
Clinical Importance of Regimens in Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma with Macrovascular Invasion

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Catheter Implantation Procedures for HAIC
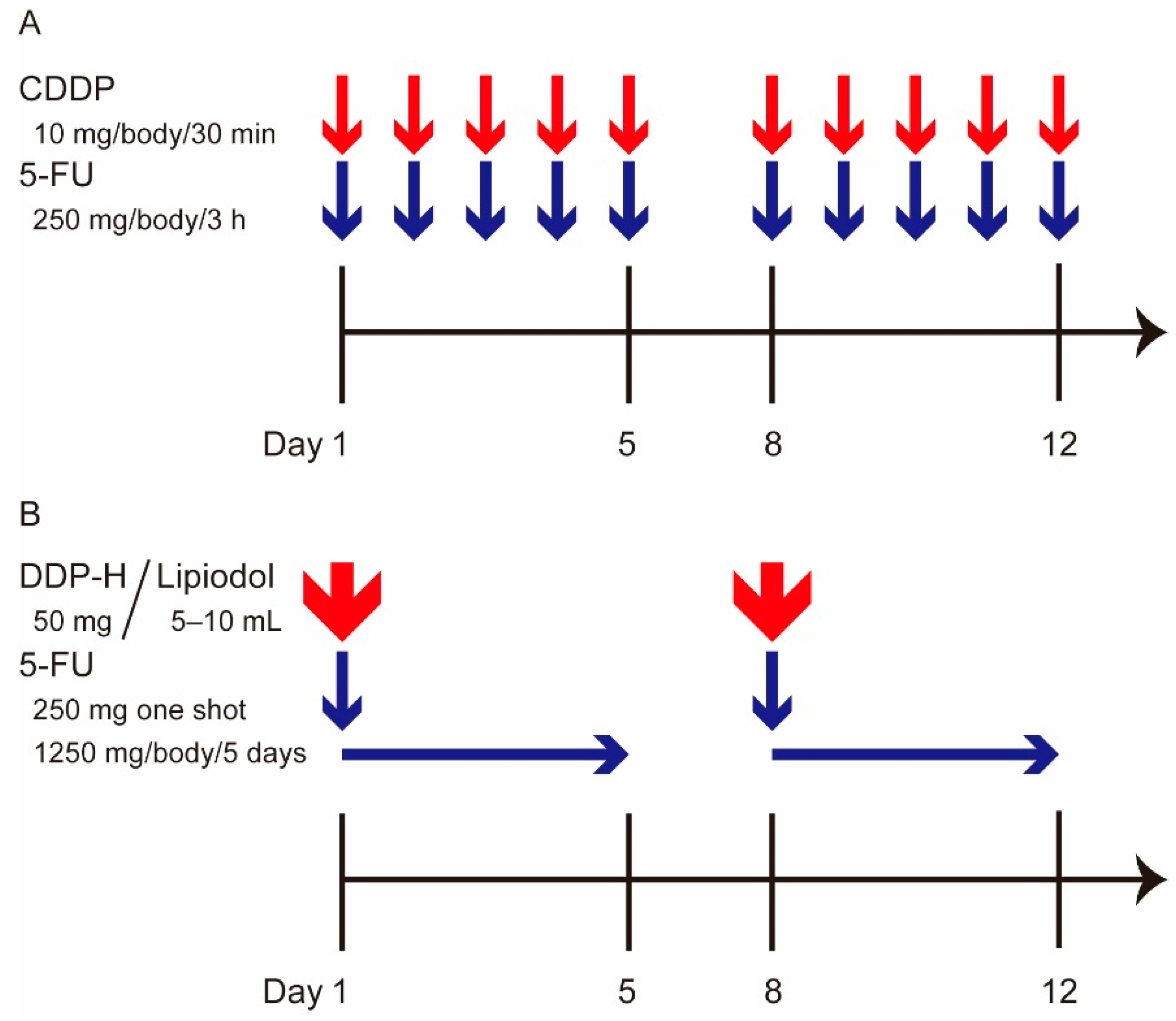
2.3. HAIC Regimens
2.3.1. LFP
2.3.2. New FP
2.4. Assessment of Therapeutic Effects and Safety
2.5. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
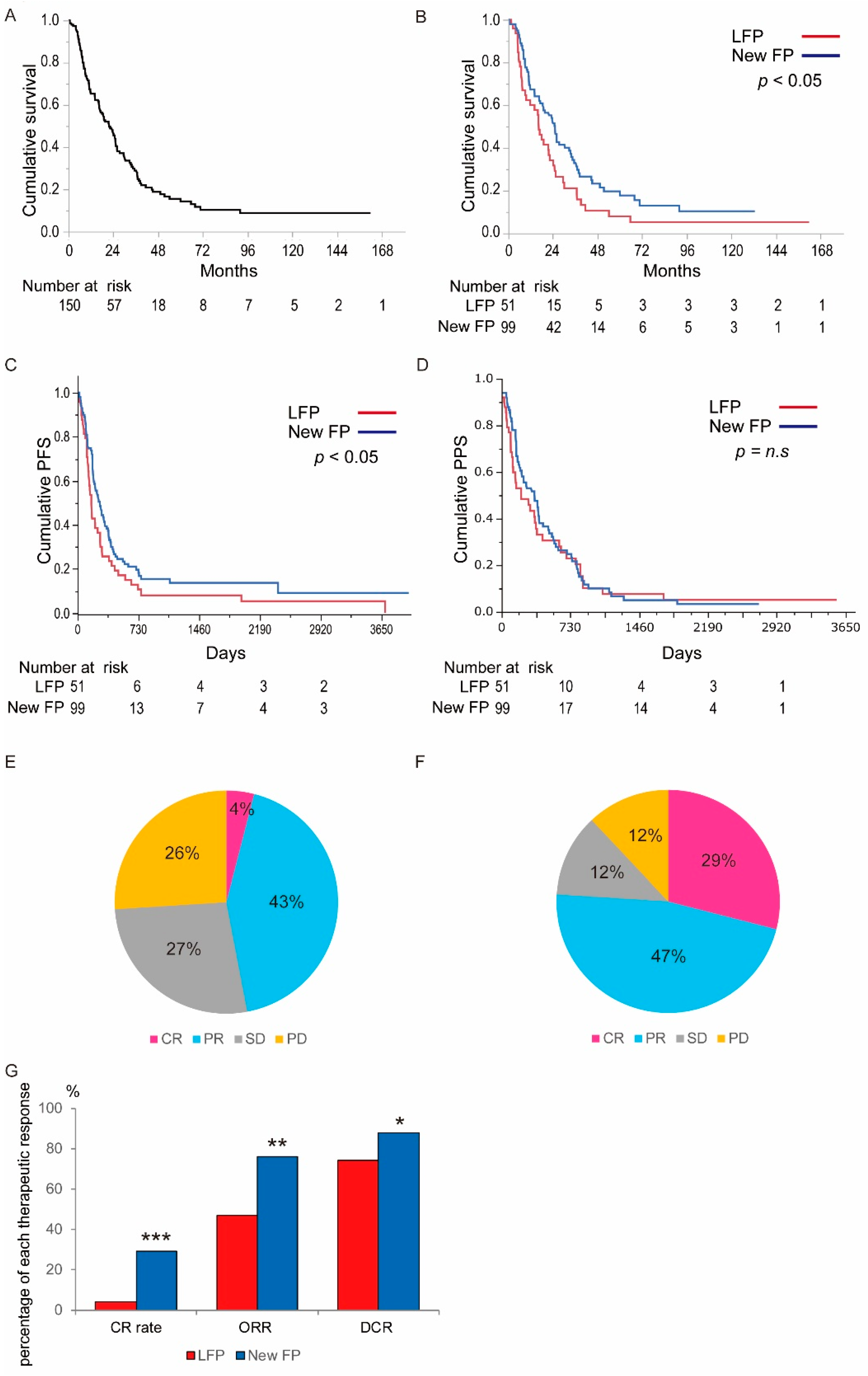
3.2. Assessment of the Therapeutic Outcomes in LFP and New FP
3.3. Assessment of Adverse Events in LFP and New FP Groups
3.4. Factors That Associate with Prognosis in Patients Treated with LFP or New FP
3.5. Factors Associating with Prognosis in Patients Treated with Each Regimen
3.6. Factors Associating with the Therapeutic Response in HAIC Treatment
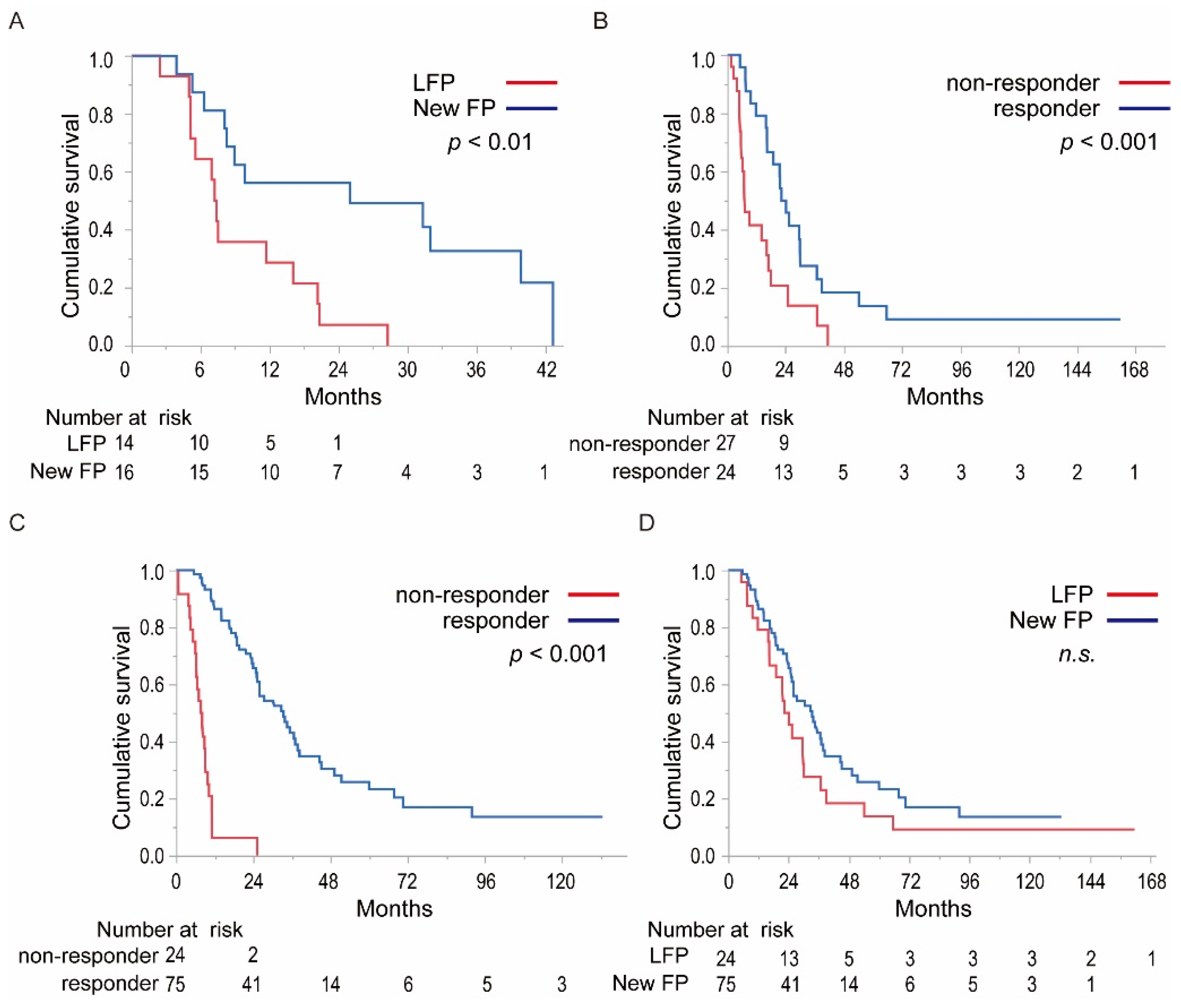
3.7. Comparing OS of the Responders and Non-Responders in LFP and New FP
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Me, J.F.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grandhi, M.S.; Kim, A.K.; Ronnekleiv-Kelly, S.; Kamel, I.R.; Ghasebeh, M.A.; Pawlik, T.M. Hepatocellular carcinoma: From diagnosis to treatment. Surg. Oncol. 2016, 25, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of Hepatocellular Carcinoma: The BCLC Staging Classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef]
- Bruix, J.; Reig, M.; Sherman, M. Evidence-Based Diagnosis, Staging, and Treatment of Patients with Hepatocellular Carcinoma. Gastroenterology 2016, 150, 835–853. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Izumi, N.; Kokudo, N.; Matsui, O.; Sakamoto, M.; Nakashima, O.; Kojiro, M.; Makuuchi, M. Management of Hepatocellular Carcinoma in Japan: Consensus-Based Clinical Practice Guidelines Proposed by the Japan Society of Hepatology (JSH) 2010 Updated Version. Dig. Dis. 2011, 29, 339–364. [Google Scholar] [CrossRef]
