
X-ray-Fluorescence Imaging for In Vivo Detection of Gold-Nanoparticle-Labeled Immune Cells: A GEANT4 Based Feasibility Study


 and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Software and Setup
2.2. Procedure
2.3. Statistical Analysis
3. Results
3.1. Thorax
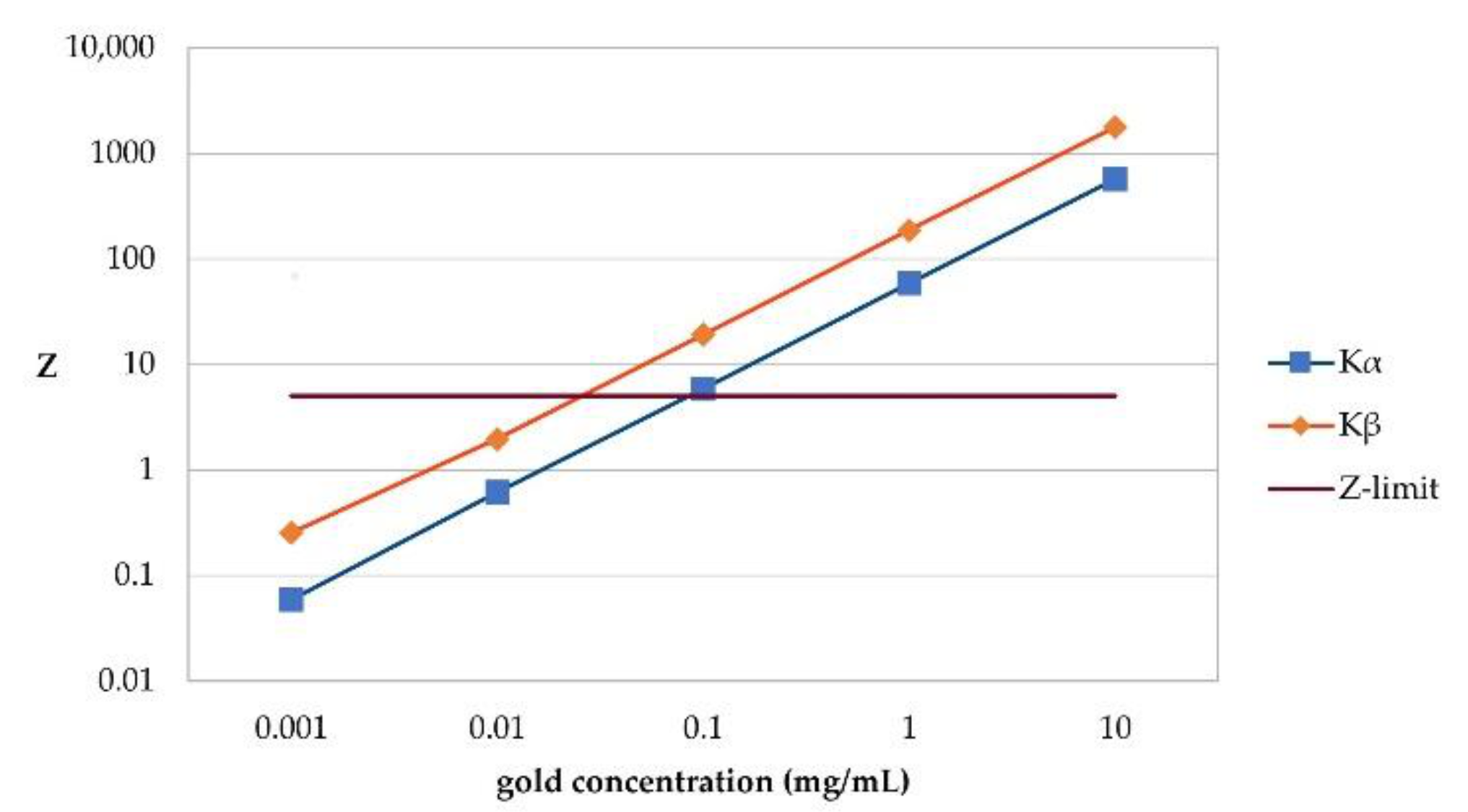
3.1.1. Detectable Gold Concentrations, Extrapolation of Sensitivity
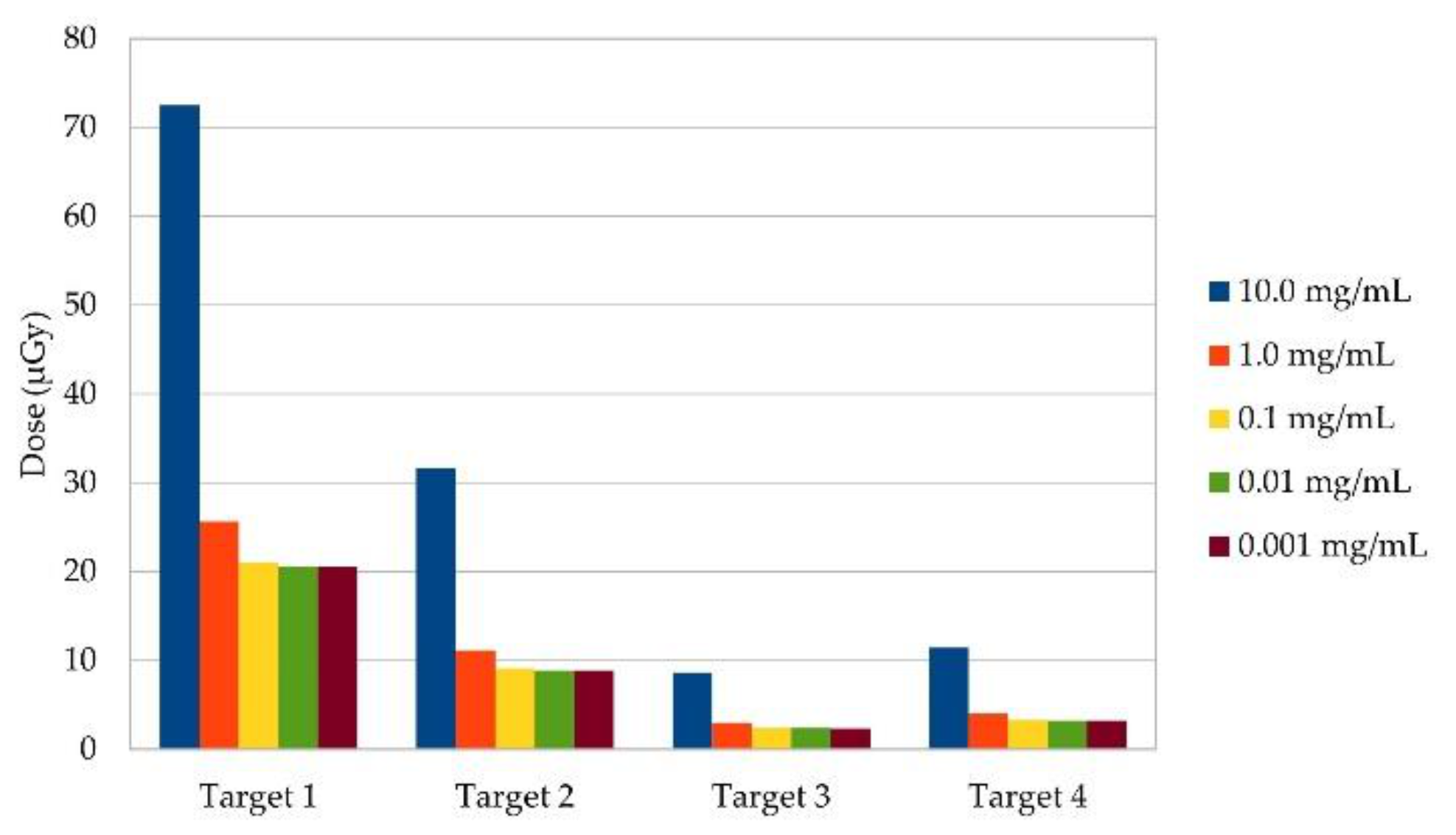
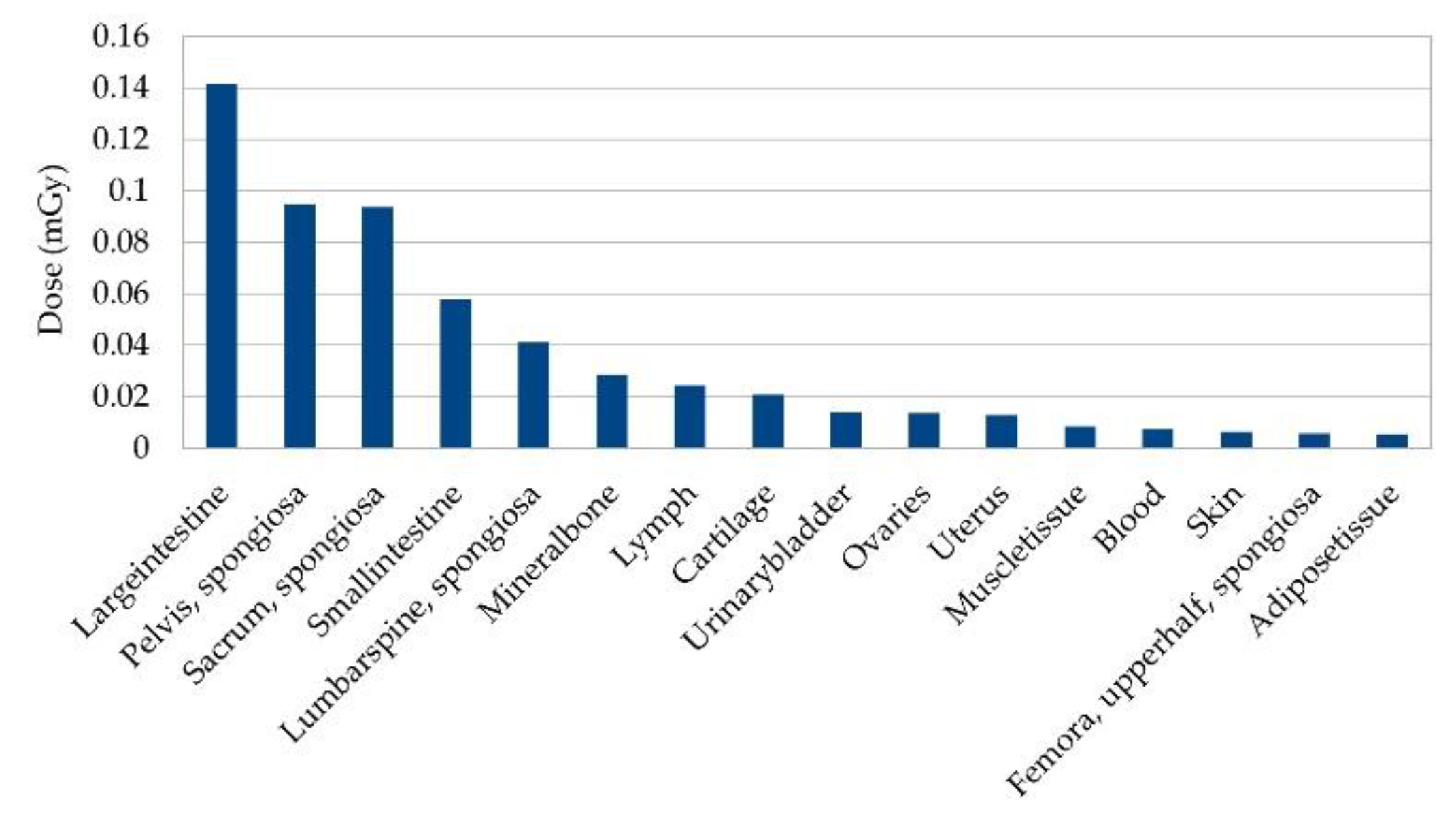
3.1.2. Radiation Doses
3.2. Abdomen
3.2.1. Detectable Gold Concentrations, Extrapolation of Sensitivity
3.2.2. Dependence on Incident Beam Angle
3.2.3. Radiation Dose
4. Discussion
4.1. Sensitivity in Thorax and Abdomen
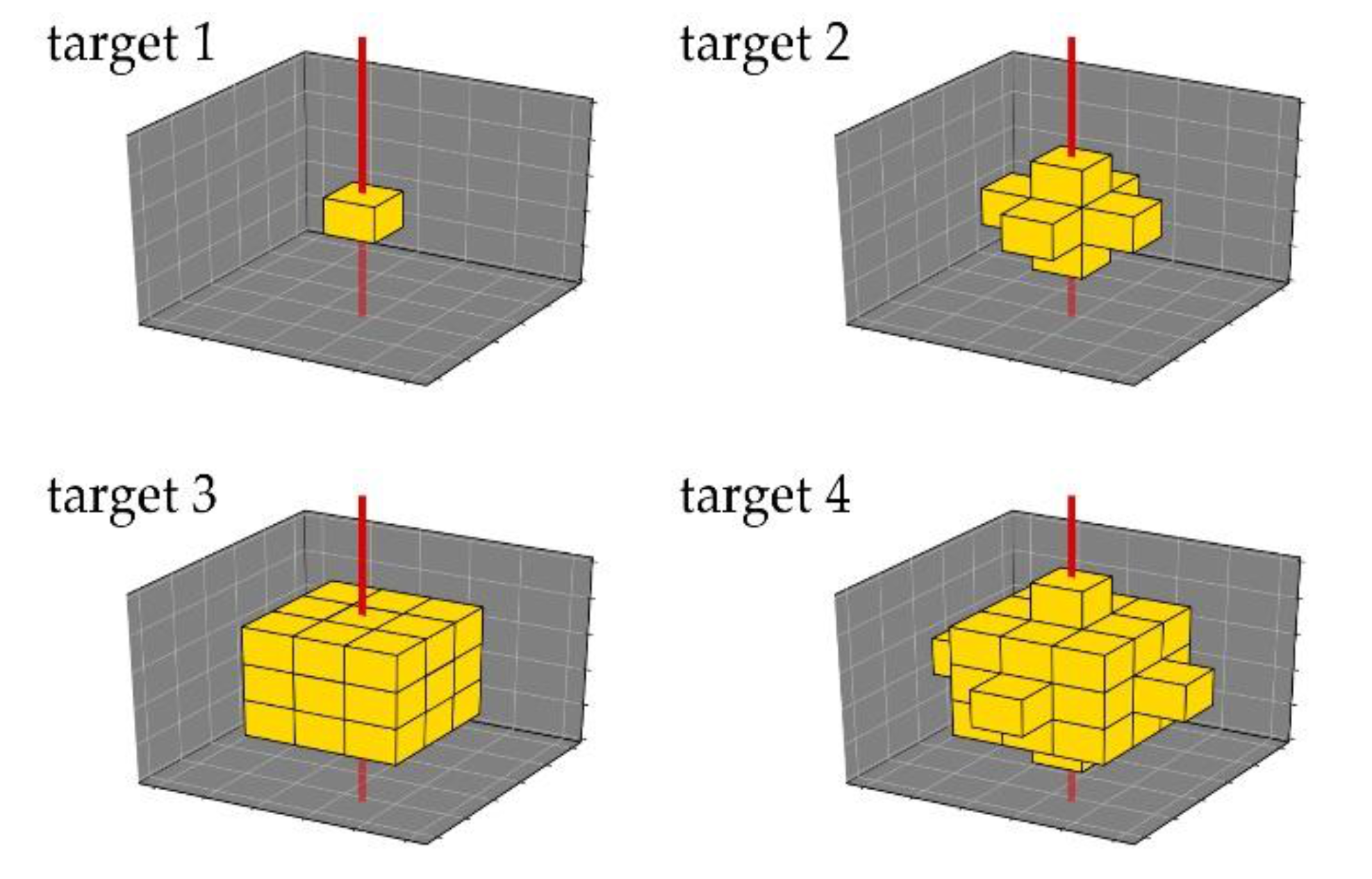
4.2. Effects of Target Size
4.3. Dose in Thorax and Abdomen
4.4. Comparison with Other Imaging Modalities
4.5. Limitations of the Setup
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mankoff, D.A. A definition of molecular imaging. J. Nucl. Med. 2007, 48, 18N–21N. [Google Scholar] [PubMed]
- Hong, H.; Yang, Y.; Zhang, Y.; Cai, W. Non-invasive cell tracking in cancer and cancer therapy. Curr. Top. Med. Chem. 2010, 10, 1237–1248. [Google Scholar] [CrossRef] [PubMed]
- Wu, A.M. Engineered antibodies for molecular imaging of cancer. Methods 2014, 65, 139–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavaré, R.; Escuin-Ordinas, H.; Mok, S.; McCracken, M.N.; Zettlitz, K.A.; Salazar, F.B.; Witte, O.N.; Ribas, A.; Wu, A.M. An Effective Immuno-PET Imaging Method to Monitor CD8-Dependent Responses to Immunotherapie. Cancer Res. 2016, 76, 73–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seth, A.; Park, H.S.; Hong, K.S. Current Perspective on In Vivo Molecular Imaging of Immune Cells. Molecules 2017, 22, 881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Li, Z. Molecular imaging in tracking tumor-specific cytotoxic T lymphocytes (CTLs). Theranostics 2014, 4, 990–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, G.K.; Hoseok, I.; Kim, G.S.; Hwang, N.S.; Choi, H.S. Optical spectroscopic imaging for cell therapy and tissue engineering. Appl. Spectrosc. Rev. 2018, 53, 360–375. [Google Scholar] [CrossRef] [Green Version]
