Molecular Alterations in Relation to Histopathological Characteristics in a Large Series of Pediatric Papillary Thyroid Carcinoma from a Single Institution

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Cohort Characteristics
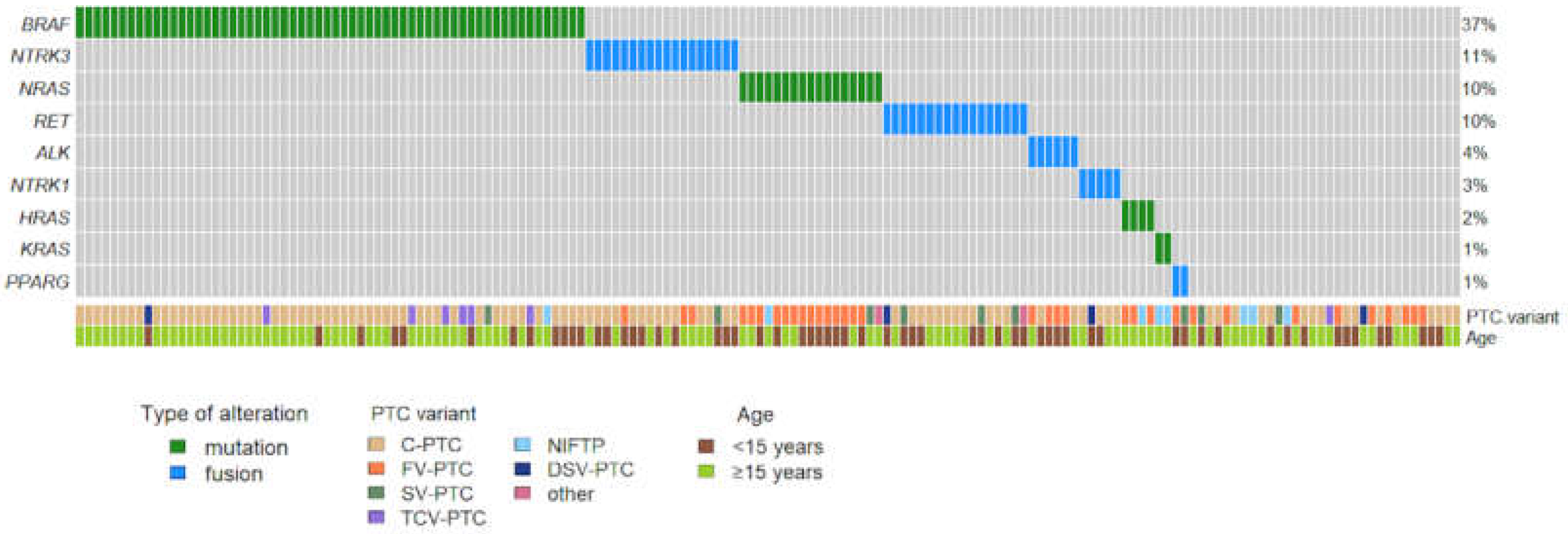
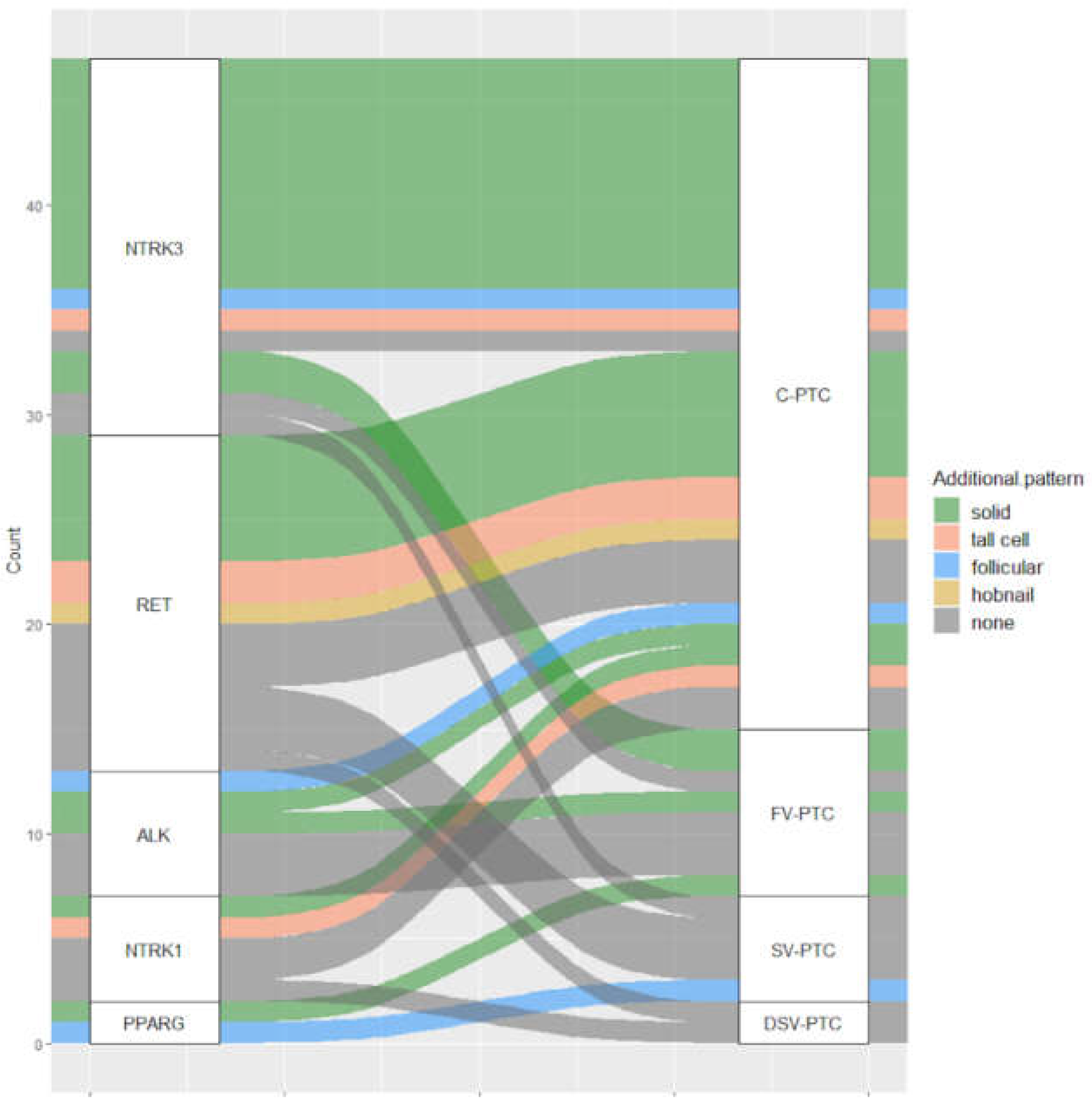
3.2. Molecular Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Francis, G.L.; Waguespack, S.G.; Bauer, A.J.; Angelos, P.; Benvenga, S.; Cerutti, J.; Dinauer, C.A.; Hamilton, J.K.; Hay, I.D.; Luster, M.; et al. Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid As-sociation Guidelines Task Force on Pediatric Thyroid Cancer. Thyroid 2015, 25, 716–759. [Google Scholar] [CrossRef] [Green Version]
- Zanella, A.B.; Scheffel, R.S.; Weinert, L.; Dora, J.M.; Maia, A.L. New insights into the management of differentiated thyroid carcinoma in children and adolescents (Review). Int. J. Oncol. 2021, 58, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dinauer, C.A.; Breuer, C.; Rivkees, S.A. Differentiated thyroid cancer in children: Diagnosis and management. Curr. Opin. Oncol. 2008, 20, 59–65. [Google Scholar] [CrossRef]
- Hogan, A.R.; Zhuge, Y.; Perez, E.A.; Koniaris, L.G.; Lew, J.I.; Sola, J. Pediatric Thyroid Carcinoma: Incidence and Outcomes in 1753 Patients. J. Surg. Res. 2009, 156, 167–172. [Google Scholar] [CrossRef]
- Koo, J.S.; Hong, S.; Park, C.S. Diffuse Sclerosing Variant Is a Major Subtype of Papillary Thyroid Carcinoma in the Young. Thyroid 2009, 19, 1225–1231. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, N.; Akbani, R.; Aksoy, B.A.; Ally, A.; Arachchi, H.; Asa, S.; Auman, J.T.; Balasundaram, M.; Balu, S.; Baylin, S.B.; et al. Integrated Genomic Characterization of Papillary Thyroid Carcinoma. Cell 2014, 159, 676–690. [Google Scholar] [CrossRef] [Green Version]
- Cordioli, M.I.C.V.; Moraes, L.; Bastos, A.U.; Besson, P.; Alves, M.T.D.S.; Delcelo, R.; Monte, O.; Longui, C.; Cury, A.N.; Cerutti, J.M. Fusion Oncogenes Are the Main Genetic Events Found in Sporadic Papillary Thyroid Carcinomas from Children. Thyroid 2017, 27, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Henke, L.E.; Perkins, S.M.; Pfeifer, J.D.; Ma, C.; Chen, Y.; DeWees, T.; Grigsby, P.W. BRAFV600E mutational status in pediatric thyroid cancer. Pediatr. Blood Cancer 2014, 61, 1168–1172. [Google Scholar] [CrossRef]
