
Association between Metabolic Disorders and Cholangiocarcinoma: Impact of a Postulated Risk Factor with Rising Incidence

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Management and Treatment Protocol
2.3. Patients with a Background of Metabolic Disorders
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparison between Groups According to Metabolic Factors
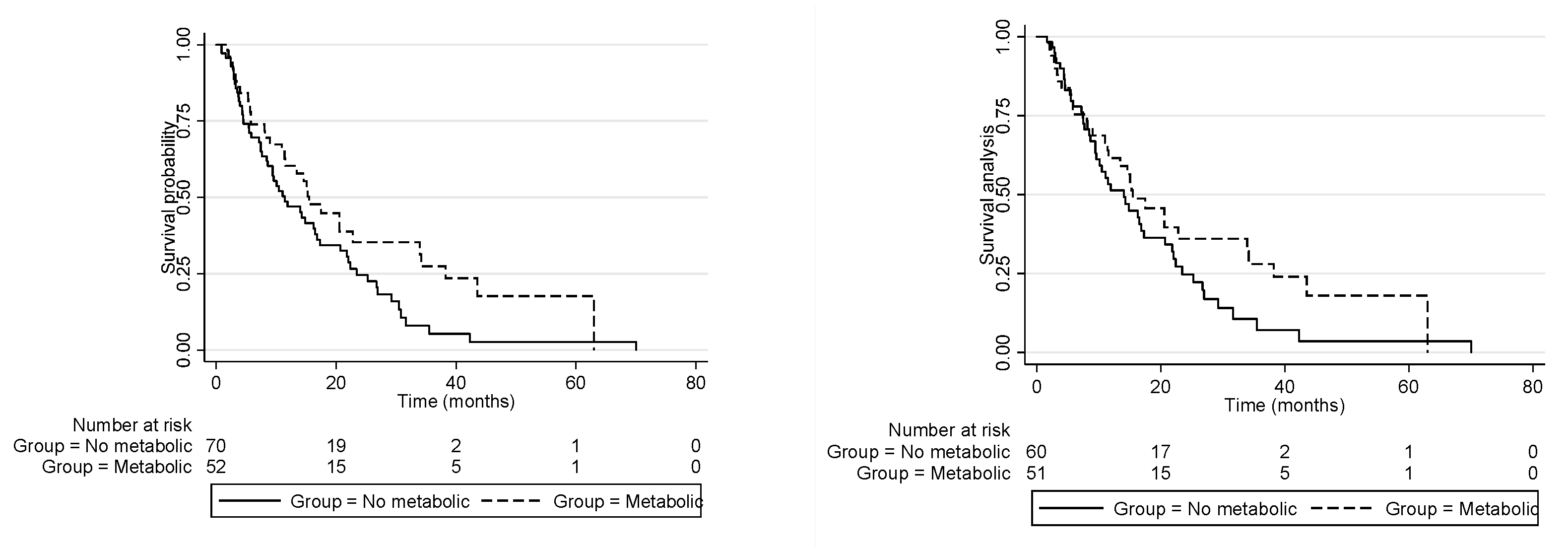
3.3. Clinical Outcomes and Overall Survival
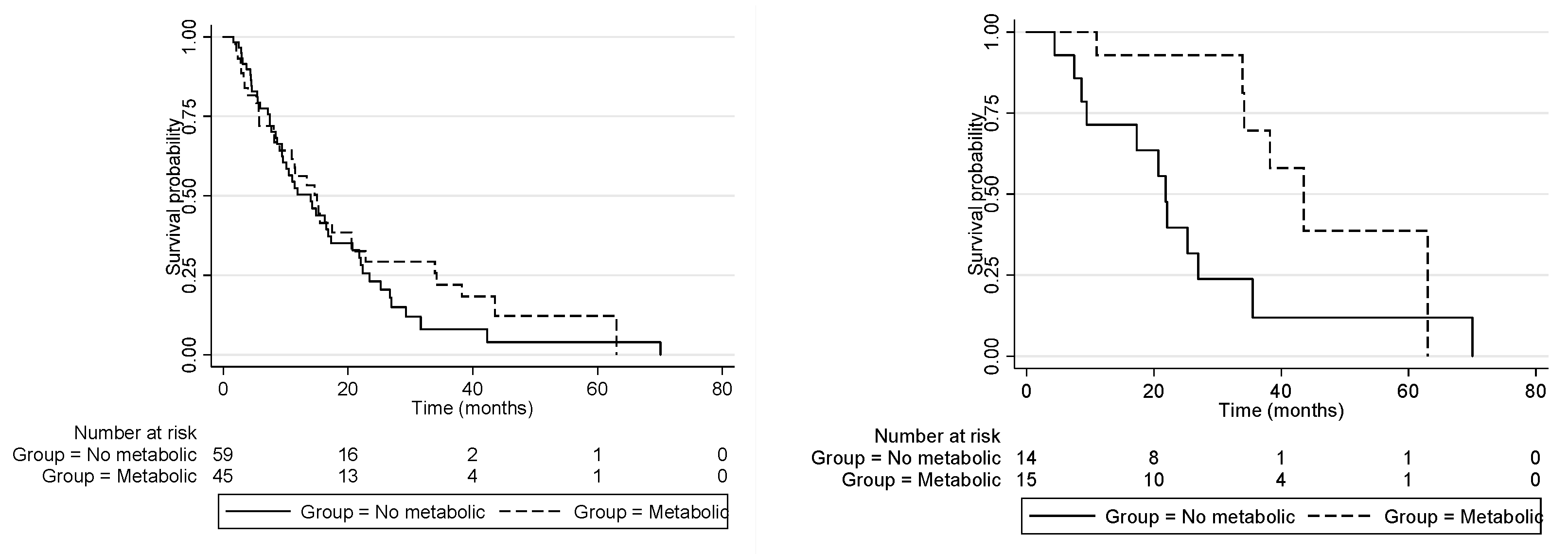
3.4. Treatment Strategies and Clinical Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Tavolari, S.; Brandi, G. Cholangiocarcinoma: Epidemiology and risk factors. Liver Int. 2019, 39, 19–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anstee, Q.M.; Targher, G.; Day, C.P. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 330–344. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.; Núñez, N.G.; Pinyol, R.; Govaere, O.; Pinter, M.; Szydlowska, M.; Gupta, R.; Qiu, M.; Deczkowska, A.; Weiner, A.; et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature 2021, 592, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Eslam, M.; Sanyal, A.J.; George, J.; Sanyal, A.; Neuschwander-Tetri, B.; Tiribelli, C.; Kleiner, D.E.; Brunt, E.; Bugianesi, E.; Yki-Järvinen, H.; et al. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014. [Google Scholar] [CrossRef]
- Neuschwander-Tetri, B.A. Hepatic lipotoxicity and the pathogenesis of nonalcoholic steatohepatitis: The central role of nontriglyceride fatty acid metabolites. Hepatology 2010, 52, 774–788. [Google Scholar] [CrossRef]
- Berres, M.L.; Nellen, A.; Wasmuth, H.E. Chemokines as immune mediators of liver diseases related to the metabolic syndrome. Dig. Dis. 2010, 28, 192–196. [Google Scholar] [CrossRef]
- Fava, G.; Alpini, G.; Rychlicki, C.; Saccomanno, S.; DeMorrow, S.; Trozzi, L.; Candelaresi, C.; Venter, J.; Di Sario, A.; Marzioni, M.; et al. Leptin enhances cholangiocarcinoma cell growth. Cancer Res. 2008, 68, 6752–6761. [Google Scholar] [CrossRef] [Green Version]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; the WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [Green Version]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D. Biliary cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graffy, P.M.; Sandfort, V.; Summers, R.M.; Pickhardt, P.J. Automated