- Kircher, M.F.; Gambhir, S.S.; Grimm, J. Noninvasive cell-tracking methods. Nat. Rev. Clin. Oncol. 2011, 8, 677–688. [Google Scholar] [CrossRef]
- Kim, J.; Chhour, P.; Hsu, J.; Litt, H.I.; Ferrari, V.A.; Popovtzer, R.; Cormode, D.P. Use of Nanoparticle Contrast Agents for Cell Tracking with Computed Tomography. Bioconjug. Chem. 2017, 28, 1581–1597. [Google Scholar] [CrossRef] [Green Version]
- Ngen, E.J.; Artemov, D. Advances in Monitoring Cell-Based Therapies with Magnetic Resonance Imaging: Future Perspectives. Int. J. Mol. Sci. 2017, 18, 198. [Google Scholar] [CrossRef]
- Ahlgren, L.; Lidén, K.; Mattsson, S.; Tejning, S. X-ray fluorescence analysis of lead in human skeleton in vivo. Scand. J. Work. Environ. Health. 1979, 2, 82–86. [Google Scholar] [CrossRef]
- Börjesson, J.; Isaksson, M.; Mattsson, S. X-ray fluorescence analysis in medical sciences: A review. Acta Diabetol. 2003, 40, 39–44. [Google Scholar] [CrossRef]
- Müller, B.H.; Hoeschen, C.; Grüner, F.; Arkadiev, V.A.; Johnson, T.R. Molecular imaging based on x-ray fluorescent high-Z tracers. Phys. Med. Biol. 2013, 58, 8063–8076. [Google Scholar] [CrossRef]
- Grüner, F.; Blumendorf, F.; Schmutzler, O.; Staufer, T.; Bradbury, M.; Wiesner, U.; Rosentreter, T.; Loers, G.; Lutz, D.; Richter, B.; et al. Localising functionalised gold-nanoparticles in murine spinal cords by X-ray fluorescence imaging and background-reduction through spatial filtering for human-sized objects. Sci. Rep. 2018, 8, 16561. [Google Scholar] [CrossRef] [Green Version]
- Vernekohl, D.; Tzoumas, S.; Zhao, W.; Xing, L. Polarized x-ray excitation for scatter reduction in x-ray fluorescence computed tomography. Med. Phys. 2018, 45, 3741–3748. [Google Scholar] [CrossRef]
- Zhang, R.; Li, L.; Sultanbawa, Y.; Xu, Z.P. X-ray fluorescence imaging of metals and metalloids in biological systems. Am. J. Nucl. Med. Mol. Imaging 2018, 8, 169–188. [Google Scholar]
