; Niv, Y.; Odes, S.; Eliakim, R.; Halak, A.; Ron, Y.; Patz, J.; et al. Measles Is More Prevalent in Crohn’s Disease Patients. A Multicentre Israeli Study. Dig. Liver Dis. 2001, 33, 472–476. [Google Scholar] [CrossRef]
- Lee, Y.M.; Leu, S.Y.; Chiang, H.; Fung, C.P.; Liu, W.T. Human Papillomavirus Type 18 in Colorectal Cancer. J. Microbiol. Immunol. Infect. 2001, 34, 87–91. [Google Scholar]
- Leveque, N.; Brixi-Benmansour, H.; Reig, T.; Renois, F.; Talmud, D.; Brodard, V.; Coste, J.F.; De Champs, C.; Andréoletti, L.; Diebold, M.D. Low Frequency of Cytomegalovirus Infection during Exacerbations of Inflammatory Bowel Diseases. J. Med. Virol. 2010, 82, 1694–1700. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, J.; Zhu, G.; Zhang, X.; Zhai, H.; Zhang, W.; Wang, W.; Huang, G. Detection of Parvovirus B19 Nucleic Acids and Expression of Viral VP1/VP2 Antigen in Human Colon Carcinoma. Am. J. Gastroenterol. 2007, 102, 1489–1498. [Google Scholar] [CrossRef]
- Lin, P.Y.; Fung, C.Y.; Chang, F.P.; Huang, W.S.; Chen, W.C.; Wang, J.Y.; Chang, D. Prevalence and Genotype Identification of Human JC Virus in Colon Cancer in Taiwan. J. Med. Virol. 2008, 80, 1828–1834. [Google Scholar] [CrossRef]
- Liu, F.; Mou, X.; Zhao, N.; Lin, J.; Teng, L.; Xiang, C. Prevalence of Human Papillomavirus in Chinese Patients with Colorectal Cancer. Colorectal. Dis. 2011, 13, 865–871. [Google Scholar] [CrossRef]
- Lu, T.; Yang, Q.; Li, M.; Zhang, J.; Zou, J.; Huang, L.; Lin, J.; Jin, H.; He, J. HBV Infection and Extra-Hepatic Cancers in Adolescents and 20s: A Retrospective Study in China. Cancer Epidemiol. 2018, 55, 149–155. [Google Scholar] [CrossRef]
- Lundstig, A.; Stattin, P.; Persson, K.; Sasnauskas, K.; Viscidi, R.P.; Gislefoss, R.E.; Dillner, J. No Excess Risk for Colorectal Cancer among Subjects Seropositive for the JC Polyomavirus. Int. J. Cancer 2007, 121, 1098–1102. [Google Scholar] [CrossRef] [Green Version]
- Lv, Y.-L.; Han, F.-F.; An, Z.-L.; Jia, Y.; Xuan, L.-L.; Gong, L.-L.; Zhang, W.; Ren, L.-L.; Yang, S.; Liu, H.; et al. Cytomegalovirus Infection Is a Risk Factor in Gastrointestinal Cancer: A Cross-Sectional and Meta-Analysis Study. Intervirology 2020, 63, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Mackey, J.K.; Green, M.; Wold, W.S.; Rigden, P. Analysis of Human Cancer DNA for DNA Sequences of Human Adenovirus Type 4. J. Natl. Cancer Inst. 1979, 62, 23–26. [Google Scholar] [PubMed]
- Maconi, G.; Colombo, E.; Zerbi, P.; Sampietro, G.M.; Fociani, P.; Bosani, M.; Cassinotti, A.; Casini, V.; Russo, A.; Ardizzone, S.; et al. Prevalence, Detection Rate and Outcome of Cytomegalovirus Infection in Ulcerative Colitis Patients Requiring Colonic Resection. Dig. Liver Dis. 2005, 37, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Malekpour Afshar, R.; Deldar, Z.; Mollaei, H.; Iranpour, M. Evaluation of HPV DNA Positivity in Colorectal Cancer Patients in Kerman, Southeast Iran. Asian Pac. J. Cancer Prev. 2018, 19, 193–198. [Google Scholar] [CrossRef]