- Kudo, M.; Matsui, O.; Izumi, N.; Iijima, H.; Kadoya, M.; Imai, Y.; Okusaka, T.; Miyayama, S.; Tsuchiya, K.; Ueshima, K.; et al. JSH Consensus-Based Clinical Practice Guidelines for the Management of Hepatocellular Carcinoma: 2014 Update by the Liver Cancer Study Group of Japan. Liver Cancer 2014, 3, 458–468. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in Advanced Hepatocellular Carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Chow, P.K.; Gandhi, M.; Tan, S.-B.; Khin, M.W.; Khasbazar, A.; Ong, J.; Choo, S.P.; Cheow, P.C.; Chotipanich, C.; Lim, K.; et al. SIRveNIB: Selective Internal Radiation Therapy Versus Sorafenib in Asia-Pacific Patients with Hepatocellular Carcinoma. J. Clin. Oncol. 2018, 36, 1913–1921. [Google Scholar] [CrossRef]
- Iwamoto, H.; Nomiyama, M.; Niizeki, T.; Shimose, S.; Shirono, T.; Nakano, M.; Satani, M.; Okamura, S.; Noda, Y.; Kamachi, N.; et al. Dose and Location of Irradiation Determine Survival for Patients with Hepatocellular Carcinoma with Macrovascular Invasion in External Beam Radiation Therapy. Oncology 2019, 96, 192–199. [Google Scholar] [CrossRef]
- Ando, E.; Tanaka, M.; Yamashita, F.; Kuromatsu, R.; Yutani, S.; Fukumori, K.; Sumie, S.; Yano, Y.; Okuda, K.; Sata, M. Hepatic arterial infusion chemotherapy for advanced hepatocellular carcinoma with portal vein tumor thrombosis: Analysis of 48 cases. Cancer 2002, 95, 588–595. [Google Scholar] [CrossRef]
- Ikeda, M.; Okusaka, T.; Furuse, J.; Mitsunaga, S.; Ueno, H.; Yamaura, H.; Inaba, Y.; Takeuchi, Y.; Satake, M.; Arai, Y. A multi-institutional phase II trial of hepatic arterial infusion chemotherapy with cisplatin for advanced hepatocellular carcinoma with portal vein tumor thrombosis. Cancer Chemother. Pharmacol. 2013, 72, 463–470. [Google Scholar] [CrossRef]
- Niizeki, T.; Sumie, S.; Torimura, T.; Kurogi, J.; Kuromatsu, R.; Iwamoto, H.; Aino, H.; Nakano, M.; Kawaguchi, A.; Kakuma, T.; et al. Serum vascular endothelial growth factor as a predictor of response and survival in patients with advanced hepatocellular carcinoma undergoing hepatic arterial infusion chemotherapy. J. Gastroenterol. 2012, 47, 686–695. [Google Scholar] [CrossRef]
- Ueshima, K.; Kudo, M.; Takita, M.; Nagai, T.; Tatsumi, C.; Ueda, T.; Kitai, S.; Ishikawa, E.; Yada, N.; Inoue, T.; et al. Hepatic Arterial Infusion Chemotherapy Using Low-Dose 5-Fluorouracil and Cisplatin for Advanced Hepatocellular Carcinoma. Oncology 2010, 78 (Suppl. 1), 148–153. [Google Scholar] [CrossRef] [PubMed]