- Westneat, M.W.; Socha, J.J.; Lee, W.K. Advances in biological structure, function, and physiology using synchrotron X-ray imaging *. Annu. Rev. Physiol. 2008, 70, 119–142. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, M.; Bazalova-Carter, M.; Fahrig, R.; Xing, L. Optimized Detector Angular Configuration Increases the Sensitivity of X-ray Fluorescence Computed Tomography (XFCT). IEEE. Trans. Med. Imaging 2015, 34, 1140–1147. [Google Scholar] [CrossRef]
- Robert, C.; Dedes, G.; Battistoni, G.; Böhlen, T.T.; Buvat, I.; Cerutti, F.; Chin, M.P.; Ferrari, A.; Gueth, P.; Kurz, C.; et al. Distributions of secondary particles in proton and carbon-ion therapy: A comparison between GATE/Geant4 and FLUKA Monte Carlo codes. Phys. Med. Biol. 2013, 58, 2879–2899. [Google Scholar] [CrossRef]
- Brualla, L.; Rodriguez, M.; Lallena, A.M. Monte Carlo systems used for treatment planning and dose verification. Strahlenther. Onkol. 2017, 193, 243–259. [Google Scholar] [CrossRef]
- Ahmed, A.M.; Chacon, A.; Rutherford, H.; Akamatsu, G.; Mohammadi, A.; Nishikido, F.; Tashima, H.; Yoshida, E.; Yamaya, T.; Franklin, D.R.; et al. A validated Geant4 model of a whole-body PET scanner with four-layer DOI detectors. Phys. Med. Biol. 2020, 65, 235051. [Google Scholar] [CrossRef]
- Baumann, K.-S.; Horst, F.; Zink, K.; Gomà, C. Comparison of penh, fluka, and Geant4/topas for absorbed dose calculations in air cavities representing ionization chambers in high-energy photon and proton beams. Med. Phys. 2019, 46, 4639–4653. [Google Scholar] [CrossRef] [Green Version]
- Carver, D.E.; Kost, S.D.; Fernald, M.J.; Lewis, K.G., 2nd; Fraser, N.D.; Pickens, D.R.; Price, R.R.; Stabin, M.G. Development and validation of a GEANT4 radiation transport code for CT dosimetry. Health Phys. 2015, 108, 419–428. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.J.; Park, H.; Shin, W.G.; Kim, J.I.; Min, C.H. Development of a Geant4-based independent patient dose validation system with an elaborate multileaf collimator simulation model. J. Appl. Clin. Med. Phys. 2019, 20, 94–106. [Google Scholar] [CrossRef]
- Carrier, J.F.; Archambault, L.; Beaulieu, L.; Roy, R. Validation of GEANT4, an object-oriented Monte Carlo toolkit, for simulations in medical physics. Med. Phys. 2004, 31, 484–492. [Google Scholar] [CrossRef]