- Mostoufi-Moab, S.; Labourier, E.; Sullivan, L.; Livolsi, V.; Li, Y.; Xiao, R.; Beaudenon-Huibregtse, S.; Kazahaya, K.; Adzick, N.S.; Baloch, Z.; et al. Molecular Testing for Oncogenic Gene Alterations in Pediatric Thyroid Lesions. Thyroid 2018, 28, 60–67. [Google Scholar] [CrossRef]
- Sisdelli, L.; Cordioli, M.I.C.V.; Vaisman, F.; Moraes, L.; Colozza-Gama, G.A.; Alves, P.A.G.; Araújo, M.L.; Alves, M.T.S.; Monte, O.; Longui, C.A.; et al. AGK-BRAF is associated with distant metastasis and younger age in pediatric papillary thyroid carcinoma. Pediatr. Blood Cancer 2019, 66, e27707. [Google Scholar] [CrossRef]
- Hardee, S.; Prasad, M.L.; Hui, P.; Dinauer, C.A.; Morotti, R.A. Pathologic Characteristics, Natural History, and Prognostic Implications of BRAFV600E Mutation in Pediatric Papillary Thyroid Carcinoma. Pediatr. Dev. Pathol. 2017, 20, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Pekova, B.; Sykorova, V.; Dvorakova, S.; Vaclavikova, E.; Moravcova, J.; Katra, R.; Astl, J.; Vlcek, P.; Kodetova, D.; Vcelak, J.; et al. RET, NTRK, ALK, BRAF, and MET Fusions in a Large Cohort of Pediatric Papillary Thyroid Carcinomas. Thyroid 2020, 30, 1771–1780. [Google Scholar] [CrossRef]
- Alzahrani, A.S.; Murugan, A.K.; Qasem, E.; Alswailem, M.; Al-Hindi, H.; Shi, Y. Single Point Mutations in Pediatric Differentiated Thyroid Cancer. Thyroid 2017, 27, 189–196. [Google Scholar] [CrossRef]
- Alzahrani, A.S.; Alswailem, M.; Alswailem, A.A.; Al-Hindi, H.; Goljan, E.; Alsudairy, N.; Abouelhoda, M. Genetic Alterations in Pediatric Thyroid Cancer Using a Comprehensive Childhood Cancer Gene Panel. J. Clin. Endocrinol. Metab. 2020, 105, 3324–3334. [Google Scholar] [CrossRef]
- Galuppini, F.; Vianello, F.; Censi, S.; Barollo, S.; Bertazza, L.; Carducci, S.; Colato, C.; Manso, J.; Rugge, M.; Iacobone, M.; et al. Differentiated Thyroid Carcinoma in Pediatric Age: Genetic and Clinical Scenario. Front. Endocrinol. 2019, 10, 552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasad, M.L.; Vyas, M.; Horne, M.J.; Virk, R.K.; Morotti, R.; Liu, Z.; Tallini, G.; Nikiforova, M.N.; Christison-Lagay, E.R.; Udelsman, R.; et al. NTRK fusion oncogenes in pediatric papillary thyroid carcinoma in northeast United States: NTRK Fusion in Papillary Thy-roid Cancer. Cancer 2016, 122, 1097–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lloyd, R.; Osamura, R.; Kloppel, G.; Rosai, J. WHO Classification of Tumours of Endocrine Organs, 4th ed.; IARC Press: Lyon, France, 2017. [Google Scholar]
