Recurrence of Uterine Smooth Muscle Tumor of Uncertain Malignant Potential: A Systematic Review of the Literature

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
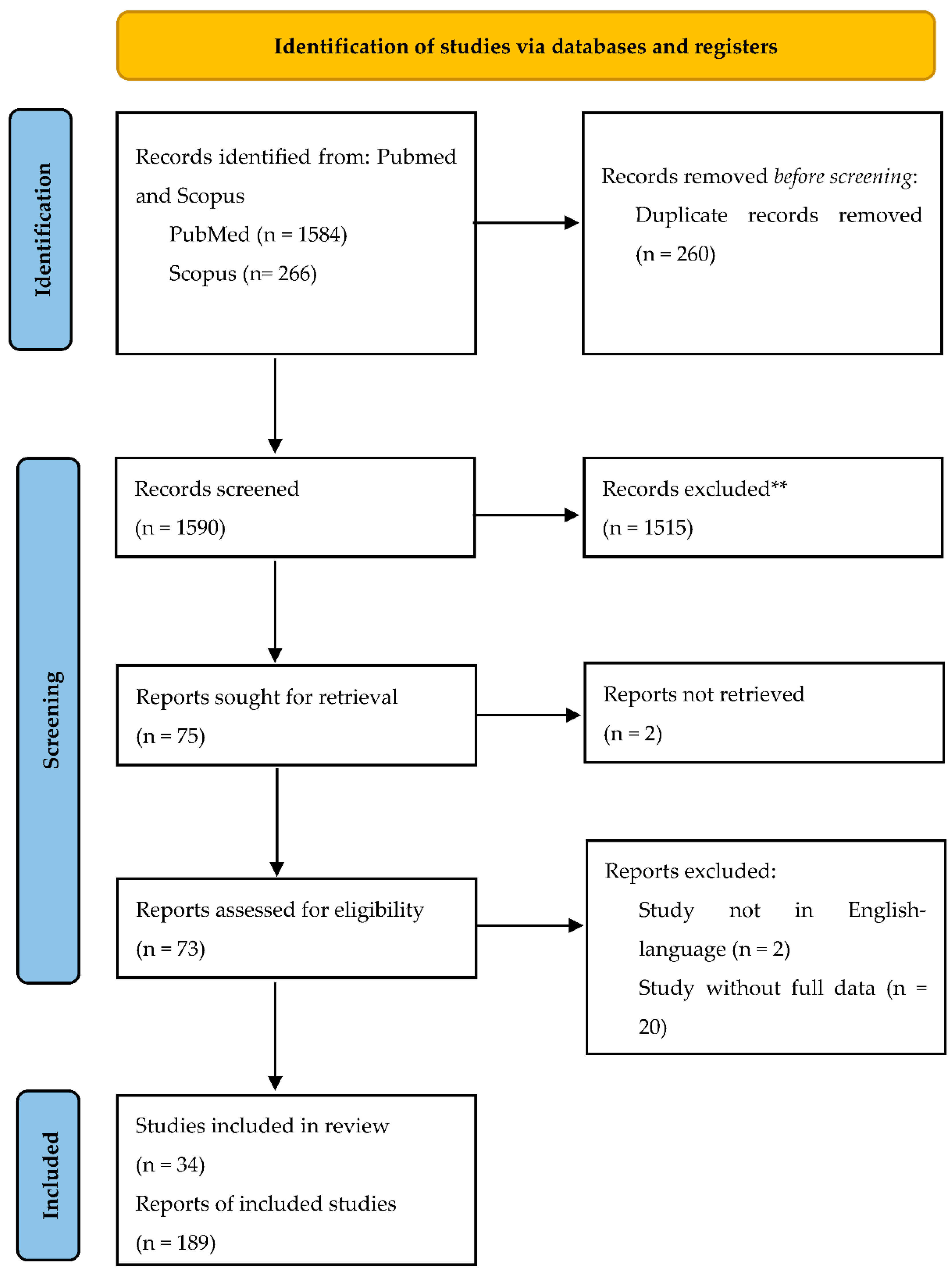
2. Materials and Methods
- Population: women diagnosed with STUMP.
- Intervention: surgical intervention (myomectomy or hysterectomy) performed for uterine mass or related symptoms.
- Comparison: patients with recurrence of disease and without recurrence.
- Outcomes: (1) descriptive analysis of patient characteristics, also evaluating the features associated with the risk of relapse, (2) distribution of the recurrence rate over time, (3) follow-up outcomes when available.
