
A Novel Method for the Evaluation of Bone Marrow Samples from Patients with Pediatric B-Cell Acute Lymphoblastic Leukemia—Multidimensional Flow Cytometry

 ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Immunophenotype Analysis
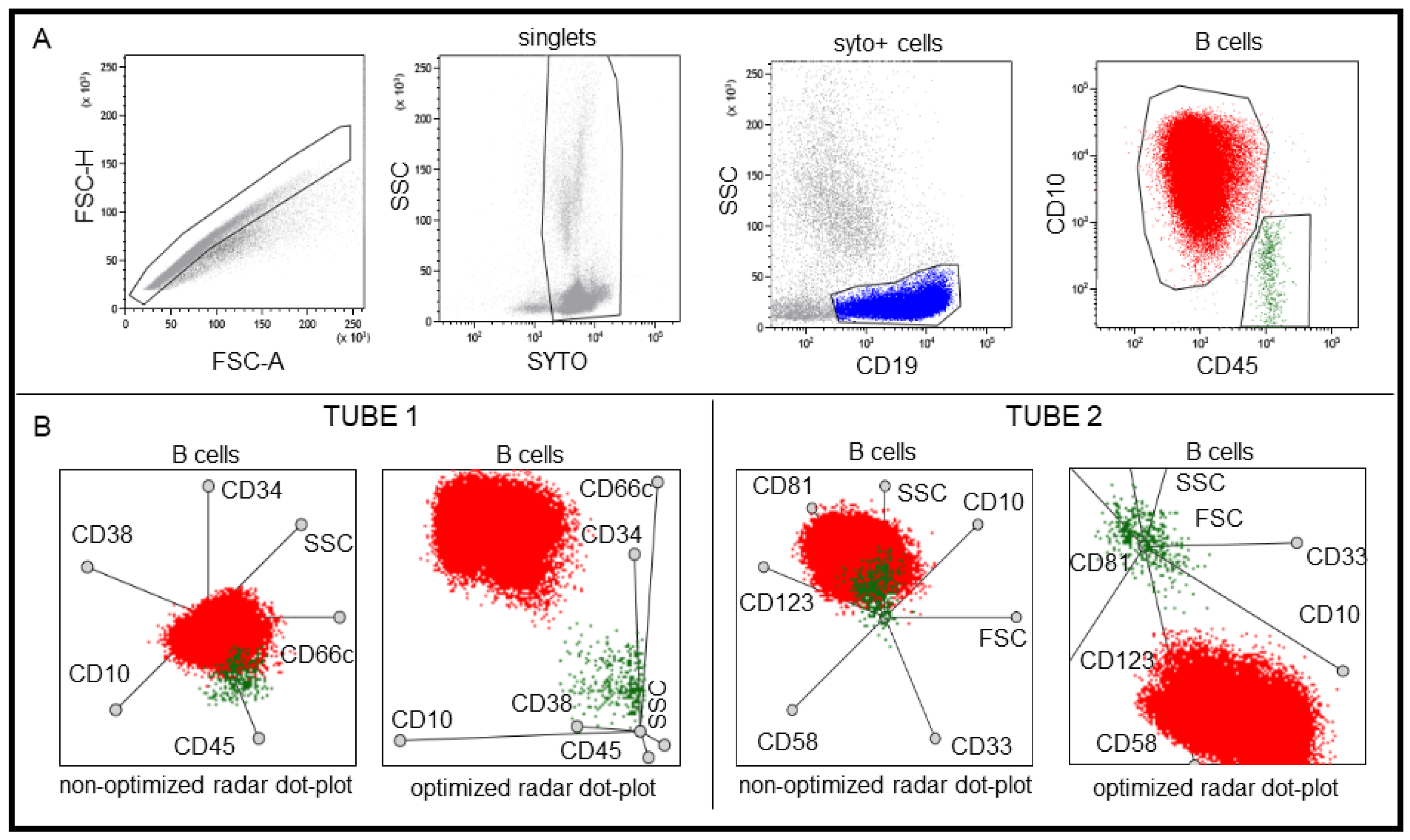
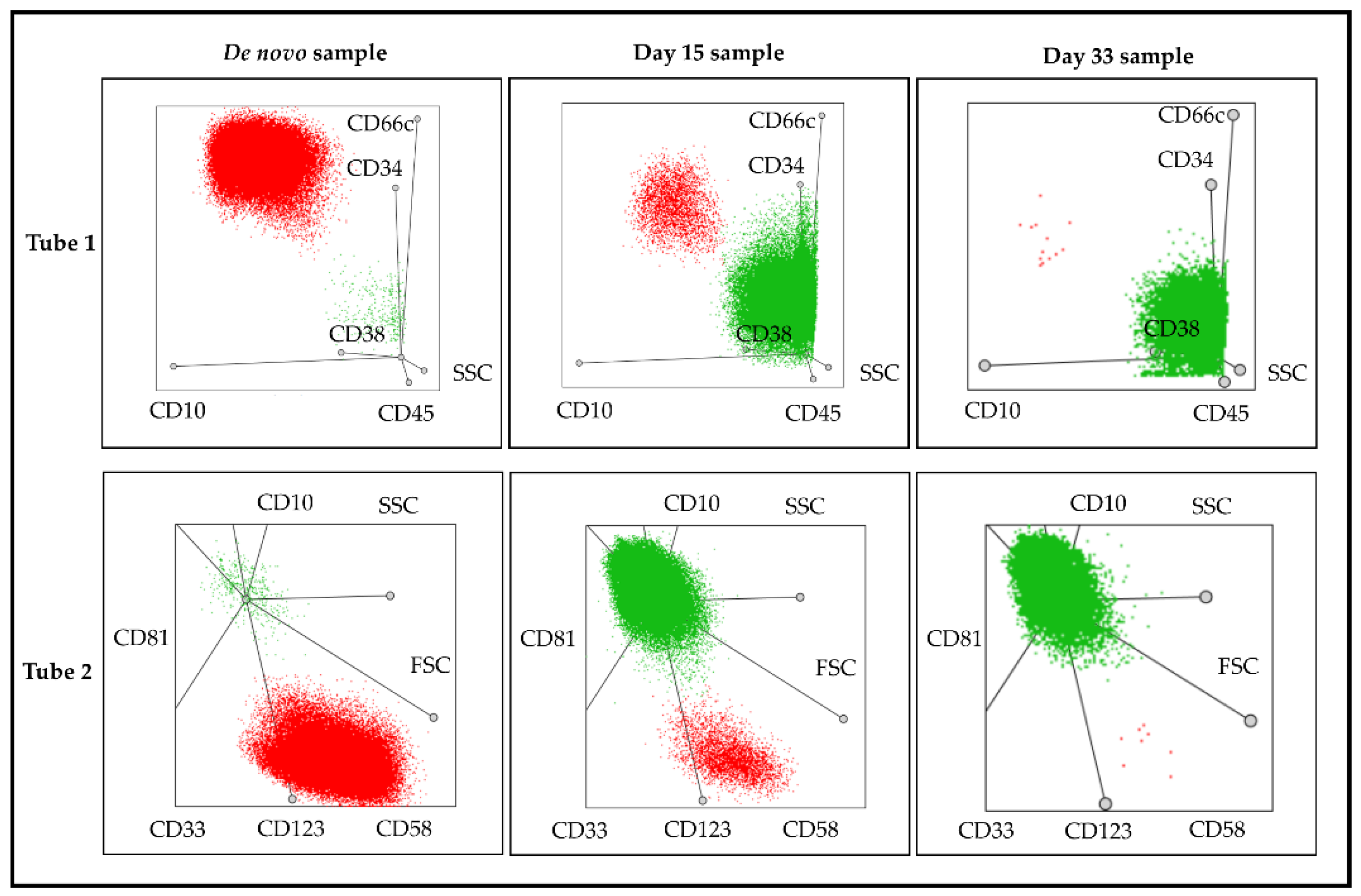
2.3. Detection of Lymphoblasts in ALL by Multidimensional Dot-Plots
2.4. Statistical Analysis
3. Results
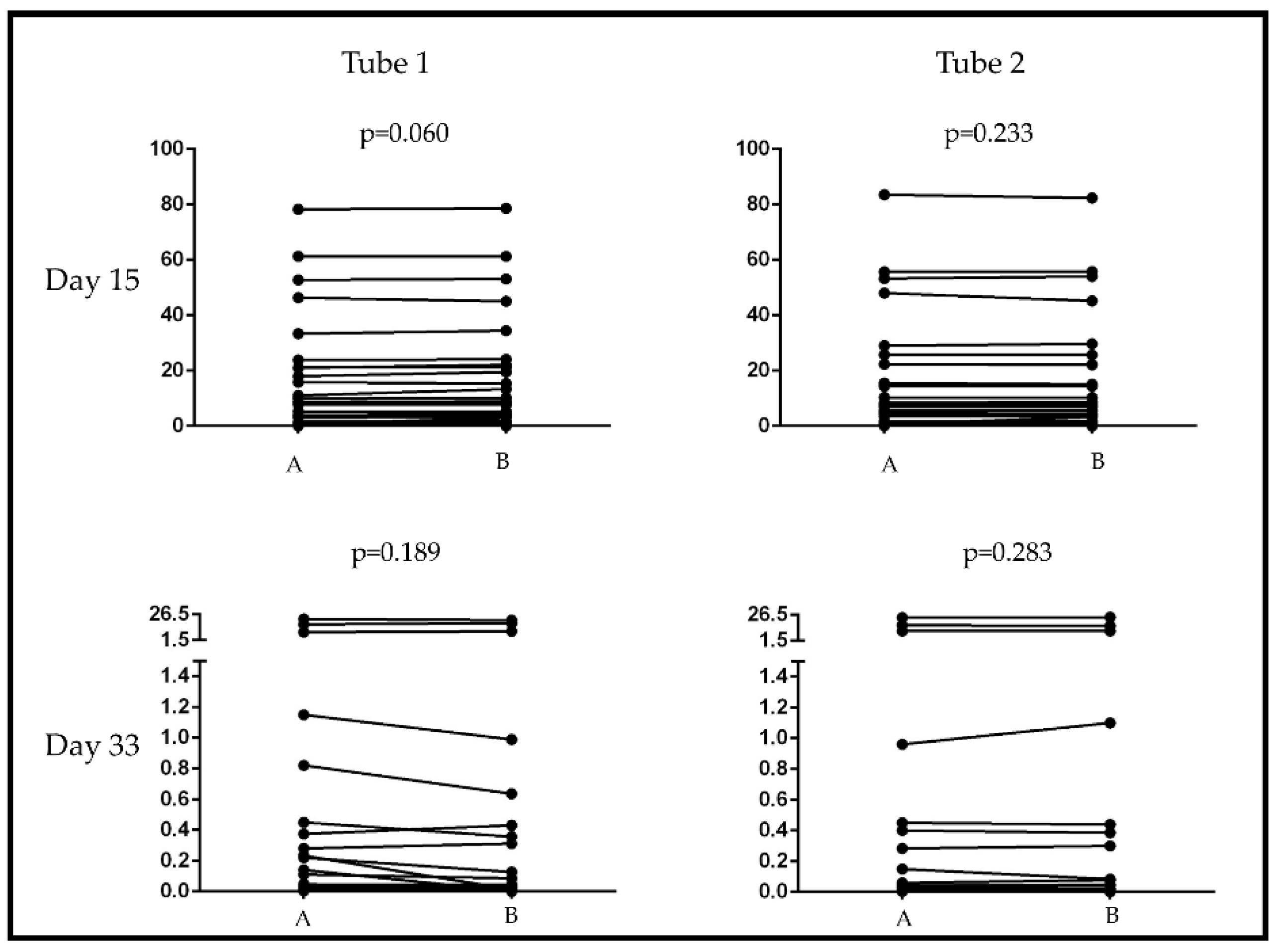
3.1. Comparison of Pathological Cell Detection and Enumeration with Multidimensional and Bivariate Dot-Plots in ALL
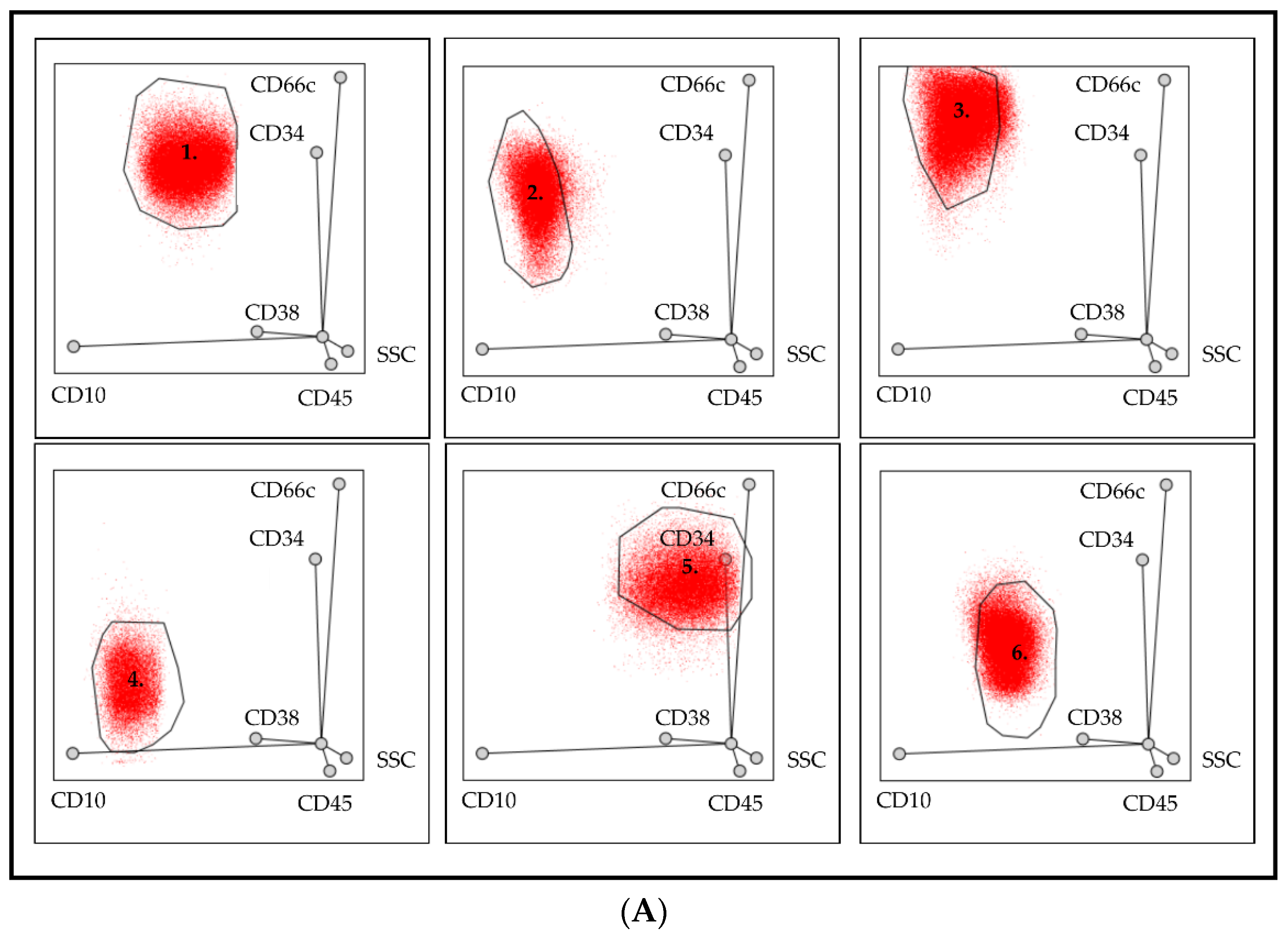
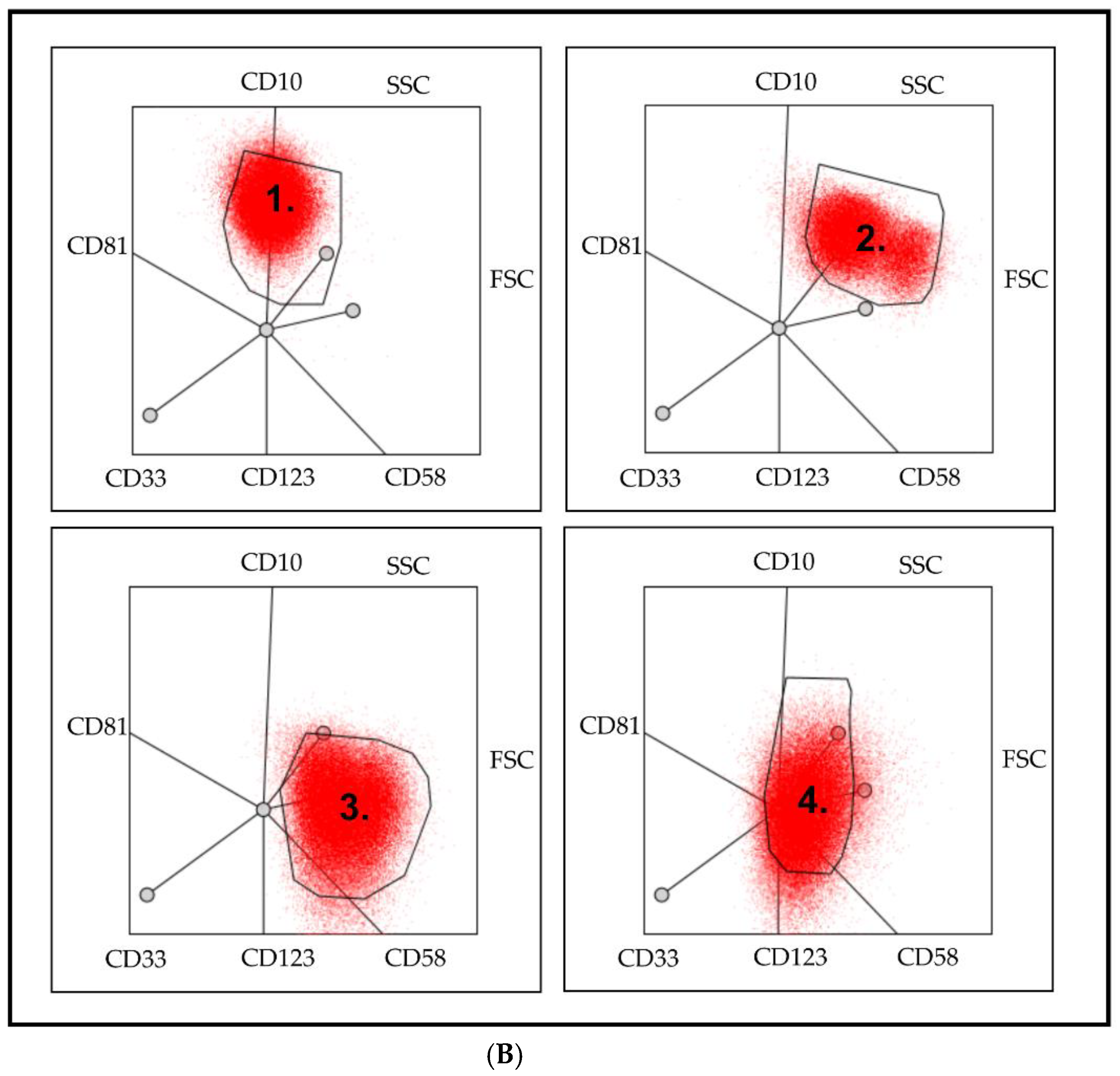
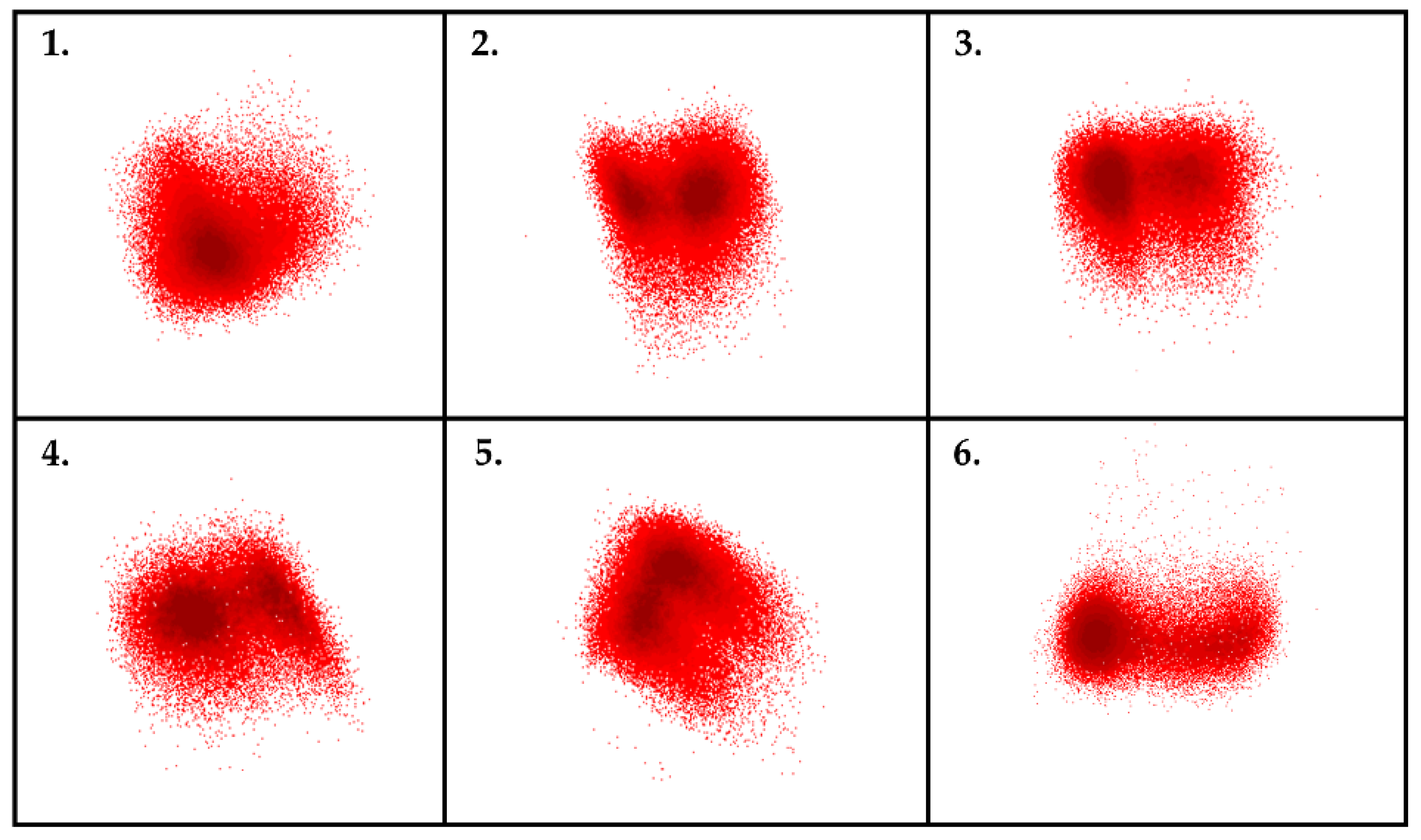
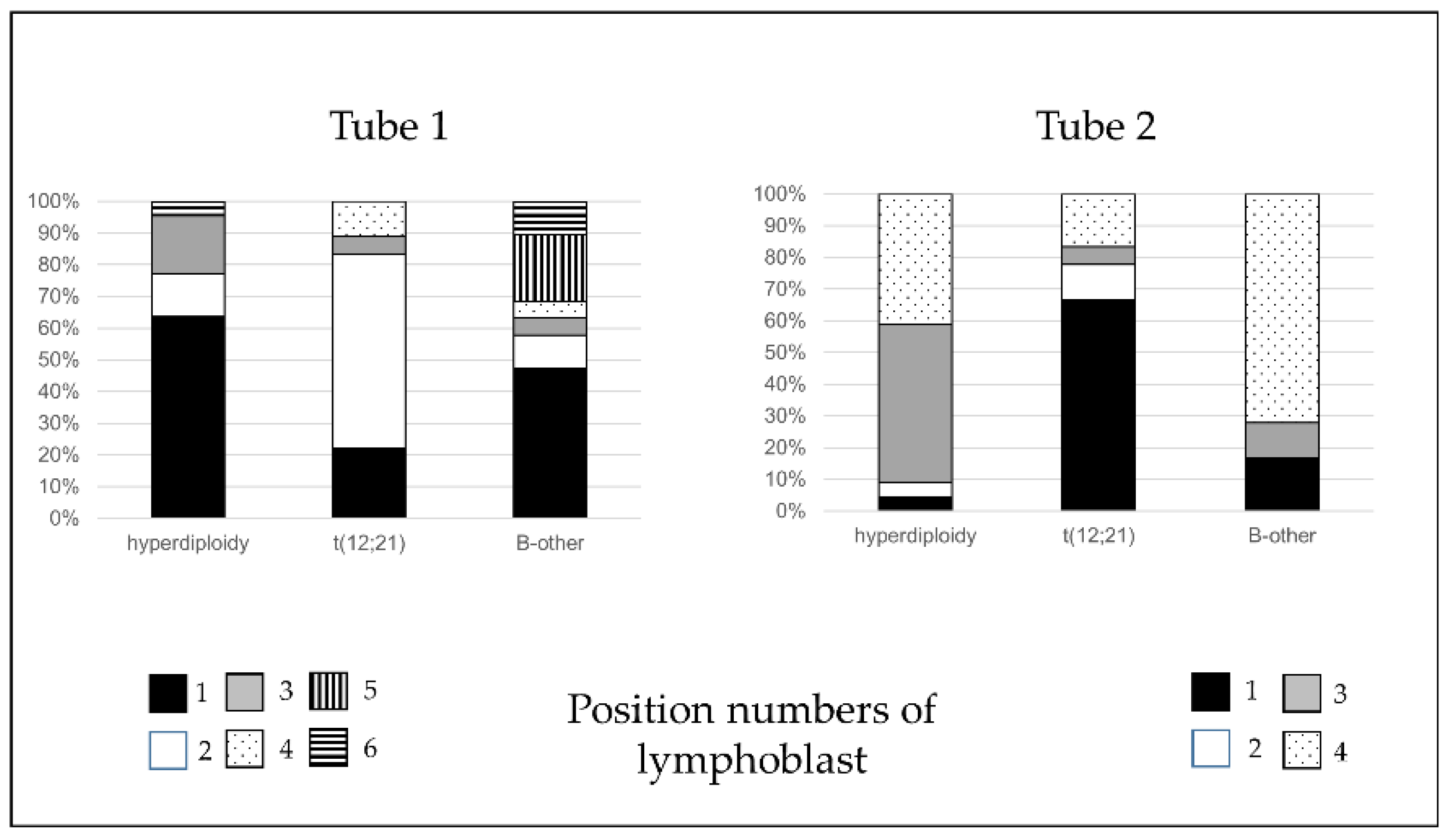
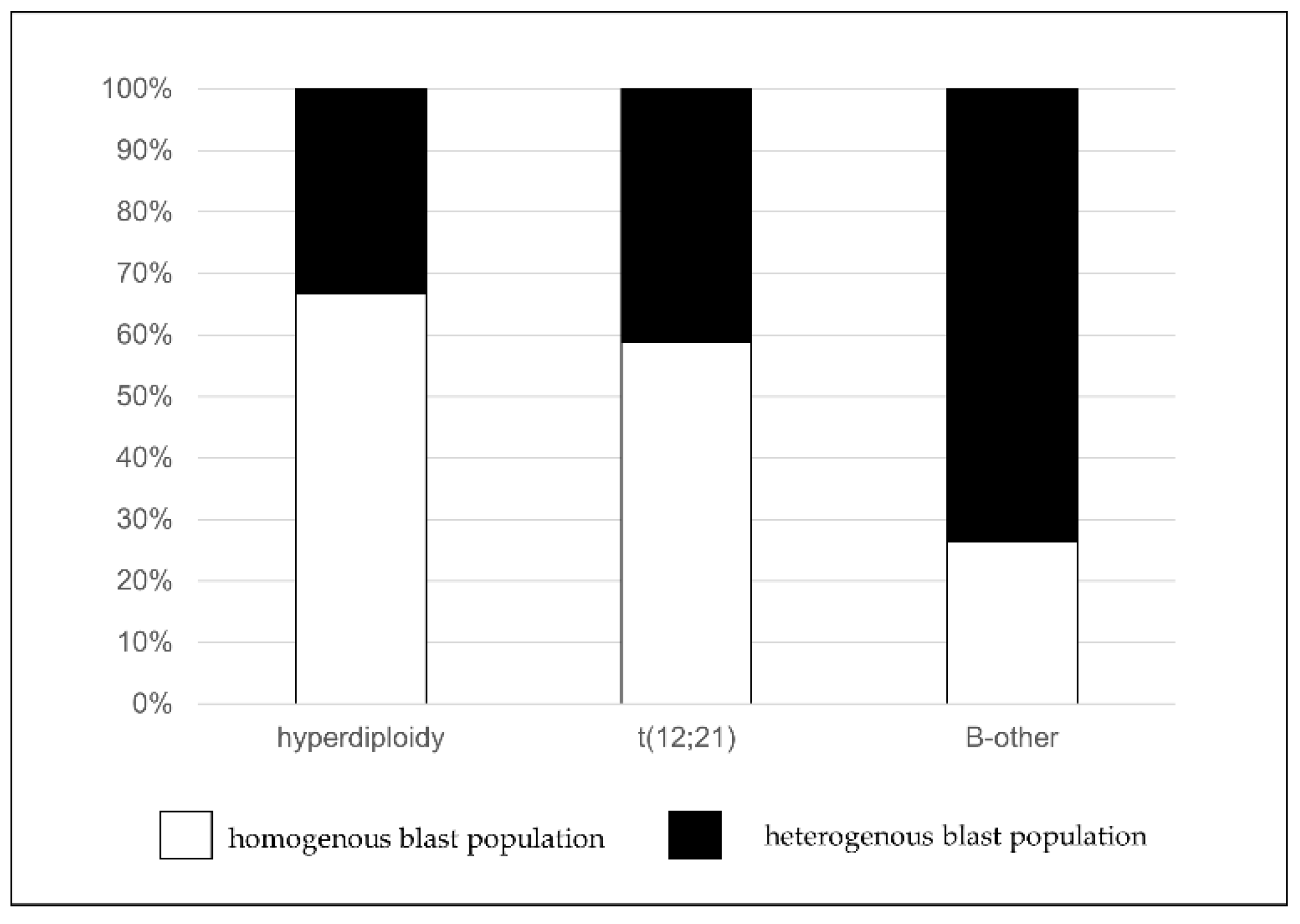
3.2. Association between the Position and the Homogeneity of Pathological Cells and Cytogenetic Alterations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Redaelli, A.; Laskin, B.L.; Stephens, J.M.; Botteman, M.F.; Pashos, C.L. A systematic literature review of the clinical and epidemiological burden of acute lymphoblastic leukaemia (ALL). Eur. J. Cancer Care 2005, 14, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Zawitkowska, J.; Lejman, M.; Romiszewski, M.; Matysiak, M.; Cwiklinska, M.; Balwierz, W.; Owoc-Lempach, J.; Kazanowska, B.; Derwich, K.; Wachowiak, J.; et al. Results of two consecutive treatment protocols in Polish children with acute lymphoblastic leukemia. Sci. Rep. 2020, 10, 20168. [Google Scholar] [CrossRef]
- Arber, D.A.; Orazi, A.; Hasserjian, R.; Thiele, J.; Borowitz, M.J.; Le Beau, M.M.; Bloomfield, C.D.; Cazzola, M.; Vardiman, J.W. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016, 127, 2391–2405. [Google Scholar] [CrossRef]
- Moorman, A.V. New and emerging prognostic and predictive genetic biomarkers in B-cell precursor acute lymphoblastic leukemia. Haematologica 2016, 101, 407–416. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.S.; Alberti, M.O.; Tirado, C.A. Childhood B-acute lymphoblastic leukemia: A genetic update. Exp. Hematol. Oncol. 2014, 3, 16. [Google Scholar] [CrossRef] [Green Version]