Liver Fat Quantification at Nonenhanced Abdominal CT for Population-based Steatosis Assessment. Radiology 2019, 293, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Boyce, C.J.; Pickhardt, P.J.; Kim, D.H.; Taylor, A.J.; Winter, T.C.; Bruce, R.J.; Lindstrom, M.J.; Hinshaw, J.L. Hepatic steatosis (fatty liver disease) in asymptomatic adults identified by unenhanced low-dose CT. AJR Am. J. Roentgenol. 2010, 194, 623–628. [Google Scholar] [CrossRef]
- Yang, H.; Wang, J.; Li, Z.; Yang, Y.; Yang, L.; Zhang, Y.; Shi, Y.; Cao, Y.; Zhou, J.; Wang, Z.; et al. Risk Factors and Outcomes of Early Relapse After Curative Resection of Intrahepatic Cholangiocarcinoma. Front. Oncol. 2019, 9, 854. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.-M.; Tsai, C.-Y.; Yeh, C.-N.; Yeh, T.-S.; Lee, W.-C.; Jan, Y.-Y.; Chen, M.-F. Characterization of intrahepatic cholangiocarcinoma after curative resection: Outcome, prognostic factor, and recurrence. BMC Gastroenterol. 2018, 18, 180. [Google Scholar] [CrossRef] [Green Version]
- Bekki, Y.; Von Ahrens, D.; Takahashi, H.; Schwartz, M.; Gunasekaran, G. Recurrent Intrahepatic Cholangiocarcinoma—Review. Front. Oncol. 2021, 11, 776863. [Google Scholar] [CrossRef]
- Welzel, T.M.; Graubard, B.I.; El–Serag, H.B.; Shaib, Y.H.; Hsing, A.W.; Davila, J.A.; McGlynn, K.A. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in the United States: A population-based case-control study. Clin. Gastroenterol. Hepatol. 2007, 5, 1221–1228. [Google Scholar] [CrossRef] [Green Version]
- Welzel, T.M.; Mellemkjaer, L.; Gloria, G.; Sakoda, L.C.; Hsing, A.W.; El Ghormli, L.; Olsen, J.H.; McGlynn, K.A. Risk factors for intrahepatic cholangiocarcinoma in a low-risk population: A nationwide case-control study. Int. J. Cancer 2007, 120, 638–641. [Google Scholar] [CrossRef]
- Chaiteerakij, R.; Yang, J.D.; Harmsen, W.S.; Slettedahl, S.; Mettler, T.A.; Fredericksen, Z.S.; Kim, W.R.; Gores, G.J.; Roberts, R.O.; Olson, J.E.; et al. Risk factors for intrahepatic cholangiocarcinoma: Association between metformin use and reduced cancer risk. Hepatology 2013, 57, 648–655. [Google Scholar] [CrossRef] [Green Version]