3. Results
3.1. Literature Review Details
3.2. Patient Characteristics
3.3. STUMP Lesion Characteristics
3.4. Treatment
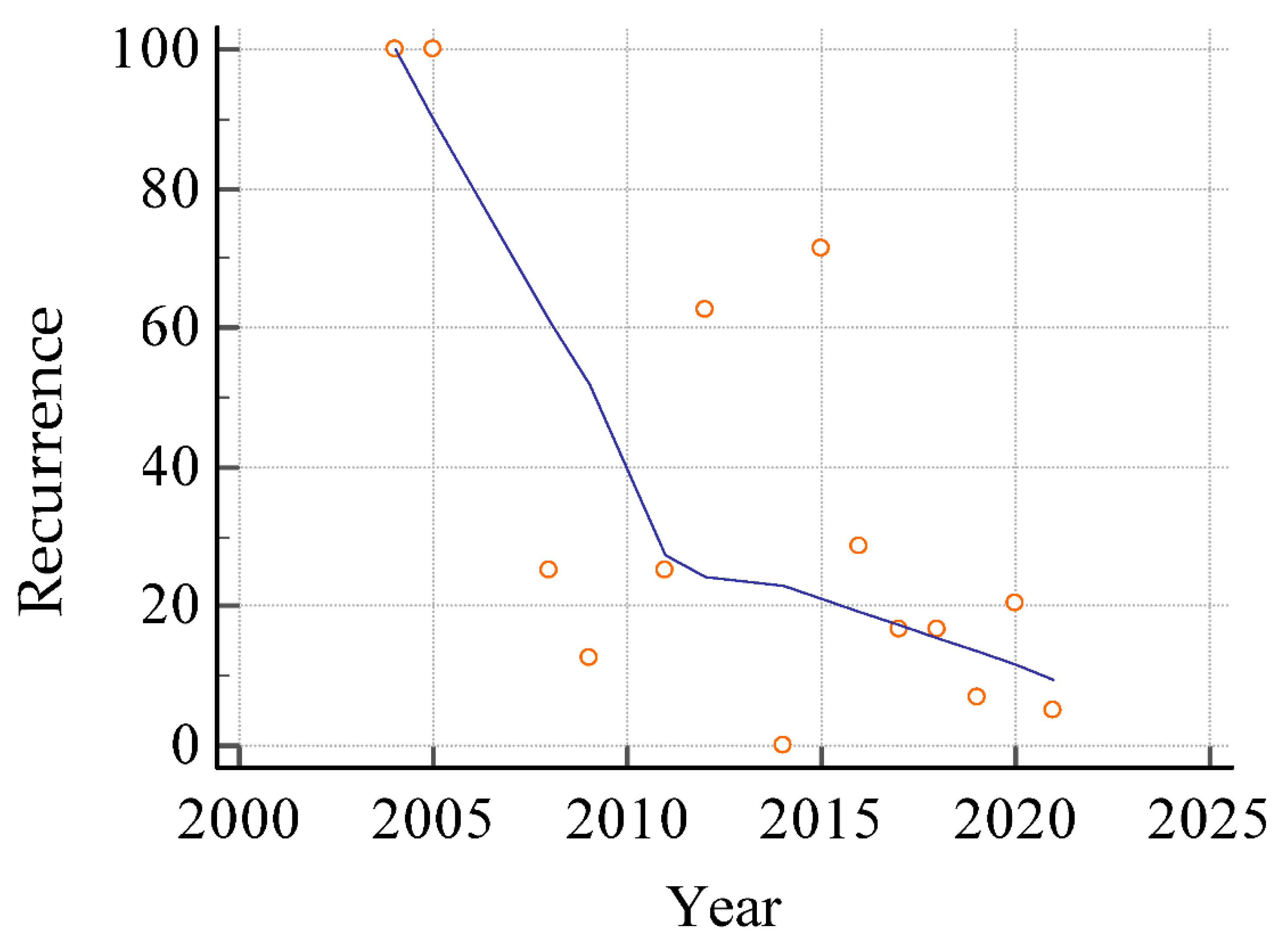
3.5. Recurrence
3.6. Missing Data
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Chapman, L.; Magos, A. Surgical and radiological management of uterine fibroids in the UK. Curr. Opin. Obstet. Gynecol. 2006, 18, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Ciarmela, P.; Delli Carpini, G.; Greco, S.; Zannotti, A.; Montik, N.; Giannella, L.; Giuliani, L.; Grelloni, C.; Panfoli, F.; Paolucci, M.; et al. Uterine fibroid vascularization: From morphological evidence to clinical implications. Reprod. Biomed. Online 2022, 44, 281–294. [Google Scholar] [CrossRef] [PubMed]
- Nieboer, T.E.; Johnson, N.; Lethaby, A.; Tavender, E.; Curr, E.; Garry, R.; van Voorst, S.; Mol, B.W.; Kluivers, K.B. Surgical approach to hysterectomy for benign gynaecological disease. Cochrane Data-Base Syst Rev. 2009, 3, CD003677. [Google Scholar]
- Sizzi, O.; Rossetti, A.; Malzoni, M.; Minelli, L.; La Grotta, F.; Soranna, L.; Panunzi, S.; Spagnolo, R.; Imperato, F.; Landi, S.; et al. Italian multicenter study on complications of laparoscopic myomectomy. J. Minim. Invasive Gynecol. 2007, 14, 453–462. [Google Scholar] [CrossRef] [PubMed]
- Theben, J.U.; Schellong, A.R.M.; Altgassen, C.; Kelling, K.; Schneider, S.; Große-Drieling, D. Unexpected malignancies after laparoscopic-assisted supracervical hysterectomies (LASH): An analysis of 1,584 LASH cases. Arch. Gynecol. Obstet. 2013, 287, 455–462. [Google Scholar] [CrossRef]
- Parker, W.H.; Fu, Y.S.; Berek, J.S. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet. Gynecol. 1994, 83, 414–418. [Google Scholar]
- Seidman, M.A.; Oduyebo, T.; Muto, M.G.; Crum, C.P.; Nucci, M.R.; Quade, B.J. Peritoneal dissemination complicating morcellation of uterine mesenchymal neoplasms. PLoS ONE 2012, 7, e50058. [Google Scholar] [CrossRef]
- Brooks, S.E.; Zhan, M.; Cote, T.; Baquet, C.R. Surveillance, epidemiology, and end results analysis of 2677 cases of uterine sarcoma 1989 to 1999. Gyn. Oncol. 2004, 93, 204–208. [Google Scholar] [CrossRef]
- Park, J.Y.; Park, S.K.; Kim, D.Y.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Nam, J.H. The impact of tumor morcellation during surgery on the prognosis of patients with apparently early uterine leiomyosarcoma. Gynecol. Oncol. 2011, 122, 255–259. [Google Scholar] [CrossRef]
- Einstein, M.H.; Barakat, R.R.; Chi, D.S.; Sonoda, Y.; Alektiar, K.M.; Hensley, M.L.; Abu-Rustum, N.R. Management of uterine malignancy found incidentally after supracervical hysterectomy or uterine morcellation for presumed benign disease. Int. J. Gynecol. Cancer. 2008, 18, 1065–1070. [Google Scholar] [CrossRef]