- Murakami, E.; Aikata, H.; Miyaki, D.; Nagaoki, Y.; Katamura, Y.; Kawaoka, T.; Takaki, S.; Hiramatsu, A.; Waki, K.; Takahashi, S.; et al. Hepatic arterial infusion chemotherapy using 5-fluorouracil and systemic interferon-α for advanced hepatocellular carcinoma in combination with or without three-dimensional conformal radiotherapy to venous tumor thrombosis in hepatic vein or inferior vena. Hepatol. Res. 2011, 42, 442–453. [Google Scholar] [CrossRef]
- Obi, S.; Sato, S.; Kawai, T. Current Status of Hepatic Arterial Infusion Chemotherapy. Liver Cancer 2015, 4, 188–199. [Google Scholar] [CrossRef] [Green Version]
- Yamasaki, T.; Kimura, T.; Kurokawa, F.; Aoyama, K.; Ishikawa, T.; Tajima, K.; Yokoyama, Y.; Takami, T.; Omori, K.; Kawaguchi, K.; et al. Prognostic factors in patients with advanced hepatocellular carcinoma receiving hepatic arterial infusion chemotherapy. J. Gastroenterol. 2005, 40, 70–78. [Google Scholar] [CrossRef] [PubMed]
- Obi, S.; Yoshida, H.; Toune, R.; Unuma, T.; Kanda, M.; Sato, S.; Tateishi, R.; Teratani, T.; Shiina, S.; Omata, M. Combination therapy of intraarterial 5-fluorouracil and systemic interferon-alpha for advanced hepatocellular carcinoma with portal venous invasion. Cancer 2006, 106, 1990–1997. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, H.; Hiraki, M.; Mizukami, N.; Yoshida, H.; Iwamoto, H.; Sumie, S.; Torimura, T.; Sata, M. Intra-arterial therapy with cisplatin suspension in lipiodol and 5-fluorouracil for hepatocellular carcinoma with portal vein tumour thrombosis. Aliment. Pharmacol. Ther. 2010, 32, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Nagamatsu, H.; Sumie, S.; Niizeki, T.; Tajiri, N.; Iwamoto, H.; Aino, H.; Nakano, M.; Shimose, S.; Satani, M.; Okamura, S.; et al. Hepatic arterial infusion chemoembolization therapy for advanced hepatocellular carcinoma: Multicenter phase II study. Cancer Chemother. Pharmacol. 