- Dworzak, M.N.; Buldini, B.; Gaipa, G.; Ratei, R.; Hrusak, O.; Luria, D.; Rosenthal, E.; Bourquin, J.P.; Sartor, M.; Schumich, A.; et al. AIEOP-BFM consensus guidelines 2016 for flow cytometric immunophenotyping of Pediatric acute lymphoblastic leukemia. Cytom. Part B Clin. Cytom. 2018, 94, 82–93. [Google Scholar] [CrossRef] [Green Version]
- Mejstrikova, E.; Fronkova, E.; Kalina, T.; Omelka, M.; Batinic, D.; Dubravcic, K.; Pospisilova, K.; Vaskova, M.; Luria, D.; Cheng, S.H.; et al. Detection of residual B precursor lymphoblastic leukemia by uniform gating flow cytometry. Pediatr. Blood Cancer 2010, 54, 62–70. [Google Scholar] [CrossRef]
- van Dongen, J.J.; Lhermitte, L.; Bottcher, S.; Almeida, J.; van der Velden, V.H.; Flores-Montero, J.; Rawstron, A.; Asnafi, V.; Lecrevisse, Q.; Lucio, P.; et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia 2012, 26, 1908–1975. [Google Scholar] [CrossRef] [Green Version]
- Burmeister, T.; Meyer, C.; Schwartz, S.; Hofmann, J.; Molkentin, M.; Kowarz, E.; Schneider, B.; Raff, T.; Reinhardt, R.; Gokbuget, N.; et al. The MLL recombinome of adult CD10-negative B-cell precursor acute lymphoblastic leukemia: Results from the GMALL study group. Blood 2009, 113, 4011–4015. [Google Scholar] [CrossRef] [PubMed]
- Owaidah, T.M.; Rawas, F.I.; Al Khayatt, M.F.; Elkum, N.B. Expression of CD66c and CD25 in acute lymphoblastic leukemia as a predictor of the presence of BCR/ABL rearrangement. Hematol. Oncol. Stem Cell Ther. 2008, 1, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Karai, B.; Hevessy, Z.; Szantho, E.; Csathy, L.; Ujfalusi, A.; Gyurina, K.; Szegedi, I.; Kappelmayer, J.; Kiss, C. Expression of Coagulation Factor XIII Subunit A Correlates with Outcome in Childhood Acute Lymphoblastic Leukemia. Pathol. Oncol. Res. 2018, 24, 345–352. [Google Scholar] [CrossRef]
- Mullighan, C.G.; Goorha, S.; Radtke, I.; Miller, C.B.; Coustan-Smith, E.; Dalton, J.D.; Girtman, K.; Mathew, S.; Ma, J.; Pounds, S.B.; et al. Genome-wide analysis of genetic alterations in acute lymphoblastic leukaemia. Nature 2007, 446, 758–764. [Google Scholar] [CrossRef]