- Oduyebo, T.; Rauh-Hain, A.J.; Meserve, E.E.; Seidman, M.A.; Hinchcliff, E.; George, S.; Quade, B.; Nucci, M.R.; Del Carmen, M.G.; Muto, M.G. The value of re-exploration in patients with inadvertently morcellated uterine sarcoma. Gynecol. Oncol. 2014, 132, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Hagemann, I.S.; Hagemann, A.R.; LiVolsi, V.A.; Montone, K.T.; Chu, C.S. Risk of occult malignancy in morcellated hysterectomy: A case series. Int. J. Gynecol. Pathol. 2011, 30, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.; Falcone, T. Tissue extraction by morcellation: A clinical dilemma. J. Minim. Invasive Gynecol. 2014, 21, 319–320. [Google Scholar] [CrossRef]
- UPDATED Laparoscopic Uterine Power Morcellation in Hysterectomy and Myomectomy: FDA Safety Communication. Available online: http://wayback.archive-it.org/7993/20170722215727/https://www.fda.gov/MedicalDevices/Safety/AlertsandNotices/ucm424443.htm (accessed on 1 February 2022).
- Stephenson, J. FDA warns against procedure used in removing fibroids. JAMA 2014, 311, 1956. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Barysauskas, C.; Serrano, C.; Oduyebo, T.; Rauh-Hain, J.A.; Del Carmen, M.G.; Demetri, G.D.; Muto, M.G. Retrospective cohort study evaluating the impact of intraperitoneal morcellation on outcomes of localized uterine leiomyosarcoma. Cancer 2014, 120, 3154–3158. [Google Scholar] [CrossRef]
- Wu, T.I.; Yen, T.C.; Lai, C.H. Clinical presentation and diagnosis of uterine sarcoma, including imaging. Best Pract. Res. Clin. Obstet. Gynaecol. 2011, 25, 681–689. [Google Scholar] [CrossRef]
- Exacoustos, C.; Romanini, M.E.; Amadio, A.; Amoroso, C.; Szabolcs, B.; Zupi, E.; Arduini, D. Can gray-scale and color Doppler sonography differentiate between uterine leiomyosarcoma and leiomyoma? J. Clin. Ultrasound. 2007, 35, 449–457. [Google Scholar] [CrossRef]
- Rha, S.E.; Byun, J.Y.; Jung, S.E.; Lee, S.L.; Cho, S.M.; Hwang, S.S.; Lee, H.G.; Namkoong, S.E.; Lee, J.M. CT and MRI of uterine sarcomas and their mimickers. AJR Am. J. Roentgenol. 2003, 181, 1369–1374. [Google Scholar] [CrossRef]
- Vellone, V.G.; Sala, P.; Abete, L.; Sarocchi, F.; Parodi, L.; Menada, M.V.; Fulcheri, E. High cellularity and mitotic activity in a primary ovarian fibro-thecomatous tumor of a young patient: A diagnostic and clinical challenge. Eur. J. Gynaecol. Oncol. 2017, 38, 294–295. [Google Scholar]
- Sato, K.; Yuasa, N.; Fujita, M.; Fukushima, Y. Clinical application of diffusion-weighted imaging for preoperative differentiation between uterine leiomyoma and leiomyosarcoma. Am. J. Obstet. Gynecol. 2014, 210, 368.e1–368.e8. [Google Scholar] [CrossRef]
- Kurman, R.; Carcangiu, M.; Herrington, C.; Young, R.H. World Health Organisation Classification of Tumors of Female Reproductive Organs, 4th ed.; Int Agency Res Cancer Press: Lyon, France, 2014. [Google Scholar]
- Shim, J.I.; Han, A.K.W.; Jeon, H.J.; Kim, M.L.; Jung, Y.W.; Yun, B.S.; Seong, S.J.; Shin, E.; Cho, Y.J.; Rha, S.H. Clinical experience of uterine smooth muscle tumor of uncertain malignant potential in two gynecological centers: Oncological and obstetrical aspects. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Prisma Transparent Reporting of Systematic Reviews and Meta-Analyses. Available online: http://www.prisma-statement.org/ (accessed on 24 January 2022).