- Allison, J.; Amako, K.; Apostolakis, J.; Araujo, H.; Arce Dubois, P.; Asai, M.; Barrand, G.; Capra, R.; Chauvie, S.; Chytracek, R.; et al. Geant4 developments and applications. IEEE Trans. Nucl. Sci. 2006, 53, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Vernekohl, D.; Ahmad, M.; Chinn, G.; Xing, L. Feasibility study of Compton cameras for x-ray fluorescence computed tomography with humans. Phys. Med. Biol. 2016, 61, 8521–8540. [Google Scholar] [CrossRef] [Green Version]
- Qin, Z.; Caruso, J.A.; Lai, B.; Matusch, A.; Becker, J.S. Trace metal imaging with high spatial resolution: Applications in biomedicine. Metallomics 2011, 3, 28–37. [Google Scholar] [CrossRef] [Green Version]
- Sayers, Z.; Avşar, B.; Cholak, E.; Karmous, I. Application of advanced X-ray methods in life sciences. Biochim. Biophys. Acta. Gen. Subj. 2017, 1861 Pt B, 3671–3685. [Google Scholar] [CrossRef]
- Cheong, S.K.; Jones, B.L.; Siddiqi, A.K.; Liu, F.; Manohar, N.; Cho, S.H. X-ray fluorescence computed tomography (XFCT) imaging of gold nanoparticle-loaded objects using 110 kVp x-rays. Phys. Med. Biol. 2010, 55, 647–662. [Google Scholar] [CrossRef]
- Bouché, M.; Hsu, J.C.; Dong, Y.C.; Kim, J.; Taing, K.; Cormode, D.P. Recent Advances in Molecular Imaging with Gold Nanoparticles. Bioconjug. Chem. 2020, 31, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Luo, D.; Wang, X.; Burda, C.; Basilion, J.P. Recent Development of Gold Nanoparticles as Contrast Agents for Cancer Diagnosis. Cancers 2021, 13, 1825. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Gupta, S.; Li, C. Research perspectives: Gold nanoparticles in cancer theranostics. Quant. Imaging Med. Surg. 2013, 3, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Cormode, D.P.; Naha, P.C.; Fayad, Z.A. Nanoparticle contrast agents for computed tomography: A focus on micelles. Contrast Media Mol. Imaging 2014, 9, 37–52. [Google Scholar] [CrossRef] [Green Version]
- Tabish, T.A.; Dey, P.; Mosca, S.; Salimi, M.; Palombo, F.; Matousek, P.; Stone, N. Smart Gold Nanostructures for Light Mediated Cancer Theranostics: Combining Optical Diagnostics with Photothermal Therapy. Adv. Sci. 2020, 7, 1903441. [Google Scholar] [CrossRef]