- Xiong, J.; Lu, X.; Xu, W.; Bai, Y.; Huang, H.; Bian, J.; Zhang, L.; Long, J.; Xu, Y.; Wang, Z.; et al. Metabolic syndrome and the risk of cholangiocarcinoma: A hospital-based case–control study in China. Cancer Manag. Res. 2018, 10, 3849–3855. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; You, L.; Xie, W.; Ning, L.; Lang, J. Smoking and risk of cholangiocarcinoma: A systematic review and meta-analysis. Oncotarget 2017, 8, 100570–100581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Djiogue, S.; Nwabo Kamdje, A.H.; Vecchio, L.; Kipanyula, M.J.; Farahna, M.; Aldebasi, Y.; Seke Etet, P.F. Insulin resistance and cancer: The role of insulin and IGFs. Endocr. Relat. Cancer 2013, 20, R1–R17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Jiménez, C.; García-Martínez, J.M.; Chocarro-Calvo, A.; De la Vieja, A. A new link between diabetes and cancer: Enhanced WNT/β-catenin signaling by high glucose. J. Mol. Endocrinol. 2013, 52, R51–R66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuriyama, K.; Higuchi, T.; Yokobori, T.; Saito, H.; Yoshida, T.; Hara, K.; Suzuki, S.; Sakai, M.; Sohda, M.; Higuchi, T.; et al. Uptake of positron emission tomography tracers reflects the tumor immune status in esophageal squamous cell carcinoma. Cancer Sci. 2020, 111, 1969–1978. [Google Scholar] [CrossRef]
- Oh, D.-Y.; He, A.R.; Qin, S.; Chen, L.-T.; Okusaka, T.; Vogel, A.; Kim, J.W.; Suksombooncharoen, T.; Lee, M.A.; Kitano, M.; et al. A phase 3 randomized, double-blind, placebo-controlled study of durvalumab in combination with gemcitabine plus cisplatin (GemCis) in patients (pts) with advanced biliary tract cancer (BTC): TOPAZ-1. J. Clin. Oncol. 2022, 40 (Suppl. 4), 378. [Google Scholar] [CrossRef]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K.; et al. Second-line FOLFOX chemotherapy versus active symptom control for advanced biliary tract cancer (ABC-06): A phase 3, open-label, randomised, controlled trial. Lancet Oncol. 2021, 22, 690–701. [Google Scholar] [CrossRef]
- Izquierdo-Sanchez, L.; Lamarca, A.; La Casta, A.; Buettner, S.; Utpatel, K.; Klümpen, H.-J.; Adeva, J.; Vogel, A.; Lleo, A.; Fabris, L.; et al. Cholangiocarcinoma landscape in Europe: Diagnostic, prognostic and therapeutic insights from the ENSCCA Registry. J. Hepatol. 2022, 76, 1109–1121. [Google Scholar] [CrossRef]
- Foerster, F.; Gairing, S.J.; Müller, L.; Galle, P.R. NAFLD-driven HCC: Safety and efficacy of current and emerging treatment options. J. Hepatol. 2022, 76, 446–457. [Google Scholar] [CrossRef]