- Bell, S.W.; Kempson, R.L.; Hendrickson, M.R. Problematic uterine smooth muscle neoplasms: A clinicopathologic study of 213 cases. Am. J. Surg. Pathol. 1994, 18, 535–558. [Google Scholar] [CrossRef]
- Hendrickson, M.R.; Tavassoli, F.A.; Kempson, R.L. Mesenchymal tumours and related lesions. In World Health Organization Classification of Tumours: Pathology and Genetics of Tumours of the Breast and Female Genital Organs; Tavassoli, F.A., Devilee, P., Eds.; IARC Press: Lyon, France, 2003; pp. 236–243. [Google Scholar]
- Ning, C.; Zhang, L.; Zhao, C.; Chen, X.; Liu, X.; Gu, C. Clinical and reproductive outcomes of uterine smooth muscle tumor of uncertain malignant potential: A single-center retrospective study. J. Int. Med. Res. 2021, 49, 3000605211008065. [Google Scholar] [CrossRef] [PubMed]
- Akad, F.; Filip, B.; Mocanu, V.; Akad, M.; Acatrinei, C.; Scripcariu, V. Rare Case of Smooth Muscle Tumor of Uncertain Malignant Potential—Clinical Case. Maedica 2021, 16, 302–306. [Google Scholar] [PubMed]
- Yadav, G.; Rao, M.; Goyal, S.B.; Singh, P.; Kathuria, P.; Gothwal, M. Risk of incidental genital tract malignancies at the time of myomectomy and hysterectomy for benign conditions. Obstet. Gynecol. Sci. 2021, 64, 209–215. [Google Scholar] [CrossRef]
- Jang, T.K.; Kwon, S.H.; Cho, C.H.; Lee, H.W.; Shin, S.J. Giant uterine mass with uterine smooth muscle tumor of uncertain malignant potential: A case report. Gynecol. Oncol. Rep. 2020, 34, 100663. [Google Scholar] [CrossRef]
- Han, A.K.W.; Hong, K.; Kim, M.; Kim, M.K.; Kim, M.L.; Jung, Y.W.; Yun, B.S.; Seong, S.J. Unexpected uterine smooth muscle tumor of uncertain malignant potential and sarcoma: A single center cohort study in South Korea. Taiwan J. Obstet. Gynecol. 2020, 59, 275–281. [Google Scholar] [CrossRef]
- Zheng, Y.Y.; Liu, X.B.; Mao, Y.Y.; Lin, M.H. Smooth muscle tumor of uncertain malignant potential (STUMP): A clinicopathologic analysis of 26 cases. Int. J. Clin. Exp. Pathol. 2020, 13, 818–826. [Google Scholar] [PubMed]
- García-Sánchez, J.M.; Bauza, M.; Pérez-García, A.; Mayordomo Aranda, E.; Ruiz Valls, A. Secondary Leiomyosarcoma of the Lower Limb Following Uterine Smooth Muscle Tumor of Uncertain Malignant Potential. Clin. Med. Insights Case Rep. 2019, 12, 1179547619857680. [Google Scholar] [CrossRef]
- Karataşlı, V.; Çakır, İ.; Ayaz, D.; Budak, A.; Sancı, M. Clinicopathologic evaluation of uterine smooth muscle tumors of uncertain malignant potential (STUMP): A single center experience. J. Gynecol. Obstet. Hum. Reprod. 2019, 48, 637–642. [Google Scholar] [CrossRef]
- Ha, H.I.; Choi, M.C.; Heo, J.H.; Kim, K.A.; Jung, S.G.; Park, H.; Joo, W.D.; Song, S.H.; Kim, T.H.; Lee, C. A clinicopathologic review and obstetric outcome of uterine smooth muscle tumor of uncertain malignant potential (STUMP) in a single institution. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Hughes, L.; Roex, A.; Parange, A. STUMP, a surprise finding in a large fibroid uterus in a 20-year-old woman. Int. J. Womens Health 2018, 10, 211–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oda, H.; Hirakawa, H. Spontaneous rupture of uterine smooth muscle tumour presenting acute abdominal pain and haemoperitoneum. BMJ Case Rep. 2018, 2018, bcr2017222806. [Google Scholar] [CrossRef] [PubMed]
- Basaran, D.; Usubutun, A.; Salman, M.C.; Narin, M.A.; Boyraz, G.; Turkmen, O.; Kimyon, G.C.; Karalok, A.; Bulbul, D.; Turan, T.; et al. The Clinicopathological Study of 21 Cases with Uterine Smooth Muscle Tumors of Uncertain Malignant Potential: Centralized Review Can Purify the Diagnosis. Int. J. Gynecol. Cancer 2018, 28, 233–240. [Google Scholar] [CrossRef]