- Kennedy, L.C.; Bear, A.S.; Young, J.K.; Lewinski, N.A.; Kim, J.; Foster, A.E.; Drezek, R.A. T cells enhance gold nanoparticle delivery to tumors in vivo. Nanoscale Res. Lett. 2011, 6, 283. [Google Scholar] [CrossRef] [Green Version]
- Yong, C.S.M.; Dardalhon, V.; Devaud, C.; Taylor, N.; Darcy, P.K.; Kershaw, M.H. CAR T-cell therapy of solid tumors. Immunol. Cell. Biol. 2017, 95, 356–363. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, W.; Zhang, X.; Cai, Z.; Huang, W. A long way to the battlefront: CAR T cell therapy against solid cancers. J. Cancer 2019, 10, 3112–3123. [Google Scholar] [CrossRef] [Green Version]
- Chapelin, F.; Capitini, C.M.; Ahrens, E.T. Fluorine-19 MRI for detection and quantification of immune cell therapy for cancer. J. Immunother. Cancer 2018, 6, 105. [Google Scholar] [CrossRef]
- Tindemans, I.; Joosse, M.E.; Samsom, J.N. Dissecting the Heterogeneity in T-Cell Mediated Inflammation in IBD. Cells 2020, 9, 110. [Google Scholar] [CrossRef] [Green Version]
- Naumova, A.V.; Modo, M.; Moore, A.; Murry, C.E.; Frank, J.A. Clinical imaging in regenerative medicine. Nat. Biotechnol. 2014, 32, 804–818. [Google Scholar] [CrossRef] [Green Version]
- Vedvyas, Y.; Shevlin, E.; Zaman, M.; Min, I.M.; Amor-Coarasa, A.; Park, S.; Park, S.; Kwon, K.W.; Smith, T.; Luo, Y.; et al. Longitudinal PET imaging demonstrates biphasic CAR T cell responses in survivors. JCI. Insight 2016, 1, e90064. [Google Scholar] [CrossRef]
- Meir, R.; Shamalov, K.; Betzer, O.; Motiei, M.; Horovitz-Fried, M.; Yehuda, R.; Popovtzer, A.; Popovtzer, R.; Cohen, C.J. Nanomedicine for Cancer Immunotherapy: Tracking Cancer-Specific T-Cells in Vivo with Gold Nanoparticles and CT Imaging. ACS Nano 2015, 9, 6363–6372. [Google Scholar] [CrossRef]
- Tumeh, P.C.; Harview, C.L.; Yearley, J.H.; Shintaku, I.P.; Taylor, E.J.; Robert, L.; Chmielowski, B.; Spasic, M.; Henry, G.; Ciobanu, V.; et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 2014, 515, 568–571. [Google Scholar] [CrossRef]
- Bamias, G.; Corridoni, D.; Pizarro, T.T.; Cominelli, F. New insights into the dichotomous role of innate cytokines in gut homeostasis and inflammation. Cytokine 2012, 59, 451–459. [Google Scholar] [CrossRef] [Green Version]