2016, 77, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Nakano, M.; Niizeki, T.; Nagamatsu, H.; Tanaka, M.; Kuromatsu, R.; Satani, M.; Okamura, S.; Iwamoto, H.; Shimose, S.; Shirono, T.; et al. Clinical effects and safety of intra-arterial infusion therapy of cisplatin suspension in lipiodol combined with 5-fluorouracil versus sorafenib, for advanced hepatocellular carcinoma with macroscopic vascular invasion without extra-hepatic spread: A prospective cohort study. Mol. Clin. Oncol. 2017, 7, 1013–1020. [Google Scholar] [CrossRef]
- Iwamoto, H.; Niizeki, T.; Nagamatsu, H.; Ueshima, K.; Nomura, T.; Kuzuya, T.; Kasai, K.; Kooka, Y.; Hiraoka, A.; Sugimoto, R.; et al. Survival Benefit of Hepatic Arterial Infusion Chemotherapy over Sorafenib in the Treatment of Locally Progressed Hepatocellular Carcinoma. Cancers 2021, 13, 646. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of Liver Function in Patients With Hepatocellular Carcinoma: A New Evidence-Based Approach—The ALBI Grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Koganemaru, M.; Abe, T.; Iwamoto, R.; Nonoshita, M.; Yoshida, S.; Uchiyama, D.; Hayabuchi, N. Hepatic arterial infusion chemotherapy with a coaxial reservoir system using a non-braided spiral tip microcatheter. Jpn. J. Radiol. 2011, 30, 10–17. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. In Seminars in Liver Disease; Thieme Medical Publishers: New York, NY, USA, 2010; Volume 30, pp. 52–60. [Google Scholar] [CrossRef] [Green Version]
- Kaneko, S.; Furuse, J.; Kudo, M.; Ikeda, K.; Honda, M.; Nakamoto, Y.; Onchi, M.; Shiota, G.; Yokosuka, O.; Sakaida, I.; et al. Guideline on the use of new anticancer drugs for the treatment of Hepatocellular Carcinoma 2010 update. Hepatol. Res. 2012, 42, 523–542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sastre, J.; Díaz-Beveridge, R.; García-Foncillas, J.; Guardeño, R.; Lopez, C.L.; Pazo, R.; Rodriguez-Salas, N.; Salgado, M.; Salud, A.; Feliu, J. Clinical guideline SEOM: Hepatocellular carcinoma. Clin. Transl. Oncol. 2015, 17, 988–995. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costentin, C.E.; Ferrone, C.R.; Arellano, R.S.; Ganguli, S.; Hong, T.S.; Zhu, A.X. Hepatocellular Carcinoma with Macrovascular Invasion: Defining the Optimal Treatment Strategy. Liver Cancer 2017, 6, 360–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, M.; Li, Q.; Zou, R.; Shen, J.; Fang, W.; Tan, G.; Zhou, Y.; Wu, X.; Xu, L.; Wei, W.; et al. Sorafenib Plus Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin vs Sorafenib Alone for Hepatocellular Carcinoma With Portal Vein Invasion: A Ran-Domized Clinical Trial. JAMA Oncol. 2019, 5, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Ueshima, K.; Yokosuka, O.; Ogasawara, S.; Obi, S.; Izumi, N.; Aikata, H.; Nagano, H.; Hatano, E.; Sasaki, Y.; et al. Sorafenib plus low-dose cisplatin and fluorouracil hepatic arterial infusion chemotherapy versus sorafenib alone in patients with advanced hepatocellular carcinoma (SILIUS): A randomised, open label, phase 3 trial. Lancet Gastroenterol. Hepatol. 2018, 3, 424–432. [Google Scholar] [CrossRef]
- Kawaoka, T.; Aikata, H.; Kobayashi, T.; Uchikawa, S.; Ohya, K.; Kodama, K.; Nishida, Y.; Daijo, K.; Osawa, M.; Teraoka, Y.; et al. Comparison of hepatic arterial infusion chemotherapy between 5-fluorouracil-based continuous infusion chemotherapy and low-dose cisplatin monotherapy for advanced hepatocellular carcinoma. Hepatol. Res. 2018, 48, 1118–1130. [Google Scholar] [CrossRef]
- Takayasu, K.; Shima, Y.; Muramatsu, Y.; Moriyama, N.; Yamada, T.; Makuuchi, M.; Hasegawa, H.; Hirohashi, S. Hepatocellular carcinoma: Treatment with intraarterial iodized oil with and without chemotherapeutic agents. Radiology 1987, 163, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Iwamoto, H.; Fujihara, M.; Nishiofuku, H.; Masada, T.; Suzuki, H.; Koga, H.; Torimura, T.; Kichikawa, K. Efficacy of a Glass Membrane Emulsification Device to Form Mixture of Cisplatin Powder with Lipiodol on Transarterial Therapy for Hepatocellular Carcinoma. Cardiovasc. Interv. Radiol. 2021, 44, 766–773. [Google Scholar] [CrossRef]
- Shirasaka, T.; Shimamoto, Y.; Ohshimo, H.; Kimura, A.; Fukushima, M. Mechanism for synergistic antitumor effect in the combination of 5-fluorouracil with cisplatin in vivo tumor models: From the view of biochemical modulation of 5-fluorouracil. Gan Kagaku Ryoho Cancer Chemother. 1991, 18, 403–409. [Google Scholar]