- Bacanakgil, B.H.; Deveci, M.; Karabuk, E.; Soyman, Z. Uterine Smooth Muscle Tumor of Uncertain Malignant Potential: Clinicopathologic-Sonographic Characteristics, Follow-Up and Recurrence. World J. Oncol. 2017, 8, 76–80. [Google Scholar] [CrossRef] [Green Version]
- Bogani, G.; Ditto, A.; Martinelli, F.; Signorelli, M.; Chiappa, V.; Lorusso, D.; Sabatucci, I.; Carcangiu, M.L.; Fiore, M.; Gronchi, A.; et al. Morcellator’s Port-site Metastasis of a Uterine Smooth Muscle Tumor of Uncertain Malignant Potential after Minimally Invasive Myomectomy. J. Minim. Invasive Gynecol. 2016, 23, 647–649. [Google Scholar] [CrossRef]
- Sakuragi, Y.; Inoue, A.; Mashima, E.; Yamaguchi, T.; Sasaki, N.; Hara, Y.; Omoto, D.; Ohmori, S.; Haruyama, S.; Sawada, Y.; et al. Dome-shaped metastatic lesion on the scalp from a uterine smooth muscle tumor of uncertain malignant potential (STUMP). Eur. J. Dermatol. 2016, 26, 193–194. [Google Scholar] [CrossRef]
- Kalogiannidis, I.; Stavrakis, T.; Dagklis, T.; Petousis, S.; Nikolaidou, C.; Venizelos, I.; Rousso, D. A clinicopathological study of atypical leiomyomas: Benign variant leiomyoma or smooth-muscle tumor of uncertain malignant potential. Oncol. Lett. 2016, 11, 1425–1428. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.E.; Knudtson, J.F.; Valente, P.T.; Robinson, R.D.; Kost, E.R. Successful pregnancy following myomectomy for uterine smooth muscle tumor of uncertain malignant potential: A case report and review of the literature. Gynecol. Oncol. Rep. 2015, 15, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Mowers, E.L.; Skinner, B.; McLean, K.; Reynolds, R.K. Effects of morcellation of uterine smooth muscle tumor of uncertain malignant potential and endometrial stromal sarcoma: Case series and recommendations for clinical practice. J. Minim. Invasive Gynecol. 2015, 22, 601–606. [Google Scholar] [CrossRef]
- Zhang, R.; Tian, X.; Qin, L.; Lu, D.; Shen, J. High 18F-FDG uptake for uterine smooth muscle tumor of uncertain malignant potential. Clin. Nucl. Med. 2015, 40, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Dall’Asta, A.; Gizzo, S.; Musarò, A.; Quaranta, M.; Noventa, M.; Migliavacca, C.; Sozzi, G.; Monica, M.; Mautone, D.; Berretta, R. Uterine smooth muscle tumors of uncertain malignant potential (STUMP): Pathology, follow-up and recurrence. Int. J. Clin. Exp. Pathol. 2014, 7, 8136–8142. [Google Scholar] [PubMed]
- Kotsopoulos, I.C.; Barbetakis, N.; Asteriou, C.; Voutsas, M.G. Uterine smooth muscle tumor of uncertain malignant potential: A rare cause of multiple pulmonary nodules. Indian J. Med. Paediatr. Oncol. 2012, 33, 176–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, J.; Collins, S.; Morosky, C.M. Periurethral smooth muscle tumor of undetermined malignant potential. Case Rep. Obstet. Gynecol. 2012, 2012, 546852. [Google Scholar] [CrossRef] [Green Version]
- Vilos, G.A.; Marks, J.; Ettler, H.C.; Vilos, A.G.; Prefontaine, M.; Abu-Rafea, B. Uterine smooth muscle tumors of uncertain malignant potential: Diagnostic challenges and therapeutic dilemmas. Report of 2 cases and review of the literature. J. Minim. Invasive Gynecol. 2012, 19, 288–295. [Google Scholar] [CrossRef]
- Canciani, G.N.; Burbos, N.; Duncan, T.J.; Lonsdale, R.; Nieto, J.J. Late presentation of metastatic smooth muscle neoplasm of the uterus with low malignant potential. J. Gynecol. Oncol. 2012, 23, 69–71. [Google Scholar] [CrossRef]
