Comparison of NGS and MFC Methods: Key Metrics in Multiple Myeloma MRD Assessment

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
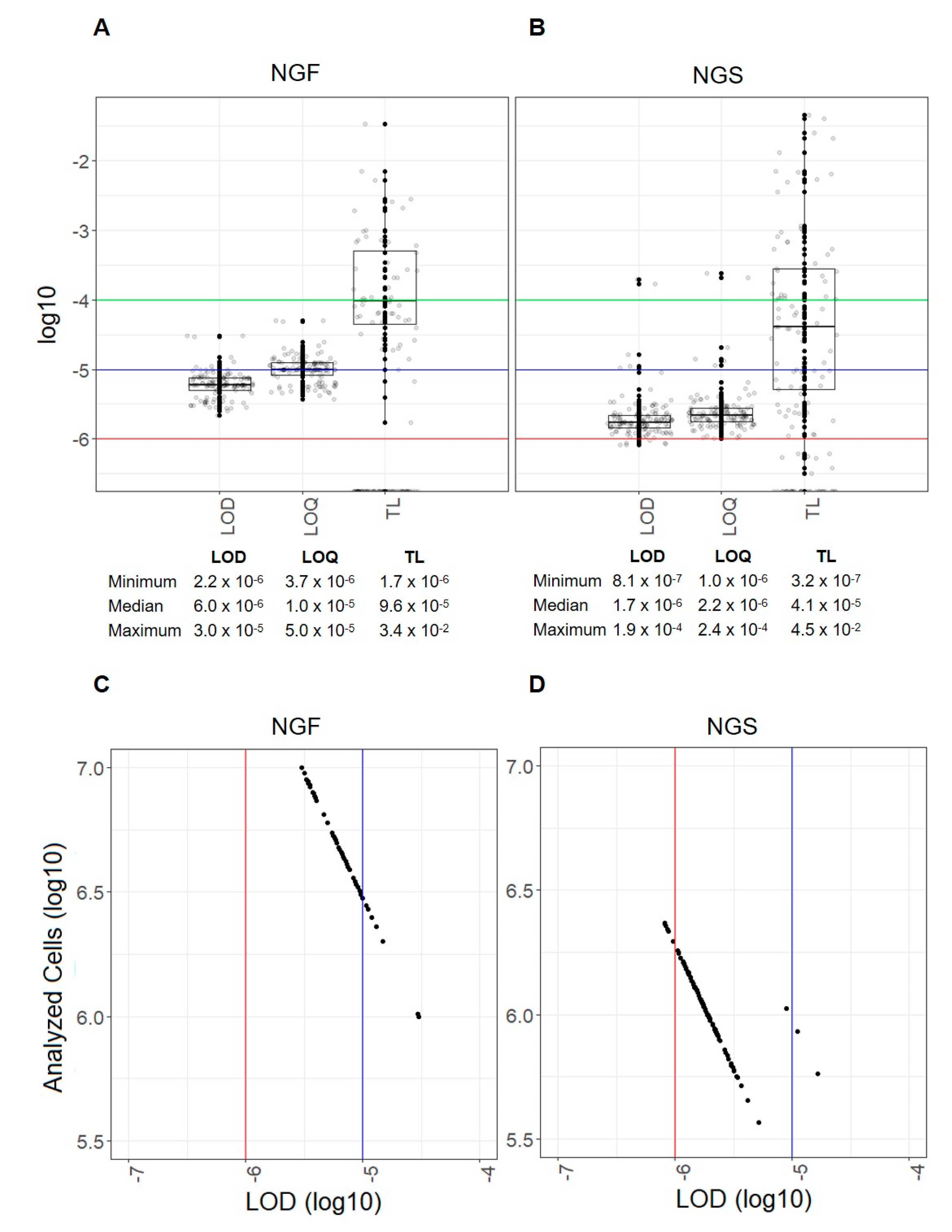
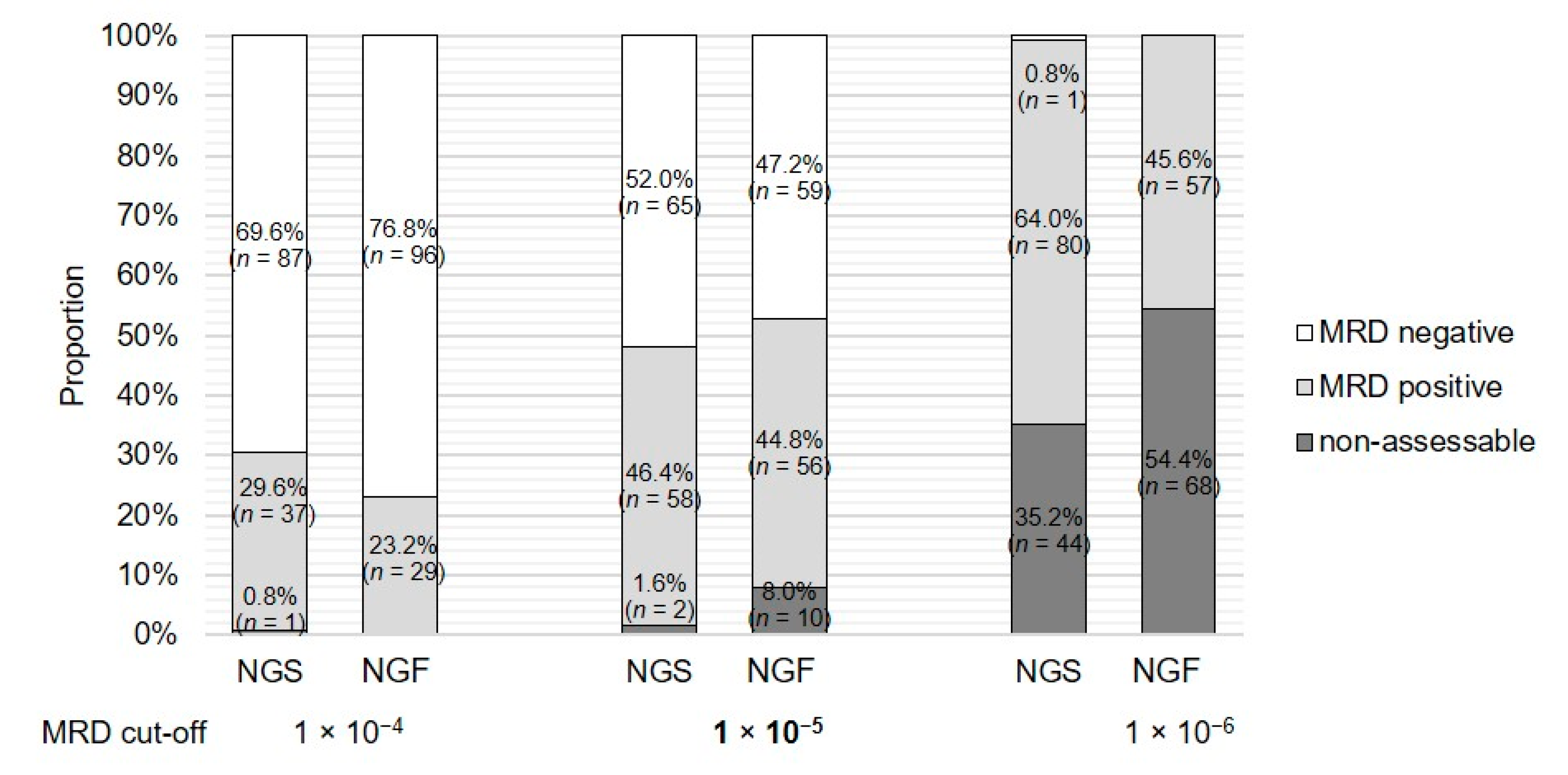
2.1. The Amount of Available Sample Is Crucial and Affects the Evaluation and Comparison of Results at Specific MRD Cut-offs
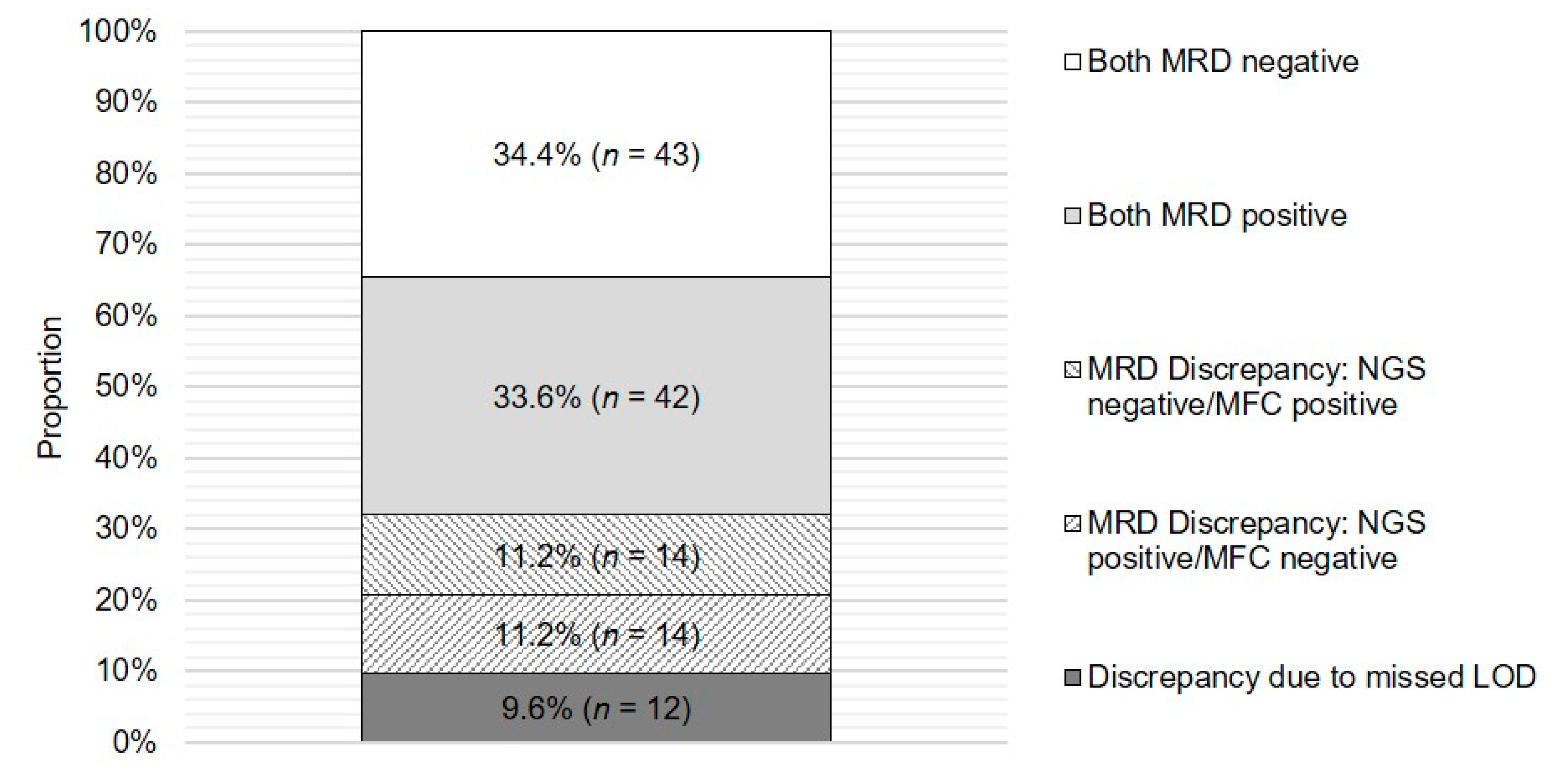
2.2. The Concordance of NGS and MFC MRD Results Reaches Almost 70%
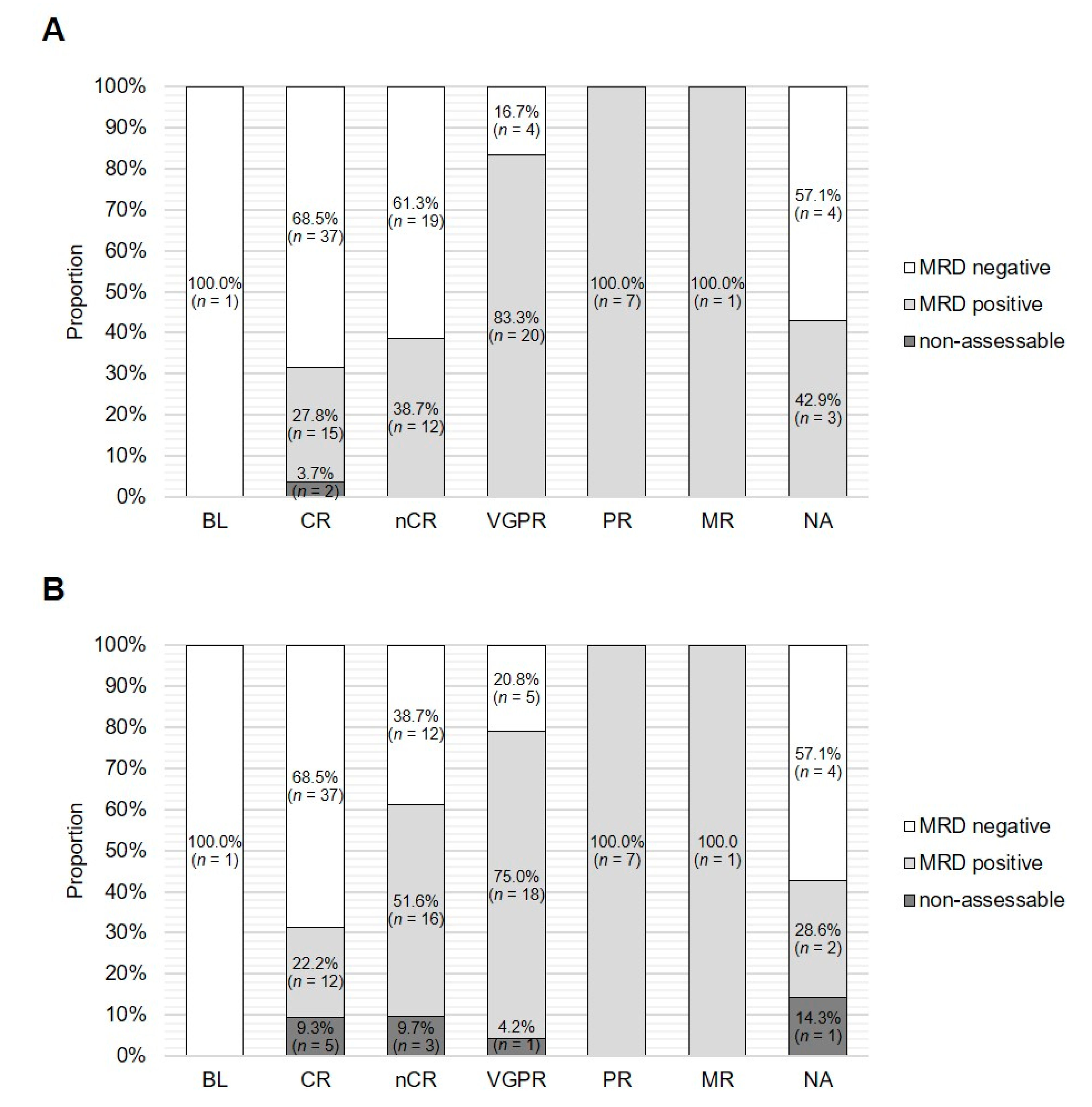
2.3. MRD Status Obtained with Both Assays Corresponds to Serological Response
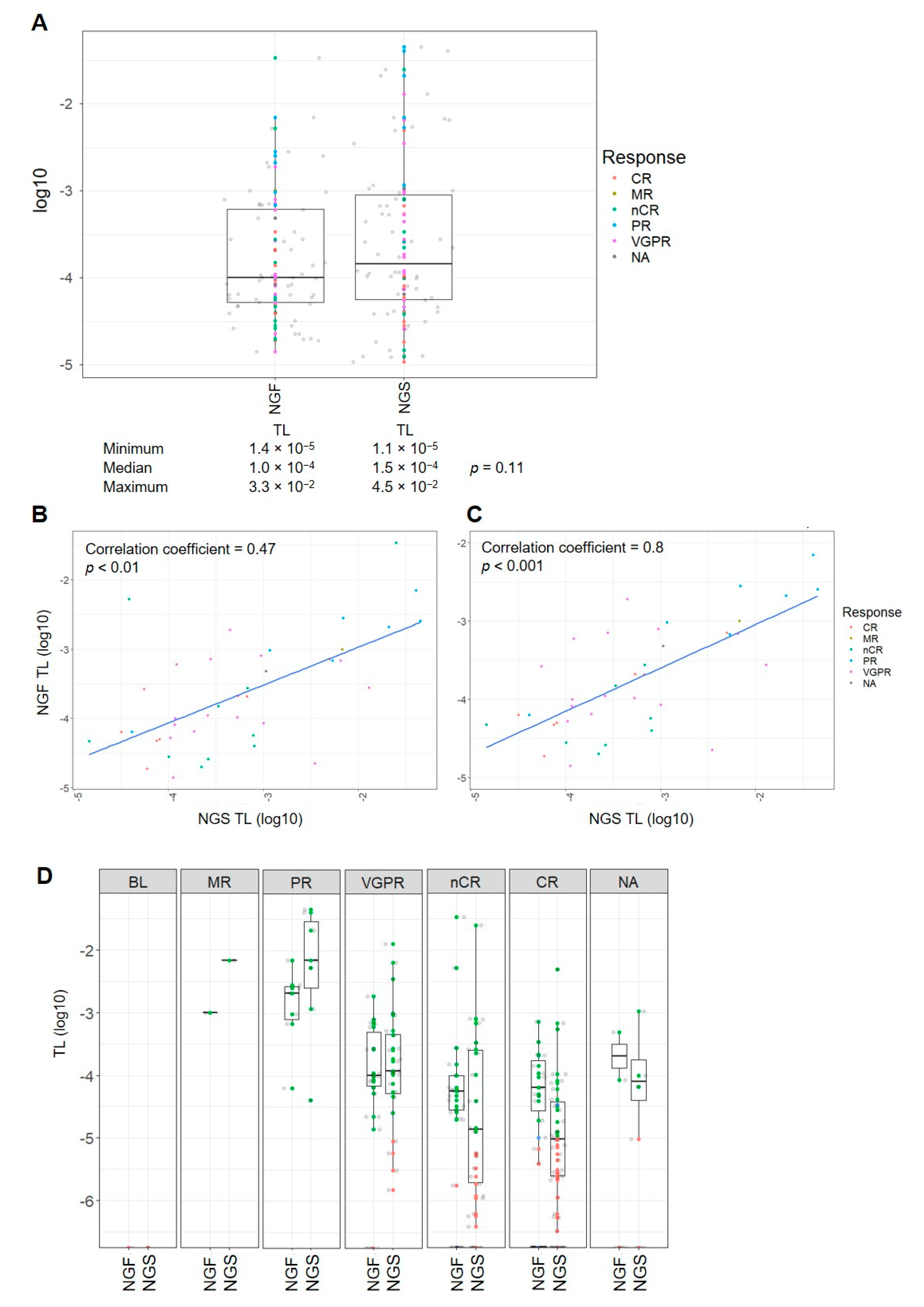