- Meir, R.; Popovtzer, R. Cell tracking using gold nanoparticles and computed tomography imaging. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2018, 10, 1480. [Google Scholar] [CrossRef]
- Chemla, Y.; Betzer, O.; Markus, A.; Farah, N.; Motiei, M.; Popovtzer, R.; Mandel, Y. Gold nanoparticles for multimodal high-resolution imaging of transplanted cells for retinal replacement therapy. Nanomedicine 2019, 14, 1857–1871. [Google Scholar] [CrossRef]
- Chen, M.; Betzer, O.; Fan, Y.; Gao, Y.; Shen, M.; Sadan, T.; Popovtzer, R.; Shi, X. Multifunctional Dendrimer-Entrapped Gold Nanoparticles for Labeling and Tracking T Cells Via Dual-Modal Computed Tomography and Fluorescence Imaging. Biomacromolecules 2020, 21, 1587–1595. [Google Scholar] [CrossRef]
- Melancon, M.P.; Lu, W.; Yang, Z.; Zhang, R.; Cheng, Z.; Elliot, A.M.; Stafford, J.; Olson, T.; Zhang, J.Z.; Li, C. In vitro and in vivo targeting of hollow gold nanoshells directed at epidermal growth factor receptor for photothermal ablation therapy. Mol. Cancer Ther. 2008, 7, 1730–1739. [Google Scholar] [CrossRef] [Green Version]
- Eck, W.; Nicholson, A.I.; Zentgraf, H.; Semmler, W.; Bartling, S. Anti-CD4-targeted gold nanoparticles induce specific contrast enhancement of peripheral lymph nodes in X-ray computed tomography of live mice. Nano Lett. 2010, 10, 2318–2322. [Google Scholar] [CrossRef]
- Depannemaecker, D.; Santos, L.E.C.; de Almeida, A.G.; Ferreira, G.B.S.; Baraldi, G.L.; Miqueles, E.X.; de Carvalho, M.; Costa, G.S.R.; Marques, M.J.G.; Scorza, C.A.; et al. Gold Nanoparticles for X-ray Microtomography of Neurons. ACS Chem. Neurosci. 2019, 10, 3404–3408. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.; Lee, N.; Arifin, D.R.; Shats, I.; Janowski, M.; Walczak, P.; Hyeon, T.; Bulte, J.W.M. In Vivo Micro-CT Imaging of Human Mesenchymal Stem Cells Labeled with Gold-Poly-L-Lysine Nanocomplexes. Adv. Funct. Mater. 2017, 27, 1604213. [Google Scholar] [CrossRef] [Green Version]
- Reuveni, T.; Motiei, M.; Romman, Z.; Popovtzer, A.; Popovtzer, R. Targeted gold nanoparticles enable molecular CT imaging of cancer: An in vivo study. Int. J. Nanomed. 2011, 6, 2859–2864. [Google Scholar] [CrossRef] [Green Version]