- Imamine, R.; Shibata, T.; Shinozuka, K.; Togashi, K. Complications in hepatic arterial infusion chemotherapy: Retrospective comparison of catheter tip placement in the right/left hepatic artery vs. the gastroduodenal artery. Surg. Today 2017, 47, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Park, J.Y.; Choi, H.J.; Kim, D.Y.; Ahn, S.H.; Kim, J.K.; Lee, D.Y.; Lee, K.H.; Han, K.-H. Long-term clinical outcomes of hepatic arterial infusion chemotherapy with cisplatin with or without 5-fluorouracil in locally advanced hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2010, 137, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Shimizu, S.; Sato, T.; Morimoto, M.; Kojima, Y.; Inaba, Y.; Hagihara, A.; Kudo, M.; Nakamori, S.; Kaneko, S.; et al. Sorafenib plus hepatic arterial infusion chemotherapy with cisplatin versus sorafenib for advanced hepatocellular carcinoma: Randomized phase II trial. Ann. Oncol. 2016, 27, 2090–2096. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Ueshima, K.; Chiba, Y.; Ogasawara, S.; Obi, S.; Izumi, N.; Aikata, H.; Nagano, H.; Hatano, E.; Sasaki, Y.; et al. Objective Response by mRECIST Is an Independent Prognostic Factor for Overall Survival in Hepatocellular Carcinoma Treated with Sorafenib in the SILIUS Trial. Liver Cancer 2019, 8, 505–519. [Google Scholar] [CrossRef]
- Lencioni, R.; Montal, R.; Torres, F.; Park, J.-W.; Decaens, T.; Raoul, J.-L.; Kudo, M.; Chang, C.; Ríos, J.; Boige, V.; et al. Objective response by mRECIST as a predictor and potential surrogate end-point of overall survival in advanced HCC. J. Hepatol. 2017, 66, 1166–1172. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Items | Total (150) | New FP (n = 99) | Low Dose FP (n = 51) | p-Value |
|---|---|---|---|---|
| Age | 68.1 ± 9.6 | 69.4 ± 9.0 | 65.6 ± 10.2 | 0.035 |
| Sex | 30/120 | 23/76 | 7/44 | 0.158 |
| Etiology (HBV */HCV **/ NBNC ***/HBV + HCV) | 27/78/43/2 | 15/48/35/1 | 12/30/8/1 | 0.079 |
| Child-Pugh score (5/6) | 89/61 | 63/36 | 26/25 | 0.136 |
| ALBI grade (1/2) | 44/106 | 33/66 | 11/40 | 0.134 |