2.4. The Tumor Load of MRD-Positive Cases Is Comparable with Both Assays
3. Discussion
4. Materials and Methods
4.1. Patient Cohort and Sample Matching
4.2. MRD Assessment by NGS
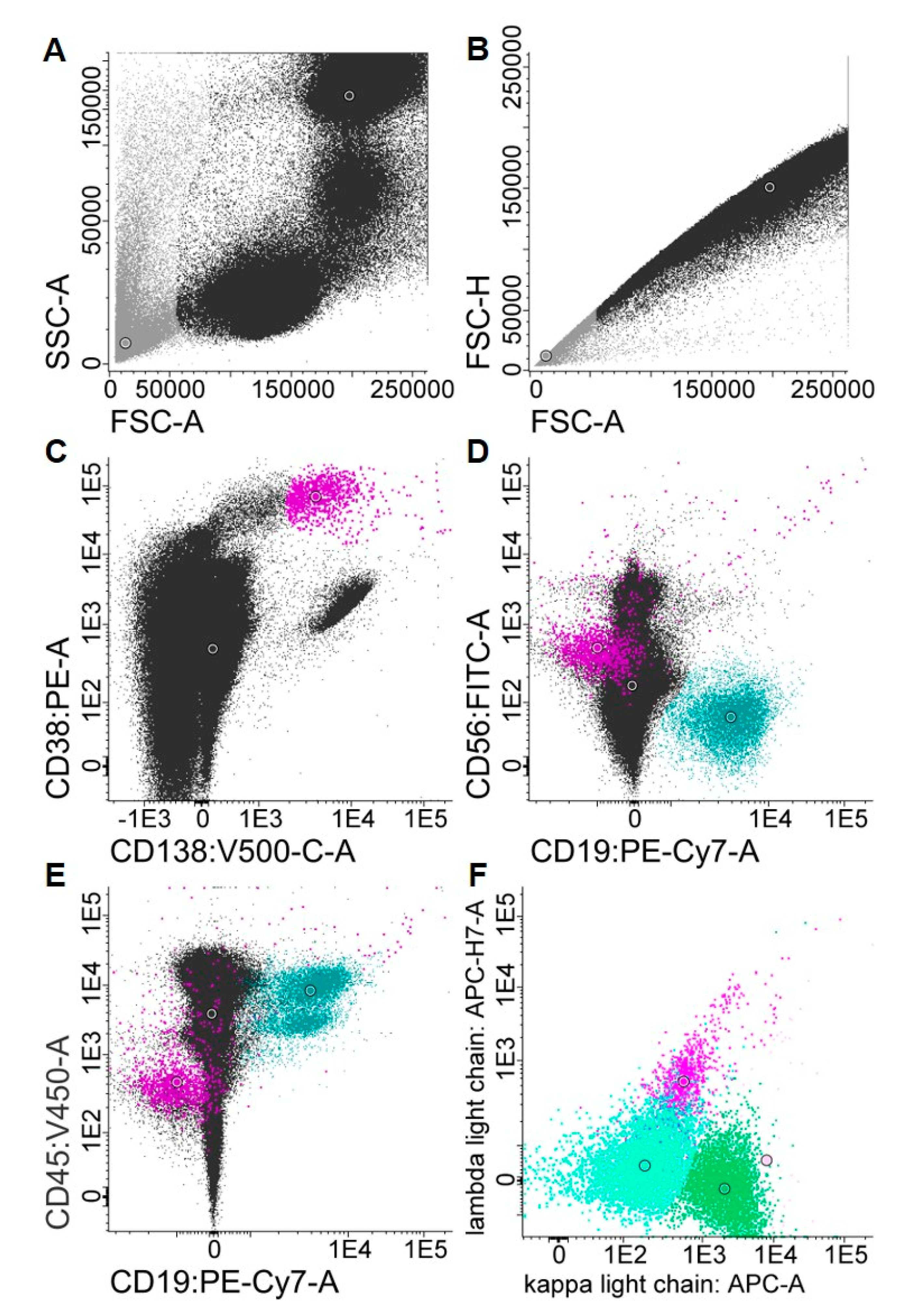
4.3. MRD Assessment by MFC
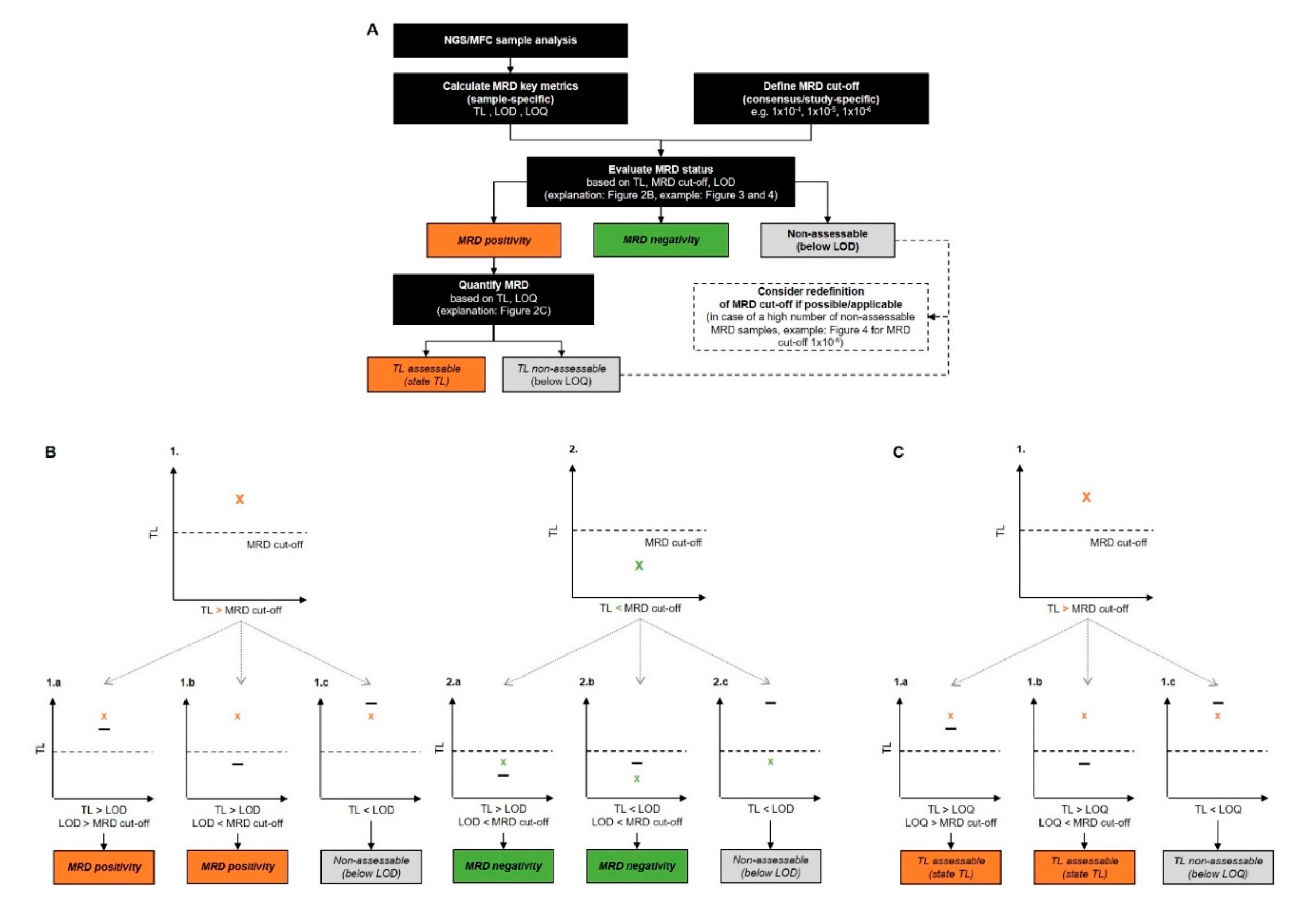
4.4. Calculation of MRD Key Metrics
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bai, Y.; Orfao, A.; Chim, C.S. Molecular detection of minimal residual disease in multiple myeloma. Br. J. Haematol. 2018, 181, 11–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flores-Montero, J.; Sanoja-Flores, L.; Paiva, B.; Puig, N.; Garcia-Sanchez, O.; Bottcher, S.; van