- Borowitz, M.J.; Devidas, M.; Hunger, S.P.; Bowman, W.P.; Carroll, A.J.; Carroll, W.L.; Linda, S.; Martin, P.L.; Pullen, D.J.; Viswanatha, D.; et al. Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia and its relationship to other prognostic factors: A Children’s Oncology Group study. Blood 2008, 111, 5477–5485. [Google Scholar] [CrossRef] [Green Version]
- Cave, H.; van der Werff ten Bosch, J.; Suciu, S.; Guidal, C.; Waterkeyn, C.; Otten, J.; Bakkus, M.; Thielemans, K.; Grandchamp, B.; Vilmer, E. Clinical significance of minimal residual disease in childhood acute lymphoblastic leukemia. European Organization for Research and Treatment of Cancer--Childhood Leukemia Cooperative Group. N. Engl. J. Med. 1998, 339, 591–598. [Google Scholar] [CrossRef]
- Coustan-Smith, E.; Sancho, J.; Hancock, M.L.; Boyett, J.M.; Behm, F.G.; Raimondi, S.C.; Sandlund, J.T.; Rivera, G.K.; Rubnitz, J.E.; Ribeiro, R.C.; et al. Clinical importance of minimal residual disease in childhood acute lymphoblastic leukemia. Blood 2000, 96, 2691–2696. [Google Scholar] [CrossRef] [PubMed]
- Dworzak, M.N.; Froschl, G.; Printz, D.; Mann, G.; Potschger, U.; Muhlegger, N.; Fritsch, G.; Gadner, H.; Austrian Berlin-Frankfurt-Munster Study Group. Prognostic significance and modalities of flow cytometric minimal residual disease detection in childhood acute lymphoblastic leukemia. Blood 2002, 99, 1952–1958. [Google Scholar] [CrossRef] [Green Version]
- Stary, J.; Zimmermann, M.; Campbell, M.; Castillo, L.; Dibar, E.; Donska, S.; Gonzalez, A.; Izraeli, S.; Janic, D.; Jazbec, J.; et al. Intensive chemotherapy for childhood acute lymphoblastic leukemia: Results of the randomized intercontinental trial ALL IC-BFM 2002. J. Clin. Oncol. 2014, 32, 174–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basso, G.; Veltroni, M.; Valsecchi, M.G.; Dworzak, M.N.; Ratei, R.; Silvestri, D.; Benetello, A.; Buldini, B.; Maglia, O.; Masera, G.; et al. Risk of relapse of childhood acute lymphoblastic leukemia is predicted by flow cytometric measurement of residual disease on day 15 bone marrow. J. Clin. Oncol. 2009, 27, 5168–5174. [Google Scholar] [CrossRef] [PubMed]