- Mariguela, V.C.; Chacha, S.G.; Cunha, A.; Troncon, L.E.; Zucoloto, S.; Figueiredo, L.T. Cytomegalovirus in Colorectal Cancer and Idiopathic Ulcerative Colitis. Rev. Inst. Med. Trop Sao Paulo 2008, 50, 83–87. [Google Scholar] [CrossRef] [Green Version]
- Mehrabani-Khasraghi, S.; Ameli, M.; Khalily, F. Demonstration of Herpes Simplex Virus, Cytomegalovirus, and Epstein-Barr Virus in Colorectal Cancer. Iran Biomed. J. 2016, 20, 302–306. [Google Scholar] [CrossRef]
- Militello, V.; Trevisan, M.; Squarzon, L.; Biasolo, M.A.; Rugge, M.; Militello, C.; Palu, G.; Barzon, L. Investigation on the Presence of Polyomavirus, Herpesvirus, and Papillomavirus Sequences in Colorectal Neoplasms and Their Association with Cancer. Int. J. Cancer 2009, 124, 2501–2503. [Google Scholar] [CrossRef]
- Montgomery, S.M.; Morris, D.L.; Pounder, R.E.; Wakefield, A.J. Paramyxovirus Infections in Childhood and Subsequent Inflammatory Bowel Disease. Gastroenterology 1999, 116, 796–803. [Google Scholar] [CrossRef]
- Morewaya, J.; Koriyama, C.; Akiba, S.; Shan, D.; Itoh, T.; Eizuru, Y. Epstein-Barr Virus-Associated Gastric Carcinoma in Papua New Guinea. Oncol. Rep. 2004, 12, 1093–1098. [Google Scholar] [CrossRef]
- Mou, X.; Chen, L.; Liu, F.; Lin, J.; Diao, P.; Wang, H.; Li, Y.; Lin, J.; Teng, L.; Xiang, C. Prevalence of JC Virus in Chinese Patients with Colorectal Cancer. PLoS ONE 2012, 7, e35900. [Google Scholar] [CrossRef] [Green Version]
- Newcomb, P.A.; Bush, A.C.; Stoner, G.L.; Lampe, J.W.; Potter, J.D.; Bigler, J. No Evidence of an Association of JC Virus and Colon Neoplasia. Cancer Epidemiol. Biomark. Prev. 2004, 13, 662–666. [Google Scholar] [CrossRef]
- Niv, Y.; Vilkin, A.; Brenner, B.; Kendel, Y.; Morgenstern, S.; Levi, Z. HMLH1 Promoter Methylation and JC Virus T Antigen Presence in the Tumor Tissue of Colorectal Cancer Israeli Patients of Different Ethnic Groups. Eur. J. Gastroenterol. Hepatol. 2010, 22, 938–941. [Google Scholar] [CrossRef]
- Nosho, K.; Yamamoto, H.; Takahashi, T.; Mikami, M.; Hizaki, K.; Maehata, T.; Taniguchi, H.; Yamaoka, S.; Adachi, Y.; Itoh, F.; et al. Correlation of Laterally Spreading Type and JC Virus with Methylator Phenotype Status in Colorectal Adenoma. Hum. Pathol. 2008, 39, 767–775. [Google Scholar] [CrossRef]
- Nosrati, A.; Naghshvar, F.; Torabizadeh, Z.; Haghshenas, M.; Sangsefidi, H. Relationship between Human Papilloma Virus and Colorectal Cancer in Northern Iran. Middle East J. Cancer 2015, 6, 237–241. [Google Scholar]