der Velden, V.H.J.; Perez-Moran, J.J.; Vidriales, M.B.; Garcia-Sanz, R.; et al. Next Generation Flow for highly sensitive and standardized detection of minimal residual disease in multiple myeloma. Leukemia 2017, 31, 2094–2103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherrod, A.M.; Hari, P.; Mosse, C.A.; Walker, R.C.; Cornell, R.F. Minimal residual disease testing after stem cell transplantation for multiple myeloma. Bone Marrow Transpl. 2016, 51, 2–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paiva, B.; van Dongen, J.J.; Orfao, A. New criteria for response assessment: Role of minimal residual disease in multiple myeloma. Blood 2015, 125, 3059–3068. [Google Scholar] [CrossRef] [Green Version]
- Vogel, W.; Kopp, H.G.; Kanz, L.; Einsele, H. Myeloma cell contamination of peripheral blood stem-cell grafts can predict the outcome in multiple myeloma patients after high-dose chemotherapy and autologous stem-cell transplantation. J. Cancer Res. Clin. Oncol. 2005, 131, 214–218. [Google Scholar] [CrossRef]
- Galimberti, S.; Morabito, F.; Guerrini, F.; Palumbo, G.A.; Azzara, A.; Martino, M.; Benedetti, E.; Di Raimondo, F.; Petrini, M. Peripheral