- Molinari, M.; Kaltenmeier, C.; Samra, P.-B.; Liu, H.; Wessel, C.; Klem, M.L.; Dharmayan, S.; Emmanuel, B.; Al Harakeh, H.; Tohme, S.; et al. Hepatic resection for hepatocellular carcinoma in nonalcoholic fatty liver disease: A systematic review and meta-analysis of 7226 patients. Ann. Surg. 2021, 2, e065. [Google Scholar] [CrossRef]
- Ghidini, M.; Ramai, D.; Facciorusso, A.; Singh, J.; Tai, W.; Rijavec, E.; Galassi, B.; Grossi, F.; Indini, A. Metabolic disorders and the risk of cholangiocarcinoma. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 999–1007. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Aby, E.S.; Ghoz, H.; Cheungpasitporn, W.; Lukens, F.J.; Harnois, D.M.; Ungprasert, P. Statins and Risk of Cholangiocarcinoma: A Systematic Review and Meta-analysis. J. Gastrointestin. Liver Dis. 2020, 29, 629–635. [Google Scholar] [CrossRef] [PubMed]
- Surapaneni, P.K.; Li, Z.; Vemireddy, L.P.; Kasi, P.M.; Starr, J.S.; Ritter, A.; McMillan, J.; Wylie, N.; Mody, K. Impact of obesity upon the survival of cholangiocarcinoma patients. J. Clin. Oncol. 2019, 37 (Suppl. 4), 288. [Google Scholar] [CrossRef]
- De Lorenzo, S.; Tovoli, F.; Mazzotta, A.; Vasuri, F.; Edeline, J.; Malvi, D.; Boudjema, K.; Renzulli, M.; Jeddou, H.; D’Errico, A.; et al. Non-Alcoholic Steatohepatitis as a Risk Factor for Intrahepatic Cholangiocarcinoma and Its Prognostic Role. Cancers 2020, 12, 3182. [Google Scholar] [CrossRef] [PubMed]
- Da Fonseca, L.G.; Izquierdo-Sanchez, L.; Hashizume, P.H.; Beca, E.L.; Carlino, Y.; Carrera, E.; Arrese, M.; Ferrer, J.D.; Balderramo, D.; Carrilho, F.J.; et al. P-10 Latin american registry of cholangiocarcinoma: Clinical features, management and outcomes. Ann. Hepatol. 2021, 24, 100376. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | Metabolic Disorder Group | Non-Metabolic-Disorder Group | p Value |
|---|---|---|---|---|
| n (%) | 122 | 52 (42.6%) | 70 (57.4%) | |
| Median age, years (IQR) | 62 (55–67) | 64 (56–68.5) | 59 (53–64) | 0.199 |
| Gender | 0.048 | |||
| Woman, n (%) | 72 (59.0%) | 36 (69.2%) | 36 (51.4%) | |
| Man, n (%) | 50 (40.9%) | 16 (30.8%) | 34 (48.6%) | |
| Conditions | ||||
| Weight, kilograms (IQR) | 59 (51.7–68) | 67.5 (59.9–79) | 55 (48–59) | <0.0001 |
| Height, centimeters (IQR) | 159 (153–166) | 157.5 (152.5–164.5) | 160 (154–168) | 0.1991 |