- Zeltsman, M.; Dozier, J.; McGee, E.; Ngai, D.; Adusumilli, P.S. CAR T-cell therapy for lung cancer and malignant pleural mesothelioma. Transl. Res. 2017, 187, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; He, Y. A narrative review of chimeric antigen receptor-T (CAR-T) cell therapy for lung cancer. Ann. Transl. Med. 2021, 9, 808. [Google Scholar] [CrossRef] [PubMed]
- Agostinelli, S.; Allison, J.; Amako, K.; Apostolakis, J.; Araujo, H.; Arce, P.; Asai, M.; Axen, D.; Banerjee, S.; Barrand, G.; et al. Geant4—a simulation toolkit. Nucl. Instrum. Methods Phys. Res. Sect. A 2003, 506, 250–303. [Google Scholar] [CrossRef] [Green Version]
- ICRP. Adult Reference Computational Phantoms. ICRP Publication 110. Ann. ICRP 2009, 39, 1–165. [Google Scholar]
- Kortright, J.B.; Thompson, A.C. 1.2 X-Ray Emission Energies, Table 1–2. In X-Ray Data Booklet, 3rd ed.; Thompson, A.C., Lindau, I., Attwood, D.T., Liu, Y., Gullikson, E.M., Pianetta, P., Howells, M.R., Robinson, A.L., Kim, K., Scofield, J.H., et al., Eds.; Lawrence Berkeley National Laboratory, University of California: Berkeley, CA, USA, 2009; pp. 16–22. [Google Scholar]
- Todd, A.C.; Chettle, D.R. In vivo X-ray fluorescence of lead in bone: Review and current issues. Environ. Health Perspect. 1994, 102, 172–177. [Google Scholar] [CrossRef]
- De Caro, L.; Giannini, C.; Bellotti, R.; Tangaro, S. A theoretical study on phase-contrast mammography with Thomson-scattering x-ray sources. Med. Phys. 2009, 36, 4644–4653. [Google Scholar] [CrossRef]
- Chi, Z.; Du, Y.; Yan, L.; Wang, D.; Zhang, H.; Huang, W.; Tang, C. Experimental feasibility of dual-energy computed tomography based on the Thomson scattering X-ray source. J. Synchrotron. Radiat. 2018, 25 Pt 6, 1797–1802. [Google Scholar] [CrossRef]
- Chi, Z.; Du, Y.; Huang, W.; Tang, C. Linearly polarized X-ray fluorescence computed tomography based on a Thomson scattering light source: A Monte Carlo study. J. Synchrotron Radiat. 2020, 27 Pt 3, 737–745. [Google Scholar] [CrossRef]