- Modvig, S.; Hallbook, H.; Madsen, H.O.; Siitonen, S.; Rosthoj, S.; Tierens, A.; Juvonen, V.; Osnes, L.T.N.; Valerhaugen, H.; Hultdin, M.; et al. Value of flow cytometry for MRD-based relapse prediction in B-cell precursor ALL in a multicenter setting. Leukemia 2021, 35, 1894–1906. [Google Scholar] [CrossRef] [PubMed]
- van Dongen, J.J.; van der Velden, V.H.; Bruggemann, M.; Orfao, A. Minimal residual disease diagnostics in acute lymphoblastic leukemia: Need for sensitive, fast, and standardized technologies. Blood 2015, 125, 3996–4009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dworzak, M.N.; Gaipa, G.; Ratei, R.; Veltroni, M.; Schumich, A.; Maglia, O.; Karawajew, L.; Benetello, A.; Potschger, U.; Husak, Z.; et al. Standardization of flow cytometric minimal residual disease evaluation in acute lymphoblastic leukemia: Multicentric assessment is feasible. Cytom. Part B Clin. Cytom. 2008, 74, 331–340. [Google Scholar] [CrossRef]
- van Lochem, E.G.; van der Velden, V.H.; Wind, H.K.; te Marvelde, J.G.; Westerdaal, N.A.; van Dongen, J.J. Immunophenotypic differentiation patterns of normal hematopoiesis in human bone marrow: Reference patterns for age-related changes and disease-induced shifts. Cytom. Part B Clin. Cytom. 2004, 60, 1–13. [Google Scholar] [CrossRef]
- Borowitz, M.J.; Pullen, D.J.; Winick, N.; Martin, P.L.; Bowman, W.P.; Camitta, B. Comparison of diagnostic and relapse flow cytometry phenotypes in childhood acute lymphoblastic leukemia: Implications for residual disease detection: A report from the children’s oncology group. Cytom. Part B Clin. Cytom. 2005, 68, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Cherian, S.; Soma, L.A. How I Diagnose Minimal/Measurable Residual Disease in B Lymphoblastic Leukemia/Lymphoma by Flow Cytometry. Am. J. Clin. Pathol. 2021, 155, 38–54. [Google Scholar] [CrossRef] [PubMed]