| BMI, kg/m2 (IQR) | 23 (20–26) | 26 (24.5–29.5) | 21 (18–23) | <0.0001 |
| Smoking, n (%) | 54 (44.3%) | 13 (25%) | 41 (58.6%) | <0.0001 |
| Alcohol, n (%) | 20 (16.4%) | 6 (11.6%) | 14 (20%) | 0.212 |
| PSC, n (%) | 2 (1.7%) | 0 (0%) | 2 (2.9%) | 0.219 |
| Cholelithiasis, n (%) | 11 (9.0%) | 4 (7.7%) | 7 (10%) | 0.354 |
| Cirrhosis, n (%) | 1 (0.8%) | 0 (0%) | 1 (1.4%) | 0.387 |
| Viral hepatitis | 4 (3.2%) | 2 (3.8%) | 2 (2.9%) | 0.742 |
| HIV | 2 (1.6%) | 0 (0%) | 2 (2.9%) | 0.219 |
| Primary site | 0.691 | |||
| Intrahepatic | 48 (39.3%) | 18 (34.6%) | 30 (42.9%) | |
| Perihilar | 30 (24.6%) | 13 (25%) | 17 (24.3%) | |
| Distal | 41 (33.6%) | 19 (36.5%) | 22 (31.4%) | |
| Undefined | 3 (2.5%) | 2 (3.9%) | 1 (1.4%) | |
| Performance status | 0.636 | |||
| 0–1, n (%) | 84 (68.9) | 37 (71.1%) | 47 (67.1%) | |
| 2–4, n (%) | 38 (31.1%) | 15 (28.9%) | 23 (32.9%) | |
| Number of liver nodules | 0.124 | |||
| Unicentric, n (%) | 73 (59.9%) | 37 (71.2%) | 36 (51.4%) | |
| Multicentric, n (%) | 44 (36.1%) | 13 (25%) | 31 (44.3%) | |
| Non-Applicable, n (%) | 5 (4.1%) | 2 (3.9%) | 3 (4.3%) | |
| Vascular invasion, n (%) | 44 (36.1%) | 17 (32.7%) | 27 (38.6%) | 0.576 |
| Clinical positive node, n (%) | 55 (45.1%) | 26 (50%) | 29 (41.4%) | 0.178 |
| Distant metastasis, n (%) | 61 (50%) | 25 (48.1%) | 36 (51.4%) | 0.595 |
| Tumor status (pT and/or cT) | 0.100 | |||
| T1, n (%) | 9 (7.4%) | 7 (13.5%) | 2 (2.9%) | |
| T2, n (%) | 39 (32.0%) | 21 (40.4%) | 18 (25.7%) | |
| T3, n (%) | 42 (34.4%) | 14 (26.9%) | 28 (40%) | |
| T4, n (%) | 25 (20.4%) | 7 (13.5%) | 18 (25.7%) | |
| Tx, n (%) | 7 (5.7%) | 3 (5.8%) | 4 (5.7%) | |
| Nodal status (pN or cN) | 0.541 | |||
| N0, n (%) | 51 (41.8%) | 18 (34.6%) | 33 (47.1%) | |
| N1, n (%) | 53 (43.4%) | 24 (46.2%) | 29 (41.4%) | |
| N2, n (%) | 4 (3.3%) | 3 (5.8%) | 1 (1.4%) | |
| Nx, n (%) | 14 (11.5%) | 7 (13.5%) | 7 (10%) | |
| Metastasis (cM and/or pM) | 0.768 | |||
| M0, n (%) | 57 (46.7%) | 27 (51.9%) | 30 (42.9%) | |
| M1, n (%) | 65 (53.8%) | 25 (48.1%) | 40 (57.1%) | |
| Growth pattern | 0.174 | |||
| Mass Forming, n (%) | 72 (59.0%) | 27 (51.9%) | 45 (64.3%) | |
| Periductal infiltrating, n (%) | 23 (18.9%) | 10 (19.2%) | 13 (18.6%) | |
| Intraductular growth, n (%) | 6 (4.9%) | 1 (1.9%) | 5 (7.1%) | |
| Not available, n (%) | 22 (18.0%) | 15 (28.5%) | 7 (10.0%) | |
| Laboratory | ||||