- Oda, K.; Koda, K.; Takiguchi, N.; Nunomura, M.; Seike, K.; Miyazaki, M. Detection of Epstein-Barr Virus in Gastric Carcinoma Cells and Surrounding Lymphocytes. Gastric. Cancer 2003, 6, 173–178. [Google Scholar] [CrossRef] [Green Version]
- Perez, L.O.; Abba, M.C.; Laguens, R.M.; Golijow, C.D. Analysis of Adenocarcinoma of the Colon and Rectum: Detection of Human Papillomavirus (HPV) DNA by Polymerase Chain Reaction. Colorectal. Dis. 2005, 7, 492–495. [Google Scholar] [CrossRef]
- Pironi, L.; Bonvicini, F.; Gionchetti, P.; D’Errico, A.; Rizzello, F.; Corsini, C.; Foroni, L.; Gallinella, G. Parvovirus B19 Infection Localized in the Intestinal Mucosa and Associated with Severe Inflammatory Bowel Disease. J. Clin. Microbiol. 2009, 47, 1591–1595. [Google Scholar] [CrossRef] [Green Version]
- Roblin, X.; Pillet, S.; Oussalah, A.; Berthelot, P.; Del Tedesco, E.; Phelip, J.M.; Chambonnière, M.L.; Garraud, O.; Peyrin-Biroulet, L.; Pozzetto, B. Cytomegalovirus Load in Inflamed Intestinal Tissue Is Predictive of Resistance to Immunosuppressive Therapy in Ulcerative Colitis. Am. J. Gastroenterol. 2011, 106, 2001–2008. [Google Scholar] [CrossRef]
- Roblin, X.; Pillet, S.; Berthelot, P.; Del Tedesco, E.; Phelip, J.M.; Chambonnière, M.L.; Peyrin-Biroulet, L.; Pozzetto, B. Prevalence of Cytomegalovirus Infection in Steroid-Refractory Crohn’s Disease. Inflamm. Bowel Dis. 2012, 18, E1396–E1397. [Google Scholar] [CrossRef]
- Roche, J.K.; Cheung, K.S.; Boldogh, I.; Huang, E.S.; Lang, D.J. Cytomegalovirus: Detection in Human Colonic and Circulating Mononuclear Cells in Association with Gastrointestinal Disease. Int. J. Cancer 1981, 27, 659–667. [Google Scholar] [CrossRef]
- Rollison, D.E.; Helzlsouer, K.J.; Lee, J.H.; Fulp, W.; Clipp, S.; Hoffman-Bolton, J.A.; Giuliano, A.R.; Platz, E.A.; Viscidi, R.P. Prospective Study of JC Virus Seroreactivity and the Development of Colorectal Cancers and Adenomas. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1515–1523. [Google Scholar] [CrossRef] [Green Version]
- Ruger, R.; Fleckenstein, B. Cytomegalovirus DNA in Colorectal Carcinoma Tissues. Klin. Wochenschr. 1985, 63, 405–408. [Google Scholar] [CrossRef]
- Salepci, T.; Yazici, H.; Dane, F.; Topuz, E.; Dalay, N.; Onat, H.; Aykan, F.; Seker, M.; Aydiner, A. Detection of Human Papillomavirus DNA by Polymerase Chain Reaction and Southern Blot Hybridization in Colorectal Cancer Patients. J. Buon 2009, 14, 495–499. [Google Scholar]
- Samaka, R.M.; Abd El-Wahed, M.M.; Aiad, H.A.; Kandil, M.A.; Al-Sharaky, D.R. Does JC Virus Have a Role in the Etiology and Prognosis of Egyptian Colorectal Carcinoma? Apmis 2013, 121, 316–328. [Google Scholar] [CrossRef]
- Sarvari, J.; Mahmoudvand, S.; Pirbonyeh, N.; Safaei, A.; Hosseini, S.Y. The Very Low Frequency of Epstein-Barr JC and BK Viruses DNA in Colorectal Cancer Tissues in Shiraz, Southwest Iran. Pol. J. Microbiol. 2018, 67, 73–79. [Google Scholar] [CrossRef]