- Schmutzler, O.; Graf, S.; Behm, N.; Mansour, W.Y.; Blumendorf, F.; Staufer, T.; Körnig, C.; Salah, D.; Kang, Y.; Peters, J.N.; et al. X-ray Fluorescence Uptake Measurement of Functionalized Gold Nanoparticles in Tumor Cell Microsamples. Int. J. Mol. Sci. 2021, 22, 3691. [Google Scholar] [CrossRef]
- La Rivière, P.J. Approximate analytic reconstruction in x-ray fluorescence computed tomography. Phys. Med. Biol. 2004, 49, 2391–2405. [Google Scholar] [CrossRef]
- Ahmed, M.F.; Yasar, S.; Cho, S.H. Development of an attenuation correction method for direct x-ray fluorescence (XRF) imaging utilizing gold L-shell XRF photons. Med. Phys. 2018, 45, 5543–5554. [Google Scholar] [CrossRef] [Green Version]
- Dunning, C.A.S.; Bazalova-Carter, M. Sheet beam x-ray fluorescence computed tomography (XFCT) imaging of gold nanoparticles. Med. Phys. 2018, 45, 2572–2582. [Google Scholar] [CrossRef]
- Lienert, U.; Gutschmidt, S.; Zimmermann, M.; Nowak, R.; Drube, W. PETRA III Extension Project Beamline P21: Swedish High Energy Materials Science Beamline Technical Design Report, Final Version 07 August 2013. Available online: https://photonscience.desy.de/sites/site_photonscience/content/e58/e176720/e177229/e298286/e299326/infoboxContent299332/P21_TDR_Final_07-08-2013_eng.pdf (accessed on 13 September 2021).










Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ungerer, A.; Staufer, T.; Schmutzler, O.; Körnig, C.; Rothkamm, K.; Grüner, F. X-ray-Fluorescence Imaging for In Vivo Detection of Gold-Nanoparticle-Labeled Immune Cells: A GEANT4 Based Feasibility Study. Cancers 2021, 13, 5759. https://doi.org/10.3390/cancers13225759
Ungerer A, Staufer T, Schmutzler O, Körnig C, Rothkamm K, Grüner F. X-ray-Fluorescence Imaging for In Vivo Detection of Gold-Nanoparticle-Labeled Immune Cells: A GEANT4 Based Feasibility Study. Cancers. 2021; 13(22):5759. https://doi.org/10.3390/cancers13225759
Chicago/Turabian StyleUngerer, Arthur, Theresa Staufer, Oliver Schmutzler, Christian Körnig, Kai Rothkamm, and Florian Grüner. 2021. "X-ray-Fluorescence Imaging for In Vivo Detection of Gold-Nanoparticle-Labeled Immune Cells: A GEANT4 Based Feasibility Study" Cancers 13, no. 22: 5759. https://doi.org/10.3390/cancers13225759