| AST, U/L median (IQR) | 44.5 (29–76) | 43.5 (24.7–57.2) | 46 (32–75.5) | 0.848 |
| ALT, U/L median (IQR) | 44 (30–68) | 45 (29–74) | 44.5 (30–76.8) | 0.202 |
| ALP, U/L median (IQR) | 272 (141–569) | 226 (143–429) | 289 (134.5–588) | 0.189 |
| GGT, U/L median (IQR) | 423 (158–752) | 413 (132.7–630.5) | 423 (165–793) | 0.098 |
| Bilirubin, mg/dL median (IQR) | 1.03 (0.45–4.50) | 0.98 (0.43–4.01) | 1.25 (0.45–4.48) | 0.707 |
| Cholesterol, mg/dL median (IQR) | 148 (132–201) | 201 (181–213) | 141 (130–143.5) | 0.404 |
| LDL, mg/dL median (IQR) | 93 (94–129) | 127 (109–140) | 87 (74–91) | 0.383 |
| TG mg/dL, median (IQR) | 118.5 (92–188) | 132 (112–199) | 92 (71–114) | 0.777 |
| AFP, ng/mL median (IQR) | 3.1 (2–5.7) | 3 (2.2–4.0) | 3.35 (2.05–5.37) | 0.157 |
| CEA, ng/L median (IQR) | 3.61 (2.08–14.5) | 3.62 (2.05–12.87) | 3.65 (2.1–16.87) | 0.223 |
| CA19.9, ng/L median (IQR) | 145 (35.6–614) | 112.45 (38.82–461.75) | 151.85 (26.64–675.2) | 0.855 |
| Glucose, mg/dL median (IQR) | 104 (100–106) | 111 (98.5–125) | 95 (83–107.5) | 0.542 |
| Albumin, g/dL median (IQR) | 3.6 (3.3–4.1) | 3.5 (3.1–4.1) | 3.7 (3.3–4.1) | 0.164 |
| Neutrophils, /mm3 median (IQR) | 6620 (5800–7400) | 6600 (5800–7400) | 6700 (5700–7405) | 0.621 |
| Lymphocytes, /mm3 median (IQR) | 2100 (1400–2950) | 2300 (1500–3020) | 1900 (1395–2950) | 0.701 |
| Hemoglobin, g/dL median (IQR) | 11.9 (10.8–12.9) | 12.05 (11.0–13.07) | 11.6 (10.4–12.7) | 0.456 |
| Platelets, 103 median (IQR) | 270 (201–351) | 279 (185–347) | 266 (212–354) | 0.173 |
| INR, median (IQR) | 1.15 (1.05–1.26) | 1.13 (1.05–1.24) | 1.16 (1.05–1.28) | 0.576 |
| Therapeutic management | ||||
| Curative intent resection, n (%) | 29 (23.8%) | 15 (28.8%) | 14 (20%) | 0.256 |
| Recurrence after surgery, n (%) | 21 (17.2%) | 8 (15.4%) | 13 (18.6%) | 0.039 |
| Chemotherapy, n (%) | 104 (85.2%) | 45 (76.9%) | 59 (84.3%) | 0.256 |
| Best supportive care, n (%) | 11 (9%) | 1 (1.9%) | 10 (14.3%) | 0.018 |
| Biliary stent, n (%) | 66 (54.1%) | 25 (48.1%) | 41 (58.6%) | 0.25 |
| Biliary drainage, n (%) | 19 (15.5%) | 9 (17.3%) | 10 (14.3%) | 0.328 |
| Subgroups (n) | n | Median Overall Survival (95% CI) | Univariate p | HR (95% CI) Multivariate, p Value |
|---|---|---|---|---|
| Man | 50 | 11.5 (8.6–20.6) | 0.88 | |
| Woman | 72 | 14.6 (9.4–17.4) | ||
| Obesity | 13 | 15.5 (5.8–NR) | 0.77 | |