- Schildgen, V.; Malecki, M.; Tillmann, R.L.; Brockmann, M.; Schildgen, O. The Human Bocavirus Is Associated with Some Lung and Colorectal Cancers and Persists in Solid Tumors. PLoS ONE 2013, 8, e68020. [Google Scholar] [CrossRef] [Green Version]
- Shah, K.V.; Daniel, R.W.; Simons, J.W.; Vogelstein, B. Investigation of Colon Cancers for Human Papillomavirus Genomic Sequences by Polymerase Chain Reaction. J. Surg. Oncol. 1992, 51, 5–7. [Google Scholar] [CrossRef]
- Shibata, D.; Hawes, D.; Stemmermann, G.N.; Weiss, L.M. Epstein-Barr Virus-Associated Gastric Adenocarcinoma among Japanese Americans in Hawaii. Cancer Epidemiol. Biomark. Prev. 1993, 2, 213–217. [Google Scholar]
- Sinagra, E.; Raimondo, D.; Gallo, E.; Stella, M.; Cottone, M.; Orlando, A.; Rossi, F.; Orlando, E.; Messina, M.; Tomasello, G.; et al. Could JC Virus Provoke Metastasis in Colon Cancer? World J. Gastroenterol. 2014, 20, 15745–15749. [Google Scholar] [CrossRef] [Green Version]
- Su, F.-H.; Le, T.N.; Muo, C.-H.; Te, S.A.; Sung, F.-C.; Yeh, C.-C. Chronic Hepatitis B Virus Infection Associated with Increased Colorectal Cancer Risk in Taiwanese Population. Viruses 2020, 12, 97. [Google Scholar] [CrossRef] [Green Version]
- Sura, R.; Gavrilov, B.; Flamand, L.; Ablashi, D.; Cartun, R.; Colombel, J.F.; Van Kruiningen, H.J. Human Herpesvirus-6 in Patients with Crohn’s Disease. Apmis 2010, 118, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Tafvizi, F.; Fard, Z.T. Detection of Human Cytomegalovirus in Patients with Colorectal Cancer by Nested-PCR. Asian Pac. J. Cancer Prev 2014, 15, 1453–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tafvizi, F.; Fard, Z.T.; Assareh, R. Epstein-Barr Virus DNA in Colorectal Carcinoma in Iranian Patients. Pol. J. Pathol 2015, 66, 154–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taherian, H.; Tafvizi, F.; Fard, Z.T.; Abdirad, A. Lack of Association between Human Papillomavirus Infection and Colorectal Cancer. Prz. Gastroenterol. 2014, 9, 280–284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theodoropoulos, G.; Panoussopoulos, D.; Papaconstantinou, I.; Gazouli, M.; Perdiki, M.; Bramis, J.; Lazaris, A. Assessment of JC Polyoma Virus in Colon Neoplasms. Colon. Rectum 2005, 48, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Tolentino, Y.F.; Fogaca, H.S.; Zaltman, C.; Ximenes, L.L.; Coelho, H.S. Hepatitis B Virus Prevalence and Transmission Risk Factors in Inflammatory Bowel Disease Patients at Clementino Fraga Filho University Hospital. World J. Gastroenterol. 2008, 14, 3201–3206. [Google Scholar] [CrossRef]