- Hong, I.K.; Kim, D.Y. F-18 FDG PET/CT of a uterine smooth-muscle tumor of unknown malignant potential. Clin. Nucl. Med. 2011, 36, 934–936, Erratum in Clin. Nucl. Med. 2011, 36, 1060. [Google Scholar] [CrossRef]
- Müller Vranjes, A.; Sijanović, S.; Vidosavljević, D.; Kasac, Z.; Abicic Zuljević, K. Surgical treatment of large smooth muscle tumor of uncertain malignant potential during pregnancy. Med. Glas. 2011, 8, 290–292. [Google Scholar]
- Gezginç, K.; Yazici, F.; Tavli, L. Uterine smooth muscle tumors of uncertain malignant potential: A case presentation. Int. J. Clin. Oncol. 2011, 16, 592–595. [Google Scholar] [CrossRef]
- Yoon, B.S.; Seong, S.J.; Park, H. Rapid recurrence of uterine smooth muscle tumor of uncertain malignant potential as leiomyosarcoma. Int. J. Gynaecol. Obstet. 2011, 113, 244–245. [Google Scholar] [CrossRef]
- Ip, P.P.; Cheung, A.N.; Clement, P.B. Uterine smooth muscle tumors of uncertain malignant potential (STUMP): A clinicopathologic analysis of 16 cases. Am. J. Surg. Pathol. 2009, 33, 992–1005. [Google Scholar] [CrossRef]
- Berretta, R.; Rolla, M.; Merisio, C.; Giordano, G.; Nardelli, G.B. Uterine smooth muscle tumor of uncertain malignant potential: A three-case report. Int. J. Gynecol. Cancer 2008, 18, 1121–1126. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.E.; Huang, S.C.; Lee, W.Y.; Hsu, K.F. Pseudo-Meigs’ syndrome caused by uterine smooth muscle tumor of uncertain malignant potential with low vascular endothelial growth factor expression. Int. J. Gynecol. Cancer 2008, 18, 851–853. [Google Scholar] [CrossRef] [PubMed]
- Amant, F.; Moerman, P.; Vergote, I. Report of an unusual problematic uterine smooth muscle neoplasm, emphasizing the prognostic importance of coagulative tumor cell necrosis. Int. J. Gynecol. Cancer 2005, 15, 1210–1212. [Google Scholar] [CrossRef]
- Shapiro, A.; Ferenczy, A.; Turcotte, R.; Bruchim, I.; Gotlieb, W.H. Uterine smooth-muscle tumor of uncertain malignant potential metastasizing to the humerus as a high-grade leiomyosarcoma. Gynecol. Oncol. 2004, 94, 818–820. [Google Scholar] [CrossRef]
- Ciavattini, A.; Di Giuseppe, J.; Stortoni, P.; Montik, N.; Giannubilo, S.R.; Litta, P.; Islam, M.S.; Tranquilli, A.L.; Reis, F.M.; Ciarmela, P. Uterine fibroids: Pathogenesis and interactions with endometrium and endomyometrial junction. Obstet. Gynecol. Int. 2013, 2013, 173184. [Google Scholar] [CrossRef] [PubMed]
- Gadducci, A.; Zannoni, G.F. Uterine smooth muscle tumors of unknown malignant potential: A challenging question. Gynecol. Oncol. 2019, 154, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, A.; Umesaki, N.; Li, L.; Tanaka, T. Use of 18F-fluorodeoxyglucose positron emission tomography for diagnosis of uterine sarcomas. Oncol. Rep. 2010, 23, 1069–1076. [Google Scholar] [PubMed] [Green Version]
- Kitajima, K.; Murakami, K.; Kaji, Y.; Sugimura, K. Spectrum of FDG PET/CT findings of uterine tumors. AJR Am. J. Roentgenol. 2010, 195, 737–743. [Google Scholar] [CrossRef]
- Ho, K.C.; Dean Fang, Y.H.; Lin, G.; Ueng, S.H.; Wu, T.I.; Lai, C.H.; Chueh, H.Y.; Chao, A.; Chang, T.C.; Yen, T.C. Presurgical Identification of Uterine Smooth Muscle Malignancies through the Characteristic FDG Uptake Pattern on PET Scans. Contrast. Media Mol. Imaging 2018, 2018, 7890241. [Google Scholar] [CrossRef] [Green Version]