- Della Starza, I.; Chiaretti, S.; De Propris, M.S.; Elia, L.; Cavalli, M.; De Novi, L.A.; Soscia, R.; Messina, M.; Vitale, A.; Guarini, A.; et al. Minimal Residual Disease in Acute Lymphoblastic Leukemia: Technical and Clinical Advances. Front. Oncol. 2019, 9, 726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jafari, K.; Tierens, A.; Rajab, A.; Musani, R.; Schuh, A.; Porwit, A. Visualization of Cell Composition and Maturation in the Bone Marrow Using 10-Color Flow Cytometry and Radar Plots. Cytom. Part B Clin. Cytom. 2018, 94, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Karai, B.; Habok, M.; Remenyi, G.; Rejto, L.; Ujfalusi, A.; Kappelmayer, J.; Hevessy, Z. A novel flow cytometric method for enhancing acute promyelocytic leukemia screening by multidimensional dot-plots. Ann. Hematol. 2019, 98, 1413–1420. [Google Scholar] [CrossRef] [Green Version]
- Gupta, M.; Jafari, K.; Rajab, A.; Wei, C.; Mazur, J.; Tierens, A.; Hyjek, E.; Musani, R.; Porwit, A. Radar plots facilitate differential diagnosis of acute promyelocytic leukemia and NPM1+ acute myeloid leukemia by flow cytometry. Cytom. Part B Clin. Cytom. 2021, 100, 409–420. [Google Scholar] [CrossRef]
- Theunissen, P.; Mejstrikova, E.; Sedek, L.; van der Sluijs-Gelling, A.J.; Gaipa, G.; Bartels, M.; Sobral da Costa, E.; Kotrova, M.; Novakova, M.; Sonneveld, E.; et al. Standardized flow cytometry for highly sensitive MRD measurements in B-cell acute lymphoblastic leukemia. Blood 2017, 129, 347–357. [Google Scholar] [CrossRef]
- Pedreira, C.E.; Costa, E.S.; Barrena, S.; Lecrevisse, Q.; Almeida, J.; van Dongen, J.J.; Orfao, A.; EuroFlow, C. Generation of flow cytometry data files with a potentially infinite number of dimensions. Cytom. Part A J. Int. Soc. Anal. Cytol. 2008, 73, 834–846. [Google Scholar] [CrossRef]
- Flores-Montero, J.; Sanoja-Flores, L.; Paiva, B.; Puig, N.; Garcia-Sanchez, O.; Bottcher, S.; van der Velden, V.H.J.; Perez-Moran, J.J.; Vidriales, M.B.; Garcia-Sanz, R.; et al. Next Generation Flow for highly sensitive and standardized detection of minimal residual disease in multiple myeloma. Leukemia 2017, 31, 2094–2103. [Google Scholar] [CrossRef] [Green Version]