blood stem cell contamination evaluated by a highly sensitive molecular method fails to predict outcome of autotransplanted multiple myeloma patients. Br. J. Haematol. 2003, 120, 405–412. [Google Scholar] [CrossRef]
- Munshi, N.C.; Avet-Loiseau, H.; Rawstron, A.C.; Owen, R.G.; Child, J.A.; Thakurta, A.; Sherrington, P.; Samur, M.K.; Georgieva, A.; Anderson, K.C.; et al. Association of Minimal Residual Disease with Superior Survival Outcomes in Patients with Multiple Myeloma: A Meta-analysis. JAMA Oncol. 2017, 3, 28–35. [Google Scholar] [CrossRef]
- Landgren, O.; Devlin, S.; Boulad, M.; Mailankody, S. Role of MRD status in relation to clinical outcomes in newly diagnosed multiple myeloma patients: A meta-analysis. Bone Marrow Transpl. 2016, 51, 1565–1568. [Google Scholar] [CrossRef] [Green Version]
- Landgren, O. MRD Testing in Multiple Myeloma: From a Surrogate Marker of Clinical Outcomes to an Every-Day Clinical Tool. Semin. Hematol. 2018, 55, 1–3. [Google Scholar] [CrossRef]
- Smith, J. FDA issues draft guidance on MRD. Available online: https://www.mdedge.com/hematology-oncology/article/184647/leukemia-myelodysplasia-transplantation/fda-issues-draft-guidance-mrd (accessed on 25 March 2019).