| No obesity | 109 | 13.4 (9.6–17.3) | ||
| Diabetes | 24 | 22.8 (5.8–38.2) | 0.04 | 0.54 (0.25–1.15), p = 0.111 |
| No diabetes | 98 | 11.9 (9.4–15.5) | ||
| Smoking | 54 | 10.1 (7.4–15.3) | 0.17 | |
| No smoking | 68 | 16.5 (11.1–21.8) | ||
| Alcohol | 20 | 16.2 (5.7–22.4) | 0.93 | |
| No alcohol | 102 | 14.0 (9.6–17.3) | ||
| Undefined primary site | 3 | 3.5 (3.5–NR) | 0.539 | |
| Distal | 41 | 20.6 (14.8–25.3) | ||
| Intrahepatic | 48 | 10.5 (7.4–14.6) | ||
| Perihilar | 30 | 8.9 (5.4–26.7) | ||
| PS0 | 42 | 16.8 (14.2–29.2) | <0.001 | 1.86 (1.43–2.41), p < 0.0001 |
| PS1 | 42 | 13.4 (9.4–20.6) | ||
| PS2 | 25 | 11.1 (5.5–22.0) | ||
| PS3 | 12 | 3.0 (2.1–5.4) | ||
| PS4 | 1 | NR (NR–NR) | ||
| Vascular invasion | 44 | 5.9 (4.5–11.4) | 0.0012 | 1.61 (1.01–2.58), p = 0.048 |
| No vascular invasion | 74 | 16.5 (11.9–22.4) | ||
| Node positive | 55 | 8.9 (5.8–15.3) | 0.14 | |
| Node negative | 62 | 16.5 (10.9–26.9) | ||
| Metastasis | 61 | 8.9 (5.4–14.0) | 0.001 | 1.47 (0.91–2.41), p = 0.118 |
| No metastasis | 59 | 21.8 (13.4–26.9) | ||
| Biliary stent | 66 | 13.4 (7.2–17.3) | 0.07 | |
| No biliary stent | 56 | 15.5 (9.6–25.3) | ||
| Resection | 29 | 34.2 (22.0–43.5) | <0.0001 | 0.42 (0.21–0.86), p = 0.018 |
| No resection | 93 | 10.5 (7.5–14.0) | ||
| Family history of neoplasia | 50 | 20.7 (11.9–25.2) | 0.11 | |
| No family history of neoplasia | 67 | 11.5 (7.7–16.2) | ||
| CA19.9 < 150 U/mL | 64 | 17.5 (11.5–22.4) | 0.0003 | 1.47 (0.91–2.36), p = 0.112 |
| CA19.9 ≥ 150 U/mL | 58 | 8.1 (5.7–14.3) | ||
| Metabolic disorder group | 52 | 15.5 (10.9–33.9) | 0.048 | 1.09 (0.62–1.94), p = 0.745 |
| Non-metabolic-disorder group | 70 | 11.5 (8.4–16.5) |
| Overall Survival | n | Median (95% CI) |
| Total cohort, months (95% CI) | 122 | 14.3 months (10.1–17.3) |
| Treated with surgery, months (95% CI) | 8 | 35.5 months (35–NR) |
| Treated with surgery plus CT at recurrence, months (95% CI) | 21 | 26.9 months (17.3–43.5) |
| Treated with chemotherapy only, months (95% CI) | 82 | 11.5 months (8.4–14.8) |
| Best supportive care only, months (95% CI) | 11 | 3.5 months (0.2–5.3) |
| “Non-metabolic group” treated with surgery, months (95% CI) | 14 | 21.8 months (95% CI 8.6–26.9) |
| “Metabolic group” treated with surgery, months (95% CI) | 15 | 43.4 months (95% CI 33.9–NR) |
| “Non-metabolic group” treated with chemotherapy, months (95% CI) | 46 | 11.5 months (95% CI 6.7–16.2) |