- Medina, A.; Puig, N.; Flores-Montero, J.; Jimenez, C.; Sarasquete, M.E.; Garcia-Alvarez, M.; Prieto-Conde, I.; Chillon, C.; Alcoceba, M.; Gutierrez, N.C.; et al. Comparison of next-generation sequencing (NGS) and next-generation flow (NGF) for minimal residual disease (MRD) assessment in multiple myeloma. Blood Cancer J. 2020, 10, 108. [Google Scholar] [CrossRef] [PubMed]
- Tembhare, P.R.; Subramanian Pg, P.G.; Ghogale, S.; Chatterjee, G.; Patkar, N.V.; Gupta, A.; Shukla, R.; Badrinath, Y.; Deshpande, N.; Narula, G.; et al. A High-Sensitivity 10-Color Flow Cytometric Minimal Residual Disease Assay in B-Lymphoblastic Leukemia/Lymphoma Can Easily Achieve the Sensitivity of 2-in-10(6) and Is Superior to Standard Minimal Residual Disease Assay: A Study of 622 Patients. Cytom. Part B Clin. Cytom. 2020, 98, 57–67. [Google Scholar] [CrossRef]
- Libert, D.; Yuan, C.M.; Masih, K.E.; Galera, P.; Salem, D.; Shalabi, H.; Yates, B.; Delbrook, C.; Shern, J.F.; Fry, T.J.; et al. Serial evaluation of CD19 surface expression in pediatric B-cell malignancies following CD19-targeted therapy. Leukemia 2020, 34, 3064–3069. [Google Scholar] [CrossRef] [PubMed]
- Costa, E.S.; Pedreira, C.E.; Barrena, S.; Lecrevisse, Q.; Flores, J.; Quijano, S.; Almeida, J.; del Carmen Garcia-Macias, M.; Bottcher, S.; Van Dongen, J.J.; et al. Automated pattern-guided principal component analysis vs expert-based immunophenotypic classification of B-cell chronic lymphoproliferative disorders: A step forward in the standardization of clinical immunophenotyping. Leukemia 2010, 24, 1927–1933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bene, M.C.; Lacombe, F.; Porwit, A. Unsupervised flow cytometry analysis in hematological malignancies: A new paradigm. Int. J. Lab. Hematol. 2021, 43 (Suppl. 1), 54–64. [Google Scholar] [CrossRef] [PubMed]