- FDA. FDA Authorizes First Next Generation Sequencing-Based Test to Detect very Low Levels of Remaining Cancer Cells in Patients with Acute Lymphoblastic Leukemia or Multiple Myeloma. Available online: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm622004.htm (accessed on 24 March 2019).
- EMA. Guideline on the Use of Minimal Residual Disease as a Clinical Endpoint in Multiple Myeloma Studies. Available online: https://www.ema.europa.eu/en/guideline-use-minimal-residual-disease-clinical-endpoint-multiple-myeloma-studies (accessed on 15 January 2020).
- Mina, R.; Oliva, S.; Boccadoro, M. Minimal Residual Disease in Multiple Myeloma: State of the Art and Future Perspectives. J. Clin. Med. 2020, 9, 2142. [Google Scholar] [CrossRef]
- Arroz, M.; Came, N.; Lin, P.; Chen, W.; Yuan, C.; Lagoo, A.; Monreal, M.; de Tute, R.; Vergilio, J.A.; Rawstron, A.C.; et al. Consensus guidelines on plasma cell myeloma minimal residual disease analysis and reporting. Cytom. B Clin. Cytom. 2016, 90, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Avet-Loiseau, H. Minimal Residual Disease by Next-Generation Sequencing: Pros and Cons. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e425–e430. [Google Scholar] [CrossRef]
- Cloos, J.; Harris, J.R.; Janssen, J.; Kelder, A.; Huang, F.; Sijm, G.; Vonk, M.; Snel, A.N.; Scheick, J.R.; Scholten, W.J.; et al. Comprehensive Protocol to Sample and Process Bone Marrow for Measuring Measurable Residual Disease and Leukemic Stem Cells in Acute Myeloid Leukemia. J. Vis. Exp. 2018, 133, e56386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stetler-Stevenson, M.; Paiva, B.; Stoolman, L.; Lin, P.; Jorgensen, J.L.; Orfao, A.; Van Dongen, J.; Rawstron, A.C. Consensus guidelines for myeloma minimal residual disease sample staining and data acquisition. Cytom. B Clin. Cytom. 2016, 90, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Moreau, P.; Zamagni, E. MRD in multiple myeloma: More questions than answers? Blood Cancer J. 2017, 7, 639. [Google Scholar] [CrossRef]
- Korde, N.; Roschewski, M.; Zingone, A.; Kwok, M.; Manasanch, E.E.; Bhutani, M.; Tageja, N.; Kazandjian, D.; Mailankody, S.; Wu, P.; et al. Treatment with Carfilzomib-Lenalidomide-Dexamethasone with Lenalidomide Extension in Patients with Smoldering or Newly Diagnosed Multiple Myeloma. JAMA Oncol. 2015, 1, 746–754. [Google Scholar] [CrossRef] [Green Version]
- ClinicalTrials.gov. A Phase III Trial on the Effect of Elotuzumab in VRD Induction/Consolidation and Lenalidomide Maintenance in Patients with Newly Diagnosed Myeloma (GMMG-HD6). Available online: https://clinicaltrials.gov/ct2/show/NCT02495922 (accessed on 25 March 2019).