- Bruno, R.; Fontanini, G. Next Generation Sequencing for Gene Fusion Analysis in Lung Cancer: A Literature Review. Diagnostics 2020, 10, 521. [Google Scholar] [CrossRef]
- Chu, Y.-H.; Dias-Santagata, D.; Farahani, A.A.; Boyraz, B.; Faquin, W.C.; Nosé, V.; Sadow, P.M. Clinicopathologic and molecular characterization of NTRK-rearranged thyroid carcinoma (NRTC). Mod. Pathol. 2020, 33, 2186–2197. [Google Scholar] [CrossRef]
- Seethala, R.R.; Chiosea, S.I.; Liu, C.Z.; Nikiforova, M.; Nikiforov, Y.E. Clinical and Morphologic Features of ETV6-NTRK3 Translocated Papillary Thyroid Carcinoma in an Adult Population Without Radiation Exposure. Am. J. Surg. Pathol. 2017, 41, 446–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuels, S.L.; Surrey, L.F.; Hawkes, C.; Amberge, M.; Mostoufi-Moab, S.; Langer, J.E.; Adzick, N.S.; Kazahaya, K.; Bhatti, T.; Baloch, Z.; et al. Characteristics of Follicular Variant Papillary Thyroid Carcinoma in a Pediatric Cohort. J. Clin. Endocrinol. Metab. 2018, 103, 1639–1648. [Google Scholar] [CrossRef]
- Morariu, E.M.; McCoy, K.L.; Chiosea, S.I.; Nikitski, A.V.; Manroa, P.; Nikiforova, M.N.; Nikiforov, Y.E. Clinicopathologic Characteristics of Thyroid Nodules Positive for the THADA-IGF2BP3 Fusion on Preoperative Molecular Analysis. Thyroid 2021. [Google Scholar] [CrossRef]
- Alessandri, A.J.; Goddard, K.J.; Blair, G.K.; Fryer, C.J.; Schultz, K.R. Age is the major determinant of recurrence in pediatric differentiated thyroid carcinoma. Med. Pediatr. Oncol. 2000, 35, 41–46. [Google Scholar] [CrossRef]
- Grigsby, P.W.; Gal-Or, A.; Michalski, J.M.; Doherty, G.M. Childhood and adolescent thyroid carcinoma. Cancer 2002, 95, 724–729. [Google Scholar] [CrossRef] [PubMed]
- O’Gorman, C.S.; Hamilton, J.; Rachmiel, M.; Gupta, A.; Ngan, B.Y.; Daneman, D. Thyroid Cancer in Childhood: A Retrospective Review of Childhood Course. Thyroid 2010, 20, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Borson-Chazot, F.; Causeret, S.; Lifante, J.-C.; Augros, M.; Berger, N.; Peix, J.-L. Predictive Factors for Recurrence from a Series of 74 Children and Adolescents with Differentiated Thyroid Cancer. World J. Surg. 2004, 28, 1088–1092. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pediatric PTCs n = 163 | ||