- Lhermitte, L.; Mejstrikova, E.; van der Sluijs-Gelling, A.J.; Grigore, G.E.; Sedek, L.; Bras, A.E.; Gaipa, G.; Sobral da Costa, E.; Novakova, M.; Sonneveld, E.; et al. Automated database-guided expert-supervised orientation for immunophenotypic diagnosis and classification of acute leukemia. Leukemia 2018, 32, 874–881. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | N | % |
|---|---|---|
| Gender | ||
| Male | 37 | 51.4 |
| Female | 35 | 48.6 |
| Age | ||
| <6 years | 42 | 58.3 |
| ≥6 years | 30 | 41.7 |
| Cytogenetic categories | ||
| high hyperdiploidy | 22 | 30.5 |
| t(12;21) (p13.2;q22.1) | 18 | 25.0 |
| t(1;19) (q23;p13.3) | 3 | 4.2 |
| “B-other” subgroup | 19 | 26.4 |
| KMT2A rearrangement | 1 | 1.4 |
| iAMP21 | 2 | 2.8 |
| t(9;22) (q34.1;q11.2) | 6 | 8.3 |
| t(1;9) (q24;q34) | 1 | 1.4 |
| FC-MRD (Day 15) * | ||
| FLR: <0.1% | 20 | 27.8 |
| FMR: 0.1– < 10% | 37 | 51.4 |
| FHR: ≥10% | 12 | 16.7 |
| N/A | 3 | 4.2 |
| FC-MRD (Day 33) * | ||
| <0.1% | 53 | 73.6 |
| 0.1– < 10% | 7 | 9.7 |
| ≥10% | 3 | 4.2 |
| N/A | 9 | 12.5 |
| (A) | |||||||
| Position 1 | Position 2 | Position 3 | Position 4 | Position 5 | Position 6 | ||
| CD66c | negative | 3.70% | 93.30% | 33.30% | 100% | 75% | 66.70% |
| weak positive | 51.90% | 6.70% | 0% | 0% | 0% | 33.30% | |
| positive | 55.60% | 0% | 66.70% | 0% | 25% | 0% | |
| bright positive | 0% | 0% | 0% | 0% | 0% | 0% | |
| CD34 | negative | 11.10% | 33.30% | 0% | 66.70% | 0% | 100% |
| weak positive | 7.40% | 40% | 0% | 33.30% | 0% | 0% | |
| positive | 74.10% | 26.70% | 100% | 0% | 100% | 0% | |
| bright positive | 7.40% | 0% | 0% | 0% | 0% | 0% | |
| CD10 | negative | 0% | 0% | 0% | 0% | 25% | 0% |
| weak positive | 7.40% | 0% | 0% | 0% | 75% | 0% | |
| positive | 66.70% | 0% | 16.70% | 0% | 0% | 100% | |
| bright positive | 25.90% | 100% | 83.30% | 100% | 0% | 0% | |
| CD38 | negative | 25.90% | 13.30% | 16.70% | 33.30% | 0% | 0% |
| weak positive | 25.90% | 0% | 16.70% | 0% | 0% | 33.30% | |
| positive | 48.20% | 86.70% | 66.70% | 66.70% | 100% | 66.70% | |
| bright positive | 0% | 0% | 0% | 0% | 0% | 0% | |
| CD45 | negative | 11.10% | 26.70% | 33.30% | 66.70% | 0% | 0% |
| weak positive | 88.90% | 0% | 66.70% | 33.30% | 100% | 100% | |
| positive | 0% | 73.30% | 0% | 0% | 0% | 0% | |