| WBC † (/μL) | 4998 ± 1676 | 4993 ± 1702 | 4993 ± 1640 | 0.926 |
| Plt †† (×104/μL) | 15.2 ± 6.8 | 16.0 ± 7.0 | 13.7 ± 6.1 | 0.057 |
| AFP ††† (median) (ng/mL) | 992 (1.4–2,397,149) | 957 (1.4–1,977,833) | 1028 (2.6–2,397,149) | 0.310 |
| DCP ‡ (median) (mAU/mL) | 16,001(14–2,009,874) | 1648 (14–2,009,874) | 3826 (27–129,000) | 0.009 |
| Maximum tumor diameter (mm) | 81.0 ± 40.0 | 77.3 ± 39.1 | 88.0 ± 40.9 | 0.094 |
| Tumor number 1/2/3/4/≥5 | 5/27/19/9/90 | 4/20/17/5/53 | 1/7/2/4/37 | 0.080 |
| Tumor occupancy (<3/≥3) | 71/79 | 49/50 | 23/28 | 0.526 |
| PVTT ‡‡ (2nd branch/1st Branch/trunk) | 56/44/30 | 43/27/16 | 13/17/14 | 0.140 |
| PVTT ‡‡ (trunk/1st or 2nd branch) | 30/100 | 16/70 | 14/30 | 0.194 |
| HVTT ‡‡‡ (present/absent) | 26/124 | 16/83 | 10/41 | 0.275 |
| BDTT § (present/absent) | 10/140 | 9/90 | 1/50 | 0.097 |
| Adverse Events | New FP (n = 99) (Severe/Discontinuation) | Low-Dose FP (n = 51) (Severe/Discontinuation) | p-Value |
|---|---|---|---|
| Drug allergy | 2/0 | 0/0 | n.s/n.s |
| Liver failure | 2/2 | 0/0 | n.s/n.s |
| Cholangitis | 6/5 | 1/1 | n.s/n.s |
| Wound dehiscence | 0/0 | 2/0 | n.s/n.s |
| Aneurysm | 1/0 | 0/0 | n.s/n.s |
| Acute kidney disorder | 1/0 | 0/0 | n.s/n.s |
| Biloma | 0/0 | 0/0 | n.s/n.s |
| Thrombocytopenia | 8/0 | 7/0 | n.s/n.s |
| Neutropenia | 1/0 | 3/0 | n.s/n.s |
| Pneumonopathy | 2/0 | 0/0 | n.s/n.s |
| Hepatic infarction | 1/0 | 0/0 | n.s/n.s |
| Somatasthenia | 1/1 | 0/0 | n.s/n.s |
| Abdominal pain | 1/0 | 0/0 | n.s/n.s |
| Total | 26/8 | 13/1 | n.s/n.s |
| Factors | Univariate Analysis p-Value | Multivariate Analysis p-Value, Hazard Ratio (95% CI) |
|---|---|---|
| Age (≥70 years) | 0.044 | 0.440 |
| Sex (Male) | 0.784 | - |
| HBs * Ag (+) | 0.055 | 0.177 |
| HCV ** Ab (−) | 0.271 | - |
| Child-Pugh score 6 | 0.016 | 0.413 |
| ALBI-grade 1 | 0.005 | 0.012, 1.912 (0.058–0.484) |
| Platelet count (≥11 × 104/μL) | 0.625 | - |
| AFP *** (≥400 ng/mL) | 0.784 | - |
| DCP † (≥1600 mAU/mL) | 0.003 | 0.126 |
| Maximum tumor diameter (≥70 mm) | 0.044 | 0.483 |
| Tumor located segments (≥3) | 0.003 | 0.026, 1.58 (−0.357 to −0.022) |