- Toumi, W.; Ripalti, A.; Ricciardiello, L.; Cherif, A.; Gargouri, D.; Bouhafa, A.; Kharrat, J.; Jarboui, S.; Benrhouma, H.; Zili, M.; et al. Detection of a New JCV Strain of Genotype A in a Subpopulation of Colorectal Adenocarcinomas in Tunisia. New Microbiol. 2017, 40, 99–106. [Google Scholar]
- Trimeche, M.; Ksiaa, F.; Ziadi, S.; Mestiri, S.; Hachana, M.; Gacem, R.B.; Sriha, B.; Korbi, S. Prevalence and Characteristics of Epstein-Barr Virus-Associated Gastric Carcinomas in Tunisia. Eur. J. Gastroenterol. Hepatol. 2009, 21, 1001–1007. [Google Scholar] [CrossRef]
- Truong, C.D.; Feng, W.; Li, W.; Khoury, T.; Li, Q.; Alrawi, S.; Yu, Y.; Xie, K.; Yao, J.; Tan, D. Characteristics of Epstein-Barr Virus-Associated Gastric Cancer: A Study of 235 Cases at a Comprehensive Cancer Center in U.S.A. J. Exp. Clin. Cancer Res. 2009, 28, 14. [Google Scholar] [CrossRef] [Green Version]
- Tsai, S.Y.; Yang, T.Y.; Lin, C.L.; Tsai, Y.H.; Kuo, C.F.; Kao, C.H. Increased Risk of Varicella Zoster Virus Infection in Inflammatory Bowel Disease in an Asian Population: A Nationwide Population-Based Cohort Study. Int. J. Clin. Pract. 2015, 69, 228–234. [Google Scholar] [CrossRef]
- Vanoli, A.; Di Sabatino, A.; Martino, M.; Dallera, E.; Furlan, D.; Mescoli, C.; Macciomei, M.C.; Biancone, L.; Neri, B.; Grillo, F.; et al. Epstein-Barr Virus-Positive Ileal Carcinomas Associated with Crohn’s Disease. Virchows Arch. 2017, 471, 549–552. [Google Scholar] [CrossRef]
- Vega, R.; Bertran, X.; Menacho, M.; Domenech, E.; de Vega, V.M.; Hombrados, M.; Ojanguren, I.; Gassull, M.A. Cytomegalovirus Infection in Patients with Inflammatory Bowel Disease. Am. J. Gastroenterol. 1999, 94, 1053–1056. [Google Scholar] [CrossRef]
- Vilkin, A.; Ronen, Z.; Levi, Z.; Morgenstern, S.; Halpern, M.; Niv, Y. Presence of JC Virus DNA in the Tumor Tissue and Normal Mucosa of Patients with Sporadic Colorectal Cancer (CRC) or with Positive Family History and Bethesda Criteria. Dig. Sci. 2012, 57, 79–84. [Google Scholar] [CrossRef]
- Wakefield, A.J.; Fox, J.D.; Sawyerr, A.M.; Taylor, J.E.; Sweenie, C.H.; Smith, M.; Emery, V.C.; Hudson, M.; Tedder, R.S.; Pounder, R.E. Detection of Herpesvirus DNA in the Large Intestine of Patients with Ulcerative Colitis and Crohn’s Disease Using the Nested Polymerase Chain Reaction. J. Med. Virol. 1992, 38, 183–190. [Google Scholar] [CrossRef]
- Weinreb, D.B. Re: Detection of JC Virus Sequences in Colorectal Cancers in Japan. Virchows Arch. 2006, 448, 239. [Google Scholar] [CrossRef]
- Wong, N.A.; Herbst, H.; Herrmann, K.; Kirchner, T.; Krajewski, A.S.; Moorghen, M.; Niedobitek, F.; Rooney, N.; Shepherd, N.A.; Niedobitek, G. Epstein-Barr Virus Infection in Colorectal Neoplasms Associated with Inflammatory Bowel Disease: Detection of the Virus in Lymphomas but Not in Adenocarcinomas. J. Pathol. 2003, 201, 312–318. [Google Scholar] [CrossRef]