|---|---|---|
| Age | ||
| median, range | 16, 8–18 | |
| <15-year-old | 61 (37.4%) | |
| ≥15-year-old | 102 (62.6%) | |
| Sex | ||
| Female | 116 (71.2%) | |
| Male | 47 (28.8) | |
| Tumor size [cm] | ||
| mean (SD) | 2.3 (1.3) | |
| PTC variant | ||
| C-PTC | 99 (60.7%) | |
| FV-PTC | 34 (20.9%) | |
| SV-PTC | 9 (5.5%) | |
| TCV-PTC | 7 (4.3%) | |
| DSV-PTC | 4 (2.5%) | |
| HCV-PTC | 1 (0.6%) | |
| Metastasis without primary tumor * | 1 (0.6%) | |
| NIFTP * | 8 (4.9%) | |
| Tumor invasiveness | ||
| Totally encapsulated | 14 (9.1%) | |
| Encapsulated with tumor capsule invasion | 20 (13.0%) | |
| Infiltration of thyroid parenchyma | 120 (77.9%) | |
| Extrathyroidal extension | ||
| Minimal | 47 (30.5%) | |
| Gross | 1 (0.7%) | |
| Absent | 106 (68.8%) | |
| Multifocality | ||
| Present | 69 (44.8%) | |
| Absent | 85 (55.2%) | |
| Lymphovascular invasion | ||
| Present | 65 (42.2%) | |
| Absent | 89 (57.8%) | |
| Tumor stage | ||
| T1a | 20 (13.0%) | |
| T1b | 68 (44.1%) | |
| T2 | 45 (29.2%) | |
| T3a | 20 (13.0%) | |
| T4a | 1 (0.7%) | |
| Lymph node metastasis | ||
| N0 | 22 (14.3%) | |
| N1a | 35 (22.7%) | |
| N1b | 27 (17.5%) | |
| NA | 70 (45.5%) | |
| Fusion n = 48 | Mutation n = 83 | Wild-Type n = 32 | p-Value | ||
|---|---|---|---|---|---|
| Age | |||||
| median, range | 14, 8–18 | 17, 8–18 | 16, 9–18 | < 0.0001 | |
| <15-year-old | 27 (56.3%) | 21 (25.3%) | 13 (40.6%) | 0.0018 | |
| ≥15-year-old | 21 (43.7%) | 62 (74.7%) | 19 (59.3%) | ||
| Sex | |||||
| Female | 34 (70.8%) | 59 (71.1%) | 23 (71.9%) | 0.9947 | |
| Male | 14 (29.2%) | 24 (28.9%) | 9 (28.1%) | ||
| Tumor size [cm] | |||||
| mean (SD) | 2.6 (1.2) | 2.1 (1.3) | 2.3 (1.5) | 0.0200 | |
| PTC variant | |||||
| C-PTC | 32 (66.7%) | 51 (61.4%) | 16 (50.0%) | 0.0955 | |
| FV-PTC | 8 (16.7%) | 17 (20.5%) | 9 (28.1%) | ||
| SV-PTC | 5 (10.4%) | 2 (2.4%) | 2 (6.2%) | ||
| TCV-PTC | 0 | 6 (7.2%) | 1 (3.1%) | ||
| DSV-PTC | 2 (4.2%) | 1 (1.2%) | 1 (3.1%) | ||
| Other a | 1 (2.1%) | 1 (1.2%) | 0 | ||
| NIFTP b | 0 | 5 (6.0%) | 3 (9.4%) | ||
| Tumor invasiveness | |||||
| Totally encapsulated | 0 | 6 (7.7%) | 8 (27.6%) | 0.0003 | |