- Guntupalli, S.R.; Ramirez, P.T.; Anderson, M.L.; Milam, M.R.; Bodurka, D.C.; Malpica, A. Uterine smooth muscle tumor of uncertain malignant potential: A retrospective analysis. Gynecol. Oncol. 2009, 113, 324–326. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Ricci, A.D.; Saponara, M.; DELeo, A.; Perrone, A.M.; DEIaco, P.; Pantaleo, M.A.; Nannini, M. Recurrent Uterine Smooth-Muscle Tumors of Uncertain Malignant Potential (STUMP): State of The Art. Anticancer Res. 2020, 40, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Cliby, W.A.; Aletti, G.D. Impact of morcellation on survival outcomes of patients with unexpected uterine leiomyosarcoma: A systematic review and meta-analysis. Gynecol. Oncol. 2015, 137, 167–172. [Google Scholar] [CrossRef]
- Chen, Q.; Shi, H.; Lu, W.; Lu, B. Unexpected uterine sarcomas in 4478 patients with electric power morcellation for leiomyomas. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 230, 85–89. [Google Scholar] [CrossRef]
- Kho, K.A.; Anderson, T.L.; Nezhat, C.H. Intracorporeal electromechanical tissue morcellation: A critical review and recommendations for clinical practice. Obstet. Gynecol. 2014, 124, 787–793. [Google Scholar] [CrossRef] [Green Version]
- Peeters, N.; Hulsbosch, S.; Ballaux, F.; Baekelandt, J. Uterine smooth muscle tumors of uncertain malignant potential: Analysis of diagnoses and therapies illustrated by two case reports. Eur. J. Gynaecol. Oncol. 2016, 37, 367–373. [Google Scholar]
- Macciò, A.; Chiappe, G.; Kotsonis, P.; Lavra, F.; Serra, M.; Demontis, R.; Madeddu, C. Abdominal leiomyosarcomatosis after surgery with external morcellation for occult smooth muscle tumors of uncertain malignant potential: A case report. Int. J. Surg. Case Rep. 2017, 38, 107–110. [Google Scholar] [CrossRef]
- Holger, M. WHO Classification of Tumours, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2020; Volume 4, pp. 279–280. [Google Scholar]
- Russo, C.; Camilli, S.; Martire, F.G.; Di Giovanni, A.; Lazzeri, L.; Malzoni, M.; Zupi, E.; Exacoustos, C. Highly vascularized uterine myomas (uterine smooth muscle tumors) on ultrasound and correlation to histopathology. Ultrasound Obstet. Gynecol. 2022; ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Sample Size (189) Available Data (%) |
|---|---|
| Age (years) (median, range) | 43 (18–75) |
| Nulligravid | 27/87 (31.0%) |
| Previous gynecological surgery (myomectomies) | 4/32 (12.5%) |
| Previous cesarean section | 4/25 (16.0%) |
| History of infertility | 4/59 (6.8%) |
| BMI > 30 kg/m2 | 13/31 (41.9%) |
| Initial symptoms (multiple choice) | |
| AUB | 41/151 (27.1%) |
| Menorrhagia | 28/151 (18.5%) |
| Dysmenorrhea | 4/151(2.6%) |
| Abdominal pain | 13/151 (8.6%) |
| Incidentally detected | 67/151 (44.4%) |
| Asthenia | 1/151 (0.7%) |
| Compression of adjacent organs | 7/151 (4.6%) |
| Initial signs (multiple choice) | |
| Anemia | 9/44 (20.4%) |
| Pelvic mass | 38/44 (86.4%) |
| CA125 levels < 35 U/L | 29/33 (87.9%) |
| Follow-up duration (months) (median, range) | 48 (1–288) |
| Characteristics | Sample Size (189) Available Data (%) |
|---|---|
| Diameter (cm) (median, range) | 8.0 (0.7–39.0) |
| STUMP localization | |
| Intramural | 65/172 (37.8%) |
| Subserosal | 18/172 (10.5%) |
| Submucosal | 12/172 (6.9%) |
| Intramural–Subserosal | 2/172 (1.2%) |
| Unknown | 75/172 (43.6%) |
| Mitosis | |
| 0–4 | 81/189 (42.9%) |
| 5–9 | 68/189 (36.0%) |
| ≥10 | 15/189 (7.9%) |
| Unknown | 25/189 (13.2%) |
| Atypia | |
| Severe | 38/189 (20.1%) |
| Mild | 53/189 (28.0%) |
| Moderate | 54/189 (28.6%) |
| None | 18/189 (9.5%) |
| Unknown | 26/189 (13.8%) |