- Yanai, H.; Takada, K.; Shimizu, N.; Mizugaki, Y.; Tada, M.; Okita, K. Epstein-Barr Virus Infection in Non-Carcinomatous Gastric Epithelium. J. Pathol. 1997, 183, 293–298. [Google Scholar] [CrossRef]
- Yanai, H.; Shimizu, N.; Nagasaki, S.; Mitani, N.; Okita, K. Epstein-Barr Virus Infection of the Colon with Inflammatory Bowel Disease. Am. J. Gastroenterol. 1999, 94, 1582–1586. [Google Scholar] [CrossRef]
- Yavuzer, D.; Karadayi, N.; Salepci, T.; Baloglu, H.; Dabak, R.; Bayramicli, O.U. Investigation of Human Papillomavirus DNA in Colorectal Carcinomas and Adenomas. Med. Oncol. 2011, 28, 127–132. [Google Scholar] [CrossRef]
- Yi, F.; Zhao, J.; Luckheeram, R.V.; Lei, Y.; Wang, C.; Huang, S.; Song, L.; Wang, W.; Xia, B. The Prevalence and Risk Factors of Cytomegalovirus Infection in Inflammatory Bowel Disease in Wuhan, Central China. Virol. J. 2013, 10, 43. [Google Scholar] [CrossRef] [Green Version]
- Yuen, S.T.; Chung, L.P.; Leung, S.Y.; Luk, I.S.; Chan, S.Y.; Ho, J. In Situ Detection of Epstein-Barr Virus in Gastric and Colorectal Adenocarcinomas. Am. J. Surg. Pathol. 1994, 18, 1158–1163. [Google Scholar] [CrossRef]
- Yunos, A.M.; Jaafar, H.; Idris, F.M.; Kaur, G.; Mabruk, M.J. Detection of Epstein-Barr Virus in Lower Gastrointestinal Tract Lymphomas: A Study in Malaysian Patients. Mol. Diagn. Ther. 2006, 10, 251–256. [Google Scholar] [CrossRef]
- Zagorowicz, E.; Bugajski, M.; Wieszczy, P.; Pietrzak, A.; Magdziak, A.; Mroz, A. Cytomegalovirus Infection in Ulcerative Colitis Is Related to Severe Inflammation and a High Count of Cytomegalovirus-Positive Cells in Biopsy Is a Risk Factor for Colectomy. J. Crohns Colitis 2016, 10, 1205–1211. [Google Scholar] [CrossRef]






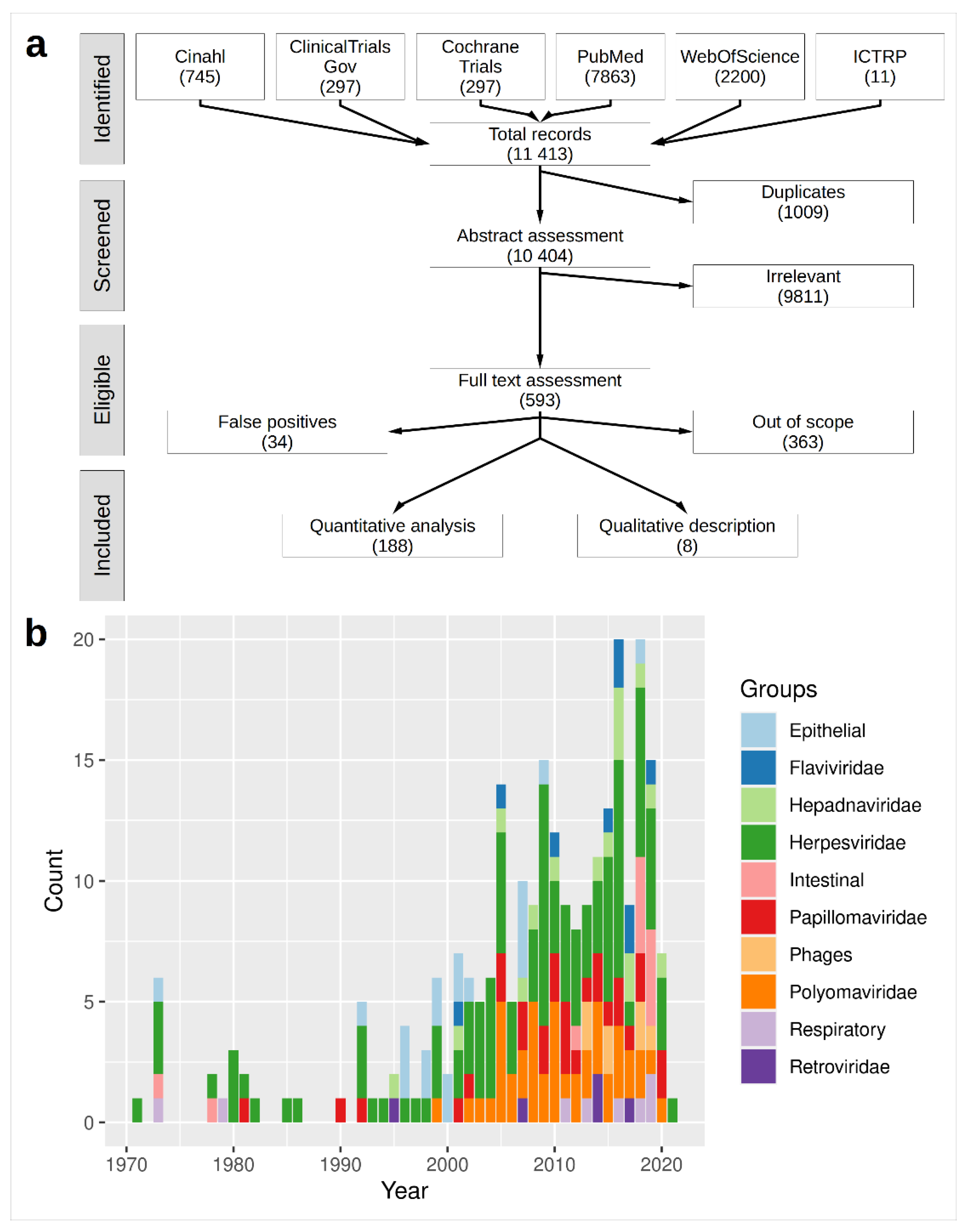{kind=link}
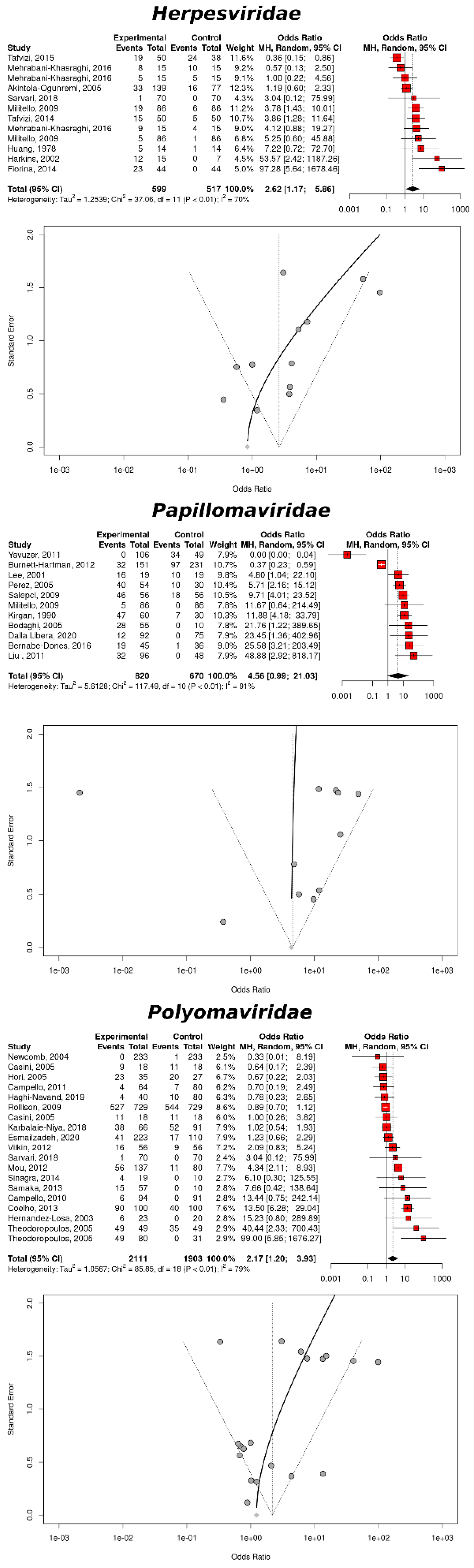{kind=link}
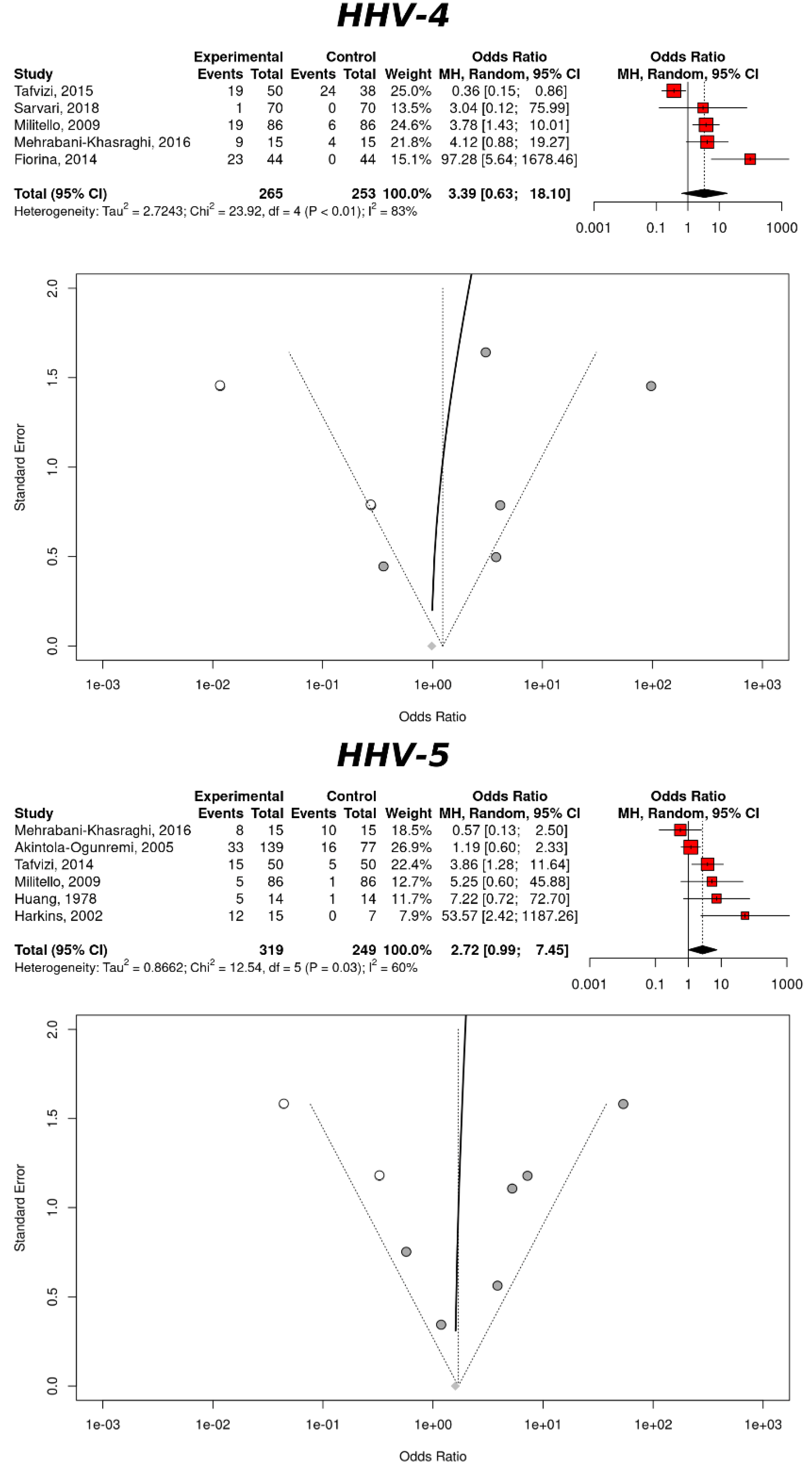{kind=link}
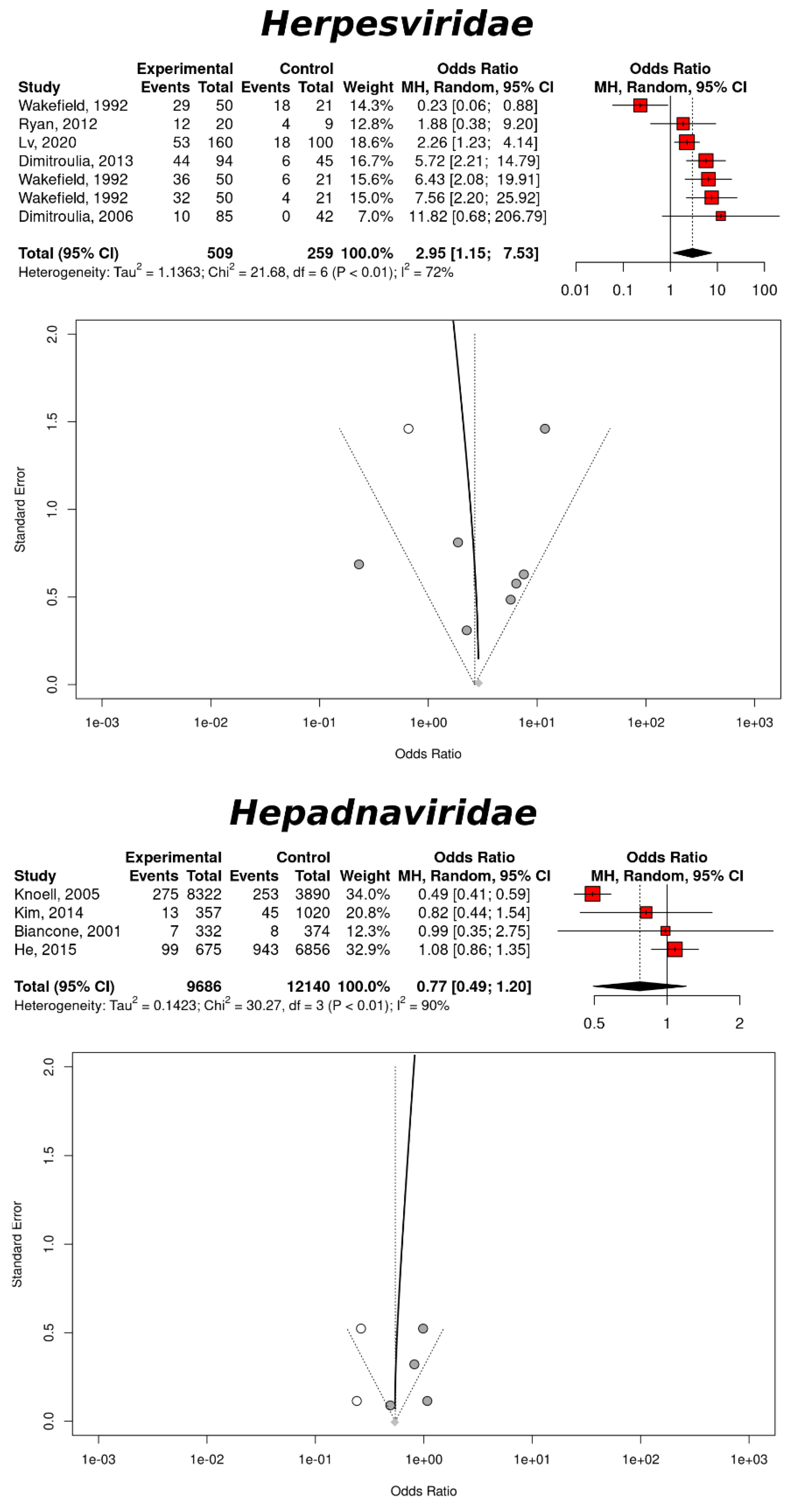{kind=link}
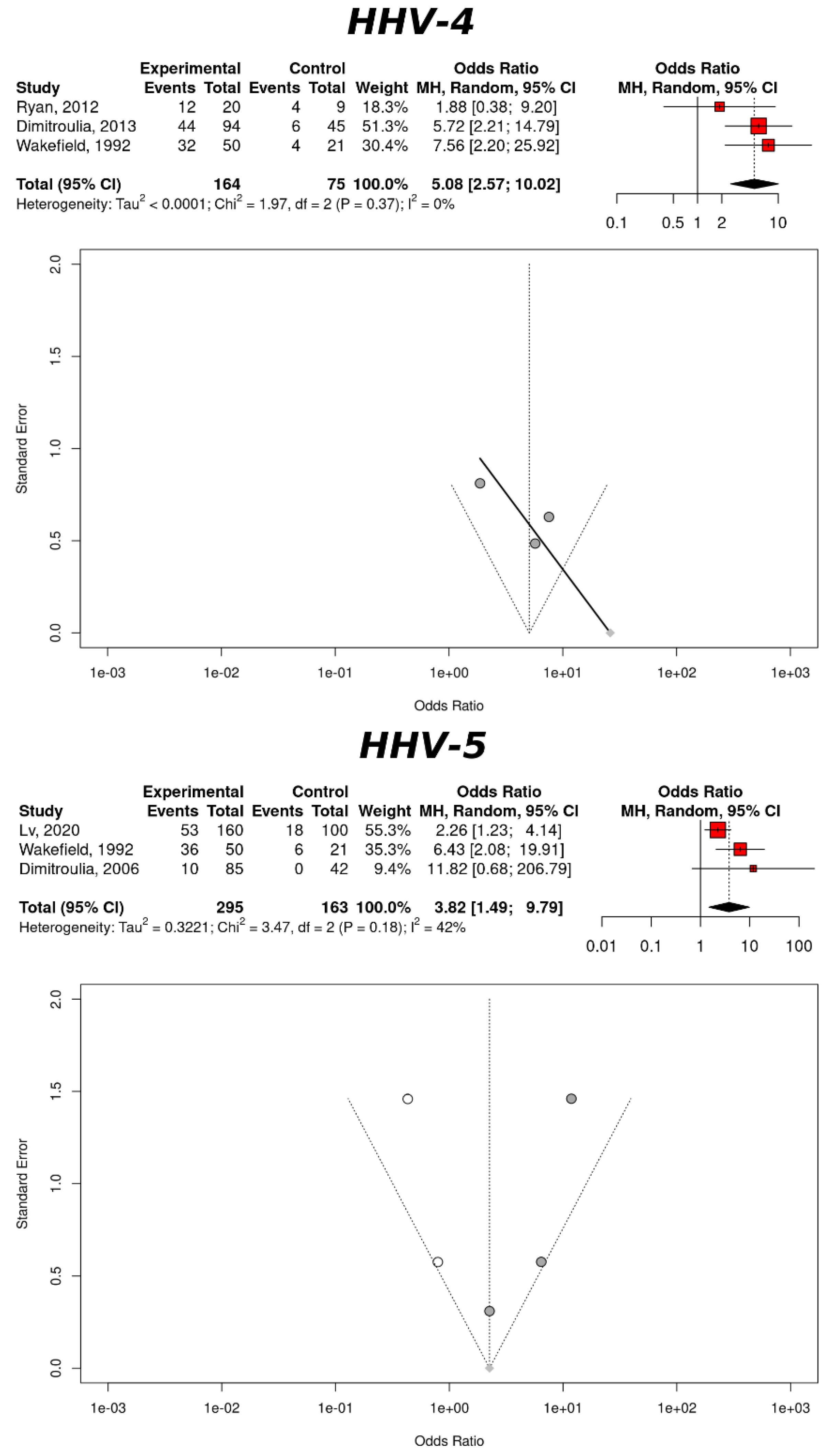{kind=link}
| Disease | Source | Group | Studies * | Cases † | Controls † | OR | p-Value | I² (%) | ERT | CQT |
|---|---|---|---|---|---|---|---|---|---|---|
| CRC | Colon/Rectum | Herpes | 12/28 | 375/1968 | 72/517 | 2.62 (1.17–5.86) | 0.0187 | 70.3 (46.4–88.6) | 0.0417 | 0.0001 |
| Papilloma | 11/26 | 517/2402 | 177/888 | 4.56 (0.99–21.03) | 0.0512 | 91.5 (86.8–94.5) | 0.1270 | < 0.0001 | ||
| Polyoma | 19/36 | 1531/3980 | 768/2029 | 2.17 (1.20–3.93) | 0.0105 | 79.0 (67.9–86.3) | 0.0413 | < 0.0001 | ||
| Hepadna | 1/1 | 3536/69,478 | 2924/69,478 | 1.22 (1.16–1.28) | <0.0001 | — | — | — | ||
| Epithelial | 2/3 | 116/132 | 86/119 | 3.76 (1.21–11.68) | 0.0221 | — | — | 0.1803 | ||
| Papilloma | 1/1 | 21/97 | 42/184 | 0.93 (0.52–1.69) | 0.8221 | — | — | — | ||
| Hepadna | 1/1 | 72/284 | 212/284 | 0.12 (0.08–0.17) | <0.0001 | — | — | — | ||