| Encapsulated with tumor capsule invasion | 3 (6.4%) | 10 (12.8%) | 7 (24.1%) | ||
| Infiltration of thyroid parenchyma | 44 (93.6%) | 62 (79.5%) | 14 (48.3%) | ||
| Extrathyroidal extension | |||||
| Present c | 24 (51.1%) | 21 (26.9%) | 3 (10.3%) | 0.0005 | |
| Absent | 23 (48.9%) | 57 (73.1%) | 26 (89.7%) | ||
| Multifocality | |||||
| Present | 27 (57.4%) | 33 (42.3%) | 9 (31.0%) | 0.0652 | |
| Absent | 20 (42.6%) | 45 (57.7%) | 20 (69.0%) | ||
| Lymphovascular invasion | |||||
| Present | 31 (66.0%) | 29 (37.2%) | 5 (17.2%) | < 0.0001 | |
| Absent | 16 (34.0%) | 49 (62.8%) | 24 (82.8%) | ||
| Tumor stage d | |||||
| T1a | 2 (4.2%) | 14 (18.0%) | 4 (13.8%) | 0.0783 | |
| T1b | 17 (36.2%) | 37 (47.4%) | 14 (48.3%) | ||
| T2 | 20 (42.6%) | 17 (21.8%) | 8 (27.6%) | ||
| T3a | 7 (14.9%) | 10 (12.8%) | 3 (10.3%) | ||
| T4a | 1 (2.1%) | 0 | 0 | ||
| Lymph node metastasis | |||||
| N0 | 7 (14.9%) | 10 (12.8%) | 5 (17.2%) | 0.0489 | |
| N1a | 11 (23.4%) | 18 (23.1%) | 6 (20.7%) | ||
| N1b | 18 (38.3%) | 6 (7.7%) | 3 (10.3%) | ||
| NA | 11 (23.4%) | 44 (56.4%) | 15 (51.7%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Macerola, E.; Proietti, A.; Poma, A.M.; Ugolini, C.; Torregrossa, L.; Vignali, P.; Basolo, A.; Materazzi, G.; Elisei, R.; Santini, F.; et al. Molecular Alterations in Relation to Histopathological Characteristics in a Large Series of Pediatric Papillary Thyroid Carcinoma from a Single Institution. Cancers 2021, 13, 3123. https://doi.org/10.3390/cancers13133123
Macerola E, Proietti A, Poma AM, Ugolini C, Torregrossa L, Vignali P, Basolo A, Materazzi G, Elisei R, Santini F, et al. Molecular Alterations in Relation to Histopathological Characteristics in a Large Series of Pediatric Papillary Thyroid Carcinoma from a Single Institution. Cancers. 2021; 13(13):3123. https://doi.org/10.3390/cancers13133123
Chicago/Turabian StyleMacerola, Elisabetta, Agnese Proietti, Anello Marcello Poma, Clara Ugolini, Liborio Torregrossa, Paola Vignali, Alessio Basolo, Gabriele Materazzi, Rossella Elisei, Ferruccio Santini, and et al. 2021. "Molecular Alterations in Relation to Histopathological Characteristics in a Large Series of Pediatric Papillary Thyroid Carcinoma from a Single Institution" Cancers 13, no. 13: 3123. https://doi.org/10.3390/cancers13133123