| Necrosis | |
| Absent | 89/189 (47.1%) |
| Present | 73/189 (38.6%) |
| Unknown | 27/189 (14.3%) |
| Characteristics | Sample Size (189) Available Data (%) |
|---|---|
| Primary surgery | 189 cases |
| Myomectomy | 79/189 (41.8%) |
| Laparoscopic myomectomy | 27/79 (34.2%) |
| Laparotomic myomectomy | 28/79 (35.4%) |
| Hysteroscopic myomectomy | 1/79 (1.3%) |
| Unknown | 23/79 (29.1%) |
| TH | 50/189 (26.5%) |
| Laparoscopic TH | 12/50 (24%) |
| Laparotomic TH | 35/50 (70%) |
| Unknown | 3/50 (6%) |
| TH + BSO | 60/189 (31.7%) |
| Laparoscopic TH + BSO | 7/60 (11.7%) |
| Laparotomic TH + BSO | 40/60 (66.6%) |
| Unknown | 13/60 (21.7%) |
| Secondary surgery | Sample size (17/79) (21.5%) |
| TH | 8/17 (47%) |
| TH + BSO | 9/17 (53%) |
| Characteristics | Sample Size (37) Available Data (%) |
|---|---|
| Local recurrence | 23 cases (62.2%) |
| Uterus | 9/23 (39.1%) |
| Pelvis | 14/23 (60.9%) |
| Distant recurrence | 14 cases (37.8%) |
| Lung | 3/14 (21.4%) |
| Abdomen | 3/14 (21.4%) |
| Other organs | 2/14 (14.3%) |
| Missing data | 6/14 (42.9%) |
| Surgical treatment of recurrence | 37 cases |
| Debulking + chemotherapy | 2/37 (5.4%) |
| Hysterectomy | 7/37 (18.9%) |
| Mass excision | 17/37 (45.9%) |
| Myomectomy | 2/37 (5.4%) |
| TH + BSO | 4/37 (10.8%) |
| Unknown | 5/37 (13.6%) |
| Characteristics | Recurrence (37 Cases) Available Data (%) | No Recurrence (152 Cases) Available Data (%) | p | C.I. |
|---|---|---|---|---|
| Age (median, years) | 46.0 | 43.0 | 0.35 | - |
| Mean tumor size (cm) | 9.0 | 8.0 | 0.63 | - |
| Previous cesarean section | -/6 | 4/19 (21.0%) | 0.16 | - |
| Primary surgery | 37 cases | 152 cases | ||
| Myomectomy | 18/37 (48.7%) | 61/152 (40.1%) | 0.34 | - |
| TH | 10/37 (27.0%) | 40/152 (26.3%) | 0.93 | - |
| TH + BSO | 9/37 (24.3%) | 51/152 (33.6%) | 0.27 | - |
| Laparoscopy | 13/31 (41.9%) | 33/119 (27.7%) | 0.12 | - |
| Laparotomy | 17/31 (54.9%) | 86/119 (72.3%) | 0.06 | - |
| Hysteroscopy | 1/31 (3.2%) | - | - | - |
| Morcellation | 11/29 (37.9%) | 12/105 (11.4%) | 0.001 | 9.523–45.184 |
| Mitosis ≥ 10 | 2/26 (7.7%) | 13/138 (9.4%) | 0.78 | - |
| Atypia (severe) | 7/25 (28%) | 31/138 (22.5%) | 0.55 | - |
| Necrosis (present) | 16/25 (64%) | 80/137 (58.4%) | 0.60 | - |
| Secondary surgery | 3 /37 (8.1%) | 14/147 (9.5%) | 0.79 | - |
| Myomectomy | - | - | - | - |
| TH + BSO | 3/37 (8.1%) | 6/147 (4.1%) | 0.31 | - |
| TH | 0/32 | 8/147 (5.4%) | 0.18 | - |
| Outcomes | 2004–2013 (n: 34) (%) | 2014–2021 (n: 155) (%) | p | C.I. |
|---|---|---|---|---|
| Recurrence | 11 (32.3) | 26 (16.7) | 0.03 | 0.8053% to 33.1464% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Giuseppe, J.; Grelloni, C.; Giuliani, L.; Delli Carpini, G.; Giannella, L.; Ciavattini, A. Recurrence of Uterine Smooth Muscle Tumor of Uncertain Malignant Potential: A Systematic Review of the Literature. Cancers 2022, 14, 2323. https://doi.org/10.3390/cancers14092323
Di Giuseppe J, Grelloni C, Giuliani L, Delli Carpini G, Giannella L, Ciavattini A. Recurrence of Uterine Smooth Muscle Tumor of Uncertain Malignant Potential: A Systematic Review of the Literature. Cancers. 2022; 14(9):2323. https://doi.org/10.3390/cancers14092323
Chicago/Turabian StyleDi Giuseppe, Jacopo, Camilla Grelloni, Lucia Giuliani, Giovanni Delli Carpini, Luca Giannella, and Andrea Ciavattini. 2022. "Recurrence of Uterine Smooth Muscle Tumor of Uncertain Malignant Potential: A Systematic Review of the Literature" Cancers 14, no. 9: 2323. https://doi.org/10.3390/cancers14092323