| “Metabolic group” treated with chemotherapy, months (95% CI) | 36 | 11.5 months (95% CI 5.8–15.3) |
| Progression-Free Survival (PFS) | n | Median (95% CI) |
| PFS to first-line chemotherapy, months (95% CI) | 82 | 4.3 months (3.5–5.1) |
| PFS to first-line chemotherapy “metabolic group”, months (95% CI) | 36 | 5.8 months (3.8–8) |
| PFS to first-line chemotherapy “non-metabolic group”, months (95% CI) | 46 | 4.2 months (2.6–4.7) |
| Recurrence-Free Survival after Surgery (RFS) | n | Median (95% CI) |
| RFS after surgery, months (95% CI) | 21 | 14 months (8.2–19.8) |
| RFS after surgery “metabolic group”, months (95% CI) | 8 | 15.6 months (8.2–24.6) |
| RFS after surgery “non-metabolic group”, months (95% CI) | 13 | 13.5 months (3.5–19.8) |
| Survival according to Radiologic Response | n | Median (95% CI) |
| Partial response, months (95% CI) | 28 | 17.4 months (14.6–38.21) |
| Stable disease, months (95% CI) | 39 | 20.5 months (11.9–22.8) |
| Progressive disease, months (95% CI) | 30 | 7.4 months (5.4–9.6) |
| No assessment, months (95% CI) | 7 | 2.8 months (1.6–4.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Da Fonseca, L.G.; Hashizume, P.H.; de Oliveira, I.S.; Izquierdo-Sanchez, L.; Saud, L.R.d.C.; Xerfan, M.P.; Alves, V.A.F.; de Mello, E.S.; Herman, P.; Banales, J.M.; et al. Association between Metabolic Disorders and Cholangiocarcinoma: Impact of a Postulated Risk Factor with Rising Incidence. Cancers 2022, 14, 3483. https://doi.org/10.3390/cancers14143483
Da Fonseca LG, Hashizume PH, de Oliveira IS, Izquierdo-Sanchez L, Saud LRdC, Xerfan MP, Alves VAF, de Mello ES, Herman P, Banales JM, et al. Association between Metabolic Disorders and Cholangiocarcinoma: Impact of a Postulated Risk Factor with Rising Incidence. Cancers. 2022; 14(14):3483. https://doi.org/10.3390/cancers14143483
Chicago/Turabian StyleDa Fonseca, Leonardo G., Pedro H. Hashizume, Irai Santana de Oliveira, Laura Izquierdo-Sanchez, Lisa Rodrigues da Cunha Saud, Mariana Pinheiro Xerfan, Venancio Avancini Ferreira Alves, Evandro Sobroza de Mello, Paulo Herman, Jesus M. Banales, and et al. 2022. "Association between Metabolic Disorders and Cholangiocarcinoma: Impact of a Postulated Risk Factor with Rising Incidence" Cancers 14, no. 14: 3483. https://doi.org/10.3390/cancers14143483