| Grade of PVTT †† (trunk) | 0.0004 | 0.019, 1.71 (−0.460 to −0.053) |
| Hepatic vein tumor thrombus (+) | 0.012 | 0.086 |
| Bile duct tumor thrombus (+) | 0.681 | - |
| Regimen (LFP †††) | 0.029 | 0.129 |
| Factors | CR or PR (n = 99) | SD or PD (n = 51) | Univariate Analysis p-Value | Multivariate Analysis p-Value, (Logarithmic Value) |
|---|---|---|---|---|
| Age (<70 years) | 52/47 | 23/28 | 0.388 | - |
| Sex (Female) | 76/23 | 44/7 | 0.158 | - |
| HBs * Ag (−) | 16/83 | 13/38 | 0.159 | - |
| HCV ** Ab (+) | 58/41 | 22/29 | 0.092 | 0.54 |
| ALBI-grade (1) | 36/63 | 8/43 | 0.006 | 0.033, (2.17) |
| Platelet count (>11 × 104/μL) | 68/31 | 41/10 | 0.121 | 0.53 |
| AFP *** (<400 ng/mL) | 56/43 | 32/19 | 0.465 | - |
| DCP † (<1600 mAU/mL) | 46/53 | 39/12 | 0.0003 | 0.37 |
| Maximum tumor diameter (<70 mm) | 38/61 | 35/16 | 0.0004 | 0.26 |
| Tumor located segments (<3) | 45/54 | 17/34 | 0.0130 | 0.17 |
| Grade of PVTT †† (2nd or 1st branch) | 18/81 | 12/39 | 0.442 | 0.38 |
| Hepatic vein tumor thrombus (−) | 14/85 | 12/39 | 0.157 | - |
| Regimen (New FP †††) | 75/24 | 24/27 | 0.0005 | 0.0008, (3.12) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niizeki, T.; Iwamoto, H.; Shirono, T.; Shimose, S.; Nakano, M.; Okamura, S.; Noda, Y.; Kamachi, N.; Hiroyuki, S.; Sakai, M.; et al. Clinical Importance of Regimens in Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma with Macrovascular Invasion. Cancers 2021, 13, 4450. https://doi.org/10.3390/cancers13174450
Niizeki T, Iwamoto H, Shirono T, Shimose S, Nakano M, Okamura S, Noda Y, Kamachi N, Hiroyuki S, Sakai M, et al. Clinical Importance of Regimens in Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma with Macrovascular Invasion. Cancers. 2021; 13(17):4450. https://doi.org/10.3390/cancers13174450
Chicago/Turabian StyleNiizeki, Takashi, Hideki Iwamoto, Tomotake Shirono, Shigeo Shimose, Masahito Nakano, Shusuke Okamura, Yu Noda, Naoki Kamachi, Suzuki Hiroyuki, Miwa Sakai, and et al. 2021. "Clinical Importance of Regimens in Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma with Macrovascular Invasion" Cancers 13, no. 17: 4450. https://doi.org/10.3390/cancers13174450