| Flavivirus | 1/1 | 51/255 | 204/255 | 0.63 (0.04–0.10) | <0.0001 | — | — | — | ||
| Retrovirus | 2/3 | 146/674 | 284/1542 | 0.82 (0.58–1.18) | 0.2898 | — | — | 0.3099 | ||
| Serum | Herpes | 5/5 | 64/89 | 37/79 | 3.06 (0.74–12.65) | 0.1227 | 54.3 (0–83.2) | — | 0.6740 | |
| Polyoma | 3/5 | 1029/1409 | 1008/1409 | 1.12 (0.89–1.42) | 0.3224 | 30.9 (0–92.8) | — | 0.2351 | ||
| Hepadna | 1/3 | 674/6333 | 3168/96,000 | 1.31 (0.89–1.95) | 0.1754 | — | — | — | ||
| Flavivirus | 1/3 | 10/820 | 806/96,000 | 1.58 (0.78–3.19) | 0.2009 | — | — | — | ||
| GC | Gastric | Herpes | 1/22 | 502/5097 | 207/225 | 1.57 (0.60–4.06) | 0.3567 | — | — | — |
| Papilloma | 0/1 | 9/302 | 0/0 | — | — | — | — | — | ||
| Polyoma | 2/2 | 18/80 | 4/82 | 5.22 (1.66–16.47) | 0.0048 | 0 | 0.6804 | — | ||
| Epithelial | 0/1 | 17/32 | 0/0 | — | — | — | — | — | ||
| Serum | Herpes | 1/1 | 43/48 | 88/93 | 0.49 (0.13–1.78) | 0.2774 | — | — | — | |
| Hepadna | 1/1 | 26/150 | 20/150 | 1.36 (0.72–2.57) | 0.3375 | — | — | — | ||
| Retrovirus | 0/1 | 0/150 | 0/150 | — | — | — | — | — | ||
| IBD | Colon/Rectum | Herpes | 9/16 | 173/882 | 10/211 | 2.71 (0.91–8.06) | 0.0723 | 50.6 (0–76.9) | — | 0.3980 |
| Stools | Herpes | 0/1 | 9/400 | 0/0 | — | — | — | — | — | |
| Intestinal | 5/7 | 65/2609 | 3108/35,321 | 0.27 (0.09–0.08) | 0.0236 | 92.0 (84.4–95.6) | — | < 0.0001 | ||
| Respiratory | 1/2 | 3/711 | 106/8826 | 0.29 (0.07–1.16) | 0.0801 | — | — | — | ||
| Gastric | Herpes | 7/10 | 235/591 | 56/259 | 2.90 (1.15–7.53) | 0.0241 | 72.3 (40.2–87.2) | — | 0.0014 | |
| Epithelial | 1/6 | 17/127 | 11/62 | 0.89 (0.27–2.97) | 0.8530 | — | — | — | ||
| Record | Herpes | 2/7 | 636/46,752 | 1083/33,355 | 1.22 (0.74–2.01) | 0.4377 | 60.8 (0–90.9) | — | 0.1100 | |
| Intestinal | 2/2 | 110/176,856 | 392/873,014 | 1.41 (0.92–2.17) | 0.1174 | 75.7 (0–94.5) | — | 0.0425 | ||
| Respiratory | 1/1 | 6/88,428 | 11/436,507 | 2.69 (1.00–7.28) | 0.0510 | — | — | 0.0000 | ||
| Hepadna | 1/2 | 196/3776 | 4/67 | 0.37 (0.13–1.07) | 0.0671 | — | — | 0.0000 | ||
| Flavivirus | 1/2 | 34/3556 | 1/57 | 0.75 (0.10–5.64) | 0.7799 | — | — | 0.0000 | ||
| Epithelial | 2/2 | 38/12,738 | 36/15,264 | 1.27 (0.80–2.00) | 0.3140 | 0 | — | 0.7617 | ||
| Retrovirus | 1/1 | 2/1816 | 1/84 | 0.09 (0.01–1.02) | 0.0519 | — | — | 0.0000 | ||
| Serum | Herpes | 5/12 | 1926/2267 | 256/438 | 1.53 (0.52–4.46) | 0.4379 | 82.7 (60.5–92.5) | — | 0.0001 | |
| Intestinal | 2/3 | 62/200 | 23/89 | 1.08 (0.47–2.49) | 0.8615 | 0 | — | 0.8542 | ||
| Respiratory | 1/1 | 11/57 | 20/52 | 0.38 (0.16–0.91) | 0.0291 | — | — | 0.0000 | ||
| Polyoma | 1/2 | 158/244 | 6/53 | 9.47 (3.46–25.92) | <0.0001 | — | — | 0.0000 | ||
| Hepadna | 4/8 | 591/10,769 | 1249/12,140 | 0.77 (0.49–1.20) | 0.2492 | 90.1 (77.6–95.6) | — | < 0.0001 | ||