- Salwender, H.; Bertsch, U.; Weisel, K.; Duerig, J.; Kunz, C.; Benner, A.; Blau, I.W.; Raab, M.S.; Hillengass, J.; Hose, D.; et al. Rationale and design of the German-speaking myeloma multicenter group (GMMG) trial HD6: A randomized phase III trial on the effect of elotuzumab in VRD induction/consolidation and lenalidomide maintenance in patients with newly diagnosed myeloma. BMC Cancer 2019, 19, 504. [Google Scholar] [CrossRef] [Green Version]
- Kumar, S.; Paiva, B.; Anderson, K.C.; Durie, B.; Landgren, O.; Moreau, P.; Munshi, N.; Lonial, S.; Blade, J.; Mateos, M.V.; et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. 2016, 17, e328–e346. [Google Scholar] [CrossRef]
- Pulsipher, M.A.; Carlson, C.; Langholz, B.; Wall, D.A.; Schultz, K.R.; Bunin, N.; Kirsch, I.; Gastier-Foster, J.M.; Borowitz, M.; Desmarais, C.; et al. IgH-V(D)J NGS-MRD measurement pre- and early post-allotransplant defines very low- and very high-risk ALL patients. Blood 2015, 125, 3501–3508. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Lopez, J.; Lahuerta, J.J.; Pepin, F.; Gonzalez, M.; Barrio, S.; Ayala, R.; Puig, N.; Montalban, M.A.; Paiva, B.; Weng, L.; et al. Prognostic value of deep sequencing method for minimal residual disease detection in multiple myeloma. Blood 2014, 123, 3073–3079. [Google Scholar] [CrossRef]
- Robillard, N.; Wuilleme, S.; Moreau, P.; Bene, M.C. Immunophenotype of normal and myelomatous plasma-cell subsets. Front. Immunol. 2014, 5, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawstron, A.C.; Orfao, A.; Beksac, M.; Bezdickova, L.; Brooimans, R.A.; Bumbea, H.; Dalva, K.; Fuhler, G.; Gratama, J.; Hose, D.; et al. Report of the European Myeloma Network on multiparametric flow cytometry in multiple myeloma and related disorders. Haematologica 2008, 93, 431–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gamer, M.; Lemon, J.; PuspendraSingh, I.F. irr: Various Coefficients of Interrater Reliability and Agreement. Available online: https://cran.r-project.org/web/packages/irr/index.html (accessed on 15 January 2020).
- Wickham, H. The Split-Apply-Combine Strategy for Data Analysis. J. Stat. Softw. 2011, 40, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer-Verlag New York: New York, NY, USA, 2016; pp. 41–62. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients, n | 125 |
|---|---|
| Median age, years (range) | 59 (33–70) |
| Gender, n (%) | |
| Female | 53 (42.4) |
| Male | 72 (57.6) |
| Heavy chain type, n (%) | |
| IgA | 24 (19.2) |
| IgD | 1 (0.8) |
| IgE | 1 (0.8) |
| IgG | 67 (53.6) |
| IgM | 2 (1.6) |
| LC | 30 (24.0) |
| Light chain type, n (%) | |
| κ | 78 (62.4) |
| λ | 47 (37.6) |
| Median BM plasma cells, % (range) | |
| Cytology | 40 (2–100) |
| Histopathology | 40 (1–98) |
| Median β2-microglobulin, mg/L (range) | 3.9 (1.1–24) |
| Median Albumin, g/L (range) | 36.9 (20.3–49.3) |
| ISS, n (%) | |
| I | 44 (35.2) |
| II | 53 (42.4) |
| III | 28 (22.4) |
| Timepoint of MRD assessment, n (%) | |
| Baseline | 1 (0.8) |
| Pos Iinduction | 22 (17.6) |
| Post Mobilization | 1 (0.8) |
| Post-HD-CT/ASCT 1 | 57 (45.6) |
| Post-HD-CT/ASCT 2 | 2 (1.6) |
| Post Consolidation | 41 (32.8) |
| NA | 1 (0.8) |
| Serological remission, n (%) | |
| Baseline | 1 (0.8) |
| CR | 54 (43.2) |
| nCR | 31 (24.8) |
| VGPR | 24 (19.2) |
| PR | 7 (5.6) |
| MR | 1 (0.8) |
| NA | 7 (5.6) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kriegsmann, K.; Hundemer, M.; Hofmeister-Mielke, N.; Reichert, P.; Manta, C.-P.; Awwad, M.H.S.; Sauer, S.; Bertsch, U.; Besemer, B.; Fenk, R.; et al. Comparison of NGS and MFC Methods: Key Metrics in Multiple Myeloma MRD Assessment. Cancers 2020, 12, 2322. https://doi.org/10.3390/cancers12082322
Kriegsmann K, Hundemer M, Hofmeister-Mielke N, Reichert P, Manta C-P, Awwad MHS, Sauer S, Bertsch U, Besemer B, Fenk R, et al. Comparison of NGS and MFC Methods: Key Metrics in Multiple Myeloma MRD Assessment. Cancers. 2020; 12(8):2322. https://doi.org/10.3390/cancers12082322
Chicago/Turabian StyleKriegsmann, Katharina, Michael Hundemer, Nicole Hofmeister-Mielke, Philipp Reichert, Calin-Petru Manta, Mohamed H.S. Awwad, Sandra Sauer, Uta Bertsch, Britta Besemer, Roland Fenk, and et al. 2020. "Comparison of NGS and MFC Methods: Key Metrics in Multiple Myeloma MRD Assessment" Cancers 12, no. 8: 2322. https://doi.org/10.3390/cancers12082322