| bright positive | 0% | 0% | 0% | 0% | 0% | 0% | |
| (B) | |||||||
| Position 1 | Position 2 | Position 3 | Position 4 | ||||
| CD58 | negative | 6.30% | 0% | 0.0% | 8% | ||
| weak positive | 37.5% | 0.0% | 14.3% | 28% | |||
| positive | 56.3% | 100.0% | 85.7% | 64% | |||
| bright positive | 0.0% | 0.0% | 0.0% | 0% | |||
| CD123 | negative | 87.5% | 67.5% | 28.6% | 48% | ||
| weak positive | 12.5% | 33.3% | 28.6% | 16% | |||
| positive | 0.0% | 0.0% | 42.8% | 36% | |||
| bright positive | 0.0% | 0.0% | 0.0% | 0% | |||
| CD33 | negative | 62.5% | 100.0% | 71.4% | 80% | ||
| weak positive | 37.5% | 0.0% | 28.6% | 16% | |||
| positive | 0.0% | 0.0% | 0.0% | 4% | |||
| bright positive | 0.0% | 0.0% | 0.0% | 0% | |||
| CD81 | negative | 0.0% | 0.0% | 0.0% | 0% | ||
| weak positive | 6.3% | 0.0% | 7.2% | 0% | |||
| positive | 93.8% | 100.0% | 71.4% | 36% | |||
| bright positive | 0.0% | 0.0% | 21.4% | 64% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kárai, B.; Tisza, K.; Eperjesi, O.; Nagy, A.C.; Ujfalusi, A.; Kelemen, Á.; Szegedi, I.; Kiss, C.; Kappelmayer, J.; Hevessy, Z. A Novel Method for the Evaluation of Bone Marrow Samples from Patients with Pediatric B-Cell Acute Lymphoblastic Leukemia—Multidimensional Flow Cytometry. Cancers 2021, 13, 5044. https://doi.org/10.3390/cancers13205044
Kárai B, Tisza K, Eperjesi O, Nagy AC, Ujfalusi A, Kelemen Á, Szegedi I, Kiss C, Kappelmayer J, Hevessy Z. A Novel Method for the Evaluation of Bone Marrow Samples from Patients with Pediatric B-Cell Acute Lymphoblastic Leukemia—Multidimensional Flow Cytometry. Cancers. 2021; 13(20):5044. https://doi.org/10.3390/cancers13205044
Chicago/Turabian StyleKárai, Bettina, Katalin Tisza, Orsolya Eperjesi, Attila Csaba Nagy, Anikó Ujfalusi, Ágnes Kelemen, István Szegedi, Csongor Kiss, János Kappelmayer, and Zsuzsanna Hevessy. 2021. "A Novel Method for the Evaluation of Bone Marrow Samples from Patients with Pediatric B-Cell Acute Lymphoblastic Leukemia—Multidimensional Flow Cytometry" Cancers 13, no. 20: 5044. https://doi.org/10.3390/cancers13205044