| Flavivirus | 2/3 | 104/8969 | 66/4264 | 0.99 (0.46–2.12) | 0.9734 | 78.2 (4.9–95.0) | — | 0.0323 | ||
| Epithelial | 7/8 | 888/1372 | 729/1058 | 0.71 (0.37–1.36) | 0.3027 | 70.4 (35.3–86.5) | — | 0.0025 |
| Disease | Source | Group | Added Studies | OR | p-Value | I² (%) | ERT | CQT |
|---|---|---|---|---|---|---|---|---|
| CRC | Colorectal tissue | Herpes | 4 | 1.45 (0.58–3.65) | 0.4284 | 73.2 (56.0–83.7) | <0.0001 | 0.7797 |
| Papilloma | 4 | 1.59 (0.36–7.04) | 0.5424 | 90.0 (85.2–93.2) | <0.0001 | 0.5741 | ||
| Polyoma | 6 | 1.13 (0.52–2.44) | 0.7596 | 84.8 (78.6–89.1) | <0.0001 | 0.7587 | ||
| Serum | Herpes | 2 | 1.40 (0.26–7.69) | 0.6958 | 66.8 (25.9–85.1) | 0.0061 | — | |
| IBD | Colorectal tissue | Herpes | 0 | 2.71 (0.91–8.06) | 0.0723 | 50.6 (0–76.9) | — | 0.398 |
| Intestinal | 3 | 0.69 (0.19–2.45) | 0.5630 | 94.2 (90.8–96.4) | — | <0.0001 | ||
| Gastric tissue | Herpes | 1 | 2.67 (1.10–6.52) | 0.0307 | 69.1 (35.6–85.2) | — | 0.0019 | |
| Serum | Herpes | 1 | 2.08 (0.60–7.20) | 0.2472 | 81.8 (61.3–91.5) | — | <0.0001 | |
| Hepadna | 2 | 0.55 (0.32–0.94) | 0.0275 | 94.5 (90.6–96.8) | — | <0.0001 | ||
| Epithelial | 0 | 0.71 (0.37–1.36) | 0.3027 | 70.4 (35.3–86.5) | — | <0.0001 |
| Disease | Source | Group | Studies * | Observations † | Events † | OR | p-Value | I² (%) | ERT | CQT |
|---|---|---|---|---|---|---|---|---|---|---|
| CRC | Colorectal tissue | HHV-1 | 1/1 | 5/15 | 5/15 | 1 (0.22–4.56) | 1 | — | — | — |
| HHV-4 | 5/11 | 140/912 | 34/253 | 3.39 (0.64–18.10) | 0.1531 | 83.3 (62.0–92.6) | — | <0.0001 | ||
| HHV-5 | 6/15 | 228/855 | 33/249 | 2.71 (0.99–7.45) | 0.0519 | 60.1 (2.2–83.8) | — | 0.0281 | ||
| HHV-8 | 0/1 | 2/186 | 0/0 | — | — | — | — | — | ||
| IBD | Gastric tissue | HHV-4 | 3/4 | 89/195 | 14/75 | 5.08 (2.57–10.02) | <0.0001 | 0 (0–89.6) | — | 0.374 |
| HHV-5 | 3/5 | 117/346 | 24/163 | 3.82 (1.49–9.79) | 0.0053 | 42.4 (0–82.6) | — | 0.1761 | ||
| HHV-6 | 1/1 | 29/50 | 18/21 | 0.23 (0.06–0.88) | 0.0323 | — | — | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marongiu, L.; Venturelli, S.; Allgayer, H. Involvement of HHV-4 (Epstein–Barr Virus) and HHV-5 (Cytomegalovirus) in Inflammatory Bowel Disease and Colorectal Cancer: A Meta-Analysis. Cancers 2022, 14, 5085. https://doi.org/10.3390/cancers14205085
Marongiu L, Venturelli S, Allgayer H. Involvement of HHV-4 (Epstein–Barr Virus) and HHV-5 (Cytomegalovirus) in Inflammatory Bowel Disease and Colorectal Cancer: A Meta-Analysis. Cancers. 2022; 14(20):5085. https://doi.org/10.3390/cancers14205085
Chicago/Turabian StyleMarongiu, Luigi, Sascha Venturelli, and Heike Allgayer. 2022. "Involvement of HHV-4 (Epstein–Barr Virus) and HHV-5 (Cytomegalovirus) in Inflammatory Bowel Disease and Colorectal Cancer: A Meta-Analysis" Cancers 14, no. 20: 5085. https://doi.org/